






Languages
Pages
Legal

Two Palliative Care Giants
Dr Jennifer VidrineST4 Palliative Medicine
Overview
• A broad overview of palliative care in relation to general practice
• Pain• Case 1• BREAK• Nausea and Vomiting• Case 2 • Round Up
Palliative Care
• Recognised as distinct entity since 1980s• First modern hospice opened 1967• Based on concept of ‘Holistic’ care • Palliative care teams• Not just for patients with cancer

GPs and palliative care

• “GPs found looking after palliative care patients satisfactory and varied but burdensome”
• Found barriers on three levels:– Personal– Relational – Organisational

Challenges faced…• Personal– Knowledge symptom and symptom control– Technical procedures in pts who want to stay at
home (ie Catheter)– Small numbers of palliative care patients in a year– Emotional – Time constraints– Lack of psychological support in an autonomous
worker

• Relational– Communication• Between pts, carers, other HCPs
– ‘Territory’ (GP? SPCT? Hospital team?)

• Organisational– Bureaucracy– Obtaining medications (Controlled drugs, CSCI etc)– Need to organise care/social work review etc

They conclude
• Barriers exist• It is imperative to support GPs as the frontline
of service provision• Role of specialist palliative care teams in this
(both specialist knowledge and emotional support)

Common Symptoms
• Pain• Nausea and Vomiting• Shortness of Breath• Anxiety/Psychological Distress

Common Symptoms
• Pain• Nausea and Vomiting• Shortness of Breath• Anxiety/Psychological Distress

Pain

Nociceptive vs neuropathic pain

Nociceptive vs neuropathic pain

Neuropathic pain
• Disproportionate to stimulation of the nociceptor
• Leads to:– Hyperalgesia (exaggerated and prolonged pain response to a mildly painful stimulus)– Allodynia(Pain produced by a stimulus that is not normally painful, such as light
touch)– Spontaneous pain
• No protective function
• Pathological pain

Distinguishing the two…
• History History History• Thinking abut possible/likely aetiologies• What has the pain responded to thus far?

• Very often in palliative care it is a combination of both
• Requires combination treatments (Often one won’t cut it)
• Often requires some lateral thinking

WHO analgesic ladder


An approach…
• Patient specific• Tend to start with low dose strong opiate
(eg Oramorph 2.5-5mg PRN)• If possible also give regular paracetamol• Ask patient/relative to write down the
following:
Date Time Site Pain Pain score /10 before
What taken
Pain Score /10 after
Notes/Side effects

• Review in a couple of days.• Establish if opioid making ANY difference• Establish any side effects• Calculate what has been taken in last 24 hours
(ie 4 doses of 5mg=20mg)• Start BD preparation of long acting opiate• Explain need to continue with Breakthroughs
and ongoing monitoring.• Breakthrough is 1/6 total daily opioid dose
(except Alfentanil which is 1/10th)

Established on Morphine but still in pain?
• Would an adjunct help?Steroids (Dexamethasone)TCA (Amitriptyline)Anti-epileptics (Gabapentin/Pregabalin)
• Very often end up on combination

Evidence Base
• Amitriptiline-OD dosing, syrup available.
• Gabapentin- syrup available, TDS
• Pregabablin- ?more tolerable, BD, only tablets
• Valporate- OD, syrup available, RCT conflicting
• Clonazepam- Concurrent anxiolytic and muscle relaxant properties, SC
Anti-epileptic NNT
Carbmazepine 3.3
Gabapentin 3.5
Lamotrigine 4
Sodium valporate
2-2.5?

Other things to consider
• NSAIDs– If no contra-indications– Esp if inflamm element of pain– Useful in bone pain– Ibuprofen used most frequently– Ketorolac useful as can be used subcut (Generally
only for short spells/at end of life)• Bisphosphonates

Particular Challenges
• Episodic Pain• High anxiety element (Total pain)• Non-concordance
Consider referral/involvement SPCT
What might be offered…
MethadoneKetamineSpinal Lines (epidural/intrathecal line)Nerve BlocksCordotomy (Division of lateral spinothalamic
tracts in the spine)Involvement of clinical psychology

Case 1
• Break up into groups of 3-5• Look at the case and start to think about the
issues involved for 20 mins• Try to approach as holistically as possible• Feed back to group.

Comfort Break
Nausea &
Vomiting

Nausea & Vomiting-Background
• Extremely common in cancer patients• Deeply distressing• Vomiting generally tolerated better than
nausea
“Last night we went to a Chinese dinner at six and a French dinner at nine, and I can feel the shark’s fins navigating unhappily in the Burgundy”Peter Flemming, Letter from Yunnanfu, March 1938

Reality of the situation
• Often as/more challenging to treat than pain• Many patients have multifactorial N&V• Absorption of the very stuff we are giving
them to make them better• May well require more than one anti-emetic• Systematic/logical approach….

