





Languages
Pages
Legal


Title Investigating the role of genetic counseling in neuromusculardisease considering life events
Author(s) Shibata, Yuka; Yabe, Ichiro; Matsushima, Masaaki;Hashimoto, Naoki; Yamada, Takahiro; Sasaki, Hidenao
Citation Journal of Human Genetics (2019), 64: 551-559
Issue Date 2019-06
URL http://hdl.handle.net/2433/241614
Right
This is the accepted manuscript of the article, which has beenpublished in final form at https://doi.org/10.1038/s10038-019-0590-8.; The full-text file will be made open to the public on13 September 2019 in accordance with publisher's 'Terms andConditions for Self-Archiving'.; This is not the publishedversion. Please cite only the published version. この論文は出版社版でありません。引用の際には出版社版をご確認ご利用ください。
Type Journal Article
Textversion author
Kyoto University

1
[Title] 1
Investigating the role of genetic counseling in neuromuscular disease considering life events 2
3
[Short running title] 4
Genetic counseling in neuromuscular disease considering life events 5
6
Manuscript word count:4,219 words 7
Tables:2, Figure:2, Additional Figure:2 8
9
[Authors] 10
Yuka Shibata1, Ichiro Yabe1,2*, Masaaki Matsushima1,2, Naoki Hashimoto3, Takahiro Yamada4, 11
Hidenao Sasaki1,2 12
13
1. Division of Clinical Genetics, Hokkaido University Hospital, Sapporo, Japan 14
2. Department of Neurology, Faculty of Medicine and Graduate School of Medicine, Hokkaido 15
University, Sapporo, Japan 16
3. Department of Psychiatry, Faculty of Medicine and Graduate School of Medicine, Hokkaido 17
University, Sapporo, Japan 18
4. Clinical Genetics Unit, Kyoto University Hospital, Kyoto, Japan 19

2
1
*Corresponding author: Ichiro Yabe 2
Department of Neurology, Hokkaido University Graduate School of Medicine, Sapporo, Japan 3
Kita-15, Nishi-7, Kita-ku, Sapporo 060-8638, Japan 4
Tel: +81-11-706-6028 5
Fax: +81-11-700-5356 6
E-mail; [email protected] 7
8
[Conflict of Interest] 9
None declared. 10
11
12
13
14
15
16
17
18
19

3
Abstract 1
Genetic diagnoses are becoming routine in the medical practice of neuromuscular diseases. 2
Many diagnoses, however, can have an influence on relatives and family members and thus must be 3
handled carefully by genetic counseling (GC). Here, we aimed to assess the purpose of undergoing GC 4
to verify the utility of collaborations between clinical and genetic divisions. We investigated 5
consecutive GC cases of neuromuscular disease and examined the role of GC. Our study included 102 6
cases who underwent GC in our hospital from July 2005 to March 2018: 86.3% were women, and 7
45.1% were in their 30’s. Disease explanation was the most common reason for attending GC (29.4%), 8
followed by prenatal diagnosis (25.5%), pre-symptomatic diagnosis (17.6%) and carrier diagnosis 9
(14.7%). Clients typically visited the hospital for GC when some kind of life event occurred, such as 10
marriage, desire to bear a child, or change in condition of the proband. Clinicians should be conscious 11
of such life events from the perspective of both the client and their relatives, and guide the GC at an 12
appropriate time. Overall, the degree of recognition of genetic risk by clients differed, thus it is 13
important for GC to determine the status of each unique situation and respond individually. 14
15
16
17
18
19

4
Introduction 1
Genetic testing is an effective approach to gain a definitive and differential diagnosis in 2
neuromuscular diseases. A survey conducted in 2013 of >1400 certified neurologists in Japan, reported 3
that 82.6% had some experience with genetic testing1. Because genetic information does not change 4
in our lifetime and is shared with relatives, the impact of obtaining genetic information is large. 5
Although genetic testing is performed in daily clinical practice, special attention should be paid to 6
these shared characteristics of genetic information when a genetic test is performed. 7
Genetic counseling (GC) aims to help people understand and cope with the medical, psychological and 8
familial implications of genetic contributions to disease2. Saskia et al. (2012) indicated that GC is 9
essential before and after genetic testing because the result of genetic testing affects not only the patient 10
but his/her family3. On the other hand, Valente et al. (2008) indicated that GC prior to diagnostic testing 11
is optimal, but not mandatory for pediatric neurological disorders4. According to the 2011 guidelines 12
on genetic testing published by the Japanese Society of Medicine5, the attending physician should give 13
informed consent to patients who are symptomatic before genetic testing. If necessary, the physician 14
should consider referring his/her patient to receive expert GC so that the patient receives appropriate 15
support when the results are available. Meanwhile, in cases where relatives are contacted for genetic 16
testing (e.g. to make a non-progressive carrier diagnosis, pre-symptomatic diagnosis or prenatal 17
diagnosis), they should also undergo GC. GC is typically carried out in multidisciplinary teams due to 18
the wide range of often rare disorders that can be identified by genetic testing. Unfortunately, GC is 19

