







Languages
Pages
Legal

Perinatal asphyxia: Pathophysiology and therapy
Peter Davis Melbourne
Australia
With thanks to Dr Sue Jacobs
Moderate or severe HIE
• Complicates ~1/1000 term live births: –Mortality: >25%
–Major neurological sequelae: >25% • Cerebral palsy, intellectual impairment, seizures
–Cognitive impairments at school-age, even without neuromotor deficits • Associated behavioural & educational
difficulties
A Little Basic Science
• Neuronal death occurs in 2 phases
• Severe insult
–Immediate neuronal death – cellular hypoxia and primary energy failure
–Delayed neuronal death – occurs at least 6 hours later i.e. allows a therapeutic window
A Little Basic Science
• Secondary phase – accounts for a major proportion of cell loss
–Pathology - hyperemia, cytotoxic oedema, mitochondrial failure, accumulation of cytotoxins, apoptosis, nitric oxide synthesis, free radical damage
–Clinically – encephalopathy, increased seizure activity
Mechanism of protection by hypothermia
• Survival of cells otherwise destined to die through apoptosis
• Reduced metabolic rate
• Reduced release of excitatory amino acids (glutamate, dopamine)
• Lower production of nitric oxide and free radicals
Methods of cooling newborns
• Selective head cooling with mild systemic hypothermia
– Rationale: ‘Cool brain more than body’
• Newborn brain produces 70% of total body heat
• Minimise adverse effects of systemic cooling
• Whole-body hypothermia
– Rationale: ‘Reduce systemic temperature to achieve deep brain cooling’
• Core body temperature & deep brain temperature are similar
• Mathematic modeling supports this
Potential Adverse Effects of Cooling
Heart
– ↓Contractility, BP
– Bradycardia
– Arrhythmias
– PPHN
Lungs
– Pulmonary oedema
– Hypoxia
Gastrointestinal
– NEC
Hematological
– Coagulopathy & platelet dysfunction
Metabolic
– Acidosis
– O2 dissociation curve to left
– Hypokalaemia
– Hypoglycaemia
Immunological
– Sepsis
Randomised Trials of Cooling for HIE
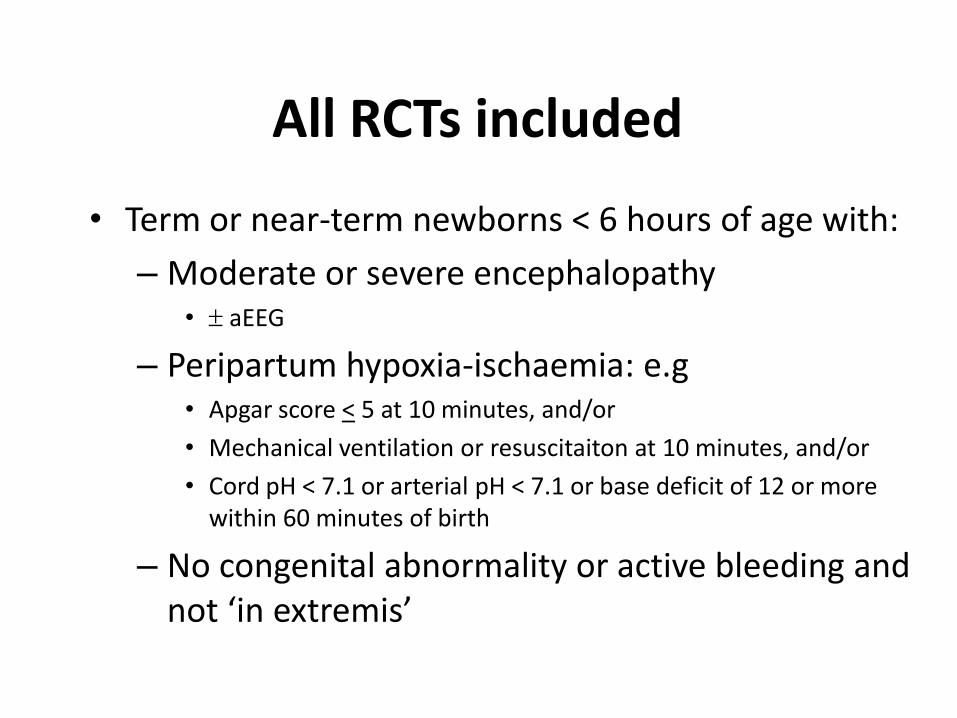
All RCTs included
• Term or near-term newborns < 6 hours of age with:
– Moderate or severe encephalopathy • aEEG
– Peripartum hypoxia-ischaemia: e.g • Apgar score < 5 at 10 minutes, and/or
• Mechanical ventilation or resuscitaiton at 10 minutes, and/or
• Cord pH < 7.1 or arterial pH < 7.1 or base deficit of 12 or more within 60 minutes of birth
