






Languages
Pages
Legal


Esophageal and Small Bowel
Karthik Ravi
November 14, 2013 Curso Internacional de Actualizacion del
Board de Medicina Interna
No financial disclosures
©2010 MFMER | slide-2

Outline • Esophageal
• GERD • Diagnosis • Management
• Dysphagia • Eosinophilic Esophagitis • Achalasia
• Small Bowel • Normal function • Steatorrhea
• Celiac Disease • Secretory and Osmotic diarrhea
©2010 MFMER | slide-3

Esophagus
©2010 MFMER | slide-4

Case
©2010 MFMER | slide-5
A 42 year-old female presents with several month history of heartburn and acid regurgitation. The heartburn is described as substernal burning, occurring 3 to 4 times a week typically after meals and when supine. In addition, she complains of nocturnal acid regurgitation occurring twice weekly. She denies any dysphagia or weight loss. She has been treated with twice daily PPI therapy without improvement.
What is the most appropriate next step?
A. Refer for fundoplication
B. Esophageal manometry study
C. Increase PPI to three times daily
D. Ambulatory pH monitoring

Case
©2010 MFMER | slide-6
A 42 year-old female presents with several month history of heartburn and acid regurgitation. The heartburn is described as substernal burning, occurring 3 to 4 times a week typically after meals and when supine. In addition, she complains of nocturnal acid regurgitation occurring twice weekly. She denies any dysphagia or weight loss. She has been treated with twice daily PPI therapy without improvement.
What is the most appropriate next step?
A. Refer for fundoplication
B. Esophageal manometry study
C. Increase PPI to three times daily
D. Ambulatory pH monitoring

GERD is common in the community • Up to 20% of the Western population have at least weekly
heartburn and/or acid regurgitation
• Clinically troublesome heartburn is seen in 6% of the population
• Patients with GERD have lower quality of life, reflected by decreased work production and lower scores on sleep scales
• GERD carries a significant health related economic burden: • Responsible for nearly 9 million outpatient visits a year • $5438 cost per patient for evaluation of suspected extra-
esophageal manifestations of GERD
©2010 MFMER | slide-7
Dent J. Gut 2005; 54: 710-717 Camilleri M. Clin Gastroenterol Hepatol 2005; 3: 543-552
Becher A. Aliment Pharmacol Ther 2011; 34: 618-627
Peery AF. Gastroenterology 2012; 143: 1179-1187
Francis DO. Am J Gastroenterol 2013; 108: 905-911

