tokoliz güncel durum - tmftp.orgtmftp.org/webkontrol/uploads/files/ZEKİ ŞAHİNOĞLU_BURSA...
72
tokoliz güncel durum Doç Dr Zeki Şahinoğlu Perinatolojide Güncel Konular Türkiye Maternal Fetal Tıp ve Perinatoloji Derneği - Uludağ Üniversitesi 13 Mart 2014 FETUS prenatal
Transcript of tokoliz güncel durum - tmftp.orgtmftp.org/webkontrol/uploads/files/ZEKİ ŞAHİNOĞLU_BURSA...

tokoliz güncel durum
Doç Dr Zeki Şahinoğlu
Perinatolojide Güncel Konular
Türkiye Maternal Fetal Tıp ve Perinatoloji Derneği - Uludağ Üniversitesi
13 Mart 2014
FETUS
prenatal
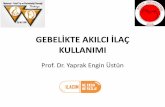
Tanım: > 24. gb hf < 37.
PTD: %70-80 spontan
Spontan PD
P-PROM
Norwitz ER, 2011
PTD: %20- 30 Maternal - fetal
Preeklampsi-eklampsi
IUGR - Fetal distress
Çoğul gebelikler
Koryoamnionitis
Ablasyo plasenta
P. Previa, kanama
Maternal sistemik hastalık
Servikal yetersizlik / Uterin anomali
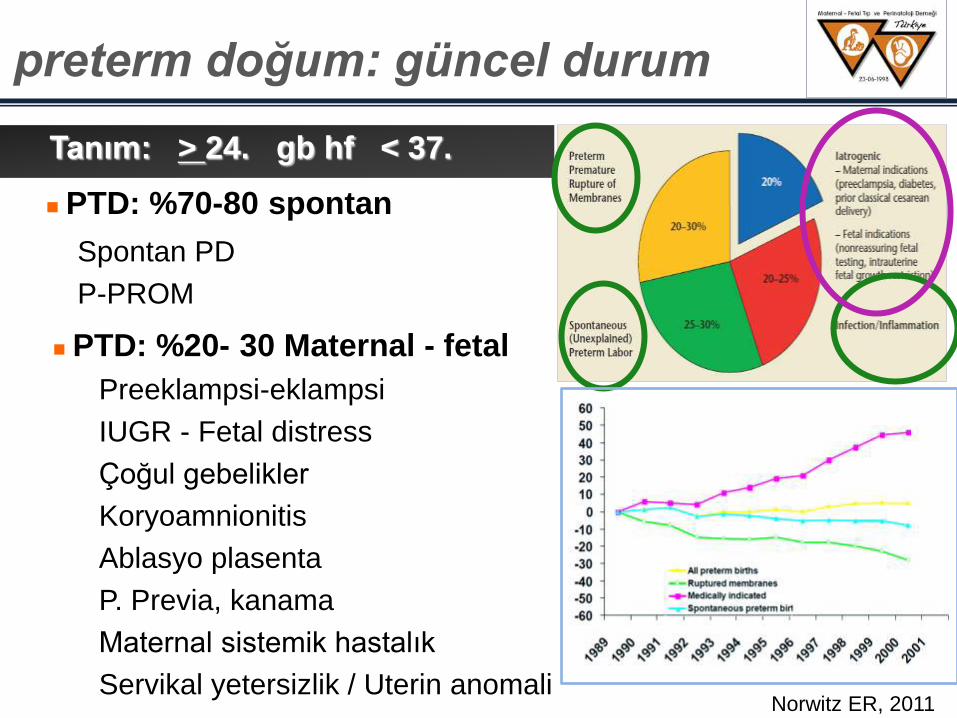
preterm doğum: güncel durum
preterm doğum: güncel durum
Tek (%) Ġkiz (%) Üçüz (%)
< 32 hf 1.6 11.8 36.7
< 37 hf 10.4 57.4 92.4
< 1500g 1.1 10.2 34.8
< 2500g 6.1 54.9 94.0

preterm doğum: güncel durum
% 10 – 18
15 MĠLYON PRETERM DOĞUM / YIL
1.1 milyon bebek ölümü
> % 10 uzun dönem sekel – mağduriyet
• % 50 nörolojik sekel
ilk 1 hafta bebek ölümleri: 1. sırada
< 5 yaş çocuk ölümü (pnömoni sonrası) 2. sırada
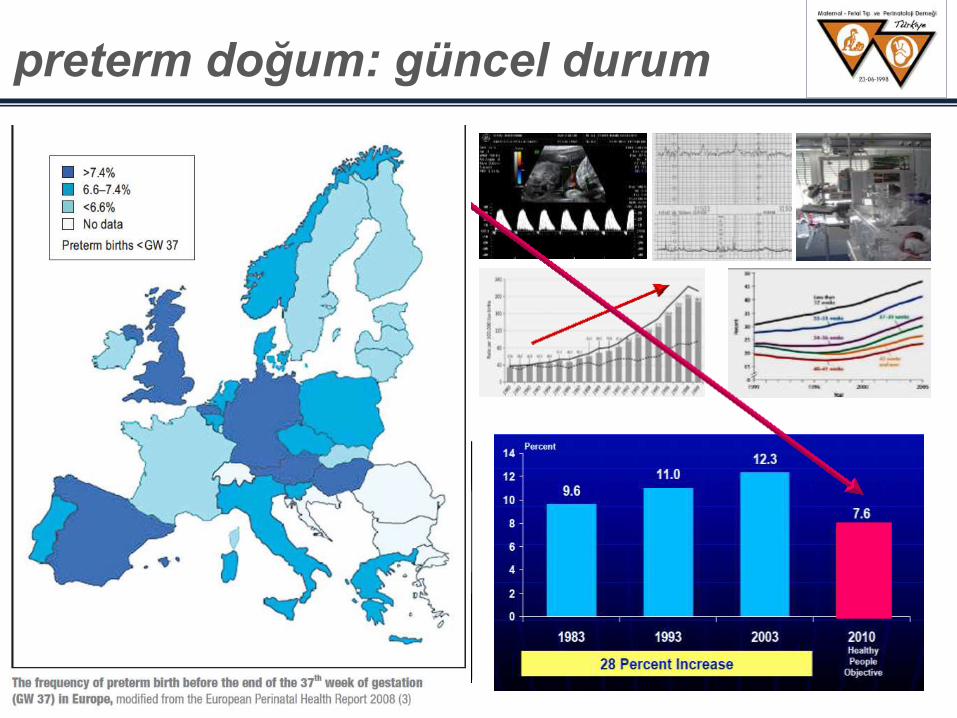
Fuchs K, Clin Perinatol, 2006
% 85
RDS
BPD
NEC
İVK
HİPOTERMİ
HİPOGLİSEMİ
ENFEKSİYON
ROP
■ prematürite komplik
■ Konjenital malform
■ SIDS
■ injury
■ premat. dışı enf
■ diğer
< 30 hf
< 30. HAFTA
preterm doğum: güncel durum
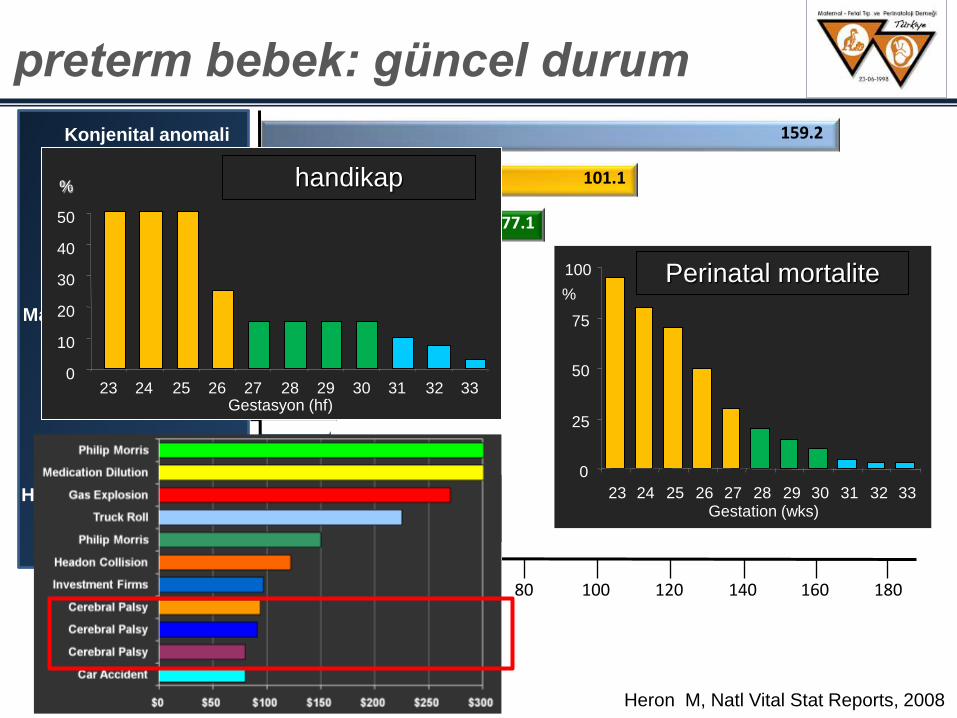
0
25
50
75
100
23 24 25 26 27 28 29 30 31 32 33
%
Ölüm oranı
Gestation (wks)
Perinatal mortalite
Heron M, Natl Vital Stat Reports, 2008
preterm bebek: güncel durum
10.8
11.6
19.7
20.0
24.7
32.1
33.5
77.1
101.1
159.2
0 20 40 60 80 100 120 140 160 180
Pnömoni/Influenza
Hipoksi/Doğum Asfiksi
Kazalar
Enfeksiyon
Plasenta, kord komp.
Maternal gebelik komp.
RDS
Ani bebek ölümü
PRETERM / DDA
Konjenital anomali
Beyin
hasarı
0
10
20
30
40
50
23 24 25 26 27 28 29 30 31 32 33 Gestasyon (hf)
handikap %
Creasy & Resnik, 2009
Kontraksiyon inhibisyonu: doğumu en az 48 saat ertelemek
Kortikosteroid uygulama fırsatını yaratmak
YDYB içeren merkeze transfer etmek
preterm eylem
tokoliz
fetal travma preterm eylem
Kontraksiyonların durdurulması
Fetal travmanın minimalize edilmesi
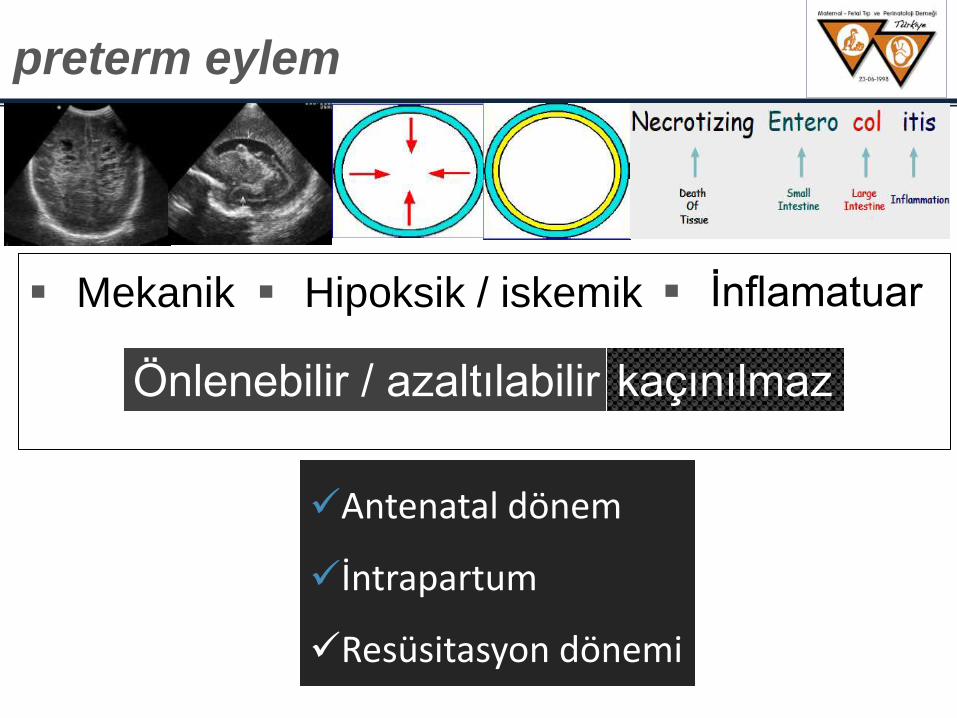
Önlenebilir / azaltılabilir
Mekanik
Antenatal dönem
İntrapartum
Resüsitasyon dönemi
kaçınılmaz
Hipoksik / iskemik
preterm eylem
Ġnflamatuar
Green NS, AJOG 2005 ;193:626-35.
PATHWAYS
FA
CT
OR
S
External Environment
Immune Status
Nutrition
Behaviors
Medical Conditions
Medical Interventions
Psychosocial
Oth
ers
: Ho
rmo
nes?
To
xin
s?
Ble
edin
g / T
hro
mb
oph
ilias
Ab
norm
al U
terin
e D
iste
ntio
n
Mate
rnal / F
eta
l Stre
ss
Infla
mm
atio
n / In
fectio
n
PRETERM BIRTH
OUTCOMES
Preterm Labor / pPROM
Racial / Ethnic Disparities
Genetics / Family History
Fetal Gro
wth
İnfla
ma
syo
n / e
nf.
