The Use of Probiotics in Pediatric Gastroenterology: A Review ......2014/07/15 · This paper aims...
18
REVIEW ARTICLE The Use of Probiotics in Pediatric Gastroenterology: A Review of the Literature and Recommendations by Latin-American Experts Sylvia Cruchet • Raquel Furnes • Aldo Maruy • Eduardo Hebel • Jorge Palacios • Fernando Medina • Nelson Ramirez • Marina Orsi • Lysette Rondon • Vera Sdepanian • Luis Xo ´chihua • Manuel Ybarra • Roberto Arturo Zablah Published online: 24 March 2015 Ó The Author(s) 2015. This article is published with open access at Springerlink.com Abstract Objective The stability and composition of intestinal flora plays a vital role in human wellbeing throughout life from as early as birth. Over the past 50 years, several studies have been conducted to evaluate the effect of probiotic adminis- tration in pediatric gastroenterology. This document aims to provide a recommendation score on probiotic utilization in pediatric gastroenterology, together with a review of current knowledge concerning its benefits, tolerability, and safety. Study Design Published literature was selected without study design restriction: clinical guidelines, meta-analyses, randomized controlled trials (RCTs), cohort studies, out- comes research and case–controlled studies were selected using the following MESH-validated terms: probiotics, diarrhea, acute diarrhea, antibiotic-associated diarrhea, traveler’s diarrhea, bacterial diarrhea, nosocomial diarrhea, prophylactic diarrhea, Helicobacter pylori infection, colic, infantile colic, necrotizing enterocolitis (NEC), inflamma- tory bowel disease, constipation, and allergy. Once the On behalf of the Latin-American (LATAM) expert consensus group. S. Cruchet (&) Institute of Nutrition and Food Technology, University of Chile, El Libano 5524, Macul Santiago, Chile e-mail: [email protected] R. Furnes Pediatric Gastroenterology, Hospital Privado de Co ´rdoba, Co ´rdoba, Argentina A. Maruy Pediatric Gastroenterology, Nacional Cayetano Heredia Hospital, Peruvian University Cayetano Heredia, Lima, Peru E. Hebel Pediatric Gastroenterology, Medical Department, University La Frontera, Temuco, Chile J. Palacios University of San Carlos de Guatemala, Guatemala City, Guatemala F. Medina Medicine and Nutrition in Pediatric University Industrial de Santander, Bucaramanga, Colombia N. Ramirez Pediatric Gastroenterology, N Del Nino Hospital, La Paz, Bolivia M. Orsi Department of Pediatrics and Gastroenterology, Hospital Italiano of Buenos Aires, Buenos Aires, Argentina L. Rondon Department of Pediatrics and Gastroenterology, Hospital Universitario de Caracas, Caracas, Venezuela V. Sdepanian Department of Pediatric Gastroenterology, Sa ˜o Paulo, Federal University, Sa ˜o Paulo, Brazil L. Xo ´chihua Pediatrics Infectious Diseases, Universidad Auto ´noma de Mexico, Mexico City, Mexico M. Ybarra Pediatrics Infectious Diseases, Hospital Espan ˜ol, Veracruz, Mexico R. A. Zablah Pediatrics and Gastroenterology, Clı ´nica Multipedia ´trica Colonia Escalo ´n San Salvador, San Salvador, El Salvado Pediatr Drugs (2015) 17:199–216 DOI 10.1007/s40272-015-0124-6
Transcript of The Use of Probiotics in Pediatric Gastroenterology: A Review ......2014/07/15 · This paper aims...

REVIEW ARTICLE
The Use of Probiotics in Pediatric Gastroenterology: A Reviewof the Literature and Recommendations by Latin-AmericanExperts
Sylvia Cruchet • Raquel Furnes • Aldo Maruy • Eduardo Hebel • Jorge Palacios •
Fernando Medina • Nelson Ramirez • Marina Orsi • Lysette Rondon •
Vera Sdepanian • Luis Xochihua • Manuel Ybarra • Roberto Arturo Zablah
Published online: 24 March 2015
� The Author(s) 2015. This article is published with open access at Springerlink.com
Abstract
Objective The stability and composition of intestinal flora
plays a vital role in human wellbeing throughout life from as
early as birth. Over the past 50 years, several studies have
been conducted to evaluate the effect of probiotic adminis-
tration in pediatric gastroenterology. This document aims to
provide a recommendation score on probiotic utilization in
pediatric gastroenterology, together with a review of current
knowledge concerning its benefits, tolerability, and safety.
Study Design Published literature was selected without
study design restriction: clinical guidelines, meta-analyses,
randomized controlled trials (RCTs), cohort studies, out-
comes research and case–controlled studies were selected
using the following MESH-validated terms: probiotics,
diarrhea, acute diarrhea, antibiotic-associated diarrhea,
traveler’s diarrhea, bacterial diarrhea, nosocomial diarrhea,
prophylactic diarrhea, Helicobacter pylori infection, colic,
infantile colic, necrotizing enterocolitis (NEC), inflamma-
tory bowel disease, constipation, and allergy. Once the
On behalf of the Latin-American (LATAM) expert consensus group.
S. Cruchet (&)
Institute of Nutrition and Food Technology, University of Chile,
El Libano 5524, Macul Santiago, Chile
e-mail: [email protected]
R. Furnes
Pediatric Gastroenterology, Hospital Privado de Cordoba,
Cordoba, Argentina
A. Maruy
Pediatric Gastroenterology, Nacional Cayetano Heredia
Hospital, Peruvian University Cayetano Heredia, Lima, Peru
E. Hebel
Pediatric Gastroenterology, Medical Department, University La
Frontera, Temuco, Chile
J. Palacios
University of San Carlos de Guatemala, Guatemala City,
Guatemala
F. Medina
Medicine and Nutrition in Pediatric University Industrial
de Santander, Bucaramanga, Colombia
N. Ramirez
Pediatric Gastroenterology, N Del Nino Hospital,
La Paz, Bolivia
M. Orsi
Department of Pediatrics and Gastroenterology, Hospital Italiano
of Buenos Aires, Buenos Aires, Argentina
L. Rondon
Department of Pediatrics and Gastroenterology, Hospital
Universitario de Caracas, Caracas, Venezuela
V. Sdepanian
Department of Pediatric Gastroenterology, Sao Paulo, Federal
University, Sao Paulo, Brazil
L. Xochihua
Pediatrics Infectious Diseases, Universidad Autonoma
de Mexico, Mexico City, Mexico
M. Ybarra
Pediatrics Infectious Diseases, Hospital Espanol,
Veracruz, Mexico
R. A. Zablah
Pediatrics and Gastroenterology, Clınica Multipediatrica Colonia
Escalon San Salvador, San Salvador, El Salvado
Pediatr Drugs (2015) 17:199–216
DOI 10.1007/s40272-015-0124-6

validity and the quality of results were evaluated, a rec-
ommendation score and level of evidence were assigned
for pediatric gastrointestinal-related conditions, according
to the updated Evidence-Based Medicine guidelines: 1a for
systematic review (SR) of RCTs, 1b for individual RCT, 1c
for SR and individual RCT, 2a for SR of cohort studies, 2b
for individual cohort studies, 2c for outcomes research, and
3a for SR of case-control studies.
Results and Conclusions The Latin American Expert
group consensus recommends the use of the following
probiotics for pediatric gastrointestinal conditions: pre-
vention of acute infectious diarrhea (AID): 1b for Bifi-
dobacterium lactis, Lactobacillus rhamnosus GG (LGG),
and L. reuteri; prevention of nosocomial diarrhea: 1 b for
B. lactis Bb12, B. bifidum, LGG and Streptococcus ther-
mophiles; treatment of AID: 1a for LGG and S. boulardii,
1b for L. reuteri; prevention of antibiotic-associated diar-
rhea: 1b for LGG and S. boulardii; prevention of traveler’s
diarrhea: 1b for S. boulardii; prevention of infantile colic:
1a for L. reuteri DSM 17938; treatment of infantile colic:
1b for L. reuteri DSM 17938; prevention of NEC: 1a for B.
breve, mixtures of Bifidobacterium and Streptococcus,
LGG, L. acidophilus and L. reuteri DSM 17938; induction
and maintenance of remission in ulcerative colitis: 1b for
VSL#3; improving symptoms of irritable bowel syndrome:
2c for LGG and VSL#3.
Key Points
Certain probiotics have demonstrated efficacy and
are widely used for preventing and treating medical
conditions involving the gastrointestinal tract in
children.
Lactobacillus rhamnosus GG (LGG), L. reuteri and
Saccharomyces boulardii are the best studied
probiotics and have been shown to be most effective
as treatment if introduced early in the course of the
disease.
Due to strain specificity, only clinically tested
probiotics can be recommended to treat specific
indications in children.
1 Introduction
The stability and composition of intestinal flora plays a
vital role in good health and wellbeing of a human being
throughout life from as early as birth.
In order to improve the microbial intestinal environ-
ment, several studies have been carried out to evaluate the
effect of probiotic administration for the prevention and
treatment of various medical conditions. This paper aims to
provide a detailed review of scientific evidence based on
the use of probiotics in pediatrics, along with current
knowledge concerning its benefits, tolerability, and safety.
This position paper was conceived with the objective to
develop a consensus document that may unify and guide
pediatric healthcare providers in the management of pro-
biotics in Latin America, while incorporating the critical
variable of the benefit of probiotic use.
1.1 Objectives
The purpose of this review was to update scientific evidence
and grade of recommendation to develop future guidance in
the medical use of probiotics in pediatric patients. Three
main objectives were established by the working group:
1. To develop evidence-based guidelines for probiotic
use in pediatric patients through a critical and
comprehensive literature review.
2. To provide a useful tool for probiotic use aimed at
general practitioners, pediatricians, and pediatric
gastroenterologists.
3. To contribute to the rational clinical use of probiotics
in pediatric diseases, supported by scientific evidence.
1.2 Methodology
The present consensus guidelines paper is a result of the
discussions of the Latin American (LATAM) expert con-
sensus group representing ten Latin-American countries:
Argentina, Bolivia, Brazil, Chile, Columbia, El Salvador,
Guatemala, Mexico, Peru, and Venezuela.
The topics selected for this paper were centered on
probiotic use in children in the following indications: acute
infectious diarrhea (AID), antibiotic-associated diarrhea
(AAD), traveler’s diarrhea, Helicobacter pylori infection,
infantile colic, necrotizing enterocolitis (NEC), inflamma-
tory bowel disease (IBD), and functional gastrointestinal
disorders; e.g., irritable bowel syndrome (IBS), constipa-
tion, and allergy. Relevant clinical questions were used as a
basis for discussion and topics were divided between au-
thors according to their field of expertise in the afore-
mentioned various childhood diseases.
The protocol for evidence research was established us-
ing the following validated ‘Medical Subject Headings’
(MeSH�) terms: probiotics, diarrhea, acute diarrhea, AAD,
traveler’s diarrhea, bacterial diarrheal, nosocomial diar-
rhea, prophylactic diarrhea, Helicobacter pylori, infant
colic, infantile colic, NEC, IBD, constipation, and allergy.
A literature search was conducted using PubMed,
MEDLINE, Embase, and the Cochrane database of sys-
tematic reviews (SRs) in Spanish and English, covering the
200 S. Cruchet et al.

