







Languages
Pages
Legal

Lichamelijk onderzoek
(klinisch onderzoek)
Na anamnese is KO hoeksteen van diagnose
Rustige, professionele houding
zorg voor privacy, patiënt voldoende laten uitkleden
ontwikkel systematiek ‘van kop tot teen’
algemeen klinisch onderzoek
onderzoek van hoofd en hals
cardiovasculair onderzoek
onderzoek van de longen
abdominaal onderzoek
locomotorisch stelsel
neurologisch onderzoek
arts in principe aan rechterzijde neerliggende patiënt
1

Lichamelijk onderzoek
(klinisch onderzoek)
video’s: http://stanford25.wordpress.com/
2
Hoe volledig klinisch onderzoek?
Bij “gezonde patiënt” heeft een volledig lichamelijk onderzoek maar beperkt nut (behalve BD meting, borstonderzoek bij vrouw, …)
zeker bij vage of algemene klachten kan KO helpen om antwoord te vinden op hulpvraag patiënt
KO kan ook elementen opleveren voor geven van gezondheidsadvies
volledig KO vergt vaardigheid :
om te verwerven
om te behouden
duur KO : beginneling misschien 30 minuten, ervaren arts 5-10 min.
Afwegen beschikbare tijd: anamnese-KO-informatie en uitleg geven aan patiënt
3

Graden uitgebreidheid (volgens van der Meer)
klinisch onderzoek alleen gericht op een lokaal probleem
(bv bij onstoken vinger zal geen volledig klinisch
onderzoek worden verricht)
Screenend volledig onderzoek
Het (zeer) uitgebreid lichamelijk onderzoek= screenend,
plus aanvullende onderzoeken afhankelijk van klacht
4

5
?

6

7

8
(=plasgeluid)

9

Volgorde onderzoek
“van kop tot teen” (bv vermijd eerst voeten te
onderzoeken, en dan gezicht)
Vermijd nodeloze positieveranderingen
Voor comfort patiënt
Voor vermijden tijdverlies
Aan te passen aan de omstandigheden
Bv bedlegerige patiënten of minder mobiele patiënten tov goed
mobiele patiënten
Ontwikkel een eigen systematiek, bv:
10

11
Bates’ guide to physical examination; 11 th edition, p. 17)
Algemeen onderzoek
Indruk van algemene gezondheidstoestand,
inschatten ernst van de ziekte, en vitale parameters
(anemie, cyanose, ademhalingsfrequentie, bewustzijn, pols, BD)
Temperatuur
gewicht en voedingstoestand: weeg de patiënt!,
evt buikomtrek meten
Lichaamsbouw
Hydratatiegraad
Oedemen
herkennen bepaalde syndromen
Huid (vanuit “internistisch” oogpunt)
onderzoek van lymfeklierstations
12

Cachexie bij patiënt met
leverlijden
13

Uit : BASO-gids : obesitas
14

Buikomtrek als parameter obesitas
R ecent verlaagd: - 8 cm
15

Evaluation of loss of subcutaneous fat
16

Evaluation of loss of muscular mass
17

Lichaamsbouw / lichaamsverzorging
Mager, obees, slank ?
Gespierd ?
Groot ? Klein ?
Motoriek en gang
Voldoende hygiëne ?
Verwaarloosd ?
Nicotinevingers ?
18

Temperatuur
Meten in geval van ernstige ziekten, infecties, of indien
patiënt zelf meent koorts te hebben
rectaal 0,5° hoger dan oraal
axillair nog 0,5 ° lager
tympane temperaturen: relatief goede maat voor rectale
temperatuur (-0.7 tot +0.8 vlgs bepaalde studie)
(indien correct gebruikt, bv geen cerumenprop)
19

Anemie opsporen
20

Evaluatie huidturgor
21

Evaluatie oedemen
22

Causes of edema
I. Decreased oncotic pressure
Nephrotic syndrome
Cirrhosis
Malnutrition
II. Increased vascular permeability to proteins
Angioneurotic edema (usually allergic)
III. Increased hydrostatic pressure
Congestive heart failure
Cirrhosis
Venous stasis
IV. Obstruction of lymph flow
V. Inappropriate renal sodium and water retention
Renal failure
Nephrotic syndrome
23

