Surviving sepsis campaign
56
Surviving sepsis campaign พพ.พพพพพพพพพ พพพพพพพ
-
Upload
ava-morrison -
Category
Documents
-
view
372 -
download
0
description
Surviving sepsis campaign. พญ.ปัทมาภรณ์ จงเจริญ. Crit Care Med. 2013 Feb;41(2):580-637. 1. What is sepsis. Pitfall. 2. Treat sepsis. 3. 4. Contents. Severe Sepsis. Septic Shock. SIRS. Sepsis. The Sepsis Continuum. - PowerPoint PPT Presentation
Transcript of Surviving sepsis campaign

Surviving sepsis campaign
พญ.ปั�ทมาภรณ์� จงเจร�ญ

Company Logo
Crit Care Med. 2013 Feb;41(2):580-637

Contents
What is sepsis1
Pitfall2
Treat sepsis3
4

The Sepsis Continuum
Chest 1992;101:1644.
SepsisSIRSSevere Sepsis
SepticShock
clinical response arising from nonspecific insult, with 2 of the following: T >38oC or <36oC HR >90 beats/min RR >20/min WBC >12,000/mm3 or
<4,000/mm3 or >10% bands
clinical response arising from nonspecific insult, with 2 of the following: T >38oC or <36oC HR >90 beats/min RR >20/min WBC >12,000/mm3 or
<4,000/mm3 or >10% bands
SIRS = systemic inflammatory response syndrome
SIRS with a presumed or confirmed infectious process
SIRS with a presumed or confirmed infectious process
Sepsis with organ failure Sepsis with organ failure
Refractoryhypotension

Severe sepsis
Company Logo

การดู�แลร�กษาหล�กภาวะการติ�ดูเชื้��อแบคท"เร"ยในร&างกายชื้น�ดู
ร'นแรง
Company Logo

Cycle Diagram
Treat sepsis

Ref: - 2013 41 2 580637Crit Care Med. Feb; ( ): . สรุ�ปโดย JJJJJJJ JJJJJ
Initial resuscitate and infection issue
เปั)าหมายของการชื้&วยให+พ+นภาวะว�กฤติ (resuscitation) ใน 6 ชื้ม. แรกCVP 8 -12 มม.ปรุอทMean arterial pressure (MAP) 65 มม.ปรุอทปรุ�มาณป�สสาวะ 0.5 มล/กก/ชม.SCVO2 or mixed venous oxygen 70%
การให+สารน.�าเล�อก crystalloids เป�นอ�นด�บแรุก ในการุ resuscitationเรุ��ม challenge โดยให้! crystalloid อย"างน!อย 30 มล/กก.

Initial resuscitate and infection issue
DiagnosisCultures as clinically appropriate before antimicrobial therapy if no significant delay (> 45 mins) in the start of antimicrobial(s)
At least 2 sets of blood cultures (both aerobic and anaerobic bottles) be obtained before antimicrobial therapy with at least 1 drawn percutaneously and 1 drawn through each vascular access device, unless the device was recently (<48 hrs) inserted

Initial resuscitate and infection issue
การให+ยาปัฏิ�ชื้"วนะให้!ยาปฏิ�ช%วนะทางห้ลอดเล�อดด&าภายใน 1 ชม. เม��อตรุวจพบว"าเป�น septic shock และ severe sepsisEmpiric combination therapy should not be administered for more than 3–5 days. De-escalation to the most appropriate single therapy should be performed as soon as the susceptibility profile is known Duration of therapy typically 7–10 days; longer courses may be appropriate in patients who have a slow clinical response, undrainable foci of infection, bacteremia with S. aureus; some fungal and viral infections or immunologic deficiencies, including neutropenia Antimicrobial agents should not be used in patients with severe inflammatory states determined to be of noninfectious cause

Hemodynamic support and adjunctive therapy
Fluid Therapy of Severe Sepsis Crystalloids as the initial fluid of choice in the resuscitation of severe sepsis and septic shock
Against the use of hydroxyethyl starches for fluid resuscitation of severe sepsis and septic shock
Albumin in the fluid resuscitation of severe sepsis and septic shock when patients require substantial amounts of crystalloids

