
Spi res Cleft Lip and · study to develop a patient‐reported outcome measure for cleft lip and/or...
26
Spi Lip Pal Cen Annua ires p an late ntre al Repor Cle nd e rt 2014/1 eft 15
Transcript of Spi res Cleft Lip and · study to develop a patient‐reported outcome measure for cleft lip and/or...

SpiLipPalCenAnnua
ires p anlate ntreal Repor
Clend
e rt 2014/1
eft
15
The Spire
The CentrHubs. Othcloser to h
Salisbury FOdstock RSalisbury SP2 8BJ
es Cleft Lip
re comprisesher services home by eith
Foundation NRoad
and Palate
s of two sitese.g., speech
her local spec
NHS Trust
Centre. htt
s (Hubs) shoh therapy, ocialist clinicia
tp://www.s
wn below –orthodonticsans or those
spirescentre
patients rec and ENT m from the Hu
OxfHeaOxfOX
e.nhs.uk/
ceive their sumay be provubs.
ford Universadley Way ford 3 9DU
urgery at eacided at the
ity Hospital T
ch of the Hubs or
Trusts
1

2 Spire Cleft Lip and Palate Team
Stephen Robinson – Clinical Director / Orthodontic Consultant
Norma Patterson – Network Service Manager
Clinical Team – Oxford Clinical Team ‐ Salisbury
Tim Goodacre ‐ Primary surgeon Michael Cadier – Primary surgeon
Marc Swan – Primary surgeon Tim Flood – Secondary surgeon
Andrew Currie – Secondary surgeon Steve Robinson–Consultant orthodontist
Giles Kidner – Consultant orthodontist Marcel Geyer – ENT Consultant
Penny Lennox – ENT Consultant Nichola Hudson – Lead Nurse Specialist
Sandip Popat – Consultant in Restorative dentist Maureen Warren – Nurse Specialist
Tina O’Neill – Nurse Specialist Ginette Phippen – Lead Speech therapist
Jane Sibley – Nurse Specialist Fiona Jeyes – Principal Speech therapist
Emma Waterworth – Nurse Specialist Sandra Treslove – Speech therapist
Carrie Luscombe–Principal Speech therapist Catherine Caterall –Speech therapist
Lucy McAndrew – Speech therapist Cindy Williams – Speech therapy assistant
Sarah Kilcoyne – Speech therapist /research assistant
Jane Lewendon – Clinical psychologist Mary‐Ann Brewer – Co‐ordinator
Helen Piggott – Speech therapist Teresa Rodgers – Cleft secretary
Lucy Southby – Speech therapist Janet Orriss – Cleft secretary
Louise Dalton – Lead psychologist
Sian Thomas – Clinical psychologist
Debbie Clarke – Research assistant
Steven Berry – Co‐ordinator
Lorraine Linekar – Cleft secretary
Kayleigh Preston – Cleft secretary
Vicky Ludlow – Junior Cleft secretary
3
CONTENTS
Executive summary ………………………………………………………………………………………………………… 4
Summary of achievements ……………………………………………………………………………………………. 5
Management/administration ……………………………………………………………………………………………. 6
SPECIALITY REPORTS
Nursing ………….. …………………………………………………………………………………………… 7
Surgery ………….. …………………………………………………………………………………………… 9
Clinical psychology …………………………………………………………………………………………… 11
Speech and Language therapy ………………………………………………………………………………. 15
Dental ………………………………………………………………………………………………………… 17
Research ………………………………………………………………………………………………………… 19
Publications ………………………………………………………………………………………………………… 21
Objectives for 2015 ………………………………………………………………………………………………………… 23
Appendix 1
Centre activity 2007‐2014 …………………………………………………………………………………………… 24

4
Executive summary
2014 saw the tenth anniversary of the formation of the current 9 regional cleft centres in England and Wales following the recommendations set out in the CSAG report of 1998. Those who have been around long enough to observe the developments over the last ten years have seen great changes in treatment pathways and subsequent improvement in patient outcomes which can now be seen as Key Performance Indicators on our Quality Dashboard.
One of our main achievements in 2014 was hosting the Annual Scientific Craniofacial Conference at Keble College in Oxford. Our national and international speakers created great interest amongst our cleft colleagues and we received very positive feedback on a successful conference. Great thanks must go to Steven Berry, Co‐ordinator in Oxford, his excellent organisational skills and attention to detail enabled the 3 days to run smoothly and this was acknowledged in the post conference evaluation – thank you Steven!
