







Languages
Pages
Legal

PTA 120Pathophysiology
Week 7-Nervous System

Discuss anatomic structures and physiologic processes related to the neurological system.
Discuss physical effects of aging on the
body. Explain the difference between the gate
control and endogenous opiate theories of pain.
Objectives

Arnold-Chiari Malformation Autism Spectrum Disorder Cerebral Palsy Alzheimer’s Disease Amyotrophic Lateral Sclerosis Cerebral Vascular Accident
Pathological Conditions
Transient Ischemic Attack Creutzfeldt-Jacob Disease Dementia Epilepsy Guillain-Barré Syndrome Huntington’s Disease Multiple Sclerosis Drowning
Objectives
Peripheral Neuropathy Parkinson’s Disease Post-polio Syndrome Spinal Cord Injury Traumatic Brain Injury
Objectives

Pathology for the Physical Therapist Assistant, Ch. 7
Physical Therapy Clinical Handbook for PTAs
Textbooks

Copyright 2009 Walters Kluwer Health / Lippincott Williams & Wilkins
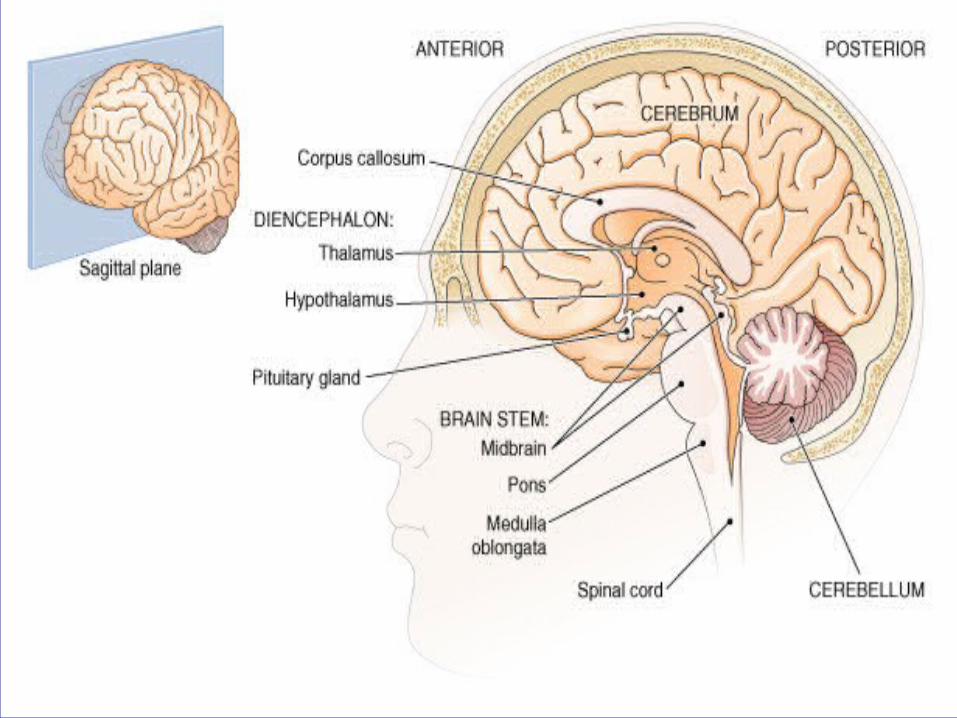
CNS develops from the neural tube that becomes the brain and spinal cord
The opening of the neural tube becomes the ventricles
Four chambers within the brain Filled with cerebrospinal fluid
CNS Development

Copyright 2009 Walters Kluwer Health / Lippincott Williams & Wilkins

Copyright 2009 Walters Kluwer Health / Lippincott Williams & Wilkins


Copyright 2009 Walters Kluwer Health / Lippincott Williams & Wilkins

Copryright 2009 Walters Kluwer Health / Lippincott Williams & Wilkins
Copyright 2009 Walters Kluwer Health / Lippincott Williams & Wilkins


Sensory input Gathers information about stimuli occurring
inside the body and outside in the environment. Integration
Processes and interprets sensory input and decides if action is needed.
Motor output Responds to integrated stimuli by activating
muscles or glands.
Functions of the Nervous System

From: Stillerman (Ed), Modalities for Massage and Bodywork, Elsevier, St Louis, 2008, in press.
Aging of the Nervous System
Physiologic Change Functional Effect
Nerve cell degeneration and decrease in cerebral blood flow (about 20% reduction between ages 50-80)
Reduced response time and decreased reflexes; loss or increased sensitivity to pain, which increases injury risk; decreased tolerance to heat or cold; decreased balance and coordination; altered gait
Decrease in neurotransmitters Increased potential for dementing processes

“An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” - Merskey, 1986
Perception is influenced by levels of attention, anxiety, arousal, suggestibility, fatigue, overall health, as well as influences from culture, religion, and past experiences.
Pain

Sensory Receptors Free Nerve Endings Nociceptors
Mechanoreceptors Thermoreceptors Chemoreceptors
Pain Pathway
A Delta Fibers/ 1st response Myelinated nerve fiber Quick response time Localized sharp sensation Short duration
C Fibers/2nd response Nonmyelinated nerve fiber Slow response time Non-localized dull sensation Longer duration
Pain Pathway