5
currently difficult to perform in the daily clinical setting because many doctors don’t have enough time 1
to gain the appropriate skills and knowledge to implement GC in busy daily practice. Therefore, it is 2
necessary to train GC experts and provide resources for GC program development6. General 3
practitioners instead, must understand the value of GC, identify those who require urgent GC and then 4
refer them to a specialized GC facility1,7. In Japan, expert clinical geneticists (physicians) and certified 5
genetic counselors (non-physicians) take charge of GC. Both experts must be certified by the Japan 6
society of Human Genetics8 and the Japanese Society for Genetic Counseling9. As of January 2019, 7
there are 1,387 clinical geneticists in Japan10. Since 2002, these clinical geneticists have been permitted 8
to respond to consultations from attending physicians from any department and conduct the appropriate 9
genetic service (including GC). As of December, 2018, there are 243 CGCs in Japan11. Since 2005, 10
these certified genetic counselors (CGC) can support clients with clinical geneticists, from an 11
independent stand point. CGCs must study medical genetics and obtain a Master’s degree in counseling, 12
and can then take employment in many different contexts, including hospitals, universities and 13
companies. At present, 115 institutions in Japan have a clinical genetics department12 that is available 14
for consultations with patients or relatives affected by hereditary neuromuscular diseases. 15
Many refractory neuromuscular diseases, such as Huntington’s disease, have been proposed 16
to require special consideration for “refractory” disease during pre-symptomatic diagnosis13-15, as well 17
as non-progressive carrier and prenatal diagnosis16. The role of GC without limiting its purpose to only 18
genetic tests needs to be examined to help understand the best methods of collaboration between 19

6
medical and genetic departments and determine the needs of the genetic division. Such studies will 1
improve genetic literacy as well as national welfare. 2
Here, we investigated the role of GC in patients with neuromuscular disease who were 3
referred to our hospital, and examined the motivations of clients to attend. To the best of our knowledge, 4
no report to date has comprehensively examined the role of GC specifically in clients affected by 5
neuromuscular disease. All GC for relatives seeking non-progressive carrier testing, pre-symptomatic 6
testing or prenatal testing and preimplantation genetic testing is available in our hospital. However, 7
because some genetic tests requested by relatives are not available in our hospital, some clients were 8
referred to other institutions after attending GC in our hospital. 9
10
Materials and Methods 11
Study design 12
This exploratory, retrospective observation study used the information described in the GC 13
medical record. 14
15
Patient inclusion 16
A total of 102 consecutive cases of neuromuscular disease in which GC was performed were 17
initially recruited to this study between July 2005 and March 2018. Patients were excluded if they or 18
their proxy refused to participate (i.e. did not provide informed consent) in this study. No patients 19

7
refused to participate. 1
2
Survey items 3
Information regarding the age, gender, family relationship, target disease, and presence of 4
accompanying person at GC was taken for each patient. The purpose of the GC visit, the motivation 5
of the visit and the outcome was extracted from individual patient medical records. We extracted 6
main purpose and motivation for GC visit from medical charts of the cases. The extraction was made 7
by discussion in multiple authors. 8
9
Ethical considerations 10
This study was conducted with approval of the Hokkaido University Hospital Institutional 11
Review Board. 12
13
Results 14
Background of the clients attending GC 15
Our retrospective study included 102 clients who visited the department of clinical genetics, 16
of which 86.3% were women (Table 1). The age distribution ranged from <20 to >70 years, with the 17
majority patients aged 30-39 years (45.1%), followed by patients aged 20-29 years (30.4%). Most of 18
the individuals who were undergoing GC were relatives (75.5%), of which 74.0% were first-degree 19