24

Lymfoedeem
25
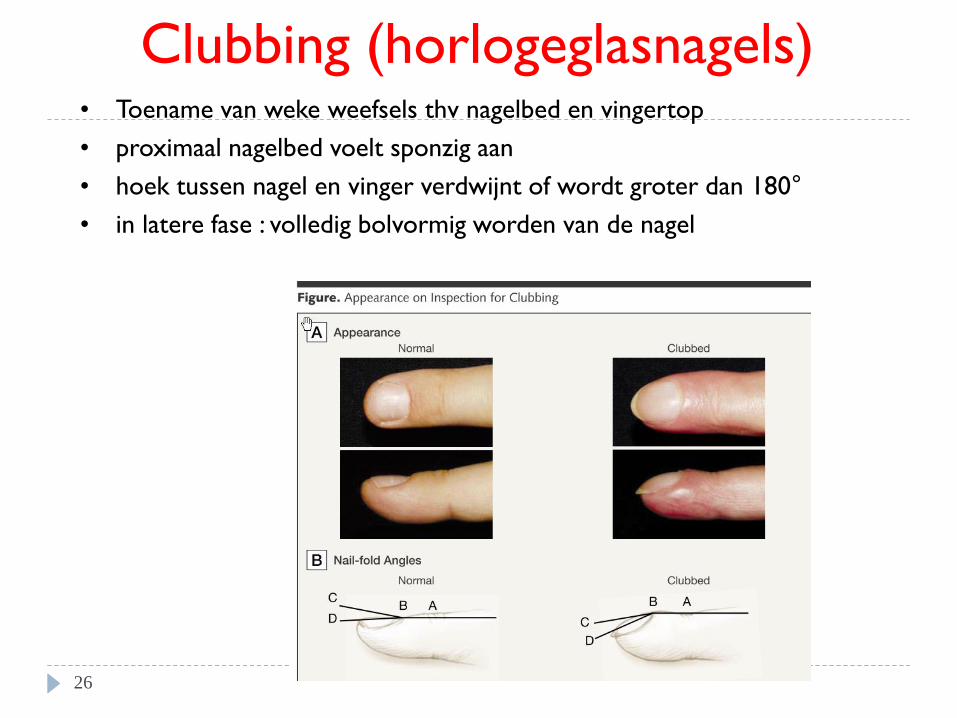
Clubbing (horlogeglasnagels) • Toename van weke weefsels thv nagelbed en vingertop
• proximaal nagelbed voelt sponzig aan
• hoek tussen nagel en vinger verdwijnt of wordt groter dan 180°
• in latere fase : volledig bolvormig worden van de nagel
26

Paar endocriene aandoeningen
27

Acromegalie
28

29

Cushing
30

Cushing
31
http://women-health-info.com/517-Cushing-disease-syndrome.html

Laag Ca, laag Mg, tetanie
32

NEJM 2000 Volume 343 Number 25 33

Huid
34

Spider naevi bij levercirrose
35

Bloedingen in de huid
Petechiën: 1-2 mm
Purpura: iets groter (3of meer mm)
Ecchymosen: enkele mm, 1-2 cm
Hematomen: extravasatie van bloed
36

37 Ned Tijdschr Geneesk 2001

Purpura bij thrombopenie
(niet palpabel bij louter bloeding)
38

Purpura bij vasculitis
(palpabel)
39

“Purpura fulminans”
40

Erythema nodosum
41

Psoriasis
42

Herpes zoster
43

Neurofibromatose (café au lait vlekken en
neurofibromen)
(autosomaal erfelijke ziekte met aantasting van vooral
huid en zenuwstelsel)
44

Septische embolen bij endocarditis
45

46

urticaria
47

Huissoon A and Krishna M. N Engl J Med 2008;358:e9
A 43-year-old woman presented with a 10-month history of an urticarial rash induced by cold, particularly
when she was swimming
48

Angio-oedeem
49

Angio-oedeem hand
50

Algemeen onderzoek
Ernst van de ziekte
(anemie, cyanose, ademhaling, bewustzijn, pols, …)
Voedingstoestand
Temperatuur
Lichaamsbouw
Hydratatiegraad
Oedemen
herkennen bepaalde syndromen
Huid
onderzoek van lymfeklierstations
51

Onderzoek lymfeklieren • Zal meestal per regio worden uitgevoerd
bv aansluitend bij onderzoek hoofd en hals, bij onderzoek thorax/borsten, bij abdominaal onderzoek
• Vergrote lymfeklieren bij infecties of maligniteit: • bij infecties: pijnlijk
• maligniteiten (hematologisch of metastatisch): meestal niet pijnlijk), en verhard (bij lymfoom “rubberachtig”),
• Veralgemeend of gelocaliseerd • Gelocaliseerd bij lokale infecties of in drainagegebied van kanker
• Veralgemeend: bij systemische infecties of hematologische maligniteit
• Belangrijke regio’s : – rond het hoofd
– axillair
– inguinaal
52
Video: http://stanford25.wordpress.com/lymph-node-exam/

http://stanford25.wordpress.com/lymph-node-exam
Findings
• Size: insignificant if < 2cm, except in axilla then < 3cm. In
the supraclaviclar fossa > 1cm is significant.
• Consistency: soft (insignificant), rubbery (classically
lymphoma) , hard (classically malignancy & granulatous
infection).
• Tender (classically infection) vs. non-tender (classically
malignancy).
• Patient 2-12 years old commonly present with insignificant
lymph nodes in neck secondary to frequent viral infection.
53

