XXXIX Congresso Nazionale ANMCO Firenze, 30 maggio- 2 giugno 2008 Minimaster Cuore e diabete –...
86
XXXIX Congresso Nazionale ANMCO Firenze, 30 maggio- 2 giugno 2008 Minimaster Cuore e diabete – Prevenzione delle recidive e aderenza alle terapie Cardioprotezione farmacologica Cardioprotezione farmacologica a lungo termine: a lungo termine: il punto sulle statine il punto sulle statine Stefano Urbinati Stefano Urbinati UOC Cardiologia UOC Cardiologia Ospedale Bellaria, Ospedale Bellaria, Bologna Bologna
-
Upload
julia-anderson -
Category
Documents
-
view
216 -
download
1
Transcript of XXXIX Congresso Nazionale ANMCO Firenze, 30 maggio- 2 giugno 2008 Minimaster Cuore e diabete –...

XXXIX Congresso Nazionale ANMCOFirenze, 30 maggio- 2 giugno 2008
MinimasterCuore e diabete – Prevenzione delle recidive e aderenza alle terapie
XXXIX Congresso Nazionale ANMCOFirenze, 30 maggio- 2 giugno 2008
MinimasterCuore e diabete – Prevenzione delle recidive e aderenza alle terapie
Cardioprotezione farmacologica Cardioprotezione farmacologica a lungo termine:a lungo termine:
il punto sulle statine il punto sulle statine
Cardioprotezione farmacologica Cardioprotezione farmacologica a lungo termine:a lungo termine:
il punto sulle statine il punto sulle statine
Stefano UrbinatiStefano Urbinati
UOC CardiologiaUOC CardiologiaOspedale Bellaria, BolognaOspedale Bellaria, Bologna
Stefano UrbinatiStefano Urbinati
UOC CardiologiaUOC CardiologiaOspedale Bellaria, BolognaOspedale Bellaria, Bologna

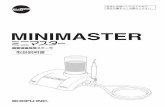
Diagnosi di nuovi casi di diabete:
siamo abbastanza attenti?

EuroHeart Surveyn=3940 pts with known glucometabolic state
Newly detected DMn= 452 (11%)
After a 1-year follow-up period
On treatment for DMn= 77 (17%)
No treatment for DMn= 375 (83%)
0 mortality 25 p<0.002 1 MI 13 1 stroke 5
Anselmino et al, Eur Heart J 2008;29:177-84

Anselmino et al, Eur Heart J 2008;29:177-84
Kaplan Meyer curves for combined CV events in pts with newly detected DM by prescribed or not prescribed
pharmacological treatment
Tx for DM
no Tx for DM

… the general impression is that pts with CAD and DM areinappropriately managed for several reasons…
1. Cardiologists neglect o are inexperienced as regards GL treatments
2. A close collaboration between cardiologists and diabetologists is absent
3. The present findings are due to the well known “clinical inertia” that affect both specialists and primary care physiscians
Anselmino et al, Eur Heart J 2008;29:177-84

Dislipidemia nel diabetico:entità del problema

7
LP267611LP267611
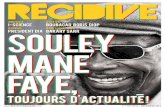
High Incidence of Dyslipidemia in the Diabetic PopulationHigh Incidence of Dyslipidemia in the Diabetic Population
Modified from Jacobs MJ et al. Modified from Jacobs MJ et al. Diabetes Res Clin PractDiabetes Res Clin Pract. 2005;70:263-269.. 2005;70:263-269.
0%
20%
40%
60%
80%
100%
Men Women Men Women Men Women
Pa
tie
nts
wit
h d
iab
ete
s (
%)*
0%
20%
40%
60%
80%
100%
Men Women Men Women Men Women
Pa
tie
nts
wit
h d
iab
ete
s (
%)*
LDL-C (mg/dL)LDL-C (mg/dL) Triglycerides (mg/dL)Triglycerides (mg/dL) HDL-C (mg/dL)HDL-C (mg/dL)
130130
100-129100-129
<100<100
200200
150-199150-199
<150<150
Men 40
Women 50
Men 40
Women 50
Men>40
Women>50
Men>40
Women>50
*245 men with diabetes and 253 women with diabetes *245 men with diabetes and 253 women with diabetes aged aged 18 years from NHANES 1999-2000.18 years from NHANES 1999-2000.

8
LP267611LP267611
MRFIT*: Cardiovascular Disease (CVD) Mortality 3 Times Greater in Men With Diabetes at All Cholesterol Levels
MRFIT*: Cardiovascular Disease (CVD) Mortality 3 Times Greater in Men With Diabetes at All Cholesterol Levels
0
20
40
60
80
100
120
140
160
<180 180-199 200-219 220-239 240-259 260-279 >279
Serum cholesterol (mg/dL)
Ag
e-ad
just
ed C
VD
dea
th r
ate
(per
10,
000
per
son
-yea
rs)
Men with diabetes (n=5163)
Men without diabetes (n=342,815)
0
20
40
60
80
100
120
140
160
<180 180-199 200-219 220-239 240-259 260-279 >279
Serum cholesterol (mg/dL)
Ag
e-ad
just
ed C
VD
dea
th r
ate
(per
10,
000
per
son
-yea
rs)
Men with diabetes (n=5163)
Men without diabetes (n=342,815)
Stamler J et al. Stamler J et al. Diabetes Care.Diabetes Care. 1993;16:434-444. 1993;16:434-444.**Multiple Risk Factor Intervention TrialMultiple Risk Factor Intervention Trial

9
LP267611LP267611
UKPDS*: Order of Importance of CHD Risk FactorsUKPDS*: Order of Importance of CHD Risk Factors
Stepwise selection of risk factors, adjusted for age and sex, in 2693 white patients with diabetes, with dependent variable as time to first CHD event.
Stepwise selection of risk factors, adjusted for age and sex, in 2693 white patients with diabetes, with dependent variable as time to first CHD event.
Turner RC et al. Turner RC et al. BMJ.BMJ. 1998;316:823-828. 1998;316:823-828.
Variable P-value
1. LDL-C1. LDL-C <0.0001<0.0001
2. HDL-C2. HDL-C 0.00010.0001
3. HbA3. HbA1c1c 0.00220.0022
4. Systolic BP4. Systolic BP 0.00650.0065
5. Smoking5. Smoking 0.0560.056
**United Kingdom Prospective Diabetes Study.United Kingdom Prospective Diabetes Study.

10
LP267611LP267611
UKPDS: LDL-C Is a Very Strong Predictor of CHD Risk in Patients With DiabetesUKPDS: LDL-C Is a Very Strong Predictor of CHD Risk in Patients With Diabetes
Relation of lipid risk factors* to CHD in 2693 patients with diabetesRelation of lipid risk factors* to CHD in 2693 patients with diabetes
Turner RC et al. Turner RC et al. BMJ.BMJ. 1998;316:823-828. 1998;316:823-828.
0.0
0.5
1.0
1.5
2.0
2.5
<189
189-
223
>223
0.0
0.5
1.0
1.5
2.0
2.5
<189
189-
223
>223
Total cholesterolP<0.0001Total cholesterolP<0.0001
0.0
0.5
1.0
1.5
2.0
2.5
<117
117-
150
>150
0.0
0.5
1.0
1.5
2.0
2.5
<117
117-
150
>150
LDL-CP<0.0001LDL-CP<0.0001
0.0
0.5
1.0
1.5
2.0
2.5
<108
108-
166
>166
0.0
0.5
1.0
1.5
2.0
2.5
<108
108-
166
>166
TriglyceridesP<0.0001TriglyceridesP<0.0001
0.0
0.5
1.0
1.5
2.0
2.5
0.0
0.5
1.0
1.5
2.0
2.5
HDL-CP<0.0001HDL-CP<0.0001
Haz
ard
ra
tio
Haz
ard
ra
tio
Lipid tertiles (mg/dL)Lipid tertiles (mg/dL)
*Age- and sex-adjusted.*Age- and sex-adjusted.