Symptoms have limited reliability in diagnosing GERD
©2010 MFMER | slide-8 Moayyedi P. JAMA 2006; 295: 1566-1576
• Heartburn and Regurgitation most predictive: • Sensitivity of only 30 -76% for erosive
esophagitis • Specificity of only 62 to 90% for erosive
esophagitis
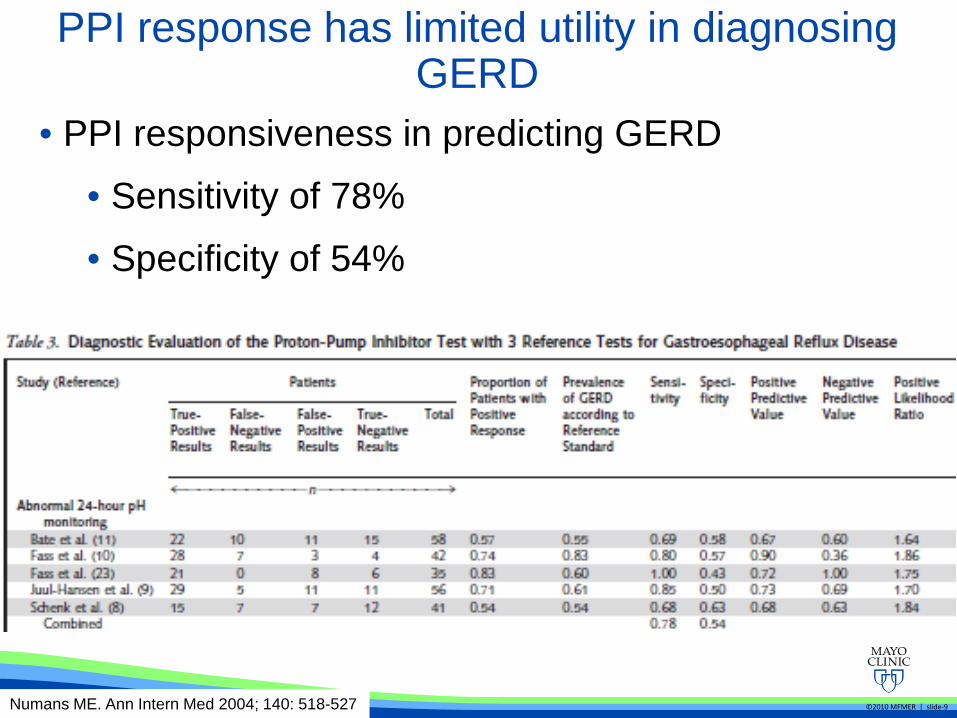
PPI response has limited utility in diagnosing GERD
©2010 MFMER | slide-9 Numans ME. Ann Intern Med 2004; 140: 518-527
• PPI responsiveness in predicting GERD
• Sensitivity of 78%
• Specificity of 54%
©2010 MFMER | slide-10
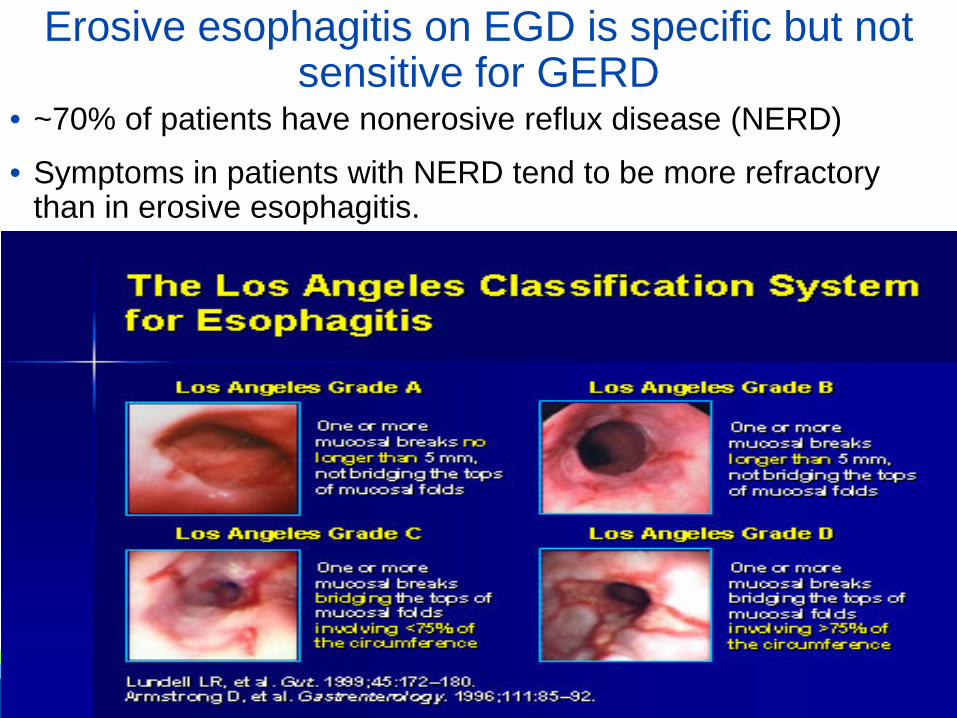
Erosive esophagitis on EGD is specific but not sensitive for GERD
• ~70% of patients have nonerosive reflux disease (NERD)
• Symptoms in patients with NERD tend to be more refractory than in erosive esophagitis.
©2010 MFMER | slide-11
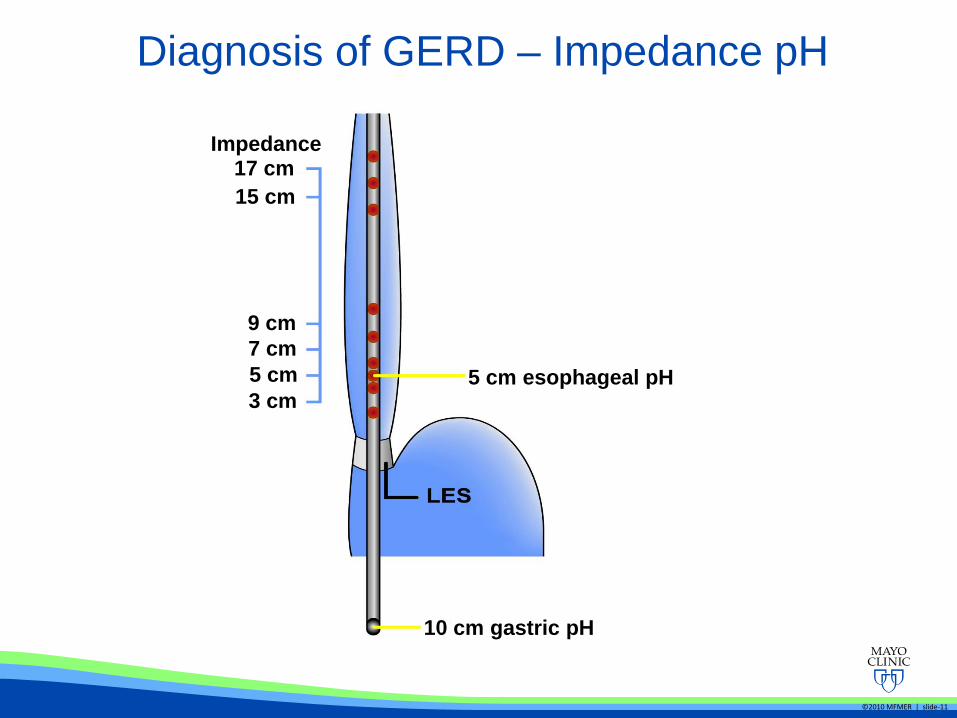
Diagnosis of GERD – Impedance pH
17 cm 15 cm
9 cm 7 cm 5 cm 3 cm
5 cm esophageal pH
10 cm gastric pH
Impedance
©2010 MFMER | slide-12
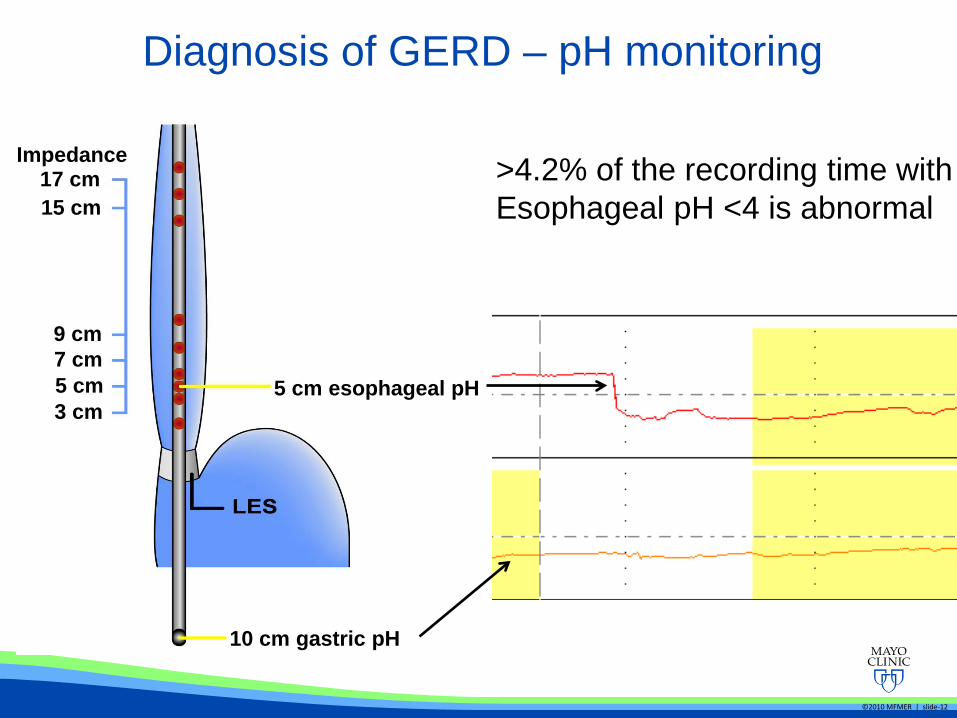
Diagnosis of GERD – pH monitoring
17 cm 15 cm
9 cm 7 cm 5 cm 3 cm