Lymfeklieren hals
54

Lymfeklieren hals: van ventraal
55

Lymfeklieren hals
onderzoek van dorsaal
56

Klieren axillair
57

Klieren axillair
58
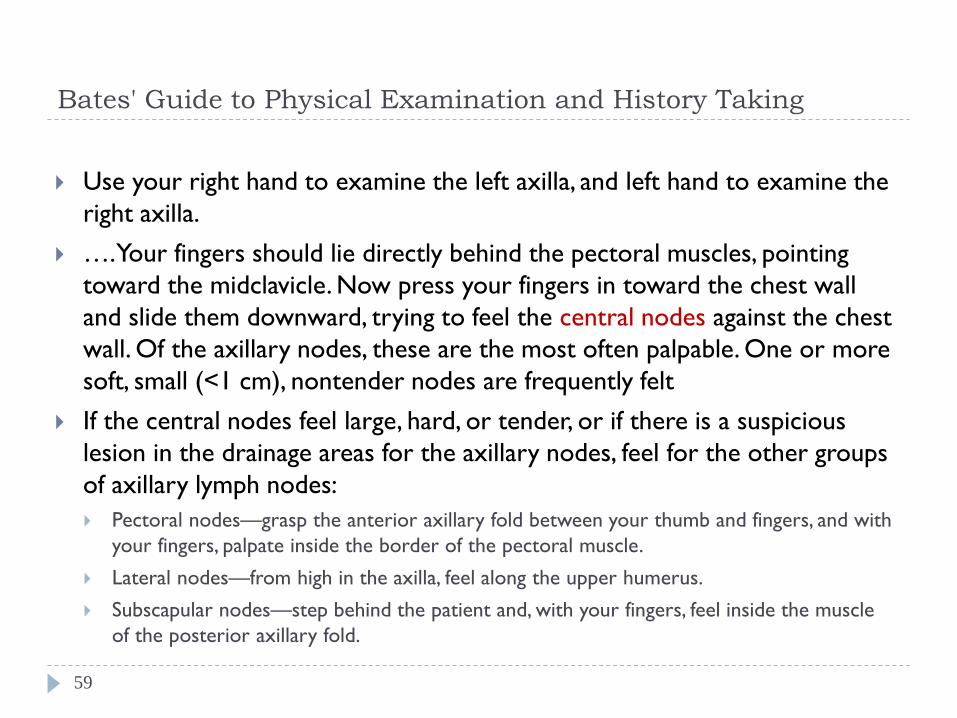
Bates' Guide to Physical Examination and History Taking
Use your right hand to examine the left axilla, and left hand to examine the
right axilla.
…. Your fingers should lie directly behind the pectoral muscles, pointing
toward the midclavicle. Now press your fingers in toward the chest wall
and slide them downward, trying to feel the central nodes against the chest
wall. Of the axillary nodes, these are the most often palpable. One or more
soft, small (<1 cm), nontender nodes are frequently felt
If the central nodes feel large, hard, or tender, or if there is a suspicious
lesion in the drainage areas for the axillary nodes, feel for the other groups
of axillary lymph nodes:
Pectoral nodes—grasp the anterior axillary fold between your thumb and fingers, and with
your fingers, palpate inside the border of the pectoral muscle.
Lateral nodes—from high in the axilla, feel along the upper humerus.
Subscapular nodes—step behind the patient and, with your fingers, feel inside the muscle
of the posterior axillary fold.
59

60

Lymfeklieren inguinaal
61
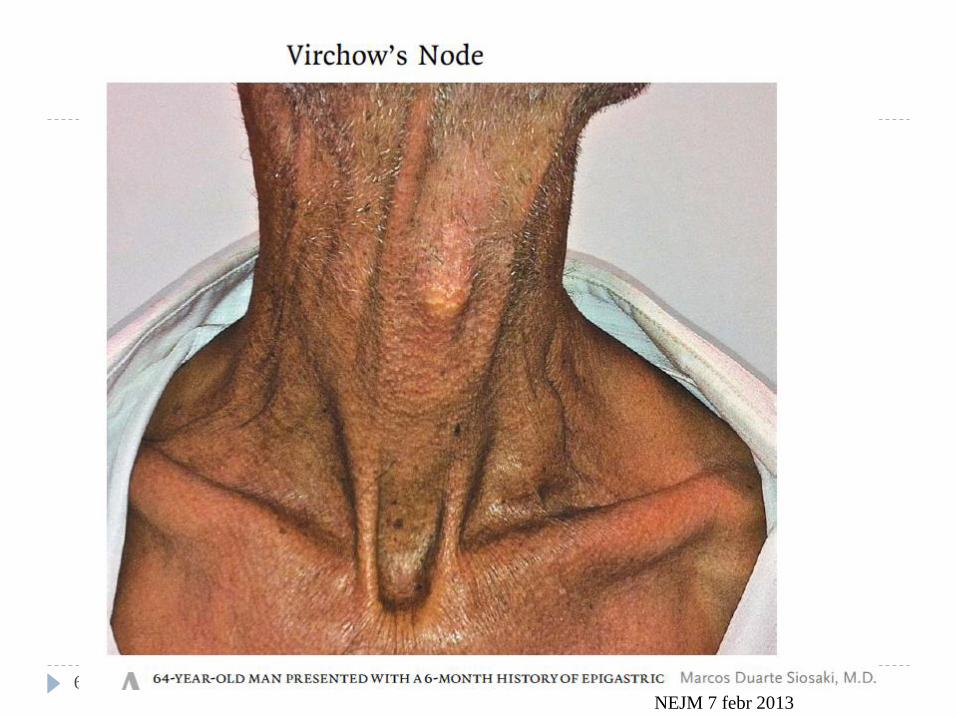
62 NEJM 7 febr 2013

Klinisch onderzoek
• Algemeen onderzoek (lymfeklieren)
• Onderzoek van hoofd en hals
• Onderzoek van de thorax (longen)
• Cardiovasculair onderzoek
• Abdominaal onderzoek
• Locomotorisch onderzoek
• Neurologisch onderzoek
63