> % 75
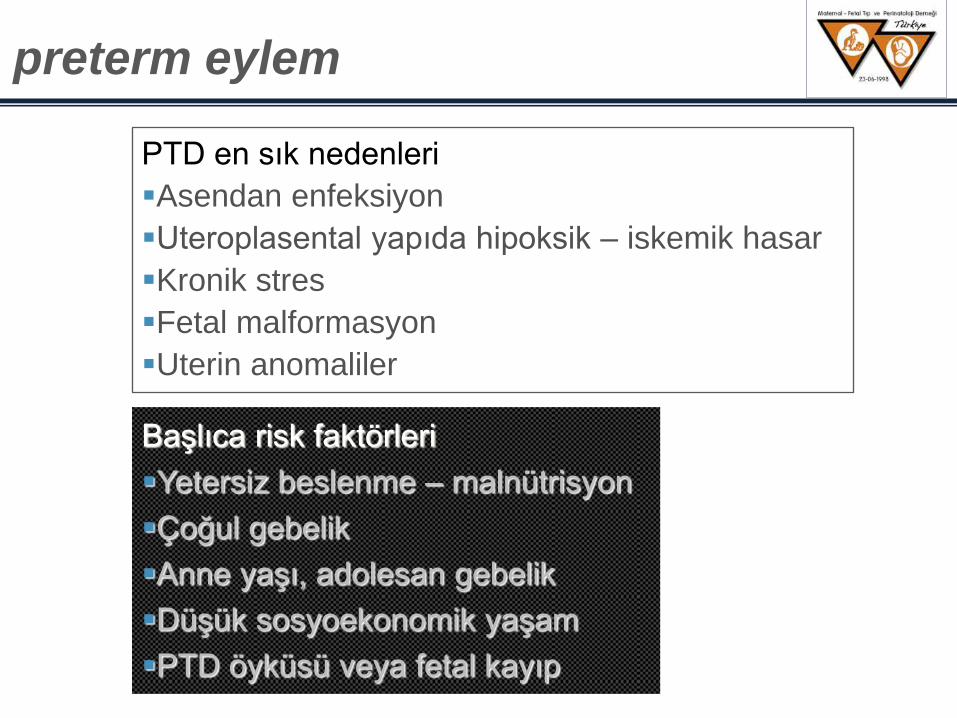
preterm eylem
PTD en sık nedenleri
Asendan enfeksiyon
Uteroplasental yapıda hipoksik – iskemik hasar
Kronik stres
Fetal malformasyon
Uterin anomaliler
Başlıca risk faktörleri
Yetersiz beslenme – malnütrisyon
Çoğul gebelik
Anne yaşı, adolesan gebelik
Düşük sosyoekonomik yaşam
PTD öyküsü veya fetal kayıp
Tokoliz 1960 -
Bibl Gynaecol. 1966;42:198-216. Tocolysis. Mosler KH. PMID: 6007135
Serum amyloid A upsurge precedes standard biomarkers of hepatotoxicity in ritodrine-injected mice. Tsuchiya H, Sato J, Tsuda H, Fujiwara Y, Yamada T, Fujimura A, Koshimizu TA. Toxicology. 2013 Mar 8;305:79-88. doi: 10.1016/j.tox.2013.01.012. Epub 2013 Jan 28. PMID: 23370008
tocolytic search
Results: 1 to 20 of 60598 Page of 3030
2-adren. res. agonisti
nitrik oksit donörleri
MgSO4
Ca++ kanal blokerleri
oksitosin res. antagonisti
PG sentetaz inhibitörleri
Tokolitik ilaçlar
1. Kontraksiyon sağlayan proteinlere etkili intracellular
messanger üzerinden etkinlik gösteren ilaçlar
2-adren. reseptör agonisti
nitrik oksit donörleri
MgSO4
Ca++ kanal blokerleri
2. Myometrial endojen stimulanların (oksitosin, PG)
etkinliğini bloke eden ilaçlar
oksitosin reseptör antagonistleri (atosiban)
PG sentetaz inhibitörleri
2-agonist cAMP
myosin light kinase aktiv.
myosin fosforilizasyonu
MgSO4 intracellular Ca++ transferi
Ca++ kan.blokeri myosin light kinase aktiv.
myosin fosforilizasyonu
NO donör cGMP
myosin light kinase aktiv.
myosin fosforilizasyonu
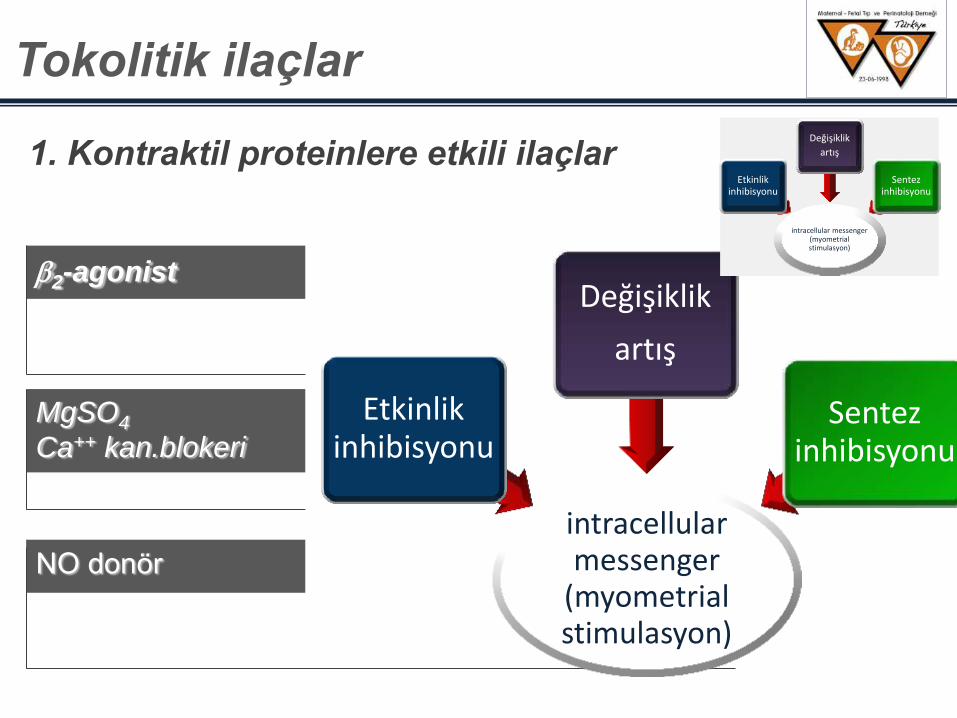
intracellular messenger
(myometrial stimulasyon)
Etkinlik inhibisyonu
Değişiklik
artış
Sentez inhibisyonu
1. Kontraktil proteinlere etkili ilaçlar
Tokolitik ilaçlar
intracellular messenger (myometrial stimulasyon)
Etkinlik inhibisyonu
Değişiklik
artış
Sentez inhibisyonu
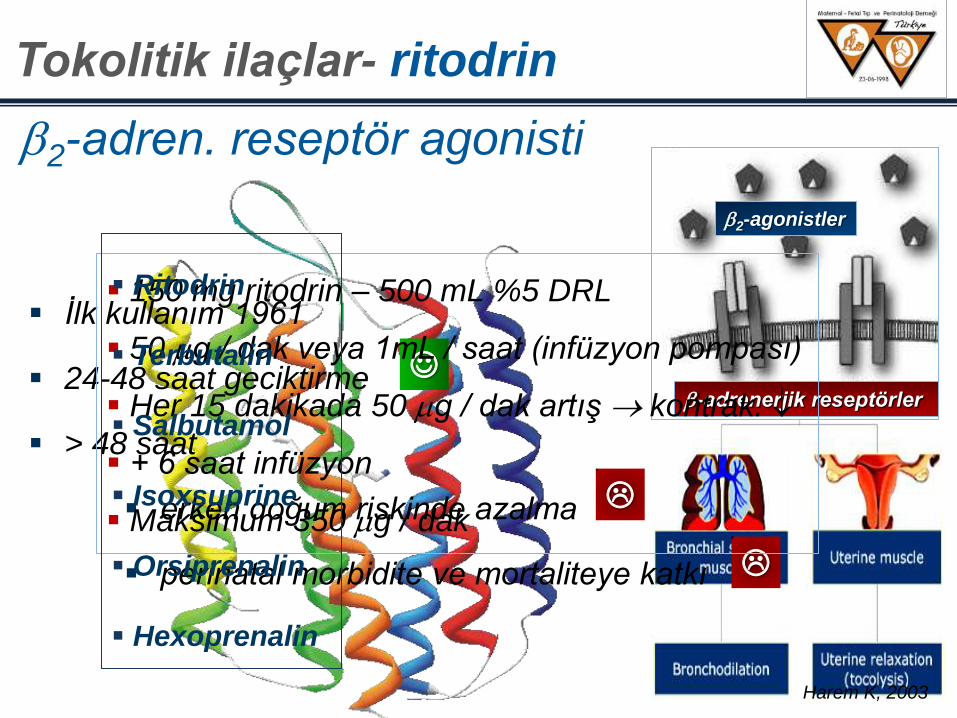
2-adren. reseptör agonisti
Ġlk kullanım 1961
24-48 saat geciktirme
> 48 saat
erken doğum riskinde azalma
perinatal morbidite ve mortaliteye katkı
Harem K, 2003
2-agonistler
-adrenerjik reseptörler
150 mg ritodrin – 500 mL %5 DRL
50 g / dak veya 1mL / saat (infüzyon pompası)
Her 15 dakikada 50 g / dak artış kontrak.
+ 6 saat infüzyon
Maksimum 350 g / dak
Ritodrin
Terbutalin
Salbutamol
Isoxsuprine
Orsiprenalin
Hexoprenalin
Tokolitik ilaçlar - ritodrin
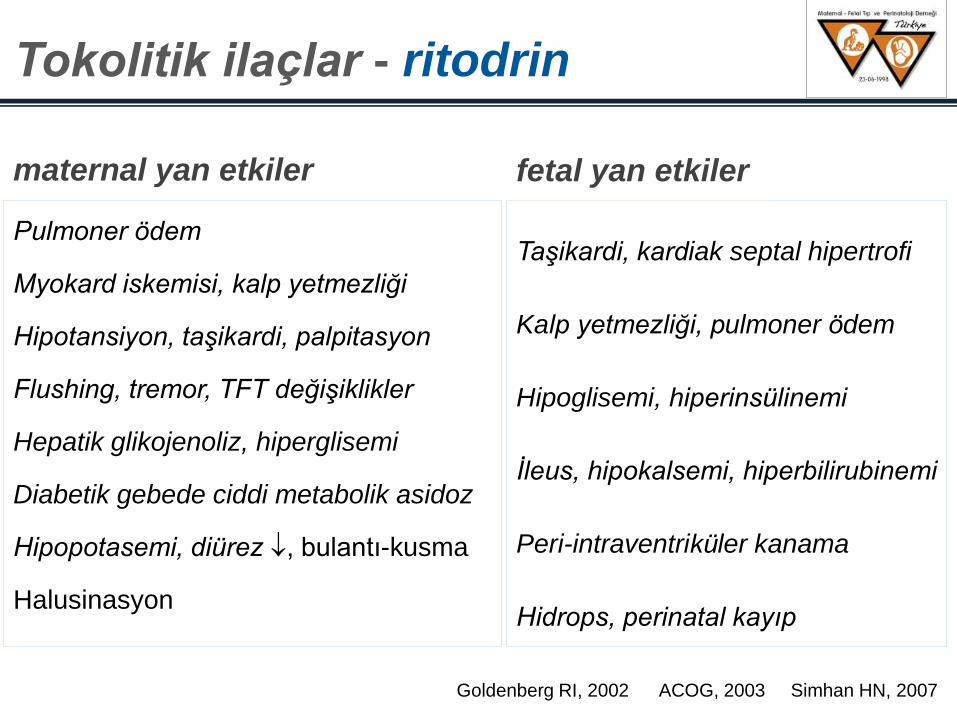
maternal yan etkiler
Pulmoner ödem
Myokard iskemisi, kalp yetmezliği
Hipotansiyon, taşikardi, palpitasyon
Flushing, tremor, TFT değişiklikler
Hepatik glikojenoliz, hiperglisemi
Diabetik gebede ciddi metabolik asidoz
Hipopotasemi, diürez , bulantı-kusma
Halusinasyon
Taşikardi, kardiak septal hipertrofi
Kalp yetmezliği, pulmoner ödem
Hipoglisemi, hiperinsülinemi
Ġleus, hipokalsemi, hiperbilirubinemi
Peri-intraventriküler kanama
Hidrops, perinatal kayıp
fetal yan etkiler
Goldenberg RI, 2002 ACOG, 2003 Simhan HN, 2007
Tokolitik ilaçlar - ritodrin
plasebo -mimetik Ca++ k.blok. MgSO4 Atosiban
Gebe g
rubu %
Ritodrin: Maternal kardiovasküler YE: aritmi, kalp yetm, göğüs ağrısı
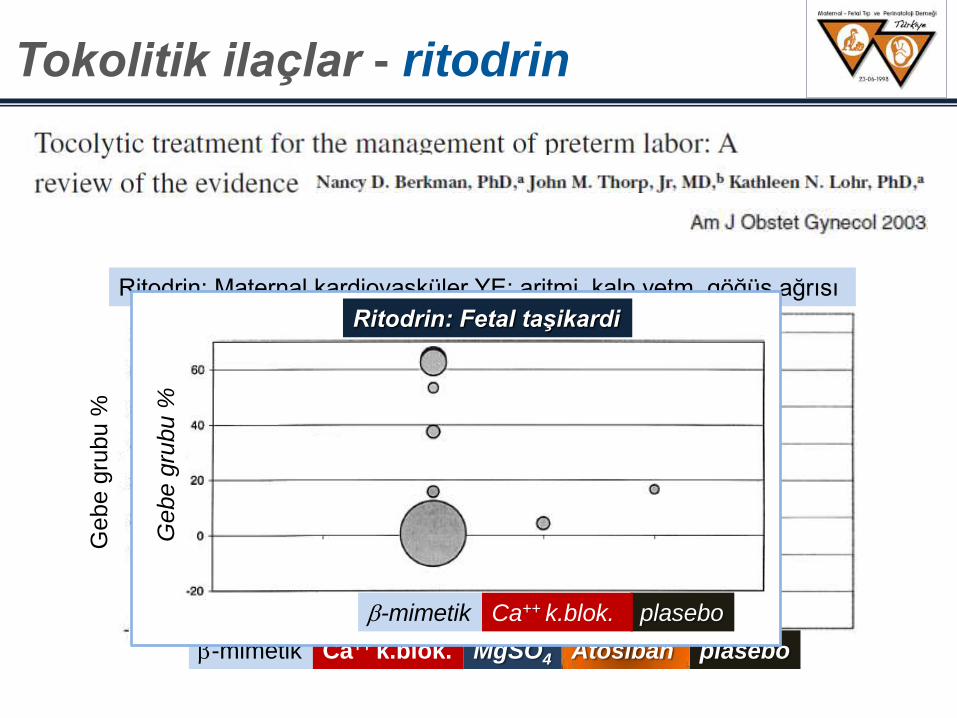
Tokolitik ilaçlar - ritodrin
plasebo -mimetik Ca++ k.blok.
Gebe g
rubu %
Ritodrin: Fetal taşikardi
kontrendikasyonlar
Ciddi kalp hastalığı ve/veya aritmi
Hipertiroidizm *
Diabetes mellitus *
Taşikardi nedeniyle -bloker kullanımı
* kontrolsuz olgular
Goldenberg RL, 2002 ACOG practice bulletin 2003
Tokolitik ilaçlar - ritodrin
1. Nabız, TA: her 15 – 30 dak.
2. Glisemi: her 4 saat
3. Üre ve elektrolitler: her 24 saat
4. Akciğer – solunum sayısı: 4 saat
5. Günlük sıvı alımı - diürez
izlem
RCOG guideline 2002
Tokolitik ilaçlar - ritodrin
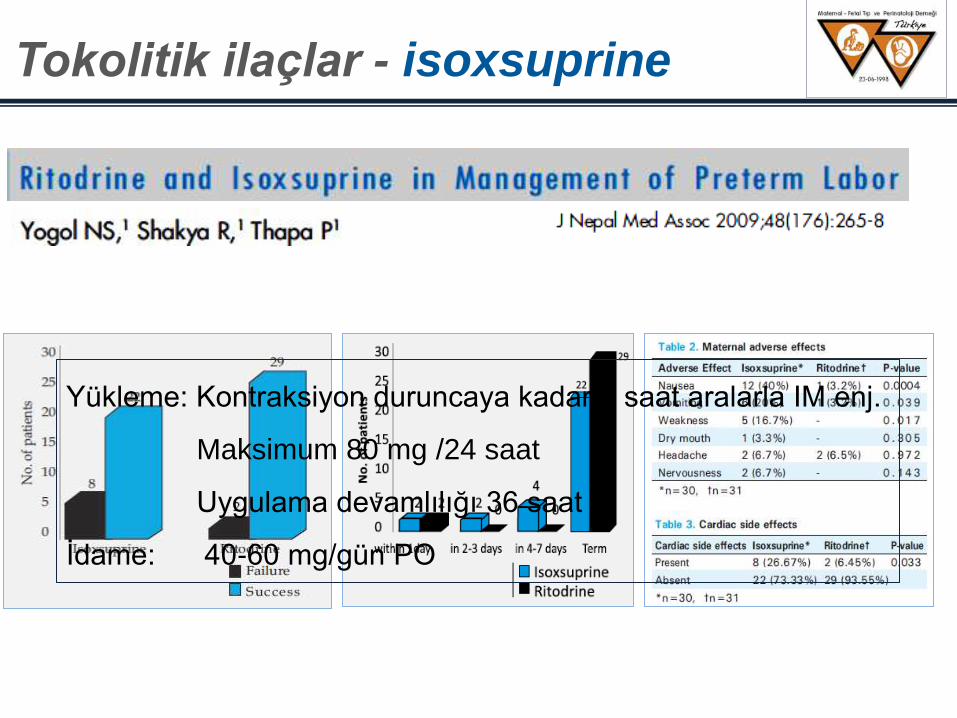
Yükleme: Kontraksiyon duruncaya kadar 3 saat aralarla IM enj.
