6- Vesiculobullous Diseases

of 10
-
Upload
prince-ahmed -
Category
Documents
-
view
216 -
download
0
Transcript of 6- Vesiculobullous Diseases
-
7/30/2019 6- Vesiculobullous Diseases
1/10
Dr. Tahani Abualteen
/10
Vesiculobullous diseases
Vesiculobullous diseases: Diseases that result in collection of clear fluid (blisters) within or below the epithelium Blisters are classified into (vesicles and bullae) Vesicles:
o Fluid filled lesiono Smaller in sizeo Mostly arise intra-epithelially
Bullae:o Fluid filled lesiono Larger in sizeo Mostly arise sup- epithelially
Vesiculobullous diseases are present as oral ulceration following rupture of the vesicles & bullae Classification of vesiculobullous diseases:
o Vesiculobullous diseases are classified into 2 major groups depending on the histologicallocation of the lesions:
o Intraepithelial vesiculobullous diseases (lesions form within the epithelium): Intraepithelial vesiculobullous diseases are classified into 2 groups depending on the
mechanism of formation of the lesion
Acantholytic lesions:- Pemphigus vulgaris
** Lesions are produced by breakdown of intercellular attachments (desmosomes)
between epithelial cells
Non-acantholytic lesions:- Viral infections of the oral mucosa (e.g. ballooning degeneration in herpetic infections)
** Lesions are produced by death and rupture of groups of epithelial cells
o Subepithelial vesiculobullous diseases(lesions form between the epithelium & lamina propria): Pemphigoid Erythema multiforme Dermatitis herpetiformis Linear IgA disease Epidermolysis bullosa Angina bullosa hemorrhagica (oral blood blisters) Bullous lichen planus
History is importanto Duration (ulceration lasts weeks to months)o Recurrenceo Other lesions: skin, eye, genital lesionso Systemic manifestationso Certain types may be associated with medications
-
7/30/2019 6- Vesiculobullous Diseases
2/10
Dr. Tahani Abualteen
/102
Pemphigus vulgaris: Pemphigus is a group of uncommon autoimmune blistering diseases of
which Pemphigus vulgaris is the most common type
Classified as intraepithelial acantholytic vesiculobullous disease Clinical features:
o Present in middle ageo More common in women than in meno More common in certain ethnic groups, particularly
Ashkenazi Jews, where there may be a genetic link
o Characterized by widespread bullous eruptions involvingthe skin and mucous membranes
o Oral mucosa is involved in nearly all patients and in about50% of cases is the site of initial lesions
o Bullae are fragile (since they are intra-epithelial & notcovered with a thick layer of tissue) and so, they readily
rupture forming crusted areas on the skin and irregular,
ragged mucosal ulcers
o Any part of the oral mucosa may be involved, but the softpalate, buccal mucosa, and lips are most frequently
affected
o There may be also a desquamative gingivitis (a clinicalterm indicating sloughing and ulceration of attached
gingiva that might be a manifestation of different diseases)
o Bullae are produced as a result of acantholysis and thisprocess extends laterally in the surrounding epithelium,
often for a considerable distance
o As a result, gentle lateral pressure to the mucosa in an involved areacan lead to the formation of abulla (Nikolsky's sign)
** Rubbing the oral mucosa gently with a blunt instrument may result (within minutes) in
vesicles or bullae formation; and this indicates the presence ofimmune mechanisms (like Ab
attached to desmosomes) that are waiting for maybe a minor trauma to cause damage
Histopathological features:o Intraepithelial separationo Cleft-like spaces produced by acantholysis in stratum spinosum cellsjust above basal cell layero Basal cells forming the base of the lesion remain
attached to the lamina propria
o Little subepithelial inflammatory cell infiltrationuntil the lesion ruptures
o Acantholytic stratum spinosum cellsare small androunded and contain enlarged hyper-chromatic
nuclei (the so called Tzanck cells)
Nikolsky's sign
-
7/30/2019 6- Vesiculobullous Diseases
3/10
Dr. Tahani Abualteen
/103
Intercellular attachment s of epithelial cells are mediated
by desmosomes comprising opposing attachment plaques
(P) and intercellular adhesion proteins
Pathogenesis:o Autoimmune diseaseauto-
antibodies against desmosomes
** Desmosome is a junctional complex
mediating cell-cell contact** Desmosome = intercellular
attachment plaque + intercellular
adhesion protein
