







Languages
Pages
Legal

第一屆整合照護師課程會談技巧與實作
授課時間:108年3月16日上午 10:10~12:00地點:台北榮總致德樓第四會議室講師:衛生福利部台中醫院家庭醫學科暨社區健康部主任 許碧珊
醫療風險之基本說明
醫療行為本身極具有一定風險
當事人試圖免除特定風險(原有疾病)進而選擇承擔另一項風險(醫療行為)
當事人對於醫療風險之認知與掌控能力並非對等
風險承擔通常必須建立在『當事人同意』之基礎上

受理委託醫事鑑定案件數統計表

歷年衛生局調處、司法委託醫糾鑑定案件數(民、刑事)、醫改會的醫療爭議諮詢案件數等歷年趨勢---資料來源:除醫改會服務案件數為醫改會統計資料外,其他數字來源為衛福部網站
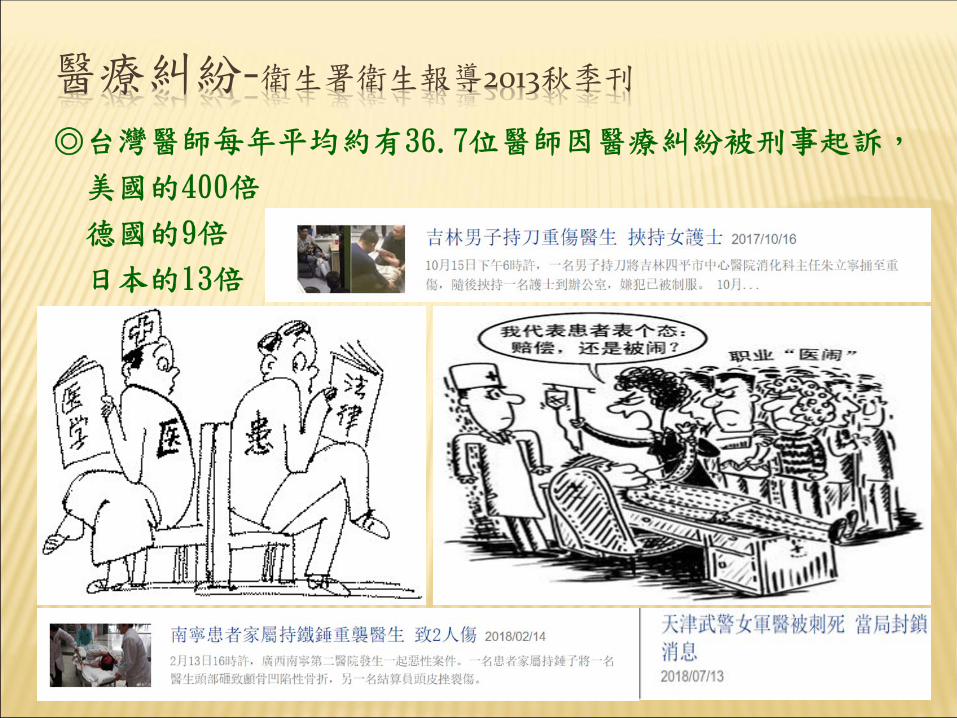
醫療糾紛-衛生署衛生報導2013秋季刊
民眾心目中好醫生的條件
人病
以病人為中心
〝好〞醫師眼中的病人
人為中心
健康導向
系統統合
身心靈合一
全人整合照護To Care Often
To Comfort Always