Hemodynamic support and adjunctive therapy
Fluid Therapy of Severe Sepsis
Initial fluid challenge in patients sepsis-induced tissue hypoperfusion with suspicion of hypovolemia to achieve a minimum of 30 mL/kg of crystalloids (a portion of this may be albumin equivalent)
Fluid challenge technique be applied wherein fluid administration is continued as long as there is hemodynamic improvement either based on dynamic (eg, change in pulse pressure, stroke volume variation) or static (eg, arterial pressure, heart rate) variables

Hemodynamic support and adjunctive therapy
ยาท"0ชื้&วยในการหดูติ�วของหลอดูเล�อดูและยากระติ'+นการบ"บติ�วของห�วใจ vasopressor and inotropeเล�อก norepinephrine เป�นอ�นด�บแรุก รุ"วมก�บการุให้! epinephrine ห้รุ�ออาจจะให้!แทนเม��อความด�นโลห้�ตท%�ต&�าย�งไม"สามารุถแก!ไขได!
Phenylephrine ไม"แนะน&ายกเว!นว"า norepinephrine ท%�ให้!ม%ความส�มพ�นธ์1ก�บภาวะห้�วใจเต!นผิ�ดปกต�ท%�รุ�นแรุง, ถ!าปรุ�มาณเล�อดท%�ออกจากห้�วใจส3งและความด�นโลห้�ตต&�าอย"างต"อเน��อง ห้รุ�อเป�นล�กษณะแบบก3!ก�บค�น (salvage therapy) เม��อ MAP ไม"ได!ตามเป5าห้มาย
พ�จารุณาให้! dobutamine โดยสามารุถให้!ได!ท%�ขนาด 20 ไมโครุกรุ�ม/กก/นาท% ห้รุ�อเพ��มยาท%�ช"วยในการุห้ดต�วของห้ลอดเล�อดในกรุณ%ท%�ม%ความผิ�ดปกต�ของกล!ามเน�6อห้�วใจห้รุ�อม%การุให้ลเว%ยนโลห้�ตไปย�งเน�6อเย��อลดลงอย"างต"อเน��อง
Ref: - 2013 41 2 580637Crit Care Med. Feb; ( ): . สรุ�ปโดย JJJJJJJ JJJJJ

Hemodynamic support and adjunctive therapy

Hemodynamic support and adjunctive therapy
Dopamine as an alternative vasopressor agent to norepinephrine only in highly selected patients (eg, patients with low risk of tachyarrhythmias and absolute or relative bradycardia)
Low-dose dopamine should not be used for renal protection
All patients requiring vasopressors have an arterial catheter placed as soon as practical if resources are available

Hemodynamic support and adjunctive therapy
คอร�ติ�โคสเติอรอยดู�ไม"ให้!คอรุ1ต�โคสเตอรุอยด1ในกรุณ%ท%�ไม"ได!เก�ดภาวะความด�นโลห้�ตต&�าท%�ด�6อต"อการุรุ�กษา (refractory shock)

Other Supportive Therapy of Severe Sepsis
การให+ส&วนปัระกอบของเล�อดูห้ล�งจากการุให้ลเว%ยนเล�อดไปย�งเน�6อเย��อได!รุ�บการุแก!ไข การุให้!เม7ดเล�อดแดง (PRC) จะให้!เฉพาะกรุณ%ท%� Hb น!อยกว"า 7.0 กรุ�ม/ดล เพ��อให้! Hb อย3"ในช"วง 7.0-9.0 กรุ�ม/ดล ในผิ3!ให้ญ่"
Ref: - 2013 41 2 580637Crit Care Med. Feb; ( ): . สรุ�ปโดย JJJJJJJ JJJJJ

Other Supportive Therapy of Severe Sepsis
Glucose Control protocolized approach to blood glucose management in ICU patients with severe sepsis commencing insulin dosing when 2 consecutive blood glucose levels are >180 mg/dL. This protocolized approach should target an upper blood glucose ≤180 mg/dL rather than an upper target blood glucose ≤ 110 mg/dL
Blood glucose values be monitored every 1–2 hrs until glucose values and insulin infusion rates are stable and then every 4 hrs thereafter
Glucose levels obtained with point-of-care testing of capillary blood be interpreted with caution, as such measurements may not accurately estimate arterial blood or plasma glucose values
Company Logo