** Desmogleins are important
intercellular adhesion proteins
** Autoantibodies to desmoglein 3 are
found in Pemphigus limited to mucosal
sites
** Autoantibodies to desmoglein 1 and desmoglein 3 are found Pemphigus involving skin and
mucosa
o There's strong evidence that IgG autoantibodies against the intercellular proteins of thedesmosomes (Ab-Ag complex) are responsible for the acantholysisbut the mechanism by
which this occurs is unclear! however, it is likely to involve the activity of proteineases
Diagnosis:o Immunological studies are important in establishing the diagnosis and may be helpful in
monitoring the progression of the disease
o Indirect immunoflourescence: Circulating autoantibodies (IgG) to desmosomes can be demonstrated in the serum of patients Their titer is related to the severity of the disease and monitoring the titer over time may
be helpful in disease monitoring and response to treatment
Circulating autoantibodies may not be detected in all patients (especially in the earlystages of the disease)
o Direct immunoflourescence:- Detection of antibodies while in their place
using another florescent antibody
- Biopsy of peri-lesional mucosa to detect thebinding of autoantibodies (IgG) to desmosomes** IgG autoantibodies can be detected within
the epithelial thicknessproducing a
characteristic fish-net pattern
- Positive in all patients Other forms of Pemphigus include:
o P. vegetanso Drug inducedo Paraneoplastic (associated with some malignancies, e.g. leukemia and lymphoma)
-
7/30/2019 6- Vesiculobullous Diseases
4/10
Dr. Tahani Abualteen
/104
Pemphigoid: Pemphigoid is a group of autoimmune
blistering diseases characterized by the
production of autoantibodies against
hemidesmosomes and basement membrane
(which mediate attachment between
epithelium and underlying connective tissue)
Classified as subepithelial vesiculobullousdisease
The different subtypes and their clinicalmanifestations most likely reflect damage to
different target antigens, however, they can be
divided into 2 groups clinically:
o Bullous Pemphigoid (involving skin mainly)o Mucous membrane Pemphigoid (involving mucosa mainly)
** Oral manifestations occur in almost all patients with mucous membrane Pemphigoid
group,but they are very uncommon in bullous Pemphigoid
Mucous membrane (cicatrical) Pemphigoid:o Etiology: the most common target antigen in mucous membrane Pemphigoid with oral
manifestations is a Transmembrane protein bridging the hemidesmosomes and the basement
membrane together known as BP antigen 2
oClinical features: More common in women than in men Oral mucosa is almost always affected (either alone or
in association with other mucosae)
Bullae occuranywhere on the oral mucosa ** But over 90% of cases involve the gingiva where the
condition presents as desquamative gingivitis
** In some patients, desquamative gingivitis is the onlymanifestation, and thus the condition is then called oral
Pemphigoid
Bullae are tense and tough (unlike those of Pemphigusvulgaris) since they consist offull thickness-epithelium
and thus they remain intact for few days
When bullae rupture, they give rise to erosions whichheal slowly, sometimes with scarring (hence the other
name cicatrical Pemphigoid)
Bullae are produced as a result of acantholysis andthis process extends laterally in the surrounding
epithelium, often for a considerable distance
As a result, gentle lateral pressure to the mucosa in an involved area can lead to theformation of abulla (Nikolsky's sign)
Attachment op epithelium to connective tissue is
mediated by hemidesmosomes (HD) and proteins of
basement membrane zone (BMZ)
-
7/30/2019 6- Vesiculobullous Diseases
5/10
Dr. Tahani Abualteen
/105
Extraoral lesions:- Mucosa of nose, larynx, pharynx,
esophageous, and genitalia
- Skin-
Conjunctiva: may cause blindness** Ocular involvement is the most serious
complicationwith scarring leading to
opacity of the cornea and blindness
o Histopathological features: Subepithelial separation (separation of the full
thickness of the epithelium from the lamina
propria)
Initially, there's no evidence of aninflammatory reaction in the lamina propria
Later on, as the bulla develops, there'sinfiltration by variable numbers ofneutrophils
& Eosinophils around and within the developing
bulla
Peri-vascular lymphocytic infiltrate in thelamina propria
Release of proteases from neutrophils andEosinophils enhances bulla formation in the
basement membrane zone