11
LP267611LP267611
Atherogenicity of DiabetesAtherogenicity of Diabetes
Lipid abnormalities may represent an atherogenic phenotype in type 2 diabetes patients that accelerates atherosclerosis and CHD
Characteristic abnormalities of type 2 diabetes include: Decreased HDL-C
Elevated triglycerides
Absolute concentration of LDL-C not significantly increased; however, people with diabetes often have a preponderance of smaller, denser LDL particles, which may increase atherogenicity
Lipid abnormalities may represent an atherogenic phenotype in type 2 diabetes patients that accelerates atherosclerosis and CHD
Characteristic abnormalities of type 2 diabetes include: Decreased HDL-C
Elevated triglycerides
Absolute concentration of LDL-C not significantly increased; however, people with diabetes often have a preponderance of smaller, denser LDL particles, which may increase atherogenicity
American Diabetes Association. American Diabetes Association. Diabetes Care.Diabetes Care. 2003;26:S83-S86. 2003;26:S83-S86.

Dislipidemia nel diabetico:l’importanza di un
approccio multidisciplinare

Gaede et al for the STENO-2 Investigators, NEJM 2003;348:383-93
Our study was not designed to identify which elements ofintensive diabetes therapy contributed most to the reduction in CV risk.
Using a risk calculator based on UKPDS, we concluded thatthe use of statins and antihypertensive drugs have the largest effect in reducing CV risk during the 7.8 yrs ofinterventions, with hypoglicemic agents and aspirin the nextmost important interventions.
Effect of a multifactorial intervention on mortality in type 2 diabetes

Evidenze sull’efficacia delle statine nel diabetico

15
LP267611LP267611
Early Statin Secondary Prevention Trials: Design OverviewEarly Statin Secondary Prevention Trials: Design Overview
Primary end point: All-cause mortalityPrimary end point: All-cause mortality
Median follow-up: 5.4 yearsMedian follow-up: 5.4 years
Simvastatin 20-40 mg/daySimvastatin 20-40 mg/day(n=2221)(n=2221)
PlaceboPlacebo(n=2223)(n=2223)
4444 patients4444 patients
4S4S Age: 35-70 yearsAge: 35-70 years Previous MI or anginaPrevious MI or angina TC: 5.5-8.0 mmol/L (213-309 mg/dL)TC: 5.5-8.0 mmol/L (213-309 mg/dL) Triglycerides: Triglycerides: 2.5 mmol/L (2.5 mmol/L (221 mg/dL)221 mg/dL)
CARECARE Age: 21-75 yearsAge: 21-75 years MI in previous 3-20 monthsMI in previous 3-20 months TC: <240 mg/dL (<6.2 mmol/L)TC: <240 mg/dL (<6.2 mmol/L) LDL-C:115-174 mg/dL (3.0-4.5 mmol/L)LDL-C:115-174 mg/dL (3.0-4.5 mmol/L) Triglycerides: <350 mg/dL (<4.0 mmol/L)Triglycerides: <350 mg/dL (<4.0 mmol/L)
4159 patients4159 patients
Pravastatin 40 mg/dayPravastatin 40 mg/day(n=2081)(n=2081)
PlaceboPlacebo(n=2078)(n=2078)
Median follow-up: 5.0 yearsMedian follow-up: 5.0 years
Primary end point: CHD death + nonfatal MIPrimary end point: CHD death + nonfatal MI
Primary end point: CHD deathPrimary end point: CHD death
LIPIDLIPID Age: 31-75 yearsAge: 31-75 years MI or unstable angina in previousMI or unstable angina in previous
3-36 months3-36 months TC: 155-271 mg/dL (4.0-7.0 mmol/L)TC: 155-271 mg/dL (4.0-7.0 mmol/L) Triglycerides <445 mg/dL (<5.0 mmol/L)Triglycerides <445 mg/dL (<5.0 mmol/L)
9014 patients9014 patients
Pravastatin 40 mg/dayPravastatin 40 mg/day(n=4512)(n=4512)
PlaceboPlacebo(n=4502)(n=4502)
Mean follow-up: 6.1 yearsMean follow-up: 6.1 years
4S Study Group. 4S Study Group. LancetLancet. 1994;334:1383-1389.. 1994;334:1383-1389.
Sacks F et al. Sacks F et al. N Engl J MedN Engl J Med. 1996;335:1001-1009.. 1996;335:1001-1009.
LIPID Study Group. LIPID Study Group. N Engl J MedN Engl J Med. 1998;339:1349-1357.. 1998;339:1349-1357.

16
LP267611LP267611
4S: Major CHD Event Reduction in Patients With Diabetes*4S: Major CHD Event Reduction in Patients With Diabetes*
PyöräläPyörälä K et al. K et al. Diabetes CareDiabetes Care. 1997;20:614-620.. 1997;20:614-620.*Post-hoc analysis of the secondary end point: *Post-hoc analysis of the secondary end point: CHD death + nonfatal MI.CHD death + nonfatal MI.
40
50
60
70
80
90
100
0 1 2 3 4 5 640
50
60
70
80
90
100
0 1 2 3 4 5 6
RRR=32%RRR=32%PP=0.0001=0.0001
Pat
ien
ts w
ith
ou
t m
ajo
r C
VD
eve
nt
(%)
Pat
ien
ts w
ith
ou
t m
ajo
r C
VD
eve
nt
(%)
Time (years)Time (years)
Diabetes, simvastatin 20-40 mg (n=105)Diabetes, simvastatin 20-40 mg (n=105)
Diabetes, placebo (n=97)Diabetes, placebo (n=97)
No diabetes, simvastatin 20-40 mg (n=2116)No diabetes, simvastatin 20-40 mg (n=2116)
No diabetes, placebo (n=2126)No diabetes, placebo (n=2126)RRR=55% RRR=55% PP=0.002=0.002

17
LP267611LP267611
Goldberg RB et al. Goldberg RB et al. CirculationCirculation. 1998;98:2513-2519.. 1998;98:2513-2519.
CARE: CHD Event Reduction in Patients With Diabetes*CARE: CHD Event Reduction in Patients With Diabetes*
*Post hoc analysis of an expanded CHD end point: *Post hoc analysis of an expanded CHD end point: CHD death, nonfatal MI, CABG, and PTCA.CHD death, nonfatal MI, CABG, and PTCA.
0
5
10
15
20
25
30
35
40
45
0 1 2 3 4 5
0
5
10
15
20
25
30
35
40
45
0 1 2 3 4 5
RRR=25%RRR=25%PP=0.05=0.05
Cu
mu
lati
ve in
cid
ence
C
um
ula
tive
inci
den
ce
of
even
ts (
% o
f p
atie
nts
) o
f ev
ents
(%
of
pat
ien
ts)
Time (years)Time (years)
Diabetes, pravastatin 40 mg (n=282)Diabetes, pravastatin 40 mg (n=282)
Diabetes, placebo (n=304)Diabetes, placebo (n=304)
No diabetes, pravastatin 40 mg (n=1779)No diabetes, pravastatin 40 mg (n=1779)
No diabetes, placebo (n=1774)No diabetes, placebo (n=1774)
RRR=23% RRR=23% PP<0.001<0.001

