






Languages
Pages
Legal


Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
A Practical Guide for Hysteroscopy
in the Offi ce (Didactic)
PROGRAM CHAIR
Amy L. Garcia, MD
PROGRAM CO-CHAIR
Isabel C. Green, MD
Andrew I. Brill, MD Micah Harris, MD Eileen C. Young, RN

Professional Education Information Target Audience Educational activities are developed to meet the needs of surgical gynecologists in practice and in training, as well as, other allied healthcare professionals in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.
Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 3 Getting Started with Hysteroscopic Procedures in Your Office: Patient Safety, Regulation and Financial Considerations M. Harris ....................................................................................................................................................... 5 Local Anesthesia, Oral and Injectable Medication for Office Procedures I.C. Green .................................................................................................................................................... 15 Diagnostic Hysteroscopy: Evaluation of the Uterine Cavity and Preoperative Decision Making A.L. Garcia .................................................................................................................................................. 20 Office Operative Hysteroscopic Procedures: Directed Biopsy, Polypectomy, Metroplasty and IUD Retrieval A.L. Garcia .................................................................................................................................................. 27 Hysteroscopic Sterilization: The Essure Procedure in the Office I.C. Green .................................................................................................................................................... 31 Hysteroscopic Morcellators: What’s on the Horizon for Hysteroscopic Polypectomy and Myomectomy in the Office? A.I. Brill ....................................................................................................................................................... 37 Identifying and Managing Hysteroscopic Complications in the Office M. Harris ..................................................................................................................................................... 46 Equipment Maintenance: The Rigid and Flexible Hysteroscope E.C. Young .................................................................................................................................................. 52 Cultural and Linguistics Competency ......................................................................................................... 55

PG 208 A Practical Guide for Hysteroscopy in the Office (Didactic)
Amy L. Garcia, Chair
Isabel C. Green, Co-Chair
Faculty: Andrew I. Brill, Micah Harris, Eileen C. Young
Course Description This course provides the practical guidance necessary to perform hysteroscopic procedures safely and efficiently in the office setting. Designed for the gynecologist who wants to overcome common barriers, this course offers essential instruction, tools and information needed to begin or enhance a comprehensive in-office hysteroscopy practice. The course addresses billing and coding issues including RVU with CPT codes for hysteroscopic procedures and use of modifiers for reimbursement. Patient counseling, informed consent and documentation of procedures. Patient safety and regulatory guidelines, procedure checklists and personnel requirements guide the participant. Equipment acquisition, set-up and maintenance for both rigid and flexible hysteroscopes are presented. Office use of local anesthesia and oral medication for hysteroscopic procedures is examined in detail. Video based didactics address specific office operative hysteroscopic procedures in depth including tips, tricks and troubleshooting techniques as well as identification and management of office hysteroscopic complications.
Course Objectives At the conclusion of this course, the participant will be able to: 1) Implement patient safety regulations and safety protocols for in-office procedures; 2) use correct coding and billing to maximize reimbursement for office hysteroscopic procedures; 3) appropriately counsel patients regarding in-office hysteroscopic procedures, obtain informed consent and document procedures correctly; 4) acquire, set-up and maintain equipment and supplies needed for office hysteroscopic procedures; 5) use cervical anesthesia, oral and injectable medication effectively for patient comfort with office hysteroscopic procedures; 6) utilize hysteroscopy for in office procedures such as biopsy, polypectomy, myomectomy, metroplasty, sterilization and IUD removal; 7) discern new technologies for hysteroscopic morcellation of polyps and myomas in the office; and 8) identify and address common complications encountered with office hysteroscopic procedures.
Course Outline
8:00 Welcome, Introductions and Course Overview A.L. Garcia 8:05 Getting Started with Hysteroscopic Procedures in Your Office: Patient Safety,
Regulation and Financial Considerations M. Harris
8:30 Local Anesthesia, Oral and Injectable Medication for Office Procedures I.C. Green
8:55 Diagnostic Hysteroscopy: Evaluation of the Uterine Cavity and
Preoperative Decision Making A.L. Garcia
1

9:20 Office Operative Hysteroscopic Procedures: Directed Biopsy, Polypectomy,
Metroplasty and IUD Retrieval A.L. Garcia
9:45 Questions & Answers All Faculty 9:55 Break 10:10 Hysteroscopic Sterilization: The Essure Procedure in the Office I.C. Green
10:35 Hysteroscopic Morcellators: What’s on the Horizon for Hysteroscopic Polypectomy
and Myomectomy in the Office? A.I. Brill
11:00 Identifying and Managing Hysteroscopic Complications in the Office M. Harris
11:25 Equipment Maintenance: The Rigid and Flexible Hysteroscope E.C. Young
11:50 Questions & Answers All Faculty 12:00 Course Evaluation
2

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor Consultant: Conceptus Incorporated Frank D. Loffer, Executive Vice President/Medical Director, AAGL* Linda Michels, Executive Director, AAGL* Jonathan Solnik Other: Lecturer - Olympus, Lecturer - Karl Storz Endoscopy-America SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: CooperSurgical, Ethicon Women's Health & Urology, Intuitve Surgical Other: Royalties - CooperSurgical Linda Bradley Grants/Research Support: Elsevier Consultant: Bayer Healthcare Corp., Conceptus Incorporated, Ferring Pharmaceuticals Speaker's Bureau: Bayer Healthcare Corp., Conceptus Incorporated, Ferring Pharm Keith Isaacson Consultant: Karl Storz Endoscopy Rosanne M. Kho Other: Honorarium - Ethicon Endo-Surgery C.Y. Liu* Javier Magrina* Ceana H. Nezhat Consultant: Intuitve Surgical, Lumenis, Karl Storz Endoscopy-America Speaker's Bureau: Conceptus Incorporated, Ethicon Women's Health & Urology William H. Parker Grants/Research Support: Ethicon Women's Health & Urology Consultant: Ethicon Women's Health & Urology Craig J. Sobolewski Consultant: Covidien, CareFusion, TransEnterix Stock Shareholder: TransEnterix Speaker's Bureau: Covidien, Abbott Laboratories Other: Proctor - Intuitve Surgical FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Amy L. Garcia Grants/Research Support: Hologic Consultant: Conceptus Incorporated, Ethicon Endo-Surgery, Ethicon Women's Health & Urology, IOGYN, Minerva Surgical Speaker's Bureau: Conceptus Inc. Isabel C. Green*
3

Andrew I. Brill Consultant: Karl Storz Endoscopy-America, Ethicon Endo-Surgery, Conceptus Incorporated, CooperSurgical Speaker's Bureau: Karl Storz Endoscopy-America, Ethicon Endo-Surgery, Conceptus Incorporated, CooperSurgical Micah Harris Grants/Research Support: Halt Medical Eileen C. Young Other: Employee - Olympus Gary N. Frishman* Asterisk (*) denotes no financial relationships to disclose.
4

Principles of Office Based Gynecologic Surgery
Office Based Hysteroscopy:Office Based Hysteroscopy:
MICAH HARRIS M.D.
OB/GYN CONSULTANTS ANDWOMEN’S HEALTH RESEARCH
PHOENIX, AZ
Safety and RegulationSafety and Regulation
Principles of Office Based Gynecologic Surgery
Office Based Hysteroscopy
Grants/Research Support: Halt Grants/Research Support: Halt MedicalMedicalpppp
Principles of Office Based Gynecologic Surgery
Office Based Hysteroscopy
At the conclusion of this activity, the participant will be able to:
List patient co-morbidities that are contraindications to office surgery.
List qualities of surgical procedures that make them f ffappropriate for the office setting.
List the Levels of Office-Based Surgery
List important features of an office-based surgical practice to promote patient safety.
Describe the types of documentation necessary to maintain an office-based surgical practice
List the various agencies and associations that have published guidelines concerning office-based surgery
Principles of Office Based Gynecologic Surgery
So Many New Procedures..
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Overview
Gynecology is a procedureGynecology is a procedure--based specialtybased specialty Range from very minor (Range from very minor (egeg, Pap smear) to very , Pap smear) to very
major (major (egeg, hysterectomy and pelvic support), hysterectomy and pelvic support)
Majority of income is from proceduresMajority of income is from proceduresj y pj y p Better income per hour spent of actual effortBetter income per hour spent of actual effort
Income potential diluted by associated activitiesIncome potential diluted by associated activities PaperworkPaperwork
Travel between office and surgery centers or hospitalsTravel between office and surgery centers or hospitals
PeriPeri--operative care operative care –– nonnon--operative time with patientoperative time with patient
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Overview
Traditional procedure model keeps us out of Traditional procedure model keeps us out of the officethe office Hospitals or surgery centersHospitals or surgery centers
Time out of office is not reimbursedTime out of office is not reimbursed
Must become more efficientMust become more efficient Integrate procedures into office when possibleIntegrate procedures into office when possible
Allows greater productivityAllows greater productivity
Work smarter, not longer!Work smarter, not longer!
5
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:General Considerations
Must be the correct surgeonMust be the correct surgeon Must be the correct patientMust be the correct patient Must be the correct procedureMust be the correct procedure Patient safety a priority!Patient safety a priority! Patient safety a priority!Patient safety a priority!
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Patient Selection
Patient Selection (ASA class I or II)Patient Selection (ASA class I or II)
Avoid CoAvoid Co--morbid conditionsmorbid conditions AnxietyAnxiety
AsthmaAsthma
ObesityObesity
Heart diseaseHeart disease
Psychosocial issuesPsychosocial issues Prior experience with office proceduresPrior experience with office procedures
Realistic patient expectationsRealistic patient expectations
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Procedure Choice
Appropriate for performing in officeAppropriate for performing in office Brief and focusedBrief and focused Not overly complicatedNot overly complicated Basic technological requirementsBasic technological requirementsg qg q
Anticipation of patient comfortAnticipation of patient comfort How long will patient be immobilized?How long will patient be immobilized? Comfortable table / bed for patientComfortable table / bed for patient Adequate room / time for recoveryAdequate room / time for recovery Anticipation of analgesiaAnticipation of analgesia
Reasonable anticipation of patient safetyReasonable anticipation of patient safety
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Procedure Choice
Safe and effective proceduresSafe and effective procedures Minimal analgesia / anesthesia requirementsMinimal analgesia / anesthesia requirements
No increase in liabilityNo increase in liability
Easy to learn and performEasy to learn and perform
I d i b tI d i b t Improved reimbursementImproved reimbursement Global fee for inGlobal fee for in--office proceduresoffice procedures
Efficient use of timeEfficient use of time
Reasonable capital investmentReasonable capital investment Leasing incentivesLeasing incentives
Cost per procedure based on volumeCost per procedure based on volume
Principles of Office Based Gynecologic Surgery
Office Surgery Patient Safety Issues
Increasing number of office Increasing number of office proceduresprocedures
Less oversight and scrutinyLess oversight and scrutiny
ACOG Presidential Task Force on ACOG Presidential Task Force on Office SurgeryOffice Surgery “Patients have a right to expect the “Patients have a right to expect the
same level of safety regardless of where same level of safety regardless of where they seek treatment.”they seek treatment.”
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Safety and Regulatory Considerations
Patient safety must remain primaryPatient safety must remain primary Desire for convenience should NOT increase riskDesire for convenience should NOT increase risk
Desire for convenience should NOT trump safetyDesire for convenience should NOT trump safety
Accreditation requirements by certain statesAccreditation requirements by certain states Accreditation requirements by certain statesAccreditation requirements by certain states
6
Principles of Office Based Gynecologic Surgery
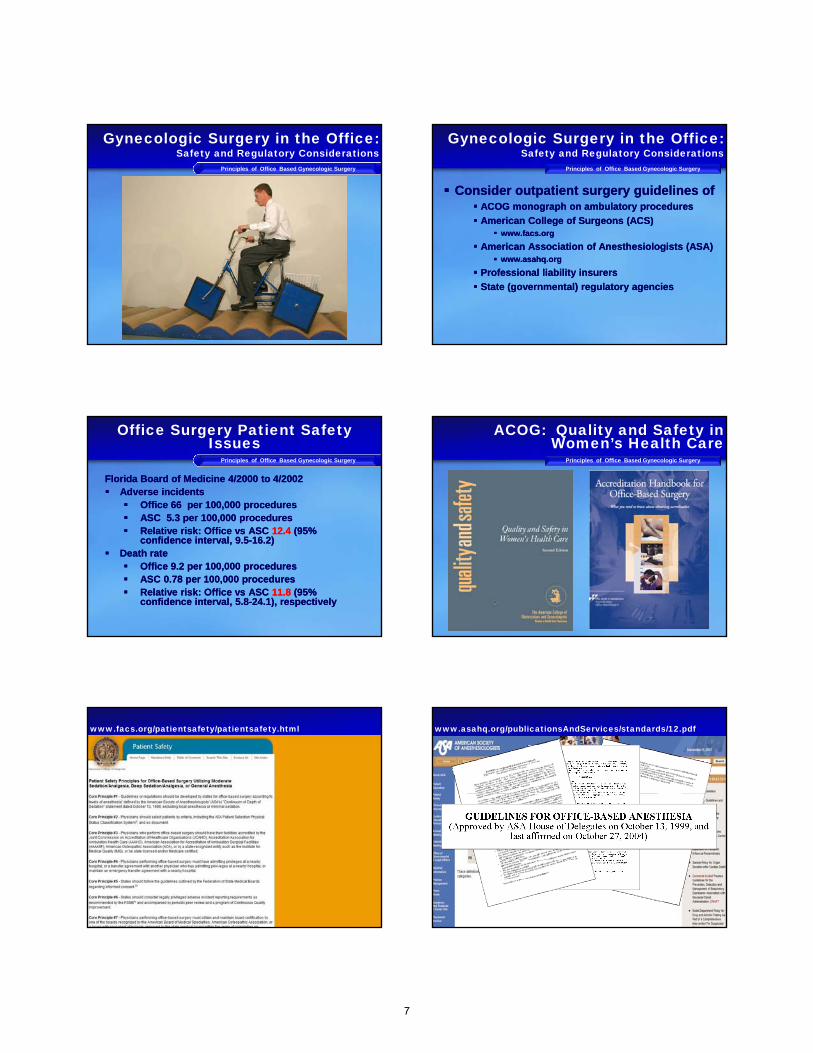
Gynecologic Surgery in the Office:Safety and Regulatory Considerations
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Safety and Regulatory Considerations
Consider outpatient surgery guidelines ofConsider outpatient surgery guidelines of ACOG monograph on ambulatory proceduresACOG monograph on ambulatory procedures
American College of Surgeons (ACS)American College of Surgeons (ACS) www facs orgwww facs orgwww.facs.orgwww.facs.org
American Association of Anesthesiologists (ASA)American Association of Anesthesiologists (ASA) www.asahq.orgwww.asahq.org
Professional liability insurersProfessional liability insurers
State (governmental) regulatory agencies State (governmental) regulatory agencies
Principles of Office Based Gynecologic Surgery
Office Surgery Patient Safety Issues
Florida Board of Medicine 4/2000 to 4/2002Florida Board of Medicine 4/2000 to 4/2002 Adverse incidents Adverse incidents
Office 66 per 100,000 proceduresOffice 66 per 100,000 procedures ASC 5.3 per 100,000 proceduresASC 5.3 per 100,000 procedures Relative risk: Office vs ASCRelative risk: Office vs ASC 12.4 12.4 (95% (95%
confidence interval, 9.5confidence interval, 9.5--16.2) 16.2) Death rate Death rate
Office 9.2 per 100,000 procedures Office 9.2 per 100,000 procedures ASC 0.78 per 100,000 proceduresASC 0.78 per 100,000 procedures Relative risk: Office vs ASC Relative risk: Office vs ASC 11.811.8 (95% (95%
confidence interval, 5.8confidence interval, 5.8--24.1), respectively24.1), respectively
Principles of Office Based Gynecologic Surgery
ACOG: Quality and Safety in Women’s Health Care
Principles of Office Based Gynecologic Surgery
www.facs.org/patientsafety/patientsafety.html
Principles of Office Based Gynecologic Surgery
www.asahq.org/publicationsAndServices/standards/12.pdf
7