Maksimum 80 mg /24 saat
Uygulama devamlılığı 36 saat
Ġdame: 40-60 mg/gün PO
Tokolitik ilaçlar - isoxsuprine
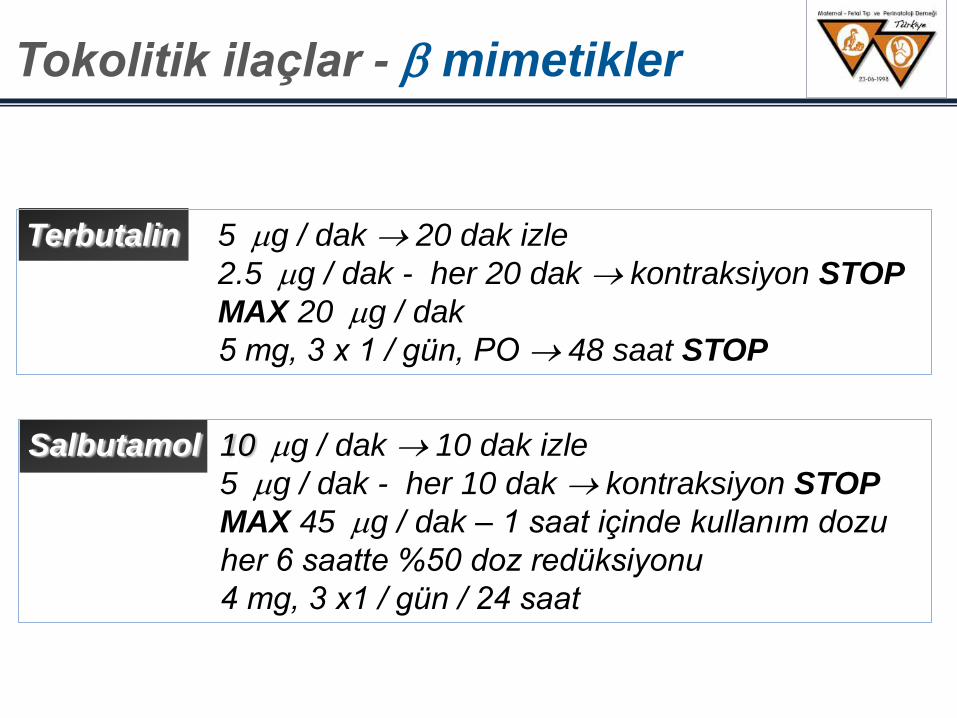
Terbutalin 5 g / dak 20 dak izle
2.5 g / dak - her 20 dak kontraksiyon STOP
MAX 20 g / dak
5 mg, 3 x 1 / gün, PO 48 saat STOP
Salbutamol 10 g / dak 10 dak izle
5 g / dak - her 10 dak kontraksiyon STOP
MAX 45 g / dak – 1 saat içinde kullanım dozu
her 6 saatte %50 doz redüksiyonu
4 mg, 3 x1 / gün / 24 saat
Tokolitik ilaçlar - mimetikler
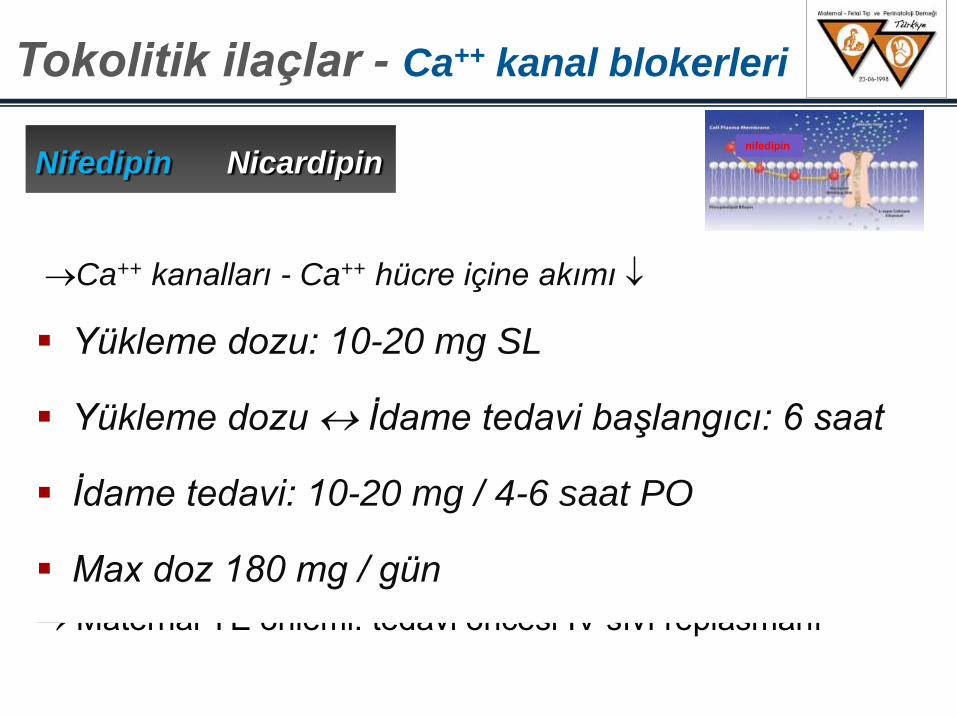
Nifedipin Nicardipin
Ca++ kanalları - Ca++ hücre içine akımı
Emilim 1-2 dakika
Maternal serum pik konsantrasyonu 15-90 dakika
Plasental geçiş 2-3 saat
Tokolitik etkinlik süresi ortalama 6 saat
Kısa sürede, hızlı etkinlik için ideal
Maternal YE önlemi: tedavi öncesi IV sıvı replasmanı
Yükleme dozu: 10-20 mg SL
Yükleme dozu Ġdame tedavi başlangıcı: 6 saat
Ġdame tedavi: 10-20 mg / 4-6 saat PO
Max doz 180 mg / gün
Tokolitik ilaçlar - Ca++ kanal blokerleri
nifedipin
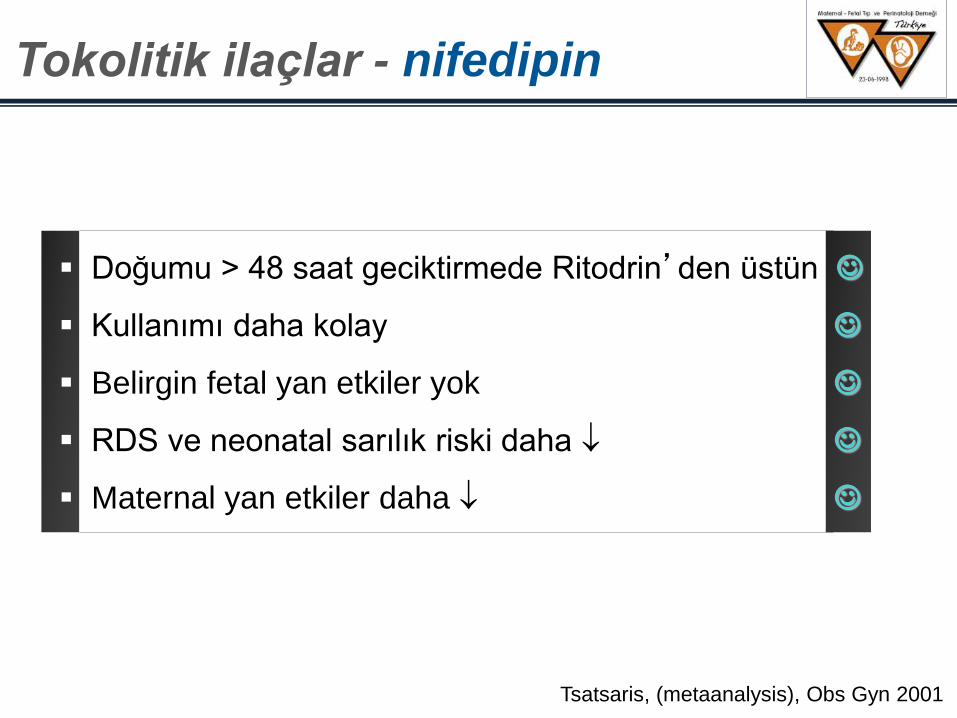
Tsatsaris, (metaanalysis), Obs Gyn 2001
Doğumu > 48 saat geciktirmede Ritodrin’den üstün
Kullanımı daha kolay
Belirgin fetal yan etkiler yok
RDS ve neonatal sarılık riski daha
Maternal yan etkiler daha
Tokolitik ilaçlar - nifedipin
SIK GÖRÜLENLER
Hipotansiyon
Palpitasyon
Baş ağrısı
Bulantı-kusma
Flushing
Periferal ödem
maternal yan etkiler
King, Cochrane 9-2002
NADĠR GÖRÜLENLER
Taşikardi
KC testlerinde bozulma
Konjestif kalp yetmezliği
Transien hiperglisemi
Göğüs ağrısı
Ġskemi (retinal, serebral)
Tinnitus
Pruritus
Tokolitik ilaçlar - nifedipin
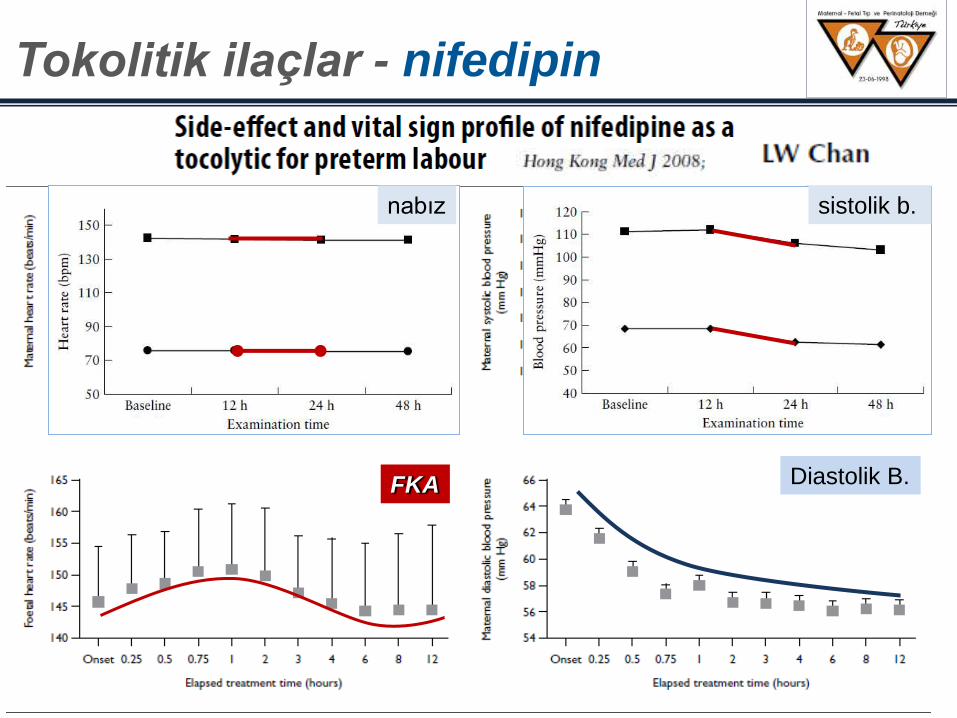
Sistolik B.
Diastolik B. FKA
Maternal KA
Tokolitik ilaçlar - nifedipin
nabız sistolik b.