18
LP267611LP267611
LIPID: CHD Event Reduction in Patients With Diabetes*LIPID: CHD Event Reduction in Patients With Diabetes*
Keech A et al. Keech A et al. Diabetes CareDiabetes Care. 2003;26:2713-2721.. 2003;26:2713-2721.*Pre-specified diabetes subgroup primary endpoint: *Pre-specified diabetes subgroup primary endpoint: CHD death and nonfatal MI.CHD death and nonfatal MI.
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7
RRR=19%RRR=19%PP=0.11=0.11
Cu
mu
lati
ve in
cid
ence
C
um
ula
tive
inci
den
ce
of
even
ts (
% o
f p
atie
nts
)o
f ev
ents
(%
of
pat
ien
ts)
Time (years)Time (years)
Diabetes, pravastatin 40 mg (n=542)Diabetes, pravastatin 40 mg (n=542)
Diabetes, placebo (n=535)Diabetes, placebo (n=535)
No diabetes, pravastatin 40 mg (n=3496)No diabetes, pravastatin 40 mg (n=3496)
No diabetes, placebo (n=3501)No diabetes, placebo (n=3501)
RRR=23%RRR=23%PP=0.001=0.001

19
LP267611LP267611
Mean follow-up 4.8 yearsMean follow-up 4.8 years
HPS: Primary and Secondary Prevention of CVD in Patients With DiabetesHPS: Primary and Secondary Prevention of CVD in Patients With Diabetes
Without CVDWithout CVD(n=2912)(n=2912)
With CVDWith CVD(n=3051)(n=3051)
5963 patients 5963 patients with diabeteswith diabetes
Pre-specified diabetes subgroupPre-specified diabetes subgroupend points:end points: Major coronary events Major coronary events Major vascular eventsMajor vascular events
Patient population:Patient population: Age: 40-80 yearsAge: 40-80 years TC: TC: 3.5 mmol/L (135 mg/dL)3.5 mmol/L (135 mg/dL) At least one of:At least one of:
– Diabetes mellitusDiabetes mellitus– CHDCHD– Occlusive noncoronary artery diseaseOcclusive noncoronary artery disease– Treated hypertension (men aged Treated hypertension (men aged 65 years)65 years)
Simvastatin 40 mg/daySimvastatin 40 mg/day(n=1455)(n=1455)
Simvastatin 40 mg/daySimvastatin 40 mg/day(n=1523)(n=1523)
PlaceboPlacebo(n=1457)(n=1457)
PlaceboPlacebo(n=1528)(n=1528)
HPS Collaborative Group. HPS Collaborative Group. LancetLancet. 2003;361:2005-2016.. 2003;361:2005-2016.

20
LP267611LP267611HPS: Subgroup Evaluation Shows Consistent Benefit in Diabetic Patients Regardless of CVD
HPS: Subgroup Evaluation Shows Consistent Benefit in Diabetic Patients Regardless of CVD
HPS Collaborative Group. HPS Collaborative Group. LancetLancet. 2003;361:2005-2016.. 2003;361:2005-2016.Numbers in bars represent number of patients Numbers in bars represent number of patients in category at baseline.in category at baseline.
0
10
20
30
40
50
Inc
ide
nc
e o
f m
ajo
r v
as
cu
lar
ev
en
ts (
%)
Placebo
Simvastatin 40 mg
0
10
20
30
40
50
Inc
ide
nc
e o
f m
ajo
r v
as
cu
lar
ev
en
ts (
%)
Placebo
Simvastatin 40 mg
RRRRRR12%12%
RRRRRR23%23%
RRRRRR22%22%
RRRRRR19%19%
RRRRRR31%31%
Diabetes Diabetes + CHD+ CHD
No diabetes No diabetes + CHD+ CHD
Diabetes Diabetes + other CVD+ other CVD
No diabetes No diabetes + other CVD+ other CVD
Diabetes Diabetes + no CVD+ no CVD
10091009 972972 56835683 57225722 519519 551551 14811481 14491449 14571457 14551455

21
LP267611LP267611
HPS: Consistent Benefit in Diabetic Patients Regardless of Baseline LDL-CHPS: Consistent Benefit in Diabetic Patients Regardless of Baseline LDL-C
HPS Collaborative Group. HPS Collaborative Group. LancetLancet. 2003;361:2005-2016.. 2003;361:2005-2016.Numbers in bars represent number of patients Numbers in bars represent number of patients in category at baseline.in category at baseline.
0
10
20
30
40
Diabetes No diabetes Diabetes No diabetes
Inc
ide
nc
e o
f m
ajo
r v
as
cu
lar
ev
en
ts (
%) Placebo
Simvastatin 40 mg
0
10
20
30
40
Diabetes No diabetes Diabetes No diabetes
Inc
ide
nc
e o
f m
ajo
r v
as
cu
lar
ev
en
ts (
%) Placebo
Simvastatin 40 mg
RRRRRR25%25%
RRRRRR18%18%
RRRRRR16%16%
RRRRRR24%24%
12071207 12191219 21972197 21702170 17781778 17591759 50855085 51215121
LDL <116 mg/dLLDL <116 mg/dL LDL LDL 116 mg/dL116 mg/dL

22
LP267611LP267611
HPS: ImplicationsHPS: Implications
Contributed to changes in treatment recommendations for diabetic patients:
2003 European Guidelines for the Management of CVD:
> total cholesterol <175 mg/dL and LDL-C <100 mg/dL
2004 ADA recommendations:> focus on LDL-C lowering as the primary lipid goal (<100 mg/dL)> statins recommended as the initial pharmacologic approach
2004 NCEP ATP update:> LDL-C goal of <70 mg/dL in very high-risk patients
Contributed to changes in treatment recommendations for diabetic patients:
2003 European Guidelines for the Management of CVD:
> total cholesterol <175 mg/dL and LDL-C <100 mg/dL
2004 ADA recommendations:> focus on LDL-C lowering as the primary lipid goal (<100 mg/dL)> statins recommended as the initial pharmacologic approach
2004 NCEP ATP update:> LDL-C goal of <70 mg/dL in very high-risk patients

CTT Collaborators, Lancet 2008; 371: 117-125

CTT Collaborators, Lancet 2008; 371: 117-125

CTT Collaborators, Lancet 2008; 371: 117-125

CTT Collaborators, Lancet 2008; 371: 117-125

CTT Collaborators, Lancet 2008; 371: 117-125

CTT Collaborators, Lancet 2008; 371: 117-125

CTT Collaborators, Lancet 2008; 371: 117-125

CTT Collaborators, Lancet 2008; 371: 117-125

Uno studio randomizzato con statine
realizzato espressamentenei diabetici:
lo studio CARDS

