SITO PERIS-SDSC 21-22 Aprile 2017 Aggiornamenti sugli ...€¦ · Sally Ibbotson10, Ketty Peris11,...
29
Istituto di Dermatologia Università Cattolica, Roma Ketty Peris SCUOLA DERMATOLOGICA S E R G I O C H I M E N T I Aggiornamenti sugli algoritmi terapeutici per la cheratosi attinica
Transcript of SITO PERIS-SDSC 21-22 Aprile 2017 Aggiornamenti sugli ...€¦ · Sally Ibbotson10, Ketty Peris11,...

Istituto di DermatologiaUniversità Cattolica,
Roma
Ketty Peris
Segreteria Organizzativa
SCUOLA DERMATOLOGICA
S E R G I O C H I M E N T I
MEETMEETERERcongressi
Il presente programma è soggetto e deposito AIFA ai sensi e per gli effetti di cui all’art. 124 del D. Lgs 219/06. Il Provider Meeter Congressi Srl è accreditato dalla Commissione Nazionale ECM a fornire programmi di formazione continua per Medici Chirurghi e si assume la responsabilità per i contenuti, la qualità e la correttezza etica di questa attività.
ISCRIZIONIPer iscriversi inviare una e-mail a: [email protected] nome, cognome e titolo dell’Eventooppure chiamare il numero 06 33680034
Segreteria Organizzativa
Tel. [email protected] - www.meeter.it
MEETMEETERERcongressi
ROMA, 10 - 11 APRILE 2017
LESIONI INFIAMMATORIE E NEOPLASTICHE DELLA CUTEPoliclinico di Roma Tor Vergata Aula Anfiteatro Piano -1, Viale Oxford 81
Responsabili scientificiKetty Peris, Luca Bianchi, Maria Concetta Fargnoli
Assegnati 7 crediti ECMAggiornament i sug l i a lgor i tmi terapeut ic i per
la cheratos i att in ica

v Eradicate as many clinical and subclinical AK lesions as
possible
v Achieve clinical remission that is as prolonged as possible
v Provide a good cosmetic result
v Prevent the progression to invasive SCC
Goals of AK therapy

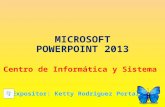
Treatment algorithm for actinic keratosis
Stockfleth et al EJD 2008
+
Diagnosis of AK
High risk actinic keratosis(e.g. immunosuppressed
and/or high risklocation levels)
Actinic keratosis
Solitary lesionsMultiple lesions(high number
concentrated in asmall area) or history
of multiple lesions
Refer to adermatologistfor a specificmanagement
Lesion and fielddirected treatment
recommended
Lesiondirected
treatment
CryotherapyLaser therapy
Surgery*All + Sun protectionTreatment of lesion
and surrounding skin/field(Diclofenac 3% gel
lmiquimodPDT5-FU)
All + Sun protection
Diclofenac 3% gellmiquimod
PDT5-FU
All + Sun protection
Chemical peelsRetinoids
All + Sun protection
Specialist pathwayGP pathway
*Histological investigation isrecommended before surgery
Treatment Options
Lesion Evaluation
Figure 1. Treatment algorithm for actinic keratosis.
EJD, vol. 18, n° 6, November-December 2008 653

