การกินธาตุเหลก็เกินขนาดResemblance of iron tablets to...
16
การกินธาตุเหล็กเกินขนาด เสาวณีย์ สว่าง นักศึกษาแพทย์ปีที่ 6 ภาควิชาเวชศาสตร์ฉุกเฉิน โรงพยาบาลรามาธิบดี ผู้ป่วยหญิงไทยอายุ 18 ปี มาโรงพยาบาลด้วยเรื่องปวดท้องประมาณ 1 ชั่วโมง โดยมีประวัติ ประทานยาบารุงเลือด 50 เม็ด ก่อนมีอาการปวดเนื่องจากทะเลาะกับสามี ได้ประวัติเพิ่มเติมจากผู้ป ่ วยว่า ขณะนี ้ตั ้งครรภ์ได ้ประมาณ 2 เดือน ตรวจร่างกายในผู้ป่วยรายนี ้เบื ้องต ้นพบว่า ผู้ป่วยตื่นรู้ตัวดี พูดคุยรู้เรื่อง ไม่ซึม ไม่มีไข้ หายใจหอบเหนื่อยเล็กน้อยอัตราการหายใจ 24 ครั ้ง/นาที ชีพจรเต้น 86 ครั ้งต่อนาที ความดัน ปกติ ตรวจร่างกายระบบหัวใจและหลอดเลือดอยู ่ในเกณฑ์ปกติ การหายใจอยู ่ในเกณฑ์ปกติ ตรวจระบบ ทางเดินอาหารหน้าท้องกดนุ่ม ไม่โป่งตึง คลาไม่พบตับและม้าม ตรวจร่างกายระบบประสาท รู้ตัวดีตลอด ไม่ซึม ไม่มีอ่อนแรง รูม่านตา 3 mm ตอบสนองดี ผลการตรวจเลือด พบ CBC: Hb 13.6%, Hct 39.4% ,WBC 17,800 /cumm ( N 86%,L11%,Mono 3%), platelet 330,000/cumm Coagulogram: aPTT 27.5 sec, PT 14.6 sec, INR 1.25, TT 10.5 sec ค่าเกลือแร่และค่าการทางานของไตอยู ่ในเกณฑ์ปกติ ค่าการทางานของตับอยู ่ในเกณฑ์ปกติ ผลการตรวจภาพถ่ายรังสี X-ray ในช่องท้องไม่พบลักษณะผิดปกติ การตรวจคลื่นไฟฟ้าหัวใจอยู ่ใน เกณฑ์ปกติ อภิปราย แพทย์ได้ให้ความเห็นในการวินิจฉัยผู้ป่วยรายนี ้ว่าเป็นภาวะ Iron toxicity เนื่องจากในผู้ป ่ วยรายนี ้ ได้รับประทานยาเข้าไปเกินขนาด ซึ ่งปริมาณ Iron element ที่รับประทานเท่ากับ
Transcript of การกินธาตุเหลก็เกินขนาดResemblance of iron tablets to...

การกนธาตเหลกเกนขนาด
เสาวณย สวาง
นกศกษาแพทยปท 6
ภาควชาเวชศาสตรฉกเฉน
โรงพยาบาลรามาธบด
ผปวยหญงไทยอาย 18 ป มาโรงพยาบาลดวยเรองปวดทองประมาณ 1 ชวโมง โดยมประวต
ประทานยาบ ารงเลอด 50 เมด กอนมอาการปวดเนองจากทะเลาะกบสาม ไดประวตเพมเตมจากผปวยวา
ขณะนตงครรภไดประมาณ 2 เดอน ตรวจรางกายในผปวยรายนเบองตนพบวา ผปวยตนรตวด พดคยรเรอง
ไมซม ไมมไข หายใจหอบเหนอยเลกนอยอตราการหายใจ 24 ครง/นาท ชพจรเตน 86 ครงตอนาท ความดน
ปกต ตรวจรางกายระบบหวใจและหลอดเลอดอยในเกณฑปกต การหายใจอยในเกณฑปกต ตรวจระบบ
ทางเดนอาหารหนาทองกดนม ไมโปงตง คล าไมพบตบและมาม ตรวจรางกายระบบประสาท รตวดตลอด
ไมซม ไมมออนแรง รมานตา 3 mm ตอบสนองด
ผลการตรวจเลอด พบ
CBC: Hb 13.6%, Hct 39.4% ,WBC 17,800 /cumm ( N 86%,L11%,Mono 3%), platelet 330,000/cumm
Coagulogram: aPTT 27.5 sec, PT 14.6 sec, INR 1.25, TT 10.5 sec
คาเกลอแรและคาการท างานของไตอยในเกณฑปกต คาการท างานของตบอยในเกณฑปกต
ผลการตรวจภาพถายรงส X-ray ในชองทองไมพบลกษณะผดปกต การตรวจคลนไฟฟาหวใจอยใน
เกณฑปกต
อภปราย
แพทยไดใหความเหนในการวนจฉยผปวยรายนวาเปนภาวะ Iron toxicity เนองจากในผปวยรายน
ไดรบประทานยาเขาไปเกนขนาด ซงปรมาณ Iron element ทรบประทานเทากบ

