tgs mataa1.docx
5
Close Pr int Page Non-Infective Inflammatory disease Idiopathic orbital inflammatory disease Idiopathic orbital inflammatory disease (IOID), previously referred to as orbital pseudotumour, is an uncommon disorder characteried by non-neoplastic, non-infective, space-occupying orbital lesions! "he inflammatory process may involve any or all of the orbital soft tissues, resulting in, for e#ample, myositis, dacryoadenitis, optic perineuritis or scleritis! $istopathological analysis reveals pleomorphic inflammatory cellular infiltration follo%ed by reactive fibrosis, but has thus far sho%n no correlation bet%een clinicopathological features and the subse&uent course of the disease! 'nilateral disease is the rule in adults, although in children bilateral involvement may occur! imultaneous orbital and sinus involvement is a rare distinct entity! Diagnosis 1 Presentation is %ith acute periorbital redness, s%elling and pain (ig! *!+)! 2 Signs • Congestive proptosis and ophthalmoplegia may occur! • Optic nerve dysfunction, particularly if the inflammation involves the posterior orbit! 3 CT sho%s ill-defined orbital opacification and loss of definition of contents (ig! *!+ . and C)! 4 Course! "his follo%s one of the follo%ing patterns/ • pontaneous remission after a fe% %ee0s %ithout se&uelae! • Intermittent episodes of activity %ith eventual remission! • evere prolonged inflammation eventually leading to progressive fibrosis of orbital tissues, resulting in a 1froen orbit2 characteried by ophthalmoplegia, %hich ma y be associated %ith ptosis and visual impairment caused by optic nerve involvement! Fig. 3.16 (A) 3eft idiopathic orbital inflammatory disease! (B) C" a#ial vie% sho%s ill-defined orbital opacification4 (C) coronal vie% (Courtesy of R Bates – fig. A; A Pearson – figs B and C ) "reatment 1 Observation, for relatively mild disease, in anticipation of spontaneous remission!
-
Upload
primita-ayu-damayanti -
Category
Documents
-
view
219 -
download
0
Transcript of tgs mataa1.docx
7/26/2019 tgs mataa1.docx
http://slidepdf.com/reader/full/tgs-mataa1docx 1/5
Close
Print Page
Non-Infective Inflammatory disease
Idiopathic orbital inflammatory disease
Idiopathic orbital inflammatory disease (IOID), previously referred to as orbital pseudotumour, is
an uncommon disorder characteried by non-neoplastic, non-infective, space-occupying orbital
lesions! "he inflammatory process may involve any or all of the orbital soft tissues, resulting in,for e#ample, myositis, dacryoadenitis, optic perineuritis or scleritis! $istopathological analysis
reveals pleomorphic inflammatory cellular infiltration follo%ed by reactive fibrosis, but has thus
far sho%n no correlation bet%een clinicopathological features and the subse&uent course of the
disease! 'nilateral disease is the rule in adults, although in children bilateral involvement may
occur! imultaneous orbital and sinus involvement is a rare distinct entity!
Diagnosis
1 Presentation is %ith acute periorbital redness, s%elling and pain (ig! *!+)!
2 Signs
• Congestive proptosis and ophthalmoplegia may occur!
• Optic nerve dysfunction, particularly if the inflammation involves the posterior
orbit!
3 CT sho%s ill-defined orbital opacification and loss of definition of contents (ig! *!+.
and C)!
4 Course! "his follo%s one of the follo%ing patterns/• pontaneous remission after a fe% %ee0s %ithout se&uelae!
• Intermittent episodes of activity %ith eventual remission!
• evere prolonged inflammation eventually leading to progressive fibrosis of orbital
tissues, resulting in a 1froen orbit2 characteried by ophthalmoplegia, %hich may beassociated %ith ptosis and visual impairment caused by optic nerve involvement!