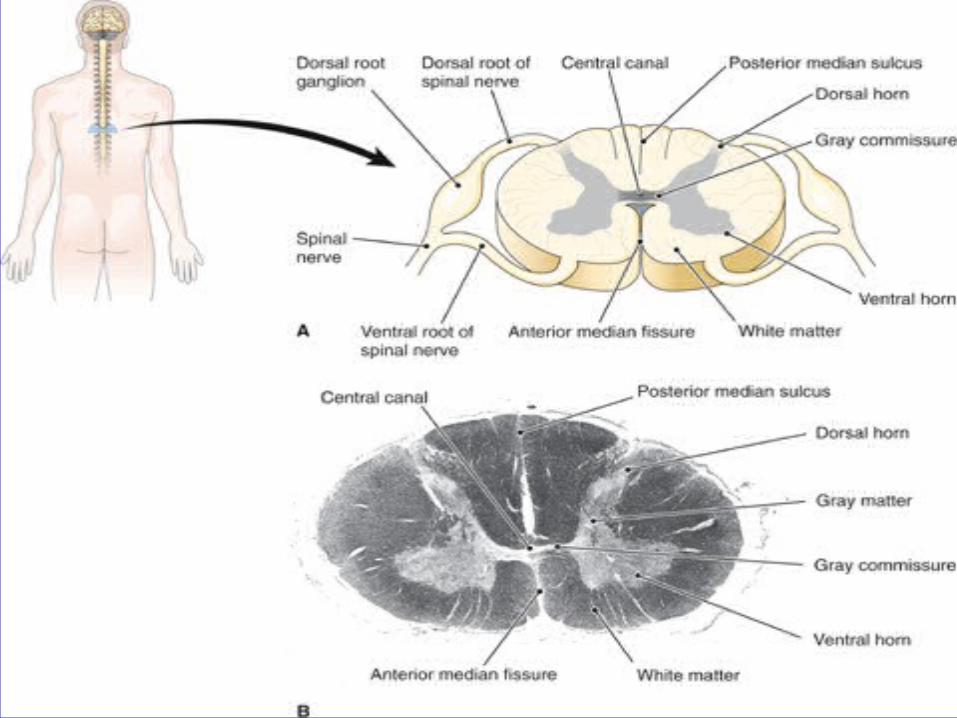
Sensory Receptor Dorsal Root Ganglion/Spinal Cord
Contains cell bodies of A and C fibers Synapse Site for A and C fibers A fibers enter spinal cord crossover and
connect to Spinothalamic tract C fibers synapse with interneurons in order to
connect to Spinothalamic tract Spinothalamic Tract
Ascending Pain Pathway

Brainstem (Autonomic Nervous System) Reticular Formation (arousal system) Influences changes in blood pressure, heart
rate and respiration Thalamus (relay station)
Receives and sorts sensory information sending them to particular areas of the cortex for interpretation
Cortex Interprets location, type of sensation, intensity and
amount of pain
Pain Pathway

1st Order Neuron A and C cell bodies in dorsal root ganglion
2nd Order Neuron A and C axons located in the dorsal horn of the
spinal cord Cross the midline in order to join the spinothalamic
tract 3rd Order Neuron
Located in parietal lobe of cortex Registers and interprets sensory information
Pain Pathway

Cortex Thalamus and Hypothalamus Midbrain/Medulla
Site in which the descending pathway synapses with ascending pathways
Spinal Cord 2nd Site in which the descending pathway
synapses with ascending pathways
Descending Pain Pathway

Function of Descending Pain Pathway Modulate the intensity of pain perception Inhibit the intensity of pain perception
Opiate nerve receptors Located in afferent nerve endings of 1st Order
Neurons and cell bodies in 2nd Order Neurons Block or inhibit pain transmission
Descending Pain Pathway

Inflammatory response Releases histamine, bradykinin, serotonin,
prostaglandins Edema -> pressure on nerves
Produces reaction in muscles -> spasm -> splinting mechanism to prevent movement
Pain production and response

Release of endogenous opiates - activities that stimulate the release and can produce analgesia, such as exercise, laughter, acupuncture, relaxation, electrical stimulation
Gate control theory – pain impulses must outnumber pain inhibiting factors for the “gate” to open to the brain; biofeedback used
Pain Control Theories

Visual Analog Scale (VAS) Visual Pain Drawing/Anatomical Pain Drawing Numeric Pain Rating Scale (NPRS) McGill Pain Questionnaire Dolorimeters/Pressure Algometers Facial Expressions Influence on daily living
Pain Assessments

Description Structural defect of the cerebellum and skull in
the developing fetus Blockage of CSF circulation in skull and spinal
cord Pressure on the spinal cord from cerebellum
through foramen magnum Three types, with Type I being the mildest and
Type III the most severe Can be accompanied by myelomeningocele
Arnold – Chiari Malformation

Etiology Unknown Genetic within families Chromosomes 9 and 15
Arnold – Chiari Malformation