5 cm esophageal pH
10 cm gastric pH
Impedance >4.2% of the recording time with Esophageal pH <4 is abnormal
©2010 MFMER | slide-13
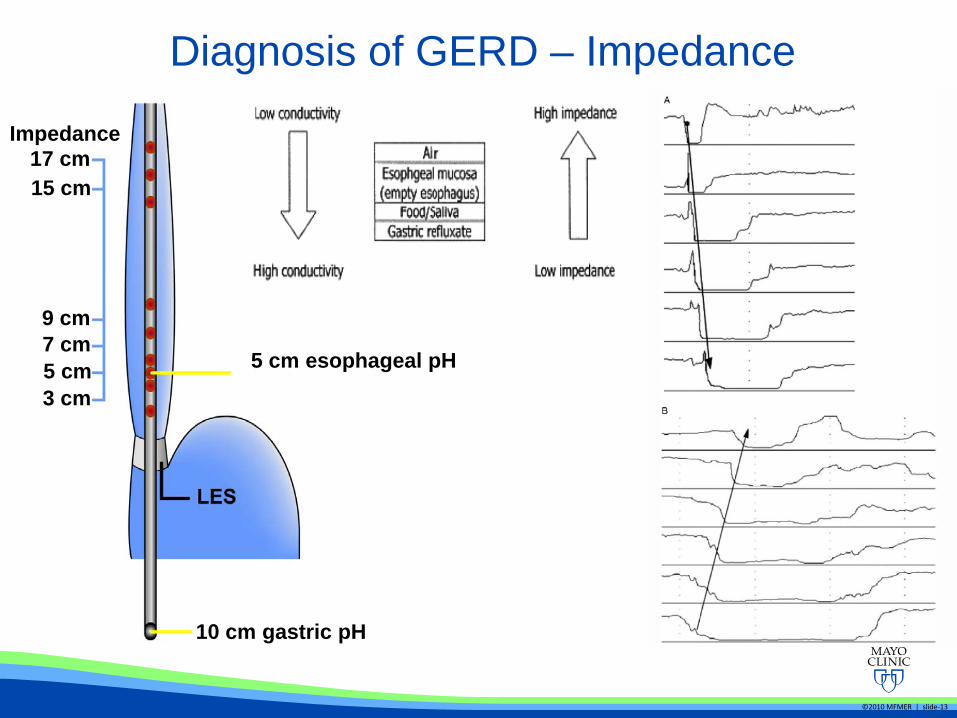
Diagnosis of GERD – Impedance
17 cm 15 cm
9 cm 7 cm 5 cm 3 cm
5 cm esophageal pH
10 cm gastric pH
Impedance
©2010 MFMER | slide-14
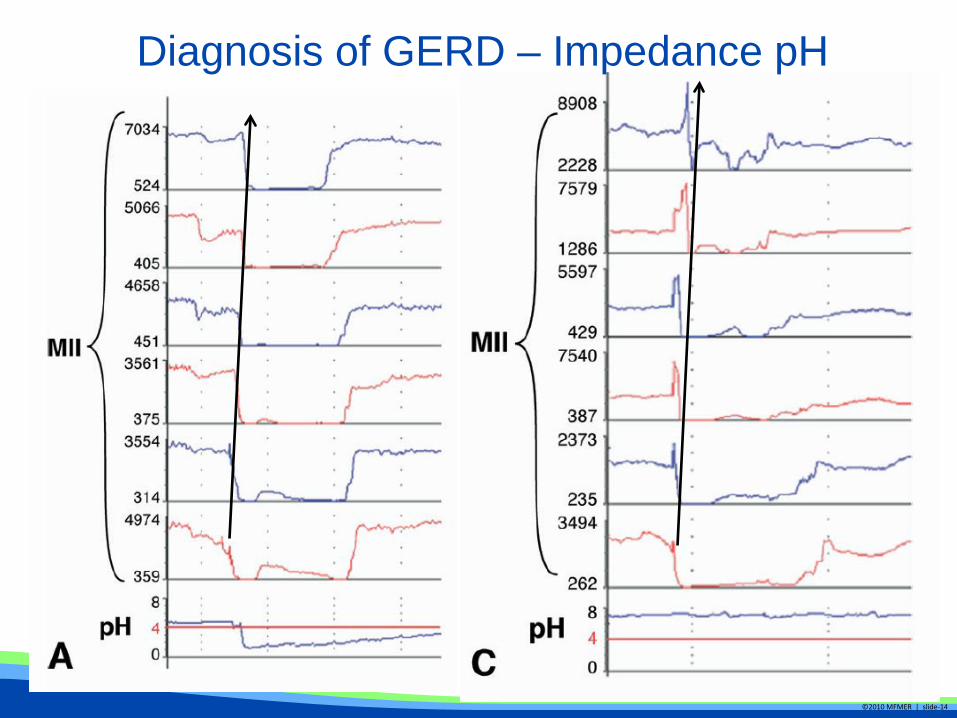
Diagnosis of GERD – Impedance pH
©2010 MFMER | slide-15 ©2012 MFMER | slide-15
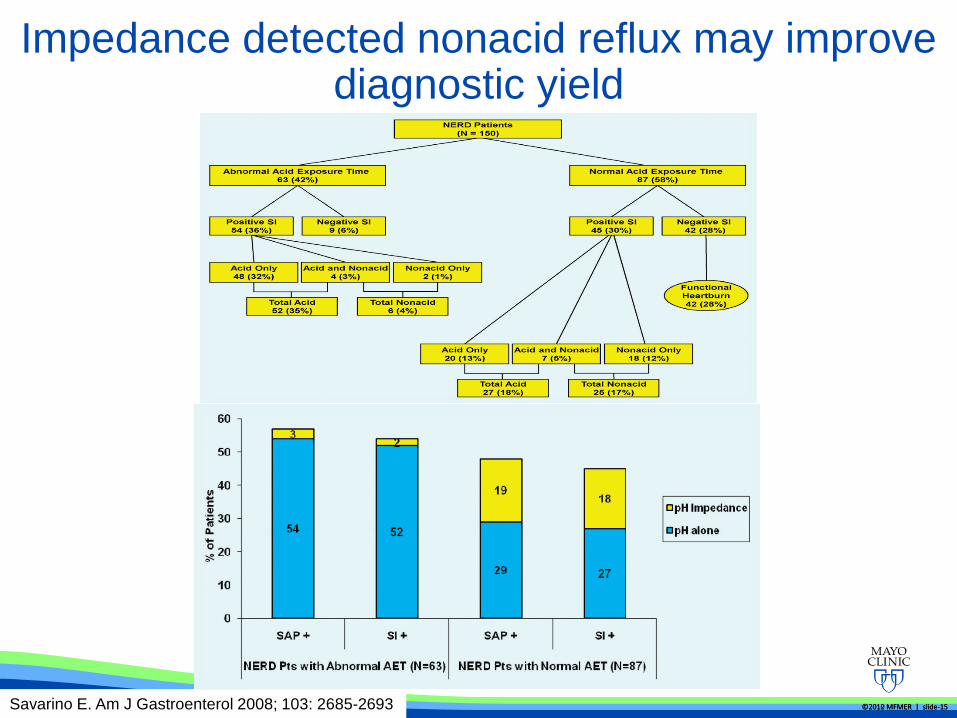
Impedance detected nonacid reflux may improve diagnostic yield
Savarino E. Am J Gastroenterol 2008; 103: 2685-2693
©2010 MFMER | slide-16
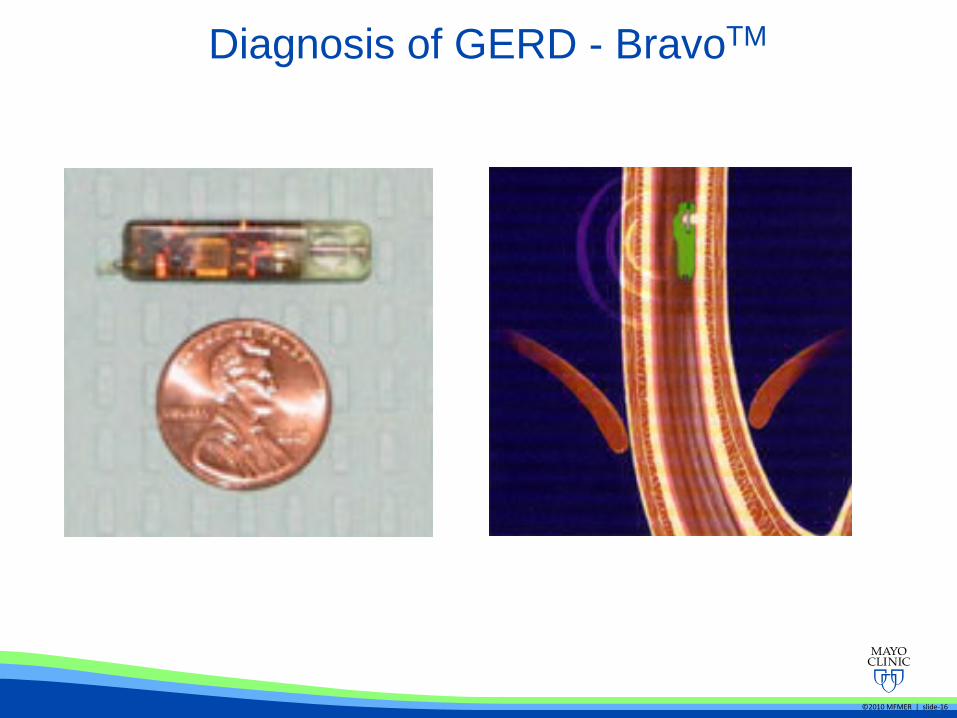
Diagnosis of GERD - BravoTM
• Prolonged measurement • 48 hours standard, up to 96 hours • Allows assessment of more intermittent symptoms
• Better tolerated • More reflux detected (normal pH <4 is 5.4% vs 4.2%) • If patient cannot tolerate catheter • Eliminates problem of catheter drift with swallow
• Limitations: • No measurement of gastric pH • Cannot measure nonacid reflux episodes • 5% get chest pain • Added cost of EGD
Diagnosis of GERD – Bravo vs MII-pH