Principles of Office Based Gynecologic Surgery
Levels of Anesthesia
I 32 4
Principles of Office Based Gynecologic Surgery
Levels of Office Based Surgery
Level I Level I -- local anesthetic with minimal local anesthetic with minimal preoperative oral anxiolyticpreoperative oral anxiolytic
Level II Level II –– Moderate sedationModerate sedation
Level III Level III –– Deep sedation or General Deep sedation or General anesthesiaanesthesia
Principles of Office Based Gynecologic Surgery
Getting Started
Identify a Medical DirectorIdentify a Medical Director
Create ChecklistsCreate Checklists
Initiate DrillsInitiate Drills
Maintain a LogMaintain a Log
Principles of Office Based Gynecologic Surgery
Getting Started
Identify a Medical DirectorIdentify a Medical Director A designated partner in the practice, or A designated partner in the practice, or
yourself if a solo practitioner.yourself if a solo practitioner.
Responsible for overseeing regulatoryResponsible for overseeing regulatory Responsible for overseeing regulatory Responsible for overseeing regulatory and safety concerns, including and safety concerns, including credentialing and protocols.credentialing and protocols.
Principles of Office Based Gynecologic Surgery
Getting Started:Checklists
Create and use checklists for each Create and use checklists for each casecase
Promotes consistent Promotes consistent behaviourbehaviour
Provides documentation for ongoing Provides documentation for ongoing quality monitoring or external quality monitoring or external reviewersreviewers
Principles of Office Based Gynecologic Surgery
Checklists for Office Based Surgery
PreoperativePreoperative Informed consent, Patient RightsInformed consent, Patient Rights
History/Physical, workHistory/Physical, work--up and resultsup and results
Current medications, past reactionsCurrent medications, past reactions
Confirmation NPO statusConfirmation NPO status
Airway assessment Airway assessment
8
Principles of Office Based Gynecologic Surgery
Checklists for Office Based Surgery
IntraoperativeIntraoperative Surgical Time OutSurgical Time Out
Record of medications administeredRecord of medications administered
Vital signs at 5 minute intervalsVital signs at 5 minute intervals Blood pressureBlood pressure
PulsePulse
Oxygen saturationOxygen saturation
End Tidal CO2 (optional)End Tidal CO2 (optional)
Principles of Office Based Gynecologic Surgery
Checklists for Office Based Surgery
PostoperativePostoperative Return of vital signs to within 20% of Return of vital signs to within 20% of
baselinebaseline
Other signs: Bleeding swellingOther signs: Bleeding swelling Other signs: Bleeding, swellingOther signs: Bleeding, swelling
Discharge instructionsDischarge instructions
Driver for procedures having required Driver for procedures having required any sedationany sedation
Follow up phone call within 48 hoursFollow up phone call within 48 hours
Principles of Office Based Gynecologic Surgery
Mock Drills
Performed quarterlyPerformed quarterly
Involve specifically identified Involve specifically identified individuals in the office (e.g. in the individuals in the office (e.g. in the
t f Ti ill llt f Ti ill llevent of an emergency Tim will call event of an emergency Tim will call 911.)911.)
Physically rehearsed for particular Physically rehearsed for particular scenariosscenarios
Principles of Office Based Gynecologic Surgery
Mock Drills
Recommended Scenarios Recommended Scenarios Vasovagal ReactionVasovagal Reaction
Local anesthetic toxicityLocal anesthetic toxicity
Allergic reactionAllergic reaction
HemorrhageHemorrhage
Respiratory arrest/excessive sedationRespiratory arrest/excessive sedation
Principles of Office Based Gynecologic Surgery
Create a Procedure Log
Documentation in addition to that in Documentation in addition to that in patient chartpatient chart
Essential for ongoing review, quality Essential for ongoing review, quality ttassessmentassessment
Documentation of compliance and Documentation of compliance and safety in one separate locationsafety in one separate location
Necessary should accreditation be Necessary should accreditation be soughtsought
Principles of Office Based Gynecologic Surgery
Accreditation
Worthwhile if all recommendations Worthwhile if all recommendations followed and documentedfollowed and documented
Process may assist in setting up Process may assist in setting up t lt lprotocolsprotocols
Many agencies availableMany agencies available
Not required in all instancesNot required in all instances State Board of MedicineState Board of Medicine
Malpractice InsurerMalpractice Insurer
Third Party Third Party PayorsPayors
9

Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office: www.jointcommission.org
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Patient Safety
General ConsiderationsGeneral Considerations Strict adherence to indications / contraindicationsStrict adherence to indications / contraindications
Thorough evaluation in advanceThorough evaluation in advancegg Imaging and other testingImaging and other testing
No surprises in procedure roomNo surprises in procedure room
Not the time or place for “atypical patient”Not the time or place for “atypical patient”
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Transition to Office
More than just a change in locationMore than just a change in location Start with full sedation in operating roomStart with full sedation in operating room
Become totally comfortable with techniqueBecome totally comfortable with technique
Slowly lessen level of anesthesiaSlowly lessen level of anesthesia
Achieve minimum needed anesthesia levelAchieve minimum needed anesthesia level Balance between comfort and alertnessBalance between comfort and alertness
Mimic office conditions in OR before moveMimic office conditions in OR before move Use only instruments you have in officeUse only instruments you have in office
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Transition to Office
Know indications / contraindicationsKnow indications / contraindications
Complete comfort with procedureComplete comfort with procedure
Review IFU completelyReview IFU completely
Have written protocols in placeHave written protocols in place
Have emergency contingency planHave emergency contingency plan
Not the time or place for “atypical” procedureNot the time or place for “atypical” procedure
Principles of Office Based Gynecologic Surgery
Gynecologic Surgery in the Office:Patient Analgesia
Learn from our oral surgeon colleaguesLearn from our oral surgeon colleagues
Comfort, convenience and safety NOT mutually exclusiveComfort, convenience and safety NOT mutually exclusive
Principles of Office Based Gynecologic Surgery
ASA Physical Status Classification System
10

Principles of Office Based Gynecologic Surgery
ASA Status and Mortality
Principles of Office Based Gynecologic Surgery
Recommendation
Only ASA Status 1 or 2 in officeOnly ASA Status 1 or 2 in office
PrescreeningPrescreening Adverse rxn to local anesthesia (personal or FH)Adverse rxn to local anesthesia (personal or FH)
Previous failure with local anesthesia or low painPrevious failure with local anesthesia or low pain Previous failure with local anesthesia or low pain Previous failure with local anesthesia or low pain thresholdthreshold
An acute respiratory processAn acute respiratory process
Failure to comply with preoperative dietary restrictionsFailure to comply with preoperative dietary restrictions
Substance abuseSubstance abuse
HighHigh--risk airway assessmentrisk airway assessment
Abnormal blood sugarsAbnormal blood sugars
Pregnancy (unless procedure is pregnancy related)Pregnancy (unless procedure is pregnancy related)
Principles of Office Based Gynecologic Surgery
Mallampati Airway ClassificationPrinciples of Office Based Gynecologic Surgery
Recommendation
Ability to Rescue PatientsAbility to Rescue Patients Level ILevel I
BLS trainingBLS training
Emergency equipment for cardiorespiratory support and Emergency equipment for cardiorespiratory support and t t t f h l it t t f h l itreatment of anaphylaxistreatment of anaphylaxis
Level IILevel II Min of 2 staff Min of 2 staff ––
Physician/ surgeonPhysician/ surgeon
Health care professional with ACLS trainingHealth care professional with ACLS training
TimeTime--OutsOuts
Principles of Office Based Gynecologic Surgery
Office Procedure Examples
Hysteroscopic sterilizationHysteroscopic sterilization
Endometrial ablationEndometrial ablation
Principles of Office Based Gynecologic Surgery
Local Anesthetic Toxicity
Agent Duration Maximum Dose
1% Lidocaine 30-60 min 4.5 mg/kg
1% Lidocaine with Epinephrine
120-360 min 7 mg/kg
0.25% Marcaine 120-240 min 2.5 mg/kg
0.25% Marcainewith Epinephrine
180-420 minDo not exceed 225 mg
11
Principles of Office Based Gynecologic Surgery
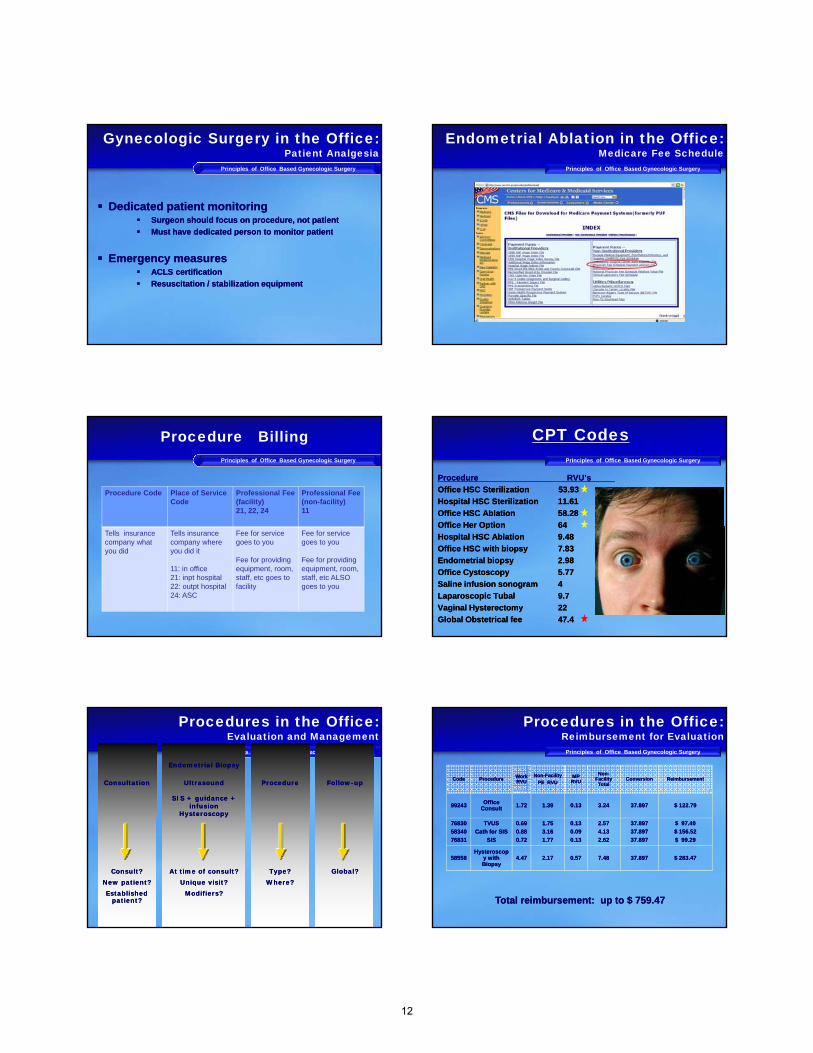
Gynecologic Surgery in the Office:Patient Analgesia
Dedicated patient monitoringDedicated patient monitoring Surgeon should focus on procedure, not patientSurgeon should focus on procedure, not patient
Must have dedicated person to monitor patientMust have dedicated person to monitor patientMust have dedicated person to monitor patientMust have dedicated person to monitor patient
Emergency measuresEmergency measures ACLS certificationACLS certification
Resuscitation / stabilization equipmentResuscitation / stabilization equipment
Principles of Office Based Gynecologic Surgery
Endometrial Ablation in the Office:Medicare Fee Schedule
Principles of Office Based Gynecologic Surgery
Procedure Billing
Procedure Code Place of Service Code
Professional Fee(facility)21, 22, 24
Professional Fee(non-facility)11
Tells insurance company what you did
Tells insurance company where you did it
11: in office21: inpt hospital22: outpt hospital24: ASC
Fee for service goes to you
Fee for providing equipment, room, staff, etc goes to facility
Fee for service goes to you
Fee for providing equipment, room, staff, etc ALSO goes to you
Principles of Office Based Gynecologic Surgery
CPT Codes
ProcedureProcedure RVU’sRVU’s
Office HSC Sterilization Office HSC Sterilization 53.9353.93
Hospital HSC SterilizationHospital HSC Sterilization 11.6111.61
Office HSC AblationOffice HSC Ablation 58.2858.28
Office Her OptionOffice Her Option 6464Office Her OptionOffice Her Option 6464
Hospital HSC AblationHospital HSC Ablation 9.489.48
Office HSC with biopsyOffice HSC with biopsy 7.837.83
Endometrial biopsyEndometrial biopsy 2.982.98
Office CystoscopyOffice Cystoscopy 5.775.77
Saline infusion sonogramSaline infusion sonogram 44
Laparoscopic TubalLaparoscopic Tubal 9.79.7
Vaginal HysterectomyVaginal Hysterectomy 2222
Global Obstetrical feeGlobal Obstetrical fee 47.447.4
Principles of Office Based Gynecologic Surgery
ConsultationConsultation
Endometrial BiopsyEndometrial Biopsy
UltrasoundUltrasound
SIS + guidance + SIS + guidance + infusioninfusion
HysteroscopyHysteroscopy
ProcedureProcedure FollowFollow--upup
Procedures in the Office:Evaluation and Management
Consult?Consult?New patient?New patient?Established Established
patient?patient?
At time of consult?At time of consult?Unique visit?Unique visit?
Modifiers?Modifiers?
Type?Type?Where?Where?
Global?Global?
Principles of Office Based Gynecologic Surgery
Procedures in the Office:Reimbursement for Evaluation
CodeCode ProcedureProcedure Work Work RVURVU
NonNon--FacilityFacility
PE RVUPE RVUMP MP
RVURVU
NonNon--Facility Facility
TotalTotalConversionConversion ReimbursementReimbursement
9924399243 Office Office ConsultConsult 1.721.72 1.391.39 0.130.13 3.243.24 37.89737.897 $ 122.79$ 122.79
7683076830
5834058340
7683176831
TVUSTVUS
Cath for SISCath for SIS
SISSIS
0.690.69
0.880.88
0.720.72
1.751.75
3.163.16
1.771.77
0.130.13
0.090.09
0.130.13
2.572.57
4.134.13
2.622.62
37.89737.897
37.89737.897
37.89737.897
$ 97.40$ 97.40
$ 156.52$ 156.52
$ 99.29$ 99.29
5855858558HysteroscopHysteroscop
y with y with BiopsyBiopsy
4.474.47 2.172.17 0.570.57 7.487.48 37.89737.897 $ 283.47$ 283.47
Total reimbursement: up to $ 759.47Total reimbursement: up to $ 759.47
12

Principles of Office Based Gynecologic Surgery
Procedures in the Office:Reimbursement for Procedure
CodeCode ProcedureProcedure Work Work RVURVU
FacilityFacility
PE RVUPE RVUMP MP
RVURVUFacility Facility TotalTotal ConversionConversion ReimbursementReimbursement
5856358563HysteroscopyHysteroscopy, endometrial , endometrial
ablationablation6.166.16 2.752.75 0.740.74 9.659.65 37.89737.897 $ 365.71$ 365.71
5856358563HysteroscopyHysteroscopy, endometrial , endometrial
ablationablation6.166.16
56.1956.19
NonNon--facilityfacility
0.740.7463.0963.09
NonNon--facilityfacility
37.89737.897 $ 2390.05$ 2390.05
Place of Service: inpatient hospital (21); outpatient hospital (22); ambulatory surgery center (24)Place of Service: inpatient hospital (21); outpatient hospital (22); ambulatory surgery center (24)
Place of Service: in office (11)Place of Service: in office (11)
Principles of Office Based Gynecologic Surgery
Procedures in the Office:Effective Reimbursement in Office
Procedure ReimbursementProcedure Reimbursement $ 3000.00$ 3000.00
Device (approximate cost)Device (approximate cost) -- $ 1300 00$ 1300 00Device (approximate cost) Device (approximate cost) -- $ 1300.00$ 1300.00
Disposables (drapes / drugs)Disposables (drapes / drugs) -- $ 100.00$ 100.00
CRNA*CRNA* -- $ 250.00$ 250.00
Effective ReimbursementEffective Reimbursement $ 1350.00$ 1350.00
* * CRNA may be able to bill independentlyCRNA may be able to bill independently
Principles of Office Based Gynecologic Surgery
Procedures in the Office:Follow-up Visits
Global IntervalGlobal Interval Hysterectomy Hysterectomy –– 90 days90 days
Ablation Ablation –– 0 days0 days
Principles of Office Based Gynecologic Surgery
Procedures in the Office:Summary
Can be performed easily in officeCan be performed easily in office Adequate preparation / trainingAdequate preparation / training Logical progression from OR to officeLogical progression from OR to office
Can be performed safely in officeCan be performed safely in office Can be performed safely in officeCan be performed safely in office Adherence to indications / contraindicationsAdherence to indications / contraindications Adherence to published guidelinesAdherence to published guidelines
Is well accepted by (selected) patientsIs well accepted by (selected) patients does not need to be uncomfortabledoes not need to be uncomfortable More comfortable for someMore comfortable for some Perceived as more “confidential”Perceived as more “confidential”
Principles of Office Based Gynecologic Surgery
Procedures in the Office:Summary
Increases practice diversityIncreases practice diversity Can offer procedures in hospital or in officeCan offer procedures in hospital or in office
Ease of schedulingEase of schedulingEase of schedulingEase of scheduling
Reduces time spent out of officeReduces time spent out of office
Optimize office space and personnelOptimize office space and personnel
Principles of Office Based Gynecologic Surgery
Office Hysteroscopy
13

Office-Based Surgery
Office Based Surgery Resident Didactic October 2011
Thank youThank you
Principles of Office Based Gynecologic Surgery
References
1.1. WortmanWortman M . Instituting an Office Based Surgery Program in M . Instituting an Office Based Surgery Program in the Gynecology Office. JIMG 2010; 17, 673the Gynecology Office. JIMG 2010; 17, 673--683.683.
2.2. ACOG Guidelines for Initiating an Office Based Surgical ACOG Guidelines for Initiating an Office Based Surgical Practice. http:// Practice. http:// www.acog.org/www.acog.org/
3.3. AMA Core Principles of Office Based Surgery . AMA Core Principles of Office Based Surgery . http://www.asahq.org/washington/coreprinciples.htmhttp://www.asahq.org/washington/coreprinciples.htm
4.4. American Society of Anesthesiologists Guidelines for Office American Society of Anesthesiologists Guidelines for Office Based Anesthesia. http://www.asahg.org/Publicationsand Based Anesthesia. http://www.asahg.org/Publicationsand services/sgstoc.htmservices/sgstoc.htm
Principles of Office Based Gynecologic Surgery
References
4. ASA Physical Status Classification System 4. ASA Physical Status Classification System http://www.asahq.org/clinical/physicalstatus.htmhttp://www.asahq.org/clinical/physicalstatus.htm
5. 5. Accreditation Handbook for Office Based Surgery Accreditation Handbook for Office Based Surgery http://www.jointcommission.org/NR/rdonlyres/http://www.jointcommission.org/NR/rdonlyres/
14

Patient Comfort for Office Procedures
Isabel Green, MD
Johns Hopkins University
AAGL 2012
Disclosures
• I have no financial relationships to disclose.
Objectives
• Describe the innervations of the uterus and cervix, and apply knowledge of anatomy to consider sources of discomfort during hysteroscopy y py
• Describe the analgesic options for office hysteroscopy, including mechanism of action, risks and dosages of each class of medication.
• Apply current data on analgesic options to establish a safe analgesia protocol for the office
CHALLENGE
Pain is the most frequently cited reason for failed office hysteroscopy, it is the most important determinant of procedure acceptability
“Once a patient is invited into the office setting, they have the right to expect the same level of patient safety that occurs in a more regulated hospital setting”
Kaneshiro Cochrane 2012ACOG Presidential Task Force, 2010
Innervation of the Uterus
Superior hypogastric plexus – uterovaginalplexus
Plexus courses lateral to attachment of uterosacral ligaments
Fibers travel in the parametrial tissue
Nerves course with uterine branches and IP ligamentsMyometriumBasal layer of endometriumSubmucosal layer of the cervix
15