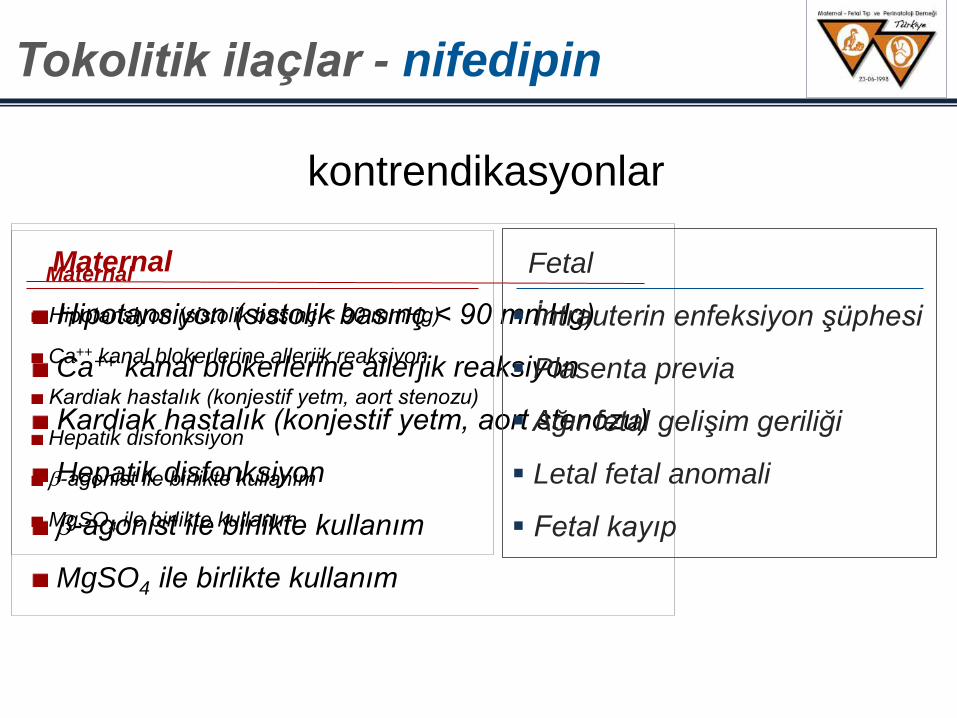
kontrendikasyonlar
Tokolitik ilaçlar - nifedipin
Maternal
Hipotansiyon (sistolik basınç < 90 mmHg)
Ca++ kanal blokerlerine allerjik reaksiyon
Kardiak hastalık (konjestif yetm, aort stenozu)
Hepatik disfonksiyon
-agonist ile birlikte kullanım
MgSO4 ile birlikte kullanım
Fetal
Ġntrauterin enfeksiyon şüphesi
Plasenta previa
Ağır fetal gelişim geriliği
Letal fetal anomali
Fetal kayıp
Maternal
Hipotansiyon (sistolik basınç < 90 mmHg)
Ca++ kanal blokerlerine allerjik reaksiyon
Kardiak hastalık (konjestif yetm, aort stenozu)
Hepatik disfonksiyon
-agonist ile birlikte kullanım
MgSO4 ile birlikte kullanım
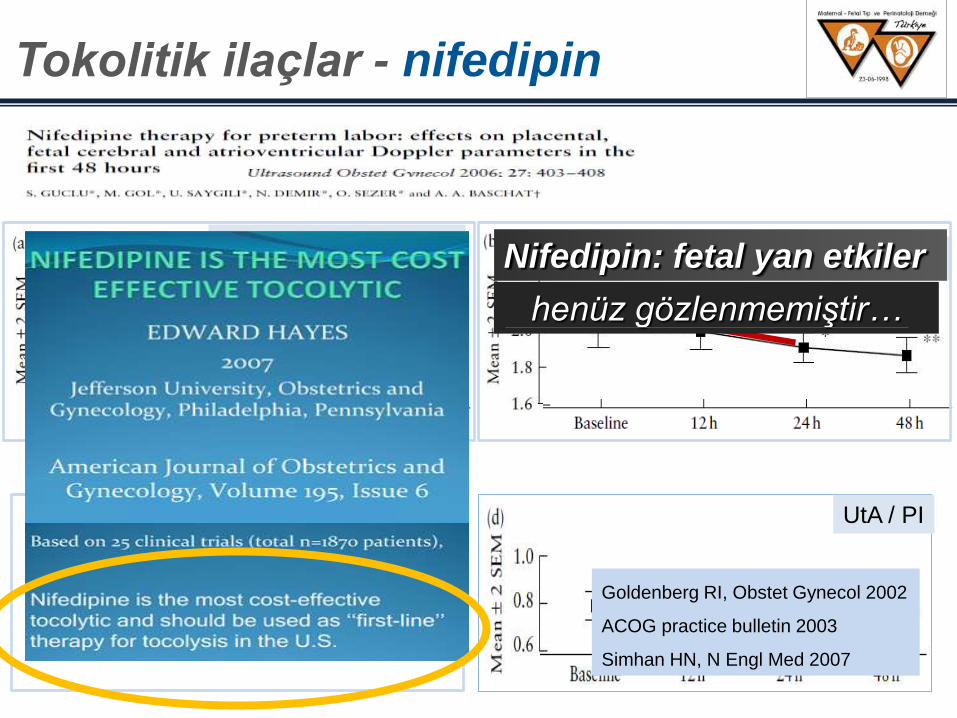
UtA / PI UA / PI
Serebroplasental oran MCA / PI Nifedipin: fetal yan etkiler
henüz gözlenmemiştir…
Goldenberg RI, Obstet Gynecol 2002
ACOG practice bulletin 2003
Simhan HN, N Engl Med 2007
Tokolitik ilaçlar - nifedipin
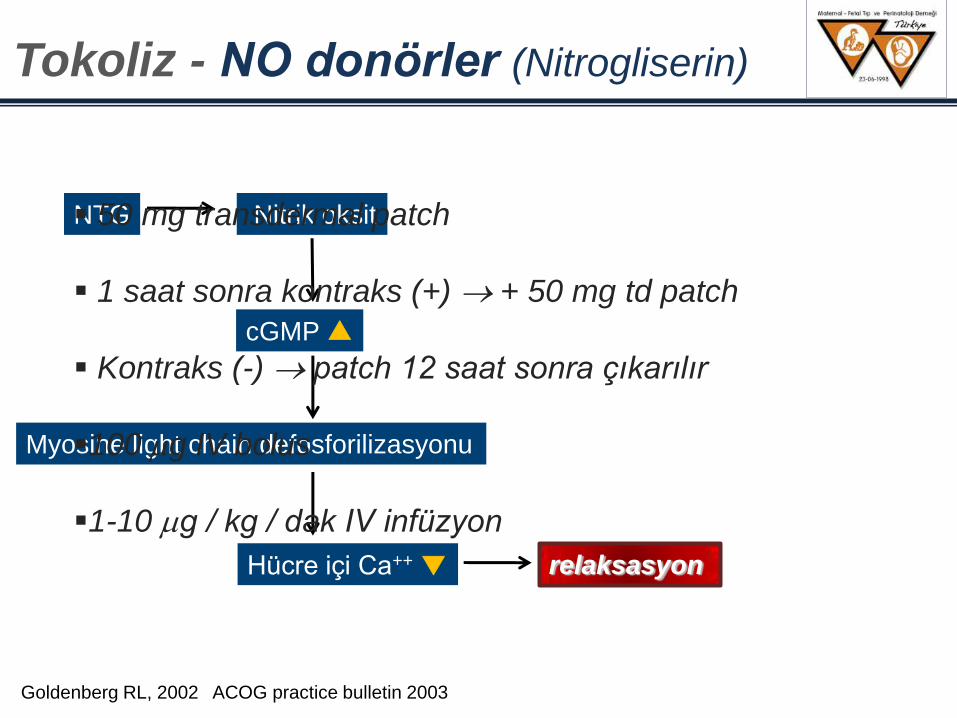
NTG Nitrik oksit
cGMP ▲
Myosine light chain defosforilizasyonu
Hücre içi Ca++ ▼ relaksasyon
50 mg transdermal patch
1 saat sonra kontraks (+) + 50 mg td patch
Kontraks (-) patch 12 saat sonra çıkarılır
100 g IV bolus
1-10 g / kg / dak IV infüzyon
Goldenberg RL, 2002 ACOG practice bulletin 2003
Tokoliz - NO donörler (Nitrogliserin)
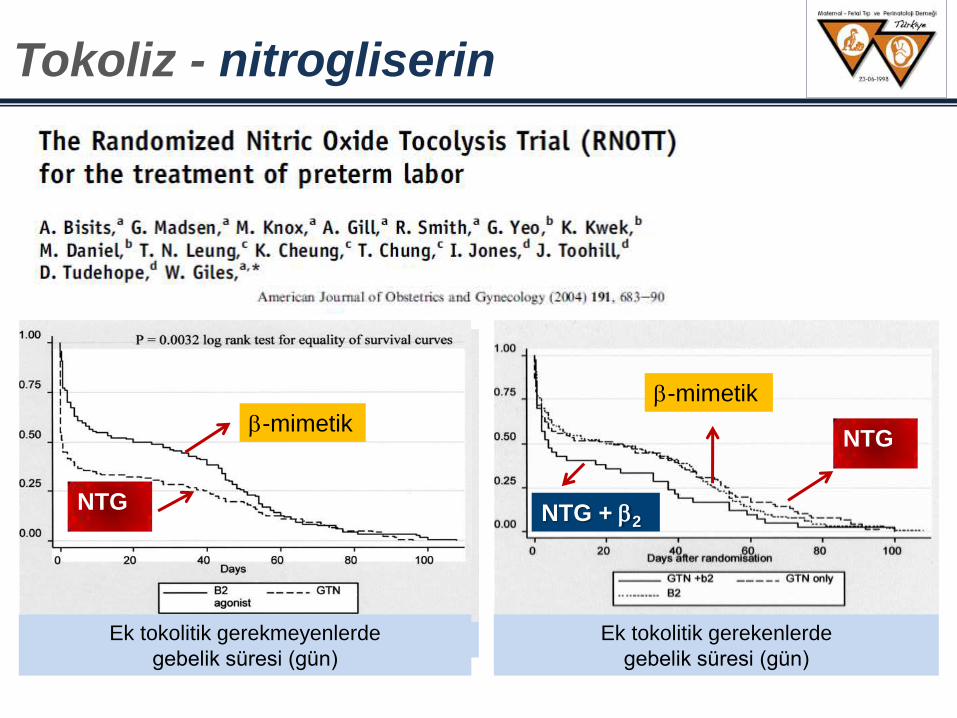
-mimetik
NTG
Tedavi sonrası gebelik süresi (gün)
-mimetik
NTG
Membran intakt gebeler
Tedavi sonrası gebelik süresi (gün)
-mimetik NTG
PPROM gebeler
Tedavi sonrası gebelik süresi (gün) Ek tokolitik gerekmeyenlerde
gebelik süresi (gün)
-mimetik
NTG
Ek tokolitik gerekenlerde
gebelik süresi (gün)
-mimetik
NTG
NTG + 2
Tokoliz - nitrogliserin
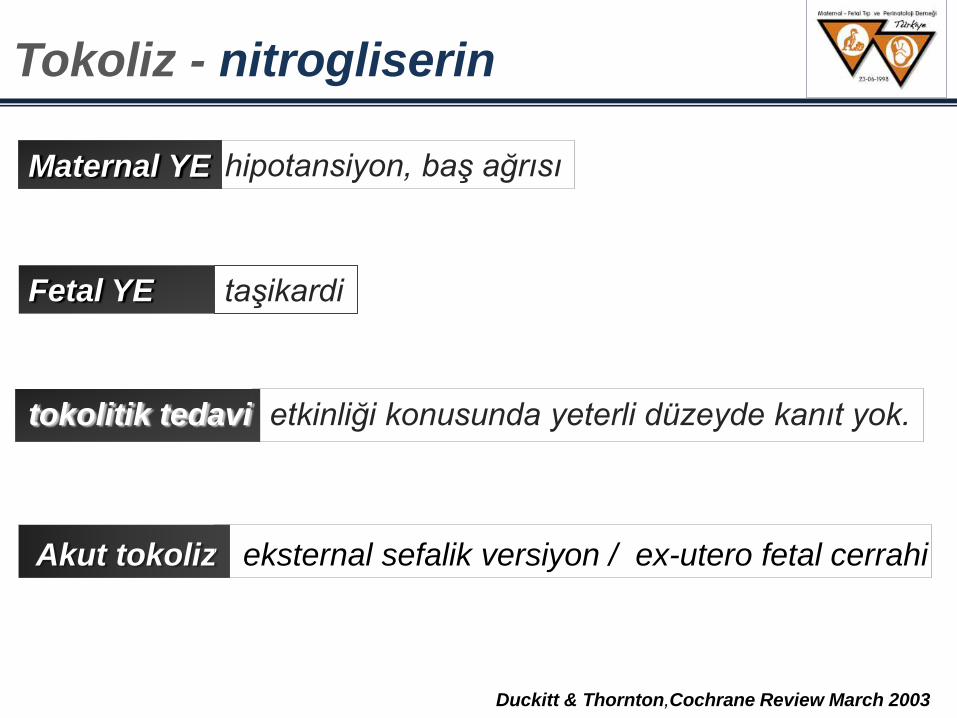
Maternal YE hipotansiyon, baş ağrısı
Fetal YE taşikardi
Tokoliz - nitrogliserin
tokolitik tedavi etkinliği konusunda yeterli düzeyde kanıt yok.
Akut tokoliz eksternal sefalik versiyon / ex-utero fetal cerrahi
Duckitt & Thornton,Cochrane Review March 2003
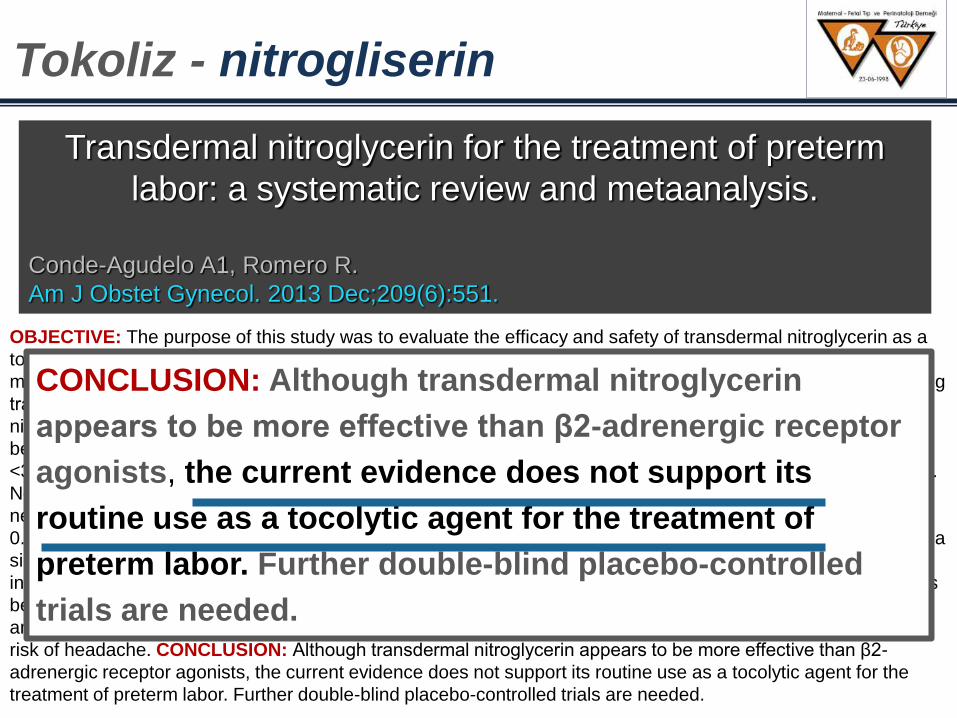
OBJECTIVE: The purpose of this study was to evaluate the efficacy and safety of transdermal nitroglycerin as a
tocolytic agent in women with preterm labor. STUDY DESIGN: We conducted a systematic review and
metaanalysis of randomized controlled trials. RESULTS: Thirteen studies were included (1302 women) comparing
transdermal nitroglycerin vs placebo (2 studies; n = 186); β2-adrenergic receptor agonists (9 studies; n = 1024);
nifedipine (1 study; n = 50); and magnesium sulfate (1 study; n = 42). There were no significant differences
between transdermal nitroglycerin and placebo for delivery within 48 hours of the initiation of treatment or at <28,
<34, or <37 weeks of gestation, adverse neonatal outcomes, and neurodevelopmental status at 24 months of life.
Nevertheless, 1 study found a marginally significant reduction in the risk of a composite outcome of major
neonatal morbidity and perinatal death (3/74 [4.1%] vs 11/79 [13.9%]; relative risk, 0.29; 95% confidence interval,
0.08-1.00). When compared with β2-adrenergic receptor agonists, transdermal nitroglycerin was associated with a
significant reduction in the risk of preterm birth at <34 and <37 weeks of gestation, admission to the neonatal
intensive care unit, use of mechanical ventilation, and maternal side effects. There were no significant differences
between transdermal nitroglycerin and nifedipine and magnesium sulfate in delivery within 48 hours of treatment
and pregnancy prolongation, respectively. Overall, women who received transdermal nitroglycerin had a higher
risk of headache. CONCLUSION: Although transdermal nitroglycerin appears to be more effective than β2-
adrenergic receptor agonists, the current evidence does not support its routine use as a tocolytic agent for the
treatment of preterm labor. Further double-blind placebo-controlled trials are needed.
Transdermal nitroglycerin for the treatment of preterm
labor: a systematic review and metaanalysis.
Conde-Agudelo A1, Romero R.
Am J Obstet Gynecol. 2013 Dec;209(6):551.
Tokoliz - nitrogliserin
CONCLUSION: Although transdermal nitroglycerin
appears to be more effective than β2-adrenergic receptor
agonists, the current evidence does not support its
routine use as a tocolytic agent for the treatment of
preterm labor. Further double-blind placebo-controlled
trials are needed.