8
relatives (i.e. parents, children and siblings), and 18.6% were patients with a neuromuscular disorder. 1
Of the neuromuscular diseases covered by the patients, relatives and other clients, the most common 2
was Duchenne muscular dystrophy (DMD; 22.5%), followed Spinocerebellar degeneration (SCD; 3
17.7%), and myotonic dystrophy (DM1; 13.7%) (Table 2). 4
5
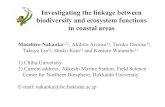
Purpose of the visit 6
Most of the clients requiring GC (29.4%) were looking for an explanation of the disease in 7
question (Figure 1): here, 26.7% were patients, 60% were relatives and 13.3% were non-relatives. 8
During GC, we found that the patients themselves (particularly those affected by DM1) also requested 9
a more detailed explanation about the disease (Additional figure 1a). DMD was the most common 10
disease (38.5%) for which affected clients wanted genetic counseling prior to a prenatal diagnosis 11
(38.5%). Here, two women had suspected DMD based on high creatine kinase values and muscle 12
weakness and were diagnosed as symptomatic carriers. There were two diseases (amyotrophic lateral 13
sclerosis and spinocerebellar degeneration) for which prenatal diagnosis was not performed in our 14
hospital (Additional figure 1b). Of the 18 clients (17.6%) who underwent GC for pre-symptomatic 15
diagnosis, the majority were suspecting SCD (44.4%). Only two clients (11.1%) with Huntington's 16
disease had been reported by many previous studies about pre-symptomatic diagnosis. Only one client 17
required consultation for a disease (namely, familial amyloid polyneuropathy) where a disease 18
modifying therapy was established. Because the degree of onset, mitochondrial disease was difficult 19

9
to predict from genetic testing results and was thus not applicable for obtaining a pre-symptomatic 1
diagnosis (Additional figure 1c). Finally, 15 (14.7%) clients underwent GC for a non-progressive 2
carrier diagnosis; all of these cases were with regard to X-linked diseases (Additional figure 1d). Of 3
the remaining clients, nine wanted to obtain a definitive diagnosis by genetic testing and four wanted 4
a deeper explanation of the test results. 5
Motivation to attend GC 6
Patients themselves 7
We next examined the opportunities that clients had to attend the hospital for GC. The affected 8
patients themselves formed the majority (36.8%) of the group that had most opportunity for GC 9
because they had considered genetic testing. Among them, there were patients who had been given a 10
clinical diagnosis of SCD despite not carrying pathogenic variants with high frequency for this disease. 11
In addition, there were patients who were suspected symptomatic carriers of DMD but exhibited rare 12
clinical symptoms that could not be managed at local hospitals. One patient attended GC to discuss 13
the timing of genetic testing as they were considering the consequential effects on their relatives. Three 14
clients (15.8%) visited after receiving a genetic diagnosis, seeking a more detailed explanation of the 15
disease and to discuss the best timing to communicate the results to their relatives. Five clients (26.3%) 16
attended GC as a result of pregnancy and/or desire to bear a child. Here, the clients wanted to discuss 17
the genetic influence on the next generation and their options for a prenatal diagnosis. Two clients 18
(10.5%) attended because relatives wanted a pre-symptomatic diagnosis, one client (5.3%) 19

10
consultation from the attending physician and for one client where the consultation center existed 1
(Additional figure 2a). 2
Relatives of patients 3
The majority of relatives (51.9%) attended GC on the basis of pregnancy and/or desire to bear 4
a child: 21 clients (52.5%) considered prenatal diagnosis, but some considered pre-symptomatic 5
diagnosis or non-progressive carrier diagnosis for their own risk assessment. For 20 clients (26.0%), a 6
genetic diagnosis had either recently been made on the proband or the proband showed a worsening 7
condition. In these cases, the purpose of the GC visit ranged from requests to explain the disease to 8
requests for further genetic testing. The motivation greatly depended on the relationship with the 9
proband and the amount of prior access to disease information. Many clients themselves and/or their 10
relatives went through a life event [such as considering their marriage (10 clients), became adults (two 11
clients), retirement (one client)] and thus they wanted to determine whether or they were in an “at-risk 12
state” before informing their relatives about their genetic condition. (Additional figure 2b). 13
Non-related clients 14
Receipt of an affected spouse’s genetic diagnosis (2 clients), impending pregnancy, desire to 15
bear a child (3 clients) and consideration of marriage (1 client) were all triggers to attend GC for un-16
related individuals. Here, some clients underwent GC without informing their partners of the visit. 17
(Additional figure 2c). 18
19