Sources of DiscomfortConsider anatomy
Speculum
Cervix
Dilation
Whittemore Enterprises
Manipulation
Uterine distension
Endometrium
Fallopian tube
PROCEDURE SPECIFICPATIENT FACTORS
MenopauseCervical StenosisObesityAnxiety
Analgesia Options
NSAIDS
NARCOTICS
ANXIOLYTIC
LOCAL
Mechanism of ActionDosagesRisks
Data supporting use
NSAIDSExamples Mechanism of Action Onset/Duration
IbuprofenKetorolacMeloxicamNabumetoneNaproxenCelecoxib
Cyclooxygenase inhibition
Inhibits PG synthesis
Anti‐inflammatory
30 – 60 minDuration 4‐6 hrs
Long acting: Duration 12 hrs
Clinical efficacy is similar, patient response is highly variable
RISKS:GI toxicityAcute renal failureDrug interactionsAllergies
Short treatment durationCheck med listCheck allergies
NSAIDS ‐ Data
Double‐blind placebo trial demonstrates significant reduction in POST procedure pain, NO significant benefit in discomfort during procedure
Nagele et al. BJOG. 1997Marsh et al. Fertility & Sterility, 2005Fothergill. Obstet Gynecol Clinics, 2008
May reduce pain post procedureMay reduce need for rescue analgesia
NarcoticsExamples Mechanism of Action Onset/Duration
OxycodoneTramadolFentanylBuprenorphine
CNS: opioid receptorsSerotonin Norepinephrine
ORAL15‐60 min/4 hour
IV<10 min/30‐6o min
RISKS:SomnolenceRespiratory DepressionHypotensionNausea/vomitingPruritusAllergic reaction
Poyhia et al 1992
Consider cumulative effects & drug interactions
Narcotics ‐ Data
IV Tramadol 30 min prior resulted in significant decrease in VAS during and immediately following procedure when compared to placebo.
Ahmad. Cochrane 2010Kaneshiro. Cochrane 2012Floris et al. Fertility & Sterility. 2007
May result in decreased pain score at placement of 2nd Essure device
Limited isolated RCT
16
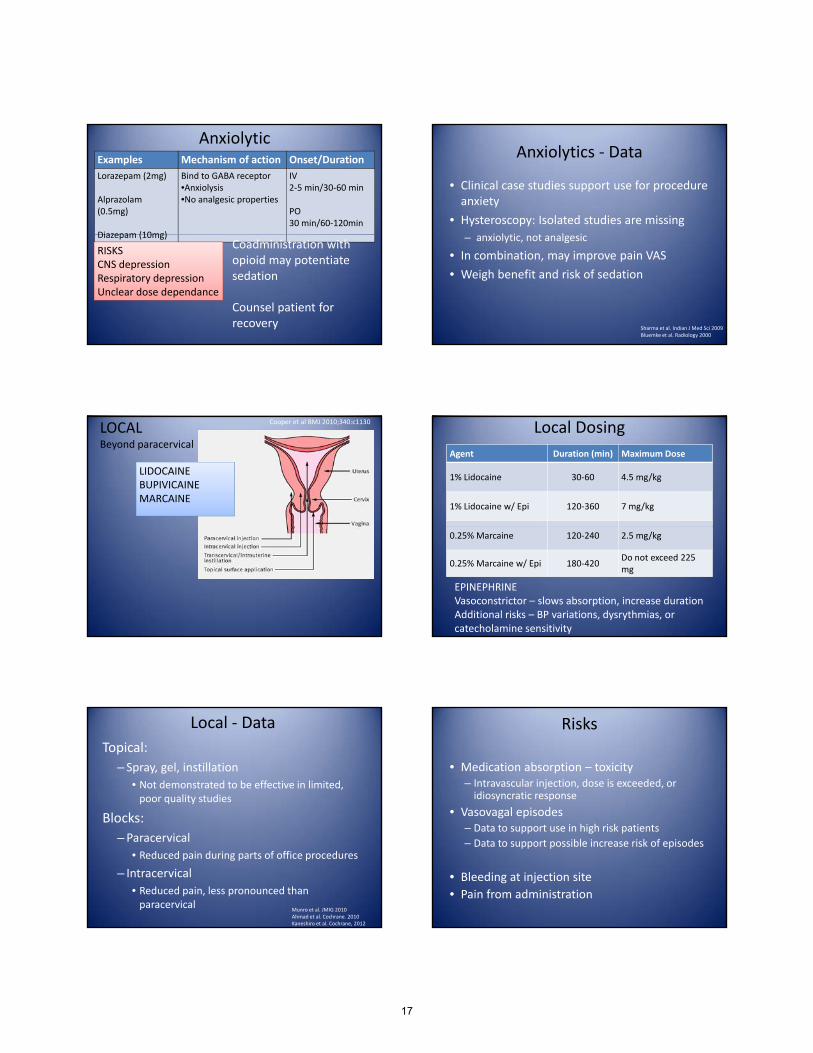
AnxiolyticExamples Mechanism of action Onset/Duration
Lorazepam (2mg)
Alprazolam(0.5mg)
Diazepam (10mg)
Bind to GABA receptor•Anxiolysis•No analgesic properties
IV2‐5 min/30‐60 min
PO30 min/60‐120min
Diazepam (10mg)
RISKSCNS depressionRespiratory depressionUnclear dose dependance
Coadministration with opioid may potentiate sedation
Counsel patient for recovery
Anxiolytics ‐ Data
• Clinical case studies support use for procedure anxiety
• Hysteroscopy: Isolated studies are missing
i l ti t l i– anxiolytic, not analgesic
• In combination, may improve pain VAS
• Weigh benefit and risk of sedation
Sharma et al. Indian J Med Sci 2009Bluemke et al. Radiology 2000
LOCALBeyond paracervical
LIDOCAINEBUPIVICAINEMARCAINE
Cooper et al BMJ 2010;340:c1130 Local Dosing
Agent Duration (min) Maximum Dose
1% Lidocaine 30‐60 4.5 mg/kg
1% Lidocaine w/ Epi 120‐360 7 mg/kg
0.25% Marcaine 120‐240 2.5 mg/kg
0.25% Marcaine w/ Epi 180‐420Do not exceed 225 mg
EPINEPHRINEVasoconstrictor – slows absorption, increase durationAdditional risks – BP variations, dysrythmias, orcatecholamine sensitivity
Local ‐ Data
Topical:
– Spray, gel, instillation
• Not demonstrated to be effective in limited, poor quality studies
Blocks:Blocks:
–Paracervical
• Reduced pain during parts of office procedures
– Intracervical
• Reduced pain, less pronounced than paracervical
Munro et al. JMIG 2010Ahmad et al. Cochrane. 2010Kaneshiro et al. Cochrane, 2012
Risks
• Medication absorption – toxicity– Intravascular injection, dose is exceeded, or idiosyncratic response
• Vasovagal episodesg p– Data to support use in high risk patients
– Data to support possible increase risk of episodes
• Bleeding at injection site
• Pain from administration
17

ComplicationsLocal anesthetic toxicity
NEURO
– Ringing in ears, tingling, metallic taste, agitation, seizures
– Stop infiltration, airway support, serial vitals,
– Consider/prepare benzodiazepine for seizuresConsider/prepare benzodiazepine for seizures
CARDIO
– Bradycardia, vasodilation, AV block, ventricular arrythmias
– Stop infiltration, airway, cardiac monitor, call for help
– ACLS
– Consider fat emulsion
ComplicationsAllergic Reaction/Anaphylaxis
– Urticaria, flushing, pruritus, respiratory distress
– Stop, position, airway, oxygen, call for help
– 1st step: epinephrine (1mg/mL): 0.3‐ 0.5 mg IM, repeat q 5‐15 min
– IV fluid boluses
Over sedation/Respiratory Depression
– Decrease responsiveness to stimuli, desaturation
– Stop meds, engage the patient, position, airway, oxygen, call for help
– Reverse w/ meds: naloxone or flumazenil
Minimize Need for Analgesia
Flexible hysteroscope
Smallest diameter
Vaginoscopy technique
Balance patient comfort and no analgesia
Yang et al. Obstet & Gynecol Survey 2002
Put it all together: example protocols
Diagnostic Hysteroscopy & Endometrial biopsy
Ibuprofen 800 mg at 10pm prior
Ibuprofen 800mg 1 hour prior
HysteroscopicSterilizationIbuprofen 800 mg q 8hr day
prior
Toradol 30 mg IM 30 min‐60 min prior
Paracervical block
1% lidocaine, 10cc total
10 min prior
min prior
Paracervical block 1% lidocaine, 10cc total, 10 min prior
Optional:
Oxycodone 5mg PO 30 min prior
Xanax 0.5mg PO 30 min prior
Analgesia Levels
Level I: Local anesthesia with limited preoperative oral anxiolyticanxiolytic
Level II: Moderate sedation
Level III: Deep sedation
ACOG, Presidential Task Force, 2010
Definitions
Analgesia: relief of pain without intentionally producing a sedated state. Altered mental status may occur as a secondary effect of medications administered for analgesiamedications administered for analgesia
18

Definitions
• Minimal sedation: patient responds normally to verbal commands. Cognitive function and coordination may be impaired, but ventilatoryand cardiovascular functions are unaffected.
• Moderate sedation: patient responds to verbal commands alone or when accompanied by light No mention of types of medications, p y gtouch. Protective airway reflexes and adequate ventilation are maintained. Cardiovascular function remains stable.
• Deep sedation: Patient cannot be easily aroused, but responds purposefully to noxious stimulation. Assistance may be needed to ensure airway is protected and ventilation maintained. Cardiovascular function is stable.
dosages, or route of administration
What to do in your office?
Beyond ACOG guidelines:
State regulation and accreditation requirements
Hospital regulations and protocols
“The decision regarding type of anesthesia shouldThe decision regarding type of anesthesia should NOT be altered based on limitations of equipment or personnel ... Such limitations might necessitate performing the procedure in a more acute care facility.”
What level of sedation are you afforded?Are you also regulated in meds and routes?
ACOG Presidential Task Force 2010
Right patient, Right procedure, Right Surgeon, Right Place
References
• Fertil Steril. 2010 Sep;94(4):1189‐94. Epub 2009 Aug 14.Analysis of pain and satisfaction with office‐based hysteroscopic sterilization.Levie M, Weiss G, Kaiser B, Daif J, Chudnoff SG.
• Fertil Steril. 2008 Oct;90(4):1182‐6. Epub 2008 Jan 16.Satisfaction and tolerance with office hysteroscopic tubal sterilization.Arjona JE, Miño M, Cordón J, Povedano B, Pelegrin B, Castelo‐Branco C.SourceDepartment of Gynecology and Obstetrics, Hysteroscopy Unit, Reina Sofía University Hospital, Cordoba, Spain.
• Cochrane Database Syst Rev. 2010 Nov 10;(11):CD007710.Pain relief for outpatient hysteroscopy.Ahmad G, O'Flynn H, Attarbashi S, Duffy JM, Watson A.SourceObstetrics & Gynaecology, Pennine Acute NHS Trust, Manchester, UK.
• Nagele F. Lockwood G. Magos AL. Randomised placebo controlled trial of mefenamic acid for premedication at outpatient hysteroscopy: a pilot study. Br J Obstet Gynaecol. 1997; 104 (4): 842‐4.
• Marsh F, Thewlis J, Duffy S. Thermachoice endometrial ablation in the outpatient setting, without local h i i d i i h d il & ili ( )anesthesia or intravenous sedation: A prospective cohort study. Fertilty & Sterility. 2005; 83 (3); 715‐720.
• Floris et al. Efficacy of intravenous tramadol treatment for reducing pain during office diagnostic hysteroscopy. Fertility & Sterility. 2007; 87 (1): 147‐151
• ACOG Presidential Task Force on Patient Safety in the Office Setting. April 2010.• Kaneshiro B, Grimes DA, Lopez LM. Pain management for tubal sterilization by hysteroscopy. The Cochrane
Collaboration. 2012.• Munro MG, Brooks PG. Use of local anesthesia for office diagnostic and operative hysteroscopy. JMIG.2010;
17 (6): 709‐18• Williams Gynecology 2008.• Bluemke DA, Breiter SN. Sedation procedures in MR imaging: safety, effectiveness and nursing effect on
examinations. Radiology. 2000; 216 (3): 645• Sharma et al. Comparison of efficacy of oral drotaverine plus mefenamic acid with parcervical block and
with intravenous sedation for pain relief during hysteroscopy and endometrial biopsy. Indian J Med Sci. 2009; 63 (6): 244‐52.
19

Diagnostic Hysteroscopy Diagnostic Hysteroscopy Evaluation of the Uterine Evaluation of the Uterine CCavity andavity and
PrePre--Operative Operative DDecision ecision MMakingaking
Amy Amy Garcia, Garcia, MDMD
AAGL/SRS FellowshipAAGL/SRS Fellowship--Trained in MIGTrained in MIG
DirectorDirector, Center for Women, Center for Women’’s Surgerys Surgery
Clinical Assistant Clinical Assistant Professor, University of New MexicoProfessor, University of New MexicoDepartment of Obstetrics and GynecologyDepartment of Obstetrics and Gynecology
Division of UrogynecologyDivision of Urogynecology
Albuquerque, New MexicoAlbuquerque, New Mexico
DisclosureDisclosure Grants/Research Support: HologicGrants/Research Support: Hologic
Consultant: Conceptus Incorporated, Ethicon EndoConsultant: Conceptus Incorporated, Ethicon Endo--Surgery, Ethicon Women's Health & Urology, IOGYN, Surgery, Ethicon Women's Health & Urology, IOGYN, Minerva SurgicalMinerva Surgical
Speaker's Bureau: Conceptus Speaker's Bureau: Conceptus IncInc
ObjectivesObjectives
Acquire, setAcquire, set--up and utilize supplies and up and utilize supplies and equipment necessary for diagnostic equipment necessary for diagnostic hysteroscopy in the officehysteroscopy in the officehysteroscopy in the office hysteroscopy in the office
Utilize a Utilize a hysteroscope (rigid and/or flexible) hysteroscope (rigid and/or flexible) for diagnostic procedures in the officefor diagnostic procedures in the office
Discern diagnostic hysteroscopy techniques Discern diagnostic hysteroscopy techniques for infor in--office proceduresoffice procedures
Indications for HysteroscopyIndications for Hysteroscopy
Evaluation of AUBEvaluation of AUB Heavy menstrual bleedingHeavy menstrual bleeding Menopausal bleedingMenopausal bleeding
Abnormal Ultrasound FindingsAbnormal Ultrasound Findings Enlarged endometrial stripeEnlarged endometrial stripe Suspected intraSuspected intra--cavitarycavitary pathologypathology
InfertilityInfertility
IUDIUD
Hysteroscopy vs. TV USHysteroscopy vs. TV USMenopausal WomenMenopausal Women
MarelloMarello, , etaletal Menopausal women with EMS </ 5 mm Menopausal women with EMS </ 5 mm
3% of symptomatic women3% of symptomatic women polypspolyps
10 % of asymptomatic women10 % of asymptomatic women 16 polyps16 polyps
3 3 myomasmyomas
Hysteroscopy (HS) & Saline Infusion Hysteroscopy (HS) & Saline Infusion Sonography (SIS) vs. TV USSonography (SIS) vs. TV US
Di i fDi i f I t itI t it P th lP th l Diagnosis of Diagnosis of IntracavitaryIntracavitary PathologyPathology TV US vs. HS TV US vs. HS BreitkopfBreitkopf et al.et al. 1 of 6 women had 1 of 6 women had intracavitaryintracavitary lesions missed by TV USlesions missed by TV US 74% sensitivity 74% sensitivity
HS and SIS vs. TV US Jansen et al.HS and SIS vs. TV US Jansen et al. HS and SIS equal in diagnosis of HS and SIS equal in diagnosis of intracavitaryintracavitary pathologypathology Significantly greater sensitivity/specificity vs. TV USSignificantly greater sensitivity/specificity vs. TV US
20

19 studies from 1980 through July 200119 studies from 1980 through July 2001 19 studies from 1980 through July 200119 studies from 1980 through July 2001
TVUS higher false negative vs. SH and HS for diagnosis of TVUS higher false negative vs. SH and HS for diagnosis of intrauterine pathologyintrauterine pathology
SH and HS excellent diagnostic accuracy for hyperplasia and SH and HS excellent diagnostic accuracy for hyperplasia and submucosalsubmucosal myomasmyomas
Hysteroscopy was the best for diagnosis of Hysteroscopy was the best for diagnosis of submucosalsubmucosalmyomasmyomas
89 patients 89 patients –– premenopausal TVUS, SIS, HSpremenopausal TVUS, SIS, HS
HS and SIS superior diagnostic accuracy to TVUSHS and SIS superior diagnostic accuracy to TVUS
HS HS best diagnostic accuracybest diagnostic accuracy Especially for endometrial polypsEspecially for endometrial polyps
2004 to 2006
38 patients TVUS, SIS and DH
DH the most accurate diagnostic technique for: Diagnosis of any endometrial pathology
Diagnosis of endometrial diseases – hyperplasia or cancer
Intracavitary mass – polyp or myoma
Structural abnormalities
Hysteroscopy and SIS Hysteroscopy and SIS are BETTER than TV US are BETTER than TV US
at evaluating the uterine cavity.at evaluating the uterine cavity.
HS vs. SISHS vs. SIS
Advantages of HysteroscopyAdvantages of Hysteroscopy Direct visualizationDirect visualization Opportunity for directed biopsyOpportunity for directed biopsy Opportunity for directed biopsyOpportunity for directed biopsy HistopathologyHistopathology
Blind BiopsyBlind Biopsy PolypsPolyps MyomasMyomas HyperplasiaHyperplasia
Sensitivity % 11 13 25
Specificity % 93 100 92
Accuracy % 59 98 80
HysteroscopyHysteroscopy PolypsPolyps MyomasMyomas HyperplasiaHyperplasia
Sensitivity % 89 100 74
Specificity % 93 99 93
Accuracy % 91 99 90
21