period February 1965–October 2014. The patient age range
was 0–18 years.
Published literature was selected without study design
restriction to include SRs and meta-analyses, clinical
guidelines, randomized controlled trials (RCTs), cohort
studies and case–control studies. Narrative reviews were
not used; neither were case series and case reports, nor
observational studies. Only articles with satisfactory
methodology—including clinical guidelines—and which
clearly responded to these questions were selected and
included in our review.
Other papers fulfilling the criteria were also included in
the review; these included papers found through searching
the bibliographies of reviews, and papers that were already
known to the authors but not found in the literature
searches, or subsequently suggested by the peer reviewers.
Since the majority of evaluated articles were RCTs, we
referred to the User Guidelines for Medical Literature and
the Grading of Recommendations Assessment, Develop-
ment and Evaluation (GRADE) system for grading evidence
[1–5] to validate papers selected for critical review by an-
swering the questions shown in Table 1. Assessment of each
article was completed by at least two independent evaluators
and discrepancies were discussed within the entire group and
resolved using scientific consensus. Once the validity and the
quality of results were evaluated, a recommendation grade
and level of evidence were assigned according to the updated
guidelines established by the Oxford Centre for Evidence-
Based Medicine (CEBM) (Table 2) [6].
2 Definition and History of Probiotics
Probiotics are live microorganisms that, when administered
in adequate amounts, confer a health benefit on the host [7]
while enhancing the properties of intestinal flora [8]. Lilly
and Stillwell [9] coined the term probiotics, and, in 1974,
Parker gave it its current significance [10].
It should be emphasized that the FAO/WHO definition
of probiotics provided by the Food and Agriculture Orga-
nization of the United Nations (FAO) and the World Health
Organization (WHO) does not mention the human origin of
the bacterial strain among the criteria for the selection and
definition of probiotics, but instead classify according to
effect caused [7].
Nowadays, probiotics use is increasingly widespread;
however, indication of their use has been evidenced since
ancient times. Over 2000 years ago in Rome in 76 AD, Pliny
the Elder used fermented milk to treat diarrhea. The term
‘probiotic’ (bios: life; pro: in favor of) was used for the first
time in the 1960s, even though the beneficial effect of certain
bacteria had been studied for over a century [5]. In 1906,
Tissier [11] observed that significant colonization of bifi-
dobacteria in stool provided protection against the devel-
opment of diarrhea in children and, in 1908, Eli Metchnikoff,
Professor at the Pasteur Institute in Paris and Nobel laureate
of Medicine and Physiology, illustrated the health benefits of
fermented yogurt (Lactobacillus bulgaricus) [12–14].
In recent years, both consumers and the medical com-
munity have developed an increased interest in the poten-
tial benefits of probiotics, which is amplified by a growing
body of research and literature.
Probiotics may be registered as food supplements or
drugs, depending on efficacy and safety evidence provided
Table 1 Questions for evaluating randomized controlled trials
(RCTs)
I. Evaluation of RCT validity
Was treatment randomly administered to patients?
Was a comprehensive and evolutionary control conducted?
Was analysis done on all patients participating in the RCT?
Was a blinding procedure maintained for the administered
treatment?
Were the study groups similar?
II. Evaluation of RCT results
What was the scope of the treatment’s effect?
How accurately was the treatment’s effect measured?
III. Applicability of results
Can these results be applied when treating my patients?
Were all outcome variables found to be clinically important?
Were benefits higher than undesirable effects?
Table 2 Oxford Centre for Evidence-Based Medicine—levels of
evidence. Adapted from CEBM [6]
Level of
evidence
Therapy/prevention, etiology/harm
1a SR (with homogeneitya) of RCTs
1b Individual RCT (with narrow CI)
1c All or noneb
2a SR (with homogeneitya) of cohort studies
2b Individual cohort study (including low-quality RCT,
e.g.\80 % follow-up)
2c ‘Outcomes’ research; ecological studies
3a SR (with homogeneitya) of case-control studies
3b Individual case-control study
CI confidence interval, RCT randomized controlled trial, SR system-
atic reviewa Homogeneity denotes a systematic review that is free of worrisome
variations (heterogeneity) in the directions and degrees of results
between individual studies. Not all systematic reviews with statisti-
cally significant heterogeneity need be worrisome, and not all wor-
risome heterogeneity need be statistically significantb Met when all patients died before the treatment became available,
but some now survive on it; or when some patients died before the
treatment became available, but none now die on it
Probiotics in Pediatric Gastroenterology 201

by manufacturers to Health Evaluation Authorities [15].
Probiotics are available as capsules, tablets, packets, or
powders and are contained in various fermented foods; in
addition, probiotic products may contain a single mi-
croorganism or a mixture of several species [16–19].
Among the scientific community, probiotics are designated
by nomenclature agreement, based on their genus, species,
and an alphanumeric designation, for example, Saccha-
romyces boulardii CNCM I-745, L. casei DN-114 001 or L.
rhamnosus GG (LGG).
A variety of bacteria have been studied to explore their
probiotic effect, including various Lactobacillus and Bifi-
dobacterium strains, which are normal inhabitants of a
healthy intestinal flora as well as the yeast S. boulardii and
some bacillus species. Criteria for probiotic use are listed
in Table 3 [20]. When evaluating this research, it is im-
portant to note that the effects of any bacteria are strain-
specific, meaning the data from research relates only to the
specific strain being evaluated [10, 15, 18, 19].
3 Mechanisms of Action
The mechanisms of action of probiotics are summarized in
Table 4. The proposed mechanisms for the protective ef-
fects of probiotics include direct hostility towards patho-
gens through competitive adherence to the mucosa and
epithelium; strengthening of the gut epithelial barrier and
modulation of the immune system to convey an advantage
to the host by restoring normal intestinal flora [21]; in-
hibiting Clostridium difficile through an antisecretory ef-
fect [22]; production of intestinal mucin; synthesis of
bacteriocins and other antimicrobial molecules; restoration
of close enterocyte bonds (by re-establishing intestinal
permeability); secretion of immunologic defensins; inter-
action with dendritic cells, Toll-like receptors (TLRs) and
intracellular inflammatory pathways; activation of macro-
phages and natural killer (NK) cells [23]; stimulation of
lymphoid tissue associated with the gut (GALT) [24]; and
modulation of innate and adaptive immunity involving
immunoglobulins and cytokines [25].
Total fecal lgA and polio antivirus are increased sig-
nificantly with live bifidobacteria. Kaila et al. [26] illustrated
that LGG significantly increased the humoral immune re-
sponse to rotavirus enteritis, and more so with live probiotics
than inactive ones; in addition, adhesion of Bifidobacteria
Bb12 improves in the presence of LGG in healthy children
and during episodes of diarrhea, suggesting that the action of
the two probiotics might be synergistic.
S. boulardii CNCM I-745 has several mechanisms of
action which may be classified into three main areas: lu-
minal action, trophic action, and mucosal—anti-inflam-
matory signaling effects. Within the intestinal lumen, S.
boulardii may interfere with pathogenic toxins (especially
C. difficile toxin A and B), preserve cellular physiology,
interfere with pathogen attachment, interact with normal
microbiota or assist in reestablishing short-chain fatty acid
levels. S. boulardii also may act as an immune regulator
(either acting as an immune stimulant or by reducing pro-
inflammatory response), both within the lumen and sys-
temically [27].
4 Results
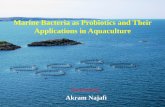
A flow chart presenting the literature search results and se-
lection process is shown in Fig. 1. The initial electronic
search identified 219 articles, plus another 18 were identified
via other sources. After de-duplication, 209 records re-
mained, and of these, 17 were excluded due to the content
being non-relevant (n = 3) or due to being published in a
language other than English, French or Spanish (n = 14). Of
the remaining 192 papers, full text examination led to an-
other 20 being excluded (Fig. 1). Another six papers were
identified by peer reviewers and added at the post-submis-
sion stage. The final number of papers included in the review
was 178, and of these, 74 provided guidance on the use of
Table 3 Criteria for use as a probiotic. Adapted from Borchers et al.
[20]
The organism must be fully identified: genus, species and strain
No pathogenic effects and toxicity, and must not be associated
with disease or be carrying antibiotic resistance genes
It must be viable and stable (at least briefly) in the gastrointestinal
tract, and resistant to bile acids and digestive enzymes
It must adhere to mucosal surface and colonize the intestine (at
least briefly)
It must be stable during processing and storage
It must have a sufficient number of viable cells
It must undergo in vivo and in vitro trials to prove any attributed
probiotic effect and documented clinical benefit
Table 4 Summary of mechanisms of action of probiotics
Immunomodulation Increase in the number of immunoglobulin-
secreting cells in the intestinal mucosa
Facilitates transport of antigens to the
submucosal lymphocytes ensuring a more
immediate immune reaction [25]
Antibacterial action Production of antibacterial substances
Action against common pathogens (E. coli,
Clostridium difficile and Salmonella spp.)
[21]
Competitive
exclusion
Competes with adhesion of pathogens to the
intestinal mucosa
Colonization of the intestine with beneficial
bacteria [23]
202 S. Cruchet et al.

probiotics in children. The papers were divided into the
specified indications and discussed in the following sections.
5 Clinical Applications of Probiotics
in Gastroenterology
5.1 Acute Infectious Diarrhea (AID)
5.1.1 Prevention of AID
Breast milk provides the best protection against infectious
gastrointestinal disease in infants. Attempts have been made
to adapt the ingredients of infant formulas made from cow’s
milk by adding probiotics and/or prebiotics to emulate the
immunological development of breastfed children. In a study
conducted in India, Saran et al. fed infants with fermented
milk for 6 months, resulting in significant weight gain and
50 % reduction of infectious diarrhea [28]. Sazawal et al.
[29] used milk fortified with B. lactis HN019 and galacto-
oligosaccharides, resulting in higher serum iron levels even
when groups received iso-caloric diets with the same iron
content, a ten percent decrease in all diarrhea types was also
observed. This effect on morbidity prevention was attributed
to a better absorption through beneficial changes in the in-
testinal flora with the side effect of preventing morbidities.
Although the majority of trials showed a positive trend in the
prevention of AID, data on evidence to support the routine
Incl
uded
Elig
ibili
tySc
reen
ing
Iden
�fica
�on
6 papers iden�fied at peer review stage and added to the review
219 records iden�fied through database searching
18 addi�onal records iden�fied through other sources
209 records a�er duplicates removed
209 abstracts screened 17 abstracts excluded:stcejbusdetalernu3
nahtrehtosegaugnalni41hsinapSrohcnerF,hsilgnE
192 full-text ar�cles assessed for eligibility
20 full-text ar�cles excluded: 3 with same pa�ents as other papers 10 with inadequate characteriza�on of the probio�c 7 with insufficient repor�ng of data for outcomes of interest
178 papers included inthe review
74 papers eligible to issue
recommenda�ons on probio�c use in
children
+
Fig. 1 Flow chart showing
papers identified and evaluated
for this review
Probiotics in Pediatric Gastroenterology 203