32
LP267611LP267611
CARDS: The RationaleCARDS: The Rationale
Elevated cardiovascular risk associated with type 2 diabetes
The role of lipid-lowering for secondary prevention of CHD in this population, particularly with statins, is clearly defined
No previous statin trial had been exclusively designed to test the benefit of statin intervention in diabetic patients without CHD and with baseline LDL-C levels below contemporary treatment guidelines
Elevated cardiovascular risk associated with type 2 diabetes
The role of lipid-lowering for secondary prevention of CHD in this population, particularly with statins, is clearly defined
No previous statin trial had been exclusively designed to test the benefit of statin intervention in diabetic patients without CHD and with baseline LDL-C levels below contemporary treatment guidelines

33
LP267611LP267611
4-year follow-up4-year follow-up
CARDS: Primary Prevention of CVD With Atorvastatin in Type 2 DiabetesCARDS: Primary Prevention of CVD With Atorvastatin in Type 2 Diabetes
Atorvastatin 10 mg/day(n=1428)
Placebo(n=1410)
2838 patients2838 patients
Primary end point: Incidence of major cardiovascular events:
– Cardiovascular-related death– Nonfatal MI– Stroke– Resuscitated cardiac arrest– Unstable angina– Coronary revascularization procedures
Patient population: Age: 40-75 years LDL-C 160 mg/dL Triglycerides 600 mg/dL Type 2 diabetes No prior MI or CHD 1+ CHD risk factor
Study completion date
Anticipated:Anticipated: Early 2005 Early 2005
Actual:Actual: Halted 2 years early Halted 2 years early due to significant resultsdue to significant results
Study completion date
Anticipated:Anticipated: Early 2005 Early 2005
Actual:Actual: Halted 2 years early Halted 2 years early due to significant resultsdue to significant results

34
LP267611LP267611
CARDS: Atorvastatin Significantly Reduces Risk of Major CV Events*CARDS: Atorvastatin Significantly Reduces Risk of Major CV Events*
*Acute CHD event, coronary revascularization, stroke.*Acute CHD event, coronary revascularization, stroke. Colhoun HM et al. Colhoun HM et al. LancetLancet. 2004;364:685-696.. 2004;364:685-696.
0
5
10
15
0 1 2 3 4 5 6
0
5
10
15
0 1 2 3 4 5 6
RRR=37% (95% CI: 17%-52%)RRR=37% (95% CI: 17%-52%)PP=0.001=0.001
Cu
mu
lati
ve in
cid
ence
C
um
ula
tive
inci
den
ce
of
even
ts (
% o
f p
atie
nts
) o
f ev
ents
(%
of
pat
ien
ts)
127 events127 events
83 events83 events
Time (years)Time (years)
Atorvastatin 10 mg (n=1428)Atorvastatin 10 mg (n=1428)
Placebo (n=1410)Placebo (n=1410)Trial stopped earlyTrial stopped early(median follow-up 3.9 years)(median follow-up 3.9 years)

35
LP267611LP267611
CARDS: Treatment Effect on the Primary End PointCARDS: Treatment Effect on the Primary End Point
Colhoun HM et al. Colhoun HM et al. LancetLancet. 2004;364:685-696.. 2004;364:685-696.
0.2 0.4 0.6 0.8 1.0 1.2 1.40.2 0.4 0.6 0.8 1.0 1.2 1.4
Event Event rate, n (%) Hazard ratio (95% CI) RRR
Placebo Atorvastatin
Event Event rate, n (%) Hazard ratio (95% CI) RRR
Placebo Atorvastatin
Primary end pointPrimary end point 127 (9.0%)127 (9.0%) 83 (5.8%)83 (5.8%) 37%37%
PP=0.001=0.001
Primary end pointPrimary end point 127 (9.0%)127 (9.0%) 83 (5.8%)83 (5.8%) 37%37%
PP=0.001=0.001
Acute coronary Acute coronary 77 (5.5%)77 (5.5%) 51 (3.6%)51 (3.6%) 36% 36%eventseventsAcute coronary Acute coronary 77 (5.5%)77 (5.5%) 51 (3.6%)51 (3.6%) 36% 36%eventsevents
Coronary Coronary 34 (2.4%)34 (2.4%) 24 (1.7%)24 (1.7%) 31%31%revascularizationrevascularizationCoronary Coronary 34 (2.4%)34 (2.4%) 24 (1.7%)24 (1.7%) 31%31%revascularizationrevascularization
StrokeStroke 39 (2.8%)39 (2.8%) 21 (1.5%)21 (1.5%) 48% 48%StrokeStroke 39 (2.8%)39 (2.8%) 21 (1.5%)21 (1.5%) 48% 48%
Placebo betterPlacebo betterAtorvastatin betterAtorvastatin better

36
LP267611LP267611
0
1
2
3
4
5
6
0 1 2 3 4 5 6
0
1
2
3
4
5
6
0 1 2 3 4 5 6
CARDS: Atorvastatin Significantly Reduces Risk of StrokeCARDS: Atorvastatin Significantly Reduces Risk of Stroke
Newman C et al. American Heart Association 78th Scientific Sessions, 2005.Newman C et al. American Heart Association 78th Scientific Sessions, 2005.
RRR= 48% (95% CI: 31%-89%)RRR= 48% (95% CI: 31%-89%)PP=0.016=0.016
Cu
mu
lati
ve in
cid
ence
C
um
ula
tive
inci
den
ce
of
even
ts (
% o
f p
atie
nts
) o
f ev
ents
(%
of
pat
ien
ts)
39 events39 events
21 events21 events
Time (years)Time (years)
Atorvastatin 10 mg (n=1428)Atorvastatin 10 mg (n=1428)
Placebo (n=1410)Placebo (n=1410)Trial stopped earlyTrial stopped early(median follow-up 3.9 years)(median follow-up 3.9 years)
Stroke was a component of the Stroke was a component of the primary endpoint, evaluated primary endpoint, evaluated individually as a secondary survival individually as a secondary survival analysisanalysis..

37
LP267611LP267611
CARDS: Treatment Effect on the Primary End Point By Median Baseline Lipid LevelCARDS: Treatment Effect on the Primary End Point By Median Baseline Lipid Level
Colhoun HM et al. Colhoun HM et al. LancetLancet. 2004;364:685-696.. 2004;364:685-696.
0.2 0.4 0.6 0.8 1.0 1.2 1.40.2 0.4 0.6 0.8 1.0 1.2 1.4
Lipid parameter Event rate, n (%) Hazard ratio (95% CI) RRR
PlaceboPlacebo AtorvastatinAtorvastatin
Placebo betterPlacebo betterAtorvastatin betterAtorvastatin better
LDL-C (mg/dL) 120120 66 (9.5%)66 (9.5%) 44 (6.1%)44 (6.1%) 38%38% <120 <120 61 (8.5%)61 (8.5%) 39 (5.6%)39 (5.6%) 37%37%
HDL-C (mg/dL) 54 54 62 (8.5%)62 (8.5%) 36 (5.2%)36 (5.2%) 41%41% <54 <54 65 (9.6%)65 (9.6%) 47 (6.4%)47 (6.4%) 34%34%
Triglycerides (mg/dL) 150150 67 (9.6%)67 (9.6%) 40 (5.5%)40 (5.5%) 44%44% <150 <150 60 (8.4%)60 (8.4%) 43 (6.1%)43 (6.1%) 29%29%
Total-C (mg/dL) 209209 71 (10.1%)71 (10.1%) 44 (6.2%)44 (6.2%) 41%41% <209 <209 56 (7.9%)56 (7.9%) 39 (5.5%)39 (5.5%) 33%33%
Tests of heterogeneity not significant Tests of heterogeneity not significant for each lipid parameter.for each lipid parameter.

