A Case of Rectal Cancer Arising from Long-Standing ...
5
2569 □ CASE REPORT □ A Case of Rectal Cancer Arising from Long-Standing Prolapsed Mucosa of the Rectum Takashi Nonaka 1,2 , Masahiko Inamori 1,3 , Tadaomi Kessoku 2 , Yuji Ogawa 2 , Shogo Yanagisawa 2 , Tadahiko Shiba 2 , Takashi Sakaguchi 2 , Eiji Gotoh 4 , Shin Maeda 1 , Atsushi Nakajima 1 , Kazuhiro Atsukawa 2 , Hisao Takahasi 2 and Yoshikiyo Akasaka 5,6 Abstract Mucosal prolapse syndrome (MPS) has been recognized as a chronic benign inflammatory disorder, char- acterized mainly by rectal mucosal prolapse. Disorders representing this condition include solitary rectal ulcer syndrome (SRUS), rectal prolapse, proctitis cystica profunda, and inflammatory cap polyps. The gross ap- pearance of rectal MPS can be occasionally misinterpreted as rectal cancer. In contrast, there have been a few reports of colorectal cancer originating from prolapsed mucosa. Herein, we report a case of MPS associated with two independent rectal cancers extending into the submucosal layer. We speculate that long-standing MPS may increase the risk of malignant transformation. Key words: mucosal prolapse syndrome, solitary rectal ulcer syndrome, rectal cancer, malignant transforma- tion (Intern Med 50: 2569-2573, 2011) (DOI: 10.2169/internalmedicine.50.5924) Introduction Solitary rectal ulcer syndrome (SRUS) is considered as a rare benign rectal disease that has a wide spectrum of clini- cal presentations, variable endoscopic findings, and charac- teristic histopathological features (1-9). Recently, the mu- cosal prolapse syndrome (MPS) was proposed as a unified concept, and has been accepted widely, based on the recog- nition that similar histopathological abnormalities can occur in other conditions and sites, such as transitional mucosa ad- jacent to large bowel tumors, prolapsed colostomies, and prolapsed hemorrhoids (10-12). Although it has been reported that rectal MPS can occa- sionally be misinterpreted as rectal carcinoma based on its clinical presentation, and endoscopic and radiographic ap- pearances (3-9), few reports have described the occurrence and characteristics of malignant transformation in this syn- drome (13-18). Neither the association of cancer with long- standing MPS nor the malignant potential of MPS has ever been investigated thoroughly. We report a highly unusual case of MPS with moderately differentiated tubular adeno- carcinoma and poorly differentiated adenocarcinoma arising from the prolapsed mucosa, both of which invaded the sub- mucosal layer. Case Report A 69-year-old man visited our hospital with lower ab- dominal pain and difficulty in passing stools. The patient had a history of hypertension and gastric ulcer. The physical examination was unremarkable. The results of laboratory ex- aminations, including urinalysis, complete blood cell count (CBC), and liver and renal function tests were normal. The serum C-reactive protein level was 0.1 mg/dL, serum carci- noembryonic antigen (CEA) level was 3.1 ng/mL, and the 1 Gastroenterology Division, Yokohama City University School of Medicine, Japan, 2 Department of Gastroenterology, Hiratsuka City Hospital, Japan, 3 Office of Postgraduate Medical Education, Yokohama City University Hospital, Japan, 4 Department of Medical Education, Yokohama City University School of Medicine, Japan, 5 Department of Pathology, Toho University School of Medicine, Japan and 6 Division of Chronic In- flammatory Diseases, Advanced Medical Research Center, Toho University Graduate School of Medicine, Japan Received for publication May 30, 2011; Accepted for publication July 25, 2011 Correspondence to Dr. Masahiko Inamori, [email protected]
Transcript of A Case of Rectal Cancer Arising from Long-Standing ...