Onderzoek van hoofd en hals
schedel en haar
gelaat
huid
ogen
neus
mond en keel
oren
schildklier
(klierstreken : cfr supra)
64

Ogen
(neurologisch:oogbewegingen, pupillen,...)
(zichtscherpte, gezichtsveld)
(“rode ogen”)
(oogziekten: (zie Bates’ 11 th ed. tabel 7.7-7.8)
Ooglidafwijkingen
“Bulten en zwellingen” in en rond het oog
Schildklierdysfunctie
Anemie
Icterus
Lipidenstoornissen
65

Ptosis
entropion ectropion
66

Xanthelasmata: (gele, vlakke, licht verheven tumoren in de ooglidhuid)
67
Kan (bij jonge mensen) duiden op lipidenstoornissen
(zie evt http://www.ntvg.nl/publicatie/xanthelasma-palpebrarum/volledig)

Hordeolum
(ontsteking van kliertje
op rand van ooglid)
Dacrocystitis
(ontsteking traanzak
68
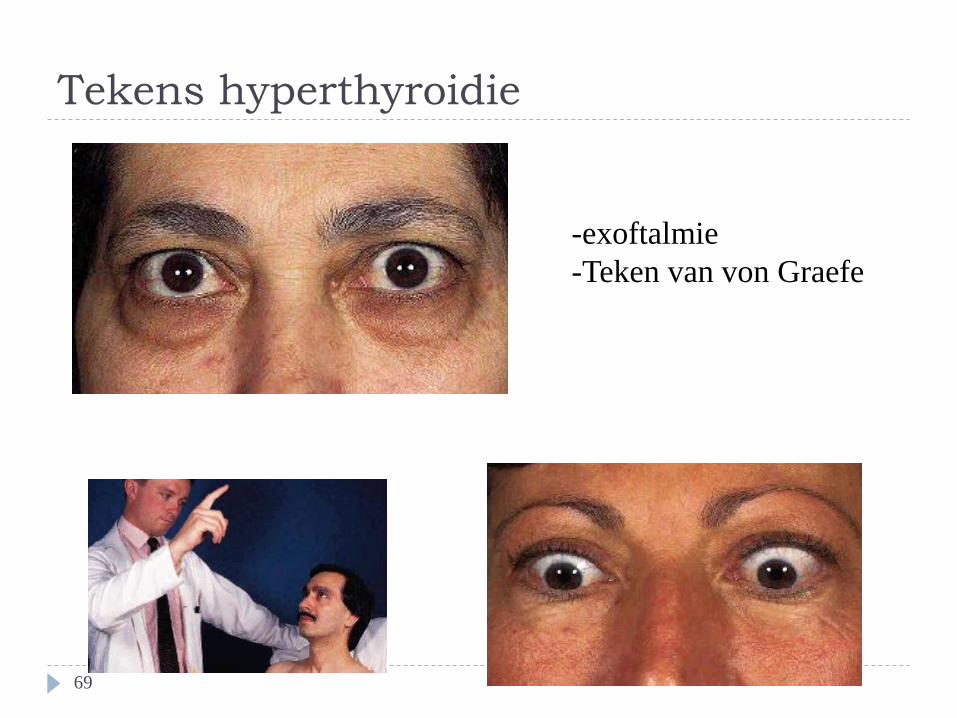
Tekens hyperthyroidie
Bilateraal ooglidretractie
Oogleden volgen blik niet
69
-exoftalmie
-Teken van von Graefe