Signs and Symptoms Dizziness Muscle weakness, paralysis Decreased sensation Headaches and vision deficits Decreased balance and coordination
Arnold – Chiari Malformation

Treatment No cure Surgical correction to restore CSF flow
Arnold – Chiari Malformation

Dependent upon level of severity Early childhood intervention to
address developmental delays and family education
Balance and coordination training
Physical Therapy Intervention for Arnold-Chiari Malformation

"Autism is a complex developmental disability that typically appears during the first three years of life and is the result of a neurological disorder that affects the normal functioning of the brain, impacting development in the areas of social interaction and communication skills.” – Autism Society of America
Autism Spectrum Disorder
Also known as ASD or PDD (Pervasive Developmental Disorder)
Encompasses a wide range of neurodevelopmental disorders (autism, Asperger syndrome, Rett syndrome, childhood disintegrative disorders, and pervasive developmental disorders (PDD-NOS)
Incidence is 1 in 150 children, as many as 1 in 94 boys; growing at a rate of 10-17 percent per year
Autism Spectrum Disorder

Etiology Not completely understood, with a
combination of both genetic and environmental factors
Environmental factors may possibly be heavy metals, viral infections, toxic chemical exposure
Abnormal serotonin levels
Autism Spectrum Disorder

Signs and Symptoms Little or no eye contact Physical and emotional distance from others;
failure to develop social attachments Insistence on sameness; resistance to change Difficulty in expressing needs; uses gestures or
pointing instead of words Repeating words or phrases in place of normal,
responsive language; echolalia
Autism Spectrum Disorder

Often self-stimulates; spins objects, flaps hands
Laughing, crying, showing distress for reasons not apparent to others
Inappropriate attachments to objects Uneven gross/fine motor skill level Can be non responsive to verbal cues May perform above average on memory or
spatial tasks 1/4 - 1/3 have IQ>70
Autism Spectrum Disorder

Autism Spectrum Disorder

Treatment Medications if necessary to reduce depression,
anxiety, obsessive-compulsive behavior, other behavioral issues, seizures
Family counseling Behavior therapy Team approach with neurologist, therapist,
psychiatrist, psychologist, teachers
Autism Spectrum Disorder

Address developmental delays Help child develop more normal
movement patterns Reeducation in motor planning Balance and coordination training
Physical Therapy Intervention for Autism Spectrum Disorder

Description Group of motor disorders caused by cerebral
damage during fetal life, birth or early childhood
Brain involvement is irreversible and not progressive
Symptoms vary from mild to extremely severe Difficulties with function as person grows
Cerebral Palsy

Classification By functional skills
The Gross Motor Function Classification System By muscle tone
Spastic / high tone Athetoid Ataxic Mixed
Cerebral Palsy
Etiology Damage to the cerebrum resulting from:
Inadequate blood flow (ischemia) Reduced oxygen supply (hypoxia or anoxia) Brain abnormalities Congenital genetic defects Hypoglycemia Traumatic brain injury Meningitis
Cerebral Palsy

Cerebral Palsy
Signs and Symptoms Related to motor
functions Lack of coordination,
exaggerated reflexes Contractures Drool excessively Difficulty swallowing
Complications can include seizures and mental retardation

Treatment Education on prevention during pregnancy Medications based upon characteristic of the
disease Surgery for tissue release, dorsal rhizotomy Intrathecal baclofen for hypertonicity Team approach including therapists,
physicians, and teachers is very important
Cerebral Palsy

Goal is to maximize independence and potential through strengthening. stretching, and mobility, with use of assistive devices if appropriate. Education of the family or caregivers is extremely important.
Physical Therapy Intervention for Cerebral Palsy

Description Progressive degenerative disease of the brain Destroys cerebral cortex neurons Leads to dementia 500,000 new cases diagnosed each year
Alzheimer’s Disease

Etiology Exact cause unknown Risk increased with advancing age, genetics,
atherosclerosis Plaques and amyloid accumulate in brain
tissue -> neurofibrils break down and become tangled -> nerve impulse transmission prevented -> function of sections on the cerebral cortex destroyed
Neurofibrillary tangles detectable at autopsy
Alzheimer’s Disease
Signs and Symptoms Loss of memory, inability to concentrate,
impairment of reasoning, apathy, personality changes
Warning signs: memory loss, problems with language, disorientation, difficulty completing familiar tasks, distorted judgment, problems with abstract thinking, misplacing things, mood, behavior, and personality changes
Alzheimer’s Disease

