The Care Transitions Intervention - A Valued Voice Care Transitions Intervention ... – The Four...
12
The Care Transitions Intervention ® Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Eric A. Coleman, MD, MPH • To provide an overview of the Care Transitions Intervention®(Developer: Eric Coleman, MD, MPH; http://www.caretransitions.org/ ) – Preparing patients and caregivers to participate in care delivered across settings – The Four Pillars – Coaching vs. Doing – Stories from the field • To discuss the importance of patient activation Objectives “Silent” Care Coordinators • Older patients and family caregivers function as their own care coordinators • First line of defense for transition related errors • CTI model explicitly recognizes their role as integral members of the interdisciplinary team http://www.caretransitions.org/ Eric A. Coleman, MD, MPH
Transcript of The Care Transitions Intervention - A Valued Voice Care Transitions Intervention ... – The Four...

The Care Transitions
Intervention®
Kimberly Irby, MPH
Colorado Foundation for Medical Care
www.cfmc.org/integratingcare
Acknowledgments: Eric A. Coleman, MD, MPH
• To provide an overview of the Care Transitions
Intervention® (Developer: Eric Coleman, MD,
MPH; http://www.caretransitions.org/)
– Preparing patients and caregivers to participate in care
delivered across settings
– The Four Pillars
– Coaching vs. Doing
– Stories from the field
• To discuss the importance of patient activation
Objectives
“Silent” Care Coordinators
• Older patients and family caregivers function as their own care coordinators
• First line of defense for transition related errors
• CTI model explicitly recognizes their role as integral members of the interdisciplinary team
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
The Care Transitions Intervention
• Self-management model
• Encourages patients and caregivers to take a more active role during transitions
• Key Elements:
– Transition Coach®
– Personal Health Record
– Medication Discrepancy Tool (MDT)®
– The Four Pillars®
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Intervention Details: Transition
Coach®• Hospital Visit
• Nursing Home Visit*
• Home Visit (ideally within 48 hours of discharge)
• 3 Phone Calls
*when applicable
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Personal Health Record
