







Languages
Pages
Legal


Hemolytic Anemia: Membrane Defects
S i Al iSamin Alavi,Pediatric Hematologist/oncologistMofid Children’s Hospital

HEMOLYTIC ANEMIASHEMOLYTIC ANEMIAS
RBC Membrane DisordersRed Cell Enzyme disordersHemoglobinopaties & Oxidant HemolysisHemolysisAutoimmune Hemolysis

MEMBRANE HEMOLYTIC DISORDERS
Defects due to abnormalities in membrane Defects due to abnormalities in membrane proteins or lipids
Defects alter membrane’s stability, shape, d f bili d bilideformability and permeability
Hemolysis occurs extravascularly



f fPhospholipid bilayer is the major structural feature (forms the matrix of the membrane); asymmetric distribution of lipids in the bilayer.
“FLUID”-- Lipids and proteins diffuse freely in plane of membrane; Proteins “float” in a “sea” of lipid (no constraints indicated). Allowed because protein lipid and lipid lipid interactions weak Allowed because protein-lipid and lipid-lipid interactions weak, compared to covalent bonds.
“MOSAIC” b d f h i f “MOSAIC”-- membrane composed of heterogeneous mixture of lipids and proteins, organized in dynamically changing patterns. Proteins also asymmetrically distributed.
P t i di t ib t d t i ll tt h d t ith id f Proteins distributed asymmetrically: attached to either side of bilayer, or partially or fully embedded in the bilayer, even traversing (penetrating) bilayer- NOT just coating the bilayer.
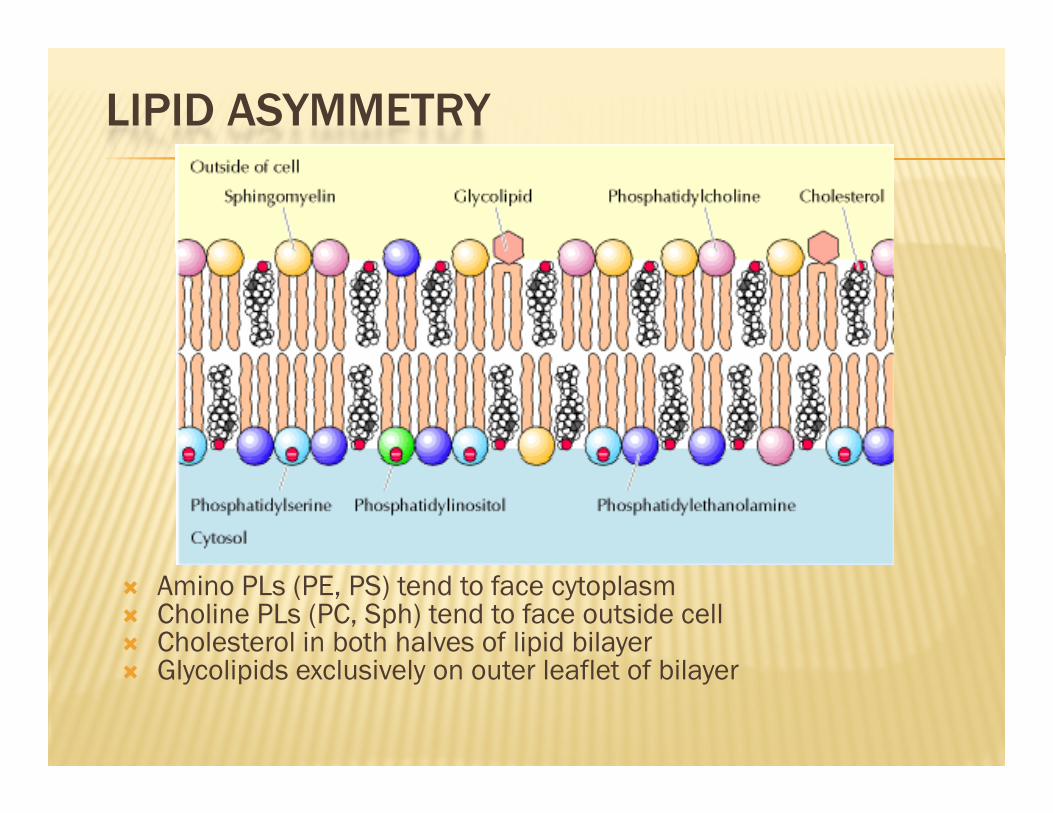
LIPID ASYMMETRY
Amino PLs (PE, PS) tend to face cytoplasmCholine PLs (PC, Sph) tend to face outside cellCholesterol in both halves of lipid bilayerGl li id l i l t l fl t f bilGlycolipids exclusively on outer leaflet of bilayer

MEMBRANES ARE ASYMMETRIC - THEY HAVE DISTINCTIVE INSIDE AND OUTSIDE FACESDISTINCTIVE INSIDE AND OUTSIDE FACES

Two Types of Membrane Proteins
Peripheral (“extrinsic”) membrane proteinsp ( ) p- loosely associated with bilayerspectrin; ankyrin; actin,pro 4.1,pro 4.2,tropomyosin, dematin
Integral (“intrinsic”) membrane proteinsIntegral ( intrinsic ) membrane proteins- strongly associated with bilayerglycophorin; Band 3, rhodopsin; β-adrenergic receptor