2569
□ CASE REPORT □
A Case of Rectal Cancer Arising from Long-StandingProlapsed Mucosa of the Rectum
Takashi Nonaka 1,2, Masahiko Inamori 1,3, Tadaomi Kessoku 2, Yuji Ogawa 2,
Shogo Yanagisawa 2, Tadahiko Shiba 2, Takashi Sakaguchi 2, Eiji Gotoh 4, Shin Maeda 1,
Atsushi Nakajima 1, Kazuhiro Atsukawa 2, Hisao Takahasi 2 and Yoshikiyo Akasaka 5,6
Abstract
Mucosal prolapse syndrome (MPS) has been recognized as a chronic benign inflammatory disorder, char-
acterized mainly by rectal mucosal prolapse. Disorders representing this condition include solitary rectal ulcer
syndrome (SRUS), rectal prolapse, proctitis cystica profunda, and inflammatory cap polyps. The gross ap-
pearance of rectal MPS can be occasionally misinterpreted as rectal cancer. In contrast, there have been a few
reports of colorectal cancer originating from prolapsed mucosa. Herein, we report a case of MPS associated
with two independent rectal cancers extending into the submucosal layer. We speculate that long-standing
MPS may increase the risk of malignant transformation.
Key words: mucosal prolapse syndrome, solitary rectal ulcer syndrome, rectal cancer, malignant transforma-
tion
(Intern Med 50: 2569-2573, 2011)(DOI: 10.2169/internalmedicine.50.5924)
Introduction
Solitary rectal ulcer syndrome (SRUS) is considered as a
rare benign rectal disease that has a wide spectrum of clini-
cal presentations, variable endoscopic findings, and charac-
teristic histopathological features (1-9). Recently, the mu-
cosal prolapse syndrome (MPS) was proposed as a unified
concept, and has been accepted widely, based on the recog-
nition that similar histopathological abnormalities can occur
in other conditions and sites, such as transitional mucosa ad-
jacent to large bowel tumors, prolapsed colostomies, and
prolapsed hemorrhoids (10-12).
Although it has been reported that rectal MPS can occa-
sionally be misinterpreted as rectal carcinoma based on its
clinical presentation, and endoscopic and radiographic ap-
pearances (3-9), few reports have described the occurrence
and characteristics of malignant transformation in this syn-
drome (13-18). Neither the association of cancer with long-
standing MPS nor the malignant potential of MPS has ever
been investigated thoroughly. We report a highly unusual
case of MPS with moderately differentiated tubular adeno-
carcinoma and poorly differentiated adenocarcinoma arising
from the prolapsed mucosa, both of which invaded the sub-
mucosal layer.
Case Report
A 69-year-old man visited our hospital with lower ab-
dominal pain and difficulty in passing stools. The patient
had a history of hypertension and gastric ulcer. The physical
examination was unremarkable. The results of laboratory ex-
aminations, including urinalysis, complete blood cell count
(CBC), and liver and renal function tests were normal. The
serum C-reactive protein level was 0.1 mg/dL, serum carci-
noembryonic antigen (CEA) level was 3.1 ng/mL, and the
1Gastroenterology Division, Yokohama City University School of Medicine, Japan, 2Department of Gastroenterology, Hiratsuka City Hospital,
Japan, 3Office of Postgraduate Medical Education, Yokohama City University Hospital, Japan, 4Department of Medical Education, Yokohama
City University School of Medicine, Japan, 5Department of Pathology, Toho University School of Medicine, Japan and 6Division of Chronic In-
flammatory Diseases, Advanced Medical Research Center, Toho University Graduate School of Medicine, Japan
Received for publication May 30, 2011; Accepted for publication July 25, 2011
Correspondence to Dr. Masahiko Inamori, [email protected]

Intern Med 50: 2569-2573, 2011 DOI: 10.2169/internalmedicine.50.5924
2570
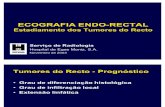
Figure 1. Thirteen years earlier, the first colonoscopic ex-amination revealed reddened lesions on the anterior wall of the lower rectum.
Figure 2. The first time biopsy specimen showed mild in-flammation in the lamina propria and upward proliferation of a splayed muscularis mucosa.