Treatment Prevention including healthy diet, higher
education Medications Stem cell research Massage Supportive environment, and long term care
Alzheimer’s Disease
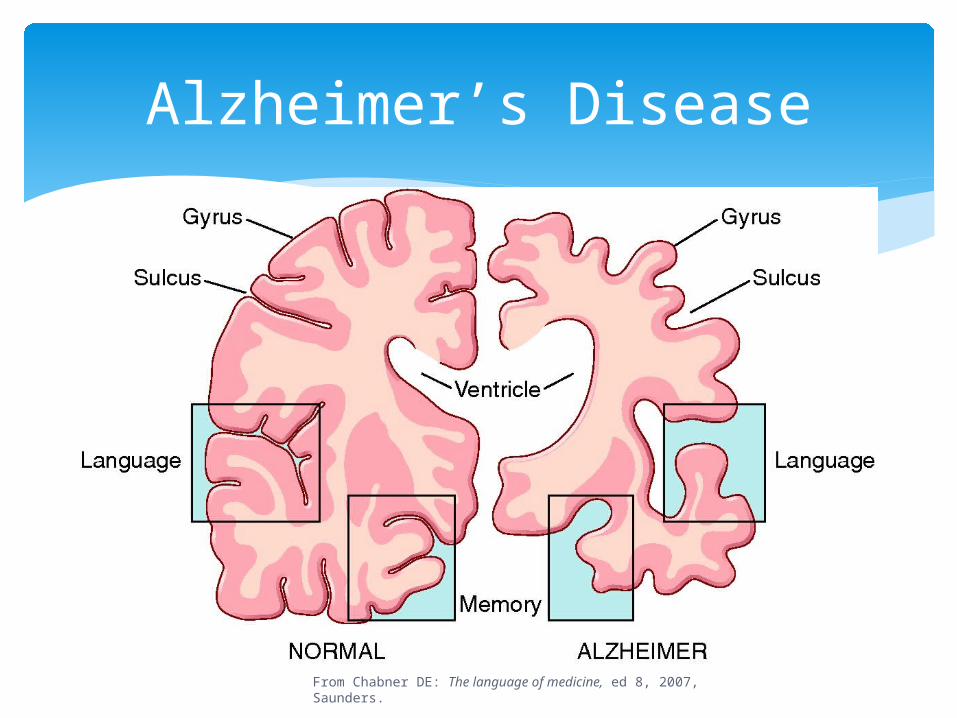
Alzheimer’s Disease
From Chabner DE: The language of medicine, ed 8, 2007, Saunders.

Alzheimer’s Disease
From Alzheimer’s Association

Goal is to maintain functional independence for as long as possible by encouraging activity, as the disease may lead to inactivity due to the cognitive restrictions. Strengthening, balance activities training, and modalities for pain relief are helpful. Due to the patient’s cognitive status, the therapist must use short, clear, and concise instructions.
Physical Therapy Intervention for Alzheimer’s Disease

Description Also called Lou Gehrig’s Disease or ALS Degeneration and demyelination of motor
neurons Leads to general paralysis and immobility;
progresses rapidly, with death usually in 3 - 10 years
Intelligence and sensations not affected Mainly occurs between 40 and 60 years of age,
with men > women; 1 case per 100,000
Amyotrophic Lateral Sclerosis

Amyotrophic Lateral Sclerosis
Etiology Cause unknown; genetics involved in 5 – 10 %
of cases Genetics 5 - 10% Possibly viral, metal or mineral exposure,
autoimmune disease High glutamate concentration in CSF causes
destruction of neurons
Amyotrophic Lateral Sclerosis
Signs and Symptoms Begins with weakness and atrophy of hands,
forearms, legs and eventually spreading to rest of the body
Severe fatigue Paralysis Difficulty with speech, chewing, swallowing,
breathing
Amyotrophic Lateral Sclerosis

Treatment Medications to control muscle spasms Assistance with breathing including
intermittent positive pressure ventilation (IPPV) or tracheostomy
Gene therapy possibly leading to development of medication to treat and delay symptoms
Speech therapy to assist with feeding
Amyotrophic Lateral Sclerosis
Goal is to maintain independence and functional independence for as long as possible
Work on functional mobility, including wheelchair evaluation and training if needed
Home modifications and assistive devices Strengthening and stretching Low-impact aerobic exercise Breathing exercises, postural drainage, chest PT
Physical Therapy Intervention for Amyotrophic Lateral Sclerosis

Description Also called CVA, a stroke, or a “brain attack” Sudden disruption in cerebral blood flow, with
death of brain tissue leading to irreversible brain damage
Symptoms last more than 24 hours Men > women Leading cause of disability and 3rd leading
cause of death in the US
Cerebrovascular Accident

Etiology Smoking is a leading cause Hemorrhagic CVA
Aneurysm ruptures -> blood seeps into surrounding tissue and creates pressure -> symptoms dependent upon which area of the brain is affected
Ischemic CVA Atherosclerosis leads to an embolus (blood clot) ->
clot travels and blocks a smaller blood vessel in the brain -> lack of oxygen leads to brain tissue necrosis
Cerebrovascular Accident

Signs and Symptoms Reflect portions of brain affected Severe headache, seizure activity, personality
changes Visual disturbances, unequal pupils Speech difficulty, difficulty understanding
others Sudden weakness; unilateral paralysis and
neglect Numbness, tingling, or burning Coma, loss of consciousness, death
Cerebrovascular Accident