SINGER-NICOLSON“FLUID MOSAIC” MODEL
PROTEINS FLOATING IN A “SEA” OF LIPIDSPROTEINS FLOATING IN A SEA OF LIPIDS
The proteins interact with the lipid bilayer by electrostatic interactions (extrinsic proteins) or penetrate partially or completely span the hydrophobic domain of th li id bil (i t i i t i ) the lipid bilayer (intrinsic proteins). The lipids of the bilayer matrix are in a liquid-crystal (fluid) state and candiffuse laterally in the plane of the membrane. The matrix of the membrane consists of a lipid bilayer The matrix of the membrane consists of a lipid bilayer. Proteins are able to freely diffuse within the bilayer plane and about their axes perpendicular to the plane of the membrane. There is no long-range order in the arrangement of components other than that which results from summation of short-range intermolecular interactions.
S.J. Singer & G. Nicolson (1972) Science 175: 720-731.
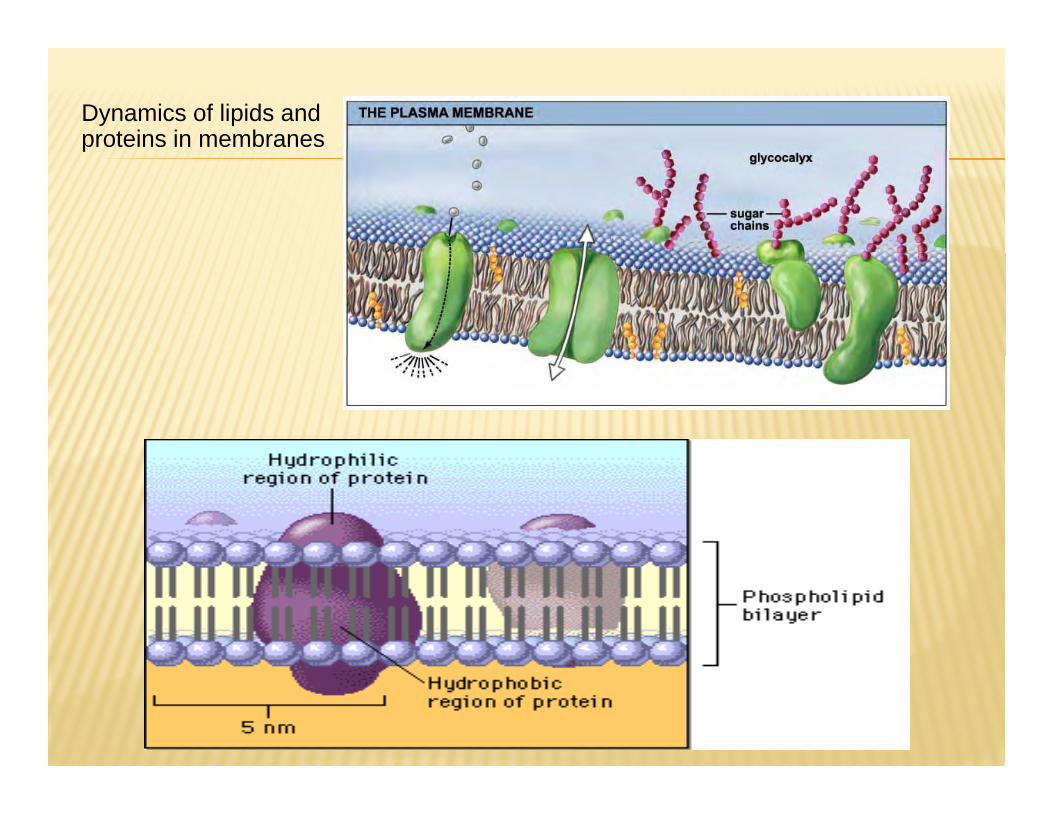
Dynamics of lipids and proteins in membranesp
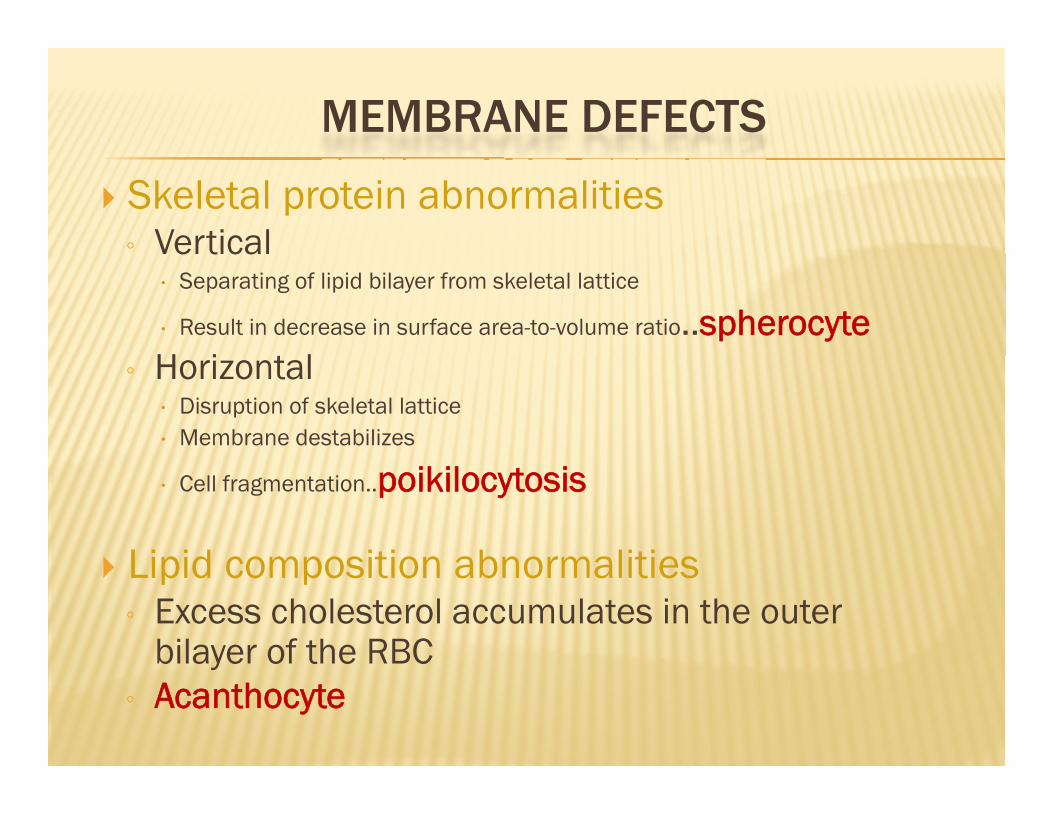
MEMBRANE DEFECTS
Skeletal protein abnormalities◦ VerticalVertical
Separating of lipid bilayer from skeletal lattice
Result in decrease in surface area-to-volume ratio..spherocyteH i l◦ Horizontal
Disruption of skeletal latticeMembrane destabilizes
Cell fragmentation..poikilocytosis
Lipid composition abnormalitiesLipid composition abnormalities◦ Excess cholesterol accumulates in the outer
bilayer of the RBCbilayer of the RBC◦ Acanthocyte