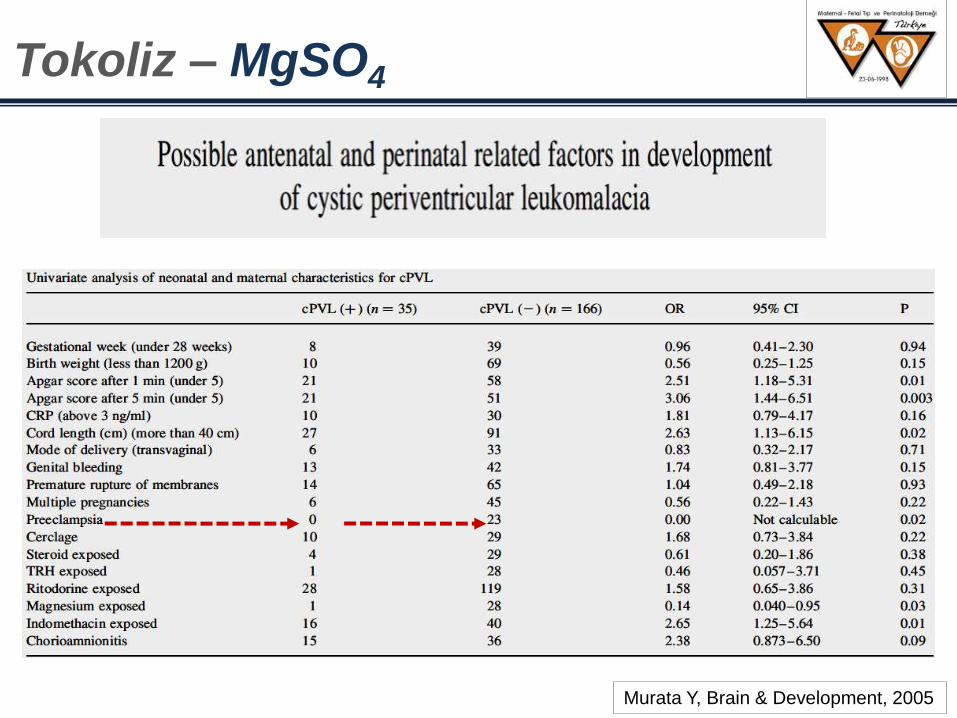
Murata Y, Brain & Development, 2005
Tokoliz – MgSO4
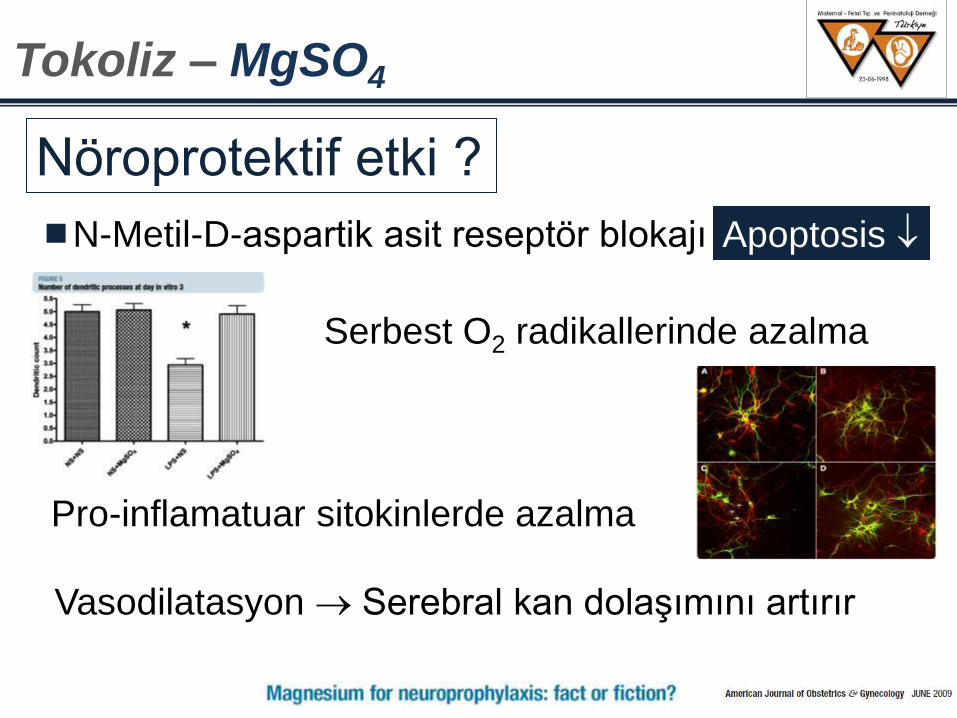
N-Metil-D-aspartik asit reseptör blokajı
Vasodilatasyon Serebral kan dolaşımını artırır
Serbest O2 radikallerinde azalma
Pro-inflamatuar sitokinlerde azalma
Nöroprotektif etki ?
Apoptosis
Tokoliz – MgSO4
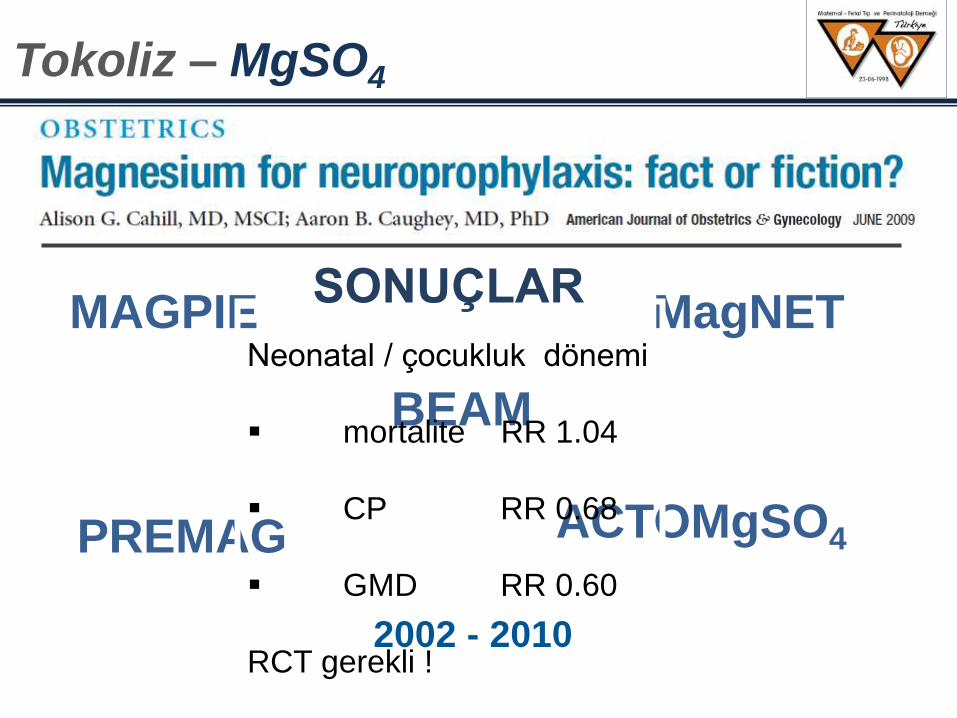
MAGPIE
PREMAG
MagNET
BEAM
ACTOMgSO4
2002 - 2010
Tokoliz – MgSO4
Neonatal / çocukluk dönemi
mortalite RR 1.04
CP RR 0.68
GMD RR 0.60
RCT gerekli !
SONUÇLAR
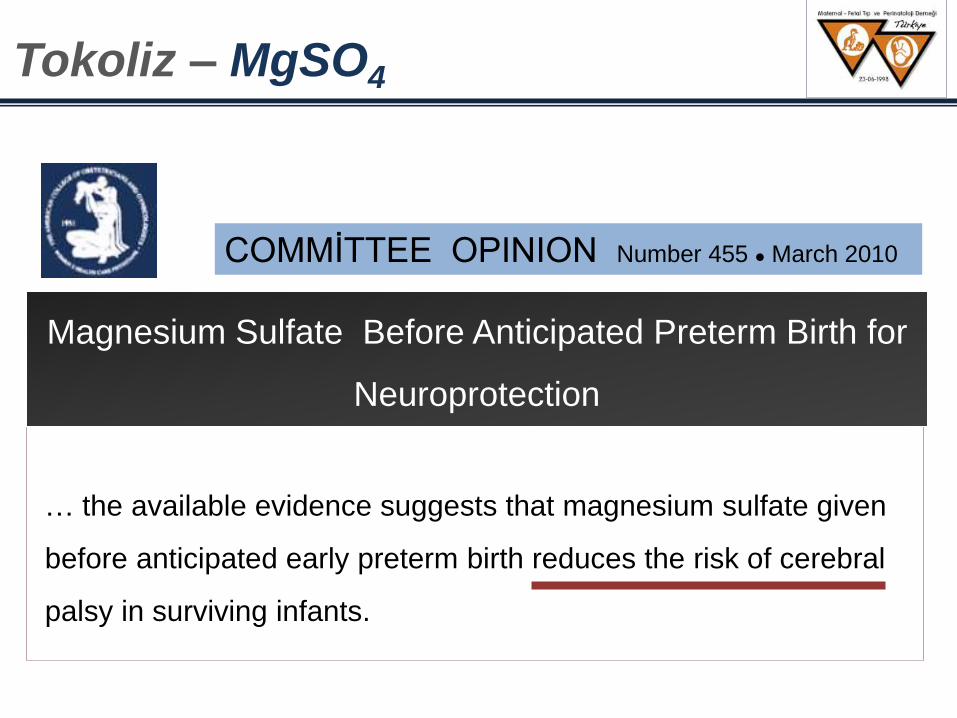
COMMĠTTEE OPINION Number 455 March 2010
… the available evidence suggests that magnesium sulfate given
before anticipated early preterm birth reduces the risk of cerebral
palsy in surviving infants.
Tokoliz – MgSO4
Magnesium Sulfate Before Anticipated Preterm Birth for
Neuroprotection
The Cochrane Library, 2010, issue 1
Tokoliz – MgSO4
- MgSO4 is ineffective at delaying birth or
preventing preterm birth.
- The meta-analysis shows no difference in
paediatric mortality (fetal and later deaths)
between the magnesium or no magnesium
treatment groups.
MgSO4
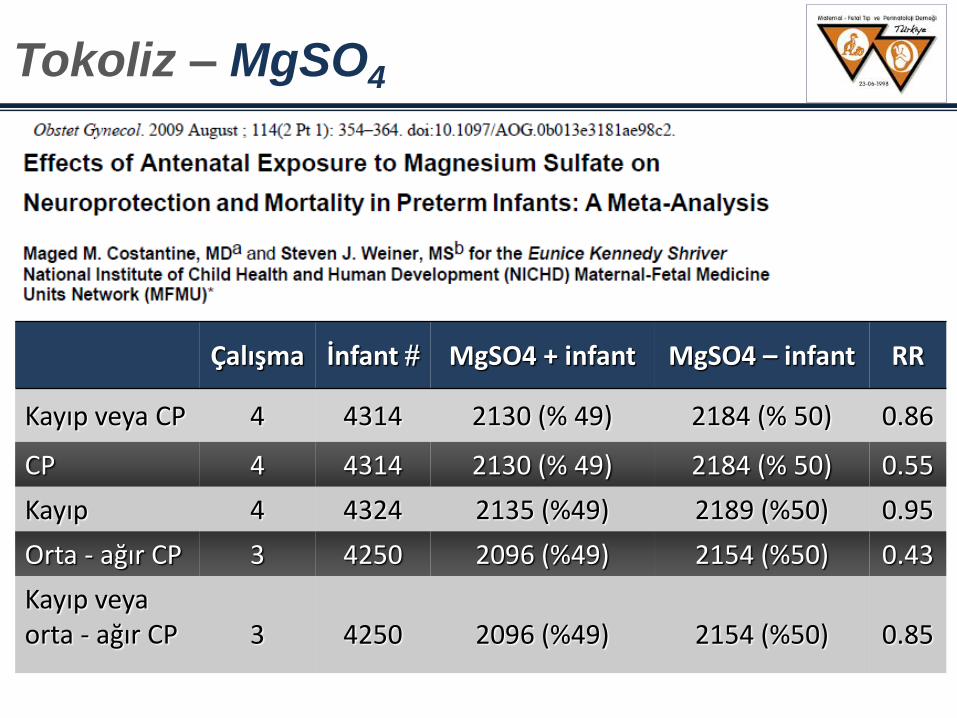
Çalışma İnfant MgSO4 + infant MgSO4 – infant RR
Kayıp veya CP 4 4314 2130 (% 49) 2184 (% 50) 0.86
CP 4 4314 2130 (% 49) 2184 (% 50) 0.55
Kayıp 4 4324 2135 (%49) 2189 (%50) 0.95
Orta - ağır CP 3 4250 2096 (%49) 2154 (%50) 0.43
Kayıp veya orta - ağır CP
3 4250 2096 (%49) 2154 (%50) 0.85
Tokoliz – MgSO4
2. Myometrial endojen stimulanların (oksitosin, PG)
etkinliğini bloke eden ilaçlar
Prostaglandin inhibitörü
Oksitosin-reseptör antagonist
Tokoliz
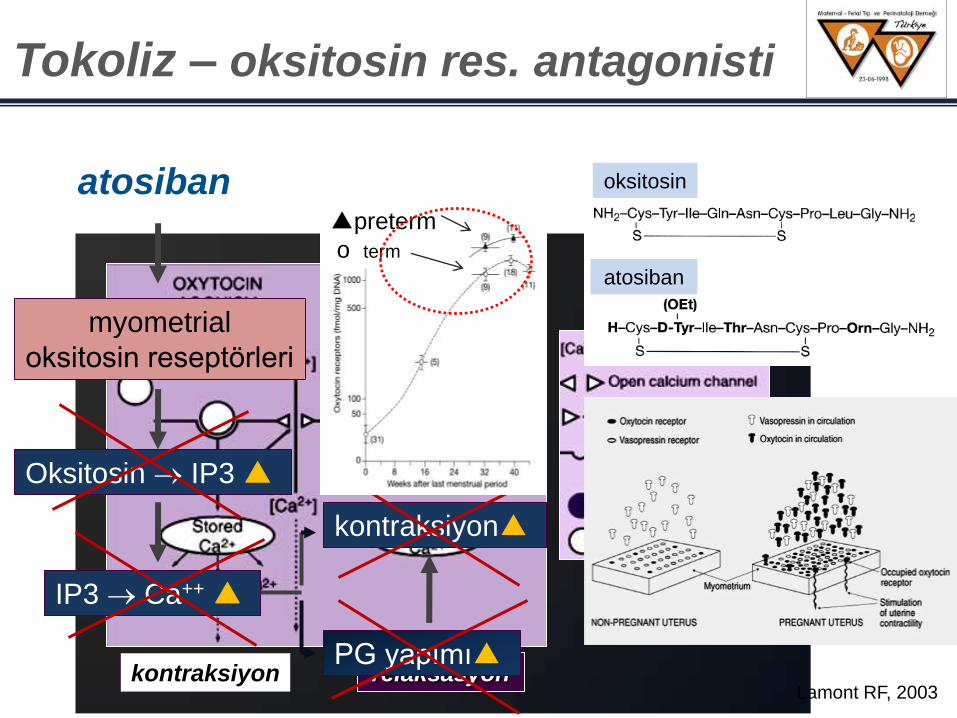
kontraksiyon relaksasyon
atosiban
myometrial
oksitosin reseptörleri
Oksitosin IP3 ▲
IP3 Ca++ ▲
kontraksiyon▲
PG yapımı▲
oksitosin
atosiban
▲preterm
o term
Tokoliz – oksitosin res. antagonisti
Lamont RF, 2003
Sentetik peptit
Kombine reseptör antagonisti: oksitosin / Vasopressin (V1A)
Plazma t1/2 = 13 dakika
Maternal / fetal transfer < 2 agonist (geçiş oranı %12)
<48 saat içinde doğumu erteleme başarısı 2 agonist
Yan etkileri minimum
2 agonistlere göre çarpıntı, taşikardi, hipotansiyon, göğüs ağrısı,
bulantı – kusma daha
Wex, 2009 Worldwide Atosiban vs Beta-agonists Study Group. BJOG 2001
Tokoliz - atosiban
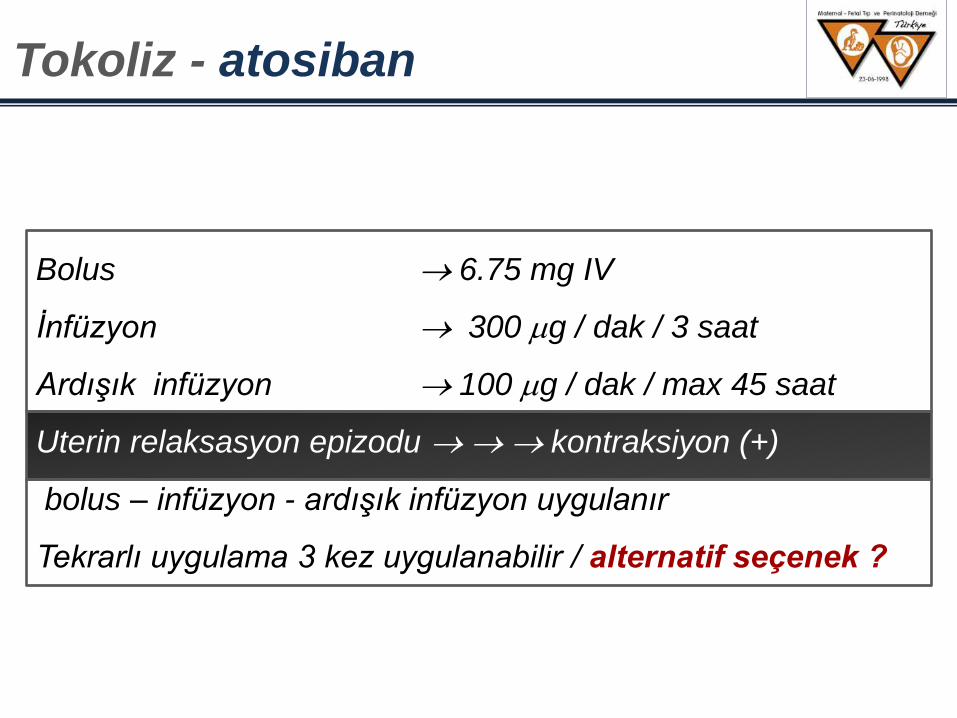
Bolus 6.75 mg IV
Ġnfüzyon 300 g / dak / 3 saat
Ardışık infüzyon 100 g / dak / max 45 saat
Uterin relaksasyon epizodu kontraksiyon (+)
bolus – infüzyon - ardışık infüzyon uygulanır
Tekrarlı uygulama 3 kez uygulanabilir / alternatif seçenek ?