11
Case presentation by purpose 1
Explanation of the disease 2
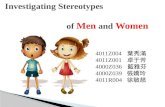
Case 1: 27year-old female (Figure 2A, III-2). 3
Purpose of GC: To understand more about DMD. 4
History prior to GC consultation: This client’s younger brother (III-4) was diagnosed with DMD at 5
3 years-of-age. His parents reported only the disease name to the client when she was a junior high 6
school student. The client’s older sister (III-1) was a carrier, but lived far away and had no opportunities 7
to talk with the client. The client recently learned that DMD was a hereditary disorder, and received a 8
positive carrier diagnosis at another facility. She visited our hospital with her husband (III-3) to gain a 9
detailed explanation of the disease. 10
Contents of the GC session: We provided the patient with an outline of the disease and how it is 11
inherited. We explained that there was a possibility that women might have mild symptoms, and that 12
recent developments for new therapies based on gene therapy were advancing. We also explained the 13
options for prenatal and pre-implantation diagnosis, and if she would like to have a baby, we would 14
schedule further GC with obstetricians. The client later requested a prenatal diagnosis and returned for 15
GC. 16
Prenatal diagnosis 17
Case 2: 19 year-old female (Figure 2B, IV-6). 18
Purpose of GC: To discuss the implications of a prenatal diagnosis of myotonic dystrophy (DM1). 19

12
History prior to GC consultation: The client was 17 weeks pregnant when she consulted the 1
department of clinical genetics. Her maternal aunt (III-3) and cousin (IV-1) were diagnosed with DM1, 2
but genetic testing was not conducted. The client knew that DM1 was hereditary, but she did not 3
understand the details and was worried about the implications for her unborn baby. The clinical 4
geneticist made the judgment that the client or her mother (III-6) had no evident symptoms indicative 5
of DM1. 6
Contents of the GC session: We explained that there was no possibility that the fetus would develop 7
the disease if the client or her mother were not carriers of DM1. However, we could not eliminate the 8
possibility that the client or her mother were DM1 carriers only from subjective symptoms as the 9
symptoms may not be noticeable when mild. We gave our opinion that it was necessary for her 10
maternal aunt to have a genetic diagnosis to warrant a prenatal diagnosis. The prenatal diagnosis 11
needed an application to be approved by the Institutional Review Board in our hospital, but it took 12
time to acquire. The client understood the situation and decided against a prenatal diagnosis. Because 13
there was a chance that the client had DM1 without overt symptoms, we decided to manage her 14
pregnancy at our hospital. We also referred the client’s mother to a neurologist to confirm whether she 15
had any clinical symptoms and thus should consider genetic testing. 16
Pre-symptomatic diagnosis 17
Case 3: 23 year-old female (Figure 2C, V-3). 18
Purpose of GC: Consultation about obtaining a pre-symptomatic diagnosis of spinocerebellar ataxia 19

13
6 (SCA6). 1
History prior to GC consultation: This client’s paternal grandfather (III-1) had a clinical diagnosis 2
of SCA6. A genetic diagnosis was made when her paternal aunt (IV-4) wanted a pre-symptomatic 3
diagnosis. After several GC sessions, genetic testing was conducted and revealed a positive result. The 4
patient’s father (IV-2) understood that it was possible that he was SCA6-positive and also requested a 5
pre-symptomatic diagnosis. Again, genetic testing was performed after several GC sessions, and the 6
result was positive. Her paternal aunt (IV-1) also underwent GC, but she did not tell her children that 7
the family had history of a hereditary disease, and pre-symptomatic diagnosis at that time was not 8
conducted. Knowing that her father was positive, the client considered the possibility that she may also 9
have inherited the condition. 10
Contents of the GC session: We confirmed the history of SCA6 and explained the impact of genetic 11
testing. The client described that she learned from her parents at a young age that her grandfather 's 12
illness was hereditary, and she assumed that she would also develop the disease. She was not worried 13
about the genetic influence on the next generation at this time because she had no current desire to 14
marry. If the result was positive, the client explained that she would consult with her employer about 15
her future work and if it was negative, she would undertake nursing care of her affected family 16
members, including her father. After several GC sessions, genetic testing was performed and the result 17
was negative. Her sister (V-4) also had GC, but she did not want a pre-symptomatic diagnosis. 18
Non-progressive carrier diagnosis 19

14
Case 4: 48 year-old female (Figure 2D, III-9) 1
Purpose of GC: Consultation about a non-progressive carrier diagnosis of Pelizaeus-Merzbacher 2
disease (PMD). 3
History prior to GC consultation: The client’s family included several sufferers of PMD, including 4
her maternal uncle and cousin. When the client’s daughter reached 20 years-of-age, she considered the 5
possibility that her daughter might marry and have children and thus underwent GC in the hope of 6
obtaining a carrier diagnosis by genetic testing. 7
Contents of the GC session: The client understood the outline of the disease as there were multiple 8
persons diagnosed as carriers in her family. She did not talk to her daughter about PMD in detail. We 9
advised her that if she was a carrier, that she consider the best timing of genetic testing and discussion 10
of the consequences of her diagnosis with her daughter. Her husband also agreed to take a carrier 11
diagnosis. Genetic testing was performed and the result was negative. 12
13
Discussion 14
This study is the first to comprehensively investigate the needs of GC in the context of 15
neuromuscular disease without limiting its purpose to only the requirement for the genetic test. 16
Previous reports from other countries have indicated that most neurologists have no training in genetic 17
diagnostics, but that education on clinical genetics is becoming more important as the complexity of 18
genetic testing is increasing17,18. Our clients had a variety of needs, identifying that neurologists need 19