CONDITIONS ASSOCIATED WITH MEMBRANE DEFECTS DEFECTS
◦ Hereditary spherocytosis◦ Hereditary elliptocytocytosis◦ Hereditary pyropoikilocytosis◦ Hereditary stomatocytosis◦ Membrane lipid disorders◦ Paroxysymal noctural hemoglobinuria

Hereditary spherocytosisDefect in ankyrin & spectrin
R lt i th f ti f f il h ti d llResults in the formation of fragile spherocytic red cells.Spherocyte becomes less flexible and more permeable to Na+

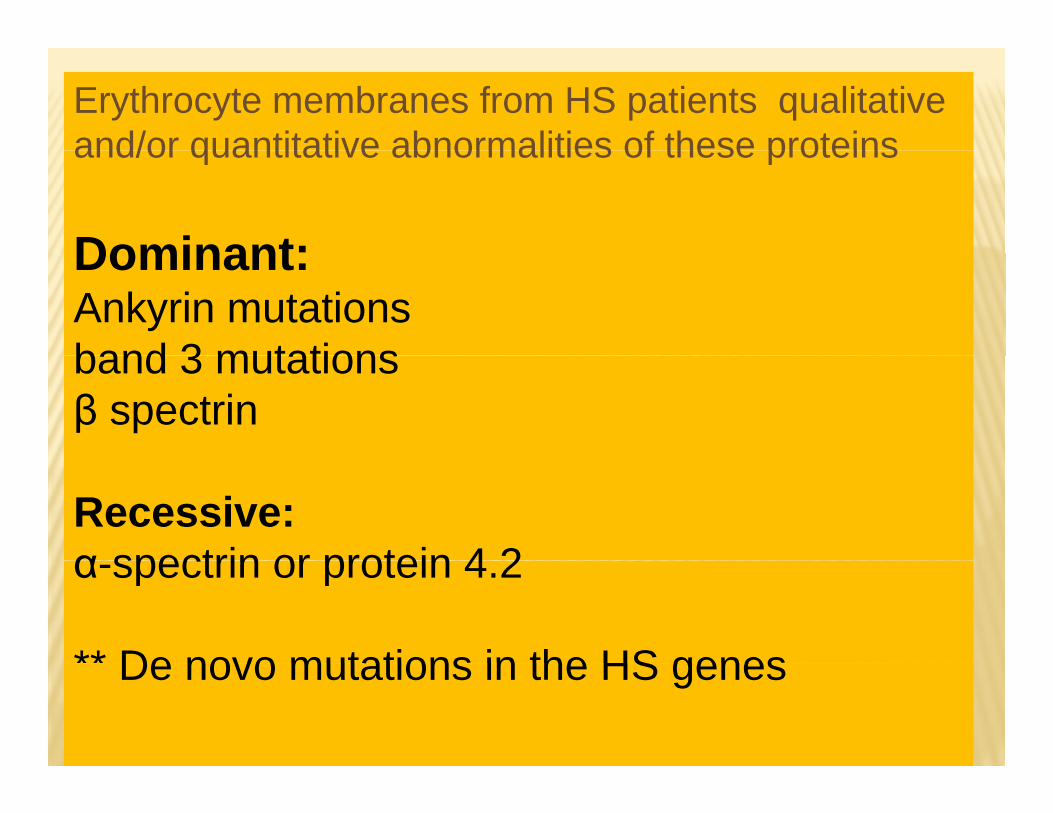
Erythrocyte membranes from HS patients qualitative and/or quantitative abnormalities of these proteinsand/or quantitative abnormalities of these proteins
Dominant:Dominant:Ankyrin mutationsband 3 mutationsband 3 mutations β spectrin
Recessive:α spectrin or protein 4 2α-spectrin or protein 4.2
** De novo mutations in the HS genes De novo mutations in the HS genes
HEREDITARY SPHEROCYTOSISHEREDITARY SPHEROCYTOSIS
• Molecular pathologyp gy• Partial deficiency of spectrin• Combined deficiency of spectrin and ankyrin• Molecular Defects:
• mutations of ankyrinmutations of band 3 protein• mutations of band 3 protein
• mutations of protein 4.2 (common in Japanese)• Others: β & α spectrin, protein 4.9 are rare

