







Languages
Pages
Legal

L’insuffisance cardiaque en ambulatoire
LL’’ insuffisance cardiaque en insuffisance cardiaque en ambulatoireambulatoire
P. JourdainUnité Thérapeutique d’Insuffisance Cardiaque,
CH R Dubos, 95300 Pontoise.
CNCH 2010
Insuffisance cardiaque : un problème médical croissant
• 970 000 admissions/an aux États-Unis avec diagnostic primaire d'insuffisance cardiaque 1, 2 (130 000 en France d’après les données du PMSI 2005). Entre 500 et 800.000 français atteints
• 3 000 000 admissions/an aux États-Unis avec diagnostic primaire ou secondaire d'insuffisance cardiaque 1
1 Haldeman GA et al. Am Heart J. 1999; 137: 3522 American Heart Association. Heart and Stroke Statistics. Mise à jour 2004. 2003 : 193 ESC Task Force. Eur Heart J. 2001; 22: 1527
Prévalence Incidence MortalitéSorties d'hôpital
Coût
Europe3 10 000 000 500 000
50 % sous 5 ans
1 000 000
États-Unis
5 000 000 550 000 1 000 000
24,3 milliards
de dollars
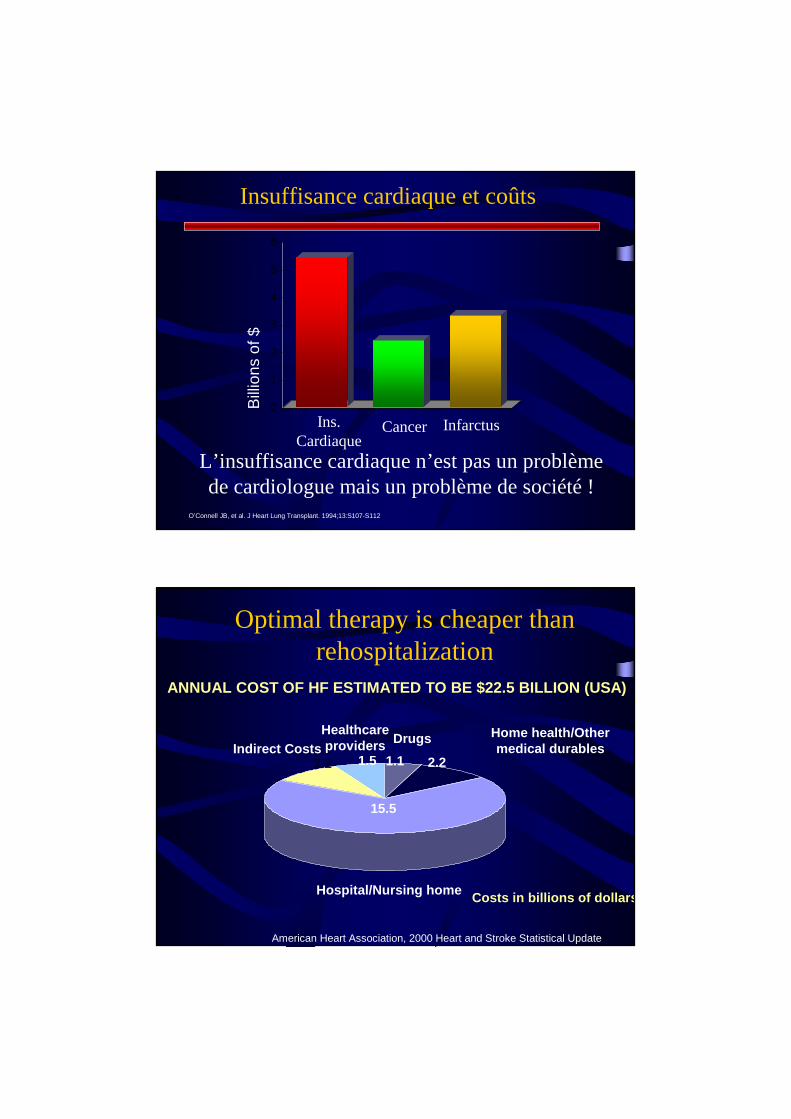
Insuffisance cardiaque et coûts
Bill
ions
of $
O’Connell JB, et al. J Heart Lung Transplant. 1994;13:S107-S112..
0
1
2
3
4
5
6
Ins. Cardiaque
Cancer Infarctus
L’insuffisance cardiaque n’est pas un problème de cardiologue mais un problème de société !