The team experienced several staff changes and some long term absence during the year but with the support of the wider team we experienced minimal disruption to our clinics and surgical activity. Our commitment to research at Spires has culminated this year in the recruitment of a part time research assistant at each site to support our growing portfolio of studies, we are fortunate that both successful applicants have a knowledge of cleft which enables the recruitment process to studies to be more streamline and hopefully more successful. Their main objective during the year was to recruit to the Cleft Collective Study, a large prospective collection of DNA from family trios for the study of genetic and environmental determinants of cleft lip/ and or palate. There was continued recruitment to TOPS (Timing of Palatal Surgery) study and we hope to start recruitment shortly to Cleft Q – an international study to develop a patient‐reported outcome measure for cleft lip and/or palate.
Work has continued nationally to improve the quality of our data collection for the dashboard and it is hoped that during the next twelve months the outcomes will be published on the Craniofacial Society website.
We would like to say thank you to Spires Smiles, a local charity in Salisbury and surrounding area who have given great support to us over the year and all those who have kindly donated to Spires this year.
Summary
Resear
Educat
Audit
Patienexperie
of achievem
rch
•Appothe c•Deveour a
ion
•Hosti•Furth
t
•Tri ce
nt nce
•Bi‐anhowe
ments in 201
ointment of resentreeloping our Reseapproach to res
ing a successfuher two Speech
entre audit with
nnual 'HowRweever there is alw
4/15
earch assistant
earch strategy/search more str
l Craniofacial So and language t
h our colleague
' data collectedways room for
t at both sites to
/ Research Boarructure
ociety of Great therapists com
es in Birmingham
d at both sites rimprovement i
o co‐ordinate o
rd/ Research Ne
Britain and Irepleted MSc and
m and South W
eflects our conn clinic waiting
our research act
etwork meeting
land Conferencd postgraduate
West
tinuing patient times!
tivities across
gs which gives
cee studies
t satisfaction
5

6
Management/ administration
As ever we have had a busy year in the admin offices in both Salisbury and Oxford. In Oxford we recruited a new part time member to the team to support the additional work from our orthodontic, maxillofacial and restorative dental colleagues. Both teams during the last year have worked with colleagues in the Oral & Maxillofacial service to improve communication across the teams, make the patient pathway more efficient and ultimately enhance the patient experience.
As part of this work the Oxford team will be linking with a project addressing the transition for young people into adult care – ‘Ready Steady Go’ devised by Dr Arvind Nagra at Southampton Hospital. Staff will be attending a workshop and training sessions to facilitate this award winning programme.
Our surgical workforce took on a new look during the year with the addition of a new cleft surgeon Mr Marc Swan, primarily based in Oxford. Having an addition to the surgical team, whilst maintaining part time hours from our senior surgeons Mr Michael Cadier and Mr Tim Goodacre enabled us to maximise capacity across both sites and from September we rotated both our Oxford based surgeons to our Salisbury site to support Michael Cadier. This has maximised our theatre usage and also contributed to the reduction of waiting times for Salisbury patients. We have continued through the year to review our clinic provision and processes to maintain as smooth an out‐patient service as possible.
Whilst the Oxford site has been challenged with recruitment of paediatric nursing staff which has had a knock on effect to available surgical beds, we have been very fortunate and managed to maintain our surgical activity throughout the year.
The addition of Marc Swan to the team has brought a fresh approach to research within the team and the initiation of a Research Board, which Marc will report on later.
7 Speciality reports
Nursing
The nursing team has now had full establishment for a year with each nurse continuing to cover their own clinical caseload by geographical area for the Spires service. They continue to provide weekend cover across the network ensuring all new born referrals have an assessment by a specialist to provide optimum care and early discharge to the community.
In line with the nursing KPI’s for the quality dashboard the initial CNS contact for both our antenatal and postnatal referrals are high this year and show improvement on previous data. On analysis of cleft classification data babies with a Forme Fruste have been recorded as if the cleft was an incomplete cleft lip. This degree of clefting would not be expected to be diagnosed at a 20 week scan and therefore the family would not be assessed by a member of the team. These figures have been removed for data analysis to enable an accurate response rate for the nursing team.
We continue to have delayed detection for infants born with an isolated cleft palate. Although rates have improved the impact on families can be significant and require ongoing support and management. It is noted that some infants may have co morbidities and therefore a later referral is appropriate. However, again we have had babies aged from 9 days to 3 years of age children referred to the team in 2014.
The CNS team have shared information re: delayed detection with the RCPCH working group to enable a UK perspective of detection rates. The Lead CNS from the SW West team has represented the nurse CEN and we now have information for both clinicians and parents available on appropriate diagnosis and referral to the national centres. There will be further audit and ongoing work with this group.