Figure 3. The current endoscopic examination. a: A protruding lesion was seen on the anal side in the reddened mucosa of the rectum. b: A depressed lesion was seen on the oral side, close to the pro-truding lesion.
a b
serum carbohydrate antigen (CA) 19-9 level was 9.3 U/mL.
He had no history of enema use or insertion of supposito-
ries, but he had tended to strain at defecation for a long
time. Interestingly, it was his past medical history that
brought him to our hospital this time; he desired further ex-
amination for a positive fecal occult blood test 14 years pre-
viously, and had undergone colonoscopy that revealed
patchy erythematous mucosa on the anterior wall of the
lower rectum (Fig. 1). At that time, biopsy specimens taken
from the lesion had shown evidence of mild inflammation,
reactive epithelial changes with hyperplastic and distorted
crypts, ectatic and congested vessels, and subtle upward pro-
liferation of a splayed muscularis mucosa. Consequently,
this lesion was initially diagnosed as idiopathic proctitis
without dysplasia or malignancy, because its histopathologi-
cal findings were weakly perceived as MPS features
(Fig. 2). Although colonoscopy had been performed repeat-
edly since the first examination, the endoscopic appearances
and histopathological findings on biopsy had remained con-
stant. His last colonoscopy had been conducted five years
previously, and biopsy specimens taken from the same red-
dened lesions had shown no evidence of malignancy. The
present time colonoscopic examination revealed a protruding
lesion on the anal side (Fig. 3a) and a depressed lesion on
the oral side (Fig. 3b) in the aforementioned reddened mu-
cosa of the rectum. Biopsy specimens taken from the pro-
truding lesion revealed a moderately differentiated tubular
adenocarcinoma. As a result, laparoscopic abdominoperineal
rectal resection with regional lymph node dissection was
performed (Fig. 4). Histopathologically, the protruding le-
sion consisted of moderately differentiated tubular adenocar-
cinoma (Fig. 5a), and the depressed lesion consisted of a
poorly differentiated adenocarcinoma (Fig. 5b, 5c), both of
which were discontinuous and extended into the submucosal
layer without vascular or lymphocytic infiltration or lymph
node metastasis. Immunohistochemically, the protruding le-
sion showed negative staining for p53, however, the de-
pressed lesion showed both strong and diffuse positive stain-
ing. Histopathological examination of the background rectal
mucosa surrounding the two cancers revealed the presence
of longitudinal smooth muscle fibers and collagen deposi-

Intern Med 50: 2569-2573, 2011 DOI: 10.2169/internalmedicine.50.5924
2571
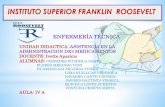
Figure 4. Gross appearance of the resected rectum. The protruding lesion (arrow) was 20 mm in diameter and 4 cm from the anal verge; the depressed lesion (arrowhead) was 15 mm in diameter and 6 cm from the anal verge. Both lesions were discontinuous and independent.
Figure 5. Histopathological examination. a: Section of the protruding lesion with a background mucosa. Moderately differentiated tubular adenocarcinoma was seen (at left), with MPS mucosa (at right) which showed thickened muscularis mucosa and ingrowth of muscle fibers in the lamina pro-pria (Hematoxylin and Eosin staining, ×4). b: Section of the depressed lesion with a background mu-cosa. The border between poorly differentiated adenocarcinoma (at left) and MPS mucosa (at right) was observed with marked collagenous fiber in the submucosa. Area outlined by the square is shown in panel c (Hematoxylin and Eosin staining, ×4). c: High magnification showed poorly differentiated adenocarcinoma and the border (Hematoxylin and Eosin staining, ×10). d: Azan-Mallory staining for Fig. 5b enhanced marked collagenous fiber in the lamina propria and submucosa (Azan-Mallory stain, ×4). e: Immunohistochemical staining using α-SMA for Fig. 5c enhanced the appearance of the fibromuscular obliteration in the lamina propria (α-smooth muscle actin stain, ×10).
a b c
d e
tion in the lamina propria, namely fibromuscular oblitera-
tion, which is a characteristic histopathological feature in
MPS (Fig. 5d, 5e).