Optimal therapy is cheaper thanrehospitalization
American Heart Association, 2000 Heart and Stroke Statistical Update
Hospital/Nursing home
HealthcareprovidersIndirect Costs
Home health/Othermedical durables
15.5
2.2 1.5 1.1 2.2
Drugs
ANNUAL COST OF HF ESTIMATED TO BE $22.5 BILLION (USA)
Costs in billions of dollars
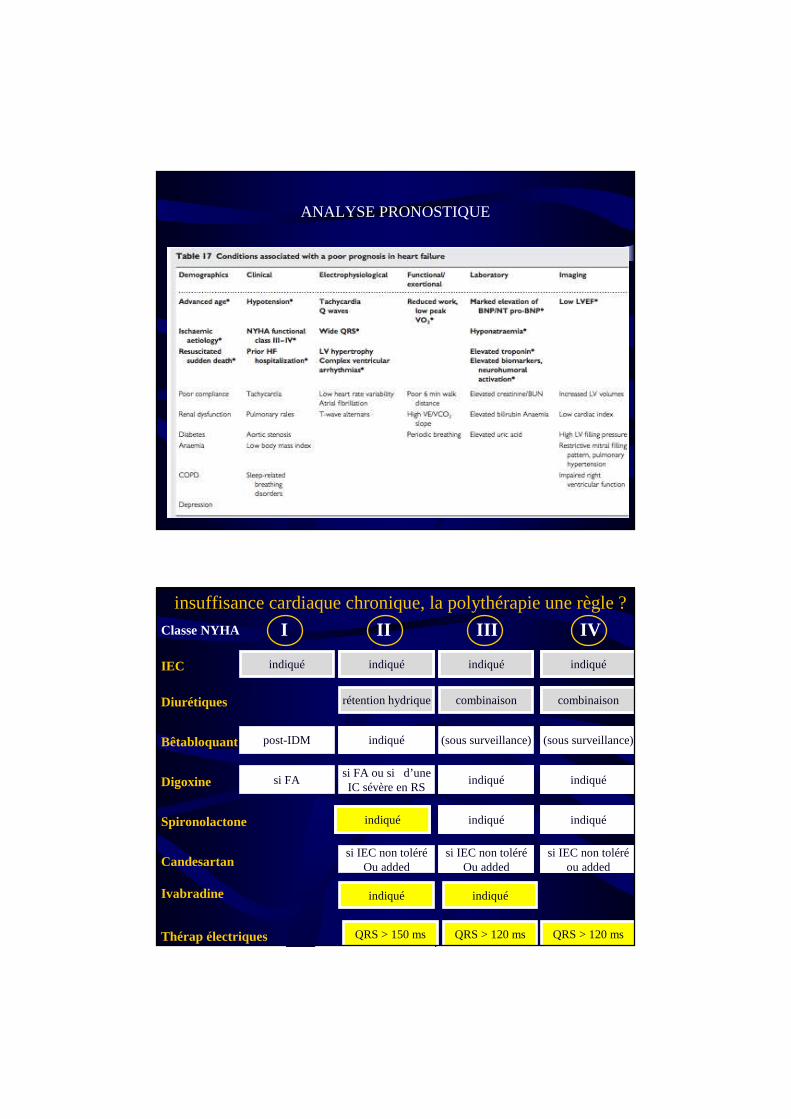
ANALYSE PRONOSTIQUE
insuffisance cardiaque chronique, la polythérapie une règle ?
rétention hydrique combinaison
(sous surveillance)
si FA ou si d’uneIC sévère en RS
I II III IVClasse NYHA
IEC
Diurétiques
Bêtabloquant
Digoxine
Spironolactone
Candesartan
post-IDM
si FA
indiqué
si IEC non toléréOu added
combinaison
(sous surveillance)
si IEC non toléréOu added
si IEC non toléréou added
indiqué indiqué indiqué
indiqué
indiqué indiqué
indiquéindiquéindiqué
Ivabradine indiquéindiqué
Thérap électriques QRS > 150 ms QRS > 120 ms QRS > 120 ms
En pratique… jusqu’ou…Traiter l’OAP, c’est bien mais
prévenir c’est mieux…
Nos missions
• Assurer ou faciliter le suivi
• Optimiser les thérapeutiques
• Faire le bilan pronostic
• Faire bénéficier les patients d’une ETP de qualité.
• Faciliter la réadaptation.