Unfortunately in April the Lead nurse sustained an injury and was unable to carry out clinical duties for 6 months of 2014. During this time the CNS team worked tirelessly to cover the whole geographical area and supporting one another to ensure new referrals continued to be seen. Providing this level of care was seen as a priority but impacted on agreed objectives and necessary development of the nursing service. Home visits for some families had to be reduced with some impact on care. Some families with a recent antenatal diagnosis also had to be seen at the hospital site as opposed to the family home, impacting both in the quality of care and increasing burden on families.
During this time North Hampshire was designated as an area covered by the Oxford nurses. But dependent on the actual geographical area could be cared for by either site.
Training /education
All areas both at the hub and at our referral units have education form the CNS team, either as adhoc sessions or more formal agreements.
Ongoing development of patient information for both inpatient and outpatient care.
8
Nichola co‐opted tutor for Manchester cleft course.
All the team continue to help in the development of the service:
All CNS ‘s attended the Craniofacial Conference in Oxford with nurse representatives and presentations at the Autumn Clinical Excellence Network (CEN ) in Manchester.
Emma Waterworth presented to the CEN which was well received. Jane Sibley presented a paper at conference; ‘MRI for definitive in utero diagnosis of cleft palate a useful adjunct to antenatal care’. This is planned for publication in 2015.
Maureen Warren presented a poster at conference ‘Great Things Can Come From Humble Beginnings: ‐ The 6C's and written information for parents and children ‐ a way forward. She continues to lead as editor for the working party on our parent booklet, a group including Tina and other members of the MDT.
Nichola Hudson and Jane Sibley attended the consensus meeting in Utrecht on Robin sequence. Further meetings in 2015/16 for further discussion.
Tina O’Neill continues to represent the team on the national audit/research group. Jane Sibley co‐ordinates the national CEN newsletter. Nichola Hudson continues both with the national steering groups, Clinical Reference Group and Cleft Development Group.
Following a request from The Craniofacial Society for nominations for Lead nurse representation for SLUMBR study, Nichola Hudson has been accepted as part of the study group. The initial work will be ongoing with a feasibility study starting 2015 in the Northern and North West teams.
Nichola Hudson
Lead Clinical Nurse Specialist

9
Surgery
The past year has probably seen the most major change in surgical service structure and provision since the network was formed. Much planning has been devoted to introducing new expertise into the team as the two senior surgeons approach retirement age. As the first stage of this, the team were delighted to welcome the appointment of Marc Swan to the position of Cleft and Plastic Surgeon following a lengthy and rigorous selection procedure during 2014. Marc trained at St Mary’s Hospital in London, and subsequently undertook a plastic surgical training which included experience at Mount Vernon and the Oxford – Wessex region. He has also spent a period of full time research into the novel area of tissue expansion using material science collaborations, with the award of a DPhil (Oxford’s equivalent of a PhD) in 2008. Marc therefore brings with him a wealth of understanding and drive to improve the scientific basis of our work, one immediate effect of which has been his instigation of a regular research board structure for the network. He does, however, have an impeccable background in cleft surgical management, having spent a year at the Hospital for Sick Children (SickKids) in Toronto and another year at Great Ormond Street in London, as well as visiting distinguished surgical teams in Boston, India and elsewhere during his training. He has been warmly welcomed by the team and patients alike, and we know that his arrival heralds a truly new era for the better in our surgical provision in the Spires network.
Marc began working at Spires in September, which allowed Tim Goodacre to begin to step down from shouldering the full role of surgeon at the Oxford hub – after over 23 years of managing the caseload single‐handedly. Tim ‘retired and returned’ in April 2014, on reduced sessions, supporting succession planning and allowing more flexibility in surgical cover. One aspect of this has been to modify the service structure to allow Michael Cadier at the Salisbury hub to reduce his sessional commitment as he takes up the prestigious national role as President of BAAPS (the British Association of Aesthetic Plastic Surgeons). In March, Tim Goodacre began operating at Salisbury alongside Marc Swan and Michael Cadier, allowing further alleviation of the service pressures which have built up over a period of time at that site. This new arrangement continues to work well, and has enabled Marc Swan to spend longer in Oxford developing his strategic aims on a more sound footing.
The surgical team continue to develop approaches to best practice which include several research projects that have been presented at national and international meetings. These include exploring the potential for robotic assisted surgery for aspects of intraoral work that involve manoeuvres which are technically demanding (and sometimes impossible) for the human hand unaided. At the other extreme, Tim Goodacre joined a small group of surgeons from Kings Hospital on a short UK government funded visit to Gaza in November to support reconstructive surgery for war injured. One aspect of the new organisation of the Spires surgical team is that it will offer greater flexibility in
10
maximising the use of available operating resources despite external commitments as well as periods of leave. We are grateful for the welcome acceptance of changes in surgical consultant by our patients and family groups, and will continue to try to support them all by ensuring that continuity of care is maintained despite these new arrangements.
