



Languages
Pages
Legal


Right Coronary Artery Dissection
Caused by Catheter: a Case Report
Xiaozeng Wang Haiwei Liu
and Yaling Han
Department of Cardiology,
Shenyang Northern Hospital

64-year-old male ; ID : 2163956
Chest pain for 10 months,
worsen for two months ;
Hypertension for 15 years ,
No history of diabetes ;
ECG : no ST-T segment changes
Case presentation

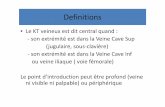
LCA 及 RCA 动脉粥样硬化改变, RCA 造影管与 RCA 近段成角,同轴差
Feb 26, 2009 SCA : Initial angiography demonstrating atherosclerosis changes in LCA and RCA. Angularity was viewed between the angiography catheter and the proximal RCA, without ideal co-axis.

RCA dissection formation from the proximal to the distal part of the vessel
Feb 26, 2009 SCA

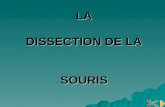
The National Heart, Lung and Blood Institute (NHLBI) Type A 血管腔内出现小的可透过区,对比剂通过即消失 dissections represent minor radiolucent areas within the coronary
lumen during contrast injection with little or no persistence of contrast after the dye has cleared.
Type B 血管腔内对比剂滞留,平行于管壁,几个周期后消失 dissections are parallel tracts or a double lumen separated by a
radiolucent area during contrast injection, with minimal or no persistence after dye clearance.
Type C 夹层突出于管壁外,对比剂通过后仍持续存在 dissections appear as contrast outside the coronary lumen
(“extraluminal cap”) with persistence of contrast after dye has cleared from the lumen.
Type D 螺旋型夹层,伴与不伴对比剂滞留 dissections represent spiral (“barber shop pole”) luminal filling
defects, frequently with excessive contrast staining of the dissected false lumen.
Type E 持续管壁充盈缺损,伴有远端血管对比剂滞留 dissections appear as new, persistent filling defects within the
coronary lumen. Type F 管腔充盈缺损,伴有管腔完全闭塞 dissections represent those
that lead to total occlusion of the coronary lumen without distal antegrade flow.

• NHLBI classification system for coronary artery dissection types.
• Types A and B are generally clinically benign,
• types C through F portend significant morbidity and mortality if untreated.


Strategy
Spiral dissection of the right coronary artery from the proximal to the distal part of the vessel, it is a NHLBI type D dissection, so select PCI with deployment stent
had no angina and hemodynamic instability, no need for IABP implantation and emergency CABG.

JR3.5, BMW 导丝, RCA 近段置入 Excel 4.0x18mm 支架
PCI for RCA JR3.5, BMW guide wire , Stent Excel 4.0x18mm was implanted
in the proximal part of the RCA

RCA 近中段再次置入 Excel 4.0x24mm 支架,与前一支架重叠 2mm
PCI for RCA The second stent Excel 4.0x24mm was implanted in the p-m RCA. Two
stents were overlapped with 2mm

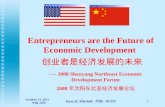
RCA 远段夹层处置入 Accrua 3.0x20mm 支架 ;RCA 远段可见血栓影像,单纯支架囊扩张消失
PCI for RCA Stent Accrua 3.0x20mm was implanted in the distal part of RCA; Thrombus
image was found in the distal part of the RCA, and disappeared with the stent balloon dilatation

RCA 中段置入 Accrua3.5x20mm 支架,与远段支架不相连,并支架内整形,最终造影结果满意。
Stent Accrua3.5x20mm was implanted in the m RCA. It was not linked with the distal stent. The final angiogram was excellent.

Final angiography at the end of the procedure
PCI for RCA

Follow-up Double oral anti-platelet therapy for eight months
(clopidogrel 75mg plus aspirin 100mg once daily)
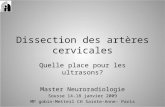
Follow-up Coronary Angiography (Oct 20, 2009) : No restenosis was found in RCA, TIMI grade 3 flow
Current oral medical therapy: aspirin 100 mg once
daily, antihypertensive medical and atorvastatin
There was absence of angina, and a normal ECG
was detected

Coronary AngiographyOct 20, 2009
No restenosis was found in RCA

Atherosclerosis changes in LCA
Coronary AngiographyOct 20, 2009

Lessons and comprehends
Catheter-induced coronary dissection
can be formed in “normal” look liked
coronary artery
Stent implantation should be from the
distal to the proximal of the dissection

Top Related