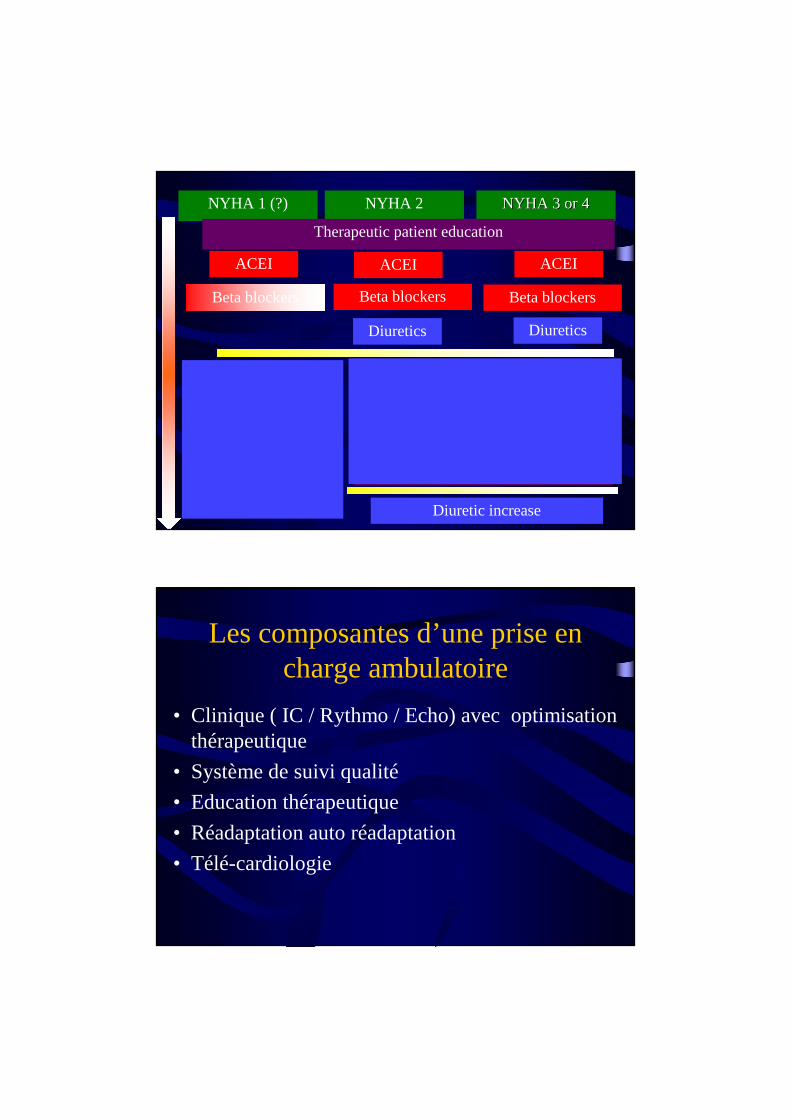
ACEI
Ivabradine
Anti aldostéroneARB 2ARB 2
Beta blockers
NYHA 2 NYHA 3 or 4NYHA 3 or 4NYHA 1 (?)
Pacemaker (resynchronization)
Therapeutic patient education
Réadaptation
ACEI ACEI
Beta blockers Beta blockers
Diuretics
Ivabradine
Heart rateHeart rateRenal functionRenal function
QRS wideQRS wideComplianceCompliance
Risk stratificatRisk stratificat°°(Echo (Echo BNP, Vo2,BNP, Vo2,……))
Diuretics
Diuretic increase
Les composantes d’une prise en charge ambulatoire
• Clinique ( IC / Rythmo / Echo) avec optimisation thérapeutique
• Système de suivi qualité
• Education thérapeutique
• Réadaptation auto réadaptation
• Télé-cardiologie

Les données règlementaires HdJ
• Hdj 450- 850 euros / passage
• Équipe identifiée
• Locaux identifiés
• Pas d’urgences (forfait urgences)
• Mais… deux examens sur deux plateaux tech indépendants.
• Mais… impossibilité de prévoir la durée de surveillance.
Contrôle• SYSTEMATIQUE
• Sur dossier
• Recherche de la réalité des examens (compte rendus et images).
• Si « éducation, biologie, … » comme motivation de l’HdJ dossier recalé.
• CH remboursera le % de dossiers recalés extrapolables sur les deux précédentes années.
Hôpital de jour
• Solution séduisante.
• Solution pratique
• Permet d’avoir une équipe ambulatoire.
• Mais nécessite une attention de tous les instants et une file active importante.
• Equilibre financier nécessite une bonne gestion.