©2010 MFMER | slide-18
Dietary changes have limited efficacy in GERD
Katz PO. Am J Gastroenterol 2013; 108: 308-328
©2010 MFMER | slide-19
Treatment of GERD – PPI therapy
• Typical • Heartburn • Acid regurgitation • Erosive esophagitis • Stricture • Barrett’s esophagus
• Atypical • Chest pain • Laryngitis • Laryngoedema • Chronic cough • Asthma • Enamel erosion • Sinusitis • Otitis
©2010 MFMER | slide-20
• Typical • Generally responsive • Moderate dose PPI • Objective findings of
reflux common
• Atypical • ENT signs non-specific
and poorly predictive • Objective testing poorly
predicts response • Cause commonly
multifactorial • Treatment to response
is the best indicator • High dose PPI and
nighttime H2-antagonist • Treatment for 3-6
months
Atypical GERD symptoms are unusual and rarely respond to PPI therapy

©2010 MFMER | slide-21 ©2012 MFMER | slide-21
Fass R. Gastroenterology 1998; 115: 42-49
PPI therapy trial is cost effective
Fass R. Aliment Pharmacol Ther 2000; 14: 389-396
©2010 MFMER | slide-22 ©2012 MFMER | slide-22
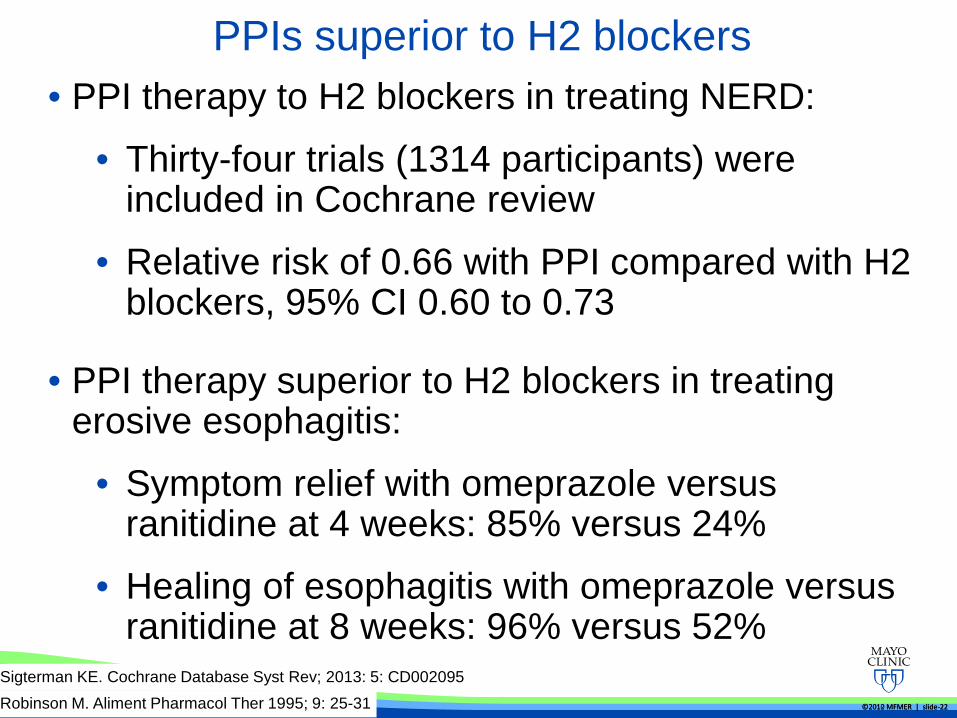
PPIs superior to H2 blockers • PPI therapy to H2 blockers in treating NERD:
• Thirty-four trials (1314 participants) were included in Cochrane review
• Relative risk of 0.66 with PPI compared with H2 blockers, 95% CI 0.60 to 0.73
Sigterman KE. Cochrane Database Syst Rev; 2013: 5: CD002095
• PPI therapy superior to H2 blockers in treating erosive esophagitis:
• Symptom relief with omeprazole versus ranitidine at 4 weeks: 85% versus 24%
• Healing of esophagitis with omeprazole versus ranitidine at 8 weeks: 96% versus 52%
Robinson M. Aliment Pharmacol Ther 1995; 9: 25-31

©2010 MFMER | slide-23 ©2012 MFMER | slide-23
• Mean follow up of 41 months
• 64% on medication at follow up
• Only 13 of 41 off medications without symptoms
Schindlbeck NE. Gut 1992; 33: 1016-1019
Pace F. Aliment Pharmacol Ther 2007; 26: 195-204
NERD can be treated with on demand PPI

©2010 MFMER | slide-24 ©2012 MFMER | slide-24
Long term PPI is needed in erosive esophagitis
Vigneri S. N Engl J Med 1995; 333: 1106-1110

©2010 MFMER | slide-25 ©2012 MFMER | slide-25
Treatment failure is often due to non compliance
El Serag HB. Am J Gastroenterol 2009; 104: 2161-2167

©2010 MFMER | slide-26 ©2012 MFMER | slide-26
Optimizing timing of PPI therapy is important
Gunaratnam NT. Aliment Pharmacol Ther 2006; 23: 1473-1477
• Timing of PPI therapy:
• Optimal if 30 min to 1 hour prior to meals
• PPI accumulate in acid environment of actively secreting parietal cells and be converted to a reactive species via an acid-catalyzed reaction.
• They then covalently inhibit ATPase molecules recruited to the luminal parietal cell surface
©2010 MFMER | slide-27 ©2012 MFMER | slide-27
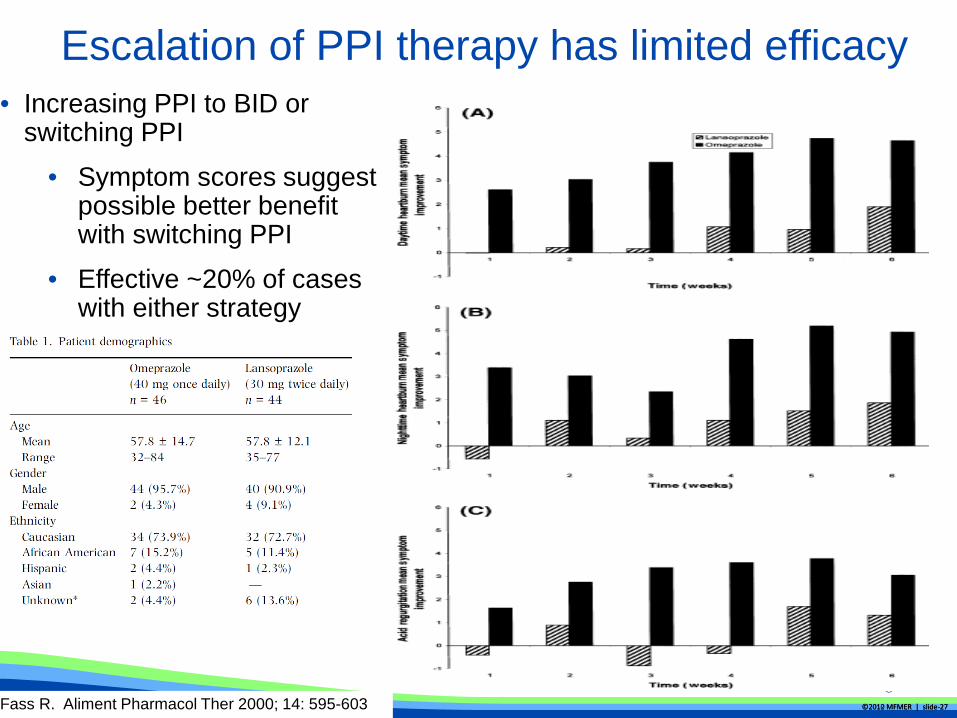
Escalation of PPI therapy has limited efficacy
Fass R. Aliment Pharmacol Ther 2000; 14: 595-603
• Increasing PPI to BID or switching PPI
• Symptom scores suggest possible better benefit with switching PPI
• Effective ~20% of cases with either strategy