Fig. 3.16 (A) 3eft idiopathic orbital inflammatory disease! (B) C" a#ial vie% sho%s ill-definedorbital opacification4 (C) coronal vie%
(Courtesy of R Bates – fig. A; A Pearson – figs B and C)
"reatment
1 Observation, for relatively mild disease, in anticipation of spontaneous remission!

7/26/2019 tgs mataa1.docx
http://slidepdf.com/reader/full/tgs-mataa1docx 2/5
2 Biops is generally re&uired in persistent cases to confirm the diagnosis and rule out
neoplasia!
3 !SA"#s are often effective and may precede steroid therapy!
4 Sste$i% steroi&s should be administered only after the diagnosis has been confirmed, as
they may mas0 other pathology such as infection and 5egener granulomatosis! Oral
prednisolone, initially 6786 mg9day, is later tapered and discontinued, depending onclinical response, although it may need to be reintroduced in the event of recurrence!
' a&ioterap may be considered if there has been no improvement after : %ee0s of
ade&uate steroid therapy! ;ven a lo% dose treatment (i!e! +6 <y) may produce remission!
6 Anti$etabo*ites such as methotre#ate or mycophenolate mofetil may be necessary in the
conte#t of resistance to both steroids and radiotherapy!
+ Sste$i% in,*i-i$ab, a tumour necrosis factor inhibitor, may be effective in recurrent or
recalcitrant cases that have failed to respond to conventional therapy!
Differential diagnosis
1 Ba%teria* orbita* %e**u*itis should be considered %hen onset is acute and the anterior
orbital tissues are mar0edly inflamed! trial of systemic antibiotics may be necessary
before the correct diagnosis becomes apparent!
2 Severe a%ute T# shares many features %ith IOID, but is commonly bilateral %hile IOID
is usually unilateral!
3 Sste$i% &isor&ers such as 5egener granulomatosis, polyarteritis nodosa and
5aldenstr=m macroglobulinaemia may manifest orbital involvement similar to IOID!
4 /a*ignant orbita* tu$ours, particularly metastatic!
' upture& &er$oi& %st may evo0e a secondary painful granulomatous inflammatory
reaction!
Orbital myositis
Orbital myositis is an idiopathic, non-specific inflammation of one or more e#traocular musclesand is considered a subtype of IOID!
1 0isto*og sho%s a chronic inflammatory cellular infiltrate in relation to muscle fibres(ig! *!+>)!
2 Presentation is usually in early adult life %ith acute pain, e#acerbated by eye movement,
and diplopia!
3 Signs
• 3id oedema, ptosis and chemosis!
• Pain and diplopia associated %ith eye movements!
• ?ascular in@ection over the involved muscle (ig! *!+>.)!
• In chronic cases the affected muscle may become fibrosed, %ith permanent
restrictive myopathy!
4 CT sho%s enlargement of the affected muscles (ig! *!+>C), %ith or %ithout involvement
of the tendons of insertion!
' #i,,erentia* &iagnosis includes orbital cellulitis, ";D and "olosa7$unt syndrome (see
belo%)!
6 Course
7/26/2019 tgs mataa1.docx
http://slidepdf.com/reader/full/tgs-mataa1docx 3/5
• cute non-recurrent involvement %hich resolves spontaneously %ithin %ee0s!
• Chronic disease characteried by either a single episode persisting for longer than :
months (often for years) or recurrent attac0s!
+ Treat$ent is aimed at relieving discomfort and dysfunction, shortening the course and
preventing recurrences!
a NSAIDs may be ade&uate in mild disease!
b Systemic steroids are generally re&uired and usually produce dramatic
improvement, although recurrences occur in A6B of cases!
% Radiotherapy is also effective, particularly in limiting recurrence!
Fig. 3.1+ Orbital myositis! (A) $istology sho%s a chronic inflammatory cellular infiltrate inrelation to muscle fibres4 (B) vascular in@ection over the insertion of the right medial rectus4 (C)
coronal C" sho%s enlargement of the right medial rectus(Courtesy of J Harry and G Misson, from Clinial !"#t#almi Pat#ology, Butter$ort#% Heinemann &'' – fig. A; J erad, * Carter and M Alford, from !ulo"lasti and
Reonstruti+e urgery, in Ra"id -iagnosis in !"#t#almology – Mosy &''/ – figs B and C)
cute dacryoadenitis
3acrimal gland involvement occurs in about :AB of patients %ith IOID! ore commonly,
dacryoadenitis occurs in isolation, resolves spontaneously and does not re&uire treatment!