Cerebrovascular Accident

Treatment Immediate medical attention, within 90
minutes after onset of symptoms Anticoagulants for ischemic type Control of hypertension and brain bleeds for
hemorrhagic type Reduce hypertension and blood cholesterol,
anticoagulants or antiplatelet treatment
Cerebrovascular Accident
Long-term medical treatment Quit smoking, reduce alcohol consumption Decrease weight Medications including low-dose daily aspirin, flu
and pneumonia vaccines Surgery
Cerebrovascular Accident

Description Brief episode of impaired brain functioning due
to a temporary reduction of blood flow Individual remains conscious Complete recovery in 24 hours with no residual
dysfunction; > 24 hours is a CVA Can indicate development of CVA or stroke Etiology, signs and symptoms, and treatment
are the same as those of a CVA
Transient Ischemic Attack

May begin in ICU if indicated for bed mobility and range of motion, progressing to strengthening exercises and ambulation as tolerated.
Training on how to use the affected and neglected extremities.
Gait training and adaptive equipment as necessary.
Follow precautions very closely – ch. 7, pg 313
Physical Therapy Intervention for Cerebrovascular Accident

Description CJD, one form is “Mad Cow Disease” Group of degenerative disorders Sporadic, hereditary, acquired, variant Fatal Onset after 60 years of age Between 200 – 300 cases in U.S. annually 85% of affected have the sporadic form
Creutzfeld-jacob disease

Etiology Sporadic form
Unknown cause, or direct contact with infected transplant organs and grafts
Hereditary form Autosomal gene Spontaneous mutation of the PRNP gene (makes
proteins that transports copper and protects neurons) Prion protein builds up -> neurons destroyed ->
extensive brain damage
Creutzfeld-jacob disease

Signs and Symptoms Dementia – rapid and progressive Severe mental impairments – personality
changes, judgment deficits Depression, insomnia Motor deficits – decreased coordination,
weakness, myoclonus, speech deficits, immobility
Blindness and coma at end stage
Creutzfeld-jacob disease

Treatment Alleviate symptoms Medications to reduce pain and myoclonus
Creutzfeld-jacob disease

Maintain mobility as long as possible with strengthening exercises and assistive devices as necessary
Treat within patient’s tolerance
Physical Therapy Intervention for Creutzfeld-Jacob Disease

Description Types include: Lewy body, senile, vascular, and
dementias precipitated by other diseases Progressive brain deterioration Decline of mental facilities (thinking,
remembering, communicating) Affect a wide age range
Dementia (Non-Alzheimer’s)

Etiology Buildup of Lewy body proteins which decreases
dopamine and acetylcholine Vascular disease resulting in ischemia Toxic substances, certain medications,
exposure to heavy metals Smoking and exposure to secondhand smoke Advancing age
Dementia (Non-Alzheimer’s)

Signs and Symptoms Begins with forgetfulness then loss of memory Personality disintegration, disorientation,
general loss of cognitive abilities Parkinson-like motor deficits Depression, aimless wandering
Treatment Dependent upon causative factors Medications and reminiscence therapy
Dementia (Non-Alzheimer’s)
Treatment is aimed at the neurological and musculoskeletal manifestations, and must be adjusted due to the patient’s cognitive status by using short instructions and a familiar location.
Work on stretching, strengthening, endurance, balance and coordination, as well as ambulation may be indicated.
Physical Therapy Intervention for Dementia

Description Epilepsy and epileptic syndromes Explosive episodes of uncontrolled and
excessive electrical activity in the brain which results in multiple involuntary muscle contractions
Diagnosis of epilepsy requires 2 seizures occur without a known cause
Seizure Disorders

Etiology Abnormalities within the neurons or with the
balance of the neurotransmitters, which cause the neurons to be triggered all at one time
Unknown, possibly genetic factors involved Head trauma or brain tumors Infections, high fevers
Seizure Disorders

Cerebrovascular disturbances Chemical imbalances Drug or alcohol withdrawal Stress
Seizure Disorders

Signs and Symptoms Uncontrolled muscular contractions; convulsions Absence seizures – “petit mal”, with brief loss of
consciousness, staring Atonic – temporary loss of muscle tone, collapses Myoclonic / myotonic – jerking and twitching Simple partial – emotion and sensation changes Complex partial – altered level of consciousness,
staring, twitching
Seizure Disorders

Treatment Prescribed medications acting on
neurotransmitters Vagal nerve stimulation Surgery to remove the affected area of brain Ketogenic diet, gene therapy, stem cell
research
Seizure Disorders
Treatment is aimed at the injuries or conditions resulting from the seizure, such as fractures or developmental delays. Treatment may include work on mobility, stretching, strengthening and balance.
It is important to be aware of seizure precautions if a patient has had a prior neurological injury.
Physical Therapy Intervention for Seizure Disorders

Description Rapidly progressing inflammatory disease in
which the immune system affects the neural tissue
1-2 people per 100,000 affected worldwide Etiology
Unknown Related to autoimmune response preceding
viral infection or immunization
Guillain-Barré Syndrome