Deux possibilités:
• Création de novo:– Locaux ?
– Créations de postes
• Réaffectation des ressources:– Utilisation de chambres de MCO
– Utilisation de ressources internes
Bilan financier
• Une chambre = 3500 * (365/11) * 0,8 = 85166 euros.
• En tarif HdJ équivalent de 121 passages.
• 4 places HdJ 320 j « donnent » 860. 000 euros par an.
• Couts: IDE 25000 PH 100000 … donc fortement bénéficiaire.
Consultation d’ insuffisance cardiaque
• Nécessite moins d’investissement
• Ne permet pas de réaliser des bilans lourds
• Ne permet aucun impact financier sauf négatif.
• Sera utile lors des transfert de compétence.
• Peut s’intriquer avec l’éducation thérapeutique
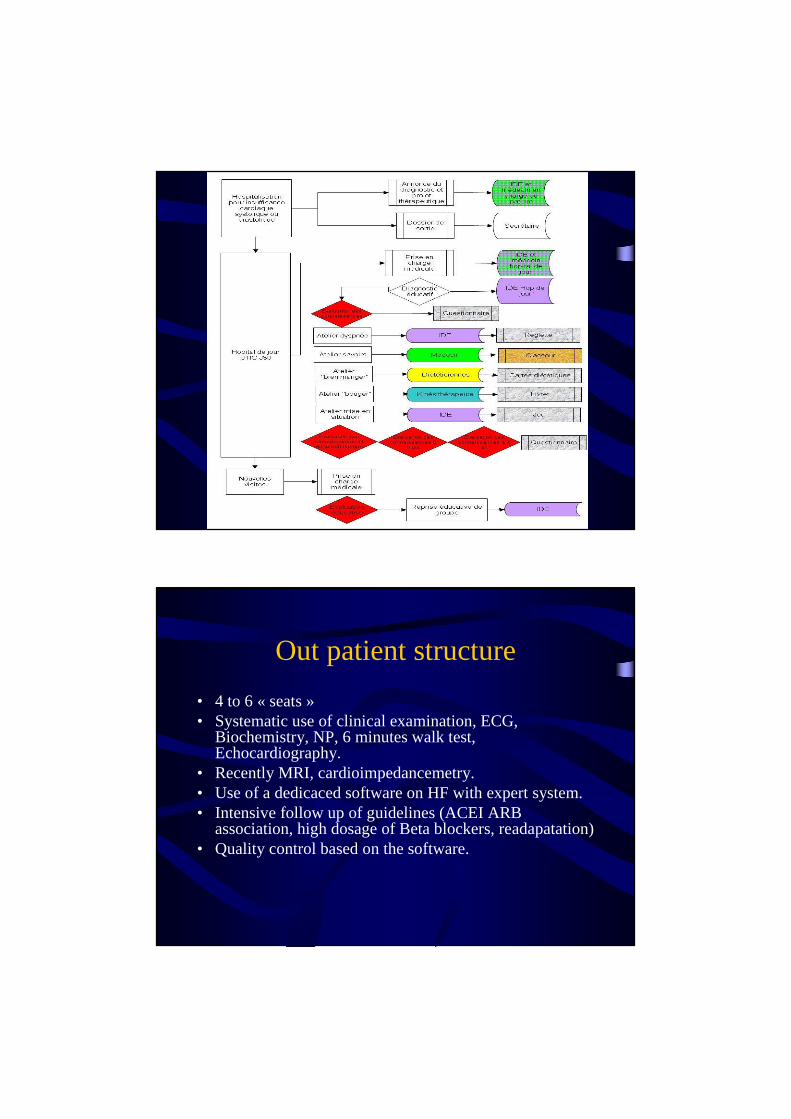
Out patient structure
• 4 to 6 « seats »• Systematic use of clinical examination, ECG,
Biochemistry, NP, 6 minutes walk test, Echocardiography.
• Recently MRI, cardioimpedancemetry.• Use of a dedicaced software on HF with expert system.• Intensive follow up of guidelines (ACEI ARB
association, high dosage of Beta blockers, readapatation)• Quality control based on the software.
Quality evaluation
• Evaluation of therapies used
• Evaluation of in hospital mortality
• Evaluation of early unplanned rehospitalizations
• Evaluation of indication of electric therapies.
• Evaluation of patient knowledge and reactions.
• Validation of Evaluation Professional practice (HAS 2006).
Mise en œuvre d’un logiciel spécifique

Prise en charge
Population
• From January 1997 to December 2007, the total number of new patients admitted for HF was 3200 (range per year: 179–377 patients).