in these patients. AK treatment should be considered before
organ transplantation. A regular clinical follow-up is carried out
by the dermatologist for early detection and treatment of these
lesions. In addition, patient education on skin self-examination is
fundamental and allows delaying the development of potential
cancerous lesions in transplant patients.64
Monitoring and secondary preventionPatients with AK should be monitored regularly because of the
chronic nature of lesions and an invasive SCC should be
detected as early as possible.
In patients at risk, the monitoring rate proposed is at least a
yearly consultation. During these consultations, the patient
should be educated on the need for reconsulting earlier if any
lesion changes rapidly or in case of recurrence after treatment.
Organ transplant patients must be managed in a particular way,
especially in terms of personalized monitoring.
Sun protective clothing and behaviour, and the use of sun-
screen products (chemical or mineral filters), should be recom-
mended to patients to minimize the worsening of
photo-induced skin damage and to prevent skin cancer. It has
been demonstrated that sunscreen is an effective AK prevention
method. Applying sunscreen (greater than SPF-15 applied every
2–3 h) reduces the risk of AK lesions by up to 24% over time,
even compared with beta-carotene and topical tretinoin cream
0.05%. The AAD (Amercian Association of Dermatology) states
that selecting a sunscreen with broad-spectrum cover (UVB/
UVA) is vital and that daily use of an SPF-30 product is recom-
mended on all exposed skin before daylight exposure.65–68
ConclusionsThe objective of this expert panel report was to provide a prag-
matic solutions for dermatologists in terms of diagnosis, monitor-
ing and a treatment algorithm that they could use in their daily
practice, based on data from the literature and former guidelines.
AcknowledgementsWe would like to thank Dr Maxime Battistella, Service de
Pathologie de l’Hopital Saint Louis in Paris, for his help in the
writing of this article.
Isolated AK
Non-hyperkeratotic AK
HyperkeratoticAK
SuspiciousAK
Non-hyperkeratotic AK
HyperkeratoticAK
Multiple AK
Evaluation of lesions
1st li
ne2nd
line
. Cryotherapy . Curettage / electrocoagulation
. Surgery if recurrence / resistance
*Confirmation of diagnosis of actinic keratosis (AK): Refer to treatment algorithmAK, actinic keratosis
. Physical treatments combined with topical treatments or surgery
. Cryotherapy . Curettage / electrocoagulation
. Biopsy + exeresis . Biopsy *
. Topical treatments -5% 5-fluorouracil -3% diclofenac sodium -5% imiquimod -150 g/g and 500 g/g ingenol mebutate . Physical treatments -laser -photodynamic therapy
. Resurfacing -manual -salicylic acid/urea
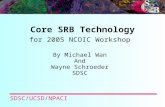
Figure 2 Treatment algorithm proposed by the experts for actinic keratosis management, depending on lesion number and appearance.
© 2014 European Academy of Dermatology and VenereologyJEADV 2014, 28, 1141–1149
Management of actinic keratosis 1147
TREATMENT ALGORITHM FOR AK MANAGEMENT, DEPENDING ON LESION NUMBER AND APPEARANCE
Dreno B, Amici JM, Basset-‐Seguin N, Cibier B, Claudel JP, Richard MA. JEADV 2014

should be noted that, after removal of hyperkeratosis with the
application of salicylic acid or thiourea, all topical therapies can
be effectively used on such lesions.
Among field-directed therapies, only IngMeb, IMQ 5% 4
week, DF/HA and MAL-PDT are available in Italy. Both pla-
cebo-controlled and head-to-head RCTs demonstrated the effi-
cacy of field-directed treatments in eliminating visible lesions,
subclinical lesions, patches of fast-growing atypical keratinocytes
within CF and decreasing recurrence rates.12 Achievement of
such intermediate endpoints is thought to translate in lower
iSCC rates. However, no long-term study has definitely proven
such well-found assumption.
The evidence base for both lesion-directed and field-directed
therapies is summarized in Appendix S1. Overall, there is a wide
variation in clearance rates across studies of the same treatment
modality, which complicates the interpretation of each RCT in
the light of the pre-existing evidence. Such variation might be
explained by heterogeneity in study design, case mix, follow-up
period, outcome definition and ascertainment methods. Ideally,
a parallel group randomized controlled trial should assess the
comparative efficacy of all options available. A phase IV RCT
comparing the clinical and pharmaco-economic outcomes of
IngMeb, IMQ 5%, MAL-PDT and 5-FU [RCT ID:
NCT02281682] along with several head-to-head RCTs are ongo-
Yes
No
Clinical diagnosis of AK
Alarm signs?
Lesion density
≥3 AK/25 cm2*
Body region
Face/scalp
Olsen III
Grade
Trunk/extremities
≤2 AK/25 cm2*
Excision and histology
1st choice: cryotherapy
Alternatives:• Curettage• CO2 laser therapy• Elettrodessiccation and
curettage
Olsen I/II
1st choice:• IngMeb**• IMQ 5%• MAL-PDT
Alternative: • DF/HA
Olsen III
1st choice:• Cryotherapy/curettage + IngMeb• Cryotherapy/curettage + IMQ 5%• Curettage + MAL-PDT
Alternative: • Cryotherapy/curettage + DF/HA• Remove hyperkeratosis (i.e.
salicylic acid, thiourea) + IngMeb, or DF/HA or IMQ 5%
Olsen I/II
1st choice:• IngMeb**• MAL-PDT
Alternative: • DF/HA
1st choice:• Cryotherapy/curettage + IngMeb• Curettage + MAL-PDT
Alternative: • Cryotherapy/curettage + DF/HA• Remove hyperkeratosis (i.e.
salicylic acid, thiourea) + IngMeb, or DF/HA or IMQ 5%
Grade
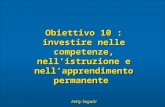
Figure 1 Treatment algorithm. *Field-directed therapies may also be considered for a large single lesion when its borders cannot bedelimited accurately or in patients who failed previous treatments with cryotherapy (i.e. recurrence in the same area within 12 months).**Single or multiple cycles depending on the extent of the affected area.
© 2016 European Academy of Dermatology and VenereologyJEADV 2016
Italian expert consensus for the management of AK 5
Peris K et al. JEADV 2015
Trunk/extremitiesFace/scalp
*Field-‐directed therapies may also be considered for a large single lesion when its borders cannot be delimited accurately or in patients who failed previous treatments with cryotherapy (i.e. recurrence in the same area within 12 months). **Single or multiple cycles depending on the extent of the affected area