o Diagnosis: Immunological studies are important in
establishing the diagnosis and may be helpful in monitoring the progression of the disease
Indirect immunoflourescence:- Circulating autoantibodies (IgG) to basement membrane antigens were seldom
identified in the past by routine techniques,but using the modern techniques, they can
now be detected in the serum of about 80% of patients
- Their titer is related to the severity of the disease and monitoring the titer over timemay be helpful in disease monitoring and response to treatment
Direct immunoflourescence:- Biopsy of peri-lesional mucosa to detect the
binding of autoantibodies (IgG) to basement
membrane zone
- Shows linear deposition of IgG and C3 in thebasement membrane
- Positive in all patientso Treatment: topical and/or systemic corticosteroidso Prognosis: good, but monitor eye lesions
-
7/30/2019 6- Vesiculobullous Diseases
6/10
Dr. Tahani Abualteen
/106
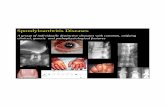
Erythema multiforme: A disease ofsudden onset involving skin and mucous membranes and has a wide range of clinical
presentations (hence the name multiforme)
Clinical features:o Mainly in young adultso More common in males than in femaleso There may or may not be a Prodromal phase with upper respiratory infection, headache,
malaise, nausea
o Severity of the disease varies considerably In its severe form, the Stevens-Johnson syndrome, there's widespread involvement of the
skin and oral, genital, and ocular mucosae
** Ocular involvement can lead to conjunctiva scarring and visual impairment
Milder forms may involve the oral mucosa (with or without skin lesions) or the skin alonemay be involved
o Disease tends to subside after 10-14 days but recurrence may occuro Recurrent Erythema multiforme is associated in particular with recurrent attacks of herpes
simplex virus infection
o Skin lesions: Have variety of forms,
including: erythematous
maculopapular rashes and
vesiculobullous eruptions
in addition to the
characteristic diagnostic
target or iris lesions
Target "iris" lesions consist ofconcentric rings of varying Erythema, in the center ofwhich may be an intact or ruptured and crusted bulla
Hands and feet are most commonly involvedo Oral lesions:
Involve any part of the mucosa Lips and anterior parts of the mouth are most
commonly affected
Appearance of lesions varies with time Erythematous patches are quickly followed by
vesiculobullous eruptions which rapidly
breakdown into erosions as the bullae disintegrate
Erosions on the lips are associated with bleedingand crusting
Circumoral crusting hemorrhagic lesions are animportant sign to reach clinical diagnosis
Pathogenesis:o Unknown (not fully understood)
-
7/30/2019 6- Vesiculobullous Diseases
7/10
Dr. Tahani Abualteen
/107
o Has been suggested that the disease represents a type III hypersensitivity reaction and that themanifestations maybe related to deposition of immune complexes in which the antigen may be
of drug, bacterial, or viral origin
o Ag - Ab complexes have been detected in Erythema Multiforme and in some cases they havebeen associated with HSV infection** Ag - Ab complexes deposition complement activation neutrophils chemotaxisVasculitis epithelial damage
o Many precipitating factors have been identified including drugs (especially sulphonamides &penicillin) and preceding infection (especially herpes simplex infection)
o Many cases appear to arise spontaneously Diagnosis:
o Diagnosis is primarily clinicalo Microscopic features are not diagnostic
May result in intraepithelial or subepithelialseparation
No autoantibodies, so negative direct &indirect immunoflourescence
Treatment and prognosis:o Remove causative drugs, if anyo Topical and systemic corticosteroidso May be recurrento May benefit from prophylactic acyclovir
Dermatitis herpetiformis: A chronic, intensely pruriticautoimmune blistering diseaseof skin Classified as sub-epithelial vesiculobullous disease Primarily skin disease, but oral manifestations are variable and range from symptomless
erythematous areas to extensive erosions
About 90% of patients with dermatitis herpetiformis have gluten hypersensitivity Biopsy shows: subepithelial separation and granular accumulation of neutrophils Direct immunoflourescence studies show granular deposits of IgA in the tips of the connective