Tim Goodacre
Cleft surgeon

11
Clinical Psychology
The Clinical Psychology Service provides specialist psychological assessment and interventions across the lifespan, through attendance at multi‐disciplinary clinics, administration of national protocols for psychological assessment and intervention for pre‐ and post‐surgery, direct referrals to Psychology and the use of screening and audit to identify individuals and families in need.
Staffing Update
There have been a number of key staffing changes to the Psychology team in 2014. We were sorry to say goodbye to Jane Lewendon, after 10 years with the Salisbury team; we are very grateful for the enormous contribution that she has made to the service and wish her well in her new post in Paediatrics at Salisbury District Hospital. We also said farewell and a heartfelt thank you to Angela Shanly at the end of her two year locum as Lead Psychologist for Spires. Finally, at the end of the year we wished Sian Thomas the very best of luck as she started her maternity leave.
Louise Dalton re‐joined the service as Lead Psychologist in November 2014, following her career break working on the SPOCCL research project. Louise was joined in Oxford by Dr May Quarmby, who has been with the team two days per week since March 2015. We are also delighted to welcome Dr Corin le Huray to the Salisbury team since January 2015; she is with us full time and brings valuable previous experience from the South West Cleft team.
Clinical Activity
Members of the Psychology Service aim to attend multi‐disciplinary clinics with the aim of screening for psychological concerns, providing immediate psychological advice and facilitating patients’ consultation with the wider cleft team. We monitor our activity in clinic using a scoring system which grades the extent of our involvement with each patient and therefore provides a snap shot of psychological need for clinic attenders.
In 2014 the Oxford Psychology team attended over 330 consultations with patients in MDT clinics. Analysis of our records indicates psychological input was required for 39% of these patients. This ranged from immediate psychological problem solving and advice, to follow up appointments and liaison with schools or other services.
Education and Training
Angela Shanly, Sian Thomas and Jane Lewendon attended the Craniofacial Society of Great Britain and Ireland conference hosted in Oxford in April. The programme included an update on the SPOCCL project and a review of psychological data collection and needs of cleft patients.

12
Sian Thomas provided teaching to the Oxford Doctoral Course in Clinical Psychology on Appearance Related Issues in Paediatrics. Louise Dalton remains on the Board of Examiners for the Oxford Doctoral Course.
Routine data collection, Outcomes and Quality Dashboard
The psychology team continues to work closely with colleagues across the UK around routine collection of audit data. The audit clinics are a clinically important opportunity for our team to screen for psychological distress and difficulties, in addition to providing a chance to look ahead for anticipated developmental challenges (e.g. transfer to secondary school, coping with questions about the cleft) with families and discuss potential coping strategies or useful resources.
Comparison of anonyms outcome data at these time points with colleagues from other cleft centers is of great importance in evaluating service quality and provision. This takes place on an annual basis at the Tri centre audit meetings. One of the many challenges we face is how to evaluate the data we routinely collect, both practically and clinically. As psychologists we use several extensive questionnaires which assess progress in a number of different domains, including behavior, peer relationships, self‐esteem and emotional wellbeing, in addition to cleft specific areas, such as subjective satisfaction with speech, hearing and appearance. This results in a large volume of data, which at present needs to be manually entered onto a database – an enormous and time consuming task! Secondly, we need to make clinical sense of the data, both for an individual patient, but also in terms of comparing outcomes for larger patient cohorts. Psychological health is multi‐faceted; this means that quoting one ‘outcome’ for patients is extremely difficult, as so many factors may contribute to an individual’s score on a questionnaire. For example, a score indicating low self‐esteem may be directly related to the way someone feels about their cleft, or may be entirely attributable to difficulties at home. This has implications for how we should evaluate psychological services, particularly on the Quality Dashboard and Psychology Key Performance Indicator (KPI).
A national decision was made to use ‘seen for a psychological screen by age 6’ as the Psychology KPI. Within the Spires service, we expect to achieve 100% and indeed hope to see all new parents before their child’s first surgery, in addition to routine screening at multi‐disciplinary clinics, 18month and 5 year audit clinics. This provides an opportunity to evaluate a child and their family’s psychosocial well‐being at a number of regular time intervals when development and change is so rapid. Secondly, these appointments are critical to introduce and normalize the role of psychology within the team, so that should difficulties arise in‐between these time points, parents have met the psychology team, are aware of our remit and will feel able to pro‐actively contact the team regarding concerns before difficulties become entrenched.