S3 Guidelines recommendationsDecreasing strength of recommendation
Weak
NO
Single AK lesions (≤5)
Multiple AK lesions ≥6
Field cancerization
Immuno-‐compromisedpatients with AK
Cryotherapy
Curettage0.5% 5-‐FU/5% 5-‐FU0.5% 5-‐FU + 10% SA3.75% imiquimod5% imiquimod
Ingenol mebutateMAL-‐PDT/ALA-‐PDT
Cryotherapy3% diclofenac in 2.5% HA
5% 5-‐FU0.5% 5-‐FU + 10% SA
5% imiquimod2.5% imiquimod
CO2-‐laser, Er:YAG-‐laser
Cryotherapycurettage5% 5-‐FU
5% imiquimodMAL-‐PDT/ALA-‐PDT
3% diclofenac2.5% imiquimodCO2-‐laser Er:YAG-‐
laser
Curettage3% diclofenac0.5% 5-‐FU
0.5% 5-‐FU + 10% SA2.5%/3.75% imiquimod
Ingenol mebutate
Strong
3.75% imiquimodMAL-‐PDT/ALA-‐PDT
0.5% 5-‐FUIngenol mebutate 0.015%-‐0.05%
ILDS and EDF JEADV 2015 Sunprotection in all patients subgroups

https://doi.org/10.1177/1203475417702994
Journal of Cutaneous Medicine and Surgery 1 –14
© The Author(s) 2017Reprints and permissions:
sagepub.com/journalsPermissions.navDOI: 10.1177/1203475417702994
jcms.sagepub.com
Actinic keratosis (AK) is mainly caused by chronic ultravio-let (UV) radiation exposure and is characterised by scaly or keratotic erythematous lesions.1 Incidence increases with age and is highly dependent on individuals’ geographical locations and skin types, as well as behaviours regarding sun exposure.2 It is estimated that, in Australia, between 11% and 40% of white people older than 40 years have some form of AK.3 Besides the cosmetic burden associated with AK, there is the risk that lesions, regardless of their clinical grade, will progress to squamous cell carcinoma (SCC).4-6 With global ageing, AK will increasingly become a focus for health care systems.7
Although numerous scientific publications on AK exist, uncertainties remain regarding the definition of AK as precancerous or in situ SCC and with respect to disease severity classification according to, for example, the Olsen grading system. Investigating these questions is among the aims of this study. The introduction of new treatments for AK has improved the standard of care for patients.8 However, many guidelines place an emphasis exclusively on clinical efficacy and safety, without accounting for practical issues. These include considerations such as the required treatment duration, adherence of patients to overly complex treatment regimens, compliance of frail patients to treatments with side
Original Article
702994 CMSXXX10.1177/1203475417702994Journal of Cutaneous Medicine and SurgeryCalzavara-Pinton et alresearch-article2017
Structured Expert Consensus on Actinic Keratosis: Treatment Algorithm Focusing on Daylight PDT
Piergiacomo Calzavara-Pinton1, Merete Hædersdal2, Kirk Barber2, Nicole Basset-Seguin4, María Emilia Del Pino Flores5, Peter Foley6, Gaston Galimberti7, Rianne Gerritsen8, Yolanda Gilarbete9, Sally Ibbotson10, Ketty Peris11, Sheetal Sapra12, Eleni Sotiriou13, Luis Torezan14, Claas Ulrich15, Jonathan Guillemot16, 17, Janek Hendrich16, and Rolf-Markus Szeimies18
AbstractBackground: A practical and up-to-date consensus among experts is paramount to further improve patient care in actinic keratosis (AK).Objectives: To develop a structured consensus statement on the diagnosis, classification, and practical management of AK based on up-to-date information.Methods: A systematic review of AK clinical guidelines was conducted. This informed the preparation of a 3-round Delphi procedure followed by a consensus meeting, which combined the opinions of 16 clinical experts from 13 countries, to construct a structured consensus statement and a treatment algorithm positioning daylight photodynamic therapy (dl-PDT) among other AK treatment options.Results: The systematic review found deficiencies in current guidelines with respect to new AK treatments such as ingenol mebutate and dl-PDT. The Delphi panel established consensus statements across definition, diagnosis, classification, and management of AK. While the diagnosis of AK essentially rests on the nature of lesions, treatment decisions are based on several clinical and nonclinical patient factors and diverse environmental attributes. Participants agreed on ranked treatment preferences for the management of AK and on classifying AK in 3 clinical situations: isolated AK lesions requiring lesion-directed treatment, multiple lesions within a small field, and multiple lesions within a large field, both requiring specific treatment approaches. Different AK treatment options were discussed for each clinical situation.Conclusions: The results provide practical recommendations for the treatment of AK, which are readily transferable to clinical practice, and incorporate the physician’s clinical judgement. The structured consensus statement positioned dl-PDT as a valuable option for patients with multiple AKs in small or large fields.
Keywordsactinic keratosis, consensus, treatment algorithm, Delphi methodology
AK definition/diagnosis and factors influencing AK treatment decision making
A set of 3 clinical cases whereby participants wererequired to assess the nature of AK, list their preferredmanagement options, and express their view on the appropriateness of dl-‐PDT use