(300 mg/tab) x 50 tab x (33% iron/tab) = 4950 mg คดเปน 110 mg/kg ซงมโอกาสเกด severe toxicity
ท Emergency department ในผปวยรายนไดท าการ Primary survey A B C D ผาน ไดท าการรกษาเบองตน
คอ ท า Gastric lavage เพอ Gastrointestinal decontamination และไดให polyethylene glycol 2L/h ในการ
ท า Whole bowel irrigation ตอมาเจาะ serum iron level = 257 mg/dl (ในผปวยรายนเจาะท 5 ชวโมง ซงไม
ตรง Peak ปกตท 4 ชวโมงซงสมพนธกบอาการมากทสด) ผลเจาะตรวจ Arterial blood gas เปน Metabolic
acidosis with wide anion gap และไดให Antidote Deferoxamine 1 g IV in first 4 h then 0.5 g IV q 4 h x 2
doses
Iron poisoning
เหลก เปนโลหะหนกทมการใชเปนยามากทสดในเวชปฏบต โดยเปนยารกษาภาวะซดจากการขาดเหลก ซง
มกจะอยในรปของเกลอเชน Ferrous gluconate, Ferrous sulfate,
Ferrous fumarate เปนตน เนองจาก เปนยา ทหาไดงาย การสงยาแก
ผปวยมกจะเปนจ านวนครงละมากๆ ประกอบกบรปแบบของ เมดยา
มกเปนรปของ เมดเคลอบน าตาล สตางๆ ท า ใหเกดภาวะเปนพษได
บอยในเดกโดยเขาใจวาเปนลกอม
Epidemiology
Incidence >4,000 รายตอป จากการรายงานของ Association of Poison Control Centers (AAPCC)
Risk Factors
การเกบรกษายาทมธาตเหลกเปนสวนประกอบโดยทเดกสามารถเขาถงได
งายๆ ท าใหเกดการรบประทานธาตเหลกโดยไมไดตงใจ
คณแมทก าลงตงครรภ หรอหลงคลอดบตร 6 เดอนทไดรบธาตเหลกเปนยา
บ ารง