38
LP267611LP267611
CARDS: ImplicationsCARDS: Implications
Established the efficacy and safety of atorvastatin 10 mgin reducing the risk of a first CVD event in patients with diabetes without high LDL-C
Authors questioned whether any patients with diabetes are at sufficiently low CVD risk for statin therapy to be withheld
Contributed to further update of ADA recommendations in 2005 In patients with diabetes aged >40 years without overt CVD, with
total cholesterol 135 mg/dL (3.5 mmol/L), statin therapy recommended to achieve LDL-C reduction of 30-40% regardless of baseline LDL-C
Primary goal is an LDL-C of <100 mg/dL (2.6 mmol/L)
Patients with diabetes and overt CVD should be treated with a statin to achieve an LDL-C goal of <70 mg/dL (1.8 mmol/L)
Established the efficacy and safety of atorvastatin 10 mgin reducing the risk of a first CVD event in patients with diabetes without high LDL-C
Authors questioned whether any patients with diabetes are at sufficiently low CVD risk for statin therapy to be withheld
Contributed to further update of ADA recommendations in 2005 In patients with diabetes aged >40 years without overt CVD, with
total cholesterol 135 mg/dL (3.5 mmol/L), statin therapy recommended to achieve LDL-C reduction of 30-40% regardless of baseline LDL-C
Primary goal is an LDL-C of <100 mg/dL (2.6 mmol/L)
Patients with diabetes and overt CVD should be treated with a statin to achieve an LDL-C goal of <70 mg/dL (1.8 mmol/L)

Atorvastatin study in the prevention of CV endpoints in subjects with DM: the ASPEN study
Knopp RH et al, Diabetes Care 2006; 29: 1478-85
Objective
To evaluate atorvastatin 10 mg vs placebo
in pts with DM and LDL cholesterol levels
below the current guidelines cut-offs

Atorvastatin study in the prevention of CV endpoints in subjects with DM: the ASPEN study.
Knopp RH et al. Diabetes Care 2006; 29: 1478-85

Cosa consigliano le LLGGnel 2008

Nel pz a basso rischio (LDL<100, TG<150, HDL>50) controlli ogni 2 aa
Nel pz con LDL > 100• CVD • > 40 aa con un fattore di rischio (retinopatia,nefropatia, ipertensione arteriosa, sindrome metabolica)
aggiungere una statina con obiettivo LDL<100(eventualmente <70 se il profilo di rischio è molto elevato)
ADA 2008-Diabetes Care 2008; 31: S5-S11

* Non approvata per uso clinico
Atorva Simva Lova Prava Fluva Rosuva LDL-C
-- 10 20 20 40 -- 22-28
10 20 40 40 80 -- 30-35
20 40 80 -- -- 10 37-43
40 80 -- -- -- 20 42-50
80 160* -- -- -- 40 50-60
Dose (mg) farmaco Riduzione%
Efficacia comparata delle diverse statine
Roberts WC. Am J Cardiol. 1997;80:106-107Roberts WC. Am J Cardiol. 1997;80:106-107Stein E et al. J Cardiovasc Pharmacol Therapeut. 1997;2:7-16Stein E et al. J Cardiovasc Pharmacol Therapeut. 1997;2:7-16Olsson A. Cardiovasc Drug Rev 2002;20:303–328Olsson A. Cardiovasc Drug Rev 2002;20:303–328

Perché l’utilizzo delle statinenei diabetici è ancora
così basso?

Barriere all’aderenza all’utilizzo delle statine nel diabetico
Efficacia e sicurezza dell’alto dosaggio
Anziani
Insufficienza renale
Donne

Uno studio randomizzato con statine
ad alto dosaggionei diabetici:
lo studio TNT-diabete

47
LP267611LP267611
Patient population:Patient population: Age: 35-75 yearsAge: 35-75 years CHDCHD LDL-C: 130-250 mg/dL (3.4-6.5 mmol/L)LDL-C: 130-250 mg/dL (3.4-6.5 mmol/L) Triglycerides: Triglycerides: 600 mg/dL (600 mg/dL (6.8 6.8
mmol/L)mmol/L)
Primary end point:Primary end point: Time to occurrence of a major CV event:Time to occurrence of a major CV event:
– CHD deathCHD death– Nonfatal, nonNonfatal, non––procedure-related MIprocedure-related MI– Resuscitated cardiac arrestResuscitated cardiac arrest– Fatal or nonfatal strokeFatal or nonfatal stroke
Atorvastatin 10 mg
Open-label run-inOpen-label run-in
8 weeks8 weeks1-8 weeks1-8 weeks
Screening and wash-out
Screening and wash-out
Atorvastatin 10 mgLDL-C target: 100 mg/dL (2.6 mmol/L)
Median follow-up = 4.9 yearsMedian follow-up = 4.9 years
Atorvastatin 80 mgLDL-C target: 75 mg/dL (1.9 mmol/L)
Double-blind periodn=1501
LDL-C: <130 mg/dL (<3.4 mmol/L)
Double-blind periodn=1501
LDL-C: <130 mg/dL (<3.4 mmol/L)
n=748n=748
n=753n=753
BaselineBaseline
TNT Study Design: Patients With DiabetesTNT Study Design: Patients With Diabetes
Shepherd J et al. Shepherd J et al. Diabetes CareDiabetes Care. 2006;29:1220-1226.. 2006;29:1220-1226.

48
LP267611LP267611
FinalFinalScreenScreen 00 33 1212 2424 3636 4848 6060
BaselineBaseline
TNT: Changes in LDL-C By Treatment Group in Patients With DiabetesTNT: Changes in LDL-C By Treatment Group in Patients With Diabetes
0
20
40
60
80
100
120
140
160
180
Study visit (months)
Mea
n L
DL
-C (
mg
/dL
)
Atorvastatin 10 mg (n=753)
Atorvastatin 80 mg (n=748)
0
20
40
60
80
100
120
140
160
180
Study visit (months)
Mea
n L
DL
-C (
mg
/dL
)
Atorvastatin 10 mg (n=753)
Atorvastatin 80 mg (n=748)
Final LDL-C = 77.0 mg/dL (2.0 mmol/L) Final LDL-C = 77.0 mg/dL (2.0 mmol/L)
Final LDL-C = 98.6 mg/dL (2.5 mmol/L)Final LDL-C = 98.6 mg/dL (2.5 mmol/L)
Shepherd J et al. Shepherd J et al. Diabetes CareDiabetes Care. 2006;29:1220-1226.. 2006;29:1220-1226.