Guillain-Barré Syndrome
Signs & Symptoms Numbness or tingling in feet and hands Followed by progressive muscle weakness
beginning in legs and traveling up the trunk, down the arms to the face, usually bilaterally, with possible complete paralysis
Vision, speech, and breathing may be impaired Absent deep tendon reflexes High level of proteins in the cerebrospinal fluid
Guillain-Barré Syndrome
Treatment No known cure Plasmapheresis to reduce the autoimmune
response and remove toxins Intravenous immunoglobulin to restore
immune defenses Manage symptoms of dehydration and skin
breakdown Psychological support for patient and family
Guillain-Barré Syndrome
Treatment follows the pace of peripheral nerve recovery, and usually begins with patient and family education in range of motion exercises to prevent contractures, progressing through wheelchair training or ambulation with assistive devices, strengthening, and balance and coordination activities. It is important not to overfatigue a patient.
Physical Therapy Intervention for Guillain-Barré Syndrome

Description Autosomal dominant degenerative disorder Caused by mutation of the gene which
produces huntingtin protein Motor disturbances, mental deterioration,
abnormal behavior Slow progression from 10 - 30 years before
death, symptoms appear in the 30s and 40s 1 in 20,000 in U.S. affected
Huntington’s Disease
Huntington’s Disease
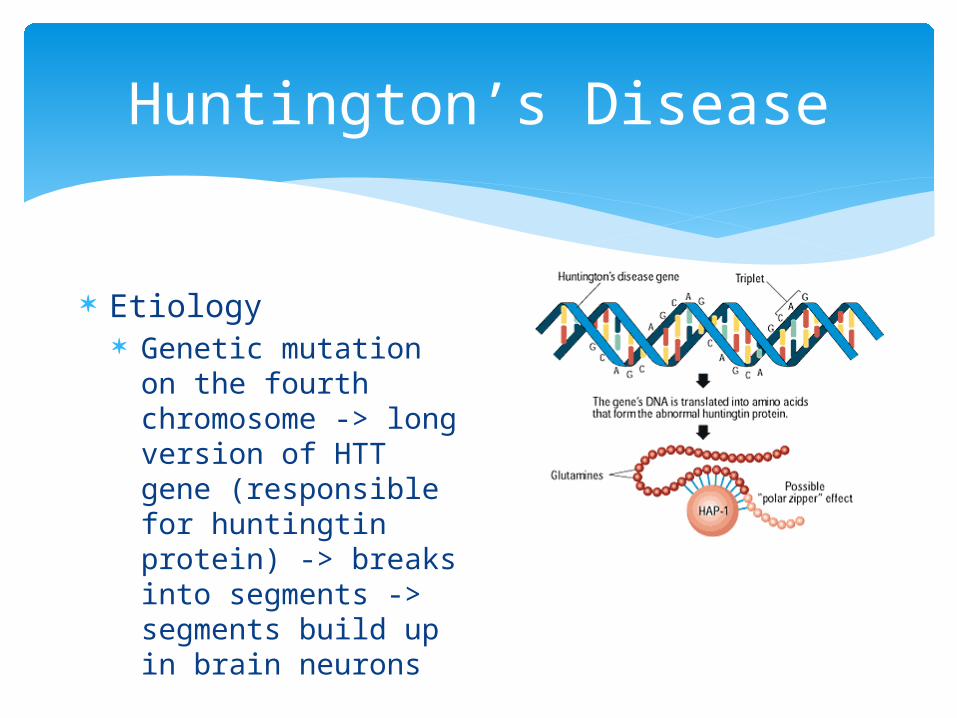
Etiology Genetic mutation on
the fourth chromosome -> long version of HTT gene (responsible for huntingtin protein) -> breaks into segments -> segments build up in brain neurons

Signs and Symptoms Chorea - involuntary, purposeless, rapid or
jerky motions of the arms and face Dystonia – increased muscle tone, involuntary
movements with rotation Myoclonus – involuntary twitching and spasm Movement tics – brief muscular spasms on the
face Parkinson – like movements – rigidity and
tremors
Huntington’s Disease
Speech and swallowing difficulties Mental and emotional deterioration and
dementia
http://www.youtube.com/watch?v=kINXIjs_V3M&feature=related
Huntington’s Disease

Treatment No successful medications to cure or prevent,
so aimed at controlling both motor and psychiatric symptoms
Botulism toxin injections, deep brain stimulation, stem cell transplants
Psychological support Speech therapy for feeding and
communication Occupational therapy for activities of daily
living
Huntington’s Disease

Treatment focuses on maintaining independence for as long as possible through strength, flexibility, and endurance training; progressing through wheelchair training or ambulation with assistive devices, as well as education regarding fall prevention and energy conservation techniques for both the patient and the family.
Physical Therapy Intervention for Huntington’s Disease
Description Autoimmune disorder. chronic Progressive demyelination of neurons of the brain,
spinal cord, cranial nerves Periods of remissions and exacerbations Women > men (at least 2:1); onset between teens - 50
years old Both relapsing-remitting (most common) and primary
progressive Exacerbations related to stress, heat, fatigue,
infections
Multiple Sclerosis (MS)
Etiology Genetic defect reducing the ability of T-cells to
turn off the immune response -> autoimmune attack on the myelin -> scar tissue causes plaques which build up in spinal cord and brain -> disruption of brain function and neural transmission
Higher prevalence in countries further from the equator; viruses and concentration of sex hormones may trigger the disease
Multiple Sclerosis (MS)