Discussion
Solitary rectal ulcer syndrome (SRUS), although origi-
nally described by Cruveilhier in 1830 (1), gained wide ac-
ceptance only after Madigan and Morson characterized the
lesion both clinically and pathologically in 1969 (2). This
entity is a rare benign disease of the rectum, which pre-
dominantly affects adults over a wide age range, with an es-
timated prevalence of 1 in 100,000 people per year (3-5).
Although the term SRUS has been widely accepted, it is
misleading in that the lesions may neither be ulcerated nor
solitary on macroscopic examination (3-9). For this reason,
recently, the unifying concept of the mucosal prolapse syn-
drome (MPS) was proposed as a common clinicopathologi-
cal term, based on the recognition of clinical and histopa-
thological similarities with other conditions and at other
sites (10-12). In other words, SRUS is now considered as
one entity in the spectrum of MPS.
The underlying etiology of SRUS/rectal MPS is not yet
fully understood. However, several hypotheses have been
proposed, including congenital malformations, paradoxical
contraction of the pelvic floor and external anal sphincter
muscles from excessive straining at defecation, localized
rectal ischemia, inflammation, and rectal pro-
lapse (10, 19-23).
The symptoms of SRUS/rectal MPS are quite variable.
Nearly all patients describe a symptom complex consisting
of rectal bleeding, passage of mucus, tenesmus, perineal and
abdominal pain, constipation, sensation of incomplete defe-
cation, straining on defecation, and rectal pro-

Intern Med 50: 2569-2573, 2011 DOI: 10.2169/internalmedicine.50.5924
2572
Table 1. Clinical Features of Patients with MPS Accompanied by Carcinoma
case(Ref) author/year Age/Sex Presenting symptoms Macroscopic findings Location Histological type of tumor Depth of tumor invasion
1 (13) Silver H/1969 49/F rectal pain, bleeding andan abnormal discharge
a tender ulcer with elevated edges rectum well differentiated mucinous adenocarcinoma ND
2 (14) Burt CA/1970 76/F rectal bleeding andmucous stool
a large polypoid mass sigmoid Papillary - mucinous adenocarcinoma subserosa
3 (15) Bhuta I/1976 27/M rectal bleeding andtenesmus
multiple elevated tumor masseswith ulceration
rectum adenocarcinoma in situ
4 (16) Li SC/1998 59/M constipation a mass rectum adenocarcinoma ND
5 (16) Li SC/1998 53/F rectal bleeding irregular nodules rectum adenocarcinoma ND
6 (16) Li SC/1998 26/M ND a mass rectum adenocarcinoma ND
7 (17) Tsuchida K/1998 45/F constipation a small ulcerated lesion rectum well differentiated tubular adenocarcinoma submucosa
8 (18) Mönkemüller KE/1999 19/F constipation, tenesmus,and lower abdominal pain
a rectal stricutre surrounded by patchygranular hyperemic mucosa
rectum poorly differentiated mucinous adenocarcinoma ND
9 Nonaka T/2011 69/M lower abdominal pain anddifficulty in defecating
a protruding lesion and a depressed lesionin the patchy erythematous mucosa
rectum moderately differentiated tubular adenocarcinoma,and poorly differentiated adenocarcinoma
submucosa
ND: not described
lapse (7, 8, 23). However, up to 26% of patients can be as-
ymptomatic (6), therefore SRUS/rectal MPS is occasionally
discovered incidentally as in the present case.
The macroscopic findings of SRUS/rectal MPS also vary.
The macroscopic appearance of SRUS/rectal MPS can be
classified into ulcerative (55.1%), polypoid (24%) and flat
(20.9%) types (8). Madigan and Morson reported multiple
lesions in 30% of cases of SRUS (2). Endoscopic misdiag-
nosis occurs frequently because of these variable find-
ings (6-8).
Although the gross appearances of SRUS/rectal MPS vary
greatly, the histopathological findings are highly characteris-
tic. The rectal mucosa in cases of SRUS/rectal MPS shows a
characteristic fibromuscular proliferation within the lamina
propria, accompanied by the thickening and fraying of the
muscularis mucosa, collagen deposition in the lamina prop-
ria, varying degrees of chronic and occasionally active in-
flammation, and reactive epithelial changes (2, 10, 16, 24).