4 Journal of Cutaneous Medicine and Surgery 00(0)
their preferred management options, and express their view on the appropriateness of dl-PDT use. The latter question was included due to the absence of dl-PDT in existing guide-lines, as demonstrated in the literature review.
The one-off questionnaire and Delphi panel were com-municated and collected via email and included 8 and 33 questions, respectively. Sixteen clinical experts were selected on the basis of their expertise on AK and their ability
to constitute a worldwide panel, represented by scientific contributions (peer-reviewed journal articles and conference keynotes) and/or clinical expertise in regards to high number of AK patients treated and/or number of AK-related clinical trials they had participated in as an investigator over the pre-vious 5 years.
A list of treatment options for the management of AK was developed from the outputs of the Delphi panel and the sys-tematic review of treatment guidelines. This was presented to the Delphi panel participants during a consensus meeting,
Figure 2. Photograph representing clinical case 1. Source: DermQuest.com.
Table 2. Systematic Literature Review Methodology and Search Results.
Description
Search details Databases searched MEDLINE
MEDLINE-in-ProcessEMBASE
Limits Population: Patients with AKIntervention: No restrictionComparator: No restrictionOutcomes: Multitreatment recommendations for management of AKStudy Type: Clinical guidelines from recognised large organisations, consensus statements
Hand searches Dermatology organisations, relevant conference abstracts/posters (from 2012)Inclusion criteria Conference abstracts of interest: published 2012-2015
Study type of interest: Treatment guideline or recommendationPopulation of interest: Patients with AKOutcome of interest: Recommendations for the management of AKLocations of interest: European Union, Latin America, Australia, Canada
Exclusion criteria Duplicate, not in the language of interest (English), abstract that is reported elsewhereSearch resultsNumber of references identified through
the systematic literature searches609
Number of references identified through the hand searches
3
Number of articles included in the systematic review
9
AK, actinic keratosis.
Figure 3. Photograph representing clinical case 2. Source: DermQuest.com.
4 Journal of Cutaneous Medicine and Surgery 00(0)
their preferred management options, and express their view on the appropriateness of dl-PDT use. The latter question was included due to the absence of dl-PDT in existing guide-lines, as demonstrated in the literature review.
The one-off questionnaire and Delphi panel were com-municated and collected via email and included 8 and 33 questions, respectively. Sixteen clinical experts were selected on the basis of their expertise on AK and their ability
to constitute a worldwide panel, represented by scientific contributions (peer-reviewed journal articles and conference keynotes) and/or clinical expertise in regards to high number of AK patients treated and/or number of AK-related clinical trials they had participated in as an investigator over the pre-vious 5 years.
A list of treatment options for the management of AK was developed from the outputs of the Delphi panel and the sys-tematic review of treatment guidelines. This was presented to the Delphi panel participants during a consensus meeting,
Figure 2. Photograph representing clinical case 1. Source: DermQuest.com.
Table 2. Systematic Literature Review Methodology and Search Results.
Description
Search details Databases searched MEDLINE
MEDLINE-in-ProcessEMBASE
Limits Population: Patients with AKIntervention: No restrictionComparator: No restrictionOutcomes: Multitreatment recommendations for management of AKStudy Type: Clinical guidelines from recognised large organisations, consensus statements
Hand searches Dermatology organisations, relevant conference abstracts/posters (from 2012)Inclusion criteria Conference abstracts of interest: published 2012-2015
Study type of interest: Treatment guideline or recommendationPopulation of interest: Patients with AKOutcome of interest: Recommendations for the management of AKLocations of interest: European Union, Latin America, Australia, Canada
Exclusion criteria Duplicate, not in the language of interest (English), abstract that is reported elsewhereSearch resultsNumber of references identified through
the systematic literature searches609
Number of references identified through the hand searches
3
Number of articles included in the systematic review
9
AK, actinic keratosis.
Figure 3. Photograph representing clinical case 2. Source: DermQuest.com.
Calzavara-Pinton et al 5
and a final treatment algorithm was produced upon agree-ment of the expert panel.