• The population consisted of 1556 men (48.6%), with a mean age per year ranging from 68.5 ± 15.7 years to 74 ± 12.7 years;
• 53.7% of patients presented with systolic HF (LVEF < 45%), 15.4% had renal insufficiency and 20.2% had diabetes mellitus. (Concerning these characteristics, no significant differences were found from 1997 to 2007, except for renal insufficiency)
• Regarding treatments, after index hospitalization, 82% of patients received renin-angiotensin system blockers and 52% of patients received beta-blockers. After outpatient hospitalization, 92% of patients received beta-blockers.
results
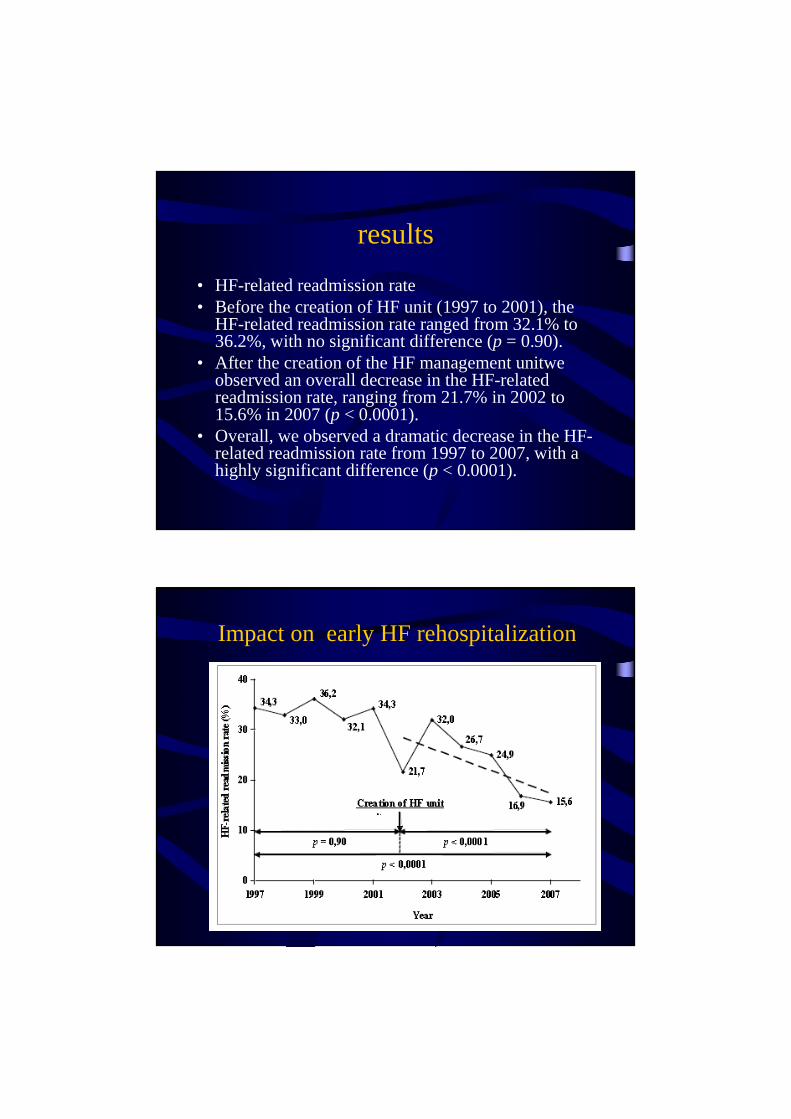
• HF-related readmission rate• Before the creation of HF unit (1997 to 2001), the
HF-related readmission rate ranged from 32.1% to 36.2%, with no significant difference (p = 0.90).
• After the creation of the HF management unitwe observed an overall decrease in the HF-related readmission rate, ranging from 21.7% in 2002 to 15.6% in 2007 (p < 0.0001).
• Overall, we observed a dramatic decrease in the HF-related readmission rate from 1997 to 2007, with a highly significant difference (p < 0.0001).