tissue papillae together with some complement component, principally C3 Indirect immunoflourescence studies are negative Pathogenesis: activation of complement system and neutrophils chemotaxis
Linear IgA disease: Rare autoimmune blistering disease of skin Classified as subepithelial vesiculobullous disease Primarily skin disease, but oral involvement is occasional Clinically, this disease overlaps with dermatitis herpetiformis & bullous Pemphigoid (differential
diagnoses) About 30% of patients with Linear IgA disease have gluten hypersensitivity
-
7/30/2019 6- Vesiculobullous Diseases
8/10
Dr. Tahani Abualteen
/108
Biopsy shows: subepithelial separation Direct immunoflourescence studies show linear IgA along basement membrane Indirect immunoflourescence studies show the circulating autoantibodies (IgA) to basement
membrane antigens in the serum of about 30% of patients
Epidermolysis Bullosa: The inherited forms of Epidermolysis bullosa form a complex group of syndromes They are due to mutation in the genes coding either for specific keratins in the basal epithelial layer
(resulting in intraepithelial separation) or for various collagens and other attachment proteins in
the basement membrane (resulting in subepithelial separation)
Clinical features:o Skin lesions:
Formation ofskin bullae which may manifest at birth or shortly afterwards Extreme fragility of the skin Bullae usually develop in response to minimal trauma or pressure but they may arise
spontaneously
Hands, feet, knees, elbows are common sites Bullae tend to heal slowly with scarring which can result in claw-like deformityof the
hands
o Oral lesions: Oral and other mucosae may be involved Bullae tend to heal slowly with scarring which
can result in difficulty in eating, speaking, and
swallowing as a result of involvement of the
mouth, larynx and pharynx
Oral lesions may appear in neonates in responseto suckling, and later on minimal trauma from
tooth brushing and routine dental treatment
can cause serious consequences
Bullae rupture to leave painful erosions and subsequent scarring can restrict the opening ofthe mouth, movement of lips and tongue, and cause obliteration of the sulci
Effective oral hygiene may be impossible and rampant caries add to the dental complications
-
7/30/2019 6- Vesiculobullous Diseases
9/10
Dr. Tahani Abualteen
/109
TYPES OF EPIDERMOLYSIS BULLOSA:o Simplexlocalized skin lesions; oral lesions, good prognosiso Dystrophic dominantnails; oral lesions; scarring; fair prognosiso Dystrophic recessivesevere skin and oral lesions, scarring, abnormal teeth, poor prognosiso Junctionalsevere skin and oral lesions, abnormal teeth, fatal
Treatment:o Avoid traumao Antibiotics, corticosteroids
Prognosis:o Simplex: goodo Recessive & Junctional: fatal
Epidermolysis bullosa acquisita: Uncommon autoimmune blistering disease Acquired in adult life Classified as subepithelial vesiculobullous disease Lesions arise mostly on the trauma-prone areas, such as: elbows and knees Oral lesions may occur Biopsy shows: subepithelial separation Direct immunoflourescence studies show linear deposition of IgG and C3 in the basement
membrane
Indirect immunoflourescence studies show the circulating autoantibodies (IgG) to basementmembrane antigens in the serum of about 30-40% of patients
Angina Bullosa Hemorrhagica (oral blood blister): Spontaneous blood filled bullae Occasionally develop on the oral mucosa Usually solitary Middle aged or elderly Occur on any part of the oral mucosa Soft palate is the most commonly involved Cause is unknown, but bullae may be related to trauma Biopsy shows: subepithelial separation No autoantibodies, so negative direct & indirect
immunoflourescence
Treatment of non-microbial mucositis with corticosteroids: Mouth rinse
o Triamcinolone acetonide Ointment
oTriamcinolone acetonide
o Fluocinonide (Lidex)
-
7/30/2019 6- Vesiculobullous Diseases
10/10
Dr. Tahani Abualteen
/101
o Clobetasol Systemic Steroids
o Prednisoneo Contraindicated in certain systemic diseases
Intralesional Steroids Triamcinolone acetonide, inject 10-40 mg Anesthetize area before injection of steroid
Differential diagnosis of subepithelial separation:
1- Pemphigoid2- Bullous lichen planus3- Linear IgA disease4-
Dermatitis herpetiformis
5- Epidermolysis bullosa (both forms)6- Erythema multiforme7- Angina bullosa hemorrhagica
Differential diagnosis of desquamative gingivitis:
1- Mucous membrane Pemphigoid2- Pemphigus vulgaris3- Erosive lichen planus4- Allergic reaction5- Drug induced