use of probiotics to prevent infectious diarrhea was not found
to be consistent [30]. Three major RCTs provide evidence of
a statistically significant but clinically questionable effect of
certain probiotic strains [LGG, L. reuteri-American Type
Culture Collection (ATCC) 55730, B. lactis Bb12] in the
prevention of community-acquired diarrhea [31]. No study
has suggested an adverse secondary effect of a probiotic-
enriched formula in healthy children.
5.1.2 Prevention of Nosocomial Diarrhea
In 1994, Saavedra et al. [32] reported that Streptococcus
(Str.) thermophilus and B. bifidum (renamed B. lactis) re-
duced the incidence of nosocomial diarrhea in a small group
of children admitted for an extended period in a healthcare
institute for chronic patients. Szajewska [33] showed that
LGG also reduces nosocomial infections, particularly in ro-
tavirus gastroenteritis; however, in a double-blind RCT with
220 children, Mastretta et al. [34] did not find any statistically
significant protective effect of LGG in nosocomial rotavirus
infection. In 2004, a multicenter, double-blind RCT con-
ducted by Chouraqui et al. evaluated the efficacy of a milk
formula supplemented with viable B. lactis strain Bb 12
(BbF) among 90 healthy children living in residential nurs-
eries or foster care centers; the study did not show a reduction
in prevalence of diarrhea with living B. lactis Bb12-fortified
formula compared with placebo [28.3 vs 38.7 %; relative
risk (RR) 0.7 (95 % confidence interval (CI) 0.4–1.3)] [35].
A double-blind RCT with 971 infants administered B. breve
C50 and Str. thermophilus 065 fermented formula for
4–6 months. The infants fed with the fermented formula had
normal growth and less severe episodes of diarrhea, with
fewer reports of dehydration, fewer doctor visits, and less
prescription of oral rehydration solution (ORS) [36]. The
authors concluded that seven children needed a probiotic
treatment in order to prevent healthy children from devel-
oping nosocomial rotavirus gastroenteritis. However, the
protective effect in preventing nosocomial diarrhea becomes
less significant if the incidence of episodes per patient and
per month accounts for more than the total percentage of
patients with diarrhea [37].
5.1.3 Treatment of AID
Diagnostics and therapeutics of AID must be based on the
pathophysiological consequences of the disease: water and
electrolyte loss and gastrointestinal ecosystem alteration [37].
Probiotic administration can protect intestinal micro-
biota against AID; in 2005, Shamir et al. showed a re-
duction in the duration of acute gastroenteritis from
1.96 ± 1.24 to 1.43 ± 0.71 days (p = 0.017), with the
addition of 109 colony-forming units (CFU) of Str. ther-
mophilus, B. lactis, L. acidophilus, 10 mg of zinc and 0.3 g
of fructo-oligosaccharide per day [38]. In addition, several
studies have demonstrated the efficacy of LGG in reducing
the duration of acute viral diarrhea and AID, as well as a
reduction in length of hospitalization, in both eutrophic and
severely malnourished children [39, 40]. Guarino et al. [41]
also demonstrated a significant reduction in rotavirus
shedding. In a prospective European RCT using LGG (1010
CFU/250 mL) to supplement ORS in 287 children with
acute diarrhea, the results showed a significant decrease in
the duration of diarrhea close to 10 % (mean duration of
123 h in the placebo group compared with 110 h in the
intervention group) with an improved response in the ro-
tavirus group [42]. Shornikova et al. [43] evaluated the
efficacy of L. reuteri ATCC 55730 in 66 children hospi-
talized with rotavirus diarrhea randomized into three
groups: a placebo group and two groups with different
doses of L. reuteri (107 and 1010 CFU/g once a day for
5 days). The probiotic reduced duration of diarrhea with a
dose-dependent effect (2.5 days in the placebo group vs 1.9
and 1.5 in the L. reuteri groups). In a recent meta-analysis,
Szajewska et al. [44] evaluated two RCTs (n = 196) using
L. reuteri DSM 17938 and three RCTs (n = 156) on the
evaluation of L. reuteri ATCC 55730 administration
among hospitalized children aged 3–60 months; compared
with placebo or no treatment, DSM 17938 significantly
reduced the duration of diarrhea (mean difference -32 h,
95 % confidence interval (CI) -41 to -24) and increased
the chance of cure on Day 3 (RR 3.5, 95 % CI 1.2–10.8,
random effects model). Similar results were obtained with
the original strain, L. reuteri ATCC 55730 [44].
Other probiotics such as L. acidophilus LB in a product
containing heat-killed Lactobacillus have also demon-
strated effectiveness in reducing the duration of the AID
when tested on 73 children with acute diarrhea (50 % ro-
tavirus positive) [45]. Comparable results were obtained in
a double-blind study in 87 Polish children with AID treated
with a mixture of three strains of L. rhamnosus (573L/1,
573L/2, 573L/3) all at a dose of 1.2 9 1010 CFU twice
daily for 5 days; L. rhamnosus reduced the duration of
rotavirus diarrhea (76 ± 35 h vs 115 ± 67 h (p = 0.03),
but not of other types of diarrhea [46]. Intestinal
colonization by administration with these strains was 80
Grade of Recommenda�on for the
preven�on of acute infec�ous diarrhea
by probio�c-enriched
formulas
1b for LGG, L. reuteri, B. lac�s
Grade of Recommenda�on for
preven�on of nosocomial diarrhea
1b for: B. lac�s Bb12,
S. thermophiles, B. bifidum,
and LGG
204 S. Cruchet et al.

and 41 % at 5 and 14 days, respectively. The intervention
also shortened the time required for intravenous rehydra-
tion [15 ± 14 vs 38 ± 33 h (p = 0.006)], although factors
such as the variability of care may have influenced the
result [46]. At least three clinical trials in developing
countries deny the beneficial effect of LGG and L. aci-
dophilus in acute diarrhea or severe diarrhea, probably
related to the difference in etiological profile [47–49]. No
decrease in the duration of diarrhea with a mixture of L.
acidophilus, B. bifidum (B. lactis) and L. bulgaricus was
observed [50]. The strain L. paracasei ST11 did not reduce
the volume of stool in rotavirus infection but improved the
results of cumulative stool output (225 ± 218 vs 381 ±
240 mL/kg), stool frequency (27.9 ± 17 vs 42.5 ± 26), and
ORS intake (180 ± 207 vs 331 ± 236 mL/kg) in children
with less severe non-rotavirus diarrhea compared with
those receiving placebo treatment in Bangladeshi children
[51]. Two meta-analyses concluded that most of the studies
were conducted in the developed world, and that LGG, L.
acidophilus and L. bulgaricus had no efficacy [52, 53]. In
an SR of double blind RCTs, Szajewska and Mrukowicz
also found that the duration of viral diarrhea was sig-
nificantly reduced (by about 17 h or 0.7 days) compared
with controls [54]. The effectiveness of LGG appears to be
connected to the logarithm of the dose ([1011 as the most
effective dose) [53]. A Cochrane review of 63 RCTs and
8014 participants (56 trials recruited infants and young
children) showed the beneficial effect of probiotics in
combination therapy with ORS in reducing the duration of
diarrhea, although the size of the effect varied considerably
between studies [55]. The average of the effect was sig-
nificant for mean duration (MD) of diarrhea (MD 24.76 h;
95 % CI 15.9–33.6; n = 4,555, 35 trials); diarrhea lasting
C4 days (RR 0.41; 95 % CI 0.32–0.53; n = 2,853, 29
trials); and stool frequency on Day 2 (MD 0.80; 95 % CI
0.45–1.14; n = 2,751, 20 trials). The two most commonly
studied probiotics were LGG (13 RCTs) and S. boulardii
(10 RCTs) [55]. The first double-blind, prospective, ran-
domized study of S. boulardii (a non-pathogenic yeast) was
completed over 15 years ago: diarrhea persisted for more
than 7 days in 12 % of the placebo group and in 3 % of the
probiotic group [56]. Since then, several other double-
blind, prospective randomized trials conducted on S. bou-
lardii in children with acute gastroenteritis have consis-
tently shown a significant improvement compared with
placebo. A consecutive series of 130 Mexican children
with AID from 3 months to 3-years-old were treated with
ORS plus placebo or with ORS plus S. boulardii
600 mg/day for 5 days. A significant decrease in the
number of stools occurred from the second day following
probiotic use. After 48 h, the percentage of children con-
sidered cured was almost 50 % (vs 8 % in the placebo
group) and, at Day 4, the percentage cured was up to 95 %
(vs 50 % in the placebo group) [57]. Kurugol and Koturoglu
[58] treated 200 children with acute diarrhea with 250 mg of
S. boulardii or placebo for 5 days: the duration of diarrhea
and length of hospitalization was reduced by about 24 h.
Villarruel and colleagues [59] showed similar results in 88
children treated in ambulatory care in Argentina. This study
concluded that diarrhea persisted for more than 7 days in
27 % of the control group, compared with 7 % of the group
treated with S. boulardii for 6 days, with a greater effect if
treatment was initiated during the first 2 days of diarrhea. In
addition, studies of diarrheal parasitic infections showed that
S. boulardii improved feeding tolerance in children with
chronic Giardia lamblia [60]. This probiotic is also shown to
be effective in amoebiasis and AIDS-associated diarrhea
[61, 62]. An open RCT in Pakistani children with acute
infectious gastroenteritis demonstrated that administration of
500 mg of S. boulardii for 5 days significantly reduced stool
frequency and duration of diarrhea (3.5 vs 4.8 days,
p = 0.001) and resulted, 2 months later, in a 50 % decrease
in re-infection rate with a 30 % bodyweight increase [63].
More recently, two international guidelines on diarrheal
management in children addressed the use of probiotics in
acute diarrhea with ORS; experts concluded that LGG and
S. boulardii reduced the duration of diarrhea by 1 day,
giving evidence level 1? for these two probiotics only [64,
65]. Finally, the Probiotics and Prebiotics Global Guideli-
nes published by the World Gastroenterology Organization
(WGO) in 2011 confirmed the use of the above-mentioned
probiotics in the management of children with acute diar-
rhea with ORS, level of evidence 1a for the same probiotics
only [66].
Regarding the treatment of AID in children, the
LATAM consensus estimates that a decrease in the dura-
tion of diarrhea, as well as hospitalization length, is an
important benefit from the standpoint of social and eco-
nomic development in acute infectious gastroenteritis in
children. While there have been numerous published clin-
ical studies evaluating different probiotics in the treatment
of acute gastroenteritis, tests differ in relation to the strains
tested, dosages, methodological quality, definitions of di-
arrhea and the results obtained. Most studies show statis-
tically significant effects in terms of clinical benefit, with
greater effect on viral diarrhea [31]. In general, published
meta-analyses conclude that the duration of diarrhea epi-
sodes is shortened by approximately 24 h (17–30 h) with
the selected strains of lactobacilli and LGG, L. acidophilus,
L. bulgaricus, L. reuteri, and S. boulardii [31, 33, 52, 54,
55, 67]. In addition, studies have proven the increased ef-
fectiveness of probiotics when they were administered in
the early stages of the disease; in at least three studies in
children with acute diarrhea of different etiologies, probi-
otic use reduced the average duration of episodes by 57 %
(35–71 %) [44, 64, 68]. Only LGG and S. boulardii have
Probiotics in Pediatric Gastroenterology 205