– No congenital abnormality or active bleeding and not ‘in extremis’
RCTs Intervention
Therapeutic hypothermia (whole body or selective head cooling)
Or
No cooling (standard care)
Active (device) and/or Passive cooling
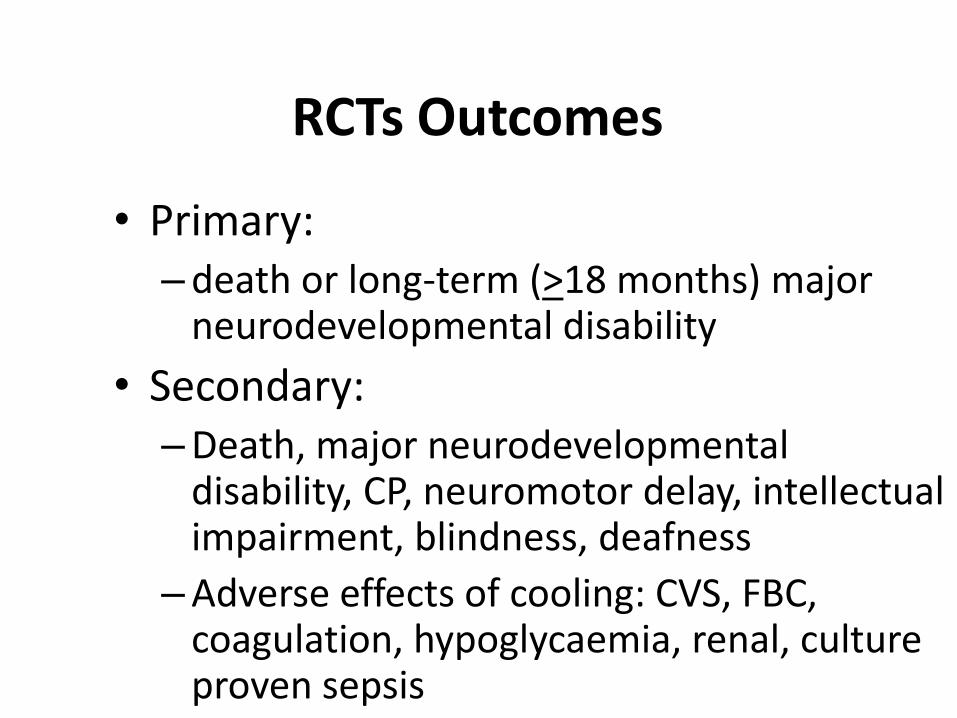
RCTs Outcomes
• Primary: –death or long-term (>18 months) major
neurodevelopmental disability
• Secondary: –Death, major neurodevelopmental
disability, CP, neuromotor delay, intellectual impairment, blindness, deafness
–Adverse effects of cooling: CVS, FBC, coagulation, hypoglycaemia, renal, culture proven sepsis
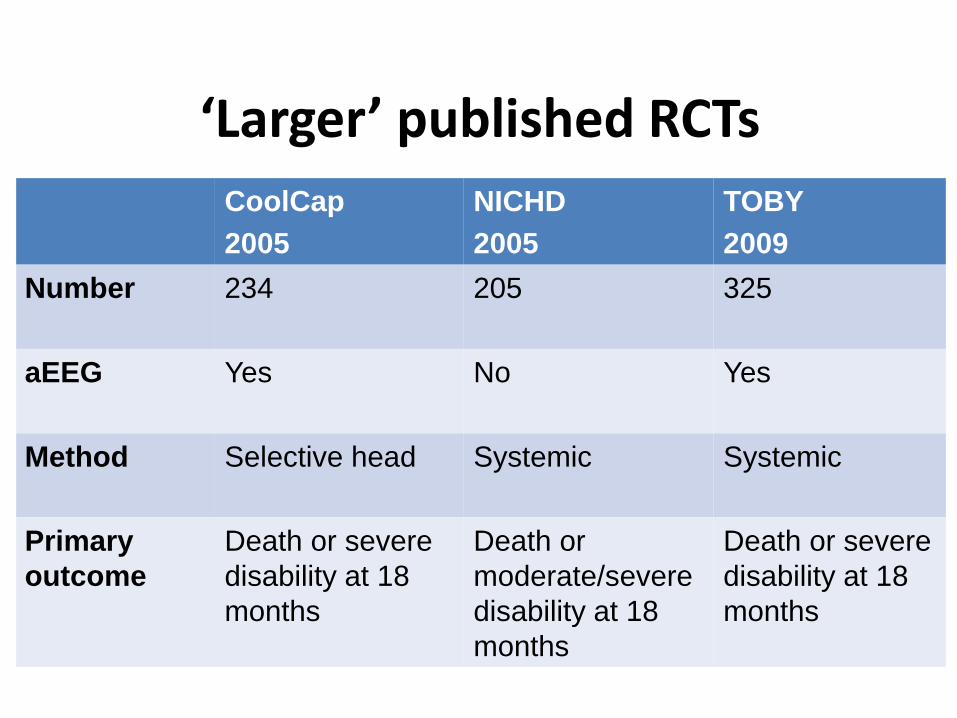
‘Larger’ published RCTs
CoolCap
2005
NICHD
2005
TOBY
2009
Number 234 205 325
aEEG Yes No Yes
Method Selective head Systemic Systemic
Primary
outcome
Death or severe
disability at 18
months
Death or
moderate/severe
disability at 18
months
Death or severe
disability at 18
months
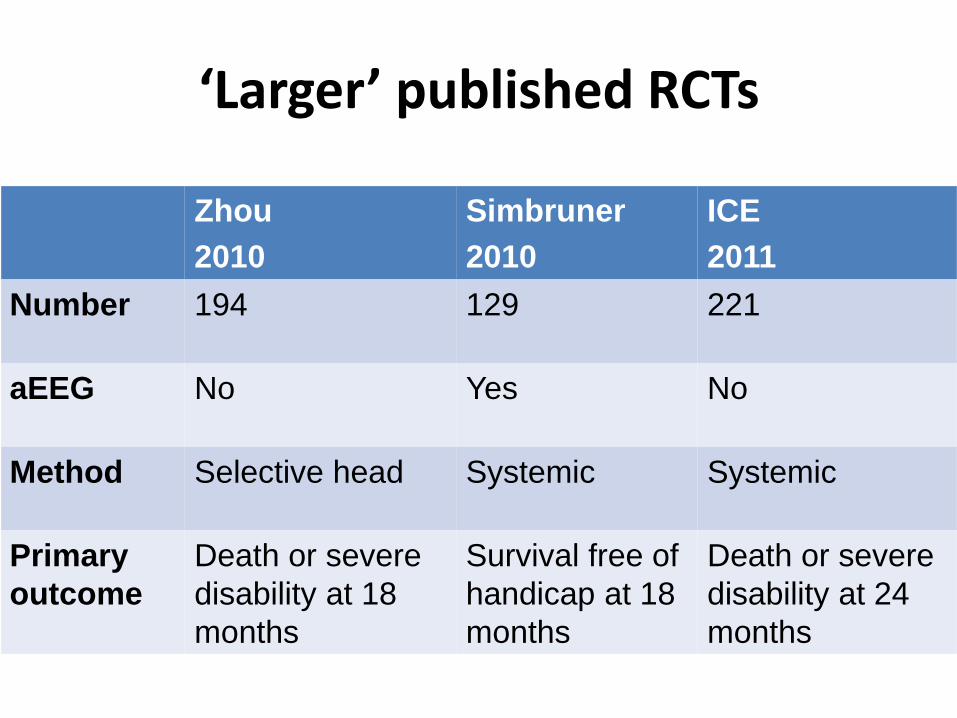
‘Larger’ published RCTs
Zhou
2010
Simbruner
2010
ICE
2011
Number 194 129 221
aEEG No Yes No
Method Selective head Systemic Systemic
Primary
outcome
Death or severe
disability at 18
months
Survival free of
handicap at 18
months
Death or severe
disability at 24
months

The ‘ICE’ randomized trial of whole body hypothermia for hypoxic-ischemic
encephalopathy (HIE)
Sue Jacobs Morley CJ, Inder TE, Stewart MJ, Smith KR, McNamara PJ, Wright IMR, Kirpalani HM, Darlow BA, Doyle LW and The ICE Collaboration
Arch Pediatr Adolesc Med. 2011 Aug;165(8):692-700.
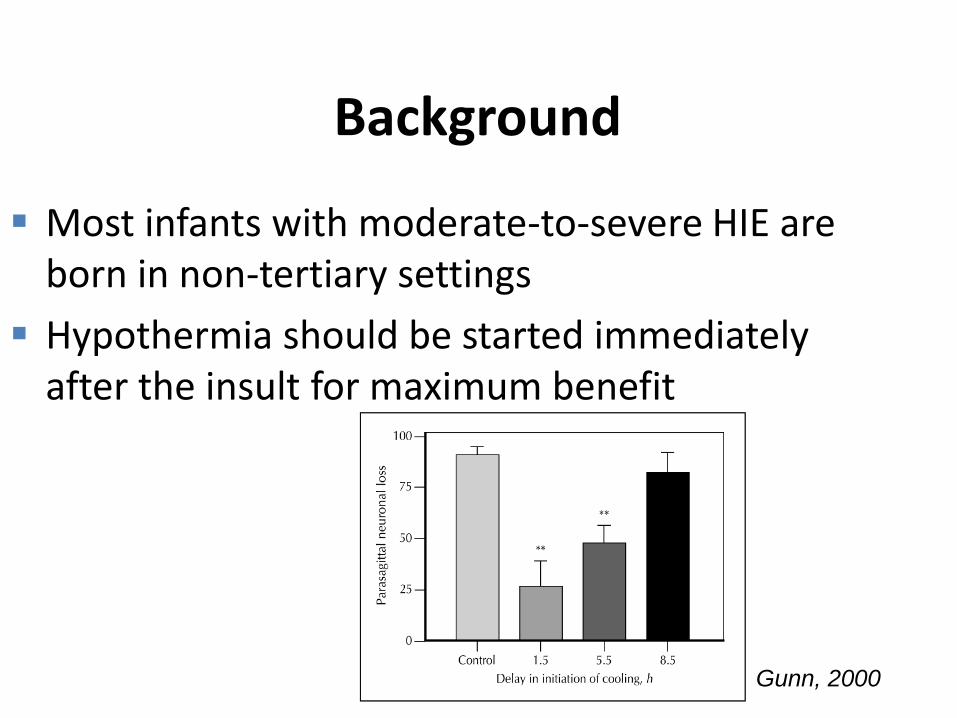
Background
Most infants with moderate-to-severe HIE are born in non-tertiary settings
Hypothermia should be started immediately after the insult for maximum benefit
Gunn, 2000
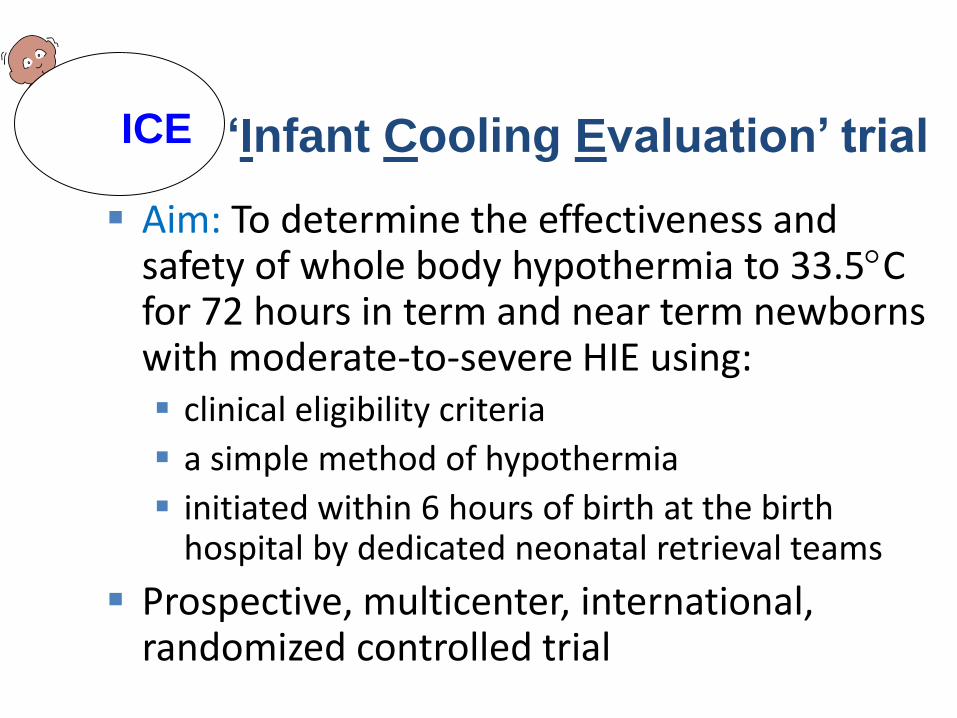
Aim: To determine the effectiveness and safety of whole body hypothermia to 33.5C for 72 hours in term and near term newborns with moderate-to-severe HIE using: clinical eligibility criteria
a simple method of hypothermia
initiated within 6 hours of birth at the birth hospital by dedicated neonatal retrieval teams
Prospective, multicenter, international, randomized controlled trial
‘Infant Cooling Evaluation’ trial ICE ICE
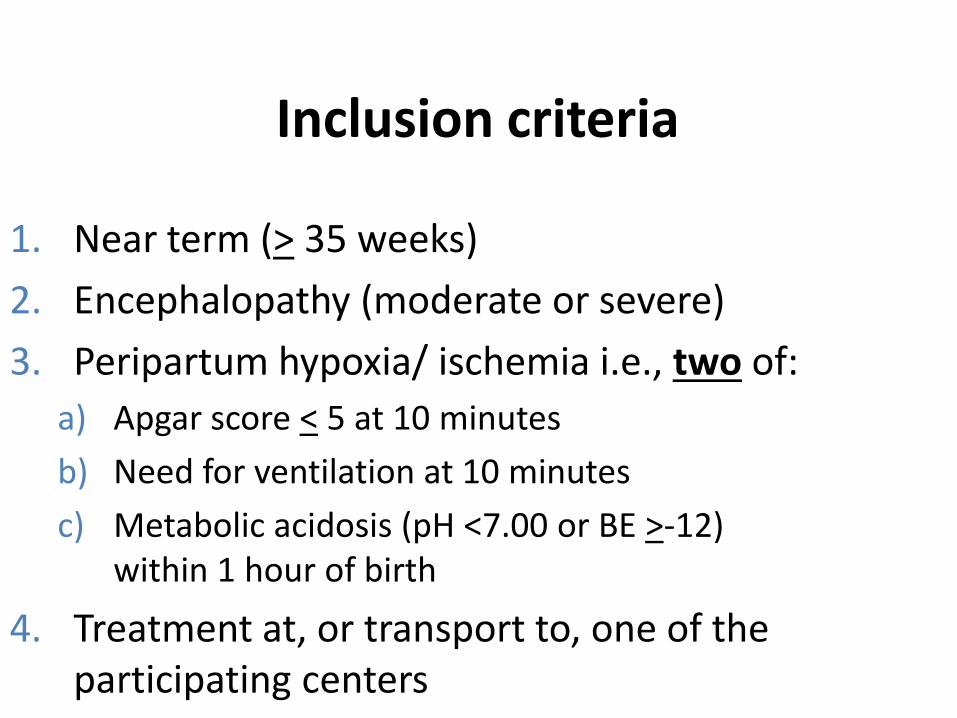
Inclusion criteria
1. Near term (> 35 weeks)
2. Encephalopathy (moderate or severe)