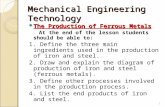
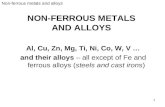
Resemblance of iron tablets to candy.
At left, from top, ferrous sulfate 300
mg, ferrous fumarate 200 mg and
ferrous gluconate 300 mg. These tablets
contain 60, 66 and 36 mg of elemental
iron respectively.
Pharmacology and Toxicokinetic
ธาตเหลกเปนสวนประกอบส าคญในการท างานของอวยวะระบบตางๆในรางกาย โดยธาตเหลกจะ
เปลยนจาก Fe3+ เปน Fe2+ ซงจะไปมบทบาทในการท างานของ protein และ enzymes ตางๆในรางกาย และ
เปนสวนประกอบของ Hemoglobin และ erythrocytes ถารางกายมธาตเหลกไมเพยงพอจะท าใหเกด ภาวะ
ซด ในทางตรงกนขามถารางกายมธาตเหลกมากเกนไปท าใหเกด Hemochromatosis คอการท ferrous ion
ขดขวางตอ lipid peroxidase ของ organelles ตางๆ ใน cells และ lysosomes ท าใหมการท าลายเซลลตางๆ
อวยวะทเกยวของคอตบ หวใจ ตบออน ขอตางๆ โดยเฉพาะขอขนาดเลก และอวยวะของตอมไรทอตาง ๆ
ผปวยเกดกลมอาการจากความผดปกตอวยวะดงกลาวขางตนชา ๆ
รางกายของเรานนไมสามารถทจะก าจดธาตเหลกไดโดยตรง รางกายเราจงมกลไกในการควบคม
ปรมาณธาตเหลกในรางกายโดยการควบคมผานการดดซมทางระบบทางเดนอาหาร ธาตเหลกจะถกดดซม
มากทสดทบรเวณล าไสเลกสวนตน (Duodenum) โดยการดดซมจะมากหรอนอยขนอยกบความตองการของ
รางกาย ในภาวะทรางกายขอดแคลนธาตเหลก จะมการเพมการดดซมขนจากภาวะปกตคอ 10 – 35% เปน 80
– 95% โดยธาตเหลกจะถกเกบไวใน cell ในรปของ Ferritin และจะหายไปเมอ cell หลดลอก หรอ ถกปลอย
ไปเปน Transferrin (Serum iron-binding protein) ซงในภาวะทธาตเหลกอยใน Therapeutic doses
กระบวนการดดซมจะมการอมตว และการดดซมเขาส intestinal cells จะถกจ ากด แตในภาวะธาตเหลกเกน
ในรางกาย Oxidative effects ของธาตเหลกตอ cell เยอบล าไส จะท าใหการควบคมการท างานของธาตเหลก
ผดปกต เพม passive absorption ของธาตเหลก ท าใหเกดภาวะเสยสมดล

Toxicity
Elemental Fe Peak serum concentration Toxicity < 20 mg/kg 50 – 150 μg/dL none 20 – 40 mg/kg 150 – 300 μg/dL mild 40 – 60 mg/kg 300 – 500 μg/dL Moderate >60 mg/kg >500 μg/dL severe Local Toxicity
ฤทธในการกดกรอนตอ gastric and intestinal mucosa คลนไส อาเจยน ปวดทอง ทองเสย ถายเหลว เลอดออกในทางเดนอาหาร ล าไสทะล, Peritonitis
Systemic Toxicity Ferrous iron (Fe2+) ---------> ferric iron (Fe3+) + hydrogen ion Cellular concentration in mitochondria ---------> inhibits oxidative phosphorylation ---------->
anaerobic metabolism, lactic acidosis, cellular/tissue/organ death Inhibits thrombin formation -----------> coagulopathy Direct negative ionotrope -------> hypotension Hemorrhagic periportal liver necrosis Vasodilation thus hypovolemic Mechanisms of increased anion-gap metabolic acidosis
- Fe2+-----> Fe3+ + H+ - Anaerobic metabolism: lactate - Hypovolemia from V/D: lactate - Hypovolemia from GI bleed: lactate - Negative ionotropy: lactate - Vasodilation: lactate
ธาตเหลกนนมอยในหลายรปแบบ ไดแก Iron salt: Ferrous gluconate, Ferrous sulfate, and Ferrous
fumarate ในรปแบบ nonionic preparations: carbonyl iron and polysaccharide iron นอกจากนยงมอยใน
รปแบบของวตามนรวมตางๆ เชน Prenatal vitamin, Children vitamin เปนตน

ตารางแสดง Common iron formulations และปรมาณธาตเหลก
Iron Formulation Elemental Iron Ionic Ferrous chloride 28% Ferrous fumarate 33% Ferrous gluconate 12% Ferrous lactate 19% Ferrous sulfate 20% Nonionic Carbonyl iron 98% Iron polysaccharide 46% Prenatal vitamin จะมสวนประกอบของธาตเหลกแตกตางกนอยในชวง 60 – 90 mg/tablet
วตามนของเดก จะมปรมาณธาตเหลกอยในชวง 5 – 18 mg/tablet
ดงนน ในFerrous sulfate 1 tablet(325mg) จะม iron element เทากบ65mg ดงนน ใน serious
toxicity จะเทากบการรบประทาน ferrous sulfate 1 tablet/kg
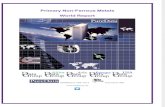
Ferrous sulfate
Ferrous gluconate
Ferrous fumarate