Evidence Level 1? for the treatment of acute diarrhea with
ORS in children [64–66]. In developing countries, for va-
rieties of lactobacilli, we found few study-based assays in
the community while we observed sufficient data on S.
boulardii.
5.2 Antibiotic-Associated Diarrhea (AAD)
Antibiotic treatment alters the gastrointestinal microflora,
which produces various clinical symptoms, particularly di-
arrhea. AAD incidence in children is approximately 10 % in
first-line treatment, regardless of the reason for antibiotic
administration [69]; children under 2 years of age are more
likely to experience an episode of AAD, especially those
treated with antibiotics or antibiotic combinations such as
amoxillin–clavulanic acid (23 %) [70]. Nevertheless, the
large majority of AAD cases are mild to moderate and rarely
require hospitalization. According to the meta-analysis
performed by Szajeweska in 2006, probiotics reduce the risk
of AAD in children. Analysis of subgroups of children to
whom probiotics were administered preventively showed
that reduction in AAD risk was mainly associated with the
use of LGG (95 % CI 0.15–0.6), S. boulardii (95 % CI
0.07–0.6), or B. lactis and Str. thermophilus (95 % CI
0.3–0.95) [70]. These data indicated that one of seven pa-
tients who develop diarrhea during antibiotic treatment
would benefit from AAD prevention if they were to simul-
taneously receive any of these probiotics.
The use of S. boulardii has proven to be the only ef-
fective method of preventing diarrhea caused by C. difficile
[71]. Randomized controlled trials provide moderate evi-
dence of a beneficial effect produced by LGG, B. lactis, Str.
thermophilus and S. boulardii. Nonetheless, there is no
evidence to support the use of probiotics in the prevention
of recurring symptoms caused by C. difficile [31].
Potential effects of probiotics in preventing AAD in
children require more studies for routine indication. Such
studies should focus on probiotic strains that have proved
to be beneficial such as LGG, or S. boulardii, as well as on
dosages that have showed to be more effective. There are
not enough publications on treating children with severe
AAD with probiotics.
5.3 Traveler’s Diarrhea
The past two decades have seen an unprecedented, sus-
tained growth in international travel. Although much of the
growth represents increased travel to Europe and Asia,
travel to South America has also increased. Traveler’s di-
arrhea is a common condition with major economic and
health impacts. In traveling children, the etiologies of di-
arrhea are likely to be similar to those described for diar-
rhea in adults [71, 72]. Children who travel are at risk of
developing the same well known illnesses that affect adult
travelers [73]. In the assessment of the ill pediatric traveler,
physicians must consider geographic, seasonal, and envi-
ronmental factors and assess compliance to pre-travel ad-
vice. Treatment recommendations for pediatric traveler’s
diarrhea have come from expert opinion, anecdotal evi-
dence, limited case reports, the World Health Organization,
The Medical Letter [71, 72] and extrapolation from treat-
ment recommendations for traveler’s diarrhea in adults
[73].
Various randomized clinical studies have evaluated the
efficacy of probiotics in the prevention of this medical
condition. One trial using L. acidophilus and two other
trials using LGG showed negative results [74–76]. An RCT
using S. boulardii illustrated a significantly beneficial ef-
fect in terms of reduced incidence of diarrhea, which was
shown to be dose dependent, strongly dependent on ad-
herence, and which tended to differ according to geo-
graphical location [77].
According to Mackell [73], the best treatment choice for
the pediatric traveler must address a combination of effi-
cacy, adherence, and cost.
5.4 Helicobacter pylori Infection
Current interest in probiotics as therapeutic agents against
H. pylori is stimulated not only by the clinical data
showing efficacy of some probiotics in different gastroin-
testinal diseases but also by the increasing resistance of
pathogenic bacteria to antibiotics, thus the interest in de-
veloping alternative therapies. Several clinical trials have
evaluated the role of probiotics in adults and children
colonized with H. pylori. Studies on L. johnsonii, S. bou-
lardii ± inulin or L. acidophilus LB and L. gasseri
OLL2716 (LG21) indicate that they decrease colonization
density, while maintaining lower levels of the pathogen in
the gastric mucosa but that they do not eradicate H. pylori
[78–80]. However, in some studies with probiotics
Grade of Recommenda�on for
preven�on of an�bio�c-associated
diarrhea
1b for LGG and S. boulardii
Grade of Recommenda�on
for treatment of
acute infec�ous diarrhea
1a for LGG, and S. boulardii
1b for L. reuteri
Grade of Recommenda�on for
preven�on of traveler’s diarrhea
1b for S. boulardii
206 S. Cruchet et al.

combined with treatment regimens using proton pump in-
hibitors (PPIs) and antibiotics, eradication rates moderately
increased. For LGG the eradication rate was 69 % (0.98
RR, 95 % CI 0.7–1.4) [81], for L casei DN-114 001 it was
84.6 % (95 % CI 71.2–95.5) vs 57.5 % in the control group
(p = 0.0045) [82], for B. animalis and L. casei it was 45.5
vs 37.5 % with control (p = 0.345) [83], for L. reuteri
ATCC 55730 85 vs 80 % with control (p[ 0.05) [84], for
a supplement containing L. casei DN-114001, L. bul-
garicus, and S. thermophilus, eradiation rates were 88.5 vs
51.5 % with no supplementation (p\ 0.01) [85], and a
study using S. boulardii showed an eradication rate of 93.3
vs 80.9 % with control (p = 0.750) [86].
Finally, the same studies evaluated the occurrence of
adverse events during treatment and observed a non-sig-
nificant decrease in symptoms. Only the open trial by
Hurduc and collaborators showed that the incidence of side
effects was significantly reduced in the S. boulardii group:
30.9 % in the control vs 8.3 % in the probiotic group
(p = 0.047) [86].
In conclusion, there is currently a lack of sufficient
evidence to recommend the use of probiotics in this area.
5.5 Infant Colic
Infantile colic consists of repeated distress periods of irri-
tability and crying for indiscernible reasons for more than
3 h a day, 3 days a week and for 3 weeks or more [87]. It
affects between 5 and 19 % of newborns and infants in the
first months of life and creates a frustrating situation for
parents and caregivers. The following differential diag-
noses should be considered: cow’s milk protein allergy,
gastro-esophageal reflux disease, intestinal hypermotility,
and hormonal problems [88].
Despite the fact that some experiments have been per-
formed with simeticone [89] and home remedies [90–93] have
attempted to resolve this common problem, at the moment, no
treatment has proven to be fully effective. Medical literature
provides one SR [94] and eight randomized, double-blind,
controlled studies using probiotics, seven of them with L.
reuteriDSM 17938 in nursing infants [95–101] and a sixth one
with formulas supplemented with two different probiotic
strains, B lactis and Str. thermophiles [102].
The SR and published RCTs show that administration of
L. reuteri DSM 17938 led to improved infantile colic
symptoms in comparison with simeticone in exclusively
breastfed children [94–101]. The included trials were
supported by the manufacturer of the probiotic strain under
study, which raises the possibility of bias; however, the
likelihood is small since the trials were fully investigator-
initiated and data controlled with transparent disclosure of
potential conflicts of interest by the respective authors.
The RCT published in 2010 by Savino and colleagues [97]
showed that L. reuteri DSM 17938 improved symptoms of
infantile colic—as shown by a greater proportion of early
breastfed infants with C50 % reduction in crying time from
baseline vs placebo at Days 7 (p = 0.006), 14 (p = 0.007)
and 21 (p = 0.036)—and was well tolerated. More recently,
Sung and colleagues described a large, well designed RCT of
L. reuteri for the management of infant colic in a broad
community of breastfed and formula-fed infants in Australia
[101]. In total, 167 breastfed infants were randomized to
receiveL. reuteri or placebo. At multiple follow-up intervals,
the authors found no improvement in the duration of crying
time in infants who received probiotic compared with
placebo, in fact, infants receiving the studied probiotic cried
significantly more [101].
In the earlier study [97], breastfeeding mothers were
required to avoid cow’s milk, while the study by Sung et al.
[101] did not have this requirement, so environmental
factors may have played a role in the differences in out-
comes between these two studies. Furthermore, the later
study excluded infants with colic due to cow’s milk protein
allergy and included infants treated with PPIs [101]. In-
deed, 21 subjects in the probiotics group and 24 in the
placebo group received PPIs and so may have been suf-
fering from gastroesophageal reflux and not infantile colic.
Therefore, the lack of significant difference between the
two groups in the study by Sung et al. could be due to
undeclared allocation bias. Recruiting infants treated with
concomitant drugs (such as PPIs) and dietary approaches
(probiotic and hypoallergenic formulas) introduced con-
founding factors that needed to be evaluated individually in
order to perform an appropriate multivariate regression
analysis and to distinguish the effects of the tested probi-
otic from those of the drugs.
Evidence supporting the prophylactic use of L. reuteri
DSM 17938 during the first 3 months of life was shown by
Indrio et al. in an RCT investigating the prophylactic use of
L. reuteri DSM 17938 to prevent onset of functional gas-
trointestinal disorders, showing a reduction in the onset of
daily crying time, regurgitation, and constipation [100].
One well recognized limitation of all the studies of in-
fant colic is the need for a more objective way of mea-
suring duration of crying rather than relying on the parents’
compliance to establish this outcome. The Saavedra et al.
study [102] showed that supplementing formulas with B.
lactis and Str. thermophilus was well tolerated and de-
creased colic episodes in children, possibly by modifying
patterns of fermentation, which leads to less gas or water
formation, which in turn may affect gastrointestinal toler-
ance, although this remains speculative.
Grade of Recommenda�on for
eradica�on of H. pylori
Not recommended
Probiotics in Pediatric Gastroenterology 207

In addition to clinical effects, use of L. reuteri DSM
17938 was associated with decreased private and public
costs for the management of this condition [100].
5.6 Necrotizing Enterocolitis (NEC)
NEC is the most common gastrointestinal emergency in
newborns and a major cause of morbidity and mortality in
preterm infants [103], especially in those with very low birth
weight (VLBW)\1500 g [104, 105]. Incidence of NEC is
variable depending on countries and neonatal care units.
Recently there has been increasing interest in testing the
potential benefits of probiotics in preterm infants in terms
of preventing NEC [106]. The mechanisms by which pro-
biotics may protect infants at high risk of developing NEC
and/or sepsis include providing a barrier preventing the
migration of bacteria and their products through the mu-
cosa [107, 108], the competitive exclusion of potential
pathogens [109], the modification of the host response to
microbial products [110], the increased response of the
mucosal IgA, the improvement of enteral nutrition, which
inhibits pathogen growth and stimulation of immune re-
sponses while regulating TLRs, the nuclear jB factor and
inflammatory cytokine production [111, 112].
Four meta-analyses on administration of probiotics to
newborns with VLBW have been published [104, 113–
115]. Deshpande et al. observed that with gestational age
under 33 weeks there was a lower risk of mortality of any
origin and of NEC by 53 and 64 %, respectively, in new-
borns who received probiotics, when compared with a
control group [104]. The risk of sepsis did not differ sig-
nificantly between groups. Additionally, the Cochrane re-
view [113] reported that enteral supplementation of certain
probiotics reduced the risk of NEC and mortality in pre-
term infants weighing less than 1500 g with no evidence of
significant reduction of nosocomial sepsis. However, both
of these meta-analyses have shown that not all probiotics
tested were equally effective. The combinations used in the
meta-analyses by Bin-Nun et al. [114] (B. infantis plus Str.
thermophilus plus B. bifidus) and Lin et al. [115] (L. aci-
dophilus plus B. infantis) were the most effective [116].
Alfaleh et al. reached the same conclusions but the re-
sults cannot be extrapolated to newborns weighing
\1000 g because of lack of data in this high-risk group
[116, 117]. The more recent meta-analysis published by
Deshpande et al. in 2010 includes four new RCTs
(n = 783), in relation to the one published in 2007 by the
same author, one of them being a multicenter study [118].
The analysis revealed a highly statistically significant de-
crease in the risk of severe NEC and death (p\ 0.00001)
[104]. The strains evaluated were B. breve, S. boulardii,
mixtures of Bifidobacterium and Streptococcus, LGG, and
L. acidophilus. In addition, among all studies, the use of
probiotics was described as safe and well tolerated [104,
113–115].
Another study showed that the prophylactic use of L.
reuteri resulted in a statistically significant reduction in
rates of NEC in children: NEC decreased 15.1 to 2.5 %
(p = 0.0475), the need for surgery or death due to NEC
was reduced from 8.2 to 2.5 % (p = 0.1774), and no ad-
verse events related to the use of L. reuteri were reported
[119].
In conclusion, the use of probiotics significantly reduces
the risk of severe forms of NEC and death. Further studies
are needed to answer important questions such as dose,
strain, more efficient forms of administration and long-term
safety for use in patients at risk of NEC.
5.7 Inflammatory Bowel Disease (IBD)
The concept of dysbiosis, an imbalance between ‘protec-
tive’ and ‘harmful’ intestinal bacteria, is gaining credibility
among multiple etiologic factors of IBD. Nowadays, the
rationale for administering strains of live ‘beneficial’ bac-
teria for IBD is based largely on the premise of dysbiosis.
The most important attribute that makes probiotics ap-
pealing for use in IBD is their ability to regulate the host
mucosal immune response, since it is well known that
immune and epithelial cells of the small intestine can
discriminate between various microorganisms through the
activation of TLRs [120].
Many in vitro and animal studies favor this hypothesis.
The literature published on adults emphasizes the role of
probiotics in maintaining remission of IBD, especially in
pouchitis [121]. A 2-year follow-up study on LGG ad-
ministration was performed in children with Crohn’s dis-
ease in remission and resulted in a decreased relapse rate of
31 % in the probiotic group vs 17 % in the placebo group
with non-significant statistical difference. There was also
no difference in the duration of time until relapse [122].
Grade of Recommenda�on
for infan�le colic
Colic preven�on: 1a for
L. reuteri DSM 17938
Colic treatment: 1b for
L. reuteri DSM 17938
Grade of Recommenda�on
for preven�on of necro�zing enterocoli�s
1a for B. breve, mixtures of
Bifidobacterium and
Streptococcus, LGG,
L. acidophilus and L. reuteri DSM
17938
208 S. Cruchet et al.