3. Peripartum hypoxia/ ischemia i.e., two of:
a) Apgar score < 5 at 10 minutes
b) Need for ventilation at 10 minutes
c) Metabolic acidosis (pH <7.00 or BE >-12) within 1 hour of birth
4. Treatment at, or transport to, one of the participating centers
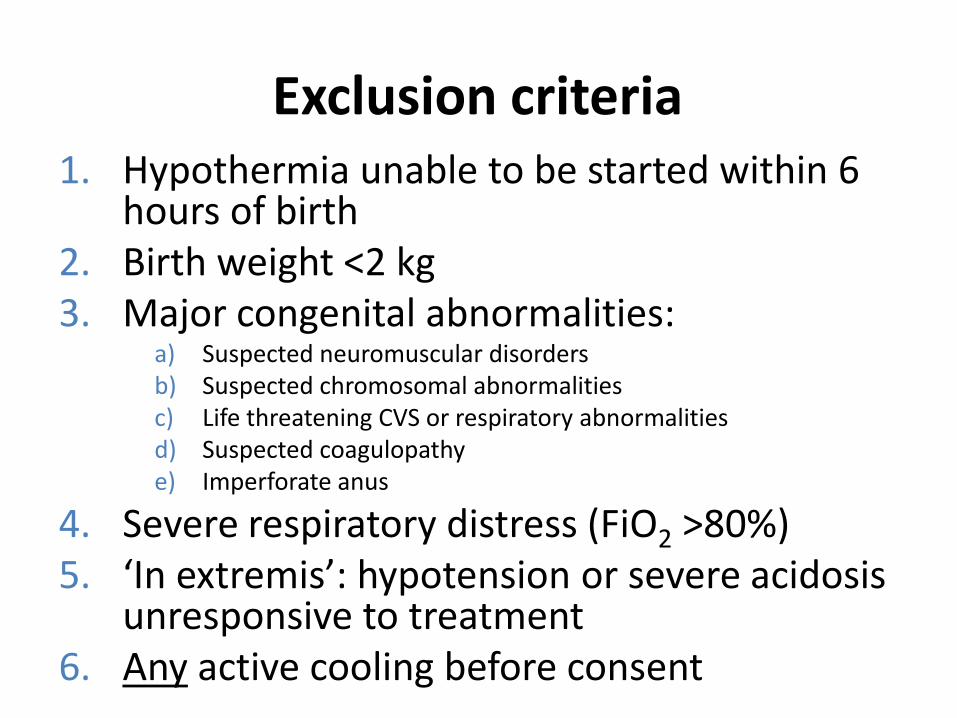
Exclusion criteria 1. Hypothermia unable to be started within 6
hours of birth 2. Birth weight <2 kg 3. Major congenital abnormalities:
a) Suspected neuromuscular disorders b) Suspected chromosomal abnormalities c) Life threatening CVS or respiratory abnormalities d) Suspected coagulopathy e) Imperforate anus
4. Severe respiratory distress (FiO2 >80%) 5. ‘In extremis’: hypotension or severe acidosis
unresponsive to treatment 6. Any active cooling before consent
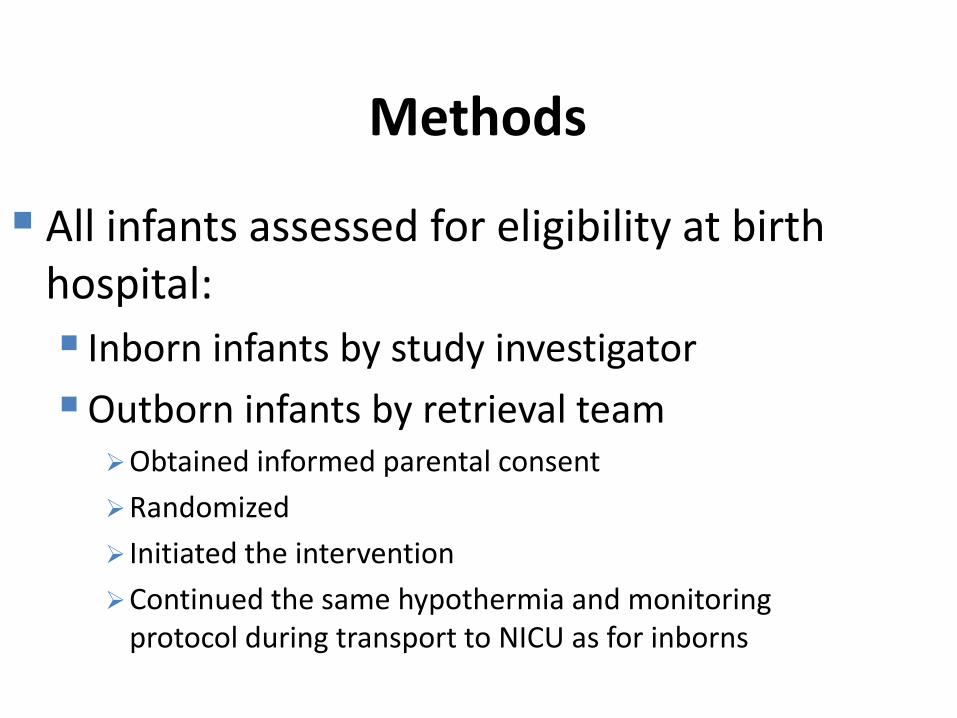
Methods
All infants assessed for eligibility at birth hospital:
Inborn infants by study investigator
Outborn infants by retrieval team Obtained informed parental consent
Randomized
Initiated the intervention
Continued the same hypothermia and monitoring protocol during transport to NICU as for inborns
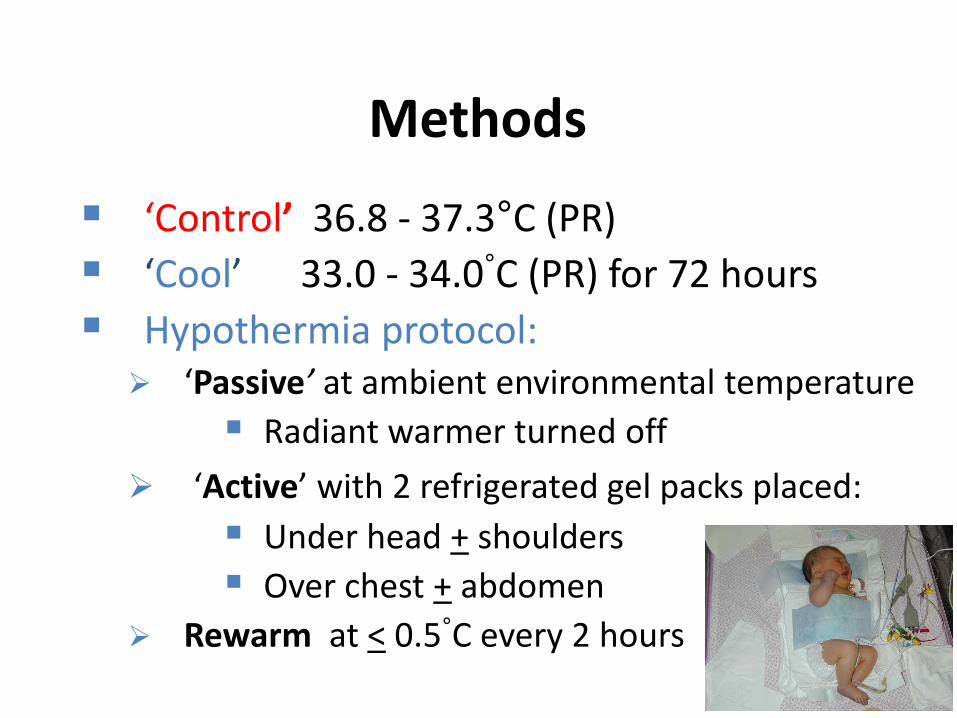
Methods
‘Control’ 36.8 - 37.3°C (PR)
‘Cool’ 33.0 - 34.0°C (PR) for 72 hours
Hypothermia protocol: ‘Passive’ at ambient environmental temperature
Radiant warmer turned off
‘Active’ with 2 refrigerated gel packs placed:
Under head + shoulders
Over chest + abdomen
Rewarm at < 0.5°C every 2 hours
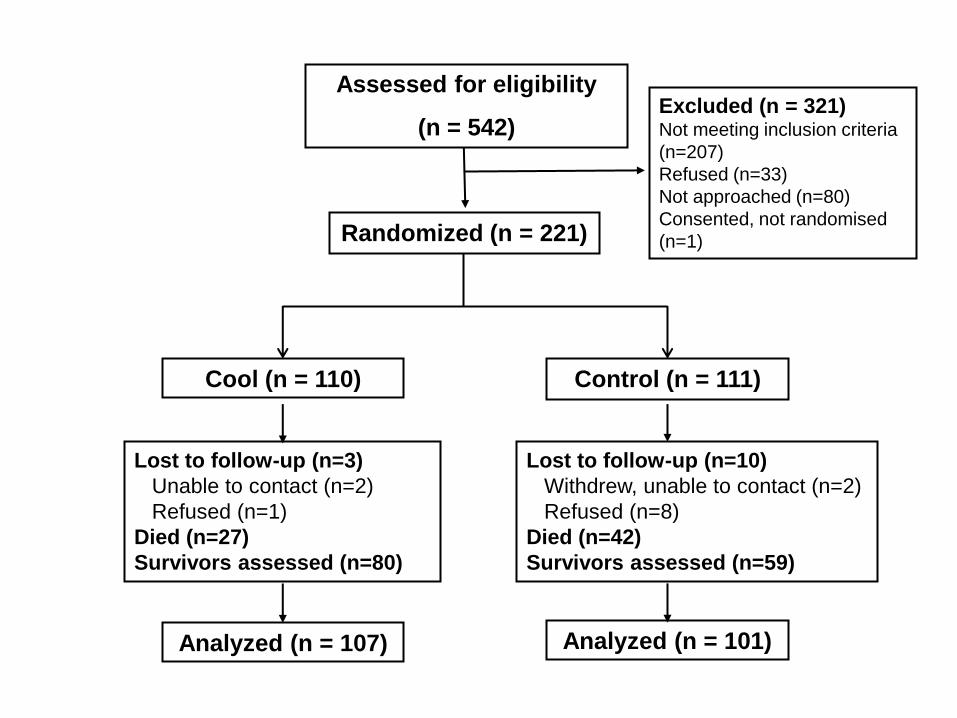
Assessed for eligibility
(n = 542)
Randomized (n = 221)
Excluded (n = 321) Not meeting inclusion criteria
(n=207)
Refused (n=33)
Not approached (n=80)
Consented, not randomised
(n=1)
Cool (n = 110) Control (n = 111)
Lost to follow-up (n=3)
Unable to contact (n=2)
Refused (n=1)
Died (n=27)
Survivors assessed (n=80)
Lost to follow-up (n=10)
Withdrew, unable to contact (n=2)
Refused (n=8)
Died (n=42)
Survivors assessed (n=59)
Analyzed (n = 107) Analyzed (n = 101)
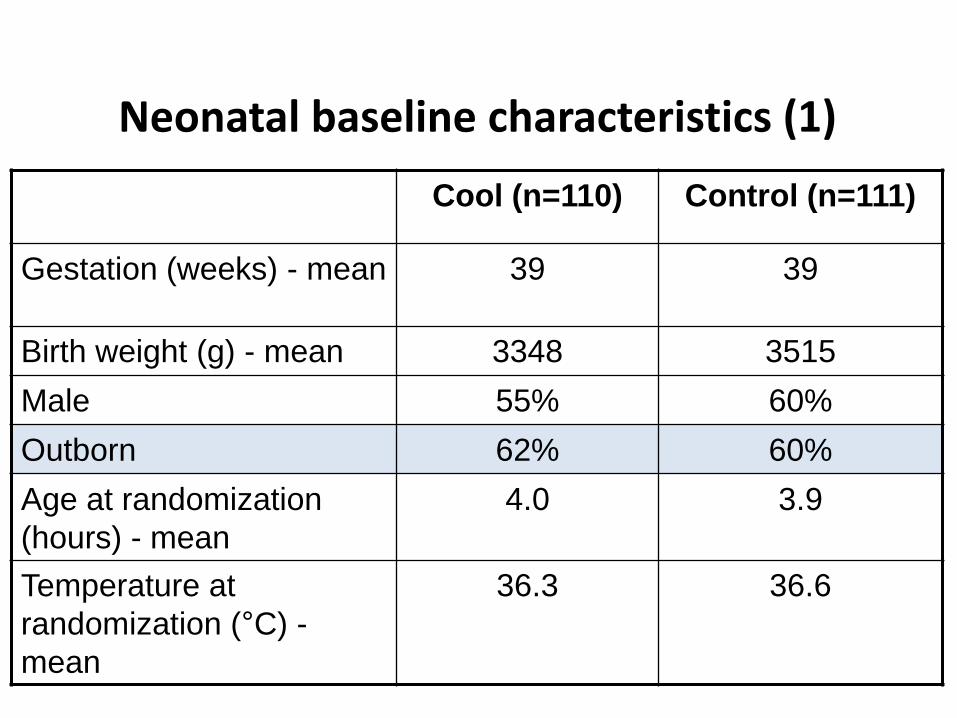
Neonatal baseline characteristics (1)
Cool (n=110) Control (n=111)
Gestation (weeks) - mean 39 39
Birth weight (g) - mean 3348 3515
Male 55% 60%
Outborn 62% 60%
Age at randomization
(hours) - mean
4.0 3.9
Temperature at
randomization (°C) -
mean
36.3 36.6
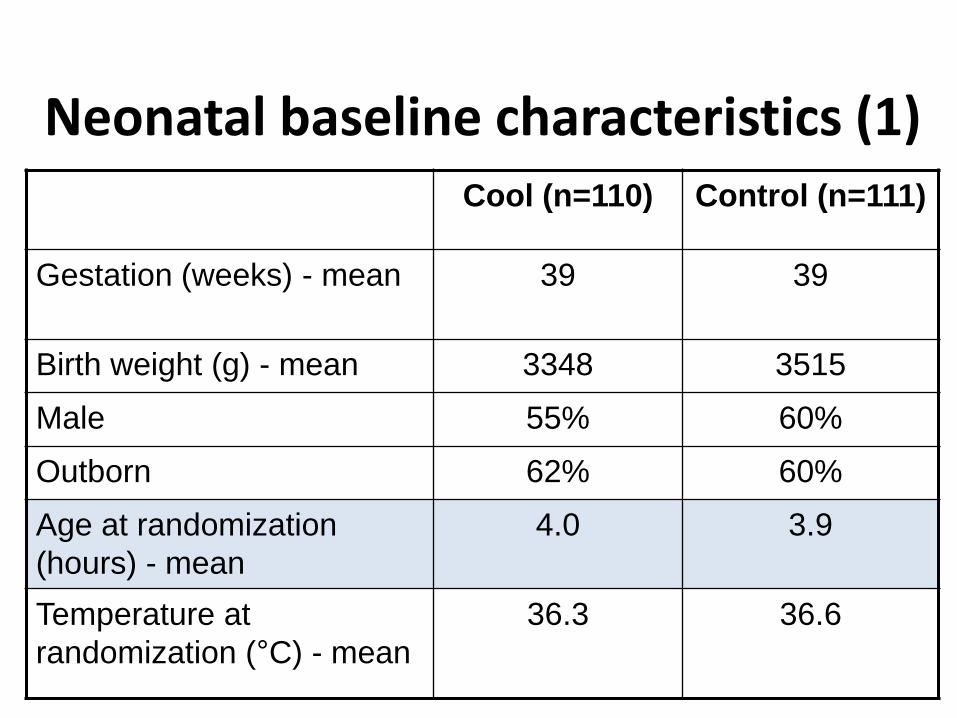
Neonatal baseline characteristics (1) Cool (n=110) Control (n=111)