Multiple Sclerosis (MS)

Signs and Symptoms Demyelination causes the primary symptoms
Paresthesias, vision disturbances, progressive muscle weakness, cognitive impairments, and bladder and bowel dysfunctions
Secondary symptoms result from primary symptoms
Tertiary symptoms include social and psychological functioning
Multiple Sclerosis (MS)

Treatment Team approach including physicians,
psychologists, social workers, physical therapists, occupational therapists, speech therapists, and family
Medications to reduce the development of new brain lesions and slow down disease progression
Multiple Sclerosis (MS)

Treatment focuses on maintaining mobility and the quality of life, as well as reducing fatigue through strengthening (including resistance training if fatigue can be avoided), stretching, aerobic exercise, and education regarding fall prevention and energy conservation techniques. Standardized tests are frequently used to monitor progress.
Physical Therapy Intervention for Multiple Sclerosis

Description Primary respiratory impairment from
submersion in a liquid “Near-drowning” term discontinued Fifth leading cause of death in U.S. > 8000 deaths annually; 1500 are children For every 1 death = 4 hospitalized, 14 in ER
Drowning

Etiology Adults
Water sports Diving Alcohol consumption Other diseases / disorders Men > women; ages 15 – 24
Drowning

Children Swimming pools Bathtubs; girls > boys; under age 4 35% fatal; 33% some neurological impairment;
11% severe impairment
Factors affecting recovery Amount of time in the water Water temperature; cold water = damage may
be slowed down
Drowning

Signs and Symptoms Immediate
Altered vital signs, hypothermia Tachycardia, bradycardia Anxiety, dyspnea, tachypnea Hypoxia Metabolic acidosis Altered level of consciousness Cardiopulmonary arrest
Drowning

Long term results Effects range from none to severe Anoxia of the brain, extensive brain damage Pulmonary damage from aspiration; ARDS Pulmonary edema, pneumonia
Can result in death Seizures, coma, changes in mental status
Drowning

Treatment PREVENTION!
Fenced areas, supervision, groups vs. alone, no alcohol, childproofing
Rescue attempt; rescue breathing; neck in neutral
Activate EMS; hospital Long-term rehabilitation Speech therapy or occupational therapy involved
for swallowing and feeding disorders
Drowning

Treatment focuses on neurological rehabilitation, including NDT, functional movement, positioning to prevent pressure ulcers and assist with breathing.
Physical Therapy Intervention for Drowning

Description Disease of the peripheral nerves Affects motor, sensory, autonomic systems > 20 million affected; more common in older
adults
Peripheral Neuropathy

Etiology Unknown; inherited Diabetes mellitus, Guillain-Barre Alcoholism Autoimmune diseases Kidney failure, thyroid dysfunction, cancer Environmental toxins; Infections Long-term medications Vitamin B deficiency, malnutrition
Peripheral Neuropathy
Signs and Symptoms Sudden or gradual, > in distal lower
extremities Mild to severe and debilitating Pain during regeneration of nerves Weakness and atrophy, fasciculations,
cramping Altered sensation: “Glove” distribution,
vibratory, touch, pressure, temperature, numbness, kinesthetic
Peripheral Neuropathy
Decreased balance, coordination, mobility Decreased weight bearing -> bone
degeneration Hypotension -> dizziness, poor balance Facial muscle weakness -> swallowing, eating
difficulties Bowel / intestinal symptoms Can result in skin breakdown, amputation
Peripheral Neuropathy

Treatment Team approach Treat underlying cause Lifestyle changes Medications to decrease pain Orthopedic shoes
Peripheral Neuropathy

Treatment begins with PT evaluation of muscle strength, skin sensation. The treatment plan may include orthotics, wound care, prevention of contractures, gait training, balance training, strengthening, endurance, and patient education.
Physical Therapy Intervention for Peripheral Neuropathy

Description Progressive, degenerative neurologic disorder Produces syndrome of abnormal movements Basal ganglia undergo degenerative changes▪ Dopamine▪ Regulates voluntary movements, emotions,
mood, motivation
Parkinson’s Disease

Etiology Primary ▪ Idiopathic origins
Secondary ▪ Traced to another cause or pathologic event▪ Infection▪ Trauma▪ Tumors▪ Atherosclerosis▪ Drug use
Parkinson’s Disease

Signs and Symptoms Tremors – “pill-rolling” Cogwheel rigidity Slowness of voluntary movements Postural abnormalities Dystonia Propulsive gait Decreased balance
Parkinson’s Disease
Masklike appearance of the face Muffled speech Difficulty with chewing and swallowing
http://www.youtube.com/watch?v=_L_WF6gv5BI&playnext=1&list=PL10AF05605106C2D6
Parkinson’s Disease

Treatment Incurable Prescribed medications to slow the
development of dopamine, or anticholinergic medications
Surgery Deep brain stimulation, stem cell implantation Speech therapy for speaking and swallowing Occupational therapy for activities of daily
living
Parkinson’s Disease