However, despite a lack of evidence regarding any benefits,
almost 80 % of children affected by IBD regularly con-
sume probiotics [123]. In a randomized pilot study on the
induction and maintenance of remission in children with
ulcerative colitis, the proprietary preparation VSL#3 (a
high-concentration mixture of probiotic bacterial strains)
has been found to be as effective as adjuvant therapy, both
in inducing and maintaining remission [124].
Although the incidence of pouchitis among Latin
American children is increasing, our group did not find
sufficient evidence in the literature among the pediatric
population to give a recommendation on this pediatric
indication.
5.8 Functional Gastrointestinal Disorders: Irritable
Bowel Syndrome (IBS)
Functional gastrointestinal disorders are among society’s
most common conditions, affecting millions of people of
all ages, including children. At any one time, ap-
proximately two out of five persons will be affected by a
functional gastrointestinal disorder. Furthermore, as
gastrointestinal disorders often overlap, many patients
could be affected by more than one functional gas-
trointestinal disorder simultaneously [125]. In the criteria
for the definition of functional gastrointestinal disor-
ders—the Rome III [126] consensus process 2006—the
disorders are grouped by type of chronic or recurrent
symptoms of functional origin. IBS is a functional gas-
trointestinal disorder characterized by abdominal dis-
comfort or pain associated with defecation or change in
bowel habits in absence of organic disease. IBS patho-
genesis is multi-factorial and involves altered reactivity
with increased intestinal motility and secretion with in-
traluminal stimuli such as food, inflammation, bacteria,
or extra-intestinal elements such as emotional factors.
IBS can also be linked to associated mechanisms such as
lactose intolerance, fructose, malabsorption of biliary
salts, bacterial overgrowth, and increased short-chain
fatty acids [127]. There is no curative treatment for IBS,
but symptom relief and periods of remission are
achievable. Probiotics reduce the manifestations of
functional disorders through modification of enzymatic
and metabolic function. Studies have shown the efficacy
of probiotics in IBS in adults but data in children are
limited. Two studies in children with LGG showed
controversial results. A 6-week RCT of LGG compared
with placebo undertaken by Bausserman and Michail
[128] showed negative results in 50 children and young
adults (aged 6–20 years). Conversely, in another RCT
with 37 participants, those in the LGG group were more
likely to have treatment success than those in the
placebo group and had reduced frequency of pain
(p = 0.02), but not severity of pain [129]. Finally,
Guandalini et al. [130] studied 59 children and con-
cluded that VSL#3 is safe and more effective than
placebo in ameliorating symptoms and improving quality
of life in children affected by IBS.
5.9 Constipation
Probiotics alter the composition of the feces of healthy
individuals. Only one randomized trial has been completed
for children with constipation; the addition of LGG to
lactulose as standard treatment offered no additional ben-
efit [131]. More recently, a systemic evaluation and up-
dated evidence on the efficacy and safety of probiotic
supplementation for the treatment of constipation was
performed in 2010 by Chmielewska and Szajewska [132].
The authors concluded that the scarce amount of data
published to date do not yet provide sufficient scientific
evidence to support a general recommendation about the
use of probiotics for treatment of functional constipation.
In the absence of new available data on the use of probi-
otics, the authors concluded that the use of probiotics for
this condition should be considered investigational.
5.10 Allergy
Much of the literature on probiotics and allergy origi-
nates from Finland. Several publications report sig-
nificant reductions in the SCORing Atopic Dermatitis
(SCORAD) score with administration of B. lactis BB-12
and LGG ATCC 53103 [133, 134]. Perinatal adminis-
tration of LGG ATCC 53103 leads to decreased atopic
eczema, even up to the age of 7 years [135, 136]. Si-
multaneous treatment with pre- and probiotics (a mixture
of four strains and galacto-oligosaccharides) adminis-
tered to pregnant women for 2–4 weeks before delivery
Grade of Recommenda�on for improving
symptoms of irritable bowel syndrome
2c for LGG and VSL#3
Grade of Recommenda�on for
Ulcera�ve coli�s
Pouchi�s
Crohn's disease
1b for VSL#3
Not recommended
Not recommended
Grade of Recommenda�on for
cons�pa�on
Not recommended
Probiotics in Pediatric Gastroenterology 209

and to children over 6 months showed no effect on the
cumulative incidence of allergic diseases at the age of
2 years compared with placebo, but tended to reduce
disease associated with allergic reactions, and a sig-
nificant reduction in atopic eczema was observed [137].
Taylor and colleagues [138], however, questioned the
role of probiotics in allergy prevention, and reported that
early supplementation with L. acidophilus did not reduce
the risk of atopic dermatitis (AD) in infants at high risk
and was even associated with increased allergic sensi-
tivity in children. The pathogenesis of AD seems to in-
volve deterioration of the intestinal barrier, considering
that supplementation with probiotics can stabilize said
function and reduce gastrointestinal symptoms in chil-
dren with AD [139]. However, the composition of the
intestinal microbiota in children with atopic eczema and
dermatitis syndrome with and without food allergy was
similar. As a result, there is no conclusive evidence re-
garding the role of the intestinal microbiota in relation to
the development of infant food allergy in children with
atopic eczema [140]. Moreover, the data from Brouwer
et al. [141] shows that neither L. rhamnosus nor LGG
had influence on the SCORAD score, sensitization, in-
flammatory parameters or cytokine production. The data
on probiotics and allergy need further clarification, as
the positive data are reported by different groups from
Finland, but have not been confirmed by others—prob-
ably because of geographic or genetic differences play-
ing a detrimental role among this population. In at least
one study, L. rhamnosus and B. lactis improved only
children sensitized to food, suggesting a genetic influ-
ence on the efficacy of probiotics in these children [142].
Treatment with LGG has been shown to reduce the in-
tensity of atopic eczema and symptoms of hyper-IgE
dermatitis syndrome but not in IgE-sensitized children
[143]. Rosenfeldt et al. [144] showed that a combination
of L rhamnosus 19070-2 and L. reuteri DSM 122460
was beneficial in the treatment of AD. The effect was
more pronounced in patients with positive skin test re-
sponse and increased levels of IgE [141]. By 1997, it
had been suggested that probiotic bacteria may encour-
age endogenous barrier mechanisms in patients with AD
and food allergy, and by reducing intestinal inflamma-
tion, may act as a useful tool in the treatment of food
allergy [133]. However, authors of the latest Cochrane
review concluded that there was inconclusive evidence
for giving prebiotics to prevent allergic disorders in in-
fants [145].
6 Probiotics in Marketed Products and Infant
Formulas
There are an increasing number of probiotics emerging in a
variety of distribution channels, especially in internet-
based sales. At the same time, one of the main issues
concerns the quality control and safety of these products
commercialized in the market. In other words, there are
more and more supplements with scarce scientific evidence
of their medicinal potency, no or little control of their
composition, no control of their shelf-life, and no knowl-
edge of side effects or supplement–drug interactions [146].
The food industry uses microbial supplements, mainly in
milk or yogurt drinks. Some of these microbial supple-
ments are also sold in capsules, increasingly blurring the
line between food and drug. Some probiotics claiming
health benefits in dairy foods have been well documented,
after identifying and isolating their microorganisms. One
study identified mislabeling in 47 % of dietary supple-
ments and 40 % milk products tested [147]. The poor la-
beling of dietary supplements is a global problem [148].
In the case of all marketed probiotics and formulas,
investigations into the mechanism of action of specific
strains should be mandatory along with conducting clinical
studies on these products since the in vitro effects of a
strain may be contrary to those observed in vivo [149]. The
effects demonstrated with one strain cannot be extrapolated
to another, even if they belong to the same species. Only a
specific strain and its commercially ‘controlled’ product for
which convincing data are available should be recom-
mended for medical use.
Probiotic bacterial strains include lactobacilli (LGG, L.
reuteri, L. johnsonii) [150] and bifidobacteria (B. lactis Bb
12), as well as strains of Escherichia coli (E. coli Nissle
1917) [151] and certain enterococci strains (although this
agent has been linked to the transfer of resistance encoded
and transmitted by plasmids) [152].
L. acidophilus LB has shown antibacterial activity
against E. coli. However, if E. coli is present in the gas-
trointestinal tract of the host before L. acidophilus LB is
administered, like in the case of acute gastroenteritis, their
antibacterial activity can be strongly reduced [153]. Ad-
hesion of Bifidobacteria Bb 12 improves in the presence of
LGG, both in healthy children and during episodes of di-
arrhea, suggesting synergy between the two strains [154].
To date, few publications on the clinical effects of
probiotic supplementation in infant formulas, follow-up
formulas, and special medical foods have addressed this
subject. It should be noted that some studies describe an
adequate safety profile and studies also report that the use
of probiotic supplementation does not affect infant growth
[155–157]. Yet, although evidence on the benefits in NEC,
treatment and prevention of AID, AAD, and atopy and
Grade of Recommenda�on for allergy Evidence inconclusive, insufficient
Not recommended
210 S. Cruchet et al.