Occasionally it may be caused by mumps, mononucleosis, and rarely bacteria!
1 Presentation is %ith acute discomfort in the region of the lacrimal gland!
2 Signs
• %elling of the lateral aspect of the eyelid giving rise to a characteristic -shaped ptosis and slight do%n%ard and in%ard dystopia (ig! *!+8)!
• "enderness over the lacrimal gland fossa!
• In@ection of the palpebral portion of the lacrimal gland and ad@acent con@unctiva
(ig! *!+8.)!
• 3acrimal secretion may be reduced!
3 CT sho%s enlargement of the gland and involvement of ad@acent tissues (ig! *!+8C)!
4 #i,,erentia* &iagnosis
a Ruptured dermoid cyst may cause localied inflammation in the region of thelacrimal gland!
b Malignant lacrimal gland tumours may cause pain but the onset is not usually
acute!
7/26/2019 tgs mataa1.docx
http://slidepdf.com/reader/full/tgs-mataa1docx 4/5
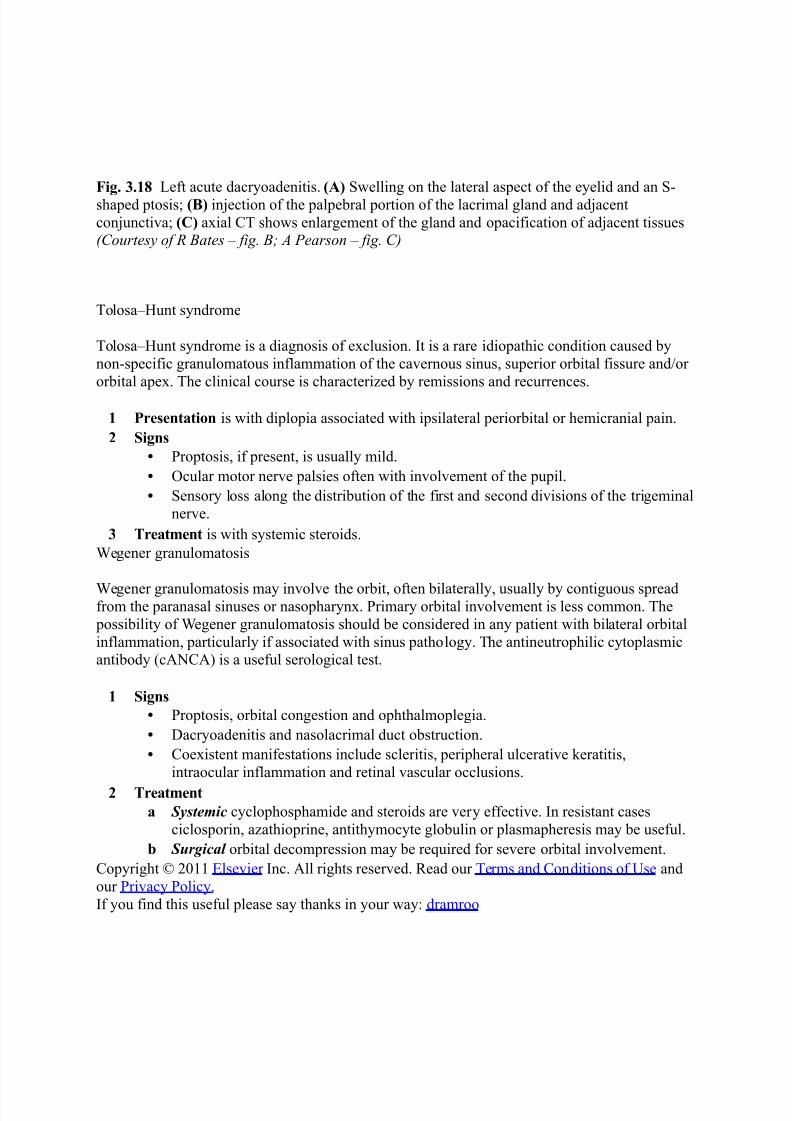
Fig. 3.1 3eft acute dacryoadenitis! (A) %elling on the lateral aspect of the eyelid and an -
shaped ptosis4 (B) in@ection of the palpebral portion of the lacrimal gland and ad@acent
con@unctiva4 (C) a#ial C" sho%s enlargement of the gland and opacification of ad@acent tissues(Courtesy of R Bates – fig. B; A Pearson – fig. C)
"olosa7$unt syndrome
"olosa7$unt syndrome is a diagnosis of e#clusion! It is a rare idiopathic condition caused by
non-specific granulomatous inflammation of the cavernous sinus, superior orbital fissure and9or
orbital ape#! "he clinical course is characteried by remissions and recurrences!