Tekens hyperthyroidie
Pro-optose / exoftalmie 70

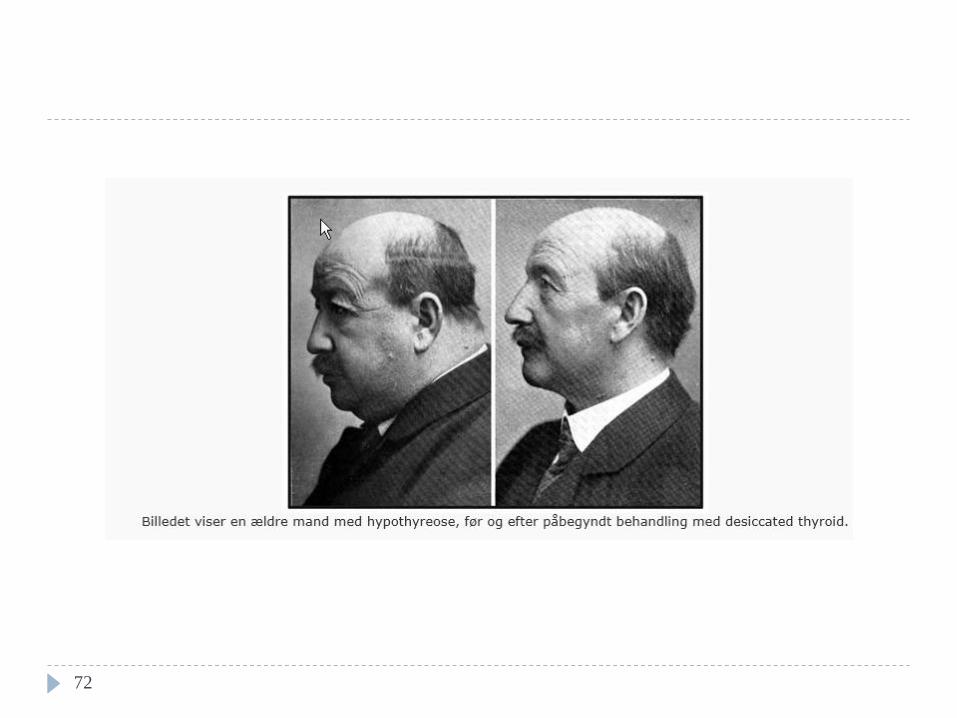
Tekens hypothyroidie :
myxoedeem
71
72
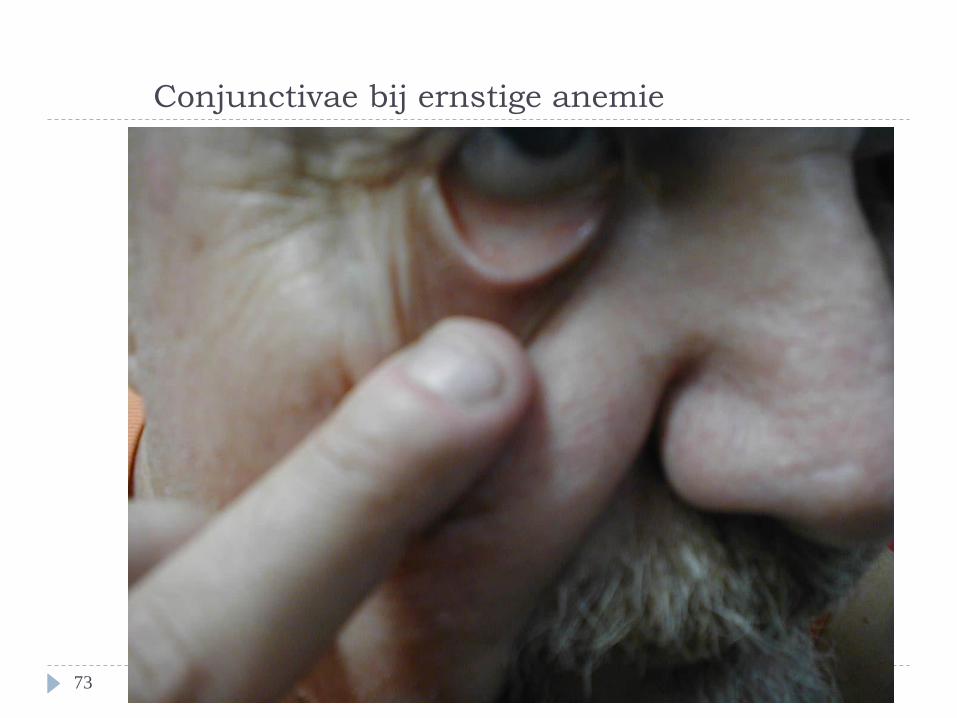
Conjunctivae bij ernstige anemie
73

74

Arcus senilis: indien bij jongere patienten : hoger risico
op coronair lijden
75

Onderzoek van de neus
Inspectie
evt evaluatie doorgankelijkheid
76

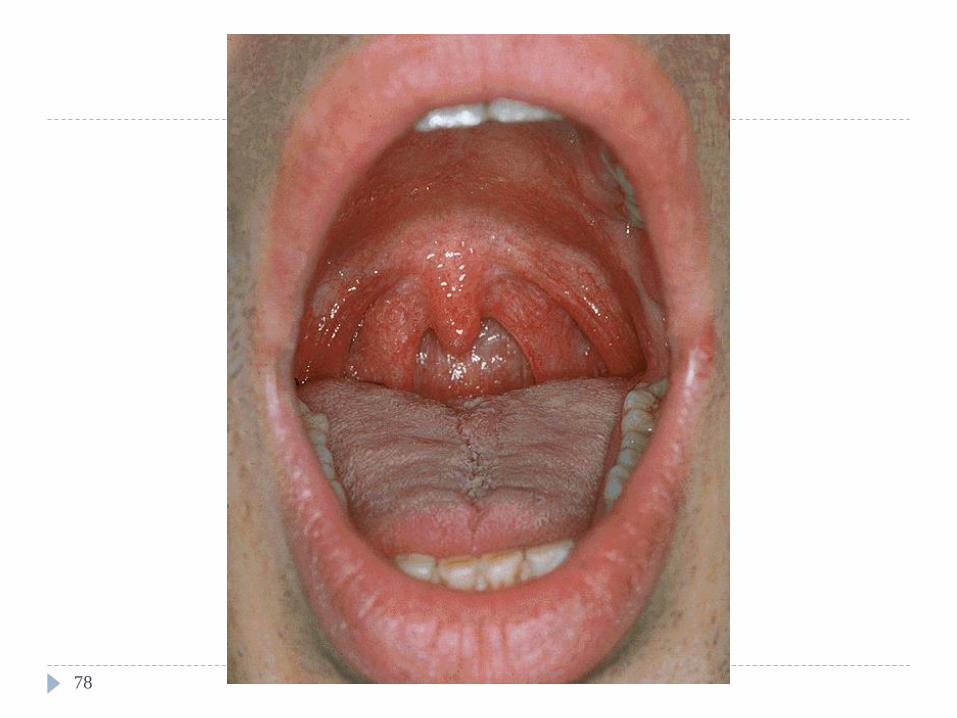
Onderzoek van mond- en
keelholte gebruik van tongspatel en lichtbron
vals gebit laten verwijderen
Systematisch onderzoeken (“van buiten naar binnen”)
inspectie tanden, gingivae, tong, wangslijmvlies, verhemelte,
mondbodem : tong met punt tegen verhemelte laten duwen
tong laten uitsteken (n. XII)
"AAA" laten zeggen : om achterste pharynxwand en amandels
te zien. (Vaak hiervoor nood aan tongspatel).
77
78