1) Defects of spectrin,ankyrin, or protein 4.2 lead to reduced density of the membrane skeleton destabilizing the overlying density of the membrane skeleton, destabilizing the overlying lipid bilayer and releasing band 3-containing microvesicles. ]
2) Defects of band 3 lead to band 3 deficiency and loss of its lipid-stabilizing effect. This results in the loss of band 3-free microvesicles microvesicles.
Both pathways result in membrane loss, decreased surface Both pathways result in membrane loss, decreased surface area, and formation of spherocytes with decreased deformability.
These deformed erythrocytes become trapped in the spleen where splenic conditioning causes further membrane damage where splenic conditioning causes further membrane damage, amplifying the cycle of membrane injury.



CLINICAL FINDINGSCLINICAL FINDINGS
Varies in severityVaries in severityCompensated hemolytic diseaseN i t i TNo anemia to severe anemia……TxIntermittent jaundiceSplenomegalyCholelithiasis: pigment bile stones from Cholelithiasis: pigment bile stones from increased bilirubin breakdown

LABORATORY FINDINGSLABORATORY FINDINGS
Typical HS patients have obvious spherocytes lacking central pallor,Less commonly, only a few spherocytes are present ,polychromatophilia is also present in most.
in severe cases, there are numerous small, densein severe cases, there are numerous small, dense spherocytes and bizarre erythrocyte morphology with anisocytosis and poikilocytosis.
Molecular studies have shown that specific morphologic findings are associated with certain membrane
protein defects such as pincered erythrocytes (band 3),spherocytic acanthocytes (β spectrin)sp e ocyt c aca t ocytes (β spect )Spherostomatocytes (protein 4.2).

HEREDITARY SPHEROCYTOSIS
• Differential diagnosisg
• Morphology is first screening test• Other causes of spherocytes:Other causes of spherocytes:
• Autoimmune hemolysis (IgG)• Autoimmune hemolysis (IgG)• Paroxysmal cold hemoglobinuria• Thermal injuryThermal injury• Clostridium sepsis • Hemolytic transfusion reactions.y• Neonatal hypophosphatemia

Laboratory Evaluation of HemolysisExtravascular Intravascular
HEMATOLOGIC
Routine blood filmReticulocyte count
Polychromatophilia PolychromatophiliaReticulocyte countBone marrow examination
Erythroidhyperplasia
Erythroid hyperplasia
PLASMA OR SERUM
Bilirubin Unconjugated UnconjugatedBilirubinHaptoglobinPlasma hemoglobinL t t d h d
Unconjugated, Absent
N/(V i bl )
UnconjugatedAbsent
(V i bl )Lactate dehydrogenase (Variable) (Variable)
URINEBilirubinHemosiderinHemoglobin
000
0++ severe cases

Signs of Intravascular Signs of Intra ORSigns of Intravascular Hemolysis
Signs of Intra OR Extravascular Hemolysis
Hemoglobinemia Increased indirect hyperbilirubin
Hemoglobinuria Hemoglobinuria
Hemosiderinuria Increased urinary and fecal urobilinogen
Decreased hemopexin Decreased haptoglobin

LAB FEATURES
CBCMild to moderate anemiaMCV is usually normal (77-87fL)(In severe HS it might be low)low)MCH normalMCHC is >36% (This is the only condition in which an MCHC b t l i d )MCHC can be truly increased.)MCHC + RDW : specificity 100%
RBC morphologySpherocyteVarying degrees of polychromasia, anisocytosis and poikilocytosis

Truncated Band 3 Is Associated with“Pincered” HS.

DIAGNOSTIC TESTS FOR HS
↑ Osmotic fragility - (s/v ) Cells are incubated in decreasing concentrations of gNaCl. Spherocytes lyse sooner than normal red cells.
Autohemolysis test̊Red cells are incubated at 37̊ C for 48 hours. Degree of
hemolysis is increased when spherocytes are present. Red cell membrane studiesRed cell membrane studiesMembrane proteins are analyzed using gel (SDS-PAGE)electrophoresis. Specialized testing, such as membrane protein quantitation, ektacytometry,
Genetic analysesy

Osmotic fragility after Osmotic fragility after Incubation is the most Incubation is the most sensitive test routinely se s t e test out e yavailable for diagnosis

DIAGNOSTIC TESTS FOR HS
lack of specificity and are not usedlack of specificity and are not used
Autohemolysis test : 15-45% lysewhich is mostly reduced with Glucose
Hypertonic cryohemolysis test
Acidified glycerol lysis test Acidified glycerol lysis test (AGLT):<5 min in HS )

Indication Autohemolysis test
PhysiologyThis test measures the degree to which patients red cells lyse without
dditi ith l d ith ATP (Ad i T i h h t ) Physiology
additives, with glucose and with ATP (Adenosine Tri-phosphate).
Glucose-6-Phosphate dehydrogenase deficient RBC’s have increased auto hemolysis, which corrects significantly with glucose or ATP.
Interpretationhemolysis, which corrects significantly with glucose or ATP.
Pyruvate kinase deficiency has increased auto-hemolysis, which does not correct or get aggravated with glucose but does correct toward normal with ATP ATP.
IndicationThis test is used to diagnose hereditary spherocytosis, spontaneous hemolysis, RBC enzyme deficiency and hemolytic anemia.