Pathophysiology
ธาตเหลกแตกตว oxidation ในปฏกรยา Redox ท าใหเกด Oxidative damage ตอเยอบล าไส Iron
ions จะจบกบ circulating binding protein โดยเฉพาะ Transferrin iron ทไมไดจบกบ transport protein จะ
กระจายไปยงอวยวะตางๆ และท าใหเกดการท าลาย oxidative process Iron ion จะไปรบกวน Mitochondrial
oxidative phosphorylation ท าใหม unused hydrogen ion เกด metabolic acidosis นอกจากน การท Fe2+
เปลยนไปเปน Fe3+ ไปจบกบ plasma ท าใหเกด 3 proton ดงสมการ Fe3+ + H2O Fe(OH)3 + 3H+Iron
ม direct inotropic effect ตอ myocardium เปนผลใหเกด venous filling pressuresลดลง, ลด preloadและเกด
relative bradycardia cardiac output ลดลง เกด Hemodynamic shock นอกจากนยงพบวาเกด Early
coagulopathy ทไมสอดคลองกบ Hepatotoxicity จากการท Iron ไป inhibit thrombin formation และ
บทบาทของthrombin ตอ fibrinogen
Clinical Manifestations
สามารถแบงอาการทางคลนกของภาวะเปนพษจากเหลกไดเปน 5 ระยะ
ระยะท1 เกดในชวงภายใน 6 ชวโมงหลงรบประทานเหลก จะเปนอาการ corrosive and gastrointestinal
symptom ไดแก คลนไส อาเจยน ปวดทอง ถายเหลว ซงท าใหเกดการสญเสยน าและเกลอแรในรางกาย
นอกจากนยงท าใหเกดIntestinal ulcer, edema, transmural inflammation และในบางรายทมภาวะรนแรงอาจ

เกด small bowel infarction และเกด necrosis ตามมา อาการอาเจยนเปนเลอด ถายด า ถายเปนเลอด สามารถ
ท าใหเกด Hemodynamic instability ได อาการแสดงทางระบบทางเดนอาหาร มกเกดตามมาจากภาวะทม
ปรมาณธาตเหลกเกนในรางกายปรมาณมาก ในทางกลบกนถาในชวง 6 ชวโมงแรกหลงรบประทานไมม
อาการเกดขน โดยเฉพาะอาการคลนไสอาเจยน จะถอวา อาจไมม ภาวะ iron toxicity ทรนแรงได
ระยะท2 เปนระยะ Latent stage เกดในชวง 6 – 24 ชวโมงหลงรบประทานเหลกอาการทางระบบอาหารจะ
ลดลง กอนทจะเรมกลายเปนอาการทางsystemic ซงจรงๆแลวไมใชระยะสงบแทจรง แตยงม การด าเนนการ
ท าลายcell อย ผปวยทอยในระยะ latent มกมอาการ Lethargy, tachycardia, metabolic acidosis โดยสรปคอ
ผปวยทมอาการด มสญญาณชพปกต mental status ปกตด ภาวะความเปนกรด เปนดางปกต จะมการด าเนน
โรคทด
ระยะท3 Shock stage เกดในชวง 24 – 72 ชวโมงหลงรบประทานธาตเหลก เปนชวง Profound toxicity
สาเหตของการShock เกดจากหลายเหตปจจย ซงเปนผลจาก Hypovolemia, vasodilation และ poor cardiac
output ท าใหลด tissue perfusion และเกด metabolic acidosis Iron ท าใหเกด coagulopathy สงผลให
bleeding และ Hypovolemia มากขน Systemic toxicity มผลตอระบบประสาท ท าใหเกด Lethargy,
Hyperventilation, Seizures, or coma ได
ระยะท4 Hepatic failure เกดในชวง 48 – 72 ชวโมงหลงรบประทาน
ระยะท5 scarring จาก Gastrointestinal injury ท าใหเกดภาวะ Gastric outlet obstruction ซงจะเกดในชวง 2 –
8 สปดาหหลงจากรบประทาน
Diagnosis
History
-ประวตจะชวยในการบอกชนด และปรมาณของธาตเหลกทผปวยไดรบ
- บนทกเวลาของการรบประทานธาตเหลกและเวลาทเรมมอาการเกดขน
- การรบประทานธาตเหลกทเกดขนเปนอบตเหตหรอตงใจรบประทาน
- หาวาผปวยมภาวะความเจบปวยทรนแรง หรอลกษณะความเจบปวยทชวยบอกวามการรบประทาน
ธาตเหลกปรมาณมาก