Tokoliz - atosiban
kontrendikasyonlar
> 30 hafta PPROM
IUGR
NST anomalileri
Uterin kanama
Preeklampsi – eklampsi
Fetal kayıp
IU enfeksiyon
Plasenta previa, dekolman
Ġlaca allerjik reaksiyon bilgisi
Tokoliz - atosiban
Tractocile®: CAP-001 Study
Multinational Centres
Atosiban (Tractocile) 2agonist (ritodrin, salbutamol, terbutalin)
Tokolitik tedavi sonrası dönem (<7 gün) ek ve/veya alternatif tedavi
Etkinlik
Güvenilirlik
Tolerans
Yan etkiler tedaviye ara verme
Worldwide Atosiban Study Group, 2000
Tokoliz - atosiban
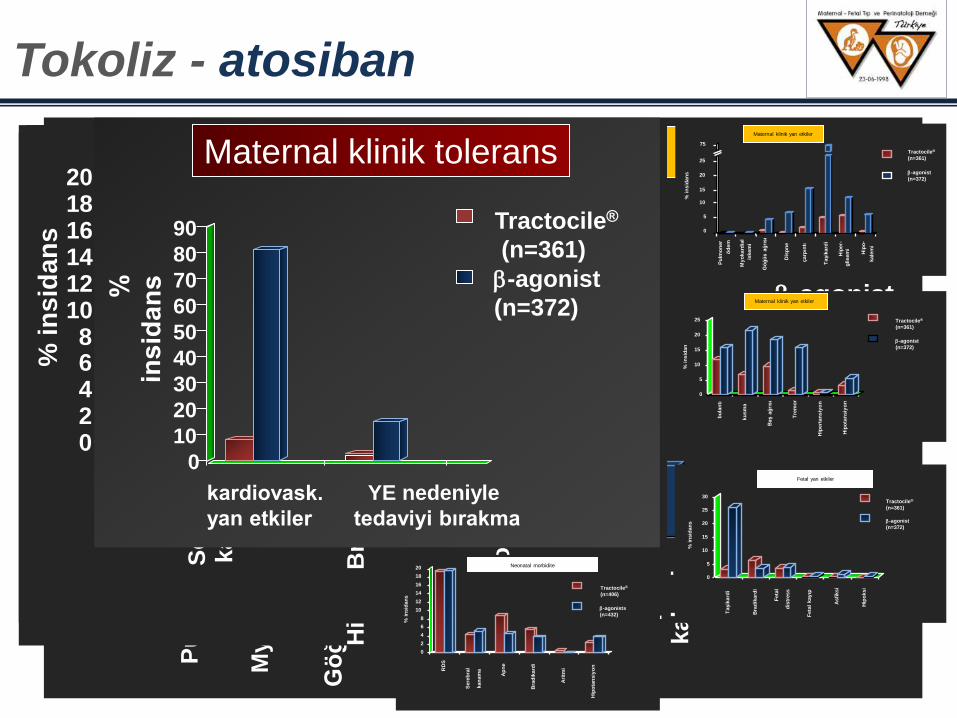
0
5
10
15
20
25 M
yo
kard
ial
Dis
pn
e
çarp
ıntı
Hip
er-
Gö
ğü
s a
ğrı
sı
Taşik
ard
i
Hip
o-
Pu
lmo
ner
öd
em
iskem
i
gli
sem
i
kale
mi
75
% i
nsid
an
s
Tractocile®
(n=361)
-agonist
(n=372)
Maternal klinik yan etkiler
Tokoliz - atosiban
0
5
10
15
20
25
My
okard
ial
Dis
pn
e
çarp
ıntı
Hip
er-
Gö
ğü
s a
ğrı
sı
Taşik
ard
i
Hip
o-
Pu
lmo
ner
öd
em
iskem
i
glisem
i
kale
mi
75
% i
nsid
an
s
Tractocile®
(n=361)
-agonist
(n=372)
Maternal klinik yan etkiler
0
5
10
15
20
25
bu
lan
tı
ku
sm
a
Baş a
ğrı
sı
Tre
mo
r
Hip
ert
an
siy
on
Hip
ota
ns
iyo
n
% i
ns
ida
n
Tractocile®
(n=361)
-agonist
(n=372)
Maternal klinik yan etkiler
0
5
10
15
20
25
bu
lan
tı
ku
sm
a
Baş a
ğrı
sı
Tre
mo
r
Hip
ert
an
siy
on
Hip
ota
nsiy
on
% i
nsid
an
Tractocile®
(n=361)
-agonist
(n=372)
Maternal klinik yan etkiler
0
5
10
15
20
25
30
Taşik
ard
i
Bra
dik
ard
i
Feta
l d
istr
ess
Feta
l kayıp
Asfi
ksi
Hip
oksi
% i
ns
ida
ns
Tractocile®
(n=361) -agonist
(n=372)
Fetal yan etkiler
0
5
10
15
20
25
30
Taşik
ard
i
Bra
dik
ard
i
Feta
l
dis
tress
Feta
l kay
ıp
Asfi
ksi
Hip
oksi
% i
nsid
an
s
Tractocile®
(n=361)
-agonist
(n=372)
Fetal yan etkiler
0 2 4 6 8
10 12 14 16 18 20
RD
S
Se
reb
ral
kan
am
a
Ap
ne
Bra
dik
ard
i
Ari
tmi
Hip
ota
ns
iyo
n
% i
ns
ida
ns
Tractocile®
(n=406)
-agonists
(n=432)
Neonatal morbidite
0
2
4
6
8
10
12
14
16
18
20
RD
S
Sere
bra
l
kan
am
a
Ap
ne
Bra
dik
ard
i
Ari
tmi
Hip
ota
nsiy
on
% i
nsid
an
s
Tractocile®
(n=406)
-agonists
(n=432)
Neonatal morbidite
0
10
20
30
40
50
60
70
80
90
-agonist
(n=372)
YE nedeniyle
tedaviyi bırakma
Tractocile®
(n=361)
Maternal klinik tolerans
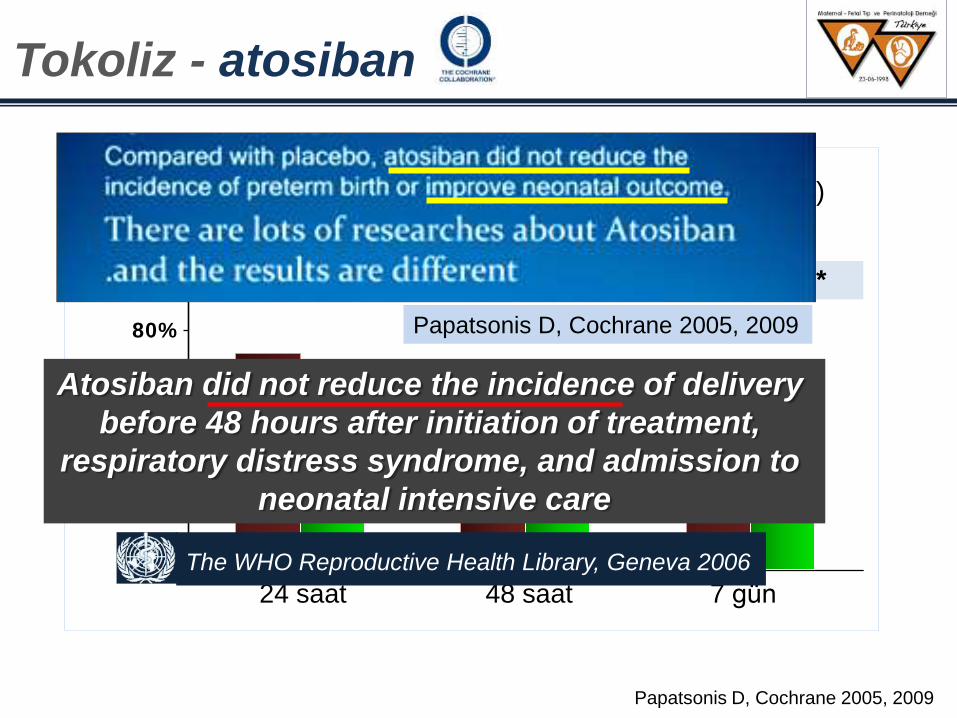
Papatsonis D, Cochrane 2005, 2009
0 %
2 0 %
4 0 %
6 0 %
8 0 %
1 0 0 %
% g
eb
ele
r
p < 0.001* p=0.008* p=0.003*
Atosiban (n =246) Plasebo (n =255)
73%
58% 67%
56% 62%
49%
24 saat 48 saat 7 gün
Papatsonis D, Cochrane 2005, 2009
The WHO Reproductive Health Library, Geneva 2006
Atosiban did not reduce the incidence of delivery
before 48 hours after initiation of treatment,
respiratory distress syndrome, and admission to
neonatal intensive care
Tokoliz - atosiban
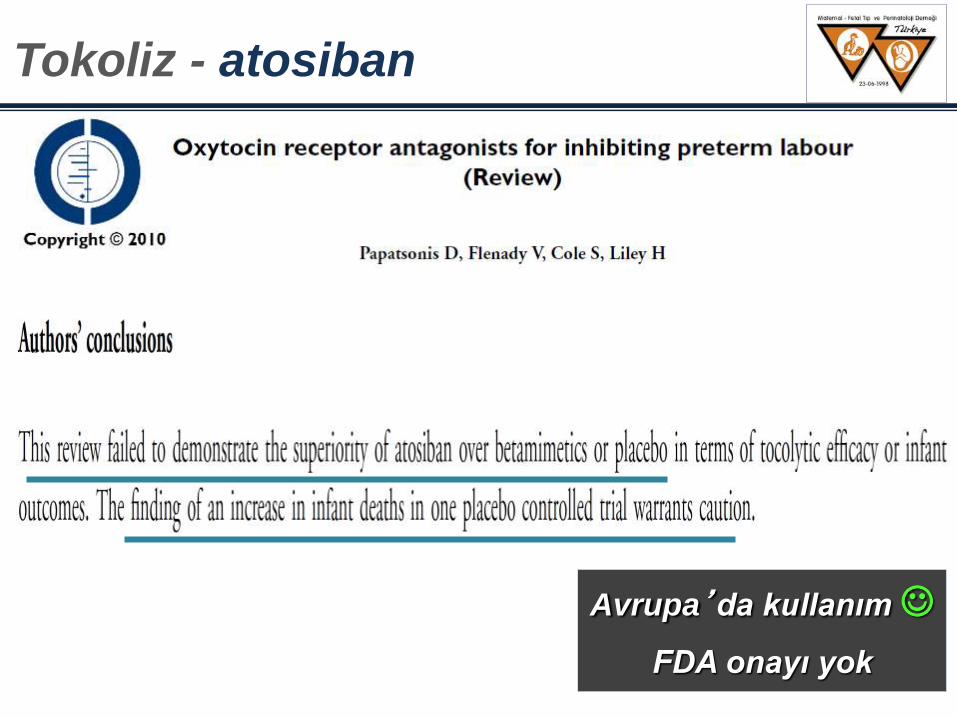
Tokoliz - atosiban
Avrupa’da kullanım
FDA onayı yok
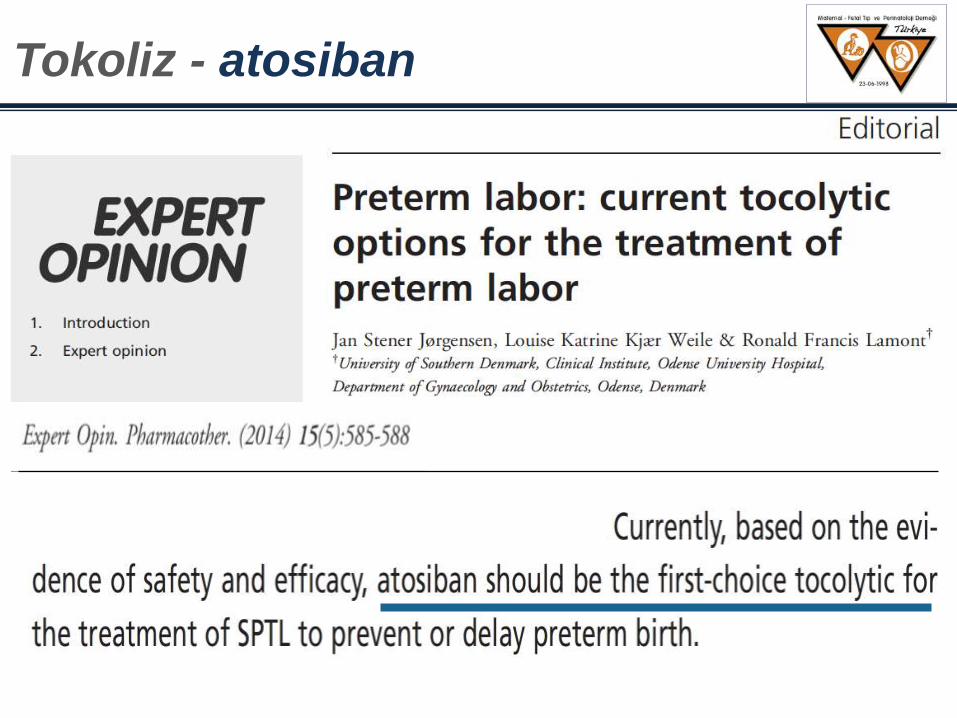
Tokoliz - atosiban
Tokoliz – nifedipin / atosiban
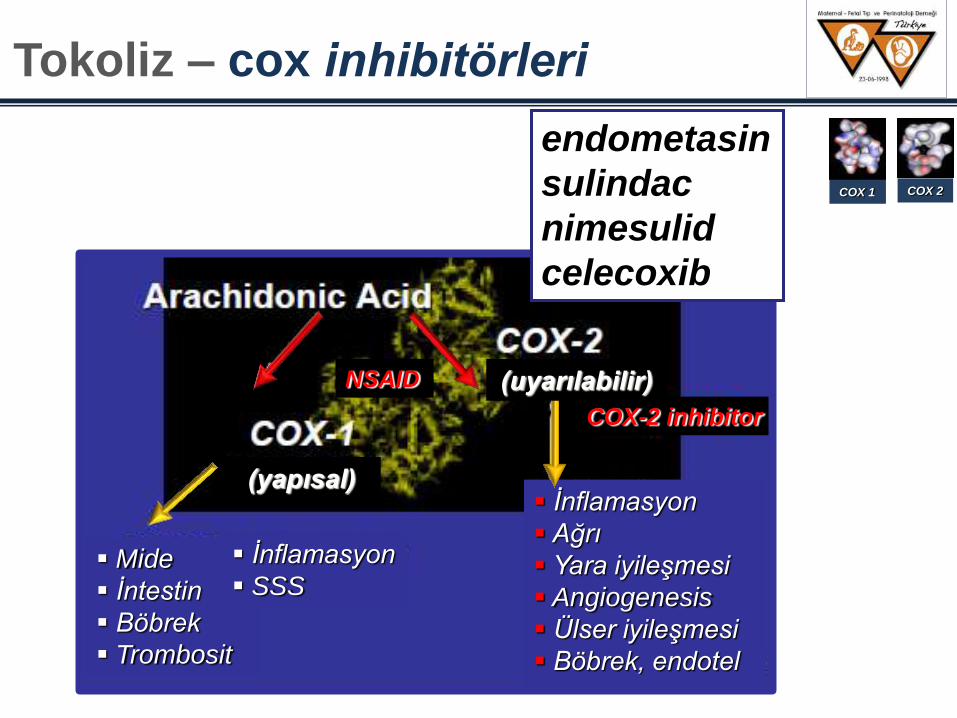
Mide
Ġntestin
Böbrek
Trombosit
Ġnflamasyon
Ağrı
Yara iyileşmesi
Angiogenesis
Ülser iyileşmesi
Böbrek, endotel
(uyarılabilir)
(yapısal)
COX-2 inhibitor
NSAID
Ġnflamasyon
SSS
endometasin
sulindac
nimesulid
celecoxib
COX 1 COX 2
Tokoliz – cox inhibitörleri
Non selektif COX inhibisyonu (endometasin, sulindac, nimesulid)
Selektif COX 2 inhibisyonu (Celecoxib)
Hücre içi PG sentez
Etkin antiinflamatuar + tokolitik etki
Plasenta fetal geçiş (+) perinatal etkiler
Tokolitik etkinlik nonselektif COX inh. Selektif COX 2 inh.
