…to talk about and focus on the circumstances. …to mourn the loss of the former self-image and...
41
-
Upload
shawn-hill -
Category
Documents
-
view
220 -
download
1
Transcript of …to talk about and focus on the circumstances. …to mourn the loss of the former self-image and...



…to talk about and focus on the circumstances.
…to mourn the loss of the former self-image and way of being in the world.
…to acquire information, support, and learn about the illness and disease process.
…to make personal meaning of the experience.

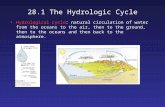
Getting a new medical diagnosis often means that one must adapt to a change in health circumstances (one’s own or a family member’s).
The news often will involve treatment that requires medical adherence to restore or maintain health.

Onset Acute…gradual
Duration Brief … intermittent … lifelong
Course Remitting … relapsing
Predictability Known and predictable … unknown or
unpredictablePrognosis
Normal life … terminal

Burdens of Care None … extensive▪ Medications, monitoring, appliances, personal
assistance…Transmission
Genetic…traumatic…contagiousObviousness
Blatant…invisibleSocial Tolerance
Stigmatizing…acceptable

Who is Anna Sthesia?Cystic Fibrosis or…
Sixty-five roses Sick-sick fibrosis
Sickle cell anemia or… Sick-as-hell anemia
Diabetes or… Die-a-betes


Adherence to (or compliance with) a medication regimen generally addresses:
The extent to which patients take medications as prescribed or otherwise follow health care providers’ recommendations.
I prefer the word "adherence", because "compliance" suggests passively following orders, rather than a therapeutic alliance or contract.

Reports of adherence rates for individual patients generally cite percentages of prescribed doses of medication taken over a specified interval.
Some studies further refine the definition by focusing on dose taking (i.e., prescribed # of pills each day) and timing (taking meds within a prescribed period).

Adherence rates typically run highest among patients with acute conditions.
Persistence among patients with chronic conditions often declines dramatically after the first six months of therapy.

Average rates of adherence reported in clinical trials can run misleadingly high due to attention focused on participants and selection biases. Even so, average adherence rates in clinical trials run only
43 to 78 % among patients receiving treatment for chronic conditions.
No consensual standard exists for what constitutes adequate adherence. Some trials consider rates greater than 80% acceptable,
while others consider rates of greater than 95 % mandatory for adequate adherence (e.g., treatment of HIV infection).

Physicians have little ability to recognize non-adherence, and interventions to improve rates have had mixed results.
Poor medical adherence accounts for substantial worsening of disease, death, and increased health care costs.
Of all medication-related hospital admissions in the U.S., 33 to 69 % follow poor medication adherence, at a cost of approximately $100 billion annually.

Direct methods observed therapy measurement of concentrations of a drug, its metabolite, or a chemical
marker Indirect methods of measurement of adherence include
asking the patient about ease in taking prescribed medication, assessing clinical response, performing pill counts ascertaining rates of refilling prescriptions collecting patient questionnaires using electronic medication monitors measuring physiologic markers asking the patient to keep a medication diary asking the help of a caregiver, school nurse, or teacher.

Consider consequences of the specific threats to patient’s or family members’ psychological adjustment. How will life activities and
goals be disrupted. The more complex and
disruptive the regimen, the greater the likelihood of adherence problems.

Koocher, G.P., McGrath, M.L., & Gudas, L. J. (1990). Typologies of non-adherence in cystic fibrosis. Journal of Developmental and Behavioral Pediatrics, 11, 353-358.

Identifying the basis for deviating from the prescribed course of treatment is the first step.

Is information available to patient and family?
Is the form of information comprehensible?

Is the information appropriate to age and culture?
Are the rationales for components of treatment clear?

Consider the practitioners’ behavior. “Referent
power” issues
“Hi, my name is Kevin. I’ll be your doctor for today.”

Explore social or cultural pressures.
Assess environmental factors
Address complexity of regimen

Assess for psychological factors Attributions Motivations Defense
mechanisms Psychopathology
“This is gonna hurt like hell.”

“Before each of you, you will find a bitter pill and a glass of water”

Czajkowski, D. R. & Koocher, G.P. (1986). Predicting Medical Compliance among Adolescents with Cystic Fibrosis. Health Psychology, 5, 297‑305. Reprinted in: Melamed, B.G., Matthews, K. A., Routh, D. K., Stabler, B., & Schneiderman, N. (Eds.) (1988). Child Health Psychology. Hillsdale, NJ: Lawrence Erlbaum and Associates, pp. 335-343.
(35% non-adherent in CF sample) N = 40 ages 13-23.
“Well, how long do you want to live?”

What has your doctor asked you to do in order to best manage your illness (or to stay healthy)?
What are the hardest pieces of medical advice to follow?
Which parts to you skip or miss most often? What gets in the way of following the
recommendations?

Osterberg, L. & Blaschke, T. (2005). Drug Therapy: Adherence to Medication. New England Journal of Medicine, 353, 487-497.
Rapoff, M. A. (2009). Adherence I Pediatric Medical Regimens (2nd Ed). New York: Springer.




Methods available to improve adherence can be grouped into four general categories: patient education improved dosing schedules increased hours when the clinic is open (including
evening hours), and therefore shorter wait times; and
improved communication between physicians and patients.

Most methods of improving adherence involve combinations of behavioral interventions and reinforcements in addition to increasing the convenience of care, providing educational information about the medical condition and the treatment, and other forms of supervision, monitoring, or attention.


Most important: how do we know that the news we are about to impart will be perceived by the patient as 'bad'? A patient may receive definite news--whether or not it is
perceived by clinicians as 'bad'--as conferring a degree of certainty and feel grateful for this, particularly if it confirms a long held suspicion or belief.
Equally important: information that the bearer may have thought of as relatively unimportant may have a severe impact on the patient and/or family members.
Hart, C., Harrison, A., & Hart, C. (2006). Breaking Bad News. In Mental health care for nurses: Applying mental health skills in the general hospital. (pp. 82-94): Blackwell Publishing: Malden.

Who should tell the patient the particular news. Someone who knows him/her. The person who has all the information available, to cover
any question the patient and/or relatives may wish to ask. The primary care physician, as the person with overall
responsibility for the patient's treatment, or a 'specialist' in such matters as breaking bad news?
Communicating bad news is most closely associated with having to tell patients about a terminal prognosis. As such, much of the literature comes from the areas of critical care and palliative care.

Try not to protect yourself with distancing. Just because
you have bad news should not prevent you from offering support
“You have a serious illness of an undisclosed nature.”

Try to understand and respect the perspective of the recipient.
“Well, I guess I’ll have the ham and eggs.”

“It was touch and go for a while, young man,
but I think we were able to save your leg.”

Deliver the bottom line first, then explain.
“You’re doing it wrong.”

The "good news/bad news approach does not help if the news is only really bad.
“Which do you prefer; sharing a room with a person who’s slightly out of
his mind from heavy medication, or a room with a person who’s throwing
up all the time?”

Have a plan or help the recipient to engage in developing one.
When stress is high written information can help.
Set up ongoing support and availability.

Be human, and be present.