




Languages
Pages
Legal


Nephrogenic Systemic Fibrosis
高雄長庚腎臟科 Fellow 2 王奕淳
VS 莊峰榮 & Chief 李建德2009.10.14
Kidney forum

Question
什麼是 NSF?
Gadolinium 會導致 NSF 嗎 ?
腎功能多差時要避免Gadolinium?
Gadolinium 需要預防性洗腎 ?

Q: 什麼是 NSF?

NSF: Clinical
Patients with renal insufficiency
Swelling of distal parts of the extremities
Subsequent thickening, indurations and hardening of the skin
Distinct nodules
Kidney International (2007) 72, 260–264

NSF: Clinical
The distal extremities are the most common area of involvement
Followed by the trunk.
The face is almost never involved.
Kidney International (2007) 72, 260–264

Diffuse thickening, induration, and hyperpigmentation of lower legs with inhibition ofjoint flexion.

Diffuse swelling of the skin, erythematous papules andnodules

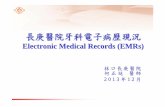
NSF :Skin biopsy
Thickened dermis
Bundles of collagen
Surrounding clefts
Mucin deposition
Proliferation of fibroblasts
Proliferation of elastic fibers
No inflammation
Kidney International (2007) 72, 260–264
The dermis is thickened and demonstrates swollen collagenbundles with surrounding clefts and spindle cell proliferation. Interstitial mucin deposition is frequently present
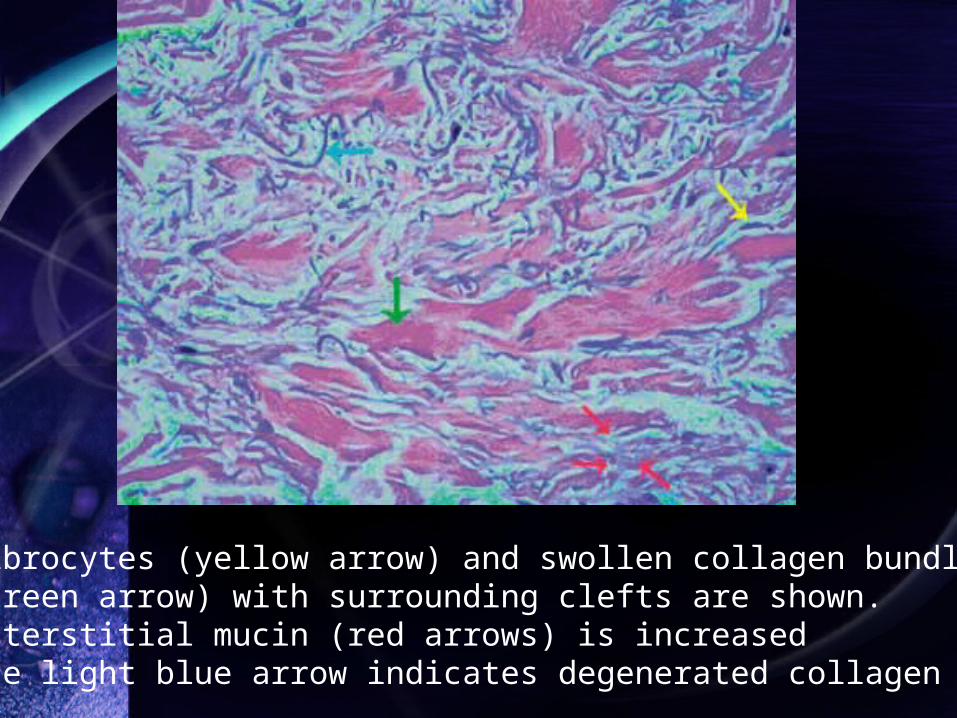
Fibrocytes (yellow arrow) and swollen collagen bundles(green arrow) with surrounding clefts are shown.Interstitial mucin (red arrows) is increasedThe light blue arrow indicates degenerated collagen fibers

Q: Gadolinium會導致 NSF 嗎 ?

NSF: History
1997: Recognition NSF
2000: First description in literature
2006: (NDT) 5 patients received MRI and subsequently developed NSF within 2–4 weeks.
2006 (JASN) 13 patients acquire NSF when exposed to gadodiamide (OR 32.5)
2007 FDA Warning
Kidney International (2007) 72, 260–264

FDA Warning
[Posted 05/23/2007]
Risk for NSF following exposure to GBCA
Acute or chronic severe renal insufficiency (GFR <30 mL/min/1.73m2)
Acute renal insufficiency of any severityHepato-renal syndrome
Peri-operative liver transplantation period.

FDA Warning
Healthcare professionals should avoid the use of a GBCA in these patients
Unless diagnostic information is essential and not available with non-contrast enhanced MRI

Radiology: Volume 245: Number 1—October 2007
A retrospective analysis was performed of all adult patients undergoing dialysis in the west of Scotland between January1, 2000, and July 1, 2006

Patient
All patients who underwent renal replacement therapy (RRT) for established chronic renal failure (stage 5 chronic kidney disease, estimated GFR <15 mL/min)
Results
14 of 1826 patients had NSF13/14 (93%) undergone gadolinium enhanced MRI
408/1812 (22.5%) unaffected
(P <001)

Conclusion
The data support a positive association between gadolinium based contrast agent administration and development of nephrogenic systemic fibrosis in the established renal failure population