Impact on early HF rehospitalization
In hospital impact
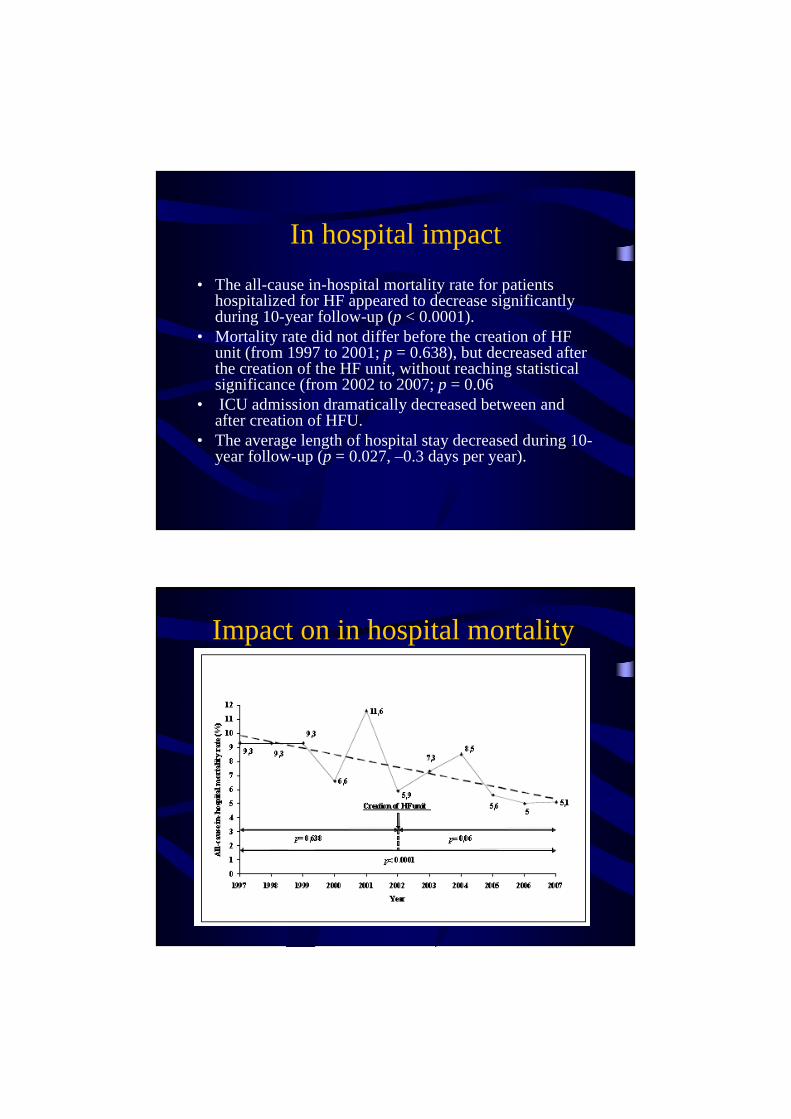
• The all-cause in-hospital mortality rate for patients hospitalized for HF appeared to decrease significantly during 10-year follow-up (p < 0.0001).
• Mortality rate did not differ before the creation of HF unit (from 1997 to 2001; p = 0.638), but decreased after the creation of the HF unit, without reaching statistical significance (from 2002 to 2007;p = 0.06
• ICU admission dramatically decreased between and after creation of HFU.
• The average length of hospital stay decreased during 10-year follow-up (p = 0.027, –0.3 days per year).
Impact on in hospital mortality
Educational structure
• Same team as for in and out patietn management.
• A « dream team » organization…• HF education (but also other educationnal
programs) systematically planned at discharge.• Educationnal disagnostic, medical knowledge,
Dietetic education, physical training, How to sessions, ….
• Evaluation and quality control.
L’éducation est un point clef pour qui sait écouter ses patients
Mais il existe des contraintes réglementaires
Accréditation ARS
• Indispensable pour faire de l’ETP a compter du 01/01/2011…
• D’ici là, les programmes existant peuvent continuer mais les nouveaux (à compter du 02/08) ne peuvent pas débuter.
• Pour les programmes interrégionaux une seule ARS suffit.
Eléments clefs
• Coordinateur médical (ou paramédical si médecin avec) formé (pas diplômé) en ETP.
• Population définie en terme de pathologie (Attention pour AVK) d’ALD et d’efficacité de l’ETP.
• Programme clair identifié.
• Outils
• Evaluation
• Financement (pas absent mais pas industrie…)
Un seul élément indispensable…
• La collaboration ville hôpital patients soignants et médecins….
Conclusion• Créer une unité de prise en charge ambulatoire
de l’IC éventuellement en y mutualisant les consultations voire les explorations fonctionnelles est utile pour les patients et efficient pour le centre hospitalier.
• Il nécessite une priorisation et un soutien de la part du service surtout en terme de recrutement et un suivi managérial.

Top Related