49
LP267611LP267611
TNT: Time to First Major Cardiovascular Event* in Patients With DiabetesTNT: Time to First Major Cardiovascular Event* in Patients With Diabetes
*CHD death, nonfatal non*CHD death, nonfatal non––procedure-related MI, procedure-related MI, resuscitated cardiac arrest, fatal or nonfatal stroke. resuscitated cardiac arrest, fatal or nonfatal stroke.
0
5
10
15
20
0 1 2 3 4 5 6
0
5
10
15
20
0 1 2 3 4 5 6
RRR=25% (95% CI: 3%-42%)RRR=25% (95% CI: 3%-42%)PP=0.026=0.026
Cu
mu
lati
ve in
cid
ence
C
um
ula
tive
inci
den
ce
of
even
ts (
% o
f p
atie
nts
)o
f ev
ents
(%
of
pat
ien
ts)
135 events135 events
103 events103 events
Time (years)Time (years)
Atorvastatin 10 mg (n=753)Atorvastatin 10 mg (n=753)
Atorvastatin 80 mg (n=748)Atorvastatin 80 mg (n=748)
Shepherd J et al. Shepherd J et al. Diabetes CareDiabetes Care. 2006;29:1220-1226.. 2006;29:1220-1226.

50
LP267611LP267611
Hazard Ratios in Patients With and Without Diabetes: Secondary Efficacy OutcomesHazard Ratios in Patients With and Without Diabetes: Secondary Efficacy Outcomes
Major CV event 17.9% 13.8%9.7%
7.8%
Major CV event 17.9% 13.8%9.7%
7.8%Any CV event 44.1% 39.8%31.6%
26.1%
Any CV event 44.1% 39.8%31.6%
26.1%Major coronary 12.9% 10.6%7.5%
6.0%
Major coronary 12.9% 10.6%7.5%
6.0%Any coronary 32.0% 29.3%25.5%
20.2%
Any coronary 32.0% 29.3%25.5%
20.2%Cerebrovascular 10.0% 7.0%4.2%
3.4%
Cerebrovascular 10.0% 7.0%4.2%
3.4%CHF with hosp. 8.2% 7.2%2.4%
1.6%
CHF with hosp. 8.2% 7.2%2.4%
1.6%PAD 8.9% 9.1%5.1%
4.9%
PAD 8.9% 9.1%5.1%
4.9%All-cause mortality 9.8% 10.8%4.9%
4.8%
All-cause mortality 9.8% 10.8%4.9%
4.8%
Atorvastatin 80 mg betterAtorvastatin 80 mg better Atorvastatin 10 mg betterAtorvastatin 10 mg better
0.4 0.6 0.8 1.0 1.2 1.4 1.60.4 0.6 0.8 1.0 1.2 1.4 1.6
Event rate (diabetes) Event rate (no diabetes)
10 mg 80 mg 10 mg 80 mg
Event rate (diabetes) Event rate (no diabetes)
10 mg 80 mg 10 mg 80 mg
Shepherd J et al. Shepherd J et al. Diabetes CareDiabetes Care. 2006;29:1220-1226.. 2006;29:1220-1226.

51
LP267611LP267611
TNT: SummaryTNT: Summary
The TNT study confirmed findings from prior studies that incidence of CV events is higher in patients with diabetes than in those without diabetes
25% reduction in risk of major CV events with atorvastatin 80 mg vs atorvastatin 10 mg (P=0.026) in patients with stable CHD and diabetes
Lower event rates observed in TNT than in other secondary prevention regimens in patients with CHD and diabetes
The TNT study strengthens the evidence for the recent recommendation of an LDL-C <70 mg/dL (1.8 mmol/L) as a therapeutic option in diabetic patients with CVD
The TNT study confirmed findings from prior studies that incidence of CV events is higher in patients with diabetes than in those without diabetes
25% reduction in risk of major CV events with atorvastatin 80 mg vs atorvastatin 10 mg (P=0.026) in patients with stable CHD and diabetes
Lower event rates observed in TNT than in other secondary prevention regimens in patients with CHD and diabetes
The TNT study strengthens the evidence for the recent recommendation of an LDL-C <70 mg/dL (1.8 mmol/L) as a therapeutic option in diabetic patients with CVD

Barriere all’aderenza all’utilizzo delle statine nel diabetico
Efficacia e sicurezza dell’alto dosaggio
Anziani
Insufficienza renale
Donne

Statins for secondary prevention in elderly patients (> 65 yrs)
Afilalo et al, JACC 2008; 51: 37-45
All cause mortality
DM in 5-29%of pts

Statins for secondary prevention in elderly patients (>65 yrs)
Afilalo et al, JACC 2008; 51: 37-45
Coronary artery disease mortality

Risk difference by FDA-approved statins
Kashani A et al, Circulation 2006;114:2788-2797

Lowest Success Rates in Patients at Highest Risk
Pearson TA, et al. Arch Intern Med. 2000;160:459-467.Pearson TA, et al. Arch Intern Med. 2000;160:459-467.
Low-risk Low-risk (n=861)(n=861)
CHD CHD (n=1352)(n=1352)
High-risk High-risk (n=1924)(n=1924)
Overall Overall (n=4137)(n=4137)
0
20
40
60
80
100
Patie
nts
Ach
ievi
ng L
DL-
C
Patie
nts
Ach
ievi
ng L
DL-
C
Goa
l (%
)G
oal (
%)
The high-risk paradox

Barriere all’aderenza all’utilizzo delle statine nel diabetico
Efficacia e sicurezza dell’alto dosaggio
Anziani
Insufficienza renale
Donne

Sheperd J et al. JACC 2008; 51: 1448-54DM in 18%
of pts

Statin therapy and mortality in elderly and very elderly patients (> 80 yrs)
Allen Maycock CA et al, JACC 2002; 40: 1777-85
statins
not usingstatins
statin prescription
28% 21% 20% DM in 5-18%of pts

Time to first CV event by treatment in pts with kidney disease (eGFR <60)
Sheperd J et al. JACC 2008; 51: 1448-54

An assessment of statin safety by nephrologists
Kasiske BL et al. Am J Cardiol 2006;97:82C-85C

Barriere all’aderenza all’utilizzo delle statine nel diabetico
Efficacia e sicurezza dell’alto dosaggio
Anziani
Insufficienza renale
Donne

63
LP267611LP267611
At same lipid levels, women with cardiovascular disease have lower mortality risk compared to men; women with diabetes have same or greater mortality risk compared to men
At same lipid levels, women with cardiovascular disease have lower mortality risk compared to men; women with diabetes have same or greater mortality risk compared to men

64
LP267611LP267611
Studies on diabetes and womenStudies on diabetes and women
Patients of physicians participating in the ADA Provider Recognition Program (n=7364)
Patients with diabetes at Kaiser Permanente Georgia (n=14,671)
Patients participating in the UCI Diabetes Coached Care Program (n=272)
Patients of physicians participating in the ADA Provider Recognition Program (n=7364)
Patients with diabetes at Kaiser Permanente Georgia (n=14,671)
Patients participating in the UCI Diabetes Coached Care Program (n=272)

65
LP267611LP267611
Gender differences in overall quality of diabetes care: PRPGender differences in overall quality of diabetes care: PRP
Quality Measure Males Females P-value
Annual HbA1c 97.7 98.4 NS
Annual urine protein 49.7 48.6 NS
Annual eye exam 68.5 69.0 NS
Annual foot exam 94.3 94.2 NS
HbA1c < 8 mg/dl 65.8 66.7 NS
BP <130/80 41.9 41.6 NS

66
LP267611LP267611
Gender differences in overall quality of diabetes care: KPGGender differences in overall quality of diabetes care: KPG
Quality Measure Males Females P-value
Annual HbA1c 67.3 62.7 <.001
Annual blood pressure 71.1 64.8 <.01
HbA1c < 8 mg/dl 53.4 57.3 <.001
BP <130/80 35.0 35.4 NS