allergy have been published, it must be stressed that these
benefits are rare and strain-specific, and thus conclusions
are limited until more scientific data become available—a
situation that prevents us from drawing definitive conclu-
sions on the subject.
7 Safety and Side Effects
Probiotics are considered ‘generally recognized as safe’
(GRAS) and well tolerated in humans. The most common
adverse effects include bloating and flatulence; however,
these are typically mild and subside with continued use
[158]. One theoretical concern associated with probiotics
includes the potential for these viable organisms to move
from the gastrointestinal tract and cause systemic infec-
tions. Although rare, probiotic-related bacteremia and
fungemia have been reported, particularly in neonates
[159–163]. It is estimated that the risk of developing bac-
teremia from ingested lactobacilli probiotics is \1 per 1
million users [164], and the risk of developing fungemia
from S. boulardii is estimated at 1 per 5.6 million users
[165].
Large-scale epidemiological studies on probiotic use in
countries where their use is widespread show low rates of
systemic infection between 0.05 and 0.40 % [166]. Of all
documented invasive infections, most of them occur
mainly in immune-compromised adults [164].
Lactobacilli have caused cases of sepsis, meningitis,
and infections in other organs in adults [167, 168]; how-
ever, invasive infections in infants and children are ex-
tremely rare [164]. Nevertheless, bacteremia has been
attributed to Lactobacillus supplementation in children
[169] and in neonates [160, 161, 163]. In a review,
Enache-Angoulvant and Hennequin found evidence of
sepsis in children with short bowel syndrome treated with
Lactobacillus and S. boulardii-related fungemia was re-
ported in about 50 patients, with central venous
catheterization as the main risk factor [170]. Fungemia
was also observed in patients with a central venous
catheter hospitalized in beds adjacent to patients treated
with the yeast [171]. There were no reports of probiotic
translocation from the gastrointestinal tract into the sys-
temic circulation. Fungemia has also been reported with
S. cerevisiae in two newborns, one of whom was being
treated with the agent and the other contracted the fun-
gemia from the first [162]. These cases highlight that
probiotic supplementation should be used with caution in
children with central catheters and those with known or
potentially compromised intestinal mucosal integrity or
those with underdeveloped immune systems.
To minimize the risk of side effects such as bacteremia
and fungemia, studies may be performed using non-viable
or inactivated preparations. These modified probiotic
preparations may be the best choice in high-risk situations.
The effects of these agents may go beyond the gastroin-
testinal tract to distant areas, such as the urogenital and
respiratory mucosa, and it may not be necessary to ad-
minister intact probiotic organisms to achieve benefits. At
basic research level, probiotic products such as secreted
proteins or DNA can block inflammation and prevent death
of intestinal epithelial cells [172].
8 Limitations
Among the seventy-four studies that met our inclusion
criteria and were included in the recommendations, the
quality varied and almost all of the included trials had
methodological limitations. The most common problems
were lack of description of randomization procedures and
group allocation and blinding. In general terms, individual
publication bias was not evaluated by our reviewers.
9 Conclusions
Probiotics have demonstrated efficacy in preventing and
treating various medical conditions, particularly those in-
volving the gastrointestinal tract in children. In addition,
probiotics are a helpful tool in specific infectious, inflam-
matory and functional disorders, but it is important to note
that evidence indicates strain specificity in each case.
Certain probiotics have been widely used for a variety of
disorders and data supports their increased use. Available
literature shows a statistically significant benefit in de-
creasing intensity, duration and number of consultations for
acute gastroenteritis caused by various infectious agents,
mostly viral and parasitic-related illnesses, when specific
probiotics are combined with ORS.
LGG, L. reuteri and S. boulardii are the best studied
probiotics. Some lactobacilli strains and S. boulardii have
proven to be most effective if treatment is introduced early.
Another particular application is NEC, where probiotics B.
breve, and specific mixtures of Bifidobacterium, Strepto-
coccus, and Lactobacillus strains significantly reduce the
risk of severe forms and associated mortality.
Due to strain specificity, only clinically tested probiotics
can be recommended to treat pediatric patients.
Acknowledgments Dr. Maruy acknowledges consulting honoraria
from Biocodex. None of the other authors have competing interests.
Grade of Recommenda�on
for marketed products and infant formulas
Evidence insufficient
Probiotics in Pediatric Gastroenterology 211

Editorial assistance—editing and styling the manuscript in prepa-
ration for submission and assistance with post-submission revisions—
was provided by Mary Hines of Springer Healthcare and funded by
Biocodex.
Conflicts of interest The Advisory Committee of the Latin-Amer-
ican (LATAM) expert consensus group coordinated the development
of this Consensus Statement with an unrestricted grant from Bioco-
dex. The opinions expressed in this Consensus Statement represent
only those of the Advisory Committee.
Open Access This article is distributed under the terms of the
Creative Commons Attribution Noncommercial License which per-
mits any noncommercial use, distribution, and reproduction in any
medium, provided the original author(s) and the source are credited.
References
1. Guyatt GH, et al. GRADE: an emerging consensus on rating
quality of evidence and strength of recommendations. BMJ.
2008;336:924–6.
2. Jaeschke R, et al. Users’ guides to the medical literature. III.
How to use an article about a diagnostic test. A. Are the results
of the study valid? Evidence-Based Medicine Working Group.
JAMA. 1994;271:389–91.
3. Laupacis A, et al. Users’ guides to the medical literature.
V. How to use an article about prognosis. Evidence-Based
Medicine Working Group. JAMA. 1994;272:234–7.
4. Levine M, et al. Users’ guides to the medical literature. IV. How
to use an article about harm. Evidence-Based Medicine Working
Group. JAMA. 1994;271:1615–9.
5. Oxman AD, et al. Users’ guides to the medical literature. VI.
How to use an overview. Evidence-Based Medicine Working
Group. JAMA. 1994;272:1367–71.
6. CEBM. Oxford Centre for Evidence-Based Medicine—levels of
evidence. Centre for Evidence-Based Medicine. 2009. http://
www.cebm.net/oxford-centre-evidence-based-medicine-levels-
evidence-march-2009/. Accessed 15 July 2014.
7. FAO/WHO. Working group on drafting guidelines for the
evaluation of probiotics in food. Guidelines for the evaluation of
probiotics in food. 2002. ftp://ftp.fao.org/es/esn/food/wgreport2.
pdf. Accessed 2 Sept 2010.
8. Huff BA. Caveat emptor. ‘‘Probiotics’’ might not be what they
seem. Can Fam Physician. 2004;50:583–7.
9. Lilly DM, Stillwell RH. Probiotics: growth-promoting factors
produced by microorganisms. Science. 1965;147:747–8.
10. Parker RB. Probiotics, the other half of the antibiotic story.
Animal Nutr Health. 1974;29:4–8.
11. Tissier H. Tritement des infections intestinales par la methode
de translormation de la flore bacterienne de l’intestin. C R Soc
Biol. 1906;60:359–61.
12. FAO/WHO. Joint FAO/WHO expert consultation on evaluation
of health and nutritional properties of probiotics in food. 2001.
ftp://ftp.fao.org/docrep/fao/009/a0512e/a0512e00.pdf. Accessed
2 Sept 2010.
13. Czerucka D, et al. Review article: yeast as probiotics—Sac-
charomyces boulardii. Aliment Pharmacol Ther. 2007;26:
767–78.
14. Lajolo F. Alimentos funcionales: Aspectos Cientıficos y
Regulatorios. Dieta y Salud. 2003;10:2–7.
15. ANMAT. Alimentos Funcionales Probioticos. 2010. http://
www.anmat.gov.ar/consumidores/alimentos/Alimentos_Funcion
ales_Probioticos.pdf. Accessed 30 Oct 2014.
16. Elmer GW, et al. Biotherapeutic agents. A neglected modality
for the treatment and prevention of selected intestinal and
vaginal infections. JAMA. 1996;275:870–6.
17. Gorbach SL. Prebioticos y lacteos fermentados: sus beneficios
para la salud. Infect Dis Clin Pract Esp. 1995;3:2–7.
18. Henriquez Moya M, Moreno C. Probioticos: Legislacion en
Marcha. Direccion Nacional de Alimentos. Secretaria de Agri-
cultura, Ganaderıa, Pesca y Alimentos. 2009. http://www.alimen
tosargentinos.gov.ar/0-3/revistas/r_39/articulos/Probioticos.htm.
Accessed 2 Sept 2010.
19. WGO. Probioticos y Prebioticos. World Gastroenterology Or-
ganisation. 2008. http://www.worldgastroenterology.org/assets/
downloads/es/pdf/guidelines/19_probioticos_prebioticos_es.pdf.
Accessed 2 Sept 2010.
20. Borchers AT, et al. Probiotics and immunity. J Gastroenterol.
2009;44:26–46.
21. Indriyani S. Effects of live versus heat-killed probiotics on acute
diarrhea in young children. Indriyani Paediatr Indones.
2012;52:249–54.
22. Chen X, et al. Saccharomyces boulardii inhibits ERK1/2 mito-
gen-activated protein kinase activation both in vitro and in vivo
and protects against Clostridium difficile toxin A-induced en-
teritis. J Biol Chem. 2006;281:24449–54.
23. Lutgendorff F, et al. The role of microbiota and probiotics in
stress-induced gastro-intestinal damage. Curr Mol Med.
2008;8:282–98.
24. Donkor ON, et al. Cytokine profile and induction of T helpertype 17 and regulatory T cells by human peripheral mononuclear
cells after microbial exposure. Clin Exp Immunol.
2012;167:282–95.
25. Guarino A, et al. Probiotics as prevention and treatment for
diarrhea. Curr Opin Gastroenterol. 2009;25:18–23.
26. Kaila M, et al. A prospective study of humoral immune re-
sponses to cow milk antigens in the first year of life. Pediatr
Allergy Immunol. 1994;5:164–9.
27. McFarland LV. Systematic review and meta-analysis of Sac-
charomyces boulardii in adult patients. World J Gastroenterol.
2010;16:2202–22.
28. Saran S, et al. Use of fermented foods to combat stunting and
failure to thrive. Nutrition. 2002;18:393–6.
29. Sazawal S, et al. Efficacy of milk fortified with a probiotic
Bifidobacterium lactis (DR-10TM) and prebiotic galacto-
oligosaccharides in prevention of morbidity and on nutritional
status. Asia Pac J Clin Nutr. 2004;13:S28.
30. Agostoni C, et al. Probiotic bacteria in dietetic products for
infants: a commentary by the ESPGHAN Committee on Nutri-
tion. J Pediatr Gastroenterol Nutr. 2004;38:365–74.
31. Szajewska H, et al. Probiotics in gastrointestinal diseases in
children: hard and not-so-hard evidence of efficacy. J Pediatr
Gastroenterol Nutr. 2006;42:454–75.
32. Saavedra JM, et al. Feeding of Bifidobacterium bifidum and
Streptococcus thermophilus to infants in hospital for prevention
of diarrhoea and shedding of rotavirus. Lancet.
1994;344:1046–9.
33. Szajewska H, et al. Efficacy of Lactobacillus GG in prevention
of nosocomial diarrhea in infants. J Pediatr. 2001;138:361–5.
34. Mastretta E, et al. Effect of Lactobacillus GG and breast-feeding
in the prevention of rotavirus nosocomial infection. J Pediatr
Gastroenterol Nutr. 2002;35:527–31.
35. Chouraqui JP, et al. Acidified milk formula supplemented with
bifidobacterium lactis: impact on infant diarrhea in residential
care settings. J Pediatr Gastroenterol Nutr. 2004;38:288–92.
36. Thibault H, et al. Effects of long-term consumption of a fer-
mented infant formula (with bifidobacterium breve c50 and
Streptococcus thermophilus 065) on acute diarrhea in healthy
infants. J Pediatr Gastroenterol Nutr. 2004;39:147–52.
212 S. Cruchet et al.