Other Supportive Therapy of Severe Sepsis
Bicarbonate Therapy Not using sodium bicarbonate therapy for the purpose of improving hemodynamics or reducing vasopressor requirements in patients with hypoperfusion-induced lactic acidemia with pH ≥7.15

Other Supportive Therapy of Severe Sepsis
Stress Ulcer Prophylaxis Stress ulcer prophylaxis using H2 blocker or proton pump inhibitor be given to patients with severe sepsis/septic shock who have bleeding risk factors
When stress ulcer prophylaxis is used, proton pump inhibitors rather than H2RA
Patients without risk factors do not receive prophylaxis

Indication
Coagulopathy, defined as a platelet count <50,000 per m3, International Normalized Ratio (INR) >1.5, or a partial thromboplastin time (PTT) >2 times the control value
Mechanical ventilation for >48 hours History of GI ulceration or bleeding within the past year Traumatic brain injury, traumatic spinal cord injury, or burn injury Two or more of the following: sepsis, an ICU stay >1 week, occult GI
bleeding for ≥6 days, or glucocorticoid therapy (more than 250 mg hydrocortisone or the equivalent)
Gerald LW,Scott M,Geraldine F,Stress ulcer prophylaxis in the intensive care unit.uptodate.Sep 30, 2013.

The Society of Critical Care Medicine, the European
Society of Intensive Care Medicine, and the
International Sepsis Forum2005







Conclusion

การดู�แลผู้�+ปั3วย Sepsis โดูยใชื้+โปัรแกรม ThaiRefer

อ�ติราการเส"ยชื้"ว�ติ (ร+อยละ) ของผู้�+ปั3วย Sepsis จ�งหว�ดูล.าปัาง
เฉล"0ยติ&อปั5
37.45%
ร+อยละ

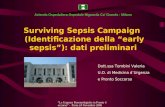
Diagnosis Sepsis
If SBP < 90 mmHg ห้รุ�อ
SBP drop จากเด�ม > 40 mmHg ห้รุ�อMAP < 70 mmHg
: ให+ load initial fluid resuscitation = 0.9%NaCl 30 ml/kg iv bolus (~1,500 ml)
Sepsis-induced
tissue hypoperfusion
1Septic shock : ย�งคงม%ภาวะ Hypotension ห้ล�งจาก load initial fluid resuscitation
2. Severe sepsis with Blood lactate > 4 mmol/L (with any BP)
ให้! Antibiotic ภายใน 1 ช��วโมงSerial vital signs
Serial blood lactate q 4-6 hr
no
yes * Activate Sepsis fast track
Continuous 0.9%NaCl 250-1,000 ml iv boluses
ให+ Antibiotic(s) ภายใน 1 ชื้�0วโมงPlace Central line

CVP
MAP
0.9% NaCl iv load< 10 cmH2O (<8 mmHg)
10-16 cmH2O
(8-12 mmHg)
ScVO2
Vasopressor
Norepinephrine *or Dopamine
> 65 mmHg
< 65 mmHg
Dobutamine
5-20 mcg/kg/min
PRC to keep
Hct > 30 vol%
> 70%
Achieve Goals
> 70%
< 70%ภายใน 6 ชื้�0วโมง(น�บจากเวลาท"0 Diagnosis Sepsis)
Keep CVP 16-20 cmH2O
(12-15 mmHg) (Mech. Vent.)

tube เล�อดูท"0ส.าค�ญใน Sepsis
DTX statCBCBUN/Cr, ElectrolyteH/C x 2 spp.ควร take H/C ก&อน start antibiotic
ท'กราย ยกเว+นถ้+าหากท.าให+เก�ดูความล&าชื้+าในการ start antibiotic เก�น 45 นาท"