- ถามถงประวตการรบประทานยาอนรวมดวย
- ในกรณผปวยเดก อยาลม ถามถงพนองทอยในความเสยงเดยวกน
Physical examination
ในชวงแรกการตรวจรางกายผปวยทรบประทานธาตเหลกเกนจะยงไมพบอะไรทเดนชด ยกเวน
ผปวยทบรโภคเขาไปจรงๆ แลวในเวลาตอมาจะตรวจพบลกษณะตางๆตาม Phase ของ iron toxicity ซงไม
จ าเปนตองมทกคน ลาอาการยงสามารถ overlap กนได
Diagnosis Testing
Radiography
-จะพบ Radiopacity ใน abdominal radiography โดยขนกบระยะเวลาทรบประทาน ปรมาณธาต
เหลกทรบประทานเขาไปซงควรจะ X-ray ภายใน 2 ชวโมงหลงรบประทาน ธาตเหลกในรปแบบน าและ
chewable iron tablet มกไมเหนจากภาพรงสX-ray ถงอยางไรกตาม การทไมพบในภาพฉายรงสไมสามารถ
ใชเปนตวบงชถงภาวะไมมพษได
Laboratory studies
Initial Labs
-Serum iron levels peak absorption 2 – 6 h ซงมกนยมเจาะในชวง 4 ชวโมงหลงรบประทาน ซง
อาจจะถงระดบ peak ชากวาปกตไดใน enteric coated หรอ sustained release
ตารางแสดงระดบ Serum iron level
Serum iron Level toxicity 0 – 100 μg/dl Normal range 100 – 350 μg/dl Definite poisoning, questionable toxicity 350 – 500 μg/dl Potential serious toxicity 500 – 1000 μg/dl Definite serious toxicity >1000 μg/dl Potential fatal -การเจาะ Total iron-binding capacity ไมแนะน าใหเจาะ เนองจากไมไดมประโยชนเพมเตม

-Arterial blood gas: Anion-gap metabolic จาก Lactate เปน common finding ในผปวยทม serious
iron ingestion
- CBC: Anemia จาก Hemorrhage หรออาจม Leukocytosis WBC count of 15,000 /mm3 สมพนธ
กบ serum iron >300 μg/dl (100% specific,50% sensitivity)
- Liver function
-Coagulogram
- Blood glucose concentration >300 mg/dL 100% ในการท านายวา Iron concentration >300 μg/dl
-Amylase and Lipase
- ยาทจะมผลตอผลของคา Lab: Deferoxamine จะท าใหคา Serum iron ดต ากวาความเปนจรงได
Follow-Up and special considerations test to monitor for complication
- Serial electrolyte BUN, Cr จะชวงบงบอกถงการด าเนนการ หรอการตอบสนองตอการใหสารน า
ทชดเชยแกผปวย
-Coagulation tests: PT/PTT/INR
-Serum bicarbonate
-Liver function tests in severe over dose
-Amylase and Lipase
-Arterial blood gas or venous blood gas เพอดเรอง metabolic acidosis
Differential diagnosis
Conditions that present similarly to acute iron toxicity: o Gastritis o Small bowel obstruction

o Drug intolerance/overdose o Alcohol toxicity o Viral illness o Diabetic ketoacidosis o Metabolic acidosis
ภาวะเปนพษจากสารชนดอน ไดแกaspirin, NSAIDs, theophylline, organophosphates, carbamates, other metals and metalloids, paraquat, caustic agents, colchicines, nicotine, and mushrooms
Management
Initial approach
-Stabilization ในผปวย serious ingestion ไดแก การให Oxygen, airway assessment, และการเปดเสน IV access ในผปวยทมภาวะซม ควรพจารณารบใส Orotracheal intubation เพอจะไดปลอดภยในการ decontaminate ระบบทางเดนอาหาร
-เจาะเลอดเพอสง Lab Chemistry, Hemoglobin, Iron concentration, coagulation, and hepatic profile, arterial blood gas, electrolytes,
-ในกรณผปวยทด clinical ด มเพยงแคอาเจยน 1 – 2 ครงอาจจะไมจ าเปนตองเจาะเลอด work up ทนทอาจรอสงเกตอาการกอนได
Limiting absorption
-Gastrointestinal decontamination
-activated charcoal ไมจบกบ ธาตเหลกดงนนการใหจงไมมประโยชน ยกเวนมการรบประทานสารอนๆดวยเชนกน
- syrup of Ipecac technique ไมแนะน า และไดประโยชนคอนขางนอย
- Gastric lavage ใหประโยชนมากกวาการกระตนใหอาเจยนแตกถกจ ากดได ถา Iron tablet มขนาดใหญและปรมาณ iron tablet มจ านวนมาก
- Whole bowel irrigation จากการศกษาใน case report พบวาไดประโยชน