ReferenceIncubation at 37 for with glucose with ATP
48hrs
Normal 0.2%- 2% 0%-0.9% 0.5%-2.5%
G6PD def 3%-5% Normal NormalG6PD def 3%-5% Normal Normal
PK deficiency 12%-16% 12%-16% Normal
H.Spherocytosis 12%-15% 3%-5% 3%-5%

OSMOTIC FRAGILITY (OF)
Incubated osmotic fragility (OF) testing is considered the gold standard in diagnosing HS standard in diagnosing HS
After incubation at 37 for 24 hours, HS red cells lose membrane After incubation at 37 for 24 hours, HS red cells lose membrane surface area more readily than normal cells because their membranes are leaky and unstable.
When the spleen is present, a subpopulation of fragile erythrocytes that have been conditioned by the spleen form the erythrocytes that have been conditioned by the spleen form the “tail” of the OF curve that disappears after splenectomy.
OF testing suffers from poor sensitivity as ~20% of mild cases of HS are missed after incubation.

A FLOW CYTOMETRIC-BASED ANALYSIS
A flow cytometric-based analysis by measuring fluorescence intensity of red cells labeled with eosin-5-maleimide (EMA) dye,reacts covalently with lysine-430 on band 3 protein
band 3 interacts ith ank rin and protein 4 2 hich interact ith band 3 interacts with ankyrin and protein 4.2, which interact with the spectrin-based cytoskeleton, and stabilizes the membrane lipid bilayer
Absent or decreased expression of red blood cell membrane t i f d i HS d l i f b d 3 t i proteins found in HS reduces normal expression of band 3 protein
at the erythrocyte membrane
This results in a reduced binding of EMA to band 3 protein and its fluorescence emission

EMA FLUORESCENCE DYE-BASED METHODEMA FLUORESCENCE DYE BASED METHOD
EMA fluorescence dye-based method is a EMA fluorescence dye based method is a sensitive, reliable and speedy diagnostic test that can be performed in less than 2 hours.that can be performed in less than 2 hours.
ifi f d bl d ll b t i specific for red blood cell membrane proteins found in HS and SAO and helped to distinguishthese two conditions from other hemolytic diseases which also might have micro spherocytes or ovalocytes

By using flow cytometric method at a
cutoff of 91.5 MCF units, we couldcutoff of 91.5 MCF units, we could
differentiate HS and SAO patients fromdifferentiate HS and SAO patients from
l d th h l ti dinormal and other hemolytic diseases
such as HE, AIHA, β-thalassemia/HbE,
α-thalassemia and PK deficiency

HEREDITARY ELLIPTOCYTOSISHEREDITARY ELLIPTOCYTOSIS
Presence of elliptical, cigar-shaped erythrocytes on Presence of elliptical, cigar shaped erythrocytes on peripheral blood smear
It is common in individuals of African and Mediterranean It is common in individuals of African and Mediterranean descent, presumably because elliptocytes confer some resistance to malaria.
Worldwide, the incidence of HE is estimated at 1:2000-4000
The actual incidence is unknown, as most patients are asymptomatic


Ankyrin HS Most common cause of typical dominant HS
Band 3 HS, SAO, “Pincered” spherocytes seen on smear
α Spectrin HS, HE, HPP, Location of mutation in spectrin determinesli i l h tclinical phenotype.
β Spectrin HS, HE, HPP “Acanthocytic” spherocytes seen on smear
Protein 4.2 HS Common in recessively inherited
Protein 4.1 HE An uncommon cause of HE.
Glycophorin C HE Concomitant protein 4.1 deficiency is basis ofHE in glycophorin C defects

RBC Membrane Disorders: RBC Membrane Disorders: ElliptocytosisElliptocytosis
HEREDITARY ELLIPTOCYTOSISHE is inherited in an autosomal dominant pattern with rare cases of de novo mutationsof de novo mutations.
PathobiologyThe principal defect in HE/HPP erythrocytes is mechanical The principal defect in HE/HPP erythrocytes is mechanical weakness or fragility of the erythrocyte membrane skeleton.
Similar to HS, study of erythrocyte membrane proteins in these disorders has identified qualitative and/or quantitative abnormalities of various erythrocyte membrane proteinsabnormalities of various erythrocyte membrane proteins
Abnormalities of either α or β spectrin associated with the majority of cases of HE/HPP are due to mutations in the spectrinheterodimer self association site

CLINICAL MANIFESTATIONS OF HE
Clinical presentation of HE is heterogeneous, from asymptomatic carriers to patients with severe anemia carriers to patients with severe anemia.
Most patients with “typical” HE are asymptomatic and are Most patients with typical HE are asymptomatic and are diagnosed incidentally
Erythrocyte life span is normal in most patients, decreased in only ~ 10% of patients
Interestingly, symptomatology may vary between members of the same family,it may vary in the same individual at different times

LABORATORY FINDINGS OF HE
Normochromic, normocytic elliptocytes may number from few to 100%;
The degree of hemolysis does not correlate with the number of elliptocytes present.
Spherocytes, stomatocytes and fragmented cells may also be seen.
The osmotic fragility is abnormal in severe HE and HPP. g y
Other laboratory findings in HE are similar to those found in other hemolytic anemias
In difficult cases or cases desiring a molecular diagnosis, specialized testing such as erythrocyte membrane protein quantitation and genetic t ti il bltesting are available.