• Patient-owned and operated
• Record of medical history and associated
warning signs
• Medication list
• Advance directives
• Space for patient questions and concerns
• Should be portable, readable, easy to locate
and update
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Medication Reconciliation
From the MDT:
50% System
1/3 discharge instructions incomplete, illegible or inaccurate
1/3 conflicting information
1/6 duplicate meds
50% Patient
2/3 non-intentional non-adherence
Coleman EA, Smith JD, Raha D, Min S. Posthospital Medication Discrepancies Prevalence and Contributing Factors. Arch Intern
Med. 2005;165:1842-1847
You’re Only
Old Once! A
Book for
Obsolete
Children,
Dr. Seuss
The Four Pillars®
1. Medication self-management
2. Use of a dynamic patient-centered
record, the Personal Health Record
3. Timely primary care/specialty care
follow up
4. Knowledge of red flags that indicate
a worsening in their condition and
how to respond
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Coaching vs. Doing
• A coach helps the patient set goals
• A coach helps the patient anticipate barriers and plan for their resolution
• A coach strategizes with the patient ways to take action to meet goals
• A coach does not do it for the patient
• A coach is not a caregiver
• A coach is not an educator
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
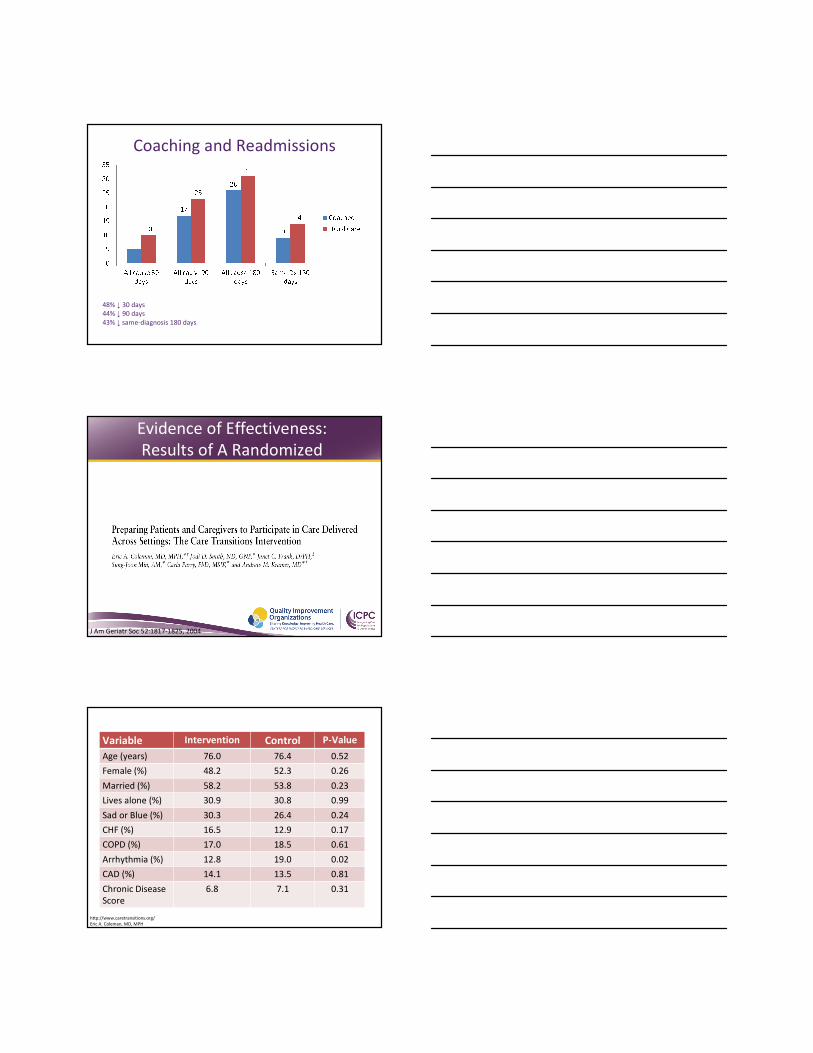
Coaching and Readmissions
48% ↓ 30 days
44% ↓ 90 days
43% ↓ same-diagnosis 180 days
Evidence of Effectiveness:
Results of A Randomized
Controlled Trial
J Am Geriatr Soc 52:1817-1825, 2004
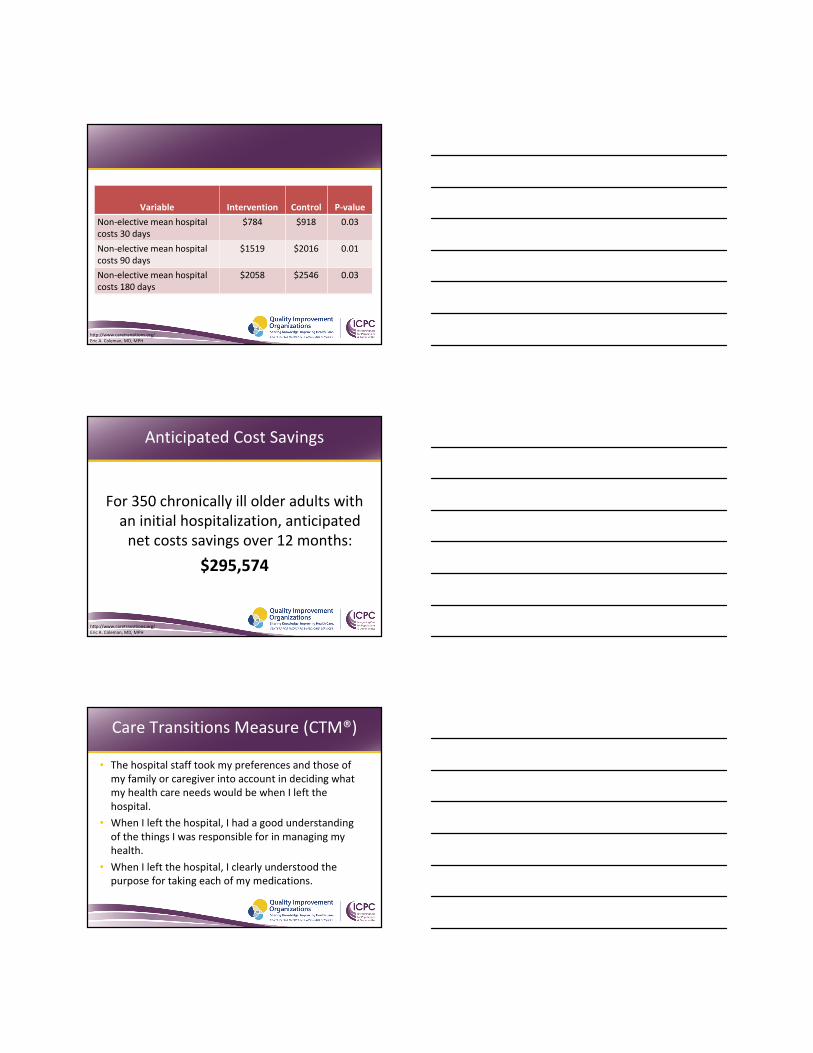
Variable Intervention Control P-Value
Age (years) 76.0 76.4 0.52
Female (%) 48.2 52.3 0.26
Married (%) 58.2 53.8 0.23
Lives alone (%) 30.9 30.8 0.99
Sad or Blue (%) 30.3 26.4 0.24
CHF (%) 16.5 12.9 0.17
COPD (%) 17.0 18.5 0.61
Arrhythmia (%) 12.8 19.0 0.02
CAD (%) 14.1 13.5 0.81
Chronic Disease
Score
6.8 7.1 0.31
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Variable Intervention Control P-Value
Prior Hosp (%)
1+ past 6 mo
29.3 26.1 0.36
Prior ED (%)
1+ past 6 mo
40.3 38.9 0.69
D/C Destin.
Home (%)
Homecare (%)
SNF (%)
Other (%)
50.8
24.7
21.0
3.5
52.9
25.9
19.3
1.9
0.71
Friday D/C (%) 14.6 16.5 0.48
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Variable Intervention Control
Adjusted
P-value