The correct diagnosis of SRUS/rectal MPS depends on a
recognition of these specific histopathological features, espe-
cially the “fibromuscular obliteration”.
SRUS/rectal MPS can occasionally be misdiagnosed as
rectal carcinoma based on its clinical presentation, and en-
doscopic and radiographic appearances, and in some in-
stances, histopathological appearances, due to the presence
of atypical proliferating epithelium ‘as a part’ reactive epi-
thelial changes. Numerous reports focusing on distinction of
MPS from rectal carcinoma have been published (3-9), how-
ever, there are only a few reports describing the occurrence
and characteristics of malignant transformation in SRUS/rec-
tal MPS (13-18) (Table 1). Occasionally, SRUS-like histopa-
thologic feature was produced by underlying malig-
nancy (16). In contrast, there was no report that implied ma-
lignant transformation in MPS based on long-term endo-
scopic observation. The relationship between MPS and col-
orectal cancer remains unclear, although the association of
colorectal cancer with long-standing inflammatory bowel
disease has been established (25-27). A previous report sug-
gested that long-standing chronic idiopathic colitis was asso-
ciated with an increased risk of colorectal dysplasia and ade-
nocarcinoma (28). The mechanism of transformation in MPS
is obscure, but it can be in the same manner as the above
conditions. Furthermore, Ball et al reported that parts of
SRUS showed focal loss of hMLH1 gene expression, indi-
cating the potential for preneoplastic change (29). We specu-
late that the rectal cancer in the present case represents a
malignant transformation from long-standing rectal MPS,
based on the long-term endoscopic observation.
Conclusion
In conclusion, we reported a highly unusual case of MPS
with two independent rectal cancers extending into the sub-
mucosal layer. Intentional colonoscopy and repeated biopsy
for MPS may facilitate the correct diagnosis of such cases,
because long-standing MPS may be associated with an in-
creased risk of malignant transformation.
The authors state that they have no Conflict of Interest (COI).
References
1. Cruveilhier J. Ulcere chronique du rectum. In: Anatomie Patholo-
gique du Corps Humain. vol. 2. JB Bailliere, Paris, 1830: 4.
2. Madigan MR, Morson BC. Solitary ulcer of the rectum. Gut 10:
871-881, 1969.
3. Martin CJ, Parks TG, Biggart JD. Solitary rectal ulcer syndrome
in Northern Ireland. 1971-1980. Br J Surg 68: 744-747, 1981.
4. Saul SH, Sollenberger LC. Solitary rectal ulcer syndrome. Its
clinical and pathological underdiagnosis. Am J Surg Pathol 9:
411-421, 1985.
5. Royes CA, Williams NP, Hanchard B, Lee MG. Solitary rectal ul-
cer syndrome. West Indian Med J 41: 152-155, 1992.
6. Tjandra JJ, Fazio VW, Petras RE, et al. Clinical and pathologic
factors associated with delayed diagnosis in solitary rectal ulcer
syndrome. Dis Colon Rectum 36: 146-153, 1993.
7. Sharara AI, Azar C, Amr SS, Haddad M, Eloubeidi MA. Solitary
rectal ulcer syndrome: endoscopic spectrum and review of the lit-
erature. Gastrointest Endosc 62: 755-762, 2005.
8. Chiang JM, Changchien CR, Chen JR. Solitary rectal ulcer syn-

Intern Med 50: 2569-2573, 2011 DOI: 10.2169/internalmedicine.50.5924
2573
drome: an endoscopic and histological presentation and literature
review. Int J Colorectal Dis 21: 348-356, 2006.
9. Thomson G, Clark A, Handyside J, Gillespie G. Solitary ulcer of
the rectum--or is it? A report of 6 cases. Br J Surg 68: 21-24,
1981.