Gestation (weeks) - mean 39 39
Birth weight (g) - mean 3348 3515
Male 55% 60%
Outborn 62% 60%
Age at randomization
(hours) - mean
4.0 3.9
Temperature at
randomization (°C) - mean
36.3 36.6

Neonatal baseline characteristics (2) Cool (n=110) Control (n=111)
Apgar score (median)
1 minute
5 minutes
10 minutes
1
3
4
1
3
4
Resuscitation
Ventilation
Chest compressions
Adrenaline
100%
63%
39%
100%
62%
45%

Neonatal baseline characteristics (2) Cool (n=110) Control (n=111)
Apgar score (median)
1 minute
5 minutes
10 minutes
1
3
4
1
3
4
Resuscitation
Ventilation
Chest compressions
Adrenaline
100%
63%
39%
100%
62%
45%
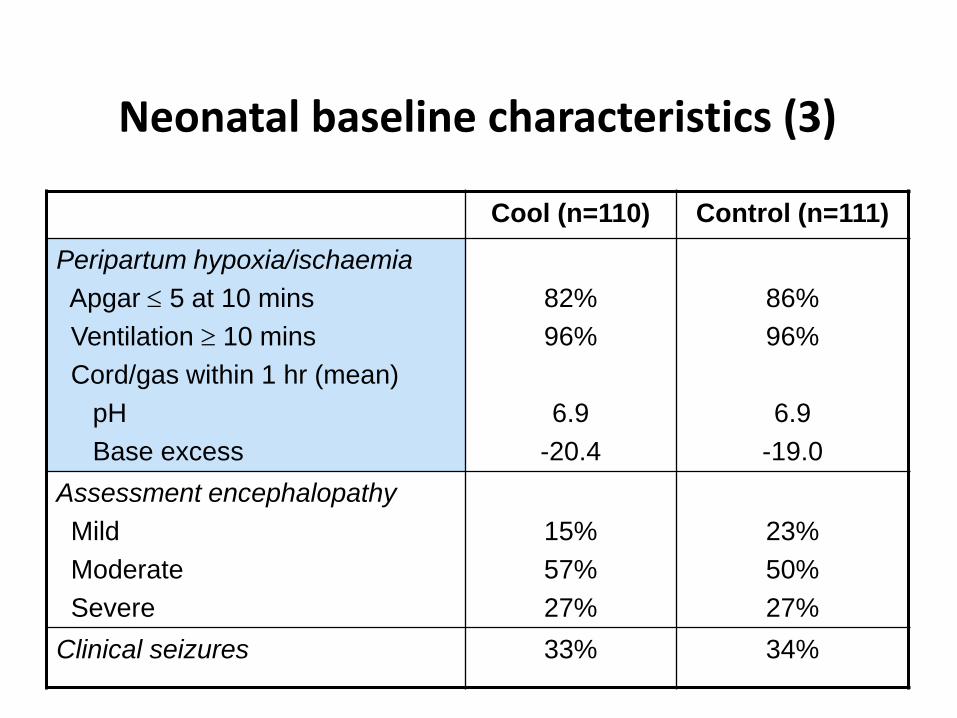
Neonatal baseline characteristics (3)
Cool (n=110) Control (n=111)
Peripartum hypoxia/ischaemia
Apgar 5 at 10 mins
Ventilation 10 mins
Cord/gas within 1 hr (mean)
pH
Base excess
82%
96%
6.9
-20.4
86%
96%
6.9
-19.0
Assessment encephalopathy
Mild
Moderate
Severe
15%
57%
27%
23%
50%
27%
Clinical seizures 33% 34%
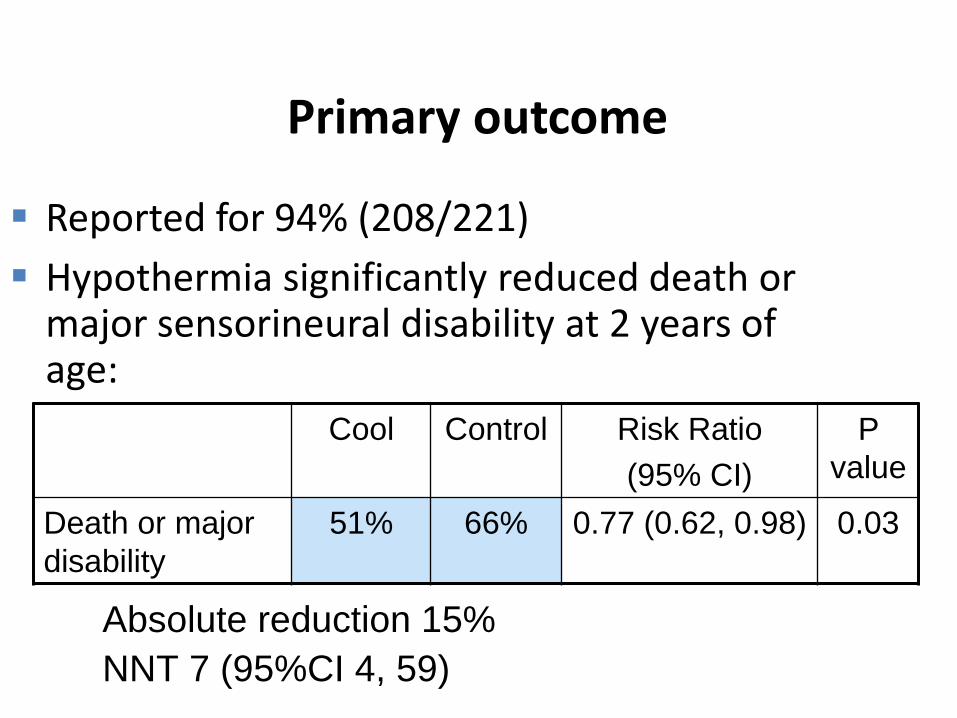
Primary outcome
Reported for 94% (208/221)
Hypothermia significantly reduced death or major sensorineural disability at 2 years of age:
Cool Control Risk Ratio
(95% CI)
P
value
Death or major
disability
51% 66% 0.77 (0.62, 0.98) 0.03
Absolute reduction 15%
NNT 7 (95%CI 4, 59)

Secondary outcomes: Mortality
Hypothermia significantly reduced mortality
Cool Control Risk Ratio (95%
CI)
P
value
Death 25% 39% 0.65 (0.43, 0.97) 0.04
Absolute reduction 14%
NNT 7
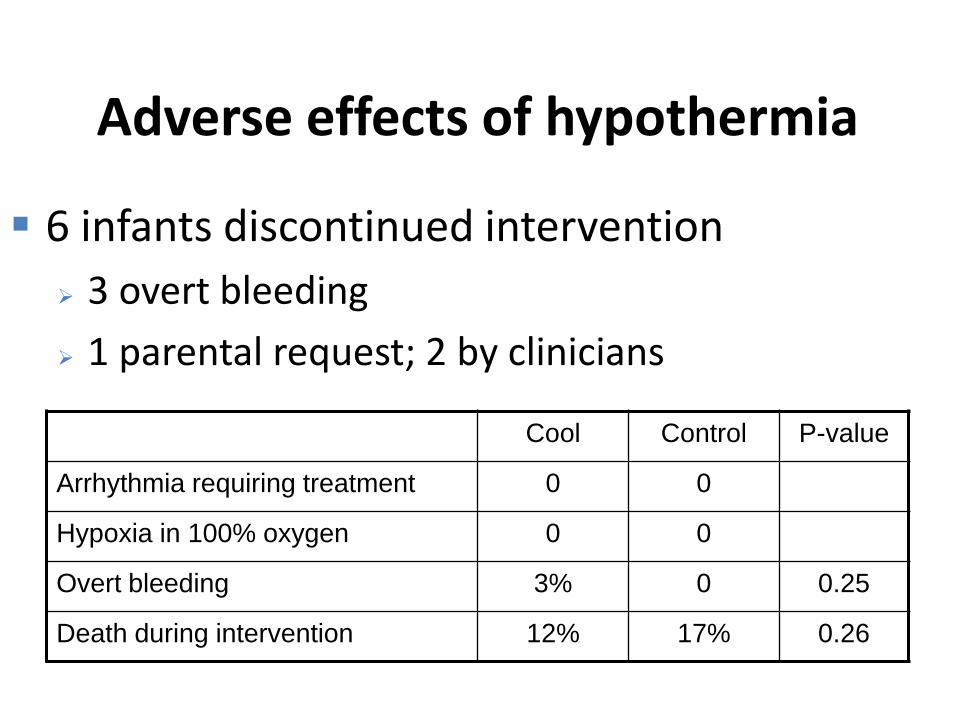
Adverse effects of hypothermia
6 infants discontinued intervention
3 overt bleeding
1 parental request; 2 by clinicians
Cool Control P-value
Arrhythmia requiring treatment 0 0
Hypoxia in 100% oxygen 0 0
Overt bleeding 3% 0 0.25
Death during intervention 12% 17% 0.26
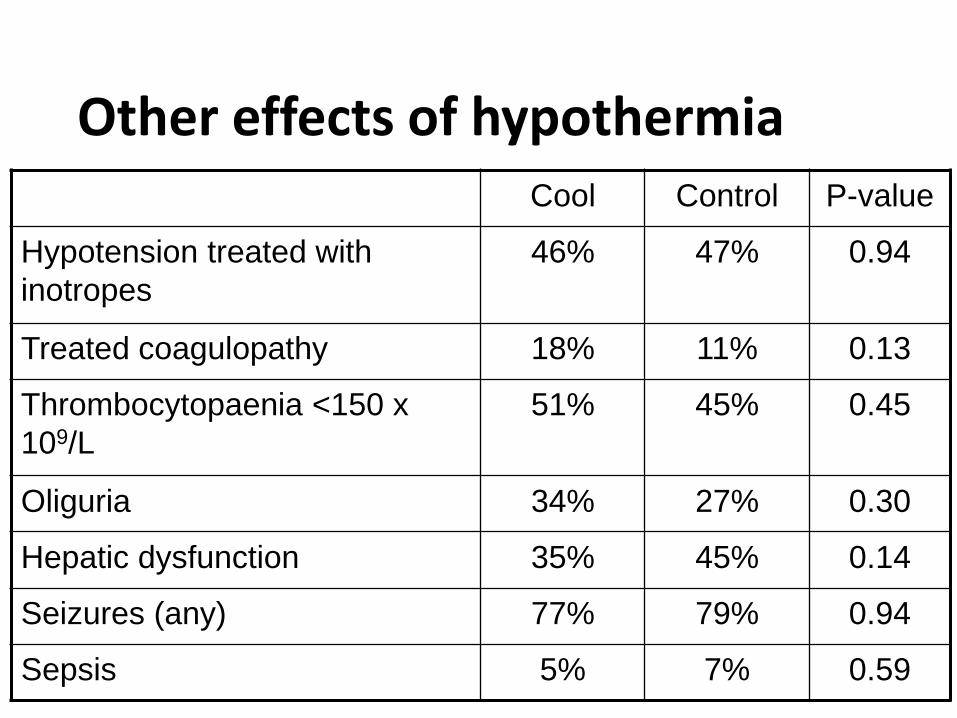
Other effects of hypothermia Cool Control P-value
Hypotension treated with
inotropes
46% 47% 0.94
Treated coagulopathy 18% 11% 0.13
Thrombocytopaenia <150 x
109/L
51% 45% 0.45
Oliguria 34% 27% 0.30
Hepatic dysfunction 35% 45% 0.14
Seizures (any) 77% 79% 0.94
Sepsis 5% 7% 0.59
Strengths of ICE
Whole body therapeutic hypothermia is beneficial No major adverse effects Results consistent with other RCTs &
meta-analyses Only ‘larger’ RCT to report safety &