Perinatal yan etkiler nonselektif COX inh. Selektif COX 2 inh.
PO endometasin
6.saat (serum konsantrasyonu) maternal Umb.Art
t1/2: 4-5 saat (maternal)
t1/2: 15 saat (term fetus)
t1/2: > 15 saat (preterm)
Duktal obstrüksiyon geb hf <32 fetuslarda %50 + geçici
Tedavi kesimi < 6-24 saat obstrüksiyon
Tokoliz – endometasin
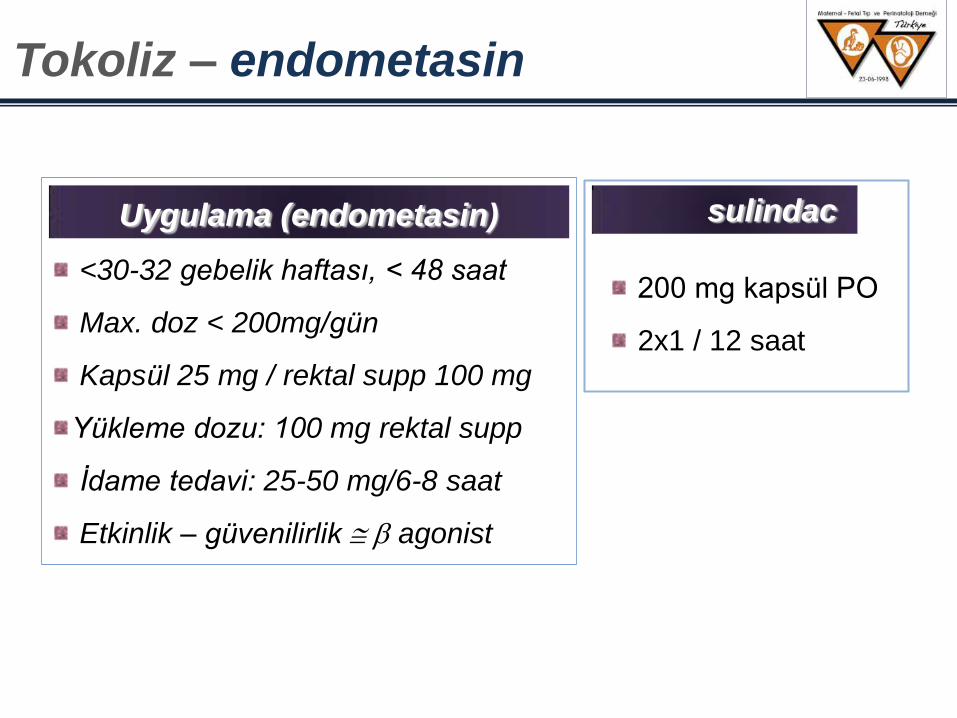
Uygulama (endometasin)
<30-32 gebelik haftası, < 48 saat
Max. doz < 200mg/gün
Kapsül 25 mg / rektal supp 100 mg
Yükleme dozu: 100 mg rektal supp
Ġdame tedavi: 25-50 mg/6-8 saat
Etkinlik – güvenilirlik agonist
sulindac
200 mg kapsül PO
2x1 / 12 saat
Tokoliz – endometasin
endometasin: tokolitik tedavide 2.sırada olabilir
Goldenberg , Obstetrics &Gynecology, 2002
endometasin: polihidramnioslarda 1.sırada olabilir
Newton eMedicine 2002
Etkinlik: endometasin agonist
Maternal yan etkiler: endometasin < agonist
Fetal yan etkiler ??
RCOG Guideline Grade B Recommendation 2002 (Valid:2005)
Tokoliz – endometasin
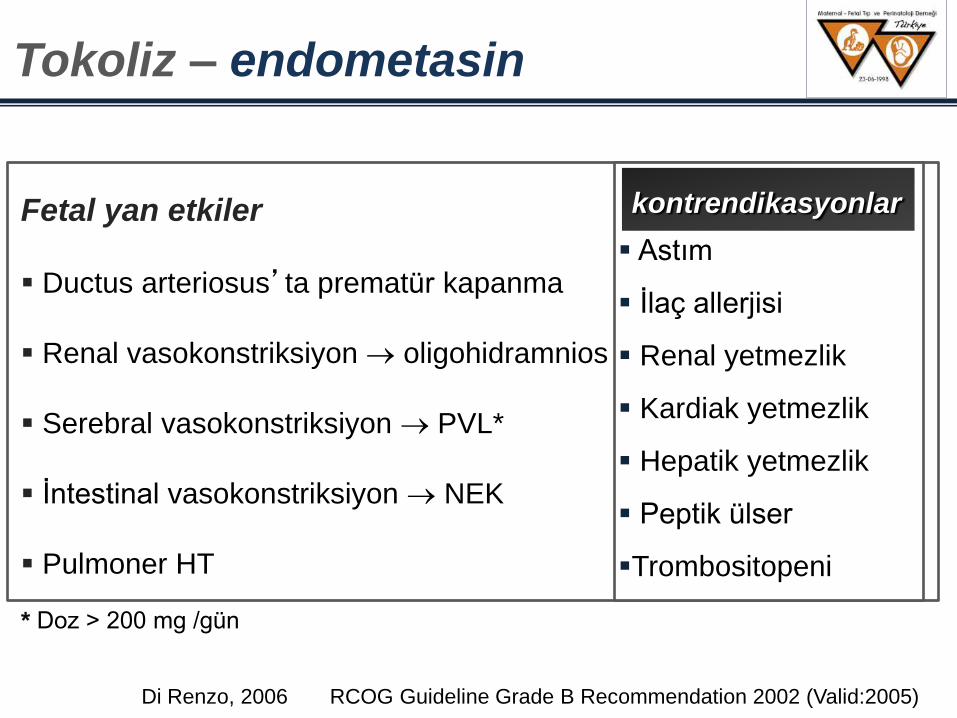
Di Renzo, 2006 RCOG Guideline Grade B Recommendation 2002 (Valid:2005)
Fetal yan etkiler
Ductus arteriosus’ta prematür kapanma
Renal vasokonstriksiyon oligohidramnios
Serebral vasokonstriksiyon PVL*
Ġntestinal vasokonstriksiyon NEK
Pulmoner HT
Maternal yan etkiler
GI şikayetler
Döküntü
Baş ağrısı
Ġnterstisyel nefrit
kontrendikasyonlar
Astım
Ġlaç allerjisi
Renal yetmezlik
Kardiak yetmezlik
Hepatik yetmezlik
Peptik ülser
Trombositopeni
* Doz > 200 mg /gün
Tokoliz – endometasin
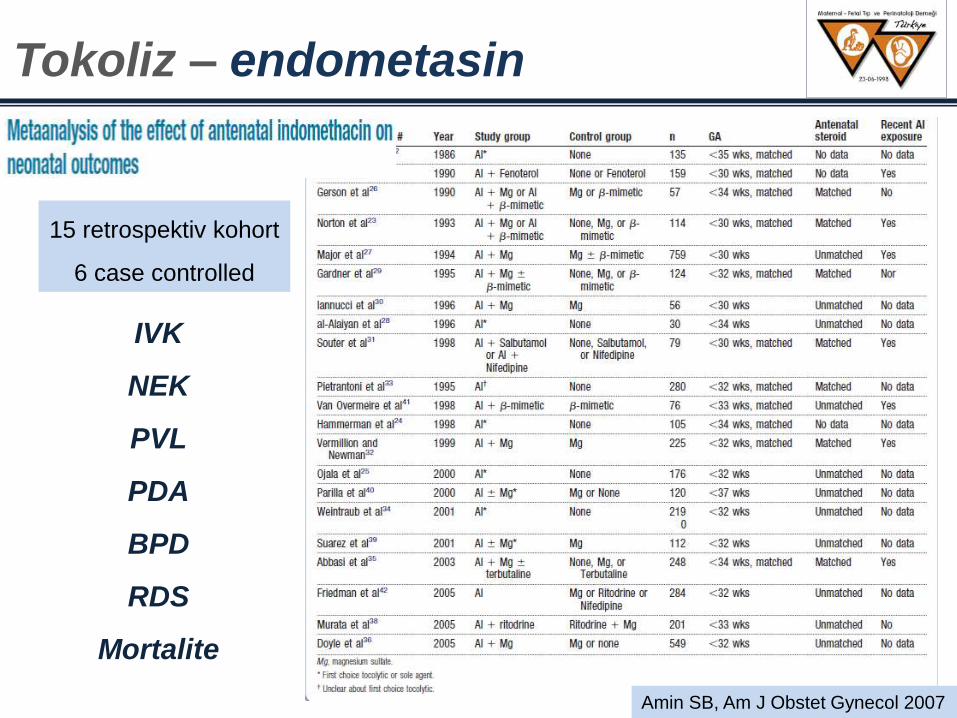
Amin SB, Am J Obstet Gynecol 2007
15 retrospektiv kohort
6 case controlled
IVK
NEK
PVL
PDA
BPD
RDS
Mortalite
Tokoliz – endometasin
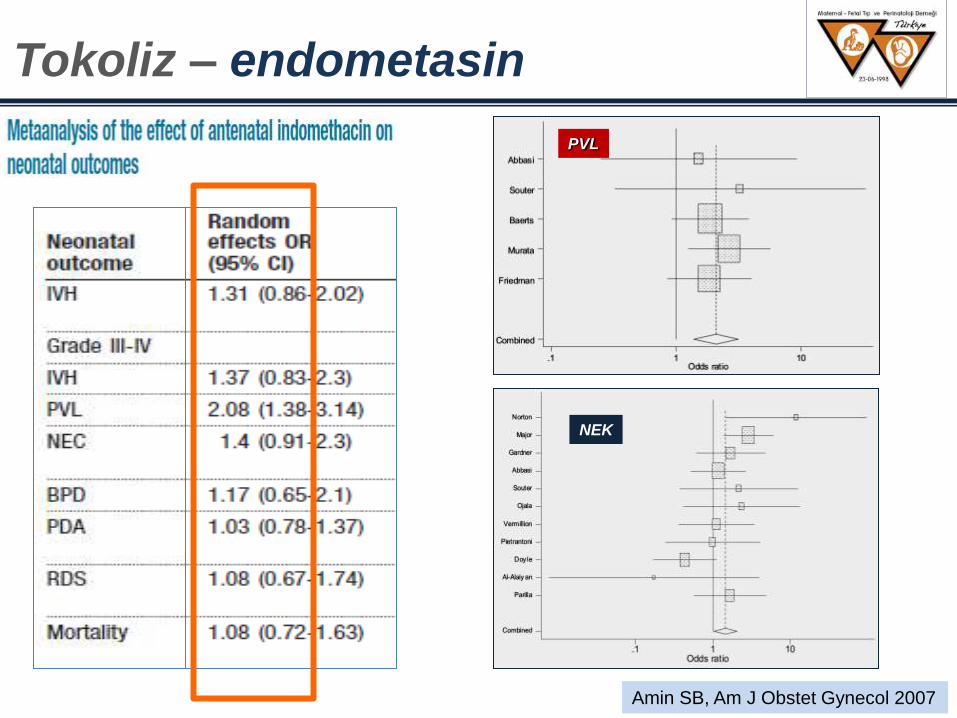
NEK
PVL
Amin SB, Am J Obstet Gynecol 2007
Tokoliz – endometasin
Tokoliz – endometasin
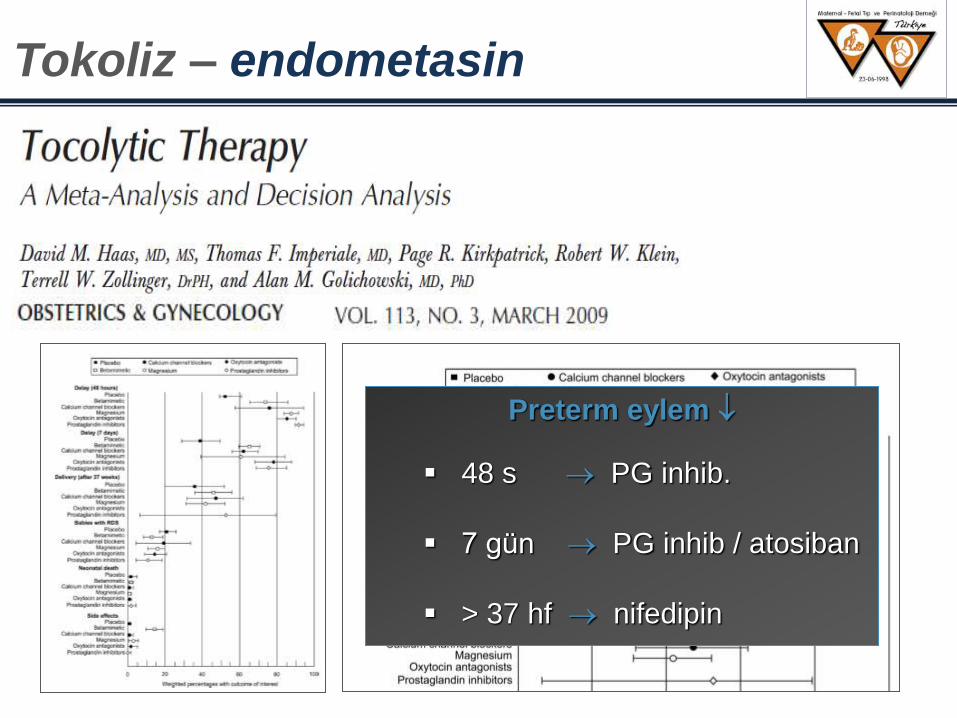
Preterm eylem
48 s PG inhib.