15
to provide not only knowledge of the neuromuscular disease itself but also knowledge on the clinical 1
genetics and to refer the client to higher-order GC at an appropriate time. 2
As standard, we consider it necessary to confirm the amount of knowledge and concept of 3
each disease held by the client. For some neuromuscular diseases, disease modifying therapies are 4
available: we consider it important to provide up-to-date information about treatment options. 5
6
Overall client characteristics and GC purpose 7
Our analyses identified that the majority of clients attending GC were women (86.3%). This 8
gender bias may explain why pregnancy and desire to bear a child comprised most of the motivations 9
for GC sessions. Most clients were aged between 20 and 30 years (75.5%), which is consistent with 10
previous reports that the predominant age range of clients undergoing GC for a pre-symptomatic 11
diagnosis is between 20 to 39 years old15,19,20. This young age encompasses the time when most 12
individuals consider marriage and try for a child. Regardless of the precise purpose for visiting, we 13
found that many patients themselves or their relatives were motivated to attend GC due to a recent or 14
impending life event (see Case 4). 15
Many clients attended GC to gain a clear explanation of the genetic disease. Despite patients 16
or relatives themselves being affected by a particular disease, some clients were not aware of the 17
precise pathophysiology (see Case 1) and the clinical geneticists and/or CGCs needed to organize the 18
relevant information. DM1 was the most frequent disease that required explanation by the clinical 19

16
geneticists and/or CGCs, perhaps because the clinical symptoms of DM1 are diverse. Anticipation in 1
genetic disorders is the phenomenon where the signs and symptoms of a genetic condition become 2
more severe and present from an earlier age with each subsequent generation. With this in mind, we 3
considered that repeat expansion was extended to the next generation and different clinical symptoms 4
were exhibited due to genetic anticipation. Several neuromuscular diseases exhibited by the clients 5
showed genetic anticipation, suggesting that input from the neurological department, and other 6
relevant medical departments, would be beneficial to GC. 7
Those considering a prenatal, pre-symptomatic or carrier diagnosis had typically learned of 8
the presence of a hereditary disease in the family line. However, some clients were diagnosed as 9
symptomatic carriers without any family history and later considered a prenatal diagnosis (Additional 10
figure 1b). 11
12
GC for patients 13
Approximately 20% clients attending GC were patients, of which many wanted clarity on the 14
disease and to obtain a definitive diagnosis. A genetic diagnosis of relatives who are non-symptomatic 15
can only be performed when a pathogenic variant is observed in the proband. Some patients requested 16
a genetic diagnosis and attended GC (see Case 3: III-1) but some relatives wanted a genetic diagnosis 17
so that genetic testing of the proband was not enforced. 18
In the 2013 survey of neurologists in Japan, 43.2% neurologists were reluctant to make a 19

17
genetic diagnosis of DM1 and 30.4% were reluctant to make a genetic diagnosis of HD1. The reasons 1
for this opinion were because it is "possible to diagnose without genetic testing", "not linked with 2
effective prevention or therapy" and "difficult to support after disclosure of the results". Based on these 3
numbers, there will be a considerable number of patients with a clinically diagnosed neuromuscular 4
disease who have not been genetically diagnosed. When relatives desire a genetic diagnosis, the person 5
in charge of GC may create an opportunity to re-examine the genetic diagnosis in cooperation with the 6
physician of the proband. 7
Some of the diseases presented to our hospital that required a genetic diagnosis were rare; 8
here, it was hoped that the patient would consent to participate in research using whole-exome 9
sequencing (WES) and whole-genome sequencing (WGS) after GC. In Japan, a genetic diagnosis 10
following suspected clinical symptoms is usually made by Sanger sequencing technique. Many 11
neuromuscular diseases, however, exhibit genetic and phenotypic heterogeneity. As the demand for 12
comprehensive genetic testing is high, and as the costs and timing of next-generation sequencing 13
(NGS) are decreasing, it is expected that comprehensive genetic diagnoses made by NGS will 14
increase21. WES and WGS are required to interpret the results and respond to secondary findings, 15
making it difficult to conduct in general practice. We expect, therefore, that the number of cases of 16
neuromuscular disease requiring involvement from Clinical Genetics Departments from the confirmed 17
diagnosis stage will increase. 18
19