37. Pawlowski SW, et al. Diagnosis and treatment of acute or per-
sistent diarrhea. Gastroenterology. 2009;136:1874–86.
38. Shamir R, et al. Evaluation of a diet containing probiotics and
zinc for the treatment of mild diarrheal illness in children
younger than one year of age. J Am Coll Nutr. 2005;24:370–5.
39. Isolauri E, et al. A human Lactobacillus strain (Lactobacillus
casei sp strain GG) promotes recovery from acute diarrhea in
children. Pediatrics. 1991;88:90–7.
40. Shornikova AV, et al. A trial in the Karelian Republic of oral
rehydration and Lactobacillus GG for treatment of acute diar-
rhoea. Acta Paediatr. 1997;86:460–5.
41. Guarino A, et al. Oral bacterial therapy reduces the duration of
symptoms and of viral excretion in children with mild diarrhea.
J Pediatr Gastroenterol Nutr. 1997;25:516–9.
42. Guandalini S, et al. Lactobacillus GG administered in oral re-
hydration solution to children with acute diarrhea: a multicenter
European trial. J Pediatr Gastroenterol Nutr. 2000;30:54–60.
43. Shornikova AV, et al. Bacteriotherapy with Lactobacillus reu-
teri in rotavirus gastroenteritis. Pediatr Infect Dis J.
1997;16:1103–7.
44. Szajewska H, et al. Meta-analysis: Lactobacillus reuteri strain
DSM 17938 (and the original strain ATCC 55730) for treating
acute gastroenteritis in children. Benef Microbes. 2014;5:285–93.
45. Simakachorn N, et al. Clinical evaluation of the addition of
lyophilized, heat-killed Lactobacillus acidophilus LB to oral
rehydration therapy in the treatment of acute diarrhea in chil-
dren. J Pediatr Gastroenterol Nutr. 2000;30:68–72.
46. Szymanski H, et al. Treatment of acute infectious diarrhoea in
infants and children with a mixture of three Lactobacillus
rhamnosus strains—a randomized, double-blind, placebo-con-
trolled trial. Aliment Pharmacol Ther. 2006;23:247–53.
47. Costa-Ribeiro H, et al. Limitations of probiotic therapy in acute,
severe dehydrating diarrhea. J Pediatr Gastroenterol Nutr.
2003;36:112–5.
48. Salazar-Lindo E, et al. Lactobacillus casei strain GG in the
treatment of infants with acute watery diarrhea: a randomized,
double-blind, placebo controlled clinical trial
[ISRCTN67363048]. BMC Pediatr. 2004;4:18.
49. Kowalska-Duplaga K, et al. Efficacy of Trilacin the treatment of
acute diarrhoea in infants and young children—a multicentre,
randomized, double-blind placebo-controlled study. Pediatria
Wspołczesna. 2004;3:295–9.
50. Khanna V, et al. Efficacy of tyndalized Lactobacillus aci-
dophilus in acute diarrhea. Indian J Pediatr. 2005;72:935–8.
51. Sarker SA, et al. Lactobacillus paracasei strain ST11 has no
effect on rotavirus but ameliorates the outcome of nonrotavirus
diarrhea in children from Bangladesh. Pediatrics.
2005;116:e221–8.
52. Huang JS, et al. Efficacy of probiotic use in acute diarrhea in
children: a meta-analysis. Dig Dis Sci. 2002;47:2625–34.
53. Van Niel CW, et al. Lactobacillus therapy for acute infectious
diarrhea in children: a meta-analysis. Pediatrics.
2002;109:678–84.
54. Szajewska H, Mrukowicz JZ. Probiotics in the treatment and
prevention of acute infectious diarrhea in infants and children: a
systematic review of published randomized, double-blind,
placebo-controlled trials. J Pediatr Gastroenterol Nutr.
2001;33(Suppl 2):S17–25.
55. Allen SJ, et al. Probiotics for treating acute infectious diarrhoea.
Cochrane Database Syst Rev. 2010;(11):CD003048. doi:10.
1002/14651858.CD003048.pub3.
56. Hochter W, et al. Saccharomyces boulardii bei akuter Erwach-
senendiarrhoe. Munch Med Wschr. 1990;132:188–92.
57. Cetina-Sauri G, Sierra Basto G. Therapeutic evaluation of
Saccharomyces boulardii in children with acute diarrhea. Ann
Pediatr. 1994;41:397–400.
58. Kurugol Z, Koturoglu G. Effects of Saccharomyces boulardii in
children with acute diarrhoea. Acta Paediatr. 2005;94:44–7.
59. Villarruel G, et al. Saccharomyces boulardii in acute childhood
diarrhoea: a randomized, placebo-controlled study. Acta Pae-
diatr. 2007;96:538–41.
60. Castaneda C, et al. Effects of Saccharomyces boulardii in
children with chronic diarrhea, especially cases due to giardia-
sis. Rev Mex Pueric Pediatr. 1995;2:12–6.
61. Mansour-Ghanaei F, et al. Efficacy of saccharomyces boulardii
with antibiotics in acute amoebiasis. World J Gastroenterol.
2003;9:1832–3.
62. Saint-Marc T, et al. Efficacy of Saccharomyces boulardii in the
treatment of diarrhea in AIDS. Ann Med Interne (Paris).
1991;142:64–5.
63. Billoo AG, et al. Role of a probiotic (Saccharomyces boulardii)
in management and prevention of diarrhoea. World J Gas-
troenterol. 2006;12:4557–60.
64. Gutierrez Castrellon P, et al. An evidence based Iberic-Latin
American guideline for acute gastroenteritis management in
infants and prescholars. An Pediatr (Barc) 2010;72:220 e1–20.
65. National Collaborating Centre for Women’s and Children’s
Health. Diarrhoea and vomiting caused by gastroenteritis: di-
agnosis, assessment and management in children younger than
5 years. National Institute for Health and Clinical Excellence
(NICE). 2009. Accessed 30 Oct 2014.
66. WGO. Probioticos y Prebioticos. World Gastroenterology Or-
ganisation. 2011. http://www.worldgastroenterology.org/assets/
export/userfiles/2012%20Probiotics_NEW%20FINAL_sp.pdf.
Accessed 30 Oct 2014.
67. Sazawal S, et al. Efficacy of probiotics in prevention of acute
diarrhoea: a meta-analysis of masked, randomised, placebo-
controlled trials. Lancet Infect Dis. 2006;6:374–82.
68. Francavilla R, et al. Randomised clinical trial: Lactobacillus
reuteri DSM 17938 vs. placebo in children with acute diar-
rhoea—a double-blind study. Aliment Pharmacol Ther.
2012;36:363–9.
69. Turck D, et al. Incidence and risk factors of oral antibiotic-
associated diarrhea in an outpatient pediatric population. J Pe-
diatr Gastroenterol Nutr. 2003;37:22–6.
70. Szajewska H, et al. Probiotics in the prevention of antibiotic-
associated diarrhea in children: a meta-analysis of randomized
controlled trials. J Pediatr. 2006;149:367–72.
71. Advice for travelers. Treat Guidel Med Lett. 2004;2(21):33–40.
72. Advice for travelers. Med Lett Drugs Ther. 1996;38(969):17–20.
73. Mackell S. Traveler’s diarrhea in the pediatric population: eti-
ology and impact. Clin Infect Dis. 2005;41(Suppl 8):S547–52.
74. Hilton E, et al. Efficacy of Lactobacillus GG as a diarrheal
preventive in travelers. J Travel Med. 1997;4:41–3.
75. Katelaris PH, et al. Lactobacilli to prevent traveler’s diarrhea?
N Engl J Med. 1995;333:1360–1.
76. Oksanen PJ, et al. Prevention of travellers’ diarrhoea by Lac-
tobacillus GG. Ann Med. 1990;22:53–6.
77. Kollaritsch H, et al. Prevention of traveler’s diarrhea with
Saccharomyces boulardii. Results of a placebo controlled dou-
ble-blind study. Fortschr Med. 1993;111:152–6.
78. Boonyaritichaikij S, et al. Long-term administration of probi-
otics to asymptomatic pre-school children for either the
eradication or the prevention of Helicobacter pylori infection.
Helicobacter. 2009;14:202–7.
79. Cruchet S, et al. Effect of the ingestion of a dietary product
containing Lactobacillus johnsonii La1 on Helicobacter pylori
colonization in children. Nutrition. 2003;19:716–21.
80. Gotteland M, et al. Effect of regular ingestion of Saccharomyces
boulardii plus inulin or Lactobacillus acidophilus LB in children
colonized by Helicobacter pylori. Acta Paediatr.
2005;94:1747–51.
Probiotics in Pediatric Gastroenterology 213

81. Szajewska H, et al. Randomized, double-blind, placebo-con-
trolled trial: effect of Lactobacillus GG supplementation on
Helicobacter pylori eradication rates and side effects during
treatment in children. J Pediatr Gastroenterol Nutr.
2009;48:431–6.
82. Sykora J, et al. Effects of a specially designed fermented milk
product containing probiotic Lactobacillus casei DN-114 001
and the eradication of H. pylori in children: a prospective ran-
domized double-blind study. J Clin Gastroenterol.
2005;39:692–8.
83. Goldman CG, et al. Effect of a probiotic food as an adjuvant to
triple therapy for eradication of Helicobacter pylori infection in
children. Nutrition. 2006;22:984–8.
84. Lionetti E, et al. Lactobacillus reuteri therapy to reduce side-
effects during anti-Helicobacter pylori treatment in children: a
randomized placebo controlled trial. Aliment Pharmacol Ther.
2006;24:1461–8.
85. Sykora J, et al. Supplements of one week triple drug therapy
with special probiotic Lactobacillus casei imunitass (Strain DN-
114 000) and Streptococcus thermophilus and Lactobacillus
bulgaricus in the eradication of H. pylori-colonized children: a
prospective randomised trial [abstract P0900]. J Pediatr Gas-
troenterol Nutr. 2004;39:S400.
86. Hurduc V, et al. A randomized, open trial evaluating the effect
of Saccharomyces boulardii on the eradication rate of Heli-
cobacter pylori infection in children. Acta Paediatr.
2009;98:127–31.
87. Hyman PE, et al. Childhood functional gastrointestinal disor-
ders: neonate/toddler. Gastroenterology. 2006;130:1519–26.
88. Savino F. Focus on infantile colic. Acta Paediatr.
2007;96:1259–64.
89. Metcalf TJ, et al. Simethicone in the treatment of infant colic: a
randomized, placebo-controlled, multicenter trial. Pediatrics.
1994;94:29–34.
90. Akcam M, Yilmaz A. Oral hypertonic glucose solution in the
treatment of infantile colic. Pediatr Int. 2006;48:125–7.
91. Danielsson B, Hwang CP. Treatment of infantile colic with
surface active substance (simethicone). Acta Paediatr Scand.
1985;74:446–50.
92. Gupta SK. Update on infantile colic and management options.
Curr Opin Investig Drugs. 2007;8:921–6.
93. Savino F, et al. A randomized double-blind placebo-controlled
trial of a standardized extract of Matricariae recutita,
Foeniculum vulgare and Melissa officinalis (ColiMil) in the
treatment of breastfed colicky infants. Phytother Res.
2005;19:335–40.
94. Anabrees J, et al. Probiotics for infantile colic: a systematic
review. BMC Pediatr. 2013;13:186.
95. Szajewska H, et al. Lactobacillus reuteri DSM 17938 for the
management of infantile colic in breastfed infants: a random-
ized, double-blind, placebo-controlled trial. J Pediatr.
2013;162:257–62.
96. Savino F, et al. Lactobacillus reuteri (American Type Culture
Collection Strain 55730) versus simethicone in the treatment of
infantile colic: a prospective randomized study. Pediatrics.
2007;119:e124–30.
97. Savino F, et al. Lactobacillus reuteri DSM 17938 in infantile
colic: a randomized, double-blind, placebo-controlled trial. Pe-
diatrics. 2010;126:e526–33.
98. Chau K, et al. Probiotics for infantile colic: a randomized,
double-blind, placebo-controlled trial investigating Lactobacil-
lus reuteri DSM 17938. J Pediatr. 2015;166(74–8):e1.
99. Savino F, et al. Preventive effects of oral probiotic on infantile
colic: a prospective, randomised, blinded, controlled trial using
Lactobacillus reuteri DSM 17938. Benef Microbes. 2014:1–7.
[Epub ahead of print].
100. Indrio F, et al. Prophylactic use of a probiotic in the prevention
of colic, regurgitation, and functional constipation: a random-
ized clinical trial. JAMA Pediatr. 2014;168:228–33.
101. Sung V, et al. Treating infant colic with the probiotic Lacto-
bacillus reuteri: double blind, placebo controlled randomised
trial. BMJ. 2014;348:g2107.
102. Saavedra JM, et al. Long-term consumption of infant formulas
containing live probiotic bacteria: tolerance and safety. Am J
Clin Nutr. 2004;79:261–7.
103. Fernandez JI, De las Cuevas T. Enterocolitis necrotizante
neonatal. Bol Pediatr. 2006;46(Suppl 1):172–8.
104. Deshpande G, et al. Probiotics for prevention of necrotising
enterocolitis in preterm neonates with very low birthweight: a
systematic review of randomised controlled trials. Lancet.
2007;369:1614–20.
105. Samanta M, et al. Prophylactic probiotics for prevention of
necrotizing enterocolitis in very low birth weight newborns.
J Trop Pediatr. 2009;55:128–31.
106. Millar M, et al. Probiotics for preterm infants? Arch Dis Child
Fetal Neonatal Ed. 2003;88:F354–8.
107. Mattar AF, et al. Effect of probiotics on enterocyte bacterial
translocation in vitro. Pediatr Surg Int. 2001;17:265–8.
108. Orrhage K, Nord CE. Factors controlling the bacterial
colonization of the intestine in breastfed infants. Acta Paediatr.
1999;88:47–57.
109. Reid G, et al. Can bacterial interference prevent infection?
Trends Microbiol. 2001;9:424–8.
110. Duffy LC. Interactions mediating bacterial translocation in the
immature intestine. J Nutr. 2000;130:432S–6S.
111. Martin CR, Walker WA. Probiotics: role in pathophysiology and
prevention in necrotizing enterocolitis. Semin Perinatol.
2008;32:127–37.
112. Schanler RJ. Probiotics and necrotising enterocolitis in prema-
ture infants. Arch Dis Child Fetal Neonatal Ed. 2006;91:F395–7.
113. Alfaleh K, Bassler D. Probiotics for prevention of necrotizing
enterocolitis in preterm infants. Cochrane Database Syst Rev.
2008;(1):CD005496. doi:10.1002/14651858.CD005496.pub2.
114. Bin-Nun A, et al. Oral probiotics prevent necrotizing entero-
colitis in very low birth weight neonates. J Pediatr.
2005;147:192–6.
115. Lin HC, et al. Oral probiotics reduce the incidence and severity
of necrotizing enterocolitis in very low birth weight infants.
Pediatrics. 2005;115:1–4.
116. Wolvers D, et al. Guidance for substantiating the evidence for
beneficial effects of probiotics: prevention and management of
infections by probiotics. J Nutr. 2010;140:698S–712S.
117. Alfaleh K, et al. Probiotics reduce the risk of necrotizing ente-
rocolitis in preterm infants: a meta-analysis. Neonatology.
2010;97:93–9.
118. Deshpande G, et al. Updated meta-analysis of probiotics for
preventing necrotizing enterocolitis in preterm neonates. Pedi-
atrics. 2010;125:921–30.
119. Hunter C, et al. Effect of routine probiotic, Lactobacillus reuteri
DSM 17938, use on rates of necrotizing enterocolitis in neonates
with birthweight \1000 grams: a sequential analysis. BMC
Pediatr. 2012;12:142.
120. Kadowaki N, et al. Subsets of human dendritic cell precursors
express different toll-like receptors and respond to different
microbial antigens. J Exp Med. 2001;194:863–9.
121. Sartor RB. Therapeutic manipulation of the enteric microflora in
inflammatory bowel diseases: antibiotics, probiotics, and pre-
biotics. Gastroenterology. 2004;126:1620–33.
122. Bousvaros A, et al. A randomized, double-blind trial of Lacto-
bacillus GG versus placebo in addition to standard maintenance
therapy for children with Crohn’s disease. Inflamm Bowel Dis.
2005;11:833–9.
214 S. Cruchet et al.