Papilla ductus parotidei
79

frenulum
Plica fimbriata
Plica sublingualis
Caruncula sublingualis
80

Lee H and Jo D. N Engl J Med 2009;360:e8
A 77-year-old woman presented with an insidious onset of fatigue and a burning sensation of the tongue on
swallowing food
A 77-year-old woman presented with an insidious onset of fatigue and a burning sensation of the tongue on swallowing food. Six
years earlier, she had undergone a total gastrectomy. On physical examination, she was pale and had a depapillated, smooth, shiny
red tongue with some central fissuring, findings that were consistent with a beefy red tongue (Panel A). Laboratory testing
revealed cytopenia (white-cell count, 3400 per cubic millimeter; hemoglobin level, 6.4 g per deciliter; and platelet count, 154,000
per cubic millimeter) with macrocytosis.
The serum vitamin B12 level was 55 pg per milliliter (normal range 118 to 716), and the serum folate level was normal. The patient
received a diagnosis of megaloblastic anemia due to vitamin B12 deficiency. She was treated with intramuscular vitamin B12 and
had a complete recovery after approximately 5 months. A smooth, thickened, depapillated tongue may be associated with a variety
of systemic disorders, including nutritional deficiency.
81

“fissured tongue” en lingua geographica
Fissured tongue, also known as scrotal tongue or lingua plicata, is a benign condition
characterized by deep grooves (fissures) in the dorsum of the tongue.
(Fissured tongue is seen in Melkersson-Rosenthal syndrome, in most patients with Down syndrome,
and in association with geographic tongue).
82

Landkaarttong of lingua geographica (bron Wikipedia)
Its cause is uncertain, though tends to run in families and is associated with several different genes. Geographic
tongue is more commonly found in people who are affected by environmental sensitivity, such as allergies,
eczema, and asthma. Some think that it may be linked to stress or diets high in sugar or processed foods. Its
prevalence also varies by ethnicity (0.6% of Americans, 4% of young Iraqis, 2% of young Finns) and gender
(females affected 3 times more than males). Causes vary, but may include vitamin deficiencies, allergies, and
hormonal changes. Geographic tongue is said to occur more often in women, especially during high hormonal
times such as during ovulation or pregnancy, and while taking birth control[1].
Studies show that there is a link between geographic tongue and psoriasis.[
83

Perleche of (angulaire) cheilitis
Ijzergebrek
Candida
Vitamine B (2) deficiëntie
Ook vaak bij oudere personen na tandverlies
84
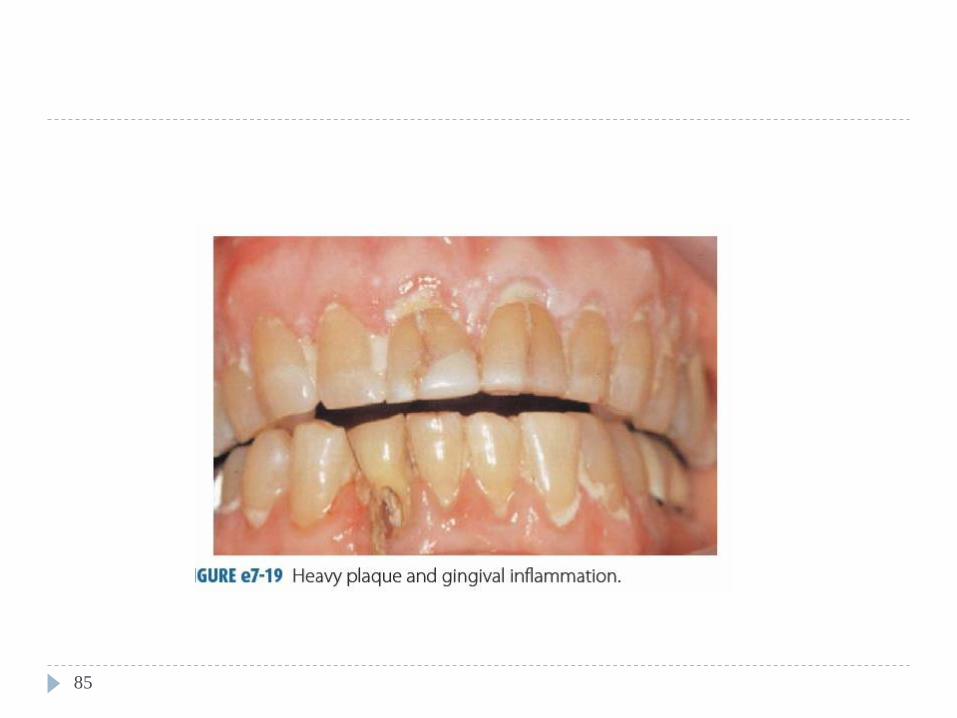
85