LABORATORY FEATURES:
:
Smear : diagnosis on % of elliptocytesSmear : diagnosis on % of elliptocytes(N < 5%) , HE 25 – 90 % in +ve family history.Elliptocytes: oval cells with long diameter > 2 Elliptocytes: oval cells with long diameter 2 times the short diameter.Retics, LDH, bil., -ve DAT (Direct Antiglobulin( g
Test)Osmotic frafility : Mild HE : normal
Severe HE :IncreasedAutohaemolysis : NL or (corrected by gl.).

ELLIPTOCYTES MAY BE SEEN IN ASSOCIATION WITH SEVERAL DISORDERS
Megaloblastic anemias, Hypochromic microcytic anemias, Myleodysplastic syndromes M elofibrosisMyelofibrosis.

HEREDITARY PYROPOIKILOCYTOSIS (HPP)( )
Hereditary pyropoikilocytosis (HPP)Severe subtype of HESevere subtype of HEDeficiency of α-spectrin and a mutant spectrin leads to disruption of skeletal lattice and cell destabilizationCells fragment when heatedTends to affect blacksP i i f l hildh d IPresents in infancy or early childhood,Icterus
CBCMCV d d (25 55 fL)MCV decreased (25-55 fL)
RBC morphologyExtreme erythrocyte morphologiesExtreme erythrocyte morphologies
Fragments, elliptocytes, triangulocytes etc

RBC Membrane Disorders:RBC Membrane Disorders:HereditaryHereditary PyropoikilocytosisPyropoikilocytosisHereditary Hereditary PyropoikilocytosisPyropoikilocytosis

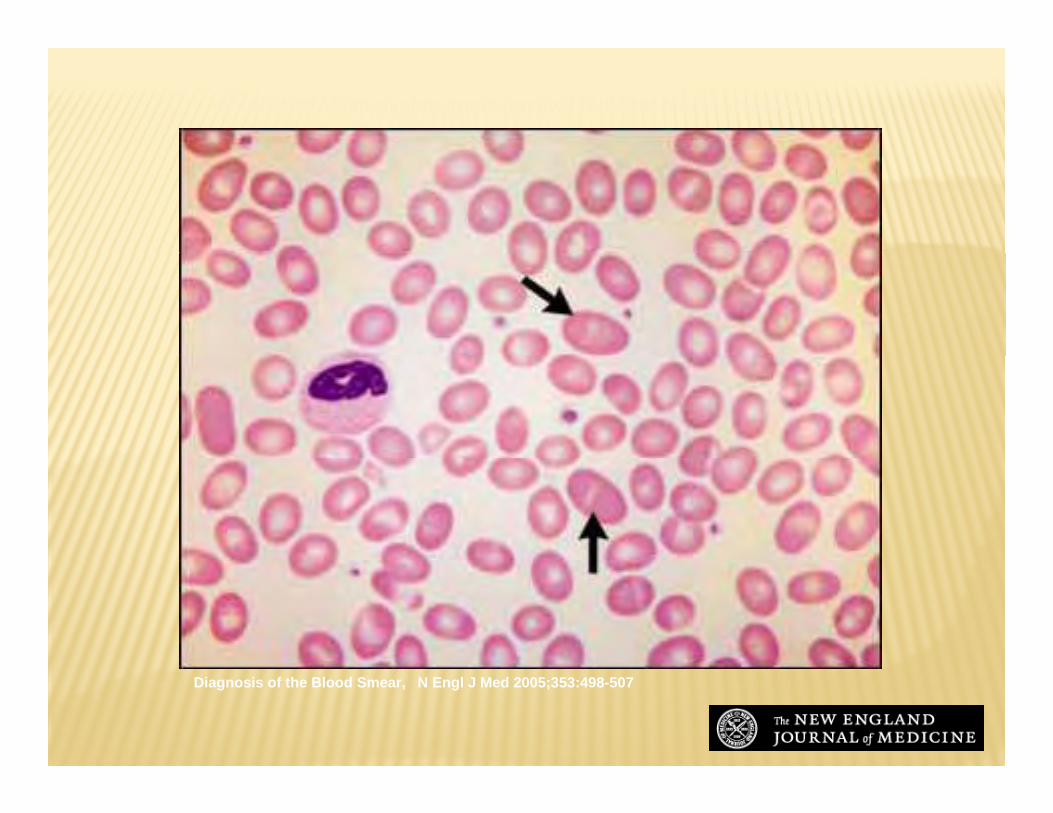
Hereditary pyropoikilocytosis
Diagnosis of the Blood Smear, N Engl J Med 2005;353:498-507