18
GC for relatives 1
Most relatives that underwent GC were first-degree relatives (74.0%), of which half were 2
parents. Many relatives had a first child with an inherited disease, and they wanted to discuss the 3
potential outcomes for a second baby when pregnant. Many relatives also wanted a prenatal diagnosis, 4
but a prenatal diagnosis that involved an invasive examination (such as chorionic villus sampling or 5
amniocentesis) was only granted when the requirements proposed by the Japan Society of Obstetrics 6
and Gynecology were met22. In cases where it is unclear whether one or both parties in a couple are 7
carriers of a genetic disease, a prenatal diagnosis cannot be granted; an Ethics Committee must judge 8
whether a case is serious or not. 9
Of the 26 (25.5%) relatives who wanted a prenatal diagnosis, 19 (73%) visited after pregnancy 10
was established. There were four cases (15.4%) where the examination could not be performed due to 11
time constraints (Case 2). Neurologists attending to patients with a hereditary disease must understand 12
the process of prenatal diagnosis, and relatives should be properly guided when they consider genetic 13
testing. 14
In cases where a child attended GC, it was typically motivated by wanting a pre-symptomatic 15
diagnosis. A study conducted in Japan in 2007 found that DM1 was the most frequent neuromuscular 16
disease for which a pre-symptomatic diagnosis was requested13; rather, we found that SCD was the 17
most frequent disease in our hospital. This discrepancy may be because three of those who wanted a 18
pre-symptomatic diagnosis of SCD were from the same family (see Case 3). As a result of one family 19

19
member’s pre-symptomatic diagnosis, other family members might consider simultaneous 1
examination, making it necessary to carefully proceed with GC while confirming the situation of each 2
family member. We found that many second-degree relative referrals considered a carrier diagnosis: 3
some clients underwent GC with little information on the disease because the proband had already 4
died. As required for patients, it was necessary to confirm the amount of knowledge held for each 5
disease. 6
One case at our hospital involved a proband who had just been genetically diagnosed and 7
another case where deterioration of the symptoms triggered a GC inquiry. A previous report described 8
the burden on caregivers and how the level of distress increases when symptoms deteriorate in the 9
proband23. We should, therefore, consider the possibility that changes to the proband’s symptoms 10
might trigger caregivers to consider themselves also at risk and seek GC. 11
12
GC for non-relatives 13
GC is available to address all genetic concerns and worries, and so clients unrelated to an 14
affected patient may also have concerns that warrant undergoing GC. In this study, non-relatives 15
accounted for 5.9% of clients. Unlike patients and relatives, non-relatives have only few chances to 16
consult with the department of clinical genetics. There are some topics that GC cannot solve, but 17
supporting autonomous decision-making by providing clear disease understanding and advice to help 18
address the current problem is a key role of GC. 19

20
1
Study limitations 2
Our hospital has pediatric and obstetric departments, and is a core medical facility in the area. 3
A high proportion of clients were motivated to undergo GC due to pregnancy and/or desire to bear a 4
child, but in Japan there are limited institutions where a prenatal diagnosis is possible and the 5
possibility that cases are gathered in one of only a few facilities should be taken into consideration. In 6
fact, a prenatal diagnosis was possible for 57.8% (59/102 diseases) of the diseases in our hospital. Thus, 7
our dataset may have a bias towards prenatal diagnoses. Finally, our hospital has been conducting SCD 8
genetic testing as part of a long-term Ethics Committee-approved study; thus, we must consider a 9
potential bias towards SCD cases in our dataset. 10
11
Future tasks 12
Most of the clients had knowledge of genetic risk and were seeking GC when a life event had 13
occurred and they experienced psychosocial changes. However, while some clients in a family chose 14
to undergo GC following a life event, some did not (Case 3). This effect may be due to the type of 15
event and level of understanding on genetic risk exhibited by each individual. A future study should 16
examine the method of GC intervention according to the client’s cognitive level. Ours is the first study 17
restricted to hereditary neuromuscular diseases, and the characteristics of these diseases may be 18
reflected in the background of the visit. Future studies should consider that the role of GC in 19

21
neuromuscular diseases will become clearer as GC is conducted in other areas, such as in the context 1
of cancers or cardiovascular diseases. 2
3
Conclusion 4
In summary, this study has examined the nature of GC required by patients with hereditary 5
neuromuscular diseases and their relatives/non-relatives. We found that many clients were motivated 6
to undergo GC in response to a life event. Practitioners should, therefore, be aware of events that affect 7
not only the patient but also their relatives, and guide GC at an appropriate time. Because of the diverse 8
requirements of each client, neurologists should be equipped with standard knowledge on clinical 9
genetics and neurological diseases. Depending on the client, the type and level of recognition of genetic 10
risk will differ, meaning that the clinical geneticists and/or CGCs should thoroughly understand the 11
present situation of the client and provide tailored treatment. 12
13
Acknowledgements 14
We thank all of the clients for their active cooperation. The manuscript has been carefully 15
reviewed by an experienced medical editor of NAI inc. whose first language is English. 16
17
Conflicts of interest 18
None 19