Re-hospitalized
w/in 30 days
8 % 12 % 0.05
Re-hospitalized
w/in 90 days
17 % 23 % 0.03
Re-hospitalized
w/in 180 days
26 % 31 % 0.09
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Variable Intervention Control
Adjusted
P-value
Readmit for Same Dx
w/in 30 days
3 % 5 % 0.04
Readmit for Same Dx
w/in 90 days
5 % 10 % <0.01
Readmit for Same Dx
w/in 180 days
9 % 14 % <0.01
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Variable Intervention Control P-value
Non-elective mean hospital
costs 30 days
$784 $918 0.03
Non-elective mean hospital
costs 90 days
$1519 $2016 0.01
Non-elective mean hospital
costs 180 days
$2058 $2546 0.03
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Anticipated Cost Savings
For 350 chronically ill older adults with
an initial hospitalization, anticipated
net costs savings over 12 months:
$295,574
http://www.caretransitions.org/
Eric A. Coleman, MD, MPH
Care Transitions Measure (CTM®)
• The hospital staff took my preferences and those of
my family or caregiver into account in deciding what
my health care needs would be when I left the
hospital.
• When I left the hospital, I had a good understanding
of the things I was responsible for in managing my
health.
• When I left the hospital, I clearly understood the
purpose for taking each of my medications.
Implementation Considerations
• Community-based implementation
• Hospital-specific implementation
• Providers as coach
• Volunteers as coach
• Partnerships with AAA and ADRC
• Local adaptations
Measurement Considerations
Process MeasuresProximal Outcome
MeasuresUtilization Measures
Care Transitions
Intervention
(CTI)
• Count of patients
coached
• Count of
medication
discrepancies
• PAM scores
• Patient Activation
Assessment
scores
• Readmission rates
• Admission rates
• Emergency
department
utilization rates
Stories from the field
“I feel that I must tell someone
about how greatly I benefited from and appreciate the services of the
nurse who follows up on patients discharged from your hospital.
She comforted me and helped
make several forceful phone calls, and soon all was well. What a
great help! What a relief! Thanks.”
Mr. H: A patient story
The personal impact
• Coleman et al. (2006): Lower 30-day
readmission; lower readmission at 90 days
and 180 days.
• Coleman et al. (2004): Lower readmission for
same diagnosis at 90 days and 180 days.