Treatment focuses on addressing the patient’s functional problems and pain relief. Range of motion exercises, strengthening, balance training, gait training, and instruction in use of assisted devices are all used to maximize the patient’s mobility.
Physical Therapy Intervention for Parkinson’s Disease

Description Seen in some patients who have had
poliomyelitis earlier in life Appears an estimate of 35 years after infection Exhibited in 28.5 to 64% of previous polio
patients Increased occurrence due to polio epidemic in
1940s and 1950s
Post-polio syndrome

Etiology Actual cause is unknown Motor neurons not affected in the original
infection -> overused -> overworked and stressed -> neuron death -> autoimmune response to neuron death
Post-polio syndrome

Signs and Symptoms Develop slowly Weakness and decreased muscular endurance,
“post-polio progressive muscular atrophy” Fatigue, loss of energy, myalgia Decreased concentration, mental exhaustion Respiratory, speech, and swallowing problems Joint problems, inflammation; leads to
decreased mobility and function
Post-polio syndrome

Treatment No cure Medications not effective Manage physical effects of weakness through
lifestyle changes
Post-polio syndrome
Energy conservation techniques including rest and use of a wheelchair
Low-impact aerobic program Strengthening program without
fatiguing
Physical Therapy Intervention for Post-polio Syndrome

Description Damage to the vertebrae, neural tissue Loss of movement and sensation distal to
injury site Quadriplegia or paraplegia Men > women 4:1; ages 15 - 25 12,000 new cases each year in the U.S.
Spinal Cord Injury

Etiology Primary injury from trauma, including motor
vehicle accidents, sports, falls, and violence Possible fracture or dislocation -> damage to
spinal cord and blood vessels -> damage to neuronal and glial cells
Secondary effects include ischemia, inflammation, delayed cell death, production of free radicals -> more damage to neural and glial cells -> scarring
Spinal Cord Injury

Spinal Cord Injury
Signs and Symptoms Immediate phase
Lasts up to 2 hours after the injury Spinal shock, with no movement, sensations, or
reflexes below the level of the injury Edema in the spinal cord -> hemorrhage and
death of gray and white matter cells -> ischemia of spinal cord
Spinal Cord Injury

Acute phase From 2 – 48 hours after injury Hemorrhage continues -> increased inflammation and
edema -> free radical production -> damaged tissue -> immune system response -> neural and glial cell damage
Sub acute phase From 2 days – 2 weeks after injury Phagocytes clean-up debris and destroy myelin ->
scarring -> barrier for axon regeneration
Spinal Cord Injury
Intermediate phase From 2 weeks – 6 months after injury Scarring matures -> axon regeneration
Chronic phase From 6 months – the end of lifetime At 1-2 years, symptoms and deficits occurs Bone density loss, pressure ulcers, depression,
suicidal thoughts, hostility, substance abuse
Spinal Cord Injury

Treatment Immediate
Immobilization and decompression of spinal cord Position changes, wound care Medications and light therapy to decrease
inflammation, stem cell research Surgery
Once injury healed Rehabilitation to maximize independence, prevent
complications
Spinal Cord Injury

Treatment focuses not only compensatory movements, but also on recovery. Strategies include functional electrical stimulation and passive range of motion, progressing to more active strengthening and balance training. Treatment also includes transfer training, wheelchair training, and gait training as necessary.
Physical Therapy Intervention for Spinal Cord Injuries

Description Also known as a head injury, with external
forces affecting brain function Impairment of cognition and physical function
which can be temporary or permanent Men > women 2:1; ages 15 – 24 5.3 million in US have long-term effects 1.4 million seen in the emergency room yearly
Traumatic Brain Injury (TBI)

Etiology Trauma from falls, motor vehicle accidents, direct
blows, as with sports Open injuries - meninges are breached and the
brain is exposed Closed head injuries
Epidural or subdural hematoma occurs -> blood creates pressure on brain tissue -> ischemia of brain tissue
Edema of brain tissue -> diffuse pressure on brain -> increased intracranial pressure
Traumatic Brain Injury (TBI)

Traumatic Brain Injury (TBI)
Coup – contrecoup injury The brain hits one part
of the brain as well as the directly opposing part of the brain
Creates a shearing effect

Signs and Symptoms Mild to severe range Loss of consciousness, seizures, coma, death Headaches, dizziness, nausea and vomiting Altered cognition, changes in personality or
emotions, retrograde or posttraumatic amnesia, post-traumatic stress disorder
Glasgow Coma Scale
Traumatic Brain Injury (TBI)

Treatment Maintaining oxygen levels in the brain, blood
pressure control Surgery to remove particles Medications for long-term effects such as
spasticity and other complications
Traumatic Brain Injury (TBI)

Treatment will begin in the ICU and continue throughout the patient’s life if necessary. Strategies include passive range of motion, progressing to more active strengthening with transfer training, wheelchair training, and gait training as necessary. It is very important to be aware of the patient’s cognitive deficits in order to communicate with and teach the patient appropriately.
Physical Therapy Intervention for Traumatic Brain Injuries
Top Related