22
Supplementary information is available at Journal of Human Genetics’s website. 1
2
References 3
1. Yoshida K, Ohata T, Muto K, Tsuchiya A, Sawada J, Hazama T, et al. Survey on the attitude toward 4
genetic testing of neurologists certified by the Japanese Society of Neurology (in Japanese). Rinsho 5
Shinkeigaku. 2013; 53: 337–44. 6
2. Resta R, Biesecker BB, Bennett RL, Blum S, Hahn SE, Strecker MN, et al. A new definition 7
of genetic counseling: National Society of Genetic Counselors’ Task Force report. J 8
Genet Couns. 2006; 15: 77–83. 9
3. Saskia B, Thomas G. Genetic testing in neurological diseases. J Neuro. 2012; 259: 1249-54. 10
4. Enza MV, Alessandro F, Bruno D. Genetic testing for paediatric neurological disorders. Lancet 11
neurol. 2008; 7: 1113-26. 12
5. The Japanese Association of Medical Sciences. Guidelines for Genetic Tests and Diagnoses in 13
Medical Practice.2011; http://jams.med.or.jp/guideline/genetics-diagnosis_e.pdf 14
6. Quintáns B, Prieto MF, Carracedo A, Sobrido MJ. Genetic counselling in Neurology: A complex 15
problem that requires regulation. Neurologia. 2011; 26: 129–36. 16
7. Shibata Y, Yamada T, Kojima T, Kawaguchi S, Akaishi R, Yabe I. The characteristic of clients who 17
are considering prenatal diagnosis was changes by the introduction of NIPT (in Japanese). Jpn J 18
Genet Counsel. 2018; 39: 61–72. 19

23
8. The Japan Society of Human Genetics. Qualifications. http://jshg.jp/e/about/license/ 1
9. Japanese Society for Genetic Counseling. Members and Qualifications. 2
http://www.jsgc.jp/english.html#members 3
10. Japanese Board of Medical Genetics and Genomics, Clinical Genetics (in Japanese). 4
http://service.kktcs.co.jp/smms2/c/jbmg/ws/license/List_jbmg.htm?id=all&t=http://www.jbmg.jp/l5
ist/senmon.html 6
11. Japanese Board of Certified Genetic Counselor (in Japanese). 7
http://plaza.umin.ac.jp/~GC/About.html 8
12. The Japan’s National Liaison Council for Clinical Sections of Medical Genetics (in Japanese). 9
http://www.idenshiiryoubumon.org/list/index.html 10
13. Yoshida K, Wada T, Sakurai A, Wakui K, Ikeda S, Fukushima Y. Nationwide survey on predictive 11
genetic testing for late-onset, incurable neurological diseases in Japan. J Hum Genet. 2007; 52: 675–12
9. 13
14. Robins Wahlin TB. To know or not to know: a review of behavior and suicidal ideation in 14
preclinical Huntington’s disease. Patient Educ Couns. 2007; 65: 279–87. 15
15. Tanaka K, Sekijima Y, Yoshida K, Mizuuchi A, Yamashita H, Tamai K, et al. Current status of the 16
predictive genetic testing for hereditary neurological diseases in Shinshu University Hospital (in 17
Japanese). Rinsho Shinkeigaku. 2013; 53: 196–204. 18
16. Miskovic M, Lalic T, Radivojevic D, Cirkovic S, Ostojic S, Guc-Scekic M. Ten years of experience 19