整合醫學跨專業團隊運作
資源整合 個案管理
全面照護疾病管理 行政護理
醫療
醫院
人疾病管理 社
區
人病
病人
病人
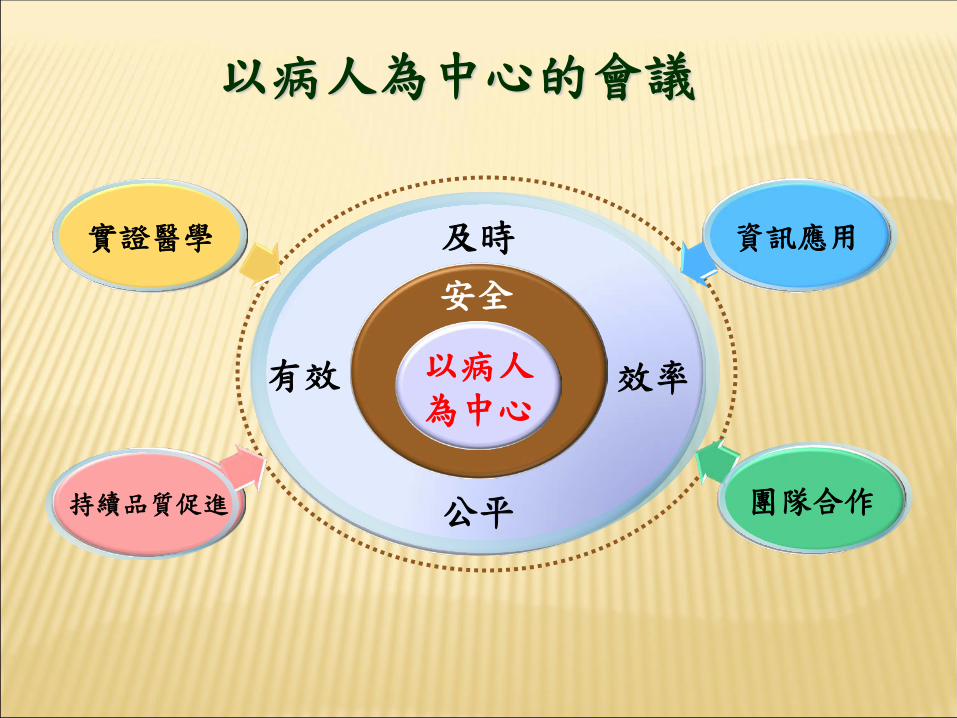
以病人為中心的會議
實證醫學
以病人為中心
安全
有效 效率
及時
公平持續品質促進
資訊應用
團隊合作

基本功
專業、專業、專業!!背景知識-他是誰?他們是誰?
面談目的
面談空間
面談技巧

專業一沒有
一切一場空

跟誰溝通?
自己
團隊
被照顧者
照顧者

團隊
TYPES OF TEAMS
Multidisciplinary Interdisciplinary Transprofessional

TEAM MEMBERS
醫師
護理人員
物理治療師
職能治療師
社工
藥事人員
營養師
個案管理師

分權 (CENTRALIZED)集權 (DECENTRALIZED)
分權:
優點: 當場、及時做決定,提升彈性與應變能力,較能發揮技術性能力與負責
缺點: 規劃與協調較為困難,決策控制力較為低下
集權:
優點:主管能協調各種活動,朝共同目標努力
缺點:主管負擔過重忙著每天做作業性決策,而降低思考長期性規劃的能量

MULTIDISCIPLINARY TEAM
discipline-oriented each team member responsible only for the
activities related to his or her own discipline (Melvin, 1989; Rothberg, 1981).
One team member is affected very little by the efforts of the other team members

INTERDISCIPLINARY TEAM
Interaction among the disciplines. Not only are individuals from several disciplines
working toward a common goal, but the team members have the additional responsibility of the group effort (Rothberg, 1981).
Effective communication is required among those involved (Melvin, 1989).
The team includes the patient/client and his/her family

TRANSPROFESSIONAL TEAM
one person can perform professionals’ roles by providing services to the patient/client under the supervision of the individuals from the other disciplines involved.
Disciplines work together in the initial evaluation and care plan, but only one or two members actually provide the services.
Professionals are still accountable for areas related to their specific discipline and for training the team member delivering the service

CHARACTERISTICS OF EFFECTIVE COLLABORATIVE INTERPROFESSIONAL TEAMS
Belief that the team is important to the outcome
Open communication Equality of resourcesRespect Shared decision makingAll members feel valued