©2010 MFMER | slide-28
Side effects of PPI

©2010 MFMER | slide-29 ©2012 MFMER | slide-29
Side effects of PPI - osteoporosis
Targownik LE. Gastroenterology 2010; 138: 896-904
©2010 MFMER | slide-30
PPI Safety
• No clear guidelines for monitoring bone density changed for PPI users or changing dose in known patients with osteoporosis
• No definitive evidence that PPI’s should be stopped in patients on clopidogrel for CAD
• Some evidence suggesting increased risk of C. dificile infection but no large studies. In addition, current evidence seems related to factors such as age and systemic illness rather than PPI use itself.

©2010 MFMER | slide-31
• Persistence of disease on therapy • Erosive esophagitis • Persistent symptoms with + pH study
• Symptoms from non-acid reflux • Large hiatal hernia • Aspiration
• Data unclear or not proven • Atypical manifestations • Equal alternative to medical therapy • Prevention of progression of Barrett’s to cancer
When do you consider fundoplication?
©2010 MFMER | slide-32
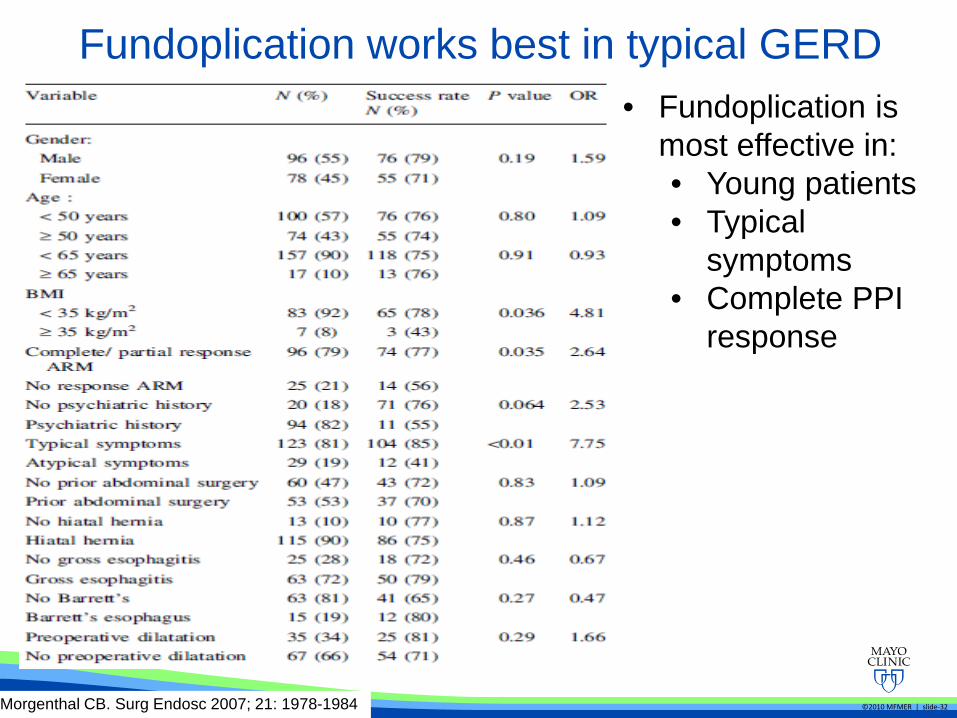
Fundoplication works best in typical GERD
Morgenthal CB. Surg Endosc 2007; 21: 1978-1984
• Fundoplication is most effective in: • Young patients • Typical
symptoms • Complete PPI
response

©2010 MFMER | slide-33 ©2012 MFMER | slide-33
Limitations of fundoplication
Spechler SJ. JAMA 2001; 285: 2331-2338
Richter JE. Clin Gastroenterol Hepatol 2013; 11: 465-471
• Fundoplication is associated with significant limitations: • ~ 50% of patients require medical therapy within 5 years • 5-10% experience significant dysphagia • 5-10% develop gas-bloat syndrome • ~ 50% fail at 10 years follow up