Polyethylene glycol (Colyte, GoLYTELY) ใหทาง nasogastric tube at 500 mL/h for children and up to 1.5–2 L/h for adults.ใหจนกวาจะอจจาระใส; ไมพบradiopacities.
พจารณาendoscopic or surgical removal of Fe-containing bezoar if unresponsive to irrigation.
-Intravenous Deferoxamine o Deferoxamine 100 mg จะ Chelate ferric ion 8.5 mg o ควรใหทนทภายใน 24 ชวโมง
-ขอบงชในการให
Metabolic acidosis repetitive vomiting or diarrhea toxic appearance: lethargy, hypotension, or signs of shock serum iron concentration >500 μg/dl ให Deferoxamine IV ในผปวยทม อาการแสดงของ ภาวะเหลกเปนพษทรนแรง ควรให intravenous Deferoxamine
infusion 15 mg/kg/h
-Administration techniques:
Increase IV infusion rate to 15 mg/kg/hr over 20 min, monitoring for hypotension. ลด infusion rate ถาม hypotension Infusion rates as high as 45 mg/kg/hr have been tolerated. Disregard manufacturer’s recommendation of maximum daily doses of 6 g in serious iron
exposures.
- Length of infusion (controversial):

Deferoxamine–iron complex จนกวาปสสาวะจะเปนส vin rose color; แนะน าให continuing infusion จนกวาปสสาวะจะกลบเปนปกต
Resolution of signs and symptoms of significant toxicity is criterion for discontinuing Deferoxamine
Prolonged Deferoxamine therapy >24–48 hr อาจเปนตวกระตน adult respiratory distress syndrome.
In severe cases with continued signs and symptoms, infusion may be continued cautiously at lower dose.
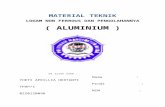
Algorithm for clinical management of patients following iron ingestion.
ในกรณผปวยเปนคนทอง

-ใหการรกษาเชนเดยวกบคนทวไป
-จากการศกษาพบวา Deferoxamine ผาน placenta ในปรมาณทจ ากด
- Phase 3 toxicity associated with spontaneous abortion, preterm delivery, maternal death
Adverse effects of Deferoxamine
-Acute lung injury
-Acute respiratory distress syndrome
Enhance elimination
- โดยการท า hemodialysis มขอบงชเมอผปวยมภาวะ renal failure และไดรบ Deferoxamine
-การท า hemodialysis หรอ hemoperfusion เพยงล าพงไมมผลในการชวยเพมการขบ free iron ออก
จากรางกาย สวน exchange transfusion มการใชรกษาบางในผปวยเดก แตประสทธภาพการรกษายงไมเปน
ทยนยน
Disposition
Admission Criteria
GI symptoms or dehydration Patients treated with Deferoxamine ICU admission for coma, shock, metabolic acidosis, or iron levels >1,000 mg/dL
Discharge Criteria
Asymptomatic with negative radiograph Minimal to no symptoms after 6-hr observation Mild GI symptoms that have resolved without evidence of metabolic acidosis and serum iron <350
mg/dL
IRON KEY POINTS