86

Tjwa E and Mattijssen V. N Engl J Med 2008;359:e21
A 46-year-old woman who was not taking any medications presented with anemia and gingival hypertrophy
that had been progressing over a period of 3 months
Diagnose: leukemie 87

Cureton E and Kim S. N Engl J Med 2007;357:e9
A previously healthy 12-year-old boy presented with abdominal pain, vomiting, and abdominal distention of
3 days' duration
The diagnosis was Peutz-Jeghers syndrome, an autosomal dominant
disorder characterized by the development of multiple hamartomatous
gastrointestinal polyps, mucocutaneous pigmented lesions on the lips or
buccal mucosa, and an increased risk of cancer within and outside the
gastrointestinal tract.
88

Orale candidiase
89

Onderzoek van de oren
90

How to Use an Otoscope (Simon Carney)
• Can I clearly see all the external
auditory canal?
• Can I see the tympanic membrane or
the handle of the malleus, or both?
• Is the tympanic membrane intact
(dwz : vorm)
• Is the tympanic membrane the right
colour and transparency?
voor achter
http://student.bmj.com/back_issues/0795/7-otos.htm (link werkt niet meer)
91

Normaal
Re trommelvlies
An annulus fibrosus
Lpi long process of incus - sometimes visible through a
healthy translucent drum
Um umbo - the end of the malleus handle and the centre
of the drum
Lr light reflex - antero-inferioirly
Lp Lateral process of the malleus
At Attic also known as pars flaccida
Hm handle of the malleus
voor
http://www.bris.ac.uk/Depts/ENT/otoscopy_tutorial.htm 92

93
Zie ook:
http://www.youtube.com/watch?v=FE0sot4OoAE
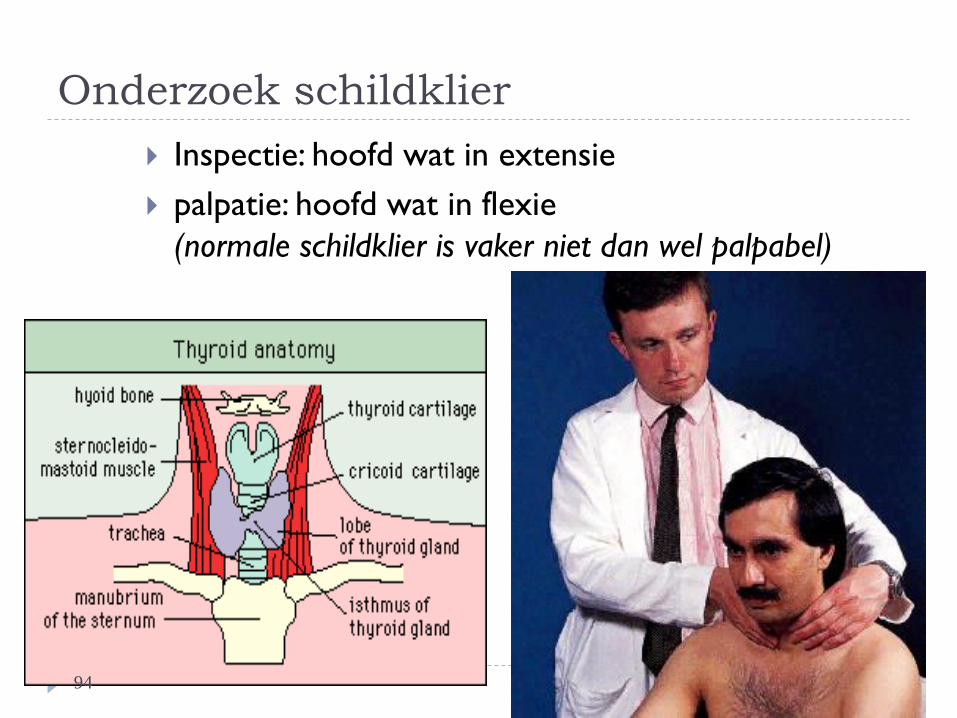
Onderzoek schildklier
Inspectie: hoofd wat in extensie
palpatie: hoofd wat in flexie
(normale schildklier is vaker niet dan wel palpabel)
94

95
Mooie (korte) video: http://stanfordmedicine25.stanford.edu/the25/thyroid.html

96
Put your finger on tip of your chin (mentalis).
Slide finger down the midline and the first hard structure you hit is the top of
the thyroid cartilage. (Surprisingly, one does not feel the hyoid bone in the
midline, although sometimes its lateral end is misidentified as a hard lymph
node).
Run your finger down the prow or the free edge of the thyroid cartilage
(Adam's apple).
The next thing you hit is the cricoid cartilage (and see if you can get your
fingernail in between the thyroid and cricoid cartilage–that is the cricothyroid
membrane which is where trans-tracheal aspirations for pneumonia can be
performed).
Inoefenenen palpatie schildklier:
Do this on yourself or someone:
Bron:
http://stanfordmedicine25.stanford.edu/the25/thyroid.html

97
Below the cricoid ring are the first two rings of the trachea, and the
ISTHMUS of the thyroid overlies those two rings.
Ask patient to flex neck slightly forward and relax.
Go through the landmarks as above.
Place first two digits of both hands just below cricoid cartilage so that left
and right fingers meet on the patient’s midline. Place thumbs posterior to
patient’s neck and flatten all fingers against the neck.
Use finger pads, not tips, to palpate.
Identify the isthmus.
Gently draw fingers laterally 1-2cm.
Gently palpate lateral lobes.
NOW ask patient to swallow (give them a glass of water if possible).
Assess for asymmetrical elevation of lobes (suggests nodularity).
When you are done with above, move to next phase, which is displacing
the soft tissues on one side to the midline while assessing for size with the
other hand. Repeat in opposite direction.