Questions to ask
• Nausea/vomiting predominant?• Timing?• What is vomited? (Consistency, volume, colour)• Feel better after vomiting?• Associated features?• Exacerbating/relieving factors• Are there are any probable causes? (eg
Constipation)
Identify specifically treated causes
• Constipation-Laxatives/PR intervention (Prevention)• Gastritis-Would PPI help?• Oropharyngeal Candida-Often difficult to treat• Hypercalcaemia-IV hydration +/- Bisphosphonate• Pain-Optimise analgesia• If drug induced how essential is drug?• Treat infection

• Think about non-drug measures• Select anti-emetic based on most likely cause• Basic principals:– Give regular antiemetics– Need to carefully assess risk of non-absorption
and consider alt routes (CSCI) early– If you are relatively sure about cause consider
maximising dose rather than switching (esp Metoclopramide)

Two ‘broad’ avenues..
1.Gastric-stasis2.Chemically mediated (central)

1. Gastric Stasis-presentation
• Early Satiety• Large volume vomits• Undigested food• Relief after vomiting• Hiccoughs/belching• Exacerbated by eating/medcations

1.Gastric stasis-causes
• Slowed gastric emptying• ‘Squashed stomach’ due to Hepatomegally• Ascites• Subacute obstruction (consider specialist
input)

1.Gastric Stasis-management
• Prokinetic eg Metoclopramide• Targets peripheral (and central) Dopamine (D2)
receptors.• Caution in young females• CAUTION IN PARKINSON’S DISEASE/SYNDROMES• Dose: 10-20mg tds/qds– CSCI 30-120mg/24 hours
• Domperidone (less side effects but limited routes)
• OBSERVE FOR INTESTINAL COLIC

Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZMetoclopramide

Two ‘broad’ avenues..
1.Gastric-stasis2.Chemically mediated (central)

2.Central Causes-presentation
• Constant nausea• No/little relief after vomiting• May be able to identify cause• Other signs drug toxicity

Central-Causes
Drugs:OpiatesAntidepressantsAEDs
Electrolyte ImbalanceRenal FailureHypercalcaemia
SepsisAnxietyPainRaised Intracranial
PressureIschemic Bowel

2. Central Causes-Management
Cyclizine• Antihistaminic/Anticholinergic antiemetic acting
at AChM and H1 receptors• Acts centrally to help with vagally mediated
nausea.• Can give anticholinergic side effects• Dose: 25-50mg tds– CSCI: 150mg/24 hour
• Particularly useful if raised intracerebral pressure

Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZ
Cyclizine

2. Central Causes-Management
Haloperidol• Useful for chemical induced nausea (inc
Drug induced) • Centrally acting anti-emetic acting at D2 receptor at the
CTZ• Contraindications• Dose: 1.5mg Nocte (0.5-1.5mg bd)– CSCI: 2.5-5mg/24 hours
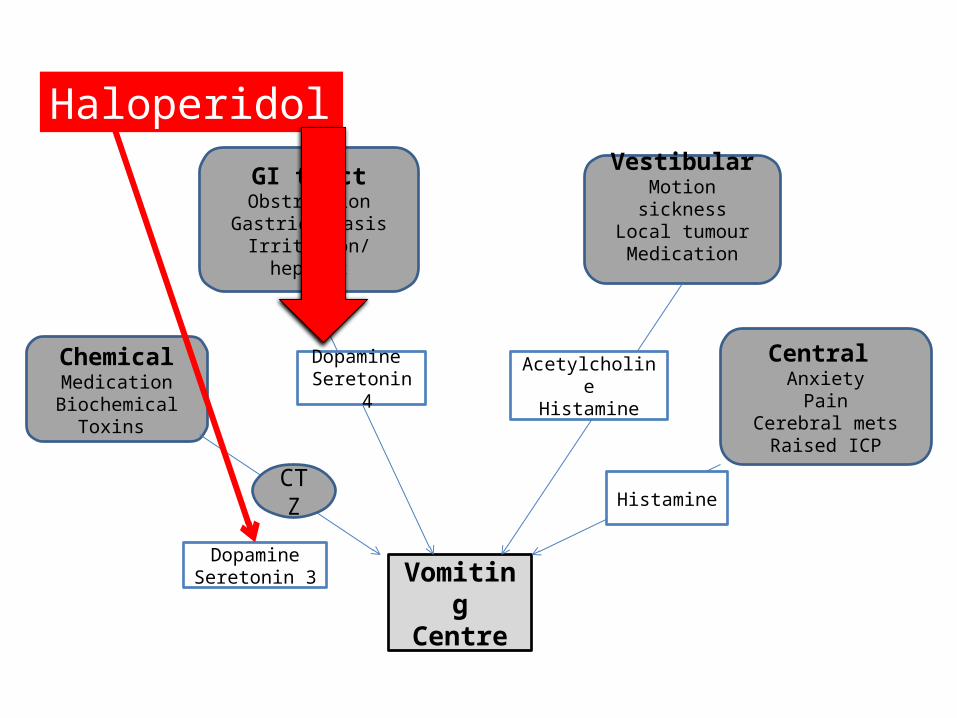
Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZ
Haloperidol

If at first you don’t succeed
• Remember often multifactorial• Consider increasing dose• Consider combinations (that target diff
receptors)• Dex 4mg will often enhance affect anti-emetic
(unknown mech)• Levomepromazine

Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZ
Levomepromazine

Chemotherapy Induced N&V
• Ondansetron often used• Best to time limit it’s use• Headaches • Constipation• Has a very specific role• Consider anticipatory n&v– Levomepromazine– Lorazapam

Case 2
• Break up into groups of 3-5• Look at the case and start to think about the
issues involved for 20 mins• Try to approach as holistically as possible• Feed back to group.

In summary
• A whistle stop tour of two pretty meaty subjects
• The importance of a thorough assessment in managing symptoms
• The importance of a systematic approach in managing them
• Make use of community SPCT/hospice advice lines if in doubt.

Any questions?

Watson, M. Lucas, C. Hoy, A. Wells, J (2010) The Oxford Handbook of palliative care. Oxford university press.
Twycross, R. Wilcock, A. Palliative care formulary 4th Edition (2012) Palliativedrugs.com
Groot, M. Vernooij-Dassen, M. Crul, B. Grol, R. (2005) General practitioners (GPs) and palliative care: percieved tasks and barriers in daily practice. J Pall Med. (19)111-118
Top Related