13
Plans for 2015/16
The staffing changes towards the end of the year have left the team temporarily very short staffed, with skeleton cover for clinics and a waiting list of patients needing psychological input. However, we hope that with our new team in place and established by April 2015, we can carry out a strategic review of the different ways in which the psychology service contributes to the patient pathway and set out our objectives for the next three years. This is likely to include examination of comprehensive screening protocols for psychological need, especially around procedural anxiety, the use of psychological resources and skills in MDT clinics and evaluation of our routine audit data collection. In due course we will also be considering how the clinical experience and results of the SPOCCL study influence the way we should support new families, in partnership with our Clinical Nurse Specialist colleagues.
We will re‐instate routine data collection of our outpatient, inpatient, MDT clinic and telemedicine activity. We also hope to make progress on considering how technology may help with some of the challenges of data collection and analysis, although this will need financial and technological support.
Dr Louise Dalton
Lead Clinical Psychologist
Supporting Parents of Children with Cleft Lip (SPOCCL)
The clinical team is still closely involved with the SPOCCL project, which has now recruited 48 mothers and infants to the study. Mothers are randomized into one of the trial arms, either ‘Watch and Discover’ which focuses on early mother/infant interaction, or ‘Support, Information and Advice’, which offers specific psychological advice and support. Dr Nicene Overkill has taken over from Louise Dalton as the trial therapist and offers each participating family for 6 home visits to deliver the SPOCCL intervention.
The first few families, recruited when the infant was aged 2 weeks, have now received the final assessment visit as their babies are now 18months of age. This lengthy follow up period means that the final results of the study will not be available for some time to come, but enables the research team to monitor both the short term and longer term effects of the two types of therapy. The
14
research team are delighted that both ‘Watch and Discover’ and ‘Support, Information and Advice’ have been very well received by participants. It is clear that there is a psychological need among participants, and the significant amount of psychological input has been very helpful for families. The study has also demonstrated very high retention of the research participants, which is a further reflection of its acceptability and value to parents.
The SPOCCL study was presented at the Surgical Grand Round at the John Radcliffe Hospital and also to the annual meeting of the Craniofacial Society of Great Britain and Ireland.

15
Speech and Language Therapy
2014/15 was a year of SLT staff changes due to maternity leave, illness and moving on for promotion. The team demonstrated great resilience and mutual support during this unsettled period with minimal service disruption. This was supported by the successful recruitment of experienced temporary and permanent specialist SLT staff. We have worked closely with our colleagues in the multidisciplinary team as well as providing ongoing liaison and support for our colleagues in community SLT services across the region.
Achievements:
1. The SLT team continues to carry out audit, research and service development activities on an individual and team basis:
Two team members completed MSc and postgraduate studies and another is working on a NIHR Clinical Doctorate Research Fellowship application.
We joined the Cleft Collective Cohort Studies; a national longitudinal study investigating outcomes for children and families.
Our SLT assistant was successful in applying for a research assistant secondment post to support the Cleft Collective and TOPS studies.
We continued to recruit to the international TOPS (Timing of Palate Surgery) trial and carry out collection of speech data for analysis.
2. We contributed to the successful Craniofacial Society of Great Britain & Ireland Conference, hosted by Spires and held in Oxford.
3. We collaborated with the Cleft Lip and Palate Association (CLAPA) to run a Superheroes day for families at the Arts Centre in Salisbury. The event was run by Hoodwink Theatre Company and funded by CLAPA. Families attended for a fun day of arts activities including costume making, storytelling, animation and superhero challenges.
16
4. We submitted speech outcome data for the pilot national Quality Dashboard commissioned by NHS England.
5. We completed the production of two DVDs for parents entitled ‘Show me a Sound’ and ‘Say and Play Together’. These DVDs demonstrate activities to promote speech and language development in very young children with cleft palate. These resources will be made available nationally via the Spires website and through CLAPA.
6. We received positive feedback from community Salts where we have provided outreach support for second opinion assessment and therapy in settings close to children’s homes.
7. We implemented a rolling programme of centre based therapy sessions. These are available throughout the year for young children as well as older children with persisting speech difficulties. Children are able to attend individually, with a therapy ‘buddy’ or as part of a group.
Quality The team monitors service delivery using an annual self‐evaluation cycle framework which includes a range of service areas and performance indicators. This is modified each year to reflect priority areas and has developed a culture of critical thinking and peer review, with an expectation that existing service models will be challenged on an on‐going basis. In 2014 there was a focus on maintaining effective service levels during recruitment to vacant posts and maternity leave as well as finalising the parent DVD resources.