outcomes of hypothermia initiated at the birth hospital, continued during retrieval & transport to the tertiary NICU
ICE Conclusions
ICE method is effective, safe and widely applicable: Identifies infants with HIE at risk of
adverse outcome soon after birth Uses a simple, inexpensive method of
whole body hypothermia Could be used in non-tertiary settings
whilst awaiting retrieval and during transport to the regional NICU
Systematic reviews & meta-analyses
• 7 reviews published
• Cochrane review ‘Cooling for newborns with HIE’ updated July 2007
• Today updated to include 12 RCT’s & 1504 term newborns with moderate or severe HIE
– 7 trials of whole-body cooling
– 5 trials of selective head cooling
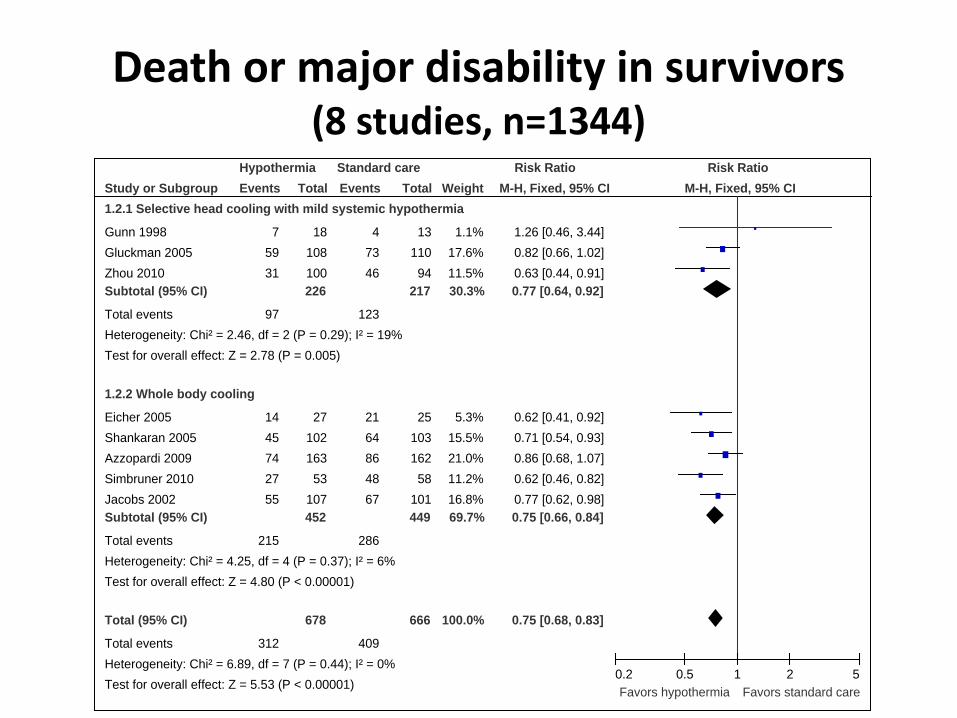
Death or major disability in survivors (8 studies, n=1344)
Study or Subgroup
1.2.1 Selective head cooling with mild systemic hypothermia
Gunn 1998
Gluckman 2005
Zhou 2010
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 2.46, df = 2 (P = 0.29); I² = 19%
Test for overall effect: Z = 2.78 (P = 0.005)
1.2.2 Whole body cooling
Eicher 2005
Shankaran 2005
Azzopardi 2009
Simbruner 2010
Jacobs 2002
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 4.25, df = 4 (P = 0.37); I² = 6%
Test for overall effect: Z = 4.80 (P < 0.00001)
Total (95% CI)
Total events
Heterogeneity: Chi² = 6.89, df = 7 (P = 0.44); I² = 0%
Test for overall effect: Z = 5.53 (P < 0.00001)
Events
7
59
31
97
14
45
74
27
55
215
312
Total
18
108
100
226
27
102
163
53
107
452
678
Events
4
73
46
123
21
64
86
48
67
286
409
Total
13
110
94
217
25
103
162
58
101
449
666
Weight
1.1%
17.6%
11.5%
30.3%
5.3%
15.5%
21.0%
11.2%
16.8%
69.7%
100.0%
M-H, Fixed, 95% CI
1.26 [0.46, 3.44]
0.82 [0.66, 1.02]
0.63 [0.44, 0.91]
0.77 [0.64, 0.92]
0.62 [0.41, 0.92]
0.71 [0.54, 0.93]
0.86 [0.68, 1.07]
0.62 [0.46, 0.82]
0.77 [0.62, 0.98]
0.75 [0.66, 0.84]
0.75 [0.68, 0.83]
Hypothermia Standard care Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favors hypothermia Favors standard care
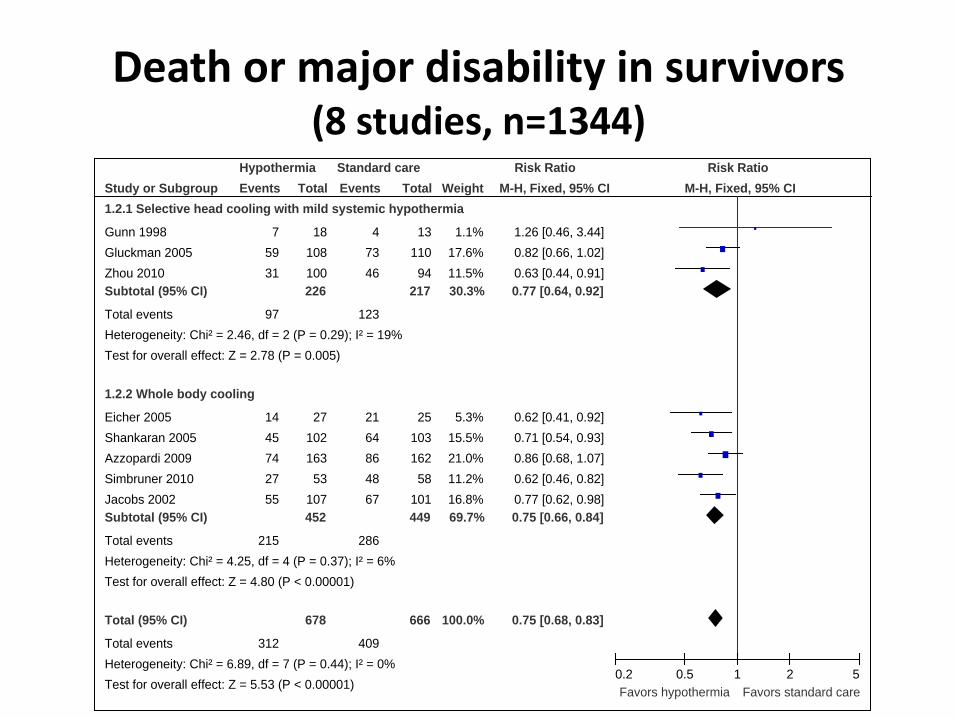
Death or major disability in survivors (8 studies, n=1344)
Study or Subgroup
1.2.1 Selective head cooling with mild systemic hypothermia
Gunn 1998
Gluckman 2005
Zhou 2010
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 2.46, df = 2 (P = 0.29); I² = 19%
Test for overall effect: Z = 2.78 (P = 0.005)
1.2.2 Whole body cooling
Eicher 2005