HS with Directed Biopsy vs. D & CHS with Directed Biopsy vs. D & CEvaluation of AUBEvaluation of AUB
LofferLoffer 19891989
Evaluation of AUBEvaluation of AUB
HS with Directed Biopsy vs. D & CHS with Directed Biopsy vs. D & C 100% specificity for both100% specificity for both
98% sensitivity for HS vs. 65% for D & C98% sensitivity for HS vs. 65% for D & C
HS with directed biopsy missed 1 HS with directed biopsy missed 1 endometritisendometritis
CLINICAL PRACTICE CLINICAL PRACTICE EVALUATION OF AUB: EVALUATION OF AUB:
Hysteroscopy with possible directedHysteroscopy with possible directedHysteroscopy with possible directed Hysteroscopy with possible directed biopsy or EMBbiopsy or EMB
Overcoming Barriers toOvercoming Barriers toInIn--Office HysteroscopyOffice Hysteroscopy
Surgeon SkillSurgeon Skill StaffStaff
Procedure awarenessProcedure awareness Procedure assistanceProcedure assistance Equipment maintenanceEquipment maintenance Equipment maintenanceEquipment maintenance
Patient ExpectationsPatient Expectations Patient comfortPatient comfort Ease of evaluationEase of evaluation Less overall riskLess overall risk Immediate visual feedbackImmediate visual feedback
Capitol ExpenditureCapitol Expenditure
2.8 procedures / office day2.8 procedures / office day
Evaluation TechniqueEvaluation Technique
Cervical Cervical evaluationevaluation
Identify Identify ccornuornu
E l ti fE l ti f itit Evaluation of Evaluation of cavitycavity Size, contour, septum, polyps, Size, contour, septum, polyps,
myomatamyomata, scaring, scaring
Evaluation of Evaluation of endometriumendometrium
Better cBetter cervical evaluationervical evaluation
Endometrial Endometrial AdenocarcinomaAdenocarcinoma
3401 3401 resectoscopicresectoscopic proceduresprocedures 16 occult, 3 known cancers16 occult, 3 known cancers Standard treatment with hysterectomyStandard treatment with hysterectomy 55--14 year follow14 year follow--upup No change in 5 year survival or longNo change in 5 year survival or long--term followterm follow--upup
22

Submucosal FibroidsSubmucosal FibroidsPreoperative Evaluation ESGEPreoperative Evaluation ESGE
Percent Intramural ExtensionPercent Intramural Extension Type 0 NoneType 0 None Type I < 50%Type I < 50% Type II > 50%Type II > 50% Type II > 50%Type II > 50%
Wamsteker K,Wamsteker K, et al. et al. Transcervical hysteroscopic resection Transcervical hysteroscopic resection
of submucous fibroids for abnormal of submucous fibroids for abnormal uterine bleeding: results regarding uterine bleeding: results regarding the degree of intramural extension. the degree of intramural extension. Obstet GynecolObstet Gynecol 1993;82:7361993;82:736--740. 740.
AnesthesiaAnesthesia
3 mm 3 mm Flexible/RigidFlexible/Rigid Usually not neededUsually not needed
5.5 mm Rigid w/o Dilation5.5 mm Rigid w/o DilationParousParous usually not neededusually not needed ParousParous usually not neededusually not needed
TenaculumTenaculum site localsite local 1% 1% LidocaineLidocaine
5.5 mm Rigid with Dilation5.5 mm Rigid with Dilation TenaculumTenaculum site localsite local ParacervicalParacervical blockblock 1% 1% LidocaineLidocaine
No Cervical PreparationNo Cervical Preparation
See and TreatSee and Treat Cervical dilation usually not neededCervical dilation usually not needed 3 mm flexible hysteroscope3 mm flexible hysteroscope
MisoprostilMisoprostil Cramping and bleedingCramping and bleeding Give narcotic pain medicationGive narcotic pain medication Not useful for menopausal womenNot useful for menopausal women
MisoprostolMisoprostol
Oral/Vaginal 400 Oral/Vaginal 400 μgmμgm 66--8 8 hrhr priorprior
Sublingual 400 Sublingual 400 μgmμgm 22--4 4 hrhr priorprior
InIn--Office EssentialsOffice Essentials Patient is Patient is awakeawake
Keep fluid pressure lowKeep fluid pressure low Remove speculumRemove speculum Minimize movementMinimize movement
ScopeScope--llight ight ccord relationshipord relationship 3030oo lenslens
Communicate with Communicate with patientpatient Position MonitorPosition Monitor
Hysteroscopy EssentialsHysteroscopy EssentialsProcedure StepsProcedure Steps
Lithotomy with boot stirrupsLithotomy with boot stirrups
Manual exam of uterusManual exam of uterus
SpeculumSpeculum PedersonPederson OpenOpen--sidedsided
Clean cervixClean cervix
Place hysteroscopePlace hysteroscope
23

Vaginoscopic HysteroscopyVaginoscopic HysteroscopyProcedureProcedure
Consideration for Consideration for misoprostolmisoprostol
No sNo speculum neededpeculum needed
B diB di ii BetadineBetadine vaginavagina
No No anesthesiaanesthesia
Fill pFill posterior fornix osterior fornix with with salinesaline
3 mm Flexible 3 mm Flexible HysteroscopeHysteroscope
R
Vaginoscopic ViewVaginoscopic View
Retroverted Uterus Anteverted Uterus
Posterior Fornix Posterior Fornix
Mucous/Blood
Recreated from the work of Dr. Martin Farrugia
EquipmentEquipment MonitorMonitor
CameraCamera Camera headCamera head Camera headCamera head ProcessorProcessor Light sourceLight source
TowerTower
Recording DeviceRecording Device
Flexible HysteroscopeFlexible Hysteroscope
EMB ftEMB ft FiberFiber--optic or digitaloptic or digital
Single channel Single channel
3 3 –– 4 mm diameter4 mm diameter
OOoo lens with 240lens with 240oo range of visual fieldrange of visual field
Saline as distention mediumSaline as distention medium
IV tubing/cystoscopy tubing or 60 cc syringeIV tubing/cystoscopy tubing or 60 cc syringe
EMB after EMB after evacuation of evacuation of
saline with saline with syringesyringe
Flexible HysteroscopeFlexible Hysteroscope1.9 to 3 1.9 to 3 mm mm
Diagnostic Rigid Diagnostic Rigid HysteroscopeHysteroscope
EMB after EMB after evacuation of evacuation of
saline with saline with syringesyringe
Office SetOffice Set--UpUpProcedure RoomProcedure Room
24

Office SetOffice Set--UpUpProcedure RoomProcedure Room Supplies and InstrumentsSupplies and Instruments
Supplies and InstrumentsSupplies and Instruments Supplies and InstrumentsSupplies and Instruments
DocumentationDocumentation ReimbursementReimbursement
InIn--Patient (21), OutPatient (21), Out--Patient (22), ASC (24)Patient (22), ASC (24)
58555 Diagnostic Hysteroscopy58555 Diagnostic Hysteroscopy
2012 RVU2012 RVUMedicareMedicareCFCF 34 03734 037
125%125%CF 42 55CF 42 55
No GlobalNo Global20122012
2012 RVU2012 RVU CFCF 34.03734.037 CF 42.55CF 42.55
5.67 $ 192.99 $ 241.24
NonNon--Facility/OfficeFacility/Office (11)(11)
8.56 $ 291.36 $ 364.20
With E/M VisitWith E/M VisitModifier 25Modifier 25
Document HS SeparatelyDocument HS Separately
25
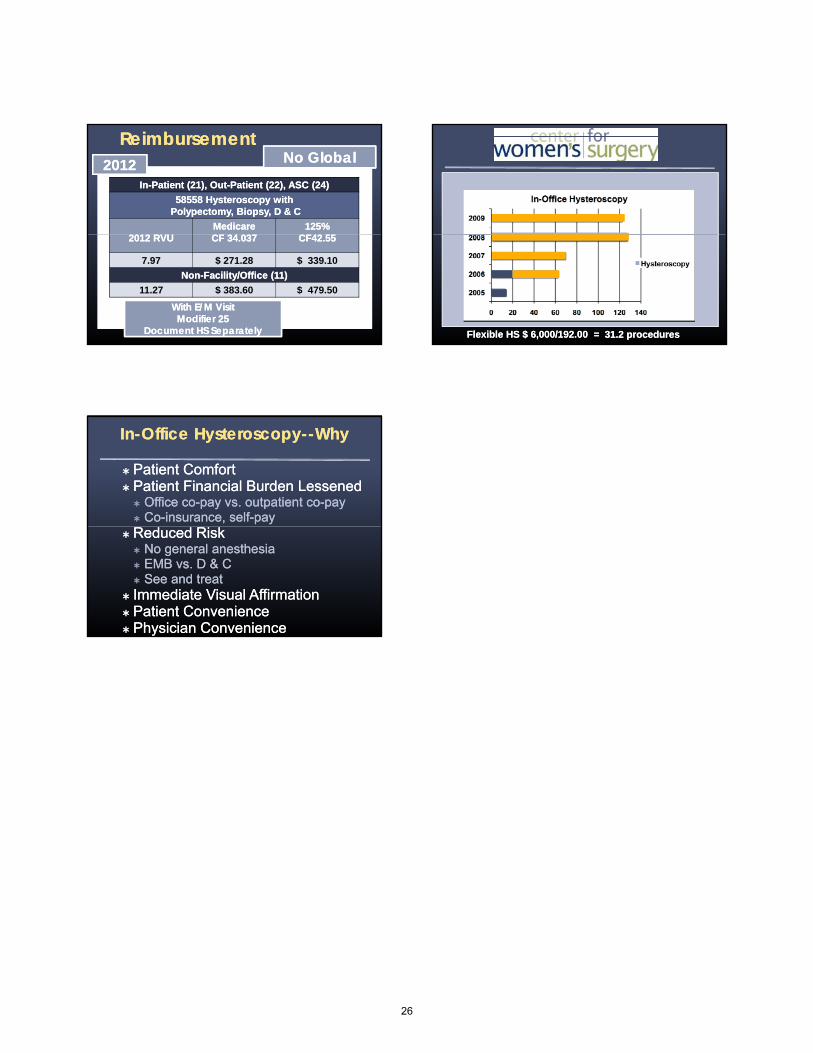
ReimbursementReimbursement
InIn--Patient (21), OutPatient (21), Out--Patient (22), ASC (24)Patient (22), ASC (24)
58558 Hysteroscopy with58558 Hysteroscopy withPolypectomy,Polypectomy, Biopsy, D & CBiopsy, D & C
2012 RVU2012 RVUMedicareMedicareCFCF 34 03734 037
125%125%CF42 55CF42 55
No GlobalNo Global20122012
2012 RVU2012 RVU CFCF 34.037 34.037 CF42.55CF42.55
7.97 $ 271.28 $ 339.10
NonNon--Facility/OfficeFacility/Office (11)(11)
11.27 $ 383.60 $ 479.50
With E/M VisitWith E/M VisitModifier 25Modifier 25
Document HS SeparatelyDocument HS Separately
HS 185
Flexible HS $ 6,000/192.00 = Flexible HS $ 6,000/192.00 = 31.2 procedures31.2 procedures
InIn--Office HysteroscopyOffice Hysteroscopy----WhyWhy
Patient ComfortPatient Comfort Patient Financial Burden LessenedPatient Financial Burden Lessened
Office coOffice co--pay vs. outpatient copay vs. outpatient co--paypay CoCo--insurance, selfinsurance, self--paypay
Reduced RiskReduced Risk No general anesthesiaNo general anesthesia EMB vs. D & CEMB vs. D & C See and treatSee and treat
Immediate Visual AffirmationImmediate Visual Affirmation Patient ConveniencePatient Convenience Physician ConveniencePhysician Convenience
26

Operative Hysteroscopy Operative Hysteroscopy
Amy Amy Garcia, Garcia, MDMD
AAGL/SRS FellowshipAAGL/SRS Fellowship--Trained in MIGTrained in MIG
DirectorDirector, Center for Women, Center for Women’’s Surgerys Surgery
Clinical Assistant Clinical Assistant Professor, University of New MexicoProfessor, University of New MexicoDepartment of Obstetrics and GynecologyDepartment of Obstetrics and Gynecology
Division of Division of UrogynecologyUrogynecology
Albuquerque, New MexicoAlbuquerque, New Mexico
DisclosureDisclosure
Grants/Research Grants/Research Support: HologicSupport: Hologic
Consultant: Conceptus Incorporated, Consultant: Conceptus Incorporated, Ethicon EndoEthicon Endo--Surgery Ethicon Women'sSurgery Ethicon Women'sEthicon EndoEthicon Endo--Surgery, Ethicon Women s Surgery, Ethicon Women s Health & Urology, IOGYN, Minerva Health & Urology, IOGYN, Minerva SurgicalSurgical
Speaker's Bureau: Conceptus Speaker's Bureau: Conceptus IncInc
ObjectivesObjectives
Acquire, setAcquire, set--up and utilize supplies and up and utilize supplies and equipment necessary for procedures in the equipment necessary for procedures in the officeofficeoffice office
Utilize an operative hysteroscope and Utilize an operative hysteroscope and operative instruments in the officeoperative instruments in the office
Discern operative hysteroscopy techniques Discern operative hysteroscopy techniques for infor in--office proceduresoffice procedures
Operative Office HysteroscopyOperative Office Hysteroscopy
MyomectomyMyomectomyUterine SeptumUterine SeptumPolypectomyPolypectomyPolypectomyPolypectomy MechanicalMechanicalScissorsScissorsMorcellatorMorcellator
Bipolar energyBipolar energy
Operative HysteroscopeOperative Hysteroscope
Rigid LensRigid Lens 2.8 2.8 –– 3.2 mm diameter3.2 mm diameter
Continuous Flow SheathContinuous Flow Sheath Continuous Flow SheathContinuous Flow Sheath 5.5 mm diameter5.5 mm diameter
Operative ChannelOperative Channel 3 3 FrFr or 5 or 5 FrFr
00oo , 12, 12oo , 25, 25oo , 30, 30oo
Operative HysteroscopeOperative Hysteroscope
ININ
OUOUTTOUOUTT
27
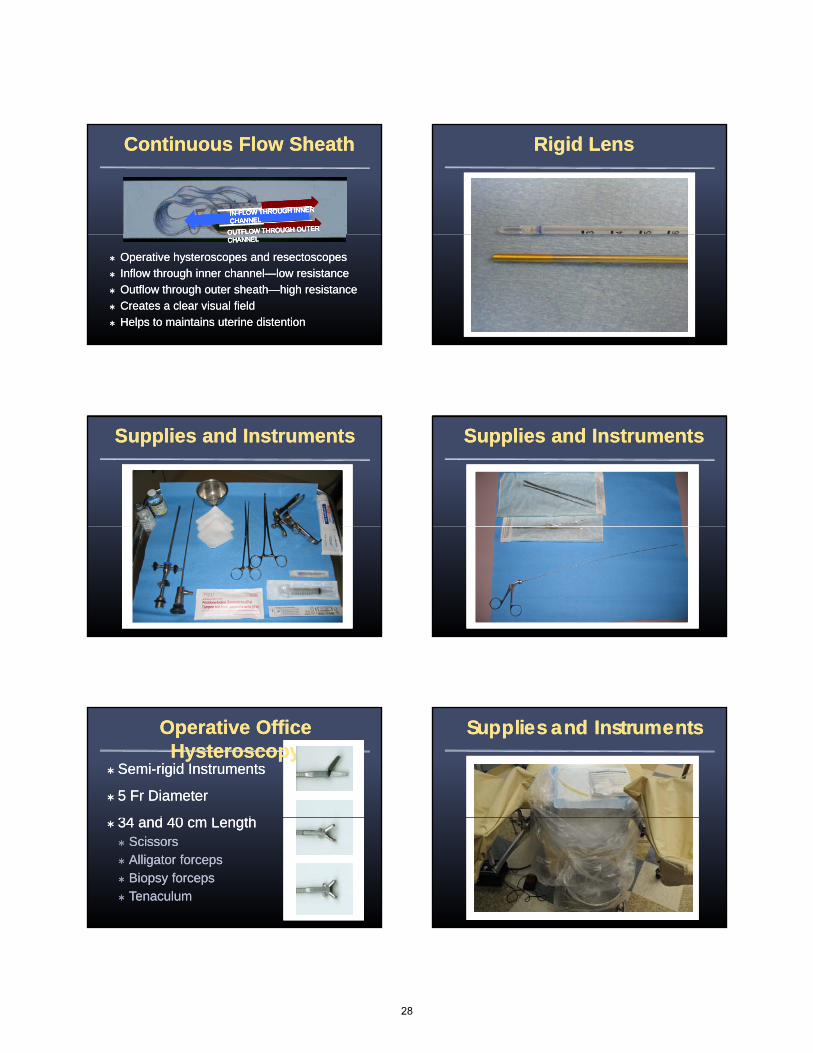
Continuous Flow Sheath Continuous Flow Sheath
Operative Operative hysteroscopeshysteroscopes and and rresectoscopesesectoscopes
Inflow through inner channelInflow through inner channel——low resistancelow resistance
Outflow through outer sheathOutflow through outer sheath——high resistancehigh resistance
Creates a clear visual fieldCreates a clear visual field
Helps to maintains uterine distentionHelps to maintains uterine distention
Rigid LensRigid Lens
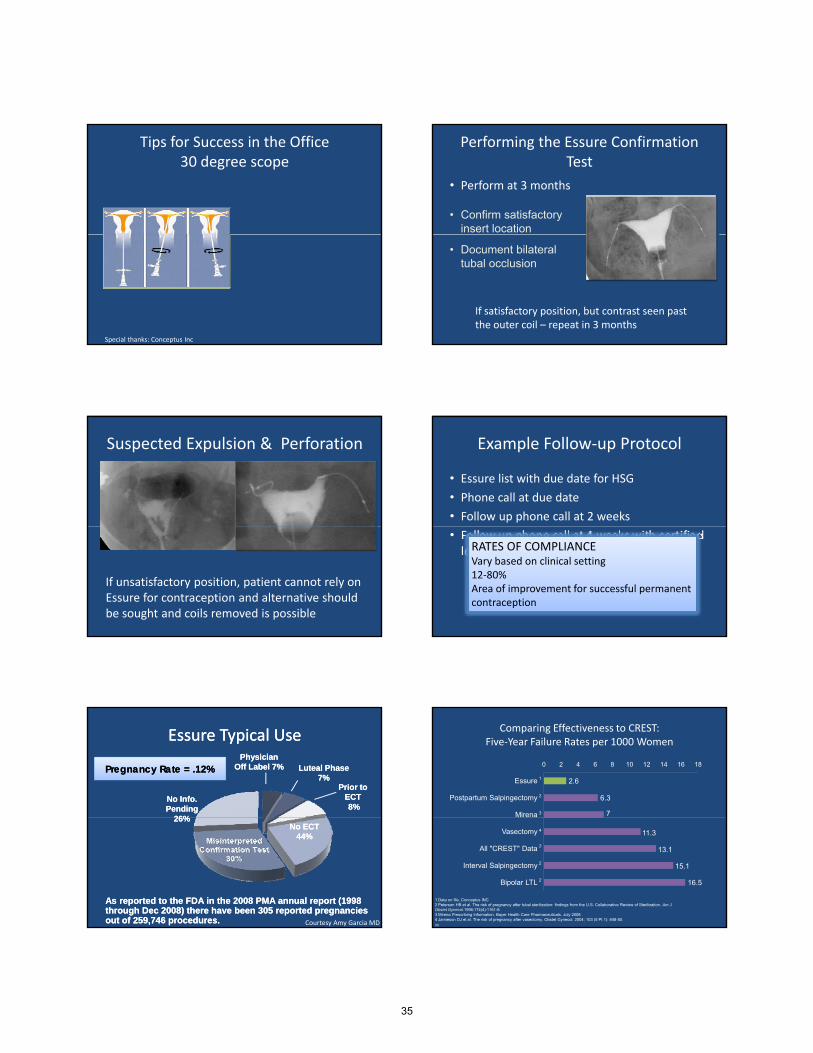
Supplies and InstrumentsSupplies and Instruments Supplies and InstrumentsSupplies and Instruments
Operative Office Operative Office HysteroscopyHysteroscopy
SemiSemi--rigid Instrumentsrigid Instruments
5 5 FrFr DiameterDiameter
34 d 40 L th34 d 40 L th 34 and 40 cm Length34 and 40 cm Length ScissorsScissors Alligator forcepsAlligator forceps Biopsy Biopsy forcepsforceps TenaculumTenaculum
Supplies and InstrumentsSupplies and Instruments
28
Supplies and InstrumentsSupplies and Instruments Risk Factors for PolypsRisk Factors for Polyps
Significance Significance associationassociation AgeAge MenopauseMenopause HTNHTN ObesityObesity
Only AGE keeps statistical significance Only AGE keeps statistical significance in in univariableunivariable analysisanalysis
Endometrial Polyps and HyperplasiaEndometrial Polyps and Hyperplasia
International Journal of Gynecological
Increased Increased risk risk of of atypical atypical hhyperplasia yperplasia in in random random ddirected biopsiesirected biopsies
International Journal of Gynecological Pathology 28;522-528. 2010
DocumentationDocumentation
ReimbursementReimbursement
InIn--Patient (21), OutPatient (21), Out--Patient (22), ASC (24)Patient (22), ASC (24)
58558 Hysteroscopy with58558 Hysteroscopy withPolypectomy,Polypectomy, Biopsy, D & CBiopsy, D & C
2012 RVU2012 RVUMedicareMedicareCFCF 34 03734 037
125%125%CF42 55CF42 55
No GlobalNo Global20122012
2012 RVU2012 RVU CFCF 34.037 34.037 CF42.55CF42.55
7.97 $ 271.28 $ 339.10
NonNon--Facility/OfficeFacility/Office (11)(11)
11.27 $ 383.60 $ 479.50
With E/M VisitWith E/M VisitModifier 25Modifier 25
Document HS SeparatelyDocument HS Separately
ReimbursementReimbursement
InIn--Patient (21), OutPatient (21), Out--Patient (22), ASC (24)Patient (22), ASC (24)
58562 Hysteroscopy with58562 Hysteroscopy withRemoval Foreign BodyRemoval Foreign Body
2012 RVU2012 RVUMedicareMedicareCFCF 34 03734 037
125%125%CF 42 55CF 42 55
No GlobalNo Global20122012
2012 RVU2012 RVU CFCF 34.03734.037 CF 42.55CF 42.55
8.62 $ 294.77 $ 368.46
NonNon--Facility/OfficeFacility/Office (11)(11)
11.72 $ 398.92 $ 498.65
With E/M VisitWith E/M VisitModifier 25Modifier 25
Document HS SeparatelyDocument HS Separately
29