The priority objectives for 2015/16 are;
1. To review and streamline SLT case note procedures in order to reduce duplication and increase efficiency and quality, with reference to information governance policies and guidelines.
2. To produce and publicise a Spires SLT Training Strategy that outlines the variety of training available from the specialist SLT team.
3. To develop a training course for specialist Salts: Instrumental Diagnostic and Therapy Approaches in Cleft Palate.
4. To write a series of SLT intervention case studies for peer‐reviewed publication.
Ginette Phippen
Lead Speech & Language Therapist

17
Dental
The levels of tooth decay amongst young children has recently become a political issue with nearly 26,000 children, aged between 5‐9 years, being admitted to hospital in England in 2013‐14 for extractions. Dental health in children with clefts continues to be a major concern for all cleft teams in the UK. We have pursed a policy at the Spires for targeting children and parents at the earliest possible opportunity with all members of the team promoting a healthy diet, good oral hygiene and visiting the local dentist for the first time before the age of 2 years when most of the deciduous dentition has become established. We are required by the national service specification to report on our dental health outcomes aged 5 years using the DMFT measure (decayed, missing or filled teeth.)We have reported good outcomes over the last few years with dental health in the cleft cohort being comparable with local epidemiological data. We would expect about 65% of the cohort to be caries free with a mean DMFT score of 1.15. The bulk of the decay is concentrated in a small group of children with very high DMFT scores. We are determined to improve our outcomes in the future and as part of that programme will target known vulnerable groups in the network for the early support and intervention. Developments planned include a dental therapist and dental health educator within the service to fulfil these aims.
The development of a national service specification and quality dashboard by NHS England will result in outcomes being published on a quarterly basis through their website allowing the general public to compare cleft centres throughout England. Measures for dental health through DMFT, orthodontic care using PAR (Peer Assessment Rating), maxillary growth through dental occlusion and the timing of alveolar bone grafting are all included within the dashboard. The QD covers all aspects of multidisciplinary cleft care and will evolve over the next few years to include parental and patient views which are a welcome development.
We have continued to develop our cleft orthodontic training scheme which exposes the trainee to the spectrum of work carried out by the MDT team rather than concentrating on orthodontics alone. During the next 12 months we will be working with a visiting orthodontist from Nigeria as part of programme designed to establish a national orthodontic service for children.
Access to restorative dentistry is variable when the different cleft centres are compared. A national specialist group of restorative dentists in cleft care has recently been established and should lead to an improvement in access over the next few years. They are currently undertaking a survey of all UK cleft centres looking for shortfalls in service and personnel. There is a continuing need for a prosthetic service to support adults with residual velopharyngeal incompetence despite surgical intervention. This service has been developed and established in both Oxford and Salisbury over the last few years for this small group of important patients.
18
Research is an important area of our work and we continue to participate in national and local research projects where dental and orthodontic input is required. We have recently been involved in a retrospective review of alveolar bone grafting in bilateral cleft of lip and palate which should be published next year and have also been involved in several presentations and lectures at national and international conferences over the last 12 months.
Steve Robinson
Lead Orthodontist

19
Research
It has been a huge privilege to join the Spires Cleft team and the welcome that I have had from
colleagues, patients and families alike has been very humbling. The coming decades will be an
extremely exciting time for us all and part of that will be developing the research strategy within the
Spires community.
We have some exceptional clinicians working at Spires and in partnership with our patients I am
confident that we can continue to develop our research portfolio at both a national and international
level. We recognise that improvements in cleft care come, in part, through robustly designed research
studies; remarkably much of what we practice in cleft surgery is based on historical dogma with little
evidence to support it! As one of the regional cleft centres in the United Kingdom we must continue to
collaborate with the Cleft and Craniofacial Clinical Studies Group in order to improve the quality of
research such that it answers the questions most frequently raised by patients and parents – as
detailed in the James Lind Alliance priority setting partnership.
As evidenced from the pages of this Annual Report there is clearly no shortage of enthusiasm for
research within Spires – we are currently committed to the Timing of Palatal Surgery Trial, the UK Cleft
Collective and the Supporting Parents of Children with Cleft Lip Study to name but a few. Cindy
Williams and Debbie Clarke have been working unceasingly as our Research Assistants across the two
sites and have allowed us to communicate better with families and to enhance the coordination of our
research activities at a grassroots level.