Shankaran 2005
Azzopardi 2009
Simbruner 2010
Jacobs 2002
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 4.25, df = 4 (P = 0.37); I² = 6%
Test for overall effect: Z = 4.80 (P < 0.00001)
Total (95% CI)
Total events
Heterogeneity: Chi² = 6.89, df = 7 (P = 0.44); I² = 0%
Test for overall effect: Z = 5.53 (P < 0.00001)
Events
7
59
31
97
14
45
74
27
55
215
312
Total
18
108
100
226
27
102
163
53
107
452
678
Events
4
73
46
123
21
64
86
48
67
286
409
Total
13
110
94
217
25
103
162
58
101
449
666
Weight
1.1%
17.6%
11.5%
30.3%
5.3%
15.5%
21.0%
11.2%
16.8%
69.7%
100.0%
M-H, Fixed, 95% CI
1.26 [0.46, 3.44]
0.82 [0.66, 1.02]
0.63 [0.44, 0.91]
0.77 [0.64, 0.92]
0.62 [0.41, 0.92]
0.71 [0.54, 0.93]
0.86 [0.68, 1.07]
0.62 [0.46, 0.82]
0.77 [0.62, 0.98]
0.75 [0.66, 0.84]
0.75 [0.68, 0.83]
Hypothermia Standard care Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favors hypothermia Favors standard care

Mortality (12 studies, n=963)

Disability in survivors assessed (8 studies, n=917)
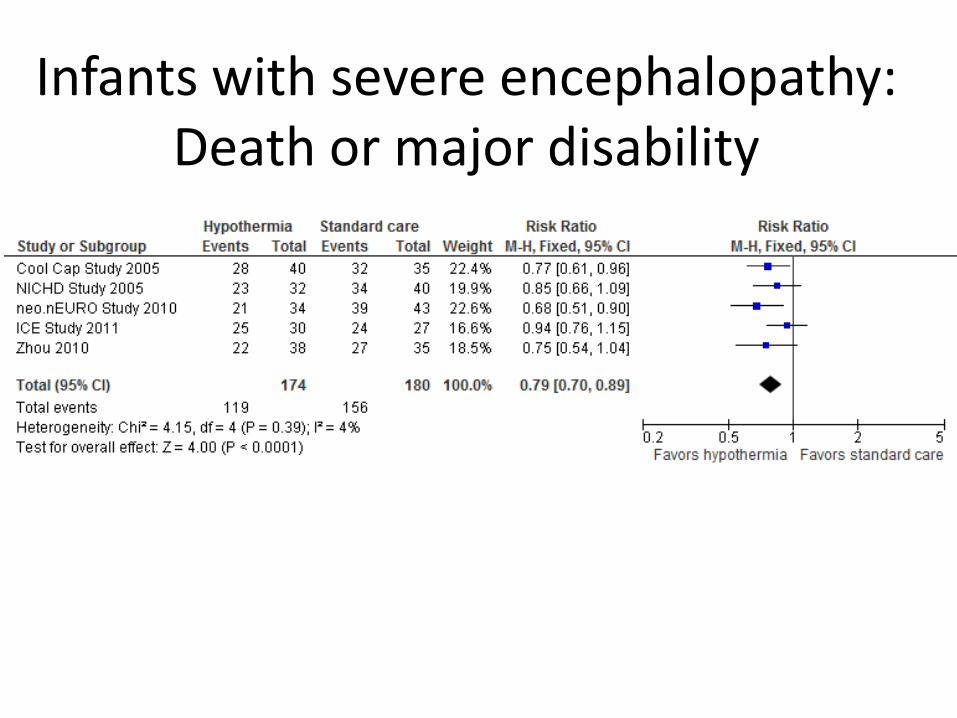
Infants with severe encephalopathy: Death or major disability
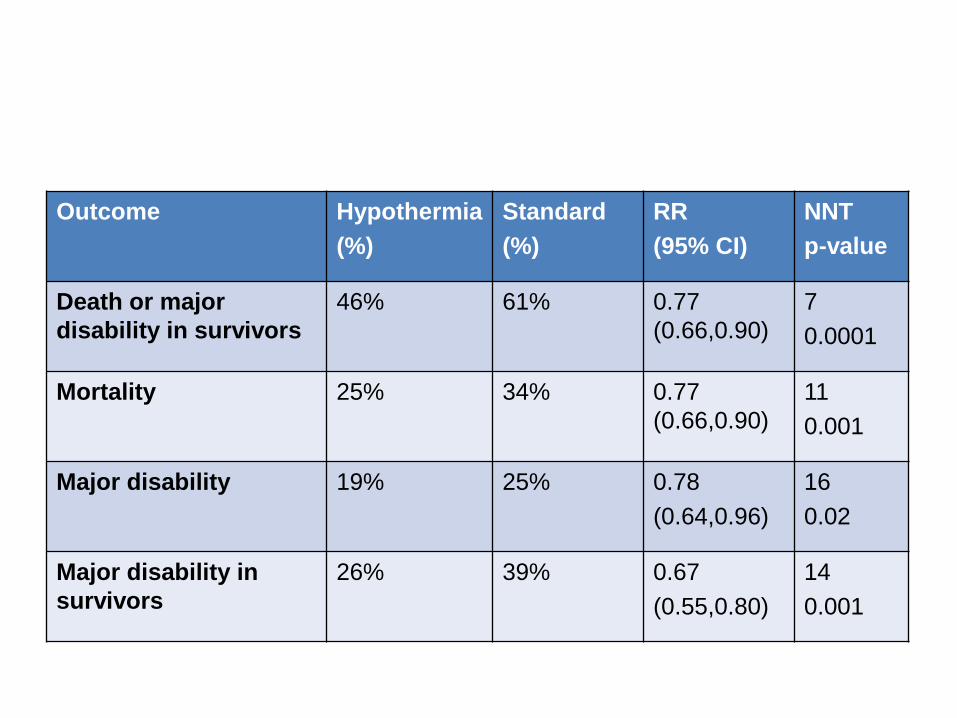
Outcome Hypothermia
(%)
Standard
(%)
RR
(95% CI)
NNT
p-value
Death or major
disability in survivors
46% 61% 0.77
(0.66,0.90)
7
0.0001
Mortality 25% 34% 0.77
(0.66,0.90)
11
0.001
Major disability 19% 25% 0.78
(0.64,0.96)
16
0.02
Major disability in
survivors
26% 39% 0.67
(0.55,0.80)
14
0.001
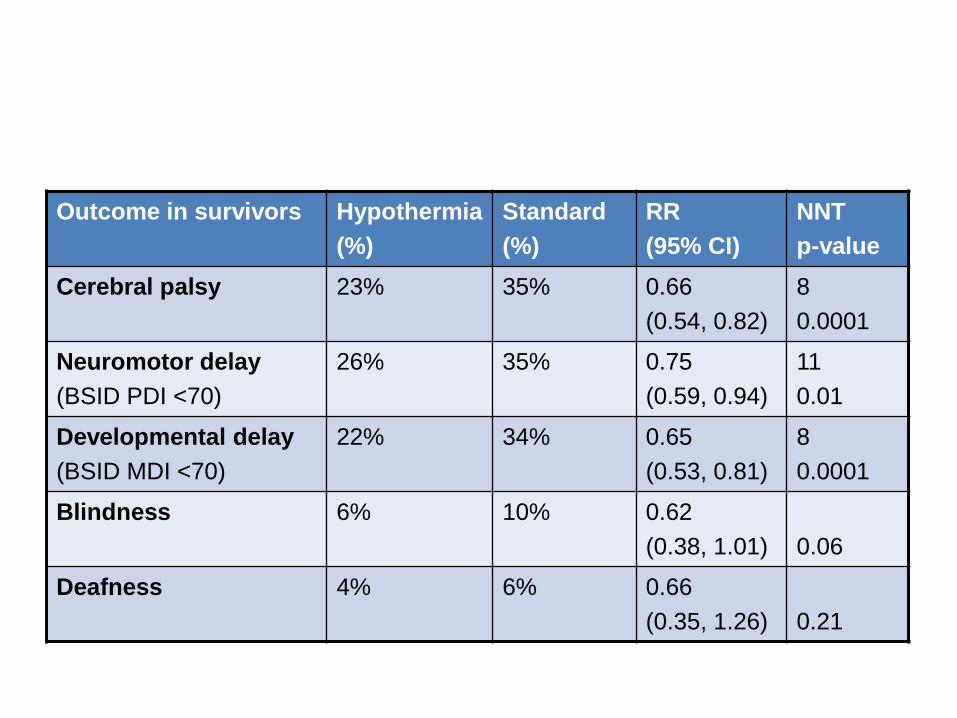
Outcome in survivors Hypothermia
(%)
Standard
(%)
RR
(95% CI)
NNT
p-value
Cerebral palsy 23% 35% 0.66
(0.54, 0.82)
8
0.0001
Neuromotor delay
(BSID PDI <70)
26% 35% 0.75
(0.59, 0.94)
11
0.01
Developmental delay
(BSID MDI <70)
22% 34% 0.65
(0.53, 0.81)
8
0.0001
Blindness 6% 10% 0.62
(0.38, 1.01)
0.06
Deafness 4% 6% 0.66
(0.35, 1.26)
0.21
Cochrane review summary
• When used within strict protocols in tertiary NICUs, therapeutic hypothermia is beneficial to near-term newborns with moderate or severe HIE. – Cooling reduces mortality and major disability.
– The benefits of cooling on survival and neurodevelopment outweigh the short term adverse effects (sinus bradycardia, thrombocytopaenia).
– Whole-body and selective head cooling both effective.
In 1997….
‘Hypothermia is the most promising option for a clinically feasible neural rescue therapy in encephalopathic newborns following acute perinatal asphyxia’