Case
©2010 MFMER | slide-34
A 78 yo man presents with dysphagia to solids and liquids for 3 months. He reports a sense of fullness towards the end of the meal and reports frequent nocturnal regurgitation, awakening with food on the pillow. He reports an associated 20 pound weight loss since onset of symptoms. An esophageal manometry is performed and reveals aperistalsis with incomplete lower esophageal sphincter relaxation.
What is the most appropriate next step?
A. Heller myotomy with partial fundoplication
B. Endoscopic pneumatic dilation
C. Esophagogastroduodenoscopy (EGD)
D. Video fluoroscopy swallow study
E. Ambulatory pH monitoring
Case
©2010 MFMER | slide-35
A 78 yo man presents with dysphagia to solids and liquids for 3 months. He reports a sense of fullness towards the end of the meal and reports frequent nocturnal regurgitation, awakening with food on the pillow. He reports an associated 20 pound weight loss since onset of symptoms. An esophageal manometry is performed and reveals aperistalsis with incomplete lower esophageal sphincter relaxation.
What is the most appropriate next step?
A. Heller myotomy with partial fundoplication
B. Endoscopic pneumatic dilation
C. Esophagogastroduodenoscopy (EGD)
D. Video fluoroscopy swallow study
E. Ambulatory pH monitoring
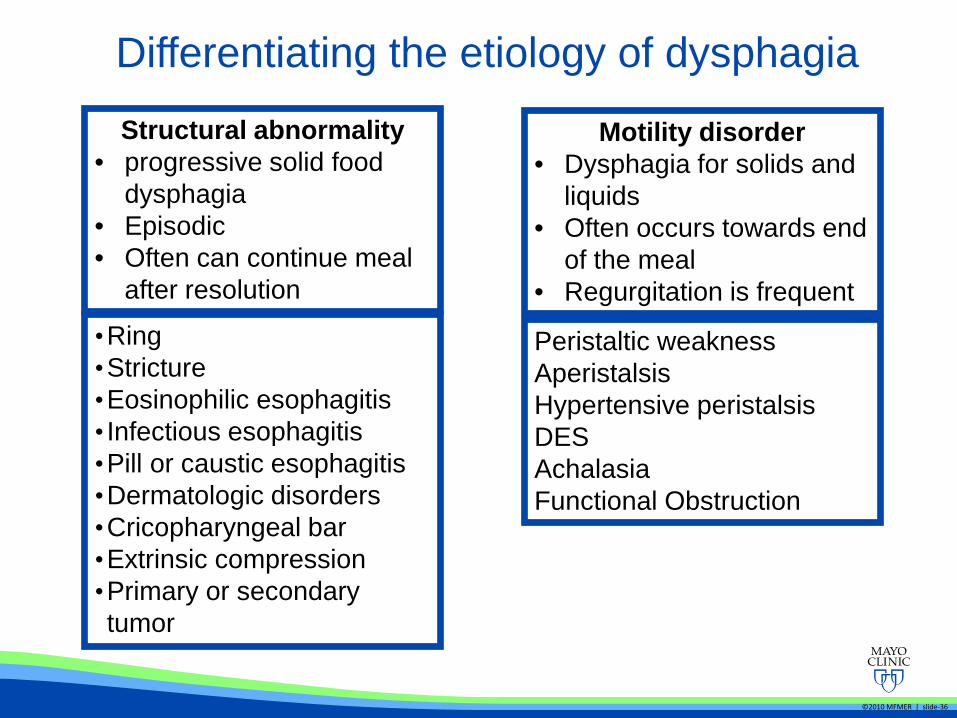
Differentiating the etiology of dysphagia
©2010 MFMER | slide-36
Structural abnormality • progressive solid food
dysphagia • Episodic • Often can continue meal
after resolution
•Ring •Stricture •Eosinophilic esophagitis • Infectious esophagitis •Pill or caustic esophagitis •Dermatologic disorders •Cricopharyngeal bar •Extrinsic compression •Primary or secondary tumor
Motility disorder • Dysphagia for solids and
liquids • Often occurs towards end
of the meal • Regurgitation is frequent
Peristaltic weakness Aperistalsis Hypertensive peristalsis DES Achalasia Functional Obstruction
©2010 MFMER | slide-37
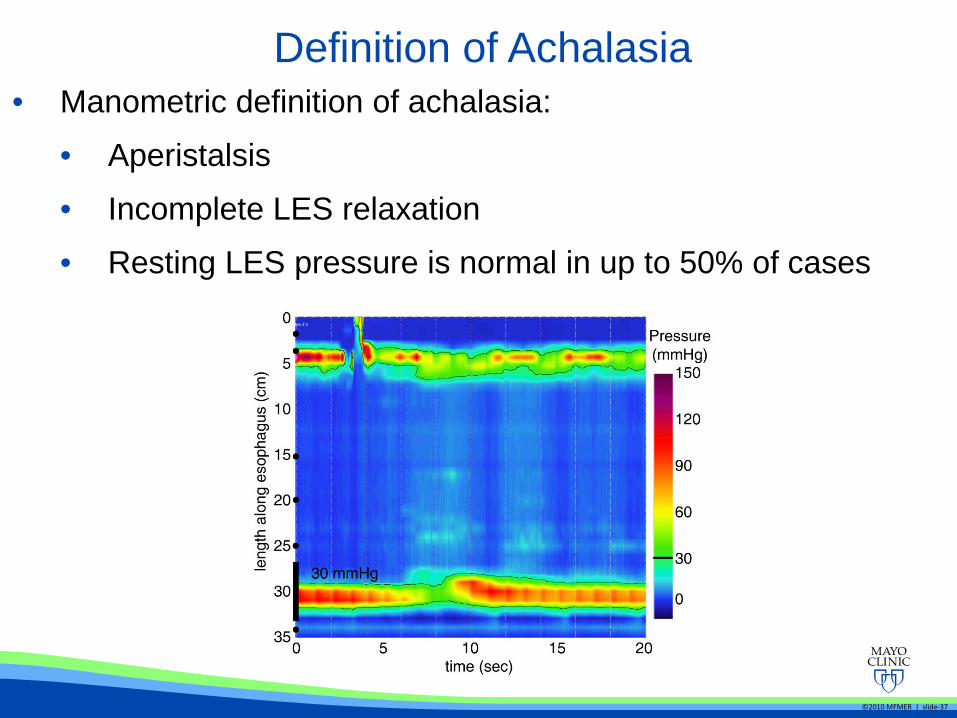
Definition of Achalasia • Manometric definition of achalasia:
• Aperistalsis
• Incomplete LES relaxation
• Resting LES pressure is normal in up to 50% of cases

Clinical presentation of Achalasia
Birgisson S. Dig Dis Sci 2007; 52: 1855-1860
©2010 MFMER | slide-39
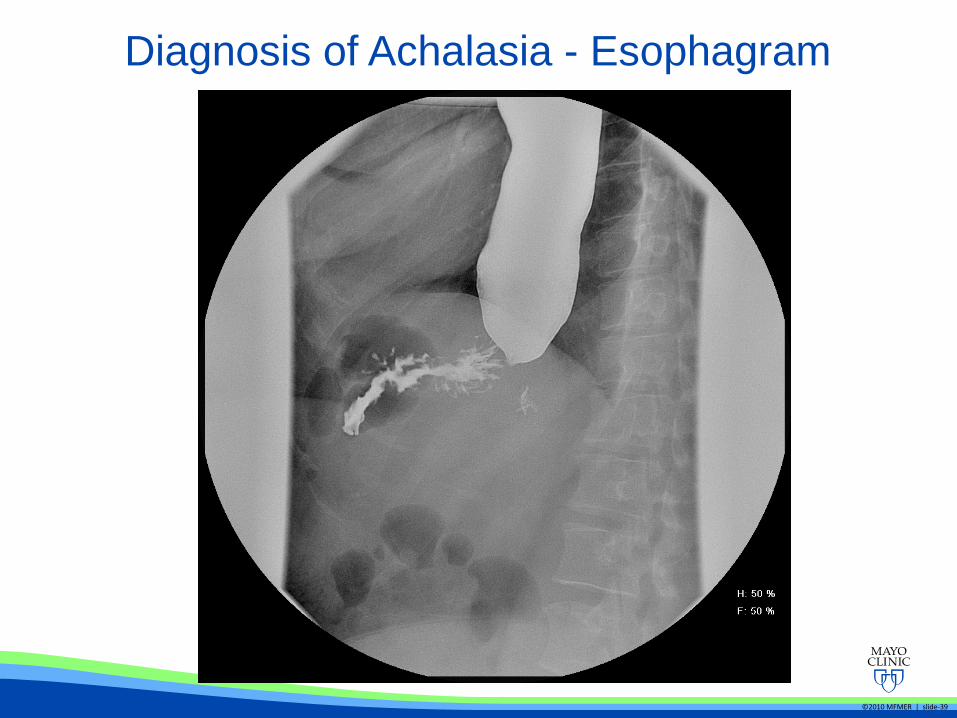
Diagnosis of Achalasia - Esophagram

Diagnosis of Achalasia - EGD
Howard PJ. Gut 1992; 33: 1011-1015
• EGD is normal in 40% of patients with achalasia
• Rule out pseudoachalasia
• up to 5% of cases
• Older patient, rapid progression of symptoms and weight loss
• Most often gastroesophageal junction malignancy
• Can represent a paraneoplastic phenomenon (lung cancer) Kharilas PJ. Am J Med 1987; 82: 439-446
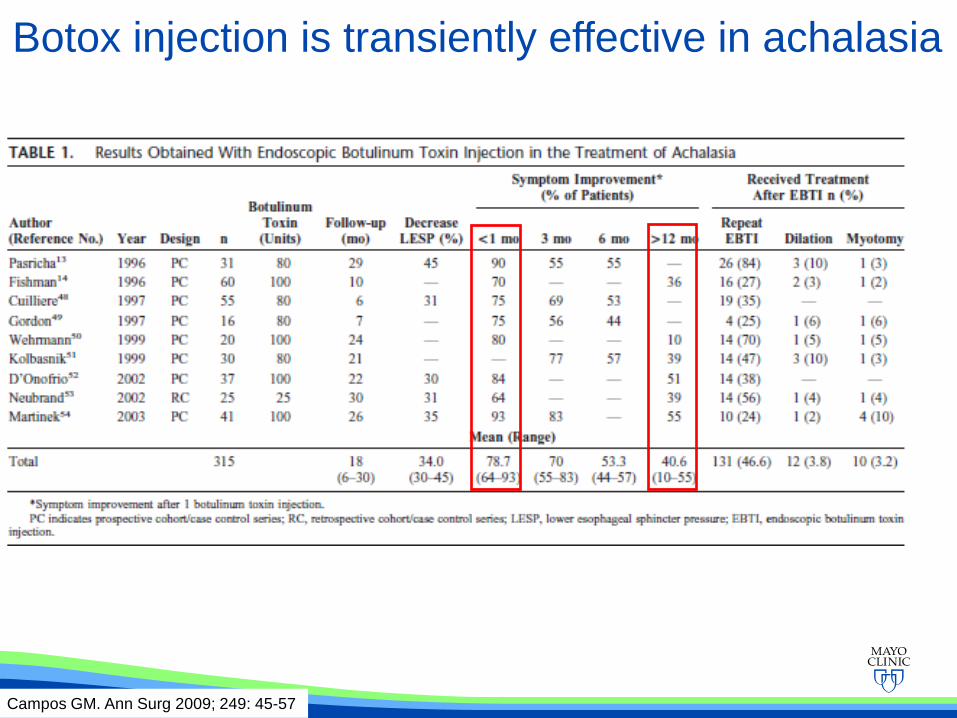
Campos GM. Ann Surg 2009; 249: 45-57
Botox injection is transiently effective in achalasia