整合內外團隊 建立溝通橋梁
社區活動中心
關懷據點
社區公益團體
老人住宅
居家服務
居家醫療
社會型日照
醫療型日照
護理之家
衛生所
愛鄰守護隊
社區醫療群
醫院
社區發展協會
鄰里長
整合區域照顧服務團隊 共享決策之跨專業團隊
Interdisciplinary team of health professionals跨專業團隊
你與你的家人
家庭醫師/老醫醫師 復健科
與其他專科醫師
個案管理師
照顧服務員
護士營養師
社工
物理/職能/語言治療師
娛樂治療師
藥師
司機
2019/3/14許碧珊醫師
21

溝通工具
面對面
身體語言
談話內容
圖片
影音
社群軟體
Keep open個資

TRANSTHEORETICAL MODEL Prochaska & DiClemente, 1983; Prochaska, DiClemente, & Norcross, 1992 an integrative, biopsychosocial model to conceptualize the process of
intentional behavior change focusing mainly on social or biological influences
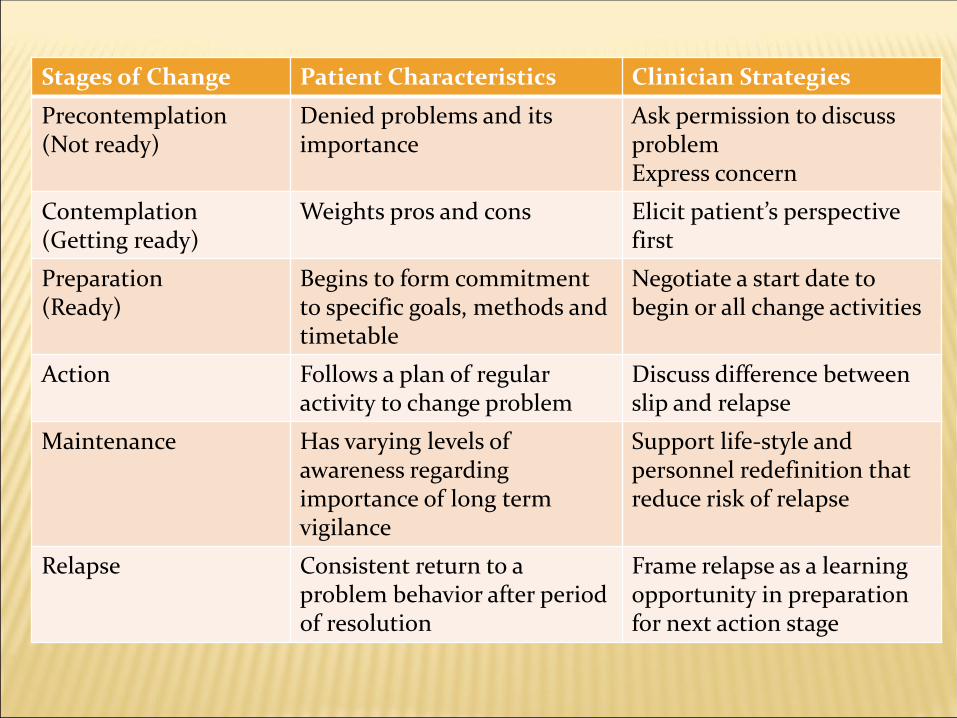
Stages of Change Patient Characteristics Clinician Strategies
Precontemplation(Not ready)
Denied problems and itsimportance
Ask permission to discuss problemExpress concern
Contemplation(Getting ready)
Weights pros and cons Elicit patient’s perspective first
Preparation(Ready)
Begins to form commitment to specific goals, methods and timetable
Negotiate a start date to begin or all change activities
Action Follows a plan of regular activity to change problem
Discuss difference between slip and relapse
Maintenance Has varying levels of awareness regarding importance of long term vigilance
Support life-style and personnel redefinition that reduce risk of relapse
Relapse Consistent return to a problem behavior after period of resolution
Frame relapse as a learning opportunity in preparation for next action stage