Thoresen and Wyatt. Acta Paediatr 1997;86:1029-33
In 2014
• Therapeutic hypothermia improves outcome after moderate or severe HIE. – But, 46% of cooled infants still die or survive with
major disability.
• Further strategies are needed: – Regional guidelines to facilitate earlier induction
of cooling
– Refinement of current hypothermia methods
– Synergistic neuroprotective therapies

ILCOR 2010 Treatment Recommendation
• Term and near-term with moderate to severe HIE should be offered cooling
• Whole body and selective head cooling are both appropriate
• Cooling should be initiated and conducted in neonatal intensive care facilities using the protocols used in the RCTS (begin within 6 hours of birth, continue for 72 hours after birth, and rewarm over at least 4 hours).
• Monitor for adverse effects: thrombocytopenia and hypotension
• All treated infants should be followed up longitudinally

http://www.healthynewbornnetwork.org/
Gaps in newborn resuscitation in resource-limited settings
Gaps in the evidence
Cord clamping
Timing
Positive pressure ventilation
Best interface
Optimal ventilation parameters
Others
Simple ways to administer blended oxygen
Thermal management of asphyxiated infant
Problems and solutions
• Most of the burden of illness occurs in resource limited settings
• Most of the evidence comes from the developed world
So ...
• Should facilitate/support research in the developing world
• Community based interventions are very important – But once NMR < 25-30 per 1000 live births
hospital based therapies are required to gain further improvements
• Small part of the puzzle – use what we know to improve their outcomes
Barriers to application in resource limited settings
• Lack of suitable cooling equipment ($)
• Lack of skilled personnel
• Higher rates of sepsis (neutrophil function)
• Lack of facilities for disabled children
• Lack of ventilatory support
Effectiveness vs efficacy
• Can accurate/reliable cooling be achieved with ice packs and passive cooling?
• Does this method of cooling improve long term outcomes?
• Is it safe?
– Infection
– Coagulopathy
– ...
What is “resource limited”?
• A continuous rather than dichotomous variable e.g. China, South Africa ...
• Self defined?
• All of us?
• What resources are needed to safely cool?