The cornerstone to developing our research strategy is the creation of the Cleft Research Board with
the remit to promote and co‐ordinate research excellence within Spires. We are delighted to have the
invaluable and insightful input of Trevor Holcroft as our lay representative on the Research Board. A
Research Network Meeting will be held every four months and will bring the entire Spires team
together to share ideas, develop projects and to ensure that all of our research output is truly
multidisciplinary. Of course quality research requires concrete funding and we are incredibly grateful
to those whom have donated to the Spires Research Fund over the past year and we hope that we can
persuade you to support some of our future projects in due course!

20
Priorities for 2015 include the introduction of our Transoral Robotic Surgery (TORS) programme for
secondary speech surgery, the development of our cleft database to incorporate real‐time data entry
through a patient‐iPad interface, field‐testing the CLEFT‐Q patient reported outcome measure and to
collaborate with the International Consortium on Health Outcomes Measurement (ICHOM) to develop
international standards in cleft surgery based on those outcomes that matter most to patients. We will
also be working with colleagues in the Division of Cardiovascular Medicine with the aim of quantifying
the clefting phenotype of patients with Loeys‐Dietz Syndrome. As always we hope to submit a number
of papers to the Annual Scientific Meeting of the Craniofacial Society of Great Britain and Ireland and
to work towards the 2017 International Cleft Conference in Chennai.
Marc C. Swan
Cleft Surgeon
21
Publications/ Abstracts/ Posters
2014
1. Songs from the Outback: The Effectiveness of Music in Treating Articulation Disorders in Children Aged 2–5 Years with Cleft Palate and Velopharyngeal Dysfunction S C Kilcoyne et al ASHA SIG Cleft Perspectives. 2014
2. Intraoperative high dose epinephrine infiltration in cleft palate repair
M C Swan et al J Craniofacial Surg.2014 Jan: 25 (1):140‐2
3. Identifying the effect of cleft type, deprivation and ethnicity speech and dental outcomes in UK cleft patients: A multi‐centred study Choa RM, Slator R, Jeremy A, Robinson S, Franklin D, Roberts A, Extence H, Collard M & Clark V. JPRAS (International Journal of Surgical Reconstruction). December 2014, 67, 12, 1637‐1643
2015
1. Early Orthopaedic Retraction of the Premaxilla in Bilateral Complete Cleft Lip and Palate: An Innovative Approach to a Difficult Problem, Mahmood R, Flood T, Robinson S and Al‐Gholmy M. Cleft Palate Craniofac J. 2015 Feb: 3
2. Comparative study of the aesthetic outcome of two techniques for unilateral complete cleft lip
repair, Phillips G, Sawyer A, Goodacre T, Swan MC, Cadier M. Abstract Craniofacial Conference 2015
3. Revision palatoplasty: early experience with unilateral buccinators flap and partial Sommerlad‐
Furlow procedure, Goodacre T, Swan MC, Coventry D. Abstract Craniofacial Conference April 2015
4. The novel use of Bio‐Alcamid in augmentation pharyngoplasty for the treatment of
Velopharyngeal Insufficiency. Khan K, Treslove S, Cadier M. Abstract Craniofacial Conference April 2015
5. The bipedicaled bilateral cleft lip repair: a novel technique, Sawyer A, Phillips G, Swan MC,
BoormanJ, Cadier M. Abstract Craniofacial Conference April 2015

22
6. ICHOM (International Consortium for Health Outcomes Measurement): A patient‐ centred clinical outcomes set for Cleft. Thorburn TG, Swan MC, Kelley T, Jones Y, Williams C, van Eden S, Goodacre T, Kangesu L. Abstract Craniofacial Conference April 2015