Asymptomatic at 6hrs r/o significant ingestion 5 stages Must consider with gastro, GI bleed, AGMA, shock NYD Absence of pills on AXR does not r/o Rx based on signs/symptoms/labs + iron level + amount ingested Don’t wait for level if patient toxic
เอกสารอางอง
1. Anderson BD, Turchen SG, Manoguerra AS, Clark RF: Retrospective analysis of ingestions of iron containing products in the United States: Are there differences between chewable vitamins and adult preparations? J Emerg Med 2000; 19: 255-258.
2. Artman M, Olson RD, Boerth RC: Depression of myocardial contractility in acute iron toxicity in rabbits. Toxicol Appl Pharmacol 1982; 66: 329-337.
3. Anderson BD, Turchen SG, Manoguerra AS, et al. Prospective analysis of ingestions of iron containing products in the United States: Are there differences between chewable vitamins and adult preparations?. J Emerg Med. 2000;19:255–258.
4. Bryant SM, Leikin J. Iron. In: Brent J, Wallace KL, Burkhart KK, et al., eds. Critical Care Toxicology. St. Louis, MO: Mosby; 2005.
5. Leikin J, Paloucek F. Iron. In: Poisoning and Toxicology Handbook. Hudson, OH: Lexi-Comp; 2002.
6. Mills KD, Curry SC. Acute iron poisoning. Emerg Med Clin North Am. 1994;12(2):397–413.
7. Tenenbein M. Benefits of parenteral deferoxamine for acute iron poisoning. J Toxicol Clin Toxicol. 1996;34(5):485–489.
8. Anderson AC. Iron poisoning in children. Curr Opin Pediatr 1994;6(3):289-94.
9. D.Juurlink, M.Tenenbein, G.Koren, D.Redelmeier. Iron poisoning in young children: association
with the birth of a sibling. CMAJ 2003;168(12):1539-42

10. Tenenbein M, Rodgers GC. The four A’s of decreasing the toll of childhoodiron poisoning deaths. Arch Fam Med 1994;3:754-5. 11. Reynolds LG, Klein M. Iron poisoning — a preventable hazard of childhood.S Afr Med J 1985;67(17):680-3. 12. Fine JS. Iron poisoning. Curr Probl Pediatr 2000;30(3):71-90. 13. Shannon M. Ingestion of toxic substances by children. N Engl J Med 2000;342(3):186-91. 14. Litovitz TL, Felberg L, White S, Klein-Schwartz W. 1995 annual report ofthe American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 1996;14(5):487-537. 15. Litovitz TL, Smilkstein M, Felberg L, Klein-Schwartz W, Berlin R, Morgan JL. 1996 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 1997;15(5):447-500. 16. Litovitz TL, Klein-Schwartz W, Dyer KS, Shannon M, Lee S, Powers M.1997 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 1998;16(5):443-97. 17. T.Tran, J. R. Wax, C. Philput, Joy D. Steinfeld, Charles J. Ingardia. The Journal of Emergency Medicine, Vol. 18, No. 2, pp. 225–228, 2000 18. Curry SC, Braitberg G. Poisoning in pregnancy. In: Foley MR,Strong T, eds. Obstetric Intensive Care. Philadelphia: WB Saunders; 1997. 19. Mills KC, Curry SC. Acute iron poisoning. Emerg Med Clin North Am 1994;12:397– 413. 20. Dugdale AE, Powell LW. Acute iron poisoning: its effects and treatment. Med J Aust 1964;2:990 –2. 21. Richards R, Brooks SEH. Ferrous iron poisoning in pregnancy (with afibrinogenemia as a complication). West Indian Med J 1966;15:134–40. 22. Strom RC, Schiller P, Seeds AE, ten Bensel R. Fatal iron poisoning in a pregnant female. Minn Med 1976;59:483–9. 23. Manoguerra AS. Iron poisoning: report of a fatal case in an adult.Am J Hosp Pharm 1976;33:1088 –90. 24. Rayburn WF, Donn SM, Wulf ME. Iron overdose during pregnancy: successful therapy with deferoxamine. Am J Obstet Gynecol 1983;147:717– 8.

25. Blanc P, Hryhorczuk D, Danel P. Deferoxamine treatment of acute iron intoxication in pregnancy. Obstet Gynecol 1984;64: 12S-14S. 26. Olenmark M, Biber B, Dottori O, Rybo G. Fatal iron intoxication in late pregnancy. Clin Toxicol 1987;25:347–9. 27. Van Ameyde KJ, Tenenbein M. Whole bowel irrigation during pregnancy. Am J Obstet Gynecol 1989;160:646 –7.