• Additional articles of interest
– http://caretransitions.org/publications.asp
23
Further Evidence
Patient Activation
Patient Activation Measure (PAM®)
http://www.insigniahealth.com/solutions/
patient-activation-measure
Blah blah blah, blah blah. Any questions?
No I’m good to
go. Whatever
you say is what
we’ll do Doctor
What’s he saying? I
sure hope my wife is
getting this..
How can you
tell?
Patient Activation
Measure(PAM ®) -
Integration with the CTI
• A 13 item measure used to guide clinical interventions that
support patient activation to maximize outcomes
• Developed by Judith Hibbard, Jean Stockard, and Martin Tusler at the University of Oregon and Eldon R. Mahoney at PeaceHealth.
• The PAM is a copyright protected instrument and is the property of the Insignia Health
• Use of the PAM must be arranged by contacting Insignia Health
Patient Activation Measure (PAM®)
Stage 1 – Believes Active Role Important:
• Taking an active role in my own health care is the most important factor in determining my health and ability to function.
Stage 2 – Confidence and Knowledge to Take Action:
• I am confident that I can follow through on medical treatments I need to do at home.
Stage 3 – Taking Action:
• I am able to handle symptoms of my health condition on my own at home.
• I have made the changes in my lifestyle like diet and exercise that are recommended for my health condition.
Stage 4 – Staying the Course Under Stress:
• I am confident I can figure out solutions when new situations or problems arise with my health condition.
• I am confident that I can maintain lifestyle changes like diet and exercise even during times of stress.
PAM Stages of Activation
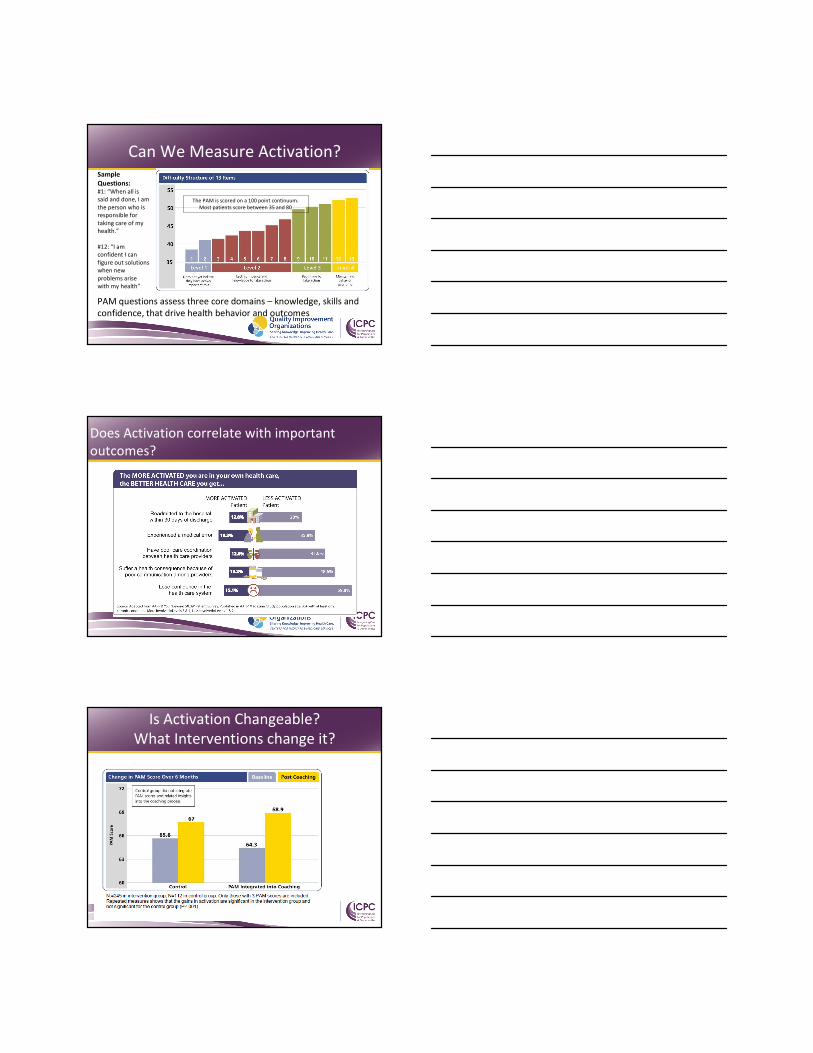
PAM questions assess three core domains – knowledge, skills and
confidence, that drive health behavior and outcomes
28
Sample
Questions:#1: “When all is
said and done, I am
the person who is
responsible for
taking care of my
health.”