67
LP267611LP267611
Gender differences in overall quality of diabetes care: UCIGender differences in overall quality of diabetes care: UCI
Quality Measure Males Females P-value
Annual HbA1c 100 100 NS
Annual foot exam 90.2 98.1 <.01
HbA1c < 8 mg/dl 89.2 92.5 <.001
BP <130/80 35.0 35.4 NS

68
LP267611LP267611
Gender Differences in Lipid Monitoring and ControlGender Differences in Lipid Monitoring and Control
Quality Measure Sample Males Females P-value
Monitoring lipids PRP 86.8 84.3 NS
LDL < 100mg/dl 38.1 31.2 <.001
Monitoring lipids KPG 67.3 65.3 NS
LDL < 100mg/dl 34.4 24.7 <.001
Monitoring lipids UCI 100 100 NS
LDL < 100mg/dl 61.7 51.8 <.001

69
LP267611LP267611
With no differences in the overall quality of diabetes care, nor in monitoring of lipids, women have poorer lipid control
Women with diabetes and poor lipid control significantly less likely to be on statins (HR 0.77, p< 0.001)
With no differences in the overall quality of diabetes care, nor in monitoring of lipids, women have poorer lipid control
Women with diabetes and poor lipid control significantly less likely to be on statins (HR 0.77, p< 0.001)

Come migliorare l’aderenza alla terapia farmacologica
(e alle raccomandazioni sullo stile di vita)nel paziente diabetico e dislipidemico

Long-term adherence with cardiovascular regimensBasal prescription and discontinuation (gray bar) after 1 yr
n= 1326 CAD pts, Duke University
Kulkarni sp et al. Am Heart J 2006;151: 185-91

Cumulative probability to returning to treatment with statins
Brookhart MA et al. Arch Intern Med 2007; 167:847-52

73
LP267611LP267611
Terapia con statine nel diabetico:
come garantire l’aderenza
Terapia con statine nel diabetico:
come garantire l’aderenza
- comunicarecomunicare- responsabilizzareresponsabilizzare- gratificaregratificare

74
LP267611LP267611
Helping pts with DM make treatment decisionHelping pts with DM make treatment decision
Weymiller AJ et al, Arch intern Med 2007; 167: 1076-82Weymiller AJ et al, Arch intern Med 2007; 167: 1076-82

75
LP267611LP267611
ConclusionsConclusions
Early clinical trials including have shown that statins benefit CHD patients with type 2 diabetes
Pre-specified analyses of patients with diabetes with and without CHD (ASCOT-LLA, HPS, LIPID) have shown significant benefits of statins in reducing cardiovascular events including stroke
CARDS—the first prospective statin trial in patients with diabetes—was terminated ~2 years earlier than anticipated due to a highly significant reduction in major cardiovascular events compared with placebo
High-dose statin therapy in patients with CHD and diabetes (TNT) has shown a significant reduction in cardiovascular events compared with lower-dose statin therapy
These trials have contributed to changes in guidelines focusing on intensive LDL-C management in patients with diabetes
Early clinical trials including have shown that statins benefit CHD patients with type 2 diabetes
Pre-specified analyses of patients with diabetes with and without CHD (ASCOT-LLA, HPS, LIPID) have shown significant benefits of statins in reducing cardiovascular events including stroke
CARDS—the first prospective statin trial in patients with diabetes—was terminated ~2 years earlier than anticipated due to a highly significant reduction in major cardiovascular events compared with placebo
High-dose statin therapy in patients with CHD and diabetes (TNT) has shown a significant reduction in cardiovascular events compared with lower-dose statin therapy
These trials have contributed to changes in guidelines focusing on intensive LDL-C management in patients with diabetes

76
LP267611LP267611
Diapositive aggiuntive Diapositive aggiuntive

77
LP267611LP267611
Secondary Prevention of CVD With Statins in Patients With Diabetes
Secondary Prevention of CVD With Statins in Patients With Diabetes

78
LP267611LP267611
Primary Prevention of CVD With Statins in Patients With DiabetesPrimary Prevention of CVD With Statins in Patients With Diabetes

79
LP267611LP267611

80
LP267611LP267611
ASCOT-LLA: Primary Prevention in Patients at Modest Risk of CHD ASCOT-LLA: Primary Prevention in Patients at Modest Risk of CHD
Highlighted boxes indicate diabetes patients enrolled in lipid-lowering arm.Highlighted boxes indicate diabetes patients enrolled in lipid-lowering arm.
-blocker ± diuretic-blocker ± diuretic CCB ± ACE inhibitorCCB ± ACE inhibitor
TC >250 mg/dLTC >250 mg/dL (>6.5 mmol/L) (>6.5 mmol/L)
2532 TC 250 mg/dL(6.5 mmol/L)
TC >250 mg/dLTC >250 mg/dL (>6.5 mmol/L) (>6.5 mmol/L)
Open lipid loweringOpen lipid lowering1258
Atorvastatin 10 mg1274
PlaceboOpen lipid loweringOpen lipid lowering
19,342 patients19,342 patients
RandomizedRandomized
RandomizedRandomized
Primary end point: Composite of fatal CHD and nonfatal MI Primary end point: Composite of fatal CHD and nonfatal MI
Adapted from Sever PS et alAdapted from Sever PS et al. J Hypertens. . J Hypertens. 2001;19:1139-1147.2001;19:1139-1147.

81
LP267611LP267611
ASCOT-LLA Post hoc Analysis: Total CV Events and Procedures in Patients With DiabetesASCOT-LLA Post hoc Analysis: Total CV Events and Procedures in Patients With Diabetes
Sever PS et al. Sever PS et al. Diabetes CareDiabetes Care. 2005;28:1151-1157.. 2005;28:1151-1157.
0
5
10
15
0 1 2 3 4 5 6
0
5
10
15
0 1 2 3 4 5 6
RRR=23% RRR=23% PP=0.036=0.036
151 events151 events
116 events116 events
Trial stopped earlyTrial stopped early(median follow-up 3.3 years) (median follow-up 3.3 years)
Cu
mu
lati
ve in
cid
ence
C
um
ula
tive
inci
den
ce
of
even
ts (
% o
f p
atie
nts
) o
f ev
ents
(%
of
pat
ien
ts)
Time (years)Time (years)
Atorvastatin 10 mgAtorvastatin 10 mg
PlaceboPlacebo

82
LP267611LP267611
ASCOT-LLA: SummaryASCOT-LLA: Summary
In hypertensive patients with diabetes but no history of CHD, relative risk reductions in all cardiovascular events and procedures with atorvastatin were similar to those in the nondiabetic subgroup, and were evident early in the trial
Small numbers of events in the individual components of the composite end point, resulting in part from early stopping of the trial, reduced the power to test significant reductions in CHD and stroke There was no significant heterogeneity among subgroups
ASCOT-LLA provides further support for the findings in CARDS concerning the benefits of atorvastatin 10 mg in patients with diabetes and without CHD
In hypertensive patients with diabetes but no history of CHD, relative risk reductions in all cardiovascular events and procedures with atorvastatin were similar to those in the nondiabetic subgroup, and were evident early in the trial
Small numbers of events in the individual components of the composite end point, resulting in part from early stopping of the trial, reduced the power to test significant reductions in CHD and stroke There was no significant heterogeneity among subgroups
ASCOT-LLA provides further support for the findings in CARDS concerning the benefits of atorvastatin 10 mg in patients with diabetes and without CHD