InIn--Office HysteroscopyOffice Hysteroscopy----WhyWhy
Patient ComfortPatient Comfort Patient Financial Burden LessenedPatient Financial Burden Lessened
Office coOffice co--pay vs. outpatient copay vs. outpatient co--paypay CoCo--insurance, selfinsurance, self--paypay
Reduced RiskReduced Risk Reduced RiskReduced Risk No general anesthesiaNo general anesthesia EMB vs. D & CEMB vs. D & C See and treatSee and treat
Immediate Visual AffirmationImmediate Visual Affirmation Patient ConveniencePatient Convenience Physician ConveniencePhysician Convenience
30

Hysteroscopic Sterilization: Changing the Paradigm of Permanent Contraception
Isabel Green, MD
Johns Hopkins University
Disclosures
• I have no financial relationships to disclose.
Objectives
• Anticipate needed equipment and supplies for successful implementation of office sterilization
• Demonstrate proper patient selection &• Demonstrate proper patient selection & counseling for office hysteroscopic sterilization
• Demonstrate proper technique of the Essureprocedure and confirmation test
• Establish protocols for office sterilization
Hysteroscopic Sterilization: Essure• Hysteroscopic
placement of
radiopaque inserts in
the proximal portion of
h f ll bthe fallopian tube
• Tissue ingrowth occurs
through the insert
creating natural barrier
4
Outer Coilmaintains placement
during ingrowth
Inner CoilPET fibers create
3cm occlusion
Special thanks: Conceptus Inc
The Essure insert Design
• Device Length: ~3.85 cm
• PET Fiber Length: ~1.75 cm
• Expanded Outer Diameter: 1.5 – 2.0 mm
• Inserts are visible by X-Ray, Ultrasound, MRI and CT Scan
PET Fiber Dynamic Expanding Super elastic Nitinol Outer CoilStainless Steel
Innercoil
Permanent Contraception
re∙li∙able adj \ri‐ˈlī‐ə‐bəl\1: suitable or fit to be relied on: dependable
SAFE
&
CONVENIENT
31

Essure Tubal Occlusion Results*
% occluded at three months
96.5%
% occluded at six% occluded at six months
100%**
7
*Essure Instructions for Use, CONCEPTUS**Tubal patency was demonstrated in 16 women at the 3-month HSG, but all 16 women were shown to have tubal occlusion at a repeat HSG performed 6-7 months after Essure placement7
Adverse EventsPhase II Trial
ESS-005Pivotal Trial
ESS-005
2009 Commercial Setting
Reported Rate1
Perforations 3.4%2 1.1% 0.177%
Expulsions 0.5% 2.9%3 0.043%
Initial tubal patency4 3.5% 3.5% 0.097%
Other unsatisfactory location
0.5% 0.6% NA
1 Based on Conceptus’ reporting system , MAUDE database and number of devices sold in 2009.2 A support catheter was utilized in this trial and resulted in a higher incidence of perforation. This catheter is not on the current design.3 3/14 devices were placed proximally. Current labeling recommends devices with ≥18 coils visible be removed and replaced. 9/14 patients opted to
have another device placed and all were successful.4 In both clinical trials, all patients were occluded at HSG 6-7 months post-procedure5 Povedano et al. BJOG 20128
COMPLICATIONSVasovagal episodes 2‐5%
Why transition to the office?
The case of Mrs. Jones….
39 ld l i h l d39 year old, multiparous, has completed her family, and after counseling desires hysteroscopic tubal occlusion.
Mrs. Jones in the office….
• Patients:– Familiar setting for patients
– Avoids hospital hassle
– Can watch procedure if desired
– “have a procedure,” not a surgery
• Surgeon:– Time‐saving
– Consistent staffing
– Higher reimbursement
Essure in the Office Of 209 women…70% experienced pain less than or equal to menses
2.53.5
2
4
6
8
10
Levie M et al. Fertil Steril 2010Arjona et al. Fertil Steril 2008Sinha et al. BJOG 2007.
0
Essure Procedure Menses
Of 1603 women…..97% would recommend the procedure to others52% state the most valuable aspect was avoidance of the operating room
Equipment
HIGH COST
• Hysteroscope– Operative
• Camera
Li ht• Light source
• Monitor
• Mobile cart
• Printer
• Recorder
• Disinfection station
32

Equipment
Low cost:• Speculum• Stirrups• Tenaculum• Paracervical block• Paracervical block• Dilators• Distending medium• Tubing• Pressure bag• Outflow pouch• Channel seal
Priceless: reliable well‐trained staff
Equipment Cost as a Barrier
• Multiple indications
• Shared equipment
• Equipment programs & trials
• Reimbursement
ICDICD‐‐9 9 V25.2V25.2Interruption of fallopian tubes or vas deferensInterruption of fallopian tubes or vas deferens
CPTCPT5856558565Bilateral fallopian tube Bilateral fallopian tube cannulationcannulation to induce to induce occlusion by placement of permanent implantsocclusion by placement of permanent implants
ReimbursementReimbursement
InIn--Patient (21), OutPatient (21), Out--Patient (22), ASC (24)Patient (22), ASC (24)
Hysteroscopic SterilizationHysteroscopic Sterilization5856558565
MedicareMedicare 125%125%
90 Day Global90 Day Global20122012
2012 RVU2012 RVUMedicareMedicareCFCF 34.03734.037
125%125%CF 42.55CF 42.55
12.96 $ 441.13 $ 551.41
NonNon--Facility/OfficeFacility/Office (11)(11)
56.82 $ 1,934.02 $ 2,417.53
Essure Device Cost $1,350.00Essure Device Cost $1,350.00Courtesy of Amy Garcia MD
Essure Candidates for the Office
Woman who….
• Qualifies for permanent sterilization
• Has no contraindications to hysteroscopicili isterilization
• Good candidate for an office procedure
• Understands follow up after Essure procedure
Contraindications*
• Uncertain about her desire to end her fertility
• Can have only 1 insert placed
• Has previously undergone a tubal ligation
• Pregnant or suspected pregnancy
• Delivery or termination less than 6 weeks prior
• Active or recent upper or lower pelvic infection
• Known allergy to contrast media**
• Should not be used concomitantly with ablation procedures
• Discouraged in women undergoing immunosuppressive therapy
* See complete Instructions for Use in Essure packaging** Non-iodine containing contrast medias are available
AnalgesiaExample Agents
• LOCAL
– Paracervical Block
– Intrauterine lidocaine
NSAIDS• NSAIDS
– Motrin, Toradol, Mefenamic Acid
• Narcotic
– IV tramadol, Oxycodone
• Anxiolytic
Kaneshiro et al. Cochrane Database Syst Rev 2012Chudnoff et al. Obstet Gynecol 2010
33

Reducing pain in the office
RCT 1% RCT 1% LidocaineLidocaine vsvs Saline for PCBSaline for PCBSignificant Lower Pain ScoresSignificant Lower Pain Scores•• TenaculumTenaculum placementplacement•• Traversing external cervical Traversing external cervical osos•• Traversing internal cervical Traversing internal cervical osos
No Difference for Device PlacementNo Difference for Device Placement
Chudnoff et al Obstet Gynecol 2010Courtesy Amy Garcia MD
Example Protocol
Preprocedure:
NSAIDS
Motrin 600 mg day prior
Toradol 30 mg IM 30 min prior
Anxiolytic
IDEAL PROTOCOL HAS YET TO BE DETERMINEDLiterature doesn’t support single protocolAnxiolytic
Xanax 0.5 mg po 30 min prior as needed
Paracervical block
1% lidocaine, 10cc total, wait time 10 min
Postprocedure: NSAIDS
Literature doesn t support single protocol
Ess305 System
Ess305 System consists of
(1) Delivery System; (2) Insert; and (3) DryFlow Introducer
1.
2.
3.
Special thanks: Conceptus Inc
Procedure Steps
2. Confirm position = gold band at ostium + green catheter in view!
3. Deploy device = push button, wheel back button toward you to hard stop again while maintaining stabilization
4. Confirm placement and record in notes
1. Insert catheter to black marker – stabilize Essure handle to hysteroscope –
wheel button toward you to hard stop
Special thanks: Conceptus Inc
Essure Procedure
Preprocedure checklist & HCGPremedicationsModerate lithotomyBimanual examSpeculumClean cervixSingle tooth tenaculumParacervical block – pause!Place Hysteroscope ‐hydrodilateDilate if neededDiagnostic hysteroscopy – identify both ostia!Place devicesPhotographAssess hemostasis at cervixDocument:
FluidsAnatomy# of coilsPain scale
Tips for Success in the Office
• Contraception before and after
• Scheduling in early proliferative phase
– Improve visualization
– Decrease risk of pregnancy
– Hormonal meds favorable
• Avoid unnecessary instrumentation
– Decrease cost and clutter
– Remove speculum for comfort
– Vaginoscopy
• Maintain back up equipment/kits
• Know your learner and use visual imagery
34
Tips for Success in the Office30 degree scope
Special thanks: Conceptus Inc
Performing the Essure Confirmation Test
• Perform at 3 months
• Confirm satisfactoryinsert location
• Document bilateral tubal occlusion
If satisfactory position, but contrast seen past the outer coil – repeat in 3 months
Suspected Expulsion & Perforation
If unsatisfactory position, patient cannot rely on Essure for contraception and alternative should be sought and coils removed is possible
Example Follow‐up Protocol
• Essure list with due date for HSG
• Phone call at due date
• Follow up phone call at 2 weeks
• Follow up phone call at 4 weeks with certified letterRATES OF COMPLIANCEVary based on clinical setting12‐80%Area of improvement for successful permanentcontraception
EssureEssure Typical UseTypical Use
No Info.No Info.PendingPending
26%26%
Prior to Prior to ECTECT8%8%
Luteal Phase Luteal Phase 7%7%
PhysicianPhysicianOff Label 7%Off Label 7%Pregnancy Rate = .12%Pregnancy Rate = .12%
No ECTNo ECT44%44%
26%26%
As reported to the FDA in the 2008 PMA annual report (1998 As reported to the FDA in the 2008 PMA annual report (1998 through Dec 2008) there have been 305 reported pregnancies through Dec 2008) there have been 305 reported pregnancies out of 259,746 procedures. out of 259,746 procedures. Courtesy Amy Garcia MD
Comparing Effectiveness to CREST: Five‐Year Failure Rates per 1000 Women
2.6
6.3
7
0 2 4 6 8 10 12 14 16 18
Essure
Postpartum Salpingectomy
Mirena
1
2
3
11.3
13.1
15.1
16.5
Vasectomy
All "CREST" Data
Interval Salpingectomy
Bipolar LTL
1 Data on file, Conceptus INC2 Peterson HB et al. The risk of pregnancy after tubal sterilization: findings from the U.S. Collaborative Review of Sterilization. Am J Obstet Gynecol.1996;174(4):1161-8.3 Mirena Prescribing Information. Bayer Health Care Pharmaceuticals. July 20084 Jamieson DJ et al. The risk of pregnancy after vasectomy. Obstet Gynecol. 2004; 103 (5 Pt 1): 848-50.30
4
2
2
2
35
Tips for Success in the Office
• Invest in your team– Vocal anesthesia
– Set the atmosphere
– Practice safety drills
• Involve the patient– Use the monitor
• Write a protocol, circulate and post it in the office
Thank you
References
• Sinha D, Kalathy V, Gupta JK, Clark TJ. The feasibility, success and patient satisfaction associated with outpatient hysteroscopic sterilisation. BJOG. 2007 Jun;114(6):676‐83.
• Miño M, Cordón J, Povedano B, Pelegrin B, Castelo‐Branco C.Satisfaction and tolerance with office hysteroscopic tubal sterilization.Arjona JE, Fertil Steril. 2008 Oct;90(4):1182‐6. Epub 2008 Jan 16.
• Shavell VI, Abdallah ME, Diamond MP, Kmak DC, Berman JM. Post‐Essure hysterosalpingography compliance in a clinic population.J Minim Invasive Gynecol. 2008 Jul‐Aug;15(4):431‐4. Epub 2008 Apr 28.
• Connor VF. Essure: a review six years later.J Minim Invasive Gynecol. 2009 May‐Jun;16(3):282‐90. Review.
• .Povedano B, Arjona JE, Velasco E, Monserrat JA, Lorente J, Castelo‐Branco C. Complications of hysteroscopic Essure(®) sterilisation: report on 4306 procedures performed in a single centreBJOG. 2012 Jun;119(7):795‐9. doi: 10.1111/j.1471‐0528.2012.03292.x. Epub 2012 Feb 23.
• .Chudnoff S, Einstein M, Levie M. Paracervical block efficacy in office hysteroscopic sterilization: a randomized controlled trialObstet Gynecol. 2010 Jan;115(1):26‐34Jan;115(1):26 34.
• .Levie M, Chudnoff SG. A comparison of novice and experienced physicians performing hysteroscopic sterilization: an analysis of an FDA‐mandated trialFertil Steril. 2011 Sep;96(3):643‐648.e1. Epub 2011 Jul 23.
• Levie M, Weiss G, Kaiser B, Daif J, Chudnoff SG. Analysis of pain and satisfaction with office‐based hysteroscopic sterilization.Fertil Steril. 2010 Sep;94(4):1189‐94. Epub 2009 Aug 14.
• Finer LB and Zolna MR, Unintended pregnancy in the United States: incidence and disparities, 2006, Contraception, 2011, 84(5):478–485.
• ACOG 2011 Women’s Health Stats & Facts Derived from 2010 CDC report
• Peterson HB et al. The risk of pregnancy after tubal sterilization: findings from the U.S. Collaborative Review of Sterilization. Am J ObstetGynecol.1996;174(4):1161-8.
• Mirena Prescribing Information. Bayer Health Care Pharmaceuticals. July 2008
• Jamieson DJ et al. The risk of pregnancy after vasectomy. Obstet Gynecol. 2004; 103 (5 Pt 1): 848-50.
• Data on file Conceptus Inc
• IFU insert Essure
36
Hysteroscopic Hysteroscopic MorcellatorsMorcellators::What’s on the horizon?What’s on the horizon?
Andrew I. Brill MDAndrew I. Brill MDAndrew I. Brill MDAndrew I. Brill MD
Director, Minimally Invasive GynecologyDirector, Minimally Invasive Gynecology
California Pacific Medical CenterCalifornia Pacific Medical Center
San Francisco, CASan Francisco, CA
DisclosureDisclosure
Consultant: Karl Storz EndoscopyConsultant: Karl Storz Endoscopy--America, Ethicon EndoAmerica, Ethicon Endo--Surgery, Surgery, Conceptus Inc., CooperSurgicalConceptus Inc., CooperSurgical
Speaker's Bureau: Karl Storz Speaker's Bureau: Karl Storz EndoscopyEndoscopy--America, Ethicon EndoAmerica, Ethicon Endo--Surgery, Conceptus Inc., Surgery, Conceptus Inc., CooperSurgicalCooperSurgical
Submucosal FibroidsSubmucosal Fibroids Clinical Indications for Clinical Indications for Hysteroscopic MyomectomyHysteroscopic Myomectomy
Molecular Causal RelationshipMolecular Causal Relationship Rackow BW, Taylor HSRackow BW, Taylor HS
Submucosal uterine leiomyomas have a global effect Submucosal uterine leiomyomas have a global effect
InfertilityInfertility
Submucosal uterine leiomyomas have a global effect Submucosal uterine leiomyomas have a global effect on molecular determinants of endometrial receptivity. on molecular determinants of endometrial receptivity. Fertil SterilFertil Steril. 2010;93(6):2027. 2010;93(6):2027--20342034
Improved Fertility After MyomectomyImproved Fertility After Myomectomy Pritts EA, Parker WH, Olive DL Pritts EA, Parker WH, Olive DL
Fibroids and Infertility: An updated systematic review of Fibroids and Infertility: An updated systematic review of the evidence. the evidence. Fertil SterilFertil Steril. 2009;91(4):1215. 2009;91(4):1215--12231223
Clinical Indications for Clinical Indications for Hysteroscopic MyomectomyHysteroscopic Myomectomy
Improved Pregnancy RatesImproved Pregnancy Rates Shokeir T, etal.Shokeir T, etal.
Submucosal myomas and their implications in the pregnancy rates of patients Submucosal myomas and their implications in the pregnancy rates of patients with otherwise unexplained primary infertility undergoing hysteroscopic with otherwise unexplained primary infertility undergoing hysteroscopic
InfertilityInfertility
myomectomy: a randomized matched control study. myomectomy: a randomized matched control study. Fertil SterilFertil Steril. . 2010;94(2):7242010;94(2):724--729729
215 women infertility longer than 12 months215 women infertility longer than 12 months Fibroids classified by US with ESGE classificationFibroids classified by US with ESGE classification
ResultsResults Myomectomy patients twice as likely as control to become Myomectomy patients twice as likely as control to become
pregnant (RR = 2.1; 95% CI = 1.59pregnant (RR = 2.1; 95% CI = 1.59--2.9)2.9) Women with type 0 and type 1 myomas removed had Women with type 0 and type 1 myomas removed had
significantly higher pregnancy rates than control (p < .001)significantly higher pregnancy rates than control (p < .001) No statistically significant difference in the type ll groupsNo statistically significant difference in the type ll groups
Clinical Indications for Clinical Indications for Hysteroscopic MyomectomyHysteroscopic Myomectomy
Genetic Genetic –– Molecular LevelMolecular Level Stewart EA, Nowak RAStewart EA, Nowak RA
MyomaMyoma--related bleeding: a classic hypothesis updated for the molecular related bleeding: a classic hypothesis updated for the molecular era. era. Human Repro UpdateHuman Repro Update 1996;2:2951996;2:295--306306
Laughlin SK Stewart EALaughlin SK Stewart EA
Abnormal Uterine BleedingAbnormal Uterine Bleeding
Laughlin SK, Stewart EALaughlin SK, Stewart EA Uterine Leiomyomas. Individualizing the Approach to a Heterogeneous Uterine Leiomyomas. Individualizing the Approach to a Heterogeneous
Condition. Condition. Obstet GynecolObstet Gynecol 2011;117:3962011;117:396--403403
Improved Bleeding after MyomectomyImproved Bleeding after Myomectomy Loffer FDLoffer FD
Improving results of hysteroscopic submucosal myomecomy for Improving results of hysteroscopic submucosal myomecomy for menorrhagia by concomitant endometrial ablation. menorrhagia by concomitant endometrial ablation. J Minim Invasive J Minim Invasive GynecolGynecol 2005;12:2542005;12:254--260260
Emanuel MHEmanuel MH LongLong--term results of hysteroscopic myomectomy for abnormal uterine term results of hysteroscopic myomectomy for abnormal uterine
bleeding. bleeding. Obstet Gynecol Obstet Gynecol 1999;93:7431999;93:743--748748
37