Achalasia treatment
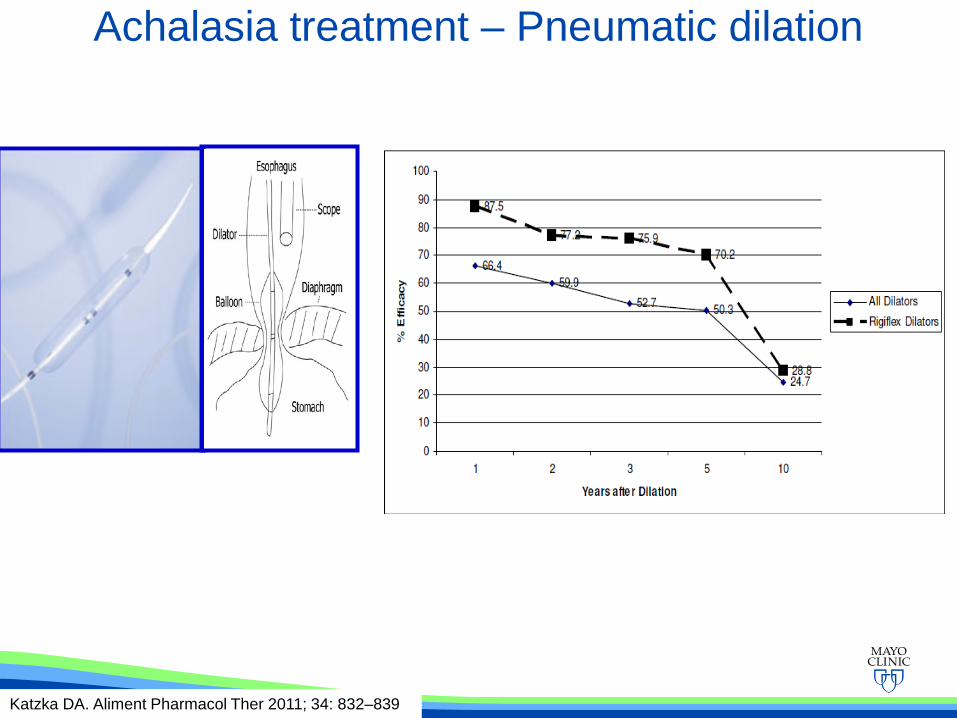
Achalasia treatment – Pneumatic dilation
Katzka DA. Aliment Pharmacol Ther 2011; 34: 832–839
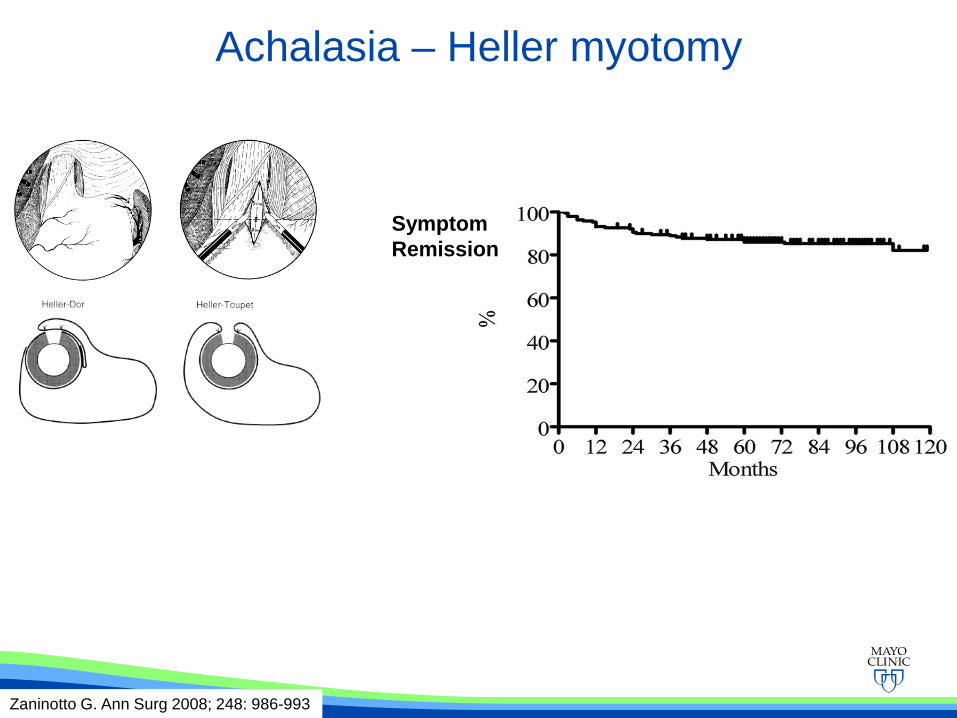
Achalasia – Heller myotomy
Zaninotto G. Ann Surg 2008; 248: 986-993
Symptom Remission
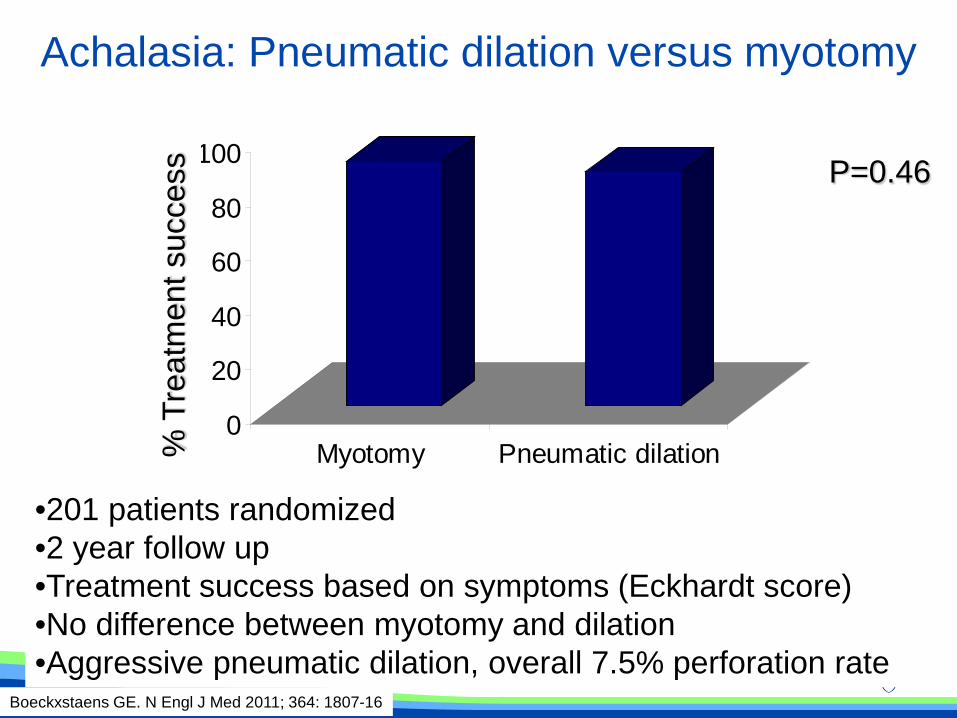
Achalasia: Pneumatic dilation versus myotomy
0
20
40
60
80
100
Myotomy Pneumatic dilation
P=0.46 %
Tre
atm
ent s
ucce
ss
Boeckxstaens GE. N Engl J Med 2011; 364: 1807-16
•201 patients randomized •2 year follow up •Treatment success based on symptoms (Eckhardt score) •No difference between myotomy and dilation •Aggressive pneumatic dilation, overall 7.5% perforation rate
©2010 MFMER | slide-46
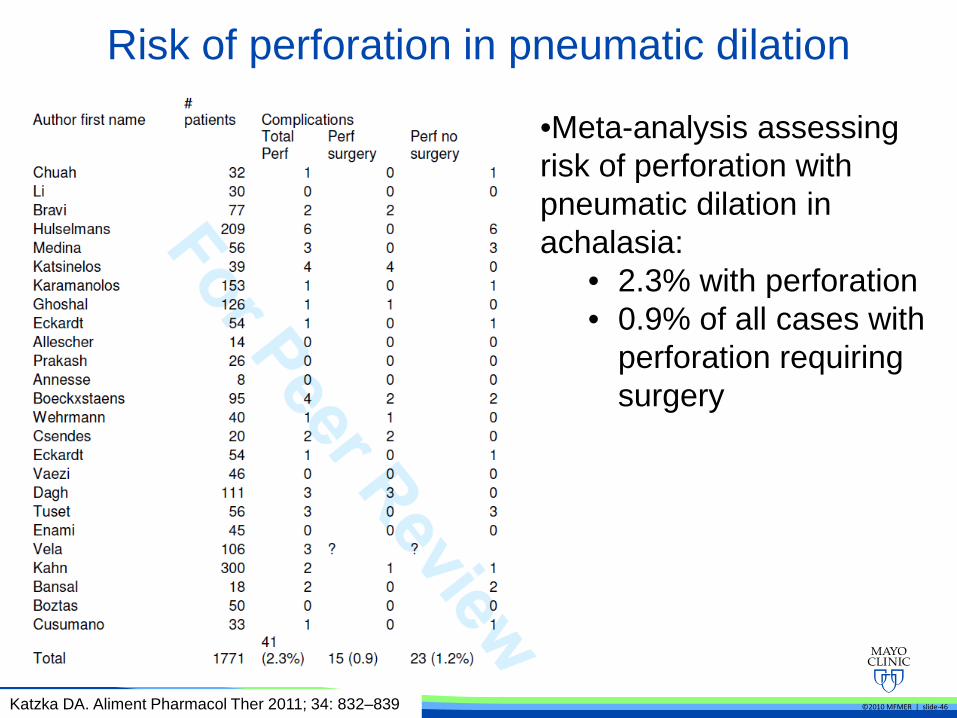
Risk of perforation in pneumatic dilation
Katzka DA. Aliment Pharmacol Ther 2011; 34: 832–839
•Meta-analysis assessing risk of perforation with pneumatic dilation in achalasia:
• 2.3% with perforation • 0.9% of all cases with
perforation requiring surgery