#12: “I am
confident I can
figure out solutions
when new
problems arise
with my health”
The PAM is scored on a 100 point continuum.
Most patients score between 35 and 80
Can We Measure Activation?
Does Activation correlate with important
outcomes?
29
Is Activation Changeable?
What Interventions change it?
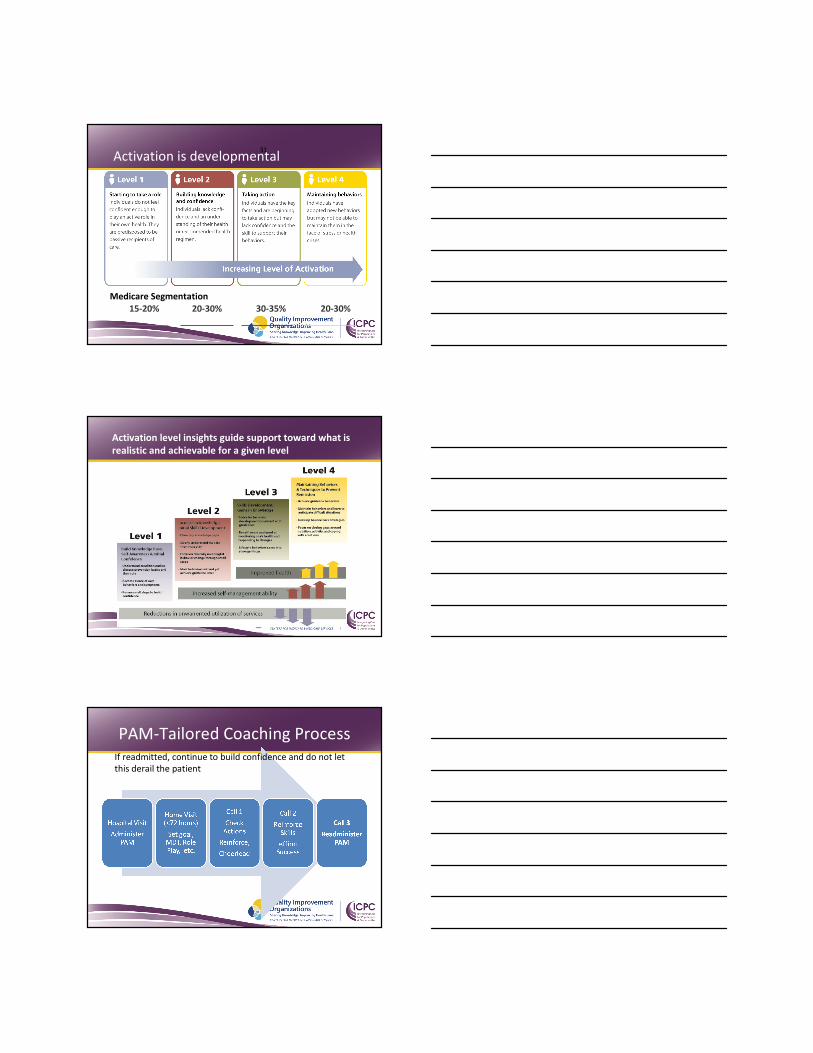
Activation is developmental
15-20% 20-30% 30-35% 20-30%
31
Medicare Segmentation
Activation level insights guide support toward what is
realistic and achievable for a given level
PAM-Tailored Coaching Process If readmitted, continue to build confidence and do not let
this derail the patient
33
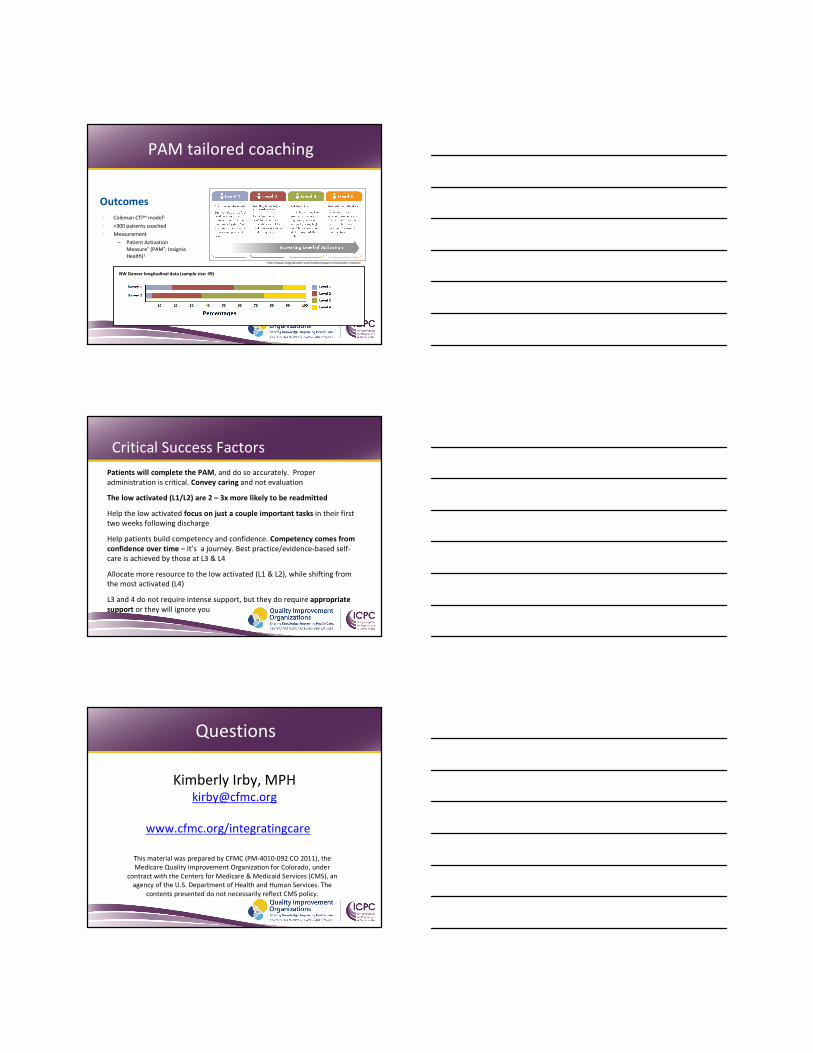
• Coleman CTI℠ model1
• >300 patients coached
• Measurement
– Patient Activation
Measure® (PAM®; Insignia
Health)2
NW Denver longitudinal data (sample size: 49)
http://www.insigniahealth.com/solutions/patient-activation-measure
Outcomes
PAM tailored coaching
Critical Success Factors
Patients will complete the PAM, and do so accurately. Proper
administration is critical. Convey caring and not evaluation
The low activated (L1/L2) are 2 – 3x more likely to be readmitted
Help the low activated focus on just a couple important tasks in their first
two weeks following discharge
Help patients build competency and confidence. Competency comes from
confidence over time – it’s a journey. Best practice/evidence-based self-
care is achieved by those at L3 & L4
Allocate more resource to the low activated (L1 & L2), while shifting from
the most activated (L4)
L3 and 4 do not require intense support, but they do require appropriate
support or they will ignore you
This material was prepared by CFMC (PM-4010-092 CO 2011), the
Medicare Quality Improvement Organization for Colorado, under
contract with the Centers for Medicare & Medicaid Services (CMS), an
agency of the U.S. Department of Health and Human Services. The
contents presented do not necessarily reflect CMS policy.
Kimberly Irby, [email protected]
www.cfmc.org/integratingcare
Questions
![Phase transitions in Interacting Systems · 2020. 5. 28. · Moreover, in statistical mechanics [Rue99], two kinds of phase transitions are con-sidered: First order phase transitions,](https://static.fdocument.pub/doc/165x107/60d3dac1d3bdbc1a9f6f5fe4/phase-transitions-in-interacting-systems-2020-5-28-moreover-in-statistical.jpg)