SubmucosalSubmucosal FibroidsFibroidsPrePre--Operative Decision MakingOperative Decision Making
PrePre--operative Assessment operative Assessment of Submucosal Myomas is of Submucosal Myomas is of Submucosal Myomas is of Submucosal Myomas is
Essential!Essential!
Submucosal FibroidsSubmucosal FibroidsPreoperative Evaluation Preoperative Evaluation
European Society for Gynaecological Endoscopy European Society for Gynaecological Endoscopy (ESGE)(ESGE)
Percent Intramural ExtensionPercent Intramural Extension Type 0 NoneType 0 None Type I < 50%Type I < 50% Type II > 50%Type II > 50%
Wamsteker K,Wamsteker K, et al. et al. Transcervical hysteroscopic resection Transcervical hysteroscopic resection
of submucous fibroids for abnormal of submucous fibroids for abnormal uterine bleeding: results regarding uterine bleeding: results regarding the degree of intramural extension. the degree of intramural extension. Obstet GynecolObstet Gynecol 1993;82:7361993;82:736--740. 740.
Hysteroscopic MyomectomyHysteroscopic Myomectomy
Type 0 Type I Type II Total
No. Patients 73 97 108 278
No. 73 102 158 333
Wamsteker K, 1993Wamsteker K, 1993
No. Procedures 73 102 158 333
Complete Resection
N = 73 100%
N = 95 98%
N = 103 95%
N = 27197%
Repeat Procedures - 5% 40% 17%
Mean Fluid Intravasation cc
437 971 1642 1110
SubmucosalSubmucosal FibroidsFibroidsPreoperative EvaluationPreoperative Evaluation
Type II Hysteroscopic MyomectomyType II Hysteroscopic Myomectomy Increased risk of:Increased risk of: Excessive fluid absorptionExcessive fluid absorption
El t l t b liti ith El t l t b liti ith l t l t dil t l t di
Wamsteker K, 1993Wamsteker K, 1993
Electrolyte abnormalities with nonElectrolyte abnormalities with non--electrolyte mediaelectrolyte media Excessive bleedingExcessive bleeding Incomplete resection Incomplete resection Need for additional procedureNeed for additional procedure Increased operative timeIncreased operative time
Even with expert Even with expert hysteroscopichysteroscopic surgeonssurgeons
SubmucosalSubmucosal FibroidsFibroidsPreoperative Evaluation New ClassificationPreoperative Evaluation New Classification
LasmarLasmar RB,RB, et al. et al.
SubmucousSubmucous myomasmyomas: A new: A newi li l l ifi ti t l t th l ifi ti t l t th presurgicalpresurgical classification to evaluate the classification to evaluate the
viability of viability of hysteroscopichysteroscopic surgical surgical treatmenttreatment——Preliminary report. Preliminary report.
J Minim Invasive J Minim Invasive GynecolGynecol 2005;12:3082005;12:308--311. 311.
38
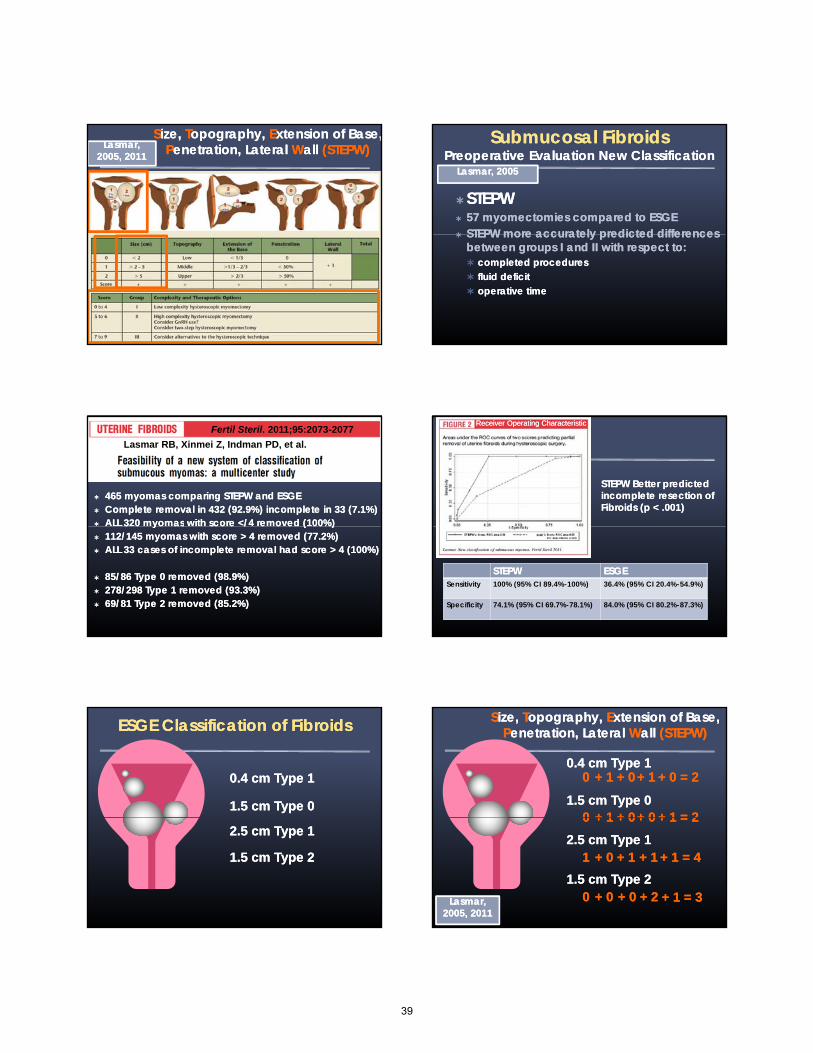
SSize, ize, TTopography, opography, EExtension of Base,xtension of Base,PPenetration, Lateral enetration, Lateral WWall all (STEPW)(STEPW)L L Lasmar, Lasmar,
2005, 20112005, 2011SubmucosalSubmucosal FibroidsFibroids
Preoperative Evaluation New ClassificationPreoperative Evaluation New Classification
STEPWSTEPW 57 myomectomies compared to ESGE57 myomectomies compared to ESGE STEPW more accurately predicted differences STEPW more accurately predicted differences
Lasmar, 2005Lasmar, 2005
STEPW more accurately predicted differences STEPW more accurately predicted differences between groups I and II with respect to:between groups I and II with respect to: completed procedurescompleted procedures fluid deficit fluid deficit operative time operative time
465 465 myomasmyomas comparing STEPW and ESGEcomparing STEPW and ESGE Complete removal in 432 (92.9%) incomplete in 33 (7.1%)Complete removal in 432 (92.9%) incomplete in 33 (7.1%) ALL 320 ALL 320 myomasmyomas with score </4 removed (100%)with score </4 removed (100%)
Fertil Steril. 2011;95:2073-2077
Lasmar RB, Xinmei Z, Indman PD, et al.
3 0 3 0 yo asyo as sco e / e o ed ( 00%) sco e / e o ed ( 00%) 112/145 112/145 myomasmyomas with score with score > 4 > 4 removed (77.2%)removed (77.2%) ALL 33 cases of incomplete removal had score ALL 33 cases of incomplete removal had score > 4 > 4 (100%)(100%)
85/86 Type 0 removed (98.9%)85/86 Type 0 removed (98.9%) 278/298 Type 1 removed (93.3%)278/298 Type 1 removed (93.3%) 69/81 Type 2 removed (85.2%)69/81 Type 2 removed (85.2%)
STEPW Better predicted STEPW Better predicted incomplete resection ofincomplete resection ofFibroids (p < .001)Fibroids (p < .001)
Receiver Operating CharacteristicReceiver Operating Characteristic
STEPWSTEPW ESGEESGESensitivity 100% (95% CI 89.4%-100%) 36.4% (95% CI 20.4%-54.9%)
Specificity 74.1% (95% CI 69.7%-78.1%) 84.0% (95% CI 80.2%-87.3%)
ESGE Classification of FibroidsESGE Classification of Fibroids
0.4 cm Type 10.4 cm Type 1
1.5 cm Type 01.5 cm Type 0
2.5 cm Type 12.5 cm Type 1
1.5 cm Type 21.5 cm Type 2
0.4 cm Type 10.4 cm Type 1
1.5 cm Type 01.5 cm Type 0
0 0
00
+ 1 + 1
+ 1+ 1
+ 0 + 0
+ 0+ 0
+ 1 + 1
+ 0+ 0
SSize, ize, TTopography, opography, EExtension of Base, xtension of Base, PPenetration, Lateral enetration, Lateral WWall all (STEPW)(STEPW)
+ 0 = 2 + 0 = 2
+ 1 = 2+ 1 = 2
2.5 cm Type 12.5 cm Type 1
1.5 cm Type 21.5 cm Type 2
0 0
1 1
0 0
+ 1+ 1
+ 0 + 0
+ 0 + 0
+ 0 + 0
+ 1 + 1
+ 0 + 0
+ 0 + 0
+ 1 + 1
+ 2 + 2 LasmarLasmar, , 20052005, 2011, 2011
+ 1 = 2 + 1 = 2
+ 1 = 4+ 1 = 4
+ 1 = 3 + 1 = 3
39