SOUTHEAST ASIAN OVALOCYTOSIS (SAO)An unusual, dominantly inherited HE variant found in Malaysiaand other parts of Southeast Asia.
o Rounded elliptocytes, or ovalocytes, and characteristic stomatoc tes ith longit dinal slits are fo nd stomatocytes with longitudinal slits are found
Most SAO patients are asymptomatic a few experience mild Most SAO patients are asymptomatic, a few experience mild hemolysis.
The cause of SAO is a 27 bp genomic deletion leading to deletion of 9 amino acids in band 3 deletion of 9 amino acids in band 3.
Southeast Asian ovalocytosis (arrows indicate macro-ovalocytes)
Diagnosis of the Blood Smear, N Engl J Med 2005;353:498-507

Mohammed laqqan

HEREDITARY STOMATOCYTOSIS SYNDROMES
A group of inherited disorders characterized by h i h h h d ( ) f erythrocytes with a mouth-shaped (stoma) area of
central pallor on peripheral smear
Stomatocytosis : abnormalities in red cell cationpermeability that lead to changes in red cell volume, which may be either increased (hydrocytosis) or which may be either increased (hydrocytosis) or decreased (xerocytosis), or, in some cases, near normal.
Stomatin, an integral membrane protein, is decreasedor absent from the erythrocyte membranes of affectedpatientspatients

Laboratory features:yAnaemia.
ReticsRetics.Smear: 10 – 25% stomatocytes.
OF & autohaemolysis.Thermal stability.Expression of certain red cell antigens.
Resistance to in vitro invasion by malaria Resistance to in vitro invasion by malaria



HYDROCYTOSIS SYNDROMESHYDROCYTOSIS SYNDROMES
known as overhydrated hereditary stomatocytosis, are characterized by significant stomatocytosissevere hemolysis,macrocytosis (110-150),
The excess cations elevate cell water, producing large, osmotically fragile cells with a low MCHC g , y g(24%-30%).
The clinical severity of overhydrated HSt (OHSt) is variable; some patients experience hemolysis and anemia while others are asymptomatic.anemia while others are asymptomatic.

DEHYDRATED STOMATOCYTOSIS SYNDROMES
known as xerocytosis, characterized by contracted and spiculated red cells, variable numbers of stomatocytes, and target cells on peripheral blood smear
Most patients have nearly normal erythrocyte morphology
The MCHC and MCV (95-115 fL) are increased
osmotic fragility is decreased.os ot c ag ty s dec eased

An unusual and important An unusual and important characteristic of the stomatocytosis syndromes is a marked predisposition to marked predisposition to thrombosis after splenectomyp y

HEMOLYTIC ANEMIASLABORATORY DIAGNOSTIC TESTS LABORATORY DIAGNOSTIC TESTS LABORATORY DIAGNOSTIC TESTS LABORATORY DIAGNOSTIC TESTS
Intravascular & Extravascular hemolysisIntravascular & Extravascular hemolysissome times components of bothDiff ti l l fDifferential values of:
Reticulocyte countbilirubinbilirubinLDH serum haptoglobinserum haptoglobinurinary hemosiderin urinary hemoglobiny g

HEMOLYTIC ANEMIAS: PNH• Clinical Presentation
Intravascular hemolysisIntravascular hemolysisThrombosisPancytopeniaHypocellular marrow & AplasiaHypocellular marrow & Aplasia
Deficiency of PI anchored membrane proteinsLaboratory diagnosisLaboratory diagnosis
Ham’s test & sugar-water tests crude, nonspecific & low sensitivityCD-59 and other PI protein deficiencies FACS analyses should p ybe used
PIG A mutationsSometimes multiple in a single patientSometimes multiple in a single patientCan be found in normal people
PNH PNH ––laboratory featureslaboratory features::
PANCYTOPENIAPANCYTOPENIA-- CHRONIC URINARY IRON LOSS CHRONIC URINARY IRON LOSS -- SERUM IRON CONCENTRATION DECREASED SERUM IRON CONCENTRATION DECREASED -- HEMOGLOBINURIAHEMOGLOBINURIA-- HEMOSIDERINURIAHEMOSIDERINURIAPOSITIVE HAM’S TEST (ACID HEMOLYSIS TEST)POSITIVE HAM’S TEST (ACID HEMOLYSIS TEST)-- POSITIVE HAM S TEST (ACID HEMOLYSIS TEST)POSITIVE HAM S TEST (ACID HEMOLYSIS TEST)
-- POSITIVE SUGARPOSITIVE SUGAR--WATER TEST WATER TEST -- SPECIFIC IMMUNOPHENOTYPE OF ERYTROCYTES SPECIFIC IMMUNOPHENOTYPE OF ERYTROCYTES SPECIFIC IMMUNOPHENOTYPE OF ERYTROCYTES SPECIFIC IMMUNOPHENOTYPE OF ERYTROCYTES
(CD(CD5959, CD, CD5555))

PERIPHERAL SMEAR
SpherocytesFragmented RBCs
Schistocytes helmet cellsSchistocytes, helmet cellsMicroangiopathic hemolytic anemia
A th t ( ll )Acanthocytes (spur cells)Liver disease
Blister or “bite” cellsG6PDG6PD
WARM AIHA - LABS
Elevated MCV (reflecting reticulocytosis)Elevated MCV (reflecting reticulocytosis)Mild leukocytosis with neutrophiliaBlood smear: Blood smear:
Polychromasia, macrocytosis, spherocytes, nucleated RBCs
Elevated LDH and indirect bilirubinHaptoglobin typically lowp g yp y
Because it is an acute phase reactant, it can also be normal or elevated in mild disease