Subtypes of Achalasia
Pandolfino JE et al, Gastroenterology 2008Nov;135(5):1526-33
Type 1 Achalasia (classic)
Type 2 Achalasia, • Panesophageal pressure
• ≥ 20% with >20mmHg
Type 3 Achalasia, • ≥ 20% spastic
• DL <4.5sec, CFV >10cm/s)
Early Type II
Late Type I
Chronic Type II--I
Netter Atlas
Subtypes of Achalasia
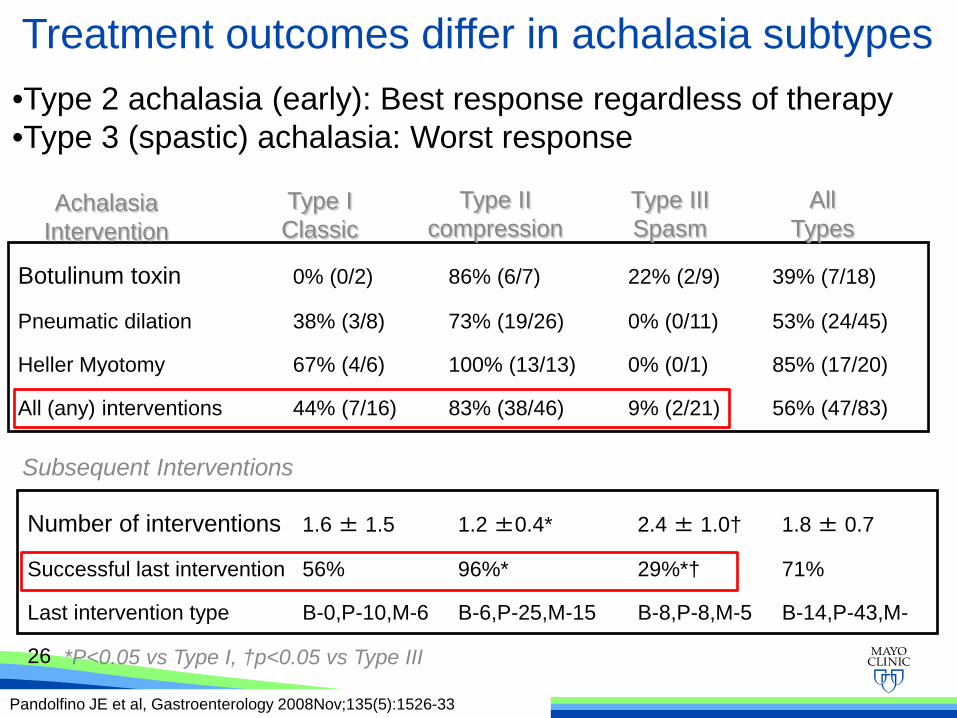
Botulinum toxin 0% (0/2) 86% (6/7) 22% (2/9) 39% (7/18)
Pneumatic dilation 38% (3/8) 73% (19/26) 0% (0/11) 53% (24/45)
Heller Myotomy 67% (4/6) 100% (13/13) 0% (0/1) 85% (17/20)
All (any) interventions 44% (7/16) 83% (38/46) 9% (2/21) 56% (47/83)
Number of interventions 1.6 ± 1.5 1.2 ±0.4* 2.4 ± 1.0† 1.8 ± 0.7
Successful last intervention 56% 96%* 29%*† 71%
Last intervention type B-0,P-10,M-6 B-6,P-25,M-15 B-8,P-8,M-5 B-14,P-43,M-
26
Subsequent Interventions
*P<0.05 vs Type I, †p<0.05 vs Type III
Achalasia Intervention
Type I Classic
Type II compression
Type III Spasm
All Types
Treatment outcomes differ in achalasia subtypes
Pandolfino JE et al, Gastroenterology 2008Nov;135(5):1526-33
•Type 2 achalasia (early): Best response regardless of therapy •Type 3 (spastic) achalasia: Worst response