STEPWSTEPWLasmarLasmar, ,
20052005, 2011, 2011
Prediction of complete removal 100% Prediction of complete removal 100%
Submucosal FibroidsSubmucosal FibroidsVaporizing ElectrodeVaporizing Electrode
BIPOLARBIPOLARBIPOLARBIPOLARSalineSaline
ResectoscopyResectoscopy
Requires Skilled SurgeonRequires Skilled Surgeon
Risk of:Risk of: Fluid overload (nonFluid overload (non electrolyte fluid)electrolyte fluid) Fluid overload (nonFluid overload (non--electrolyte fluid)electrolyte fluid) Multiple instrumentations of the uterusMultiple instrumentations of the uterus Uterine perforation, air embolus, false passagewayUterine perforation, air embolus, false passageway
Injury related to electrical energy sourceInjury related to electrical energy source
Generates Visually Obscuring Tissue Generates Visually Obscuring Tissue PiecesPieces NonNon--vaporizing or automatic tissue removingvaporizing or automatic tissue removing
Hysteroscopic ResectionHysteroscopic ResectionSurgical TrainingSurgical Training
Miller CEMiller CE Training in minimally Invasive surgeryTraining in minimally Invasive surgery——you say you want a you say you want a
revolution. revolution. J Minim Invasive GynecolJ Minim Invasive Gynecol. 2009;16(2):113. 2009;16(2):113––120.120.
The Typical ObGyn resident graduating The Typical ObGyn resident graduating b t 2002 d 2007 h d f d b t 2002 d 2007 h d f d between 2002 and 2007 had performed between 2002 and 2007 had performed a median of only 40 operative a median of only 40 operative hysteroscopic procedures hysteroscopic procedures
10 Operative 10 Operative HysteroscopicHysteroscopicProcedures Procedures Per Per YYearear!!
Clinical Indications for Clinical Indications for Hysteroscopic PolypectomyHysteroscopic Polypectomy
AUBAUB Nathani F, Clark TJ. Nathani F, Clark TJ.
Uterine polypectomy in the management of abnormal uterine bleeding: A Uterine polypectomy in the management of abnormal uterine bleeding: A systematic review. systematic review. J Minim Invasive Gynecol J Minim Invasive Gynecol 2006;13:2602006;13:260--268.268.
InfertilityInfertility Rackow etal.Rackow etal.
Endometrial polyps affect uterine receptivity. Endometrial polyps affect uterine receptivity. Fertil SterilFertil Steril 2011 (In2011 (In--Press).Press).
Afifi etal.Afifi etal. Management of endometrial polyps in subfertile women: a systematic Management of endometrial polyps in subfertile women: a systematic
review. review. Eur J Obstet Gynecol Reprod BiolEur J Obstet Gynecol Reprod Biol 2010;151:1172010;151:117--121.121.
HysteroscopicHysteroscopic MorcellatorMorcellator
40
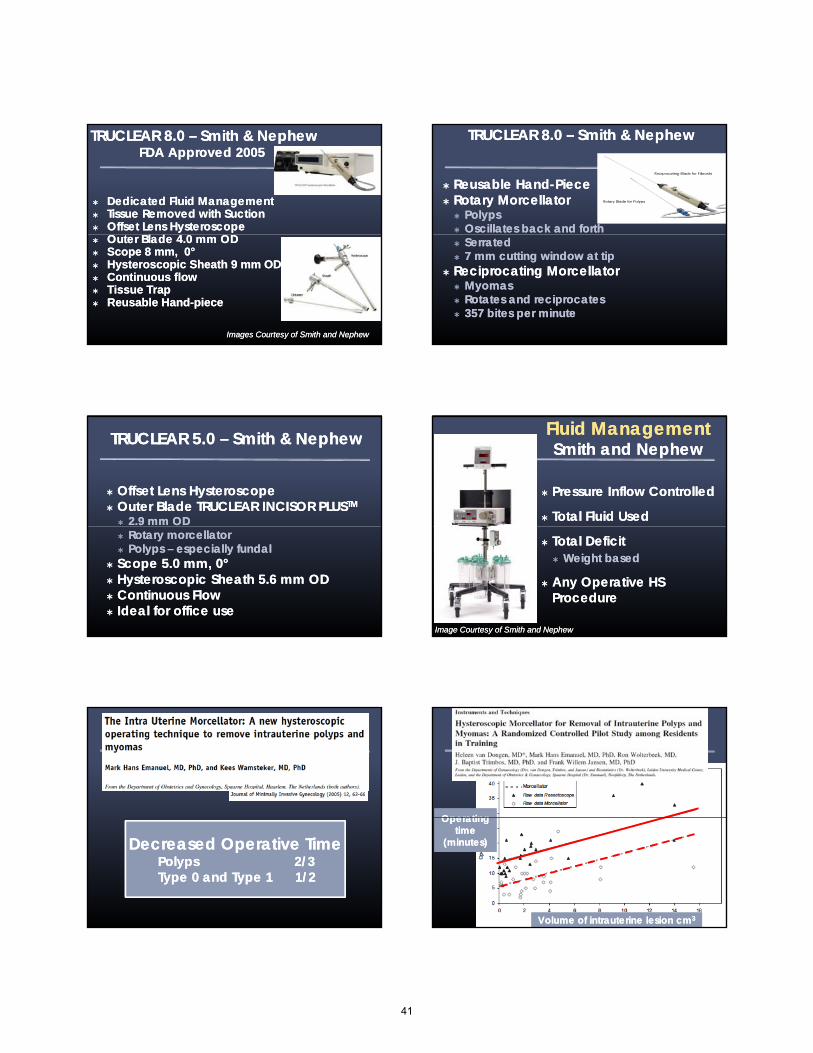
TRUCLEAR TRUCLEAR 8.0 8.0 –– Smith & Smith & Nephew Nephew FDA FDA Approved 2005Approved 2005
Dedicated Fluid ManagementDedicated Fluid Management Tissue Removed with SuctionTissue Removed with Suction Offset Lens Offset Lens HysteroscopeHysteroscope
O l d 4 0 OO l d 4 0 O Outer Blade 4.0 mm ODOuter Blade 4.0 mm OD Scope 8 mm, 0Scope 8 mm, 0°° HysteroscopicHysteroscopic Sheath 9 mm ODSheath 9 mm OD Continuous flowContinuous flow Tissue TrapTissue Trap Reusable HandReusable Hand--piece piece
Images Courtesy of Smith and NephewImages Courtesy of Smith and Nephew
TRUCLEARTRUCLEAR 8.0 8.0 –– Smith & NephewSmith & Nephew
Reusable HandReusable Hand--PiecePiece Rotary Rotary MorcellatorMorcellator
PolypsPolyps Oscillates back and forthOscillates back and forth SerratedSerrated 7 mm cutting 7 mm cutting window at tipwindow at tip
Reciprocating Reciprocating MorcellatorMorcellator MyomasMyomas Rotates and reciprocatesRotates and reciprocates 357 357 bites per bites per minuteminute
TRUCLEAR TRUCLEAR 5.0 5.0 –– Smith & Smith & NephewNephew
Offset Offset Lens Lens HysteroscopeHysteroscope Outer Blade TRUCLEAR INCISOR PLUSOuter Blade TRUCLEAR INCISOR PLUSTMTM
2.9 mm 2.9 mm ODOD Rotary Rotary morcellatormorcellator Polyps Polyps –– especially fundalespecially fundal
Scope 5.0 mm, 0Scope 5.0 mm, 0°° HysteroscopicHysteroscopic Sheath 5.6 mm Sheath 5.6 mm ODOD Continuous FlowContinuous Flow Ideal for office useIdeal for office use
Fluid Fluid ManagementManagementSmith and NephewSmith and Nephew
Pressure Inflow ControlledPressure Inflow Controlled
Total Fluid UsedTotal Fluid Used
Total DeficitTotal Deficit Weight basedWeight based
Any Operative HS Any Operative HS ProcedureProcedure
Image Courtesy of Smith and NephewImage Courtesy of Smith and Nephew
Decreased Operative TimeDecreased Operative TimePolyps Polyps 22/3/3Type 0 and Type 1 Type 0 and Type 1 11/2/2
Operating Operating Operating Operating
Volume of intrauterine lesion cmVolume of intrauterine lesion cm33Volume of intrauterine lesion cmVolume of intrauterine lesion cm33
Operating Operating time time
(minutes)(minutes)
Operating Operating time time
(minutes)(minutes)
41
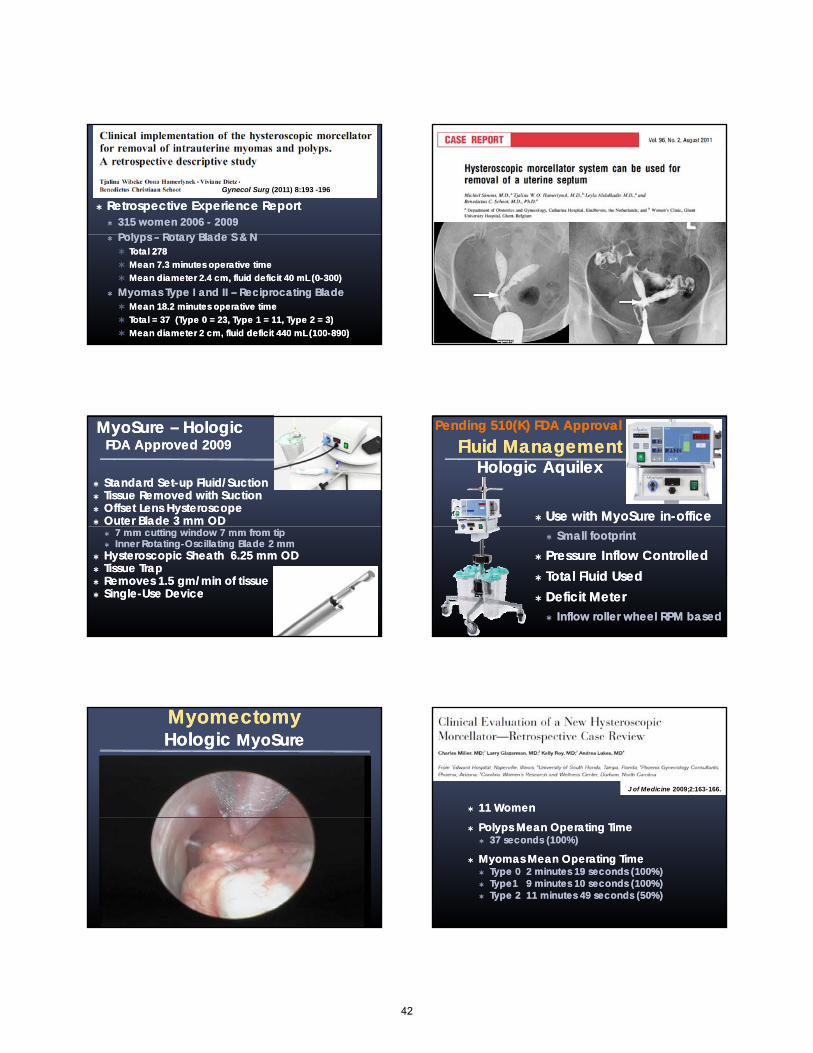
Retrospective Experience Report Retrospective Experience Report 315 women 2006 315 women 2006 -- 20092009
P l P l R t Bl d S & NR t Bl d S & N
Gynecol Surg (2011) 8:193 -196
Polyps Polyps –– Rotary Blade S & NRotary Blade S & N Total 278Total 278 Mean 7.3 minutes operative timeMean 7.3 minutes operative time Mean diameter 2.4 cm, fluid deficit 40 mL (0Mean diameter 2.4 cm, fluid deficit 40 mL (0--300)300)
MyomasMyomas Type I and II Type I and II –– Reciprocating BladeReciprocating Blade Mean 18.2 minutes operative timeMean 18.2 minutes operative time Total = 37 (Type 0 = 23, Type 1 = 11, Type 2 = 3)Total = 37 (Type 0 = 23, Type 1 = 11, Type 2 = 3) Mean diameter 2 cm, fluid deficit 440 mL (100Mean diameter 2 cm, fluid deficit 440 mL (100--890)890)
MyoSureMyoSure –– HologicHologicFDA Approved 2009FDA Approved 2009
Standard SetStandard Set--up Fluid/up Fluid/SuctionSuction Tissue Removed with SuctionTissue Removed with Suction Offset Lens Offset Lens HysteroscopeHysteroscope Outer Blade 3 mm ODOuter Blade 3 mm OD
7 mm cutting 7 mm cutting window 7 mm from tipwindow 7 mm from tip Inner RotatingInner Rotating--Oscillating Blade 2 mmOscillating Blade 2 mm
HysteroscopicHysteroscopic Sheath 6.25 mm Sheath 6.25 mm ODOD Tissue TrapTissue Trap Removes 1.5 Removes 1.5 gmgm/min of tissue/min of tissue SingleSingle--Use DeviceUse Device
Fluid Fluid ManagementManagementHologicHologic AquilexAquilex
Use with Use with MyoSureMyoSure inin--officeoffice
Pending 510(K) FDA ApprovalPending 510(K) FDA Approval
Small footprintSmall footprint Pressure Inflow ControlledPressure Inflow Controlled Total Fluid UsedTotal Fluid Used Deficit Deficit MMeter eter
Inflow roller wheel RPM basedInflow roller wheel RPM based
MyomectomyMyomectomyHologicHologic MyoSureMyoSure
11 Women11 Women
J of Medicine 2009;2:163-166.
Polyps Mean Operating TimePolyps Mean Operating Time 37 seconds (100%)37 seconds (100%)
Myomas Mean Operating TimeMyomas Mean Operating Time Type 0 2 minutes 19 seconds (100%)Type 0 2 minutes 19 seconds (100%) Type1 9 minutes 10 seconds (100%)Type1 9 minutes 10 seconds (100%) Type 2 11 minutes 49 seconds (50%)Type 2 11 minutes 49 seconds (50%)
42

InIn--Office Office PolypectomyPolypectomyHologicHologic MyoSureMyoSure
IOGYN MistralIOGYN Mistral
Integrated Office Integrated Office SSystemystem Rapid Rapid TTissue Removalissue Removal
Bipolar RF initiated plasma energyBipolar RF initiated plasma energy Hemostatic capabilitiesHemostatic capabilities
INVESTIGATIONALINVESTIGATIONAL
Offset Lens Offset Lens HysteroscopeHysteroscope HysteroscopicHysteroscopic Sheath OD 5.2 mmSheath OD 5.2 mm
Continuous FlowContinuous Flow ClosedClosed--Loop Loop FFluid luid MManagementanagement
Can eliminate fluid overloadCan eliminate fluid overload Max deficit set at 2,500 ccMax deficit set at 2,500 cc
Compatible with other RF GeneratorsCompatible with other RF Generators
Fluid ManagementFluid ManagementIOGYN MistralIOGYN Mistral
Courtesy of IOGYNCourtesy of IOGYN
PolypectomPolypectomyyIOGYN MistralIOGYN Mistral
10 grams in 50 seconds
Courtesy of IOGYNCourtesy of IOGYN
MorcellatedMorcellated MyomaMyomaIOGYN MistralIOGYN Mistral
Narrow Coagulation Narrow Coagulation ZoneZone
Adequate Tissue Adequate Tissue PreservationPreservation
HistopathologicHistopathologicEvaluation`Evaluation`
Images Courtesy of IOGYNImages Courtesy of IOGYN
Instrument TrainingInstrument TrainingTruclearTruclear
Courtesy of Smith and NephewCourtesy of Smith and Nephew
43

HysteroscopicHysteroscopic MorcellatorsMorcellatorsAdvantagesAdvantages
Operate in SalineOperate in Saline Decreased risk of fluid overloadDecreased risk of fluid overload
MechanicalMechanical No thermal injuryNo thermal injury No thermal injuryNo thermal injury
Remove Tissue PiecesRemove Tissue Pieces Clear visual fieldClear visual field Decreases risks of multiple instrument Decreases risks of multiple instrument
placementplacement Uterine perforation, false passageway and air Uterine perforation, false passageway and air
embolusembolus
HysteroscopicHysteroscopic MorcellatorsMorcellatorsAdvantagesAdvantages
Are Easy to UseAre Easy to Use Facilitate Removal Type 0 and I Facilitate Removal Type 0 and I MyomasMyomas
Decreased operative time and Decreased operative time and fluid fluid deficitdeficit Small Diameter Can Be Used in the Office Small Diameter Can Be Used in the Office
Fluid UseFluid Use Emanuel Emanuel ---- TRUCLEARTRUCLEAR
Total not recordedTotal not recorded Deficit ALL Deficit ALL MyomasMyomas
714 (0714 (0--3,000)3,000)
Van Van DongenDongen TRUCLEARTRUCLEAR
Miller Miller ---- MyoSureMyoSure Type 0 Type 0
3,400 (1,500 3,400 (1,500 –– 5,300) 5,300) Deficit 205 (200Deficit 205 (200--210)210)
Type 1 Type 1 MyomaMyoma 11,153 (4,670 11,153 (4,670 –– 24,000)24,000)
Van Van DongenDongen ----TRUCLEARTRUCLEAR All ProceduresAll Procedures
3,413 (2,2093,413 (2,209--4,617)4,617) Deficit All ProceduresDeficit All Procedures
409 (229409 (229--589)589)
WibekeWibeke ---- TRUCLEARTRUCLEAR Total not recordedTotal not recorded Deficit ALL Deficit ALL MyomasMyomas
400 (100 400 (100 –– 890) 890)
, ( ,, ( , , ), ) Deficit 1,300 (500Deficit 1,300 (500--1,900)1,900)
Operative Hysteroscopy of Operative Hysteroscopy of MyomasMyomas
(resectoscopy or morcellator)(resectoscopy or morcellator)==
Fluid Management SystemFluid Management System
Hysteroscopic MorcellatorsHysteroscopic MorcellatorsDisadvantagesDisadvantages
No No electrosurgeryelectrosurgery for for hemostasishemostasis IOGYN Mistral has IOGYN Mistral has electrosurgeryelectrosurgery
Type 2 Type 2 myomasmyomas are difficultare difficult Fundal pathology is difficultFundal pathology is difficultgg
Easier with TRUCLEAR Easier with TRUCLEAR blades and with Mistralblades and with Mistral Potential for significant fluid Potential for significant fluid useuse
MyosureMyosure Cost of fluid management Cost of fluid management systemsystem
Mistral is incorporated into deviceMistral is incorporated into device Currently no reimbursement for office useCurrently no reimbursement for office use
ReimbursementReimbursement
InIn--Patient (21), OutPatient (21), Out--Patient (22), ASC (24)Patient (22), ASC (24)
58558 Hysteroscopy with58558 Hysteroscopy withPolypectomy,Polypectomy, Biopsy, D & CBiopsy, D & C
2011 RVU2011 RVUMedicareMedicareCFCF 34 0134 01
125%125%CF 42 5125CF 42 5125
No GlobalNo Global20112011
Myosure Myosure Device CostDevice Cost
$1,300$1,3002011 RVU2011 RVU CFCF 34.0134.01 CF 42.5125CF 42.5125
7.95 $ 270.38 $ 337.97
NonNon--Facility/OfficeFacility/Office (11)(11)
10.6 $ 360.50 $ 450.63
With E/M VisitWith E/M VisitModifier 25Modifier 25
Document HS SeparatelyDocument HS Separately
ReimbursementReimbursement
InIn--Patient (21), OutPatient (21), Out--Patient (22), ASC (24)Patient (22), ASC (24)
Hysteroscopy with MyomectomyHysteroscopy with Myomectomy5856158561
MedicareMedicare 125%125%
No GlobalNo Global20112011
2011 RVU2011 RVUMedicareMedicareCFCF 34.0134.01
125%125%CF 42.5125CF 42.5125
16.33 $ 555.38 $ 694.23
NonNon--Facility/OfficeFacility/Office (11)(11)
0 $ 0 $ 0
44
HysteroscopicHysteroscopic MorcellatorsMorcellatorsSummarySummary
More women will have the More women will have the opportunity for uterine preserving opportunity for uterine preserving surgery with the removal of Type surgery with the removal of Type surgery with the removal of Type surgery with the removal of Type 0 and 1 0 and 1 myomasmyomas with safer with safer instruments, that require less instruments, that require less surgical skill. surgical skill. Removal Removal of polyps is of polyps is easier and easier and faster.faster.
Learning ObjectivesLearning Objectives
Describe intracavitary Describe intracavitary myomasmyomas using a classification systemusing a classification system
Explain the different types of hysteroscopic Explain the different types of hysteroscopic morcellatorsmorcellators
Employ techniques to reduced risk during removal of intracavitary Employ techniques to reduced risk during removal of intracavitary myomasmyomas
Enumerate the fundamental differences between traditional Enumerate the fundamental differences between traditional resectoscopyyresectoscopyy and and h i l ll ti f l f i t it l ih i l ll ti f l f i t it l imechanical morcellation for removal of intracavitary lesionsmechanical morcellation for removal of intracavitary lesions
List the potential challenges and advantages of performing hysteroscopic List the potential challenges and advantages of performing hysteroscopic removal of intracavitary lesions in the office settingremoval of intracavitary lesions in the office setting
..
45
Micah Harris M.D. Women’s Health Research
Phoenix, AZ
Grants/Research Support: Halt Medical
At the conclusion of this presentation the participant will be able to:1. List the common potential complications
encountered during or after office hysteroscopy.2. Identify the correct management of uterine
perforation dependant upon location.3. List the risk factors for uterine perforation.4. State AAGL Guidelines for hysteroscopic fluid
management.5. Identify office hysteroscopic procedures that have a
higher risk of complication.
Related to Entry/ Dilation of the cervix: 50%- Creation of a False Passage- Cervical Laceration/Hemorrhage - Uterine Perforation- Uterine Perforation
Related to Distention Medium-Fluid Overload, Hyponatremia- Air/Gas Embolism
Related to Procedure- Adhesiolysis
Vaso-vagal Reaction
Local Anesthetic Toxicity
Inadequate Analgesia/Anesthesia
Airway Management Excessive Sedation Allergic Reaction
46
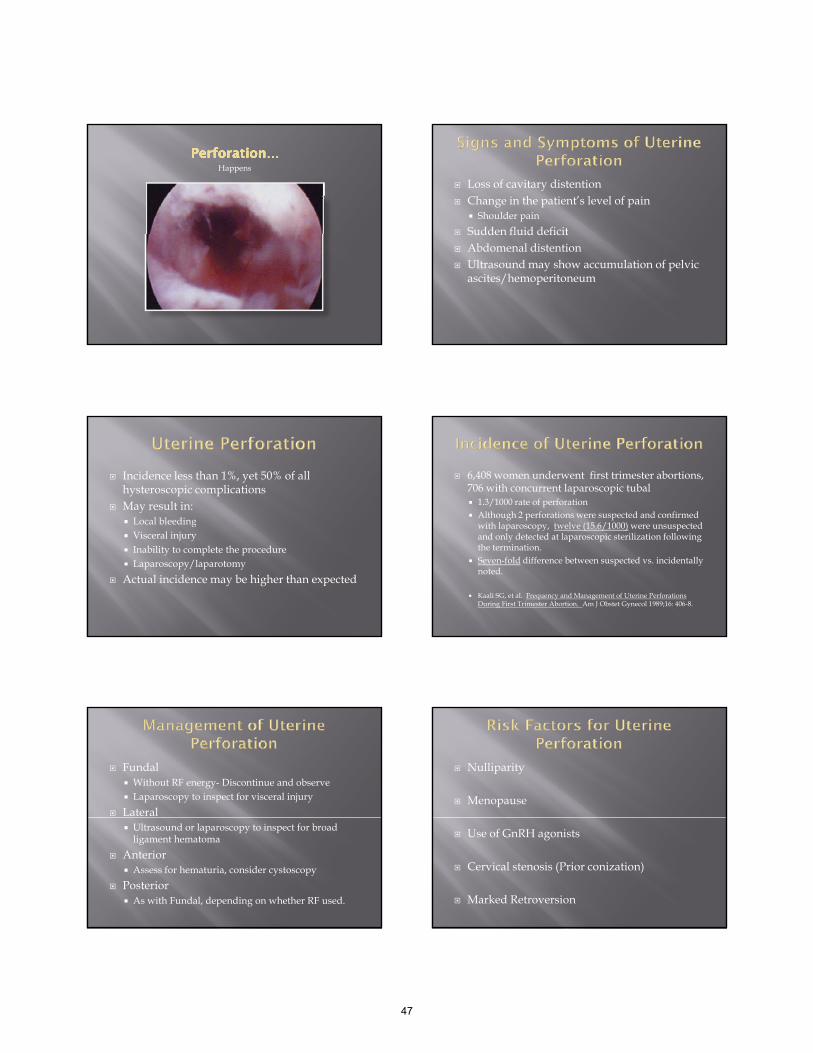
Happens
Loss of cavitary distention Change in the patient’s level of pain
Shoulder pain
Sudden fluid deficit Sudden fluid deficit Abdomenal distention Ultrasound may show accumulation of pelvic
ascites/hemoperitoneum
Incidence less than 1%, yet 50% of all hysteroscopic complications
May result in: Local bleedingg Visceral injury Inability to complete the procedure Laparoscopy/laparotomy
Actual incidence may be higher than expected
6,408 women underwent first trimester abortions, 706 with concurrent laparoscopic tubal 1.3/1000 rate of perforation Although 2 perforations were suspected and confirmed
with laparoscopy twelve (15 6/1000) were unsuspected with laparoscopy, twelve (15.6/1000) were unsuspected and only detected at laparoscopic sterilization following the termination.
Seven-fold difference between suspected vs. incidentally noted.
Kaali SG, et al. Frequency and Management of Uterine Perforations During First Trimester Abortion. Am J Obstet Gynecol 1989;16: 406-8.
Fundal Without RF energy- Discontinue and observe Laparoscopy to inspect for visceral injury
Lateral Ultrasound or laparoscopy to inspect for broad
ligament hematoma
Anterior Assess for hematuria, consider cystoscopy
Posterior As with Fundal, depending on whether RF used.
Nulliparity
Menopause
Use of GnRH agonists
Cervical stenosis (Prior conization)
Marked Retroversion
47