Goiter
98

99

100

101

Ausculatie schildklier
102
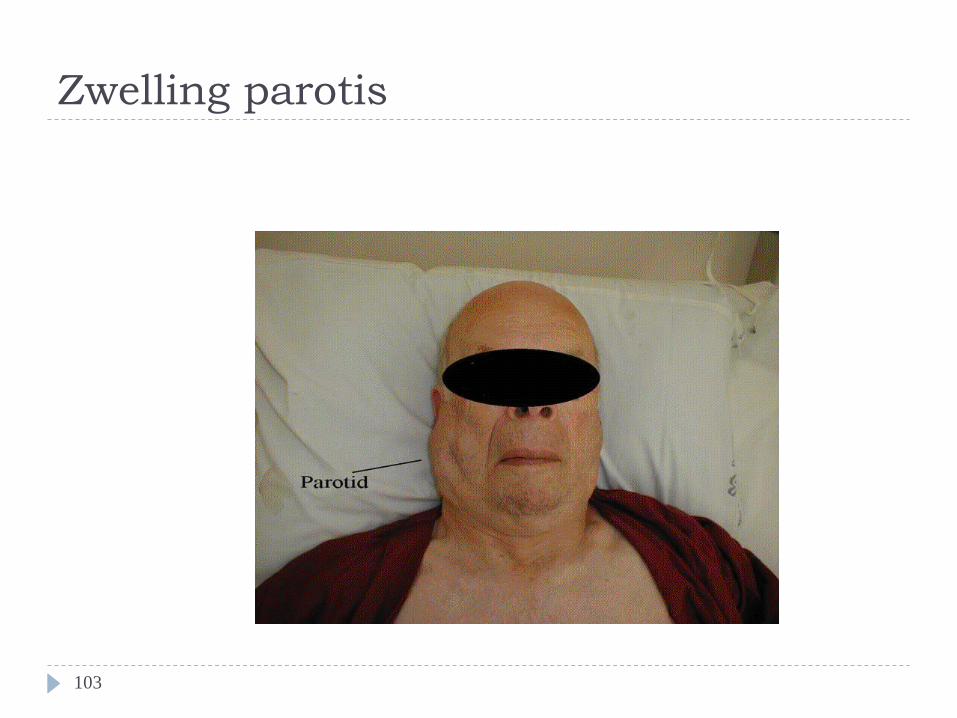
Zwelling parotis
103
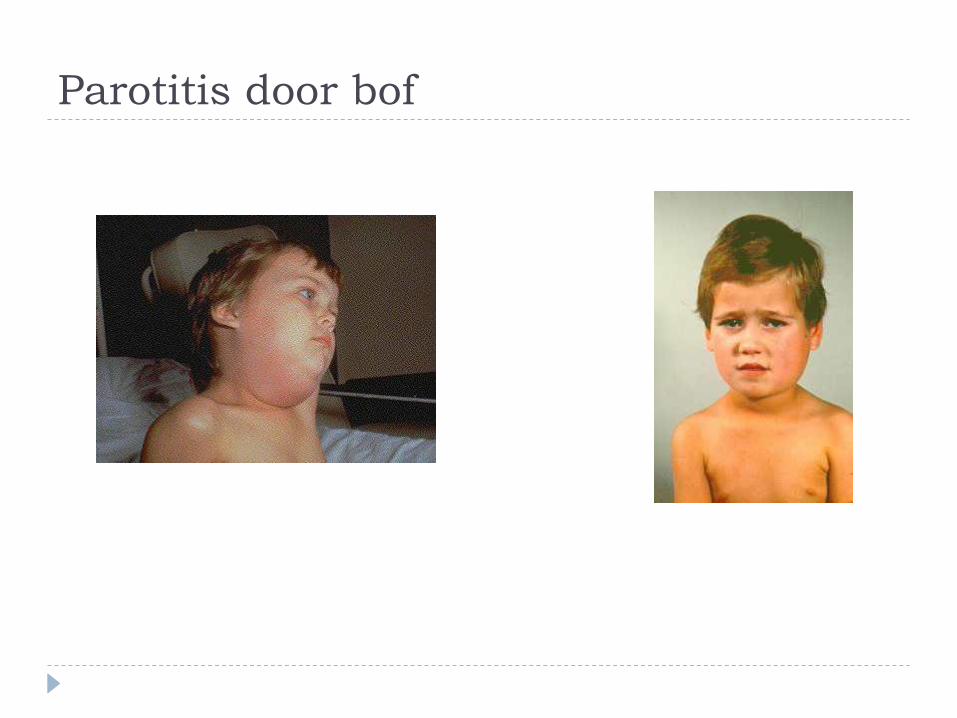
Parotitis door bof
Top Related