WARM AIHA – DAT (DIRECT COOMBS)
Detects Ab on the RBC surfacePt’s RBCs are washed then reacted with monoclonal Ab against various Ig (IgG) and C3Warm autoantibodies react at warmer temperatures (~37° C)95% of Warm AIHA will have a positive DAT95% of Warm AIHA will have a positive DATNegative tests due to:
IgG quantity too low for detectable thresholdgG qua t ty too o o detectab e t es o dIgA autoantibodiesIgM autoantibodies

MICROANGIOPATHIC SYNDROMES MICROANGIOPATHIC SYNDROMES
THROMBOCYTOPENIC PURPURA THROMBOCYTOPENIC PURPURA
HEMOLYTIC UREMIC SYNDROME

MICROANGIOPATHIC HEMOLYTIC ANEMIA –HUS DIAGNOSIS
The diagnosis can be made on the basis ofThe diagnosis can be made on the basis of thrombocytopenia and microangiopathic hemolytic anemia –without another clinically apparent cause.
It’s microangiopathic hemolytic anemia again! This form of anemia can cause fragments gwhich can artificially elevate automated platelet counts…
Elevated LDH is an important marker of MHA, and can be used both for diagnosis and asused both for diagnosis and as a marker for treatment response.
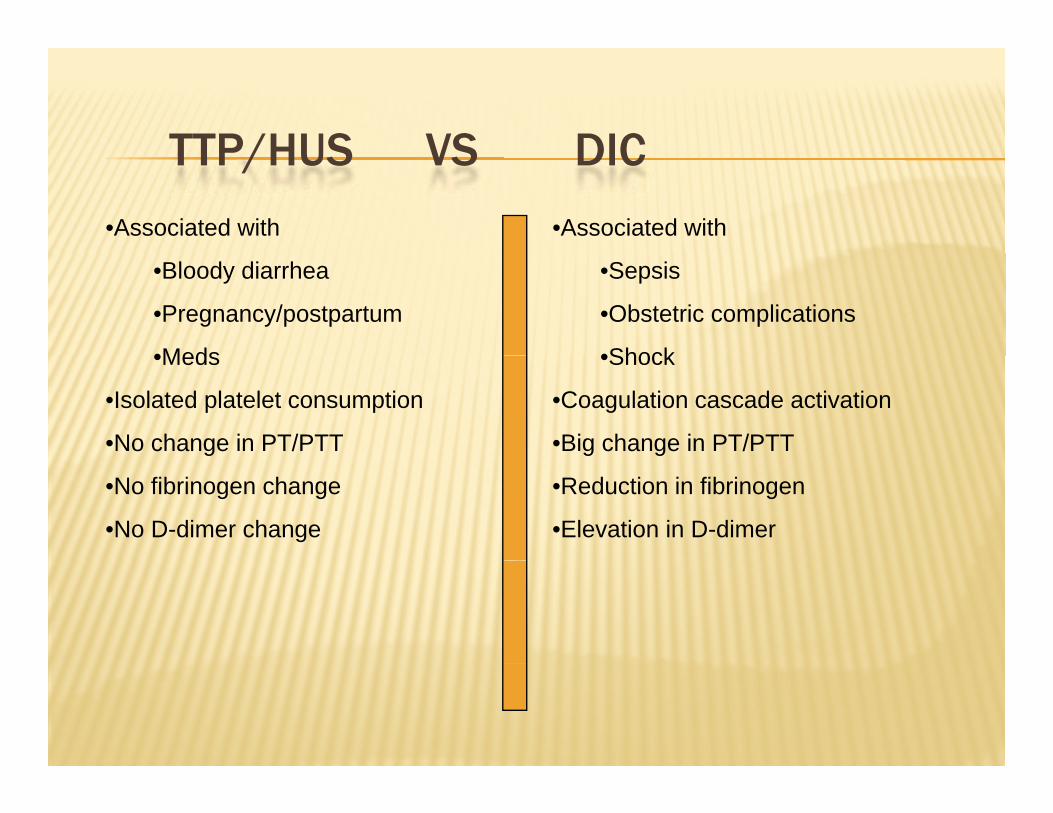
TTP/HUS VS DICTTP/HUS VS DIC
•Associated with •Associated with
•Bloody diarrhea
•Pregnancy/postpartum
•Meds
•Sepsis
•Obstetric complications
•Shock•Meds
•Isolated platelet consumption
•No change in PT/PTT
•Shock
•Coagulation cascade activation
•Big change in PT/PTT
•No fibrinogen change
•No D-dimer change
•Reduction in fibrinogen
•Elevation in D-dimer

SCHISTOCYTES!SCHISTOCYTES!

Microangiopathic hemolytic anemia resulting from cyclosporine therapy
Diagnosis of the Blood Smear, N Engl J Med 2005;353:498-507

Paroxysmal cold hemoglobinuria(arrow indicates a red cell that has been phagocytosed by a neutrophil)
Diagnosis of the Blood Smear, N Engl J Med 2005;353:498-507

Hyposplenism in celiac disease (short arrow indicates a target cell, long arrow an acanthocyte, and arrowhead a Howell-Jolly body)
Diagnosis of the Blood Smear, N Engl J Med 2005;353:498-507
Top Related