7 gün PG inhib / atosiban
> 37 hf nifedipin
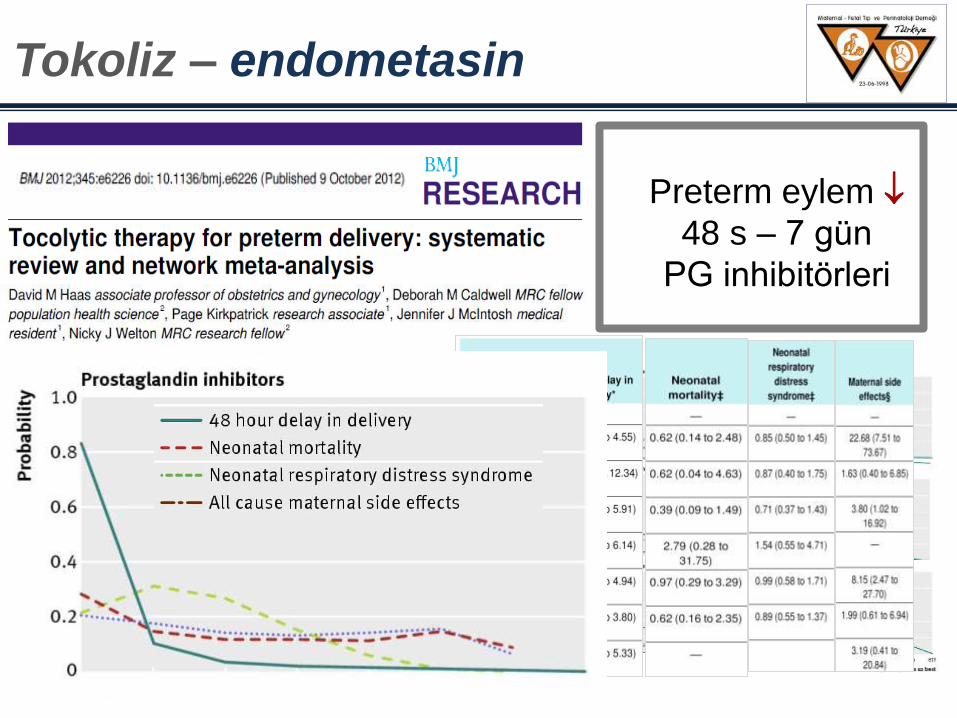
Preterm eylem
48 s – 7 gün
PG inhibitörleri
Tokoliz – endometasin
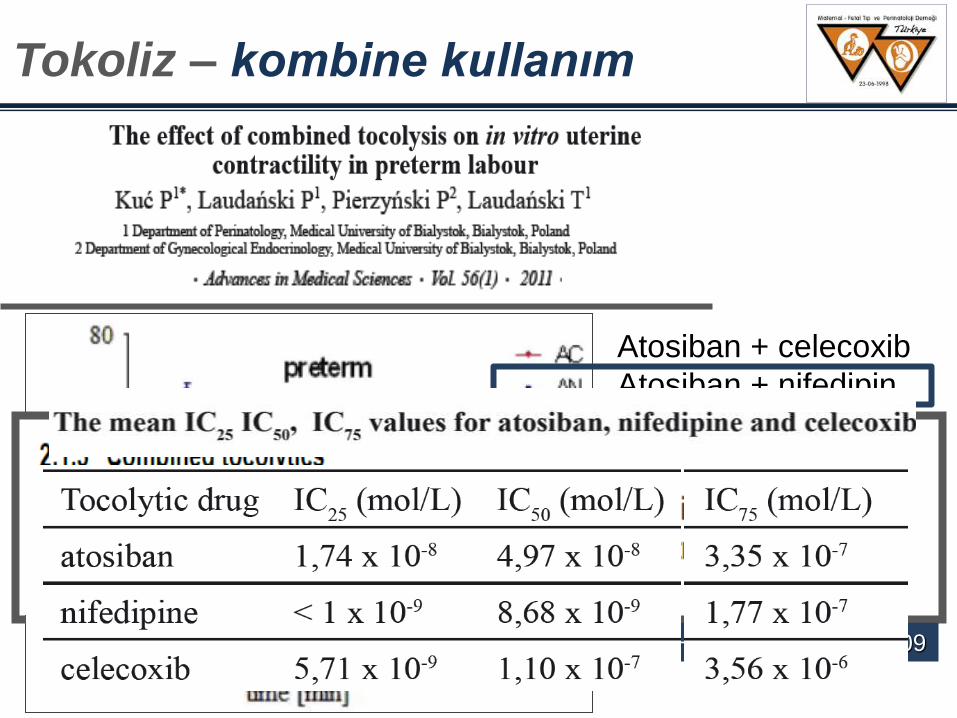
Tokoliz – kombine kullanım
Atosiban + celecoxib
Atosiban + nifedipin
Nifedipin + celecoxib
deHeus R et al. BMJ 2009
Maintenance Tocolysis Is Not
Recommended For Routine Practice.
There is insufficient evidence for any firm conclusions about
whether or not maintenance tocolytic therapy following
threatened preterm labor is worthwhile. Therefore
maintenance therapy cannot be recommended for routine…
practice. RCOG Guideline Grade A recommendation 2005
Tokoliz – idame tedavi
Tokoliz – idame tedavi
The NIFTY study: A multicentre randomised double-blind
placebo-controlled trial of nifedipine maintenance tocolysis
in fetal fibronectin-positive women in threatened preterm
labour. Parry E, Roos C, Stone P, Hayward L, Mol BW, McCowan L.
Aust N Z J Obstet Gynaecol. 2014 Feb 8. doi: 10.1111/ajo.12179.
OBJECTIVE: In an unselected group of women with signs of preterm labour, maintenance tocolysis is not effective
in the prevention of preterm birth and does not improve neonatal outcome. Among women with signs of preterm
labour, those who are fetal fibronectin positive have an increased risk of preterm birth. We investigated whether
maintenance tocolysis with nifedipine would delay delivery and improve neonatal outcome in women with
threatened preterm labour and a positive fetal fibronectin status. STUDY DESIGN: Women with a singleton
pregnancy in threatened preterm labour (24+0 to 33+6 weeks) with a positive fetal fibronectin test were
randomised to nifedipine or placebo. Study medication was continued until 36 completed weeks' gestation. The
primary endpoint was prolongation of pregnancy of seven days. Secondary endpoints were gestational age at
delivery and length of NICU admission. RESULTS:Of the 60 participants, 29 received nifedipine and 31 placebo.
Prolongation of pregnancy by >7 days occurred in 22/29 (76%) in the nifedipine group and 25/31 (81%) in the
placebo group (relative risks, RR 0.94 [0.72-1.2]). Gestational age at delivery was 36.1 ± 5.1 weeks for nifedipine
and 36.8 ± 3.6 weeks for placebo (P = 0.027). Length of NICU admission [median (interquartile ranges, IQR)] was
27 (24-41) days and 16 (8-37) days in nifedipine and placebo groups, respectively (P = 0.17). CONCLUSION:In
women with threatened preterm labour who are fetal fibronectin positive, maintenance tocolysis with nifedipine does
not seem to prolong pregnancy, nor reduce length of NICU admission.
Conclusion: In women with threatened preterm labour
who are fetal fibronectin positive, maintenance tocolysis
with nifedipine does not seem to prolong pregnancy, nor
reduce length of NICU admission.
Tokoliz – idame tedavi
Tokoliz – idame tedavi
Magnesium
does not reduce preterm birth or
improve the outcome
for the infant when given to women after contractions of preterm
labour have been stopped.
PTD Fetal inflamasyon / antibiotik
Tokoliz – pprom
2009

Antibiotik Penisillin
0.90 0.59
0.57 0.29
0.95 0.93
0.82 0.49
Perinat mortalite
Koryoamnionit
RDS
USG: major serebral bulgu
Tedavi vs. kontrol risk ratio
Tokoliz – pprom
IV hydration does not seem to be beneficial, even
during the period of evaluation soon after admission
Stan, Cochrane Review 2000
IV Hidrasyon
Tokoliz – istirahat / hidrasyon
PTD Tokolitik tedavi
1. seçenek
MgSO4
-agonist
Ca++ k.b.
PG inh.
oksitosin antag.
?
öneriler
Antibiotiğin katkısı yok
Akut tokolitik tedavinin tekrarlanması veya idame tedavinin katkısı yok
Tokolitik tedavi ile doğum ort 2-7 gün ertelenebilir
Bu sürede kortikosteroid + sevk planlanır
ACOG Guideline Summary
Preterm eylem tedavisinde ilk tercih edilen tokolitik henüz yok
Klinisyen olguya göre ilaç seçmelidir.
öneriler
Magnezyum sülfat 32.hafta öncesi preterm doğumlarda
CP riskini ve ciddiyetini
ACOG Practice Bulletin No 127: Management of Preterm Labor, 2012
Beta-mimetik. Kardiak aritmi (terbutalin), kontrol edilmemiş
tiroid hastalığı, diabetes mellitus (ritodrin)
MgSO4. Myastenia gravis
Ca++ kanal blokeri. Kalp hastalığı. Beta-mimetik ve MgSO4 ile
kombine edilmez
COX inhibitorü.Renal ve hepatik bozukluk (indometasin);
aktif peptik ülser (ketorolak);
koagulasyon bozukluğu veya trombositopeni
NSAI – sensitiv astım, aşırı duyarlılık (sulindac)
Australia
öneriler
Nifedipine and atosiban have comparable effectiveness in delaying birth for up to seven days
A systematic review using adjusted indirect comparison between nifedipine and atosiban concluded that nifedipine was associated with a non-significant trend towards increased delay in delivery by 48 hours
Rofecoxib, a COX-2 inhibitors, there is therefore no good evidence that it reduce the risk of preterm birth.
There is no clear evidence that magnesium sulphate reduces the risk of preterm birth. However, magnesium reduces the risk of cerebral palsy (RR 0.68; 95% CI 0.54–0.87; five trials; 6145 infants).
Using multiple tocolytic drugs appears to be associated with a higher risk of adverse effects and so should be avoided.
progesteron
The use of 17-hydroxy progesterone in women with arrested
preterm labor: a randomized clinical trial.
Briery CM, Klauser CK, Martin RW, Magann EF, Chauhan SP, Morrison JC.
J Matern Fetal Neonatal Med. 2014 Mar 10.
Abstract Background: The use of 17-alpha-hydroxyprogesterone caproate (17 P) has been shown
to reduce preterm delivery in women who have had a prior preterm birth. The role of 17 P in women
with arrested preterm labor is less certain. Aims: To compare the preterm birth rate and neonatal
outcome in women with arrested preterm labor randomized to receive 17 P or placebo. Materials
and methods: Women with arrested preterm labor were randomized to weekly injections of either
17 P (250 mg) or placebo. Maternal and neonatal outcome were evaluated. Results: Forty-five
singleton pregnancies were randomized after successful tocolysis; 22 received 17 P while 23 got
placebo. Gestational age at delivery (p = 0.067) and the interval from treatment to delivery
(p = 0.233) were not affected by 17 P. Significantly less women in the 17 P group delivered at <34
weeks (14 versus 21, p = 0.035). There was also a significant reduction in the risk of neonatal
sepsis (p = 0.047) and gr III/IV intraventricular hemorrhage (IVH) (p = 0.022) in the 17 P group.
Conclusion: In this study, 17 P did not delay the interval to delivery after successful preterm labor,
but births <34 weeks as well as neonatal sepsis and IVH were reduced by 17 P treatment.
Conclusion: In this study, 17 P did not delay the interval
to delivery after successful preterm labor, but births <34
weeks as well as neonatal sepsis and IVH were reduced
by 17 P treatment.
The aim of our study was to compare the efficacy and safety of nifedipine and progesterone for maintenance
tocolysis after arrested preterm labour, in prolonging pregnancy and preventing recurrence of preterm labour.
This study was a randomised comparative study conducted on 110 pregnant women with arrested preterm labour,
randomised to receive either nifedipine 20 mg Q 8-hourly or progesterone 400 mg daily for maintenance tocolysis.
Other than demographic parameters, obstetric parameters like previous history of abortions or preterm deliveries,
gestational age, cervical dilatation and effacement, ultrasound measured cervical length at admission, were noted.
Outcome measures studied were mean prolongation of pregnancy, mode of delivery, neonatal outcome and side-
effects of both the drugs. We found that there was no significant difference in the demographic profile, parity,
number of abortions, previous preterm deliveries, gestational age, cervical dilatation and effacement at admission
between the two groups. A total of 10% of the patients in the nifedipine group and 61% of the patients in the
progesterone group delivered at term (p value 0.000). The mean prolongation of pregnancy in the nifedipine group
was 16.63 days and 40.14 days in the progesterone group which was significant (p = 0.000). Neonates in the
progesterone group had better birth weight, better Apgar scores at 1 and 5 min, lesser need for ventilation and
significantly lesser composite morbidity. Nifedipine was associated significantly with side-effects. We conclude
that when compared with nifedipine, progesterone significantly prolongs pregnancy in women with arrested
preterm labour with better neonatal outcome and fewer side-effects.
Comparison of nifedipine and progesterone for
maintenance tocolysis after arrested preterm labour.
Kamat S1, Veena P, Rani R.
J Obstet Gynaecol. 2014 Jan 31
We conclude that when compared with nifedipine,
progesterone significantly prolongs pregnancy in
women with arrested preterm labour with better
neonatal outcome and fewer side-effects.
progesteron
Abstract The most significant action of progesterone appears to be on the cervix and in prevention
rather than on treatment of preterm delivery. In women with singleton gestations, no prior PTB, and
CL <20 mm at <24 weeks, vaginal progesterone, either 90 mg gel or 200 mg suppository, is
associated with reduction of both preterm birth (PTB) and perinatal morbidity/mortality. Cerclage is
as effective as vaginal progesterone in women with CL <25 mm. Treatment of women with previous
PTB with 17OHP-C from 16 to 20 weeks' gestation until 36 weeks could reduce significantly both
the risk of delivery at <37, <35 and <32 weeks' gestation, as well as the rates of NEC, the need for
supplemental oxygen and IVH. In women successfully treated with tocolytics progesterone
combined with corticosteroid therapy lengthens pregnancy, reduces occurrence of respiratory
distress syndrome and low birth weight. However, there is currently insufficient evidence on the role
of progesterone after arrested preterm labor. It is reasonable to support an approach with CL
screening of women with prior PTB starting at 16 to 19 weeks and administration of progesterone to
women with a short cervix. Cerclage may be offered to those with a CL<25 mm. A combination of
traditional tocolytics, corticosteroids and progesterone might be beneficial.
progesteron
Cerclage, progesterone and α-hydroxyprogeterone
caproate treatment in women at risk for preterm delivery.
Haram K, Mortensen JH, Morrison JC.
J Matern Fetal Neonatal Med. 2014 Mar 31.
A combination of traditional tocolytics,
corticosteroids and progesterone might be
beneficial.

DEKOLMAN
İLK SEÇİLECEK İLAÇ bireysel
İLK DÜŞÜNÜLECEK
sonuç
Preterm doğum dağılımı
sonuç

PRETERM DOĞUM
teşekkür
ederim
+ HAZIRLIK ÖNGÖRÜ ÖNLEM
sonuç
+ TOKOLĠZ


