10. du Boulay CE, Fairbrother J, Isaacson PG. Mucosal prolapse syn-
drome―a unifying concept for solitary ulcer syndrome and related
disorders. J Clin Pathol 36: 1264-1268, 1983.
11. Levine DS. “Solitary” rectal ulcer syndrome. Are “solitary” rectal
ulcer syndrome and “localized” colitis cystica profunda analogous
syndromes caused by rectal prolapse? Gastroenterology 92: 243-
253, 1987.
12. Tendler DA, Aboudola S, Zacks JF, O’Brien MJ, Kelly CP. Pro-
lapsing mucosal polyps: an underrecognized form of colonic polyp
―a clinicopathological study of 15 cases. Am J Gastroenterol 97:
370-376, 2002.
13. Silver H, Stolar J. Distinguishing features of well differentiated
mucinous adenocarcinoma of the rectum and colitis cystica pro-
funda. Am J Clin Pathol 51: 493-500, 1969.
14. Burt CA, Handler BJ, Haddad JR. Colitis cystica profunda concur-
rent with and differentiated from mucinous adenocarcinoma: re-
port of a case. Dis Colon Rectum 13: 460-469, 1970.
15. Bhuta I, Prathikanti V. Colitis cystica profunda. South Med J 69:
495-496, 1976.
16. Li SC, Hamilton SR. Malignant tumors in the rectum simulating
solitary rectal ulcer syndrome in endoscopic biopsy specimens.
Am J Surg Pathol 22: 106-112, 1998.
17. Tsuchida K, Okayama N, Miyata M, et al. Solitary rectal ulcer
syndrome accompanied by submucosal invasive carcinoma. Am J
Gastroenterol 93: 2235-2238, 1998.
18. Mönkemüller KE. Solitary rectal ulcer syndrome and rectal can-
cer. Am J Gastroenterol 94: 1417, 1999.
19. Epstein SE, Ascari WQ, Ablow RC, Seaman WB, Lattes R. Colitis
cystica profunda. Am J Clin Pathol 45: 186-201, 1966.
20. Alexander-Williams J. Solitary-ulcer syndrome of the rectum: its
association with occult rectal prolapse. Lancet 22: 170-171, 1977.
21. Lobert PF, Appelman HD. Inflammatory cloacogenic polyp. A
unique inflammatory lesion of the anal transitional zone. Am J
Surg Pathol 5: 761-766, 1981.
22. Mackle EJ, Parks TG. The pathogenesis and pathophysiology of
rectal prolapse and solitary rectal ulcer syndrome. Clin Gastroen-
terol 15: 985-1002, 1986.
23. Vaizey CJ, van den Bogaerde JB, Emmanuel AV, Talbot IC,
Nicholls RJ, Kamm MA. Solitary rectal ulcer syndrome. Br J Surg
85: 1617-1623, 1998.
24. Malik AK, Bhaskar KV, Kochhar R, et al. Solitary ulcer syndrome
of the rectum―a histopathologic characterisation of 33 biopsies.
Indian J Pathol Microbiol 33: 216-220, 1990.
25. Crohn BB, Rosenberg H. The sigmoidoscopic picture of chronic
ulcerative colitis (non-specific). Am J Med Sci 170: 220-228,
1925.
26. Lennard-Jones JE, Morson BC, Ritchie JK, Williams CB. Cancer
surveillance in ulcerative colitis. Experience over 15 years. Lancet
16: 149-152, 1983.
27. Mattar MC, Lough D, Pishvaian MJ, Charabaty A. Current man-
agement of inflammatory bowel disease and colorectal cancer.
Gastrointest Cancer Res 4: 53-61, 2011.
28. Kern SE, Redston M, Seymour AB, et al. Molecular genetic pro-
files of colitis-associated neoplasms. Gastroenterology 107: 420-
428, 1994.
29. Ball CG, Dupre MP, Falck V, Hui S, Kirkpatrick AW, Gao ZH.
Sessile serrated polyp mimicry in patients with solitary rectal ulcer
syndrome: is there evidence of preneoplastic change? Arch Pathol
Lab Med 129: 1037-1040, 2005.
Ⓒ 2011 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imindex.html