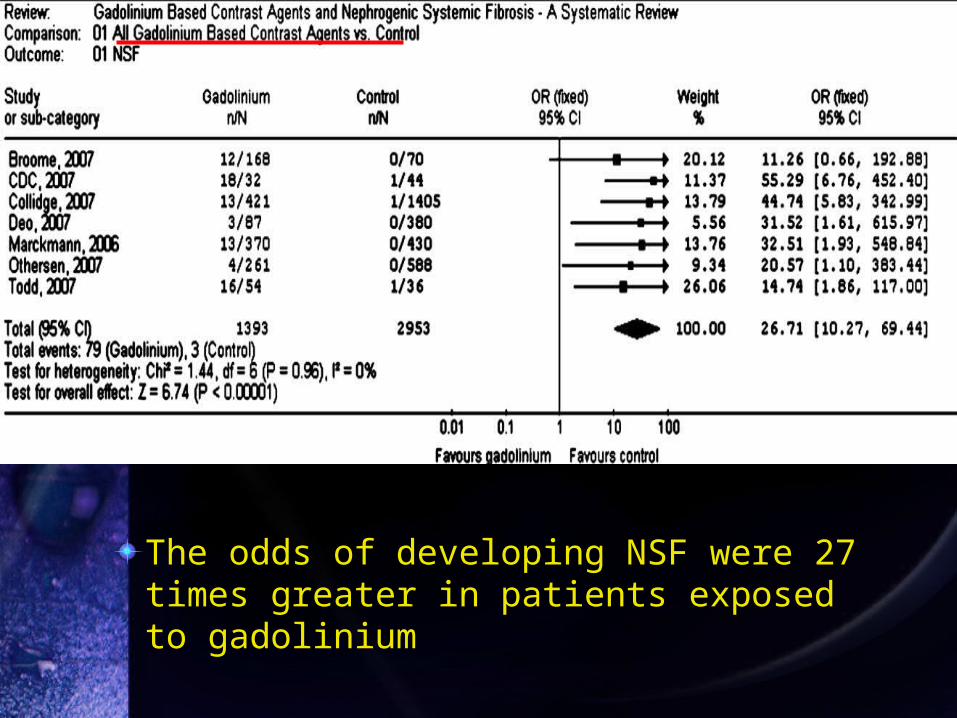
The odds of developing NSF were 27 times greater in patients exposed to gadolinium

The odds of developing NSF were 20 times greater in patients exposed to gadodiamide

Conclusion
The current state of evidence suggests an association and potentially causal link between the use of GBCAs and the development of NSF among patients with advanced kidney disease

Q: 腎功能多差時要避免Gadolinium?

Gadolinium
Patient Half life
Healthy volunteers 1.3 hr
Chronic renal failure 30–120 hr
Hemodialysis 2.6 hr
Peritoneal dialysis 52.7 hr
Kidney International (2007) 72, 260–264

NSF in CKD
Prevalence of NSFStage 1–4 CKD: 0%
Stage 5 CKD of 18%
Invest Radiol 2008; 43: 141–144

NSF in CKD
NSF has been observed in up to 18% of patients receiving chronic haemodialysis
May occur in individuals with stages 3 and 4 chronic kidney disease
Occasionally in individuals who had experienced acute renal failure
Ann Rheum Dis 2008;67(Suppl III):iii66–iii69.

American College of Radiology (ACR)
In patients with stage 3 or moderate CKD, the ACR noted that there were insufficient data to make any recommendations
Cleve ClinJ Med 2008; 75: 95–97

FDA & ACR
FDA and the ACR both recommend
Withholding all GBCAs in CKD stage 4–5 (GFR<30 mL/min/1.73m2)
Kidney International (2007) 72, 260–264

The journal of urology 180, 830-835, September 2008

Kidney International (2009) 75, 465–474
Safety studies, including USPIO administration (ferumoxytol) as iron supplement therapy in CKD patients on and not on dialysis, suggest that decreased kidney functiondoes not alter the safety profile.

Q: Gadolinium 需要預防性洗腎 ?

Prophylactic HD for NSF
Three patients have been described who developed NSF developed despite daily hemodialysis for 3 days immediately following gadodiamide exposure
Am J Roentgenol 2007;188(2):586–592.

Prophylactic HD for NSF
Patients who received hemodialysis within 24 hours still developed NSF.
Absence of controls, investigators could not ascertain whether the risk and severity of the NSF was reduced.
Hemodialysis was not started until at least 9 hours postexposure.
Fundam Clin Pharmacol. 2006;20:563-576.

Radiologist’s view
If there is no alternative to the use of gadodiamide
The lowest diagnostic dose should be used
Prompt dialysis after imaging may facilitate removal of gadodiamide
Radiology: Volume 245: Number 1—October 2007

FDA’s view
If patients with severe CKD need GBCAs
Prompt haemodialysis following contrast administration should be considered
http://www.fda.gov/CDER/drug/InfoSheets/HCP/gcca 00612HCP.htm

ACR’s view
Prophylactic use of dialysis be warranted only in patients who were already on dialysis.
For patients not already on haemodialysis (e.g. stage 3 or 4 CKD) =>The risks of initiating haemodialysis should be weighed against that of developing NSF
Am J Roentgenol 2007; 188: 1447–1474

Question
Gadolinium 會導致 NSF 嗎 ? =>Yes!腎功能多差時要避免 Gadolinium?
=>Stage 4-5 (FDA)Gadolinium 需要預防性洗腎 ?
=>Stage 5!, Stage 3-4?(ACR)

Conclusion
Potentially causal link between GBCAs and development of NSF among patients with advanced kidney diseaseWithholding all GBCAs in CKD stage 4–5 (GFR<30 mL/min/1.73m2)USPIOs such as ferumoxytol as an alternative to GBCA in patients at risk for NSFProphylactic use of dialysis after GBCAs in patients who were already on dialysis

Thanks for your attention!
Top Related