24
in molecular prenatal diagnosis and carrier testing for spinal muscular atrophy among family from 1
Serbia. Int J Gynaecol Obstet. 2014; 124: 55–8. 2
17. Laura SM, Alex RP. Genetic Diagnostics for Neurologists. Continuum. 2018; 24: 18-36. 3
18. J. Dominguz, J. Lopez, A, Macaya, M. Bueno C, M.A. Garcia, D.Natera B. Genetic testing among 4
Spanish pediatric neurologists: Knowledge, attitudes and practices. Eur J Med Genet. 2017; 60: 124-5
29. 6
19. Mandich P, Lamp M, Gotta F, Gulli R, Iacometti A, Marchese R, et al. 1993-2004: two decades of 7
predictive testing for Huntington’s disease at the Medical Genetics Unit of University of Genoa. 8
Mol Genet Genomic Med. 2017; 5: 472–80. 9
20. Ibisler A, Ocklenburg S, Stemmler S, Arning L, Epplen JT, Saft C, et al. Prospective evaluation of 10
predictive DNA testing for Huntington’s disease in a large German center. J Genet Couns. 2017; 26: 11
1029–40. 12
21. Klein CJ, Foroud TM. Neurology individualized medicine: When to use next-generation 13
sequencing panels. Mayo Clin Proc. 2017; 92: 292–305. 14
22. Japan Society of Obstetrics and Gynecology Opinions concerning prenatal genetic testing and 15
diagnosis (in Japanese), 2013; http://www.jsog.or.jp/modules/statement/index.php?content_id=33 16
23. Raggi A, Tasca D, Panerai S, Neri W, Ferri R. The burden of distress and related coping processes 17
in family caregivers of patients with Alzheimer’s disease living in the community. J Neurol Sci. 18
2015; 358: 77–81. 19

25
Titles and legends to figures 1
Figure 1. The purpose of genetic counseling. 2
3
Figure 2. GC client family trees 4
Ages are shown under each symbol where available. 5
A. DMD cases. The proband is III-4. The client is III-2 who is accompanied by III-3. 6
B. DM1 cases. The proband is III-3. The client is IV-6 who is accompanied by III-6. 7
C. SCA6 cases. The proband is III-1. The client is V-3. 8
D. Pelizaeus-Merzbacher disease cases. The client is III-9. Document evaluation (*) was used for 9
someone who underwent genetic testing. 10
11
Tables 12
Table 1. Client Characteristics 13
14
Table 2. Eligible diseases included in this study. 15
DMD, Duchenne muscular dystrophy; SCD, spinocerebellar degeneration; MJD, Machado-Joseph 16
disease; SCA, spinocerebellar ataxia; DRPLA, dentatorubralpallidoluysian atrophy; DM1, myotonic 17
dystrophy; PMD, Pelizaeus-Merzbacher disease; FCMD, Fukuyama congenital muscular dystrophy; 18
BMD, Becker muscular dystrophy; XLH, X-linked hydrocephalus; SMA, spinal muscular atrophy; 19

26
MtD, mitochondrial Disease; MELAS, mitochondrial myopathy, encephalopathy, lactic acidosis, and 1
stroke-like episodes; MERRF, myoclonus epilepsy associated with ragged-red fibers; LHON, Leber’s 2
hereditary optic neuropathy; SBMA, spinal and bulbar muscular atrophy; HD, Huntington's disease; 3
ALS, amyotrophic lateral sclerosis 4
5
Supplementary information 6
Additional Figure 1. The breakdown of diseases. 7
a. For explanation of diseases (n=30) 8
b. For prenatal diagnosis (n=26) 9
c. For pre-symptomatic diagnosis (n=18) 10
d. For non-symptomatic carrier diagnosis (n=15) 11
*including two DMD symptomatic carriers. 12
13
Additional Figure 2. Motivation for GC. 14
a. For patients themselves (n=19) 15
b. For relatives (n=77) 16
c. For non-relatives (n=6) 17
18
19

Table1 Client Characteristics
Total (N=102)
N %
Gender
Male 13 12.7
Female 88 86.3
Unknown 1 1
Age
Under 19 2 2.0
20-29 31 30.4
30-39 46 45.1
40-49 7 6.9
50-59 5 4.9
60-69 5 4.9
Over 70 3 2.9
unknown 3 2.9
Relationship
Patient 19 18.6
Relatives 77 75.5
First-degree relatives 57 74.0
Parents 28 49.1
Child 17 29.8

Sibling 12 21.1
Second-degree relatives 14 18.2
Aunt/niece 12 85.7
grandmother/grandchildren 2 14.3
Third-degree relatives 3 3.9
cousin 3 100
Other relatives 3 3.9
Non-relatives 6 5.9
Partner 3 50
Partner’s family 3 50
Companion
yes 70 68.6
no 31 30.4
unknown 1 1.0

Table2 Eligible disease included in this study
Total (N=102)
N %
DMD 23 22.5
SCD 18 17.6
MJD/SCA3 5
SCA6 5
SCA1 1
SCA2 1
DRPLA 1
Unknown 5
DM1 14 13.7
PMD 7 6.9
FCMD 5 4.9
BMD 4 3.9
XLH 4 3.9
SMA 4 3.9
SMA1 3

SMA2 1
MtD 4 3.9
MELAS 2
MELAS & MERRF 1
LHON 1
SBMA 3 2.9
HD 3 2.9
ALS 2 2.0
Others 11 10.8




Top Related