ปัร�มาณ์เล�อดูท"0ใส&ในขวดู Hemoculture
อย&างน+อย 10 ml ในแติ&ละขวดู
Mermel LA, Maki DG: Detection of bacteremia in adults: Consequences of culturing an inadequate volume of blood. Ann Intern Med 1993 119270 272; : –

สร'ปั tube เล�อดูในโรคส.าค�ญระบบส&งติ&อจ�งหว�ดู
ล.าปัาง

การส&งติ&อผู้�+ปั3วยโดูยใชื้+โปัรแกรม ThaiRefer v.1.5
upload 16 กรกฎาคม 2556

กดูส&งติ&อเฉพาะโรค “Sepsis”

ข+อม�ลเฉพาะโรค “Sepsis”
ใส& HN รพชื้.

เล�อก visit ล&าส'ดู หร�อ Load ใบส&งติ�วเดู�มไดู+

ข+อม�ลพ��นฐานของผู้�+ปั3วยข:�นอ�ติโนม�ติ�

กรอก V/S, CC/PI, Clinical syndrome
Diagnosis, ICD-10
ข:�นอ�ติโนม�ติ�

กรณ์" Sepsis + BP drop หร�อ Blood lactate > 4 mmol/L จะติ+อง load
NSS อย&างน+อย 30 ml/kg
√√√

กรณ์" load NSS, Dx, start ABO, ท.า central จะข:�นในชื้&อง management โดูยอ�ติโนม�ติ�
อย&าล�มใส&เวลาล+อหม'น

SIRS จะค.านวณ์จาก vital signs โดูยอ�ติโนม�ติ�

ข+อม�ลย�งปัรากฏิใน tab “ส&งติ&อท�0วไปั” โดูยอ�ติโนม�ติ�ดู+วย

Sepsis Management in Emergency Department
(รพ.ปัลายทาง)


อย&าล�มลงเวลาในดู+านซ้+ายม�อดู+วยนะคร�บ

ความหมายของเวลาในแติ&ละชื้&วงDx. Sepsis
เวลาท"0 recognition ว&าผู้ปั.สงส�ยม"ภาวะ sepsis
Start ABO
เวลาท"0เร�0มฉ"ดู antibiotic หร�อ drip เข+ากระแสโลห�ติ
ท.า central lineเวลาท"0เร�0มฉ"ดูยาชื้า เม�0อเร�0มห�ติถ้การ central line
CVP ไดู+ goal
CVP = 10-16 cmH20 (8-12 mmHg), (16-20 cmH20) (12-15
mmHg) (Mech. Vent.)MAP ไดู+ goal ScV02 ไดู+ goal Urine output
ไดู+ goal
MAP > 65 mmHg ติ�ดูติ&อก�น> 1 ชื้�0วโมงเปั<นติ+นไปัScV02 > 70%
Urine output > 0.5 ml/kg/hr

การบ�นท:กเวลาใน Sepsis Bundles
at ICU/RCU/ ward

ICU/RCU/ward จะลงเวลา Sepsis Bundles ให+
Sepsis Bundles
เวลาในแติ&ละชื้&วง
ค.านวณ์อ�ติโนม�ติ�

เล�อก Final Clinical syndrome ก&อน แล+วกดูปั'3ม Analyzeจะท.าการ
ว�เคราะห�ติามติ�วชื้"�
ว�ดู√
25

Acknowledgement
ค'ณ์เอกร�ฐ บ�รณ์ถ้าวรสม น�กว�ชื้าการคอมพ�วเติอร�คณ์ะกรรมการ sepsis โรงพยาบาลล.าปัางท'กท&าน

Take home message
BP drop Load NSS อย&างน+อย 30 ml/kg ก&อนพ�จารณ์า vasopressorLevophed (Norepinephrine) is preferedติ+อง H/C x 2 spp. ก&อน start Antibiotic H/C เล�อดูใชื้+อย&างน+อย 10 ml ติ&อขวดูแนะน.าเจาะเล�อดู peripheral x 2 site ติ&างติ.าแหน&งก�นกรณ์" severe sepsis + septic shock ติ+องให+ antibiotic ภายใน 1 ชื้ม . (หล�งจาก Dx)อย&าล�มลงเวลาในแติ&ละข��นติอน