Evidence pertinent to resource limited settings
• 4 RCTs
– ICE Trial: gel packs, advanced setting
– Bharadwaj (2012) India: gel packs
– Thayyil (2013) India: phase changing material mattress
– Robertson (2011, 2008) Uganda: water bottles
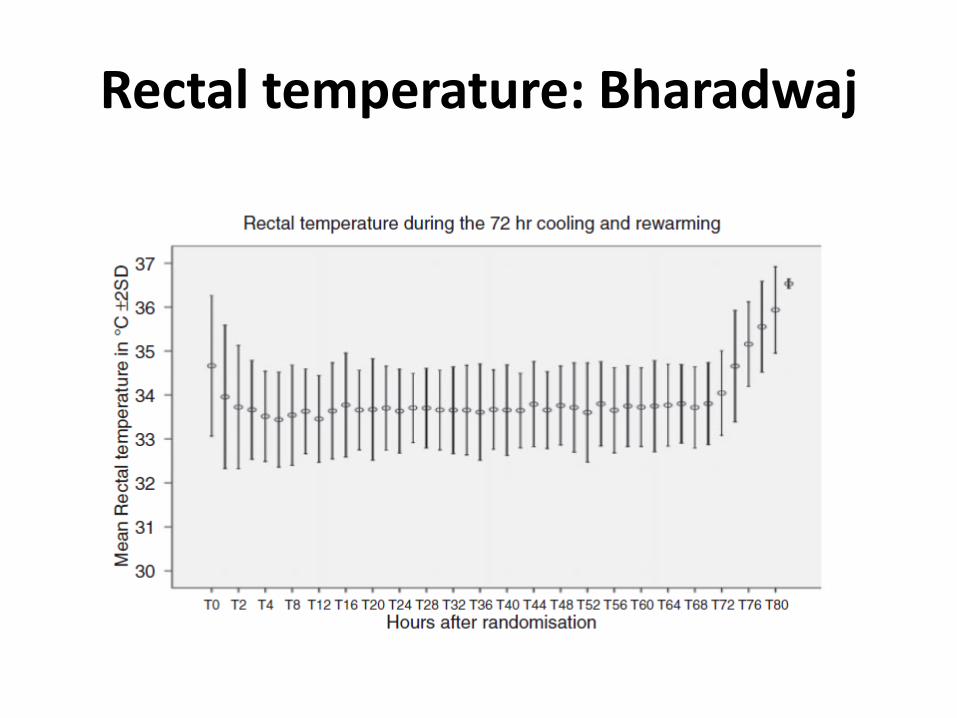
Rectal temperature: Bharadwaj
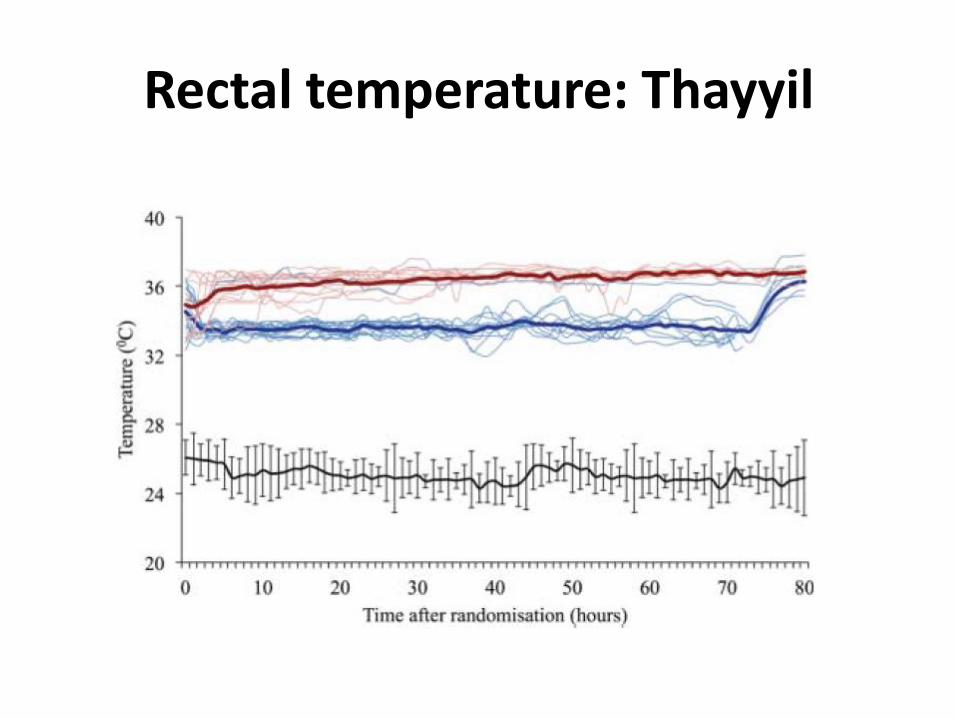
Rectal temperature: Thayyil
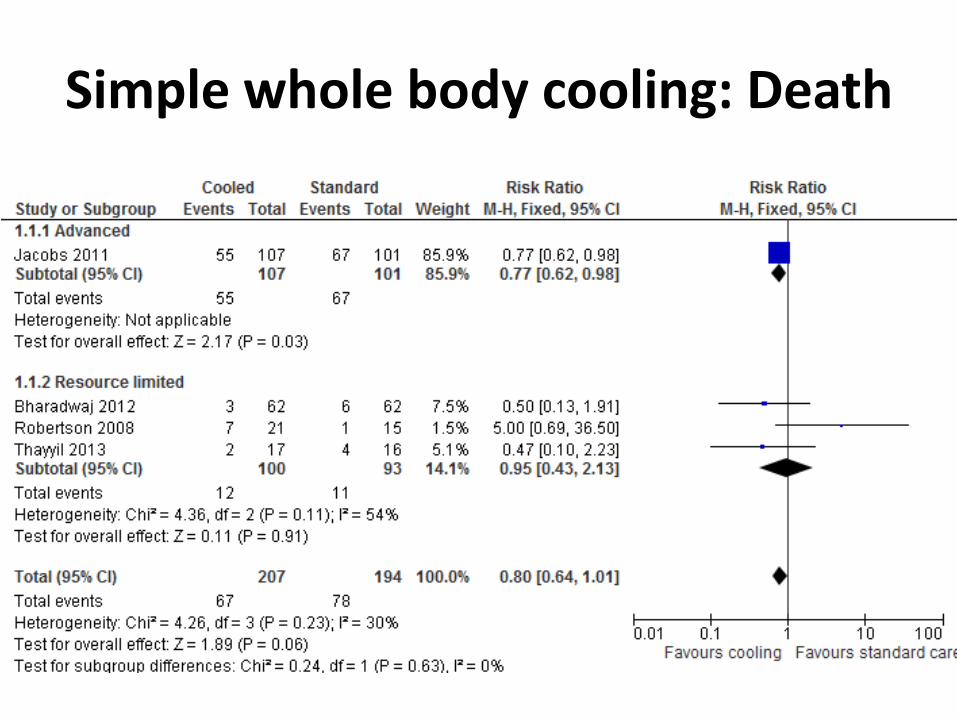
Simple whole body cooling: Death
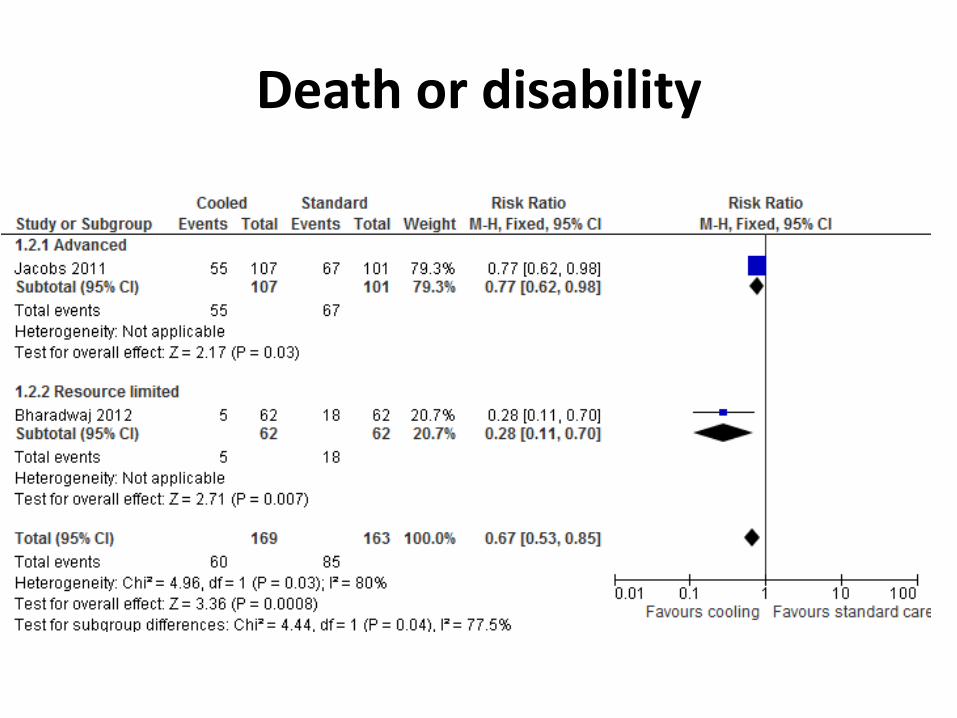
Death or disability
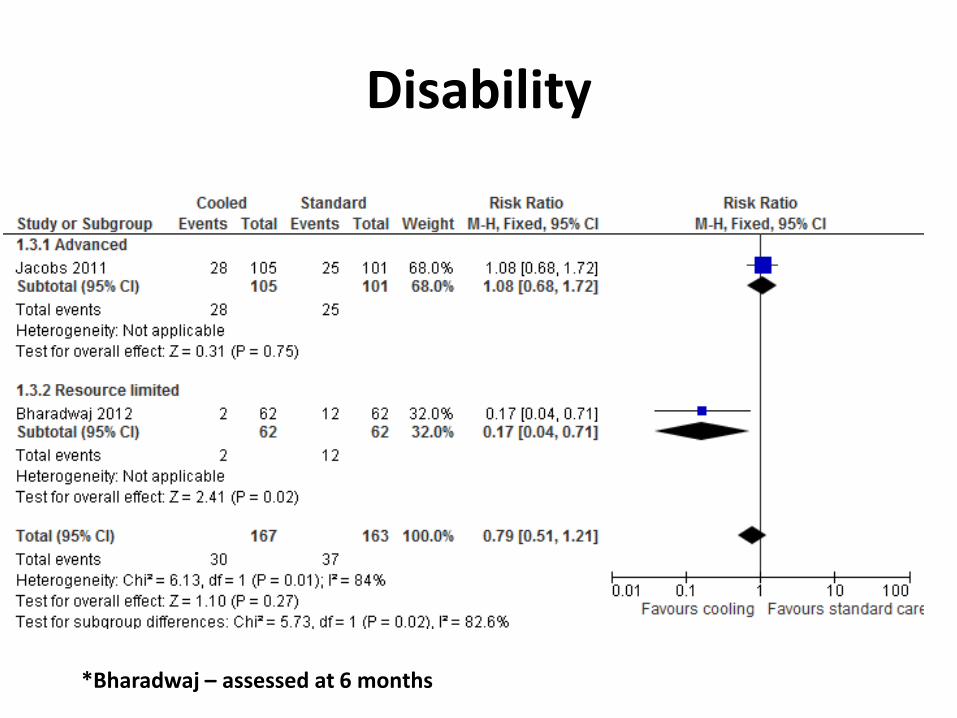
Disability
*Bharadwaj – assessed at 6 months
Results
• Simple cooling delivers reasonably precise and accurate whole body hypothermia
• The technique reduces death (and death or disability) in a developed world setting (ICE)
• No evidence of benefit or harm (mortality) in resource limited setting
Conclusions
• Insufficient evidence for effectiveness or safety in resource limited settings -- therefore cooling not recommended outside RCT
• (opportunity cost=money spent on cooling could be spent better on prevention)
OR
Conclusions
• The treatment is efficacious and safe(ish). No evidence of harm, small trials underpowered, therefore cool and audit the results.
OR
Conclusions
• Define the resources required to safely cool and let units decide where they fit – Intravenous fluids
– Supplemental oxygen
– Anticonvulsants
– Antibiotics
– Adequate trained staff
– Pathology: glucose, electrolytes, coagulation studies

Top Related