Results
Systematic Review of GuidelinesSearches identified 612 citations for screening via database and hand searches, and 9 treatment guidelines or consensus statements published between 2007 and 2015 were ulti-mately extracted (Table 2).11,12,16-22 A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram of the study flow is given in Appendix 3.
Where stated, all guidelines agreed that UV exposure was the most important causative factor for AK. Accordingly, high sun protection factor (SPF) sunscreen was recom-mended as a preventative measure in several guide-lines.11,16,18,22 Further UV avoidance behaviours recommended by guidelines included minimising peak-time exposure to the sun (11:00 AM to 3:00 PM), wearing of broad-brimmed hats outdoors, and avoidance of artificial tanning.11,22,23
Within the reviewed guidelines, low consensus existed on the definition of the condition in terms of AK status as a can-cer in situ or a precancerous lesion. AK was described as a premalignant or precancerous lesion in 3 guidelines.16,17,22 Other guidelines regarded AK as either in situ SCC or as a form of early stage SCC.12,18-21 Guidelines showed consensus in stating that a substantial risk exists for an AK lesion to progress to invasive SCC. Several guidelines produced guid-ance on grading AK severity. The Olsen grading system, or Röwbert-Huber classification, for AKs was used in some
guidelines,11,19 while others did not report specific guidance for assessing the severity of AK.12,16,17,21,22
A full summary of treatment recommendations across the guidelines is given in Appendix 4. For the medical and pro-cedural management of isolated AK, the strongest recom-mendations made, by way of the frequency and strength of recommendation, were for cryotherapy, curettage, and con-ventional photodynamic therapy (c-PDT). The weakest rec-ommendations were made for 5-fluorouracil (5-FU) and imiquimod. Recommendations relating to curettage were found to be contradictory across guidelines, with guidelines applying a strong recommendation, weak recommendation, or no stated recommendation; as such, no consensus conclu-sion could be made from this evidence. For the management of multiple AK lesions, the strongest recommendations were made for c-PDT and 5-FU, then imiquimod and ingenol mebutate. The weakest recommendations were made for cryotherapy and laser therapies.8,12,16-22 Results associated with cryotherapy are highly dependent on the physician’s experience and skills, hence the recommendation variations for cryotherapy.
Critical assessment of the extracted guidelines was per-formed using the AGREE II guideline evaluation tool. Three guidelines scored perfectly,11,12,22 and there were no major methodological concerns for the remaining guidelines (see Appendix 2). However, reporting of strength of evidence was found to be incomplete in a minority of guidelines.17,20 The recent introduction of ingenol mebutate, imiquimod 3.75%, 5-FU combined with salicylic acid, and dl-PDT also rendered all guidelines obsolete, as none fully reflected the full spectrum of currently available treatments.8 In addition, some guidelines identified in this review provided recom-mendations restricted to specific geographical areas.18,20 Some guidelines were also compromised by ignoring practi-calities associated with treatment, including patient ability to comply with treatment, as well as the overall duration/complexity of the treatment cycle. Certain guidelines imposed an overly theoretical approach to treatment, such as proposing AK maximal treatable area thresholds of 25 cm2, which is not a realistic threshold in clinical practice as a cheek and forehead represent 100 to 150 cm2 and a bald scalp extends over 200 cm2.17,18 Some guidelines also advised 4-week treatment courses (eg, 5-FU, 3.75% imiqui-mod),8 with likely physician follow-up visits afterwards—a prolonged treatment period that would likely prove difficult for some patients.11,12,16-22 Finally, specific management for immunosuppressed patients was not addressed in some treatment guidelines.16,22
One-Off Questionnaire and Delphi PanelSixteen clinical experts with extensive experience on AK participated in the Delphi panel. Over the past 5 years, par-ticipants reported a median of 75 AK patients seen on a monthly basis, 11 AK-related publications, 25 AK-related
Figure 4. Photograph representing clinical case 3. Source: Department of Dermatology, University of Brescia, Brescia, Italy.Cryotherapy
C-PDTImiquimod5-FU
Ingenol Mebutate
ISOLATED AK I/II MULTIPLE AK I-‐III IN AN AREA OF FIELD CANCERIZATION
C/dl-PDT5-FU
ImiquimodIngenol Mebutate
MULTIPLE AK I-‐III AND FIELD CANCERIZATION
C/dl-PDT5-FU
Imiquimod