123. Day AS, et al. Use of complementary and alternative medicines
by children and adolescents with inflammatory bowel disease.
J Paediatr Child Health. 2004;40:681–4.
124. Miele E, et al. Effect of a probiotic preparation (VSL#3) on
induction and maintenance of remission in children with ul-
cerative colitis. Am J Gastroenterol. 2009;104:437–43.
125. Talley NJ. Functional gastrointestinal disorders as a public
health problem. Neurogastroenterology and motility : the official
journal of the European Gastrointestinal Motility Society.
2008;20(Suppl 1):121–9.
126. Drossman DA, Dumitrascu DL, Rome III. New standard for
functional gastrointestinal disorders. J Gastrointestin Liver Dis.
2006;15:237–41.
127. Karantanos T, et al. Current insights in to the pathophysiology
of Irritable Bowel Syndrome. Gut Pathog. 2010;2:3.
128. Bausserman M, Michail S. The use of Lactobacillus GG in ir-
ritable bowel syndrome in children: a double-blind randomized
control trial. J Pediatr. 2005;147:197–201.
129. Gawronska A, et al. A randomized double-blind placebo-con-
trolled trial of Lactobacillus GG for abdominal pain disorders in
children. Aliment Pharmacol Ther. 2007;25:177–84.
130. Guandalini S, et al. VSL#3 improves symptoms in children with
irritable bowel syndrome: a multicenter, randomized, placebo-
controlled, double-blind, crossover study. J Pediatr Gastroen-
terol Nutr. 2010;51:24–30.
131. Banaszkiewicz A, Szajewska H. Ineffectiveness of Lactobacillus
GG as an adjunct to lactulose for the treatment of constipation in
children: a double-blind, placebo-controlled randomized trial.
J Pediatr. 2005;146:364–9.
132. Chmielewska A, Szajewska H. Systematic review of randomised
controlled trials: probiotics for functional constipation. World J
Gastroenterol. 2010;16:69–75.
133. Majamaa H, Isolauri E. Probiotics: a novel approach in the
management of food allergy. J Allergy Clin Immunol.
1997;99:179–85.
134. Isolauri E, et al. Probiotics in the management of atopic eczema.
Clin Exp Allergy. 2000;30:1604–10.
135. Kalliomaki M, et al. Probiotics in primary prevention of atopic
disease: a randomised placebo-controlled trial. Lancet.
2001;357:1076–9.
136. Kalliomaki M, et al. Probiotics and prevention of atopic disease:
4-year follow-up of a randomised placebo-controlled trial.
Lancet. 2003;361:1869–71.
137. Kukkonen K, et al. Probiotics and prebiotic galacto-oligosac-
charides in the prevention of allergic diseases: a randomized,
double-blind, placebo-controlled trial. J Allergy Clin Immunol.
2007;119:192–8.
138. Taylor AL, et al. Probiotic supplementation for the first 6 months of
life fails to reduce the risk of atopic dermatitis and increases the risk
of allergen sensitization in high-risk children: a randomized con-
trolled trial. J Allergy Clin Immunol. 2007;119:184–91.
139. Rosenfeldt V, et al. Effect of probiotics on gastrointestinal
symptoms and small intestinal permeability in children with
atopic dermatitis. J Pediatr. 2004;145:612–6.
140. Kendler M, et al. Comparison of fecal microflora in children
with atopic eczema/dermatitis syndrome according to IgE sen-
sitization to food. Pediatr Allergy Immunol. 2006;17:141–7.
141. Brouwer ML, et al. No effects of probiotics on atopic dermatitis
in infancy: a randomized placebo-controlled trial. Clin Exp
Allergy. 2006;36:899–906.
142. Sistek D, et al. Is the effect of probiotics on atopic dermatitis
confined to food sensitized children? Clin Exp Allergy.
2006;36:629–33.
143. Viljanen M, et al. Probiotics in the treatment of atopic
eczema/dermatitis syndrome in infants: a double-blind placebo-
controlled trial. Allergy. 2005;60:494–500.
144. Rosenfeldt V, et al. Effect of probiotic Lactobacillus strains in
children with atopic dermatitis. J Allergy Clin Immunol.
2003;111:389–95.
145. Osborn DA, Sinn JK. Prebiotics in infants for prevention of
allergic disease and food hypersensitivity. Cochrane Database
Syst Rev. 2007;(4):CD006474.
146. Petroczi A, et al. Mission impossible? Regulatory and enforce-
ment issues to ensure safety of dietary supplements. Food Chem
Toxicol. 2011;49:393–402.
147. Temmerman R, et al. Identification and antibiotic susceptibility
of bacterial isolates from probiotic products. Int J Food Micro-
biol. 2003;81:1–10.
148. Elliot E, Teversham K. An evaluation of nine probiotics avail-
able in South Africa, August 2003. S Afr Med J. 2004;94:121–4.
149. Ibnou-Zekri N, et al. Divergent patterns of colonization and
immune response elicited from two intestinal Lactobacillus
strains that display similar properties in vitro. Infect Immun.
2003;71:428–36.
150. Braegger C, et al. Supplementation of infant formula with pro-
biotics and/or prebiotics: a systematic review and comment by
the ESPGHAN committee on nutrition. J Pediatr Gastroenterol
Nutr. 2011;52:238–50.
151. Henker J, et al. Probiotic Escherichia coli Nissle 1917 versus
placebo for treating diarrhea of greater than 4 days duration in
infants and toddlers. Pediatr Infect Dis J. 2008;27:494–9.
152. Yameen MA, et al. Nasal and perirectal colonization of van-
comycin sensitive and resistant enterococci in patients of pae-
diatrics ICU (PICU) of tertiary health care facilities. BMC Infect
Dis. 2013;13:156.
153. Bernet MF, et al. Lactobacillus acidophilus LA 1 binds to
cultured human intestinal cell lines and inhibits cell attachment
and cell invasion by enterovirulent bacteria. Gut.
1994;35:483–9.
154. Juntunen M, et al. Adherence of probiotic bacteria to human
intestinal mucus in healthy infants and during rotavirus infec-
tion. Clin Diagn Lab Immunol. 2001;8:293–6.
155. Urban MF, et al. Growth of infants born to HIV-infected women
when fed a biologically acidified starter formula with and
without probiotics. South Afr J Clin Nutr. 2008;21:28–32.
156. Weizman Z, Alsheikh A. Safety and tolerance of a probiotic
formula in early infancy comparing two probiotic agents: a pilot
study. J Am Coll Nutr. 2006;25:415–9.
157. Gibson RA, et al. Safety of supplementing infant formula with
long-chain polyunsaturated fatty acids and Bifidobacterium
lactis in term infants: a randomised controlled trial. Br J Nutr.
2009;101:1706–13.
158. Probiotics. Med Lett Drugs Ther. 2007;49(1267):66–8.
159. Snydman DR. The safety of probiotics. Clin Infect Dis.
2008;46(Suppl 2):S104-11 (discussion S44–51).
160. Broughton RA, et al. Neonatal meningitis due to Lactobacillus.
Pediatr Infect Dis. 1983;2:382–4.
161. Kunz AN, et al. Two cases of Lactobacillus bacteremia during
probiotic treatment of short gut syndrome. J Pediatr Gastroen-
terol Nutr. 2004;38:457–8.
162. Perapoch J, et al. Fungemia with Saccharomyces cerevisiae in
two newborns, only one of whom had been treated with ultra-
levura. Eur J Clin Microbiol Infect Dis. 2000;19:468–70.
163. Thompson C, et al. Lactobacillus acidophilus sepsis in a neo-
nate. J Perinatol. 2001;21:258–60.
164. Borriello SP, et al. Safety of probiotics that contain lactobacilli
or bifidobacteria. Clin Infect Dis. 2003;36:775–80.
165. Karpa KD. Probiotics for Clostridium difficile diarrhea: putting
it into perspective. Ann Pharmacother. 2007;41:1284–7.
166. Fedorak RN, Madsen KL. Probiotics and prebiotics in gas-
trointestinal disorders. Curr Opin Gastroenterol.
2004;20:146–55.
Probiotics in Pediatric Gastroenterology 215

167. Mackay AD, et al. Lactobacillus endocarditis caused by a pro-
biotic organism. Clin Microbiol Infect. 1999;5:290–2.
168. Rautio M, et al. Liver abscess due to a Lactobacillus rhamnosus
strain indistinguishable from L. rhamnosus strain GG. Clin In-
fect Dis. 1999;28:1159–60.
169. Cabana MD, et al. Probiotics in primary care pediatrics. Clin
Pediatr (Phila). 2006;45:405–10.
170. Enache-Angoulvant A, Hennequin C. Invasive Saccharomyces
infection: a comprehensive review. Clin Infect Dis.
2005;41:1559–68.
171. Cassone M, et al. Outbreak of Saccharomyces cerevisiae sub-
type boulardii fungemia in patients neighboring those treated
with a probiotic preparation of the organism. J Clin Microbiol.
2003;41:5340–3.
172. Jijon H, et al. DNA from probiotic bacteria modulates murine
and human epithelial and immune function. Gastroenterology.
2004;126:1358–73.
216 S. Cruchet et al.