1 Presentation is %ith diplopia associated %ith ipsilateral periorbital or hemicranial pain!
2 Signs
• Proptosis, if present, is usually mild!
• Ocular motor nerve palsies often %ith involvement of the pupil!
• ensory loss along the distribution of the first and second divisions of the trigeminal
nerve!
3 Treat$ent is %ith systemic steroids!
5egener granulomatosis
5egener granulomatosis may involve the orbit, often bilaterally, usually by contiguous spreadfrom the paranasal sinuses or nasopharyn#! Primary orbital involvement is less common! "he
possibility of 5egener granulomatosis should be considered in any patient %ith bilateral orbital
inflammation, particularly if associated %ith sinus pathology! "he antineutrophilic cytoplasmicantibody (cNC) is a useful serological test!
1 Signs
• Proptosis, orbital congestion and ophthalmoplegia!
• Dacryoadenitis and nasolacrimal duct obstruction!
• Coe#istent manifestations include scleritis, peripheral ulcerative 0eratitis,
intraocular inflammation and retinal vascular occlusions!
2 Treat$ent
a Systemic cyclophosphamide and steroids are very effective! In resistant cases
ciclosporin, aathioprine, antithymocyte globulin or plasmapheresis may be useful!
b Surgical orbital decompression may be re&uired for severe orbital involvement!
Copyright :6++ ;lsevier Inc! ll rights reserved! Eead our "erms and Conditions of 'se and
our Privacy Policy!
If you find this useful please say than0s in your %ay/ dramroo

7/26/2019 tgs mataa1.docx
http://slidepdf.com/reader/full/tgs-mataa1docx 5/5
Close
Print Page
fre&uent cause of proptosis in adults and children is inflammatory pseudotumor! "he term
FpseudotumorF %as coined to indicate a nonneoplastic process that produces the sentinel sign of
an orbital neoplasm, ie, proptosis! In some cases there is an associated systemic vasculitis, such
as 5egenerGs granulomatosis! "he site of inflammation is usually diffuse and not amenable to
e#cision! "he process can be diffuse or localied, specifically involving any orbital structure (eg,
myositis, dacryoadenitis, superior orbital fissure syndrome, or optic perineuritis) or cell type (eg,
lymphocytes, fibroblasts, histiocytes, plasma cells)! "here may be e#tension to involve the
cavernous sinuses and intracranial meninges! Onset is usually rapid, and pain is often present!
Pseudotumor is usually unilateral4 %hen both orbits are involved, it is more often a manifestationof vasculitis! "he differential diagnosis includes <ravesG ophthalmopathy and orbital lymphoma!
"reatment %ith systemic NIDs, systemic corticosteroids, or radiation is usually effective, but
there is a sclerosing variant that is very resistant to treatment! urgery tends to e#acerbate the
inflammatory reaction, but biopsy may be re&uired to confirm the diagnosis in recurrent or
recalcitrant cases