Calzavara-Pinton et al 9
Table 8. Findings for the Assessment, Treatment, and Use of dl-PDT for Clinical Cases 1, 2, and 3.a
Assessment Treatment dl-PDT Use
Clinical case 1—round 3
Isolated AK grades I/II with uncertainty regarding field cancerisation.
(CL: 10)
Although there is a risk of hypopigmentation, cryotherapy is among the first treatment options. Then (order varies) c-PDT, imiquimod or 5-FU, and ingenol mebutate.
(CL: 8)
dl-PDT (most often to the whole face) is more appropriate when there are multiple AKs and/or suspecting a cancerisation field. In the case of single lesions, more practical alternatives are preferable. Reimbursement status may affect the use of dl-PDT.
(CL: 9)Clinical case
2—round 3Multiple AK grades I, II,
and III in an area of field cancerisation.
(CL: 10)
Biopsy is considered for thick lesions. Prior to treatment, field preparation using curettage is required. First option for treatment is c-PDT, then (order varies) dl-PDT or 5-FU. Last, imiquimod and ingenol mebutate may be used.
(CL: 9)
dl-PDT is appropriate for the thinner lesions. Thicker lesions must be treated separately and prior to dl-PDT.
(CL: 10)
Clinical case 3—round 3
Multiple AK grade I/II and field cancerisation.
(CL: 10)
Field treatment is required, with preferably dl-PDT but also c-PDT, imiquimod, and 5-FU.
(CL: 9)
Yes. This choice may depend on dl-PDT reimbursement status and sun exposure (season/location).
(CL: 10)
AK, actinic keratosis; CL, consensus level; c-PDT, conventional photodynamic therapy; dl-PDT, daylight photodynamic therapy; 5-FU, 5-fluorouracil.aExact questions asked: ‘The following three questions are clinical cases. On the basis of the following pictures, please assess the clinical features of AK and the most appropriate treatment to provide. Please assume that patients are not immunocompromised. (1) Clinical assessment of clinical case 1/2/3. (2) What are the most appropriate treatments for clinical case 1/2/3? (3) Is daylight PDT relevant for clinical case 1/2/3?’
Figure 5. Treatment algorithm for the management of AK. AK, actinic keratosis; PDT, photodynamic therapy; SPF, sun protection factor.

• Published data from RCT are the “goldstandard” evidence to support the treatment
recommendations

EMA-‐approved topical therapies for AKTHERAPY AK
TYPETxAREA
TREATMENT REGIMEN DURATION LESIONCLEARANCE (%)
-‐ 5% 5-‐FU-‐ 0.5% 5-‐FU + 10% salycilic acid
25 cm2 Twice dailyOnce daily
2-‐4 weeksUp to 12 wks
75-‐88
Imiquimod 5% cream
I-‐II 25 cm2 3 times a week for 4 wks4 wks off and 4 wks on, if needed
4 weeks 75.7
Imiquimod 3.75% cream
I-‐II 100-‐200 cm2
Daily 2 weeks on, 2 weeks off, 2 weeks on
2 + 2 weeks 92.2
Ingenol mebutate150-‐500 mcg/g gel
I-‐II 25 cm2 Face/scalp: 0.015% once daily for 3 consecutive days Trunk/extremities: 0.05% once daily for 2 consecutive days
2-‐3 days 75-‐83
Diclofenac 3% gel ns Twice daily 60-‐90 days 54-‐63
c/dlPDT 100 cm2 Prepare skin. Apply cream