Most office procedures involve small diameter scopes, and therefore little dilation is necessary.
Over-dilation results in inadequate distention Over dilation results in inadequate distention of the uterine cavity.
The use of cervical dilators can result in potentially undetected uterine perforation.
Consider using the hysteroscope as the dilator.
Directly visualize the passage
Avoid creating a False Passage
Recognize perforation
Dilate only as much as necessary
Misoprostil 400 mcg vaginally 6-12 hours pre-procedure
Reduces the force necessary for dilation Reduces pain scores associated with dilation Reduces pain scores associated with dilation Concern for over-dilation
Waddell G, et al. Cervical Ripening Using Vaginal Misoprostil Before Hysteroscopy. JMIG 2008; 15: 739-744
In dilute solutions ( 0.05-0.2 U/cc NS) promotes cervical dilation and myometrial hemostasis, as well as decreases fluid medium absorption.
Toxicity is cardiac/vascular (Hypertensive Crisis, A h th i )Arrhythmia)
Cardiac effects may be treated with Nitroglycerin
Chudnoff, S et al. Review of Vasopressin Use in Gynecologic Surgery, JMIG 2012; 19: 422-433
Prospective study of 13,600 subjects Adhesiolysis 4.48%
Endometrial Resection 0.81%
Myomectomy 0.75%
Polypectomy 0.38%
Jansen FW, et al. Complications of Hysteroscopy..Obstst Gynecol2000; 96 266-270
48

Rarely suspected at the time Associated with a sudden “give” in pressure
during placement Associated with an abnormal deployment of
th i i t ilthe microinsert coil No reported acute complication such as
hemorrhage Chronic problems include pain, lack of efficacy
Connor VF Essure: A Review Six Years Later. JIMG 2009; 16 282-90
Cervical/Vaginal Inspect, suture as necessary. Prevent cervical laceration with “solid” first
tenaculum application
Myometrial Intrauterine balloon- carries some risk of uterine
rupture if overinflated. Remember Bimanual Compression- it works!!
Carbon Dioxide- Primarily used for Diagnostic Procedures. Visualization obscured by bleeding Actually more water-soluable than Nitrogen-
containing room air The “Lethal Dose” of Room Air is 5X less than that of
CO2
Groenman FA et al, Embolism of Air and Gas in HysteroscopicProcedures, JMIG 2008; 15 241-247
Signs and Symptoms: Related to bubbles creating disturbances in gas exchange or most severly, an Air-Lock in the Right Heart.
Decreasing Oxygen Saturation
Hypotension due to decreased venous return
Decreased End-Tidal CO2
Gaseous Distention Pressures > 100mmHg
Trendelenburg Position
More frequent insertions of the hysteroscope
Procedures injuring myometrial vessels Adhesiolysis Myometrial Resection
Up to 50% Mortality
Recognize Pulmonary symptoms early
Administer 100% Oxygen
Reverse Trendelenberg, Left Decubitus (Durant Manuever)
Cardiovascular Rescuscitation/ Support
49

Non-ionic media Glycine 1.5% Sorbitol/Mannitol 3%/0.54% Mannitol 5%
Ionic Media Normal Saline
Complications arise from absorption and fluid overload. Maintain I/O’s, especially when a pressure bag is
used
Hyponatremia and Cereberal Edema Pulmonary Edema Primary treatment is Diuresis Less common in the office setting
Deficit >750cc, electrolyte poor solution Plan to terminate the procedure
Deficit >1000cc electrolyte poor, >2500cc ionic Terminate the procedure Assess serum sodium Lasix 10 mg IV
Ad Hoc Committee on Hysteroscopic Fluid Management. JAAGL 2000 7(2) 167-168.
Anesthetic Toxicity- Be aware of toxic doses of injectable anesthetics- Lidocaine, Marcaine
Vasovagal reactions- Identify, support, Vasovagal reactions Identify, support, administer Atropine 0.4-0.6mg SC/IM/IV
HAVE A FULLY STOCKED CRASH-CART, AND STAFF WHO UNDERSTANDS HOW TO USE IT.
Infectious- 0.01-1.4% ACOG guidelines do not support prophylactic
antibiotics for hysteroscopic surgery in the absence of a history of PIDT t t f l i i l d Treat symptoms of pelvic pain, malodorous discharge, fever with extended spectrum penicillinor cephalosporin
Ultrasound if on pelvic exam an mass is felt
Hematometrium 1-2% Chronic or cyclic pain Drainage with or without ultrasound guidance
Complications are fortunately rare (0.3%) Half are entry related, e.g. perforation
Avoid with entry under visualisation Cervical ripening can be helpful
b l h Air embolism is more common than CO2 embolism
Overabsorption of fluid media is preventable and easily treated.
Know the contents of your crash cart and have knowledgable support staff.
50

1. Jansen FW, Vredevoogd CB, Ulzen K et al. Complications of Hysteroscopy: A Prospective Multicenter Study. Obstet Gynecol2000; 96 266-270.
2. Propst AM, Liberman RF, Harlow BL Ginsberg ES Complications of Hysteroscopic Surgery: Predicting Patients at Risk Obstetof Hysteroscopic Surgery: Predicting Patients at Risk. ObstetGynecol 2000; 96 517-520.
3. Uckuyu A, Ozcimen EE, Sevinc FC, Zeyneloglu HB Efficacy of Vaginal Misoprostil Before Hystersocopy for Cervical Priming in Patients Who Have Undergone Cesarean Delivery and No Vaginal Deliveries. JMIG 2008; 15 739-744.
4. Wadell G, Desindes S, Takser L,Beauchermin MC, Besette P Cervical Ripening Using Misoprostil Before Hysteroscopy: A Randomized Double Blind Trial. JMIG 2008; 15 739-744.
5. Chudnoff S. Glazer S, Levie M Review of Vasopressin Use in Gynecologic Surgery JMIG 2012; 19 422 433Gynecologic Surgery. JMIG 2012; 19 422-433.
6. Groenman FA, Peters LW, Rademaker BM, Bakkum EA Embolism of Air and Gas in Hysteroscopic Procedures: Pathophysiology and Implications for Daily Practice. JMIG 2008; 15 241-247.
7. Kaali SG, Szigetvari IA, Bartfai GS. The Frequency and Management of Uterine Perforations During First Trimester Abortions Am J Obstet Gynecol. 1989; 16: 406-8
8. Ad Hoc Committee on Hysteroscopic Fluid Management. Guidelines of the AAGL JAAGL 2000 7(2) 167 168 Guidelines of the AAGL. JAAGL 2000 7(2) 167-168.
9. Antibiotic Prophylaxis for Gynecologic Procedures ACOG Practice Bulletin Number 104 May 2009- Reaffirmed 2011
10. Connor VF Essure: A Review Six Years Later. JIMG 2009; 16 282-90.
51

Equipment Maintenance: The Rigid and Flexible
Hysteroscope
Eileen Young RN BSN CNOREileen Young, RN, BSN, CNOR
• Other: Employee ‐ Olympus
Identify safe handling techniques for hysteroscopes.
Describe proper reprocessing steps for hysteroscopeshysteroscopes.
Advantages of Hysteroscope Types
Rigid with rod lens opticsClearest visualization
Easiest to insert
Semi‐rigid with fiberoptic/digital imageSemi rigid with fiberoptic/digital image
Large working channel and no additional telescopes
FlexiblePatient comfort and no additional components
Rigid Hysteroscopes
Telescope 12 and/or 30°
Sheath Standard, intermittent flow (usually smaller diameter) Continuous flow (may have inner and outer sheaths)Continuous flow (may have inner and outer sheaths)
Obturator Visual, used for atraumatic insertion
Bridge / AdaptorUsed with a seal to insert accessory devices
Biopsy forceps Tubal sterilization
Sheaths
Size dependent on patient anatomy and desired channel
Continuous flow sheaths will likely provide better visualizationbetter visualization
Small cavity size
Bleeding can obscure vision
Inflow and outflow pathways NOT interchangeable
52
Telescopes
Angle of view 30° wide angle provides best visualization of cavity and cornua
12° is more direct, better for use with resection devices
Lens is always opposite light posty pp g p
Field of view – amount of area seen through lens
Characteristics Most fragile and expensive component
Damaged telescope = no hysteroscope
Handle with eyepiece, protect lens
Semi‐Rigid Hysteroscopes
Hybrid device Fiberoptic or digital image
May have a deflecting tip
Housed in a metal shaftHoused in a metal shaft
May be easier to insert / handle than flexible
Flexible Hysteroscopes
Diagnostic
Intermittent flow only
Accessory channel is same as irrigation channelAccessory channel is same as irrigation channel
Less discomfort for patient
Require practice inserting and manipulating
Repairs can be expensive
Buying Guide
Determine patient population
Infertility and/or post‐menopausal women – small diameter
Abnormal uterine bleeding – continuous flowAbnormal uterine bleeding continuous flow
Patient comfort – flexible
Transcervical sterilization – channel size
Decontamination Supplies
Enzymatic detergent
Soft cloth, gauze and applicators
Protective attire
Syringes
Leak tester for flexible and semi‐rigid scopes
Alcohol to clean glass surfaces
Decontamination ProcessWipe and flush immediately after procedure
Clean as soon as possible with properly mixed enzymatic detergent
Flush and/or brush all lumens
Dry exterior surface and push air through channelDry exterior surface and push air through channel
High‐level disinfect or sterilize If using a steam sterilizer, may wrap devices to maintain sterility
High‐level disinfectants must be thoroughly rinsed and dried prior to storage or use
53

High‐level Disinfection Considered semi‐critical devices (not entering sterile cavity or bloodstream, moderate risk of infection) Minimum preparation is HLD, but can sterilize
Glutaraldehyde‐based HLD are most common OPA may be alternative
Exposure time and temperature, rinsing
Safety considerations Venting
Gloves
Monitoring concentration
Sterilization
Steam
High temperature and vacuum may not be compatible with device
Follow OEM recommendations for cycle type time Follow OEM recommendations for cycle type, time and temperature
Conclusion
Hysteroscopes are an investment in your practice
Require careful handling
i ifi iRequire specific reprocessing
Office procedures can enhance your practice
Repairs can be minimized with proper care and handling
Clemens, J., Dowling, R., Foley, F., Goldman, H., Gonzalez, C., Tessier, C., Wasner, M., & Young, E. (2009). Joint AUA/SUNA White Paper on Reprocessing of Flexible Cystoscopes. Retrieved from: http://www.suna.org/cgi‐bin/WebObjects/SUNAMain.woa/1/wa/viewSection?wosid=yQgi599ceBCE3lm6dhp1282yNf2&tName=whitePaper&s_id=1073743840& id 173743840&ss_id=1
Rutala, W., Weber, D., HICPAC. (2008). Guidelines for Disinfection and Sterilization in Healthcare Facilities. Retrieved from: http://www.cdc.gov/hicpac/Disinfection_Sterilization/acknowledg.html
54
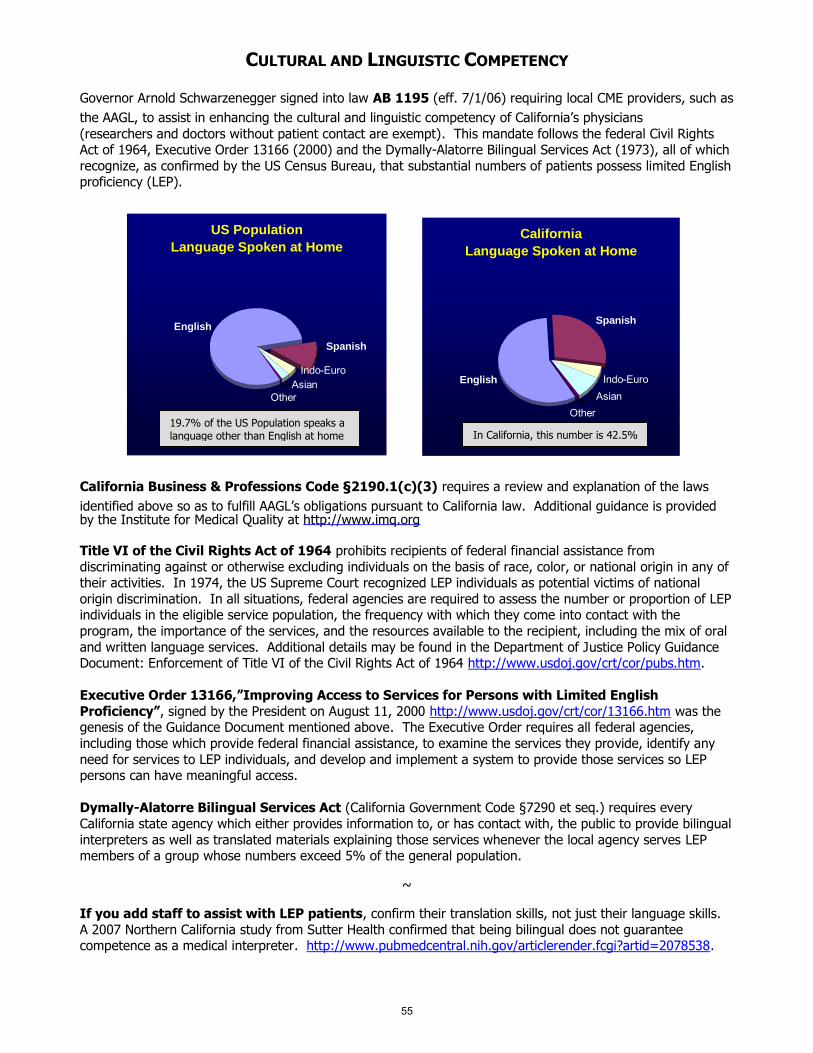
CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsianIndo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
55
Top Related