行為改變的階段模式-跨越理論
五個階段 五個步驟 (5 A’s) 五個策略 (5 R’s)
懵懂期 評估 (Assess) 關聯 (Relevance)
深思期 忠告 (Advise) 危險 (Risk)
準備期 同意 (Agree) 饋償 (Reward)
行動期 協助 (Assist) 阻礙 (Roadblock)
維持期 安排 (Arrange) 重覆 (Repetition)

需求評估與計畫執行(3C2A)
家庭生理
心理
社會心靈
功能
2017/8/4許碧珊醫師
26

以病人為中心的醫病面談的五步驟-1
Step 1. Step the stage:
準備有助於溝通的場景
歡迎病人:適當的開場白
以名字稱呼病人:或是用病人喜歡的稱呼,切記不要叫全名
自我介紹以及說明自已的專業
確定病人準備好了,也注意到隱私保護
去除溝通時的障礙:例如關掉一旁的音樂或電視
確認病人的舒適,讓他放輕鬆

以病人為中心的醫病面談的五步驟-2
Step 2. Establish chief complaint and agenda:確定要談的問題
讓病人知道有多少時間可以談
說明我們在會談中有些什麼需要
請病人將想要談的盡量提出,列成清單
歸納出主要的議題:如果想談得太多,協商出特定需要先談的部份

以病人為中心的醫病面談的五步驟-3
Step 3. Opening the History of Present ILLness(HPI):開始收集現病史
使用開放式問句:用問題答題,而非選擇或是非題
不聚焦的開放式技巧 (保持靜默、採取中立的語調、以肢體表達鼓勵發言)
從病人語言以外的線索獲得更多的訊息:非語言的訊息、身體的特徴、自主神經系統的變化、衣著外表、以及周遭環境。
以病人為中心的醫病面談的五步驟-4
Step 4. Continuing the HPI:繼續收集現病史的資料 身體症狀的故事
獲得病人對身體症狀的敘述 (運用聚焦的開放式問句的技巧)
個人的故事 讓病人詳細闡述這樣的身體症狀背後,在個人/心理社會層次的脈絡背景 (運用聚焦的開放式問句的技巧)
情緒的故事 讓病人詳細闡述情緒的焦點 (情緒探索技巧)
說出情緒 (情緒處理技巧-NURS) (1)Naming:標記出來 (如:你聽起來很難過)
(2)Understanding:告訴他這樣的情緒表達是可以的 (如:我了解你是因為…而感到…)
(3)Respecting:讚賞他 (你一直都是很樂於幫忙別人)
(4)Supporting:強調夥伴關係 (我過來看看能幫你什麼忙)
擴展故事 擴展病人的故事到新提到的部份 (運用聚焦的開放式問句的技巧、情緒探索技巧以及情緒處理技巧)
以病人為中心的醫病面談的五步驟-5
Step 5. Transition to second (Doctor-centered) phase of the interview:轉換到會談的第二階段-以醫師為中心
簡單的摘要,並且再用一次情緒處理技巧
確認所談內容的正確性
指出接下來要談得內容和詢答方式會與之前不太一樣,主要是要進一步了解身體到底怎麼了;(討論檢查治療等等選項)

STEP6.擬定治療及追蹤計畫
規劃未來(Planning for the future):1、表現出你了解病人的problem list
2、指出你對可以有彈性/會保持彈性
3、定下治療計畫並加以解釋
4、找到病人的自我調適方式並適當地加以肯定
(Identify coping strategies of patient and reinforce them.)
5、幫病人找出其他支持資源
作結語
約定後續動作
醫病關係的原則
打破隔離的原則
-打破「非我族類的原則」的隔離
-打破「不干我事」的隔離
-打破「時空不對」的隔離
-打破「自身難保」的隔離
同理心的原則
-設身處地對對方想
-考慮對方的立場

醫病關係的原則
盡力救助的原則
自知的原則
-醫師知道自己的極限
-尋找第二意見
設定界線的原則
需要雙方用心呵護

NONE OF US IS AS GOOD AS ALL OF US!
Top Related