83
LP267611LP267611
Diabetes + vascular disease
Coronary heart disease 779 (30.3) 918 (36.2) 18% (P<0.0001)Other vascular disease 127 (15.8) 156 (20.7) 22% (P=0.02)Subtotal 906 (26.8) 1074 (32.6) 19%
Diabetes + vascular disease
Coronary heart disease 779 (30.3) 918 (36.2) 18% (P<0.0001)Other vascular disease 127 (15.8) 156 (20.7) 22% (P=0.02)Subtotal 906 (26.8) 1074 (32.6) 19%
Cholesterol Treatment Trialists Collaboration: Major Vascular Events in Diabetes PatientsCholesterol Treatment Trialists Collaboration: Major Vascular Events in Diabetes Patients
Baseline vascular disease/ Event rate, n (%) Hazard ratio (CI*) Relative riskhypertension Statin Control reductionBaseline vascular disease/ Event rate, n (%) Hazard ratio (CI*) Relative riskhypertension Statin Control reduction
Diabetes, no vascular disease
Hypertension 422 (10.0) 504 (12.0) 25% (P=0.0003)No hypertension 137 (7.7) 204 (11.2) 30% (P<0.0001)Subtotal 559 (9.3) 708 (11.8) 27%
Diabetes, no vascular disease
Hypertension 422 (10.0) 504 (12.0) 25% (P=0.0003)No hypertension 137 (7.7) 204 (11.2) 30% (P<0.0001)Subtotal 559 (9.3) 708 (11.8) 27%
All diabetes patients 1465 (15.6) 1782 (19.2) 21%All diabetes patients 1465 (15.6) 1782 (19.2) 21%
Placebo betterPlacebo betterStatin betterStatin better
0.5 1.0 1.50.5 1.0 1.5
N=18,686 patients with diabetesN=18,686 patients with diabetes
** 95% CI95% CI 99% CI99% CI
Cholesterol Treatment Trialists. Presentation at the American Diabetes Association 66Cholesterol Treatment Trialists. Presentation at the American Diabetes Association 66 thth Scientific Sessions, 2006. Scientific Sessions, 2006.

ESC on diabetes and pre-diabetes EHJ 2007; 28:88-136In prevenzione secondaria nessuno studio ad hoc
>5000 pts in analisi post-hoc 4S 483 pts DM sim riduce 42% major coro events
Haffner Arch Int Med 99;159:2661-7 HPS 3050 pts DM sim riduce 18% major coro, stroke, rev
CARE 586 pts DM prava riduce 25% major coro events LIPID 782 pts DM prava riduce 19% major coro events e rev LIPS 202 pts DM fluva riduce 47% major coro events e rev
GREACE 313 pts DM atorva riduce 58% major e stroke e revNell’alto dosaggio i vantaggi osservati enl PROVE IT e nel TNT sono stati
simili anche per il pt con DM

85
LP267611LP267611
Total CV events and procedures
Diabetes 23% 0.82
No diabetes 20%
Subtotal: 21% (P<0.001)
Total CV events and procedures
Diabetes 23% 0.82
No diabetes 20%
Subtotal: 21% (P<0.001)
ASCOT-LLA: Lack of Heterogeneity of Effect in Patients With or Without DiabetesASCOT-LLA: Lack of Heterogeneity of Effect in Patients With or Without Diabetes
Hazard ratio (95% CI) Relative risk P value forreduction heterogeneity
Hazard ratio (95% CI) Relative risk P value forreduction heterogeneity
Sever PS et al. Sever PS et al. Diabetes CareDiabetes Care. 2005;28:1151-. 2005;28:1151-1157.1157.
Nonfatal MI + fatal CHD
Diabetes 16% 0.14
No diabetes 44%
Subtotal: 36% (P<0.001)
Nonfatal MI + fatal CHD
Diabetes 16% 0.14
No diabetes 44%
Subtotal: 36% (P<0.001)
Fatal and nonfatal stroke
Diabetes 33% 0.66
No diabetes 24%
Subtotal: 27% (P<0.024)
Fatal and nonfatal stroke
Diabetes 33% 0.66
No diabetes 24%
Subtotal: 27% (P<0.024)
Placebo betterPlacebo betterAtorvastatin betterAtorvastatin better
0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.60.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6

86
LP267611LP267611
Lipid Treatment Guidelines: Which Diabetes Patients Should Be Treated?Lipid Treatment Guidelines: Which Diabetes Patients Should Be Treated?
Guidelines Lipid targets in diabetes patients Treatment recommendations
NCEP ATP IIINCEP ATP III11 LDL-C <100 mg/dL (2.6 mmol/L)LDL-C <100 mg/dL (2.6 mmol/L)
Optional LDL-C goal: <70 mg/dL Optional LDL-C goal: <70 mg/dL (1.8 mmol/L)(1.8 mmol/L)
Intensity of therapy should be sufficient to Intensity of therapy should be sufficient to achieve a 30-40% reduction in LDL-Cachieve a 30-40% reduction in LDL-C
ADAADA22 Patients without CVD LDL-CLDL-C <100 mg/dL (2.6 mmol/L) <100 mg/dL (2.6 mmol/L)
Age >40 years: Statin therapy to achieve Age >40 years: Statin therapy to achieve LDL-C reduction of 30-40%, irrespective of LDL-C reduction of 30-40%, irrespective of baseline LDL-Cbaseline LDL-C
Patients with CVDOptional Optional LDL-CLDL-C goal: <70 mg/dL goal: <70 mg/dL (1.8 mmol/L)(1.8 mmol/L)
All patients should be treated with a statin to All patients should be treated with a statin to achieve LDL-C reduction of 30-40%achieve LDL-C reduction of 30-40%
Joint European Joint European SocietiesSocieties33
TC <4.5 mmol/L (175 mg/dL)TC <4.5 mmol/L (175 mg/dL)
LDL-C <2.5 mmol/L (100 mg/dL)LDL-C <2.5 mmol/L (100 mg/dL)
Joint British Joint British SocietiesSocieties44
TC <4.0 mmol/L (155 mg/dL)TC <4.0 mmol/L (155 mg/dL)
LDL-C <2.0 mmol/L (77 mg/dL)LDL-C <2.0 mmol/L (77 mg/dL)
Treat to TC and LDL-C targets (or a 25% Treat to TC and LDL-C targets (or a 25% and a 30% reduction, respectively), using and a 30% reduction, respectively), using statins at doses whose efficacy and safety statins at doses whose efficacy and safety have been shown in trialshave been shown in trials
1.1. Grundy SM et al. Grundy SM et al. CirculationCirculation. 2004;110:227-39.. 2004;110:227-39.2.2. American Diabetes Association. American Diabetes Association. Diabetes CareDiabetes Care. 2006;29(suppl 1):S4-S42.. 2006;29(suppl 1):S4-S42.3.3. De Backer G et al. De Backer G et al. Eur J Cardiovasc Prevent RehabilEur J Cardiovasc Prevent Rehabil. 2003;10(suppl 1):S1-S78.. 2003;10(suppl 1):S1-S78.4.4. British Cardiac Society et al. British Cardiac Society et al. HeartHeart. 2005;91(suppl v):v1-v52.. 2005;91(suppl v):v1-v52.