7. Patient reported impact on speech following orthognathic surgery in patients with cleft palate.
Li, Treslove and Flood. Poster, Abstract Craniofacial Conference April 2015
8. 17p 13.3 Microduplication, a Potential Novel Genetic Locus Palate Ibitoye RM, Roberts J, Goodacre T. Cleft Palate Craniofac J. 2015 May: 52, 3, 359‐362
9. Kapur‐Tonella Syndrome: a further case report and expansion of phenotype
Lefroy H, Goodacre T and Kini U. Clin Dysmorphol 2015 June 5. Epub 2015
Objective
im
R
E
Com
es for 2015/
Servicprovem
Researc
Educati
mmissio
/16
e ment
ch
on
oning
•Review oudisciplinary•Improving service and
•Member oNIHR Clinic•Field testin
•Host netwin cleft car•To host a t
•Whilst awacommissiowe will revfor the ser
r pathways iny settingour transitiond working wit
of the Speech cal Doctorate ng the Cleft Q
work study dayre in the regiotraining cours
aiting the outoning and whaview our perforvice
n each clinical
n for our younh project lead
and languageResearch \Fe
Q patient repo
y in Oxford forone for specialis
come of propat impact thatormance again
speciality and
ng patients intd on 'Ready, S
e team workinllowship Applrted outcome
r all professio
st Speech ther
posed changest may have onnst national st
d multi
to the adult Steady,Go'
ng towards licatione measure
nals involved
rapists
s in specialist n the service tandards set
2
23
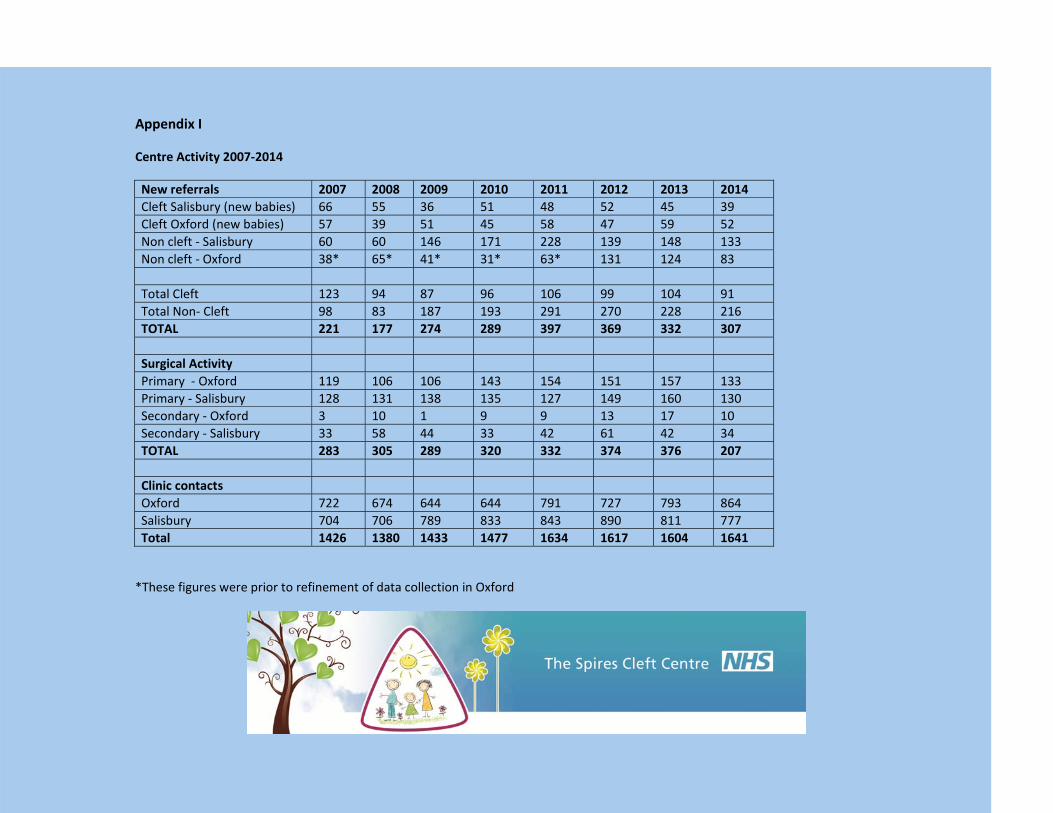
Appendix I
Centre Activity 2007‐2014
*These figures were prior to refinement of data collection in Oxford
New referrals 2007 2008 2009 2010 2011 2012 2013 2014 Cleft Salisbury (new babies) 66 55 36 51 48 52 45 39 Cleft Oxford (new babies) 57 39 51 45 58 47 59 52Non cleft ‐ Salisbury 60 60 146 171 228 139 148 133Non cleft ‐ Oxford 38* 65* 41* 31* 63* 131 124 83 Total Cleft 123 94 87 96 106 99 104 91Total Non‐ Cleft 98 83 187 193 291 270 228 216 TOTAL 221 177 274 289 397 369 332 307 Surgical Activity Primary ‐ Oxford 119 106 106 143 154 151 157 133 Primary ‐ Salisbury 128 131 138 135 127 149 160 130 Secondary ‐ Oxford 3 10 1 9 9 13 17 10 Secondary ‐ Salisbury 33 58 44 33 42 61 42 34TOTAL 283 305 289 320 332 374 376 207 Clinic contacts Oxford 722 674 644 644 791 727 793 864 Salisbury 704 706 789 833 843 890 811 777 Total 1426 1380 1433 1477 1634 1617 1604 1641


















![Ang Bingot (cleft lip o cleft palate) [Pananaliksik]](https://static.fdocument.pub/doc/165x107/552029d24a79595e718b467b/ang-bingot-cleft-lip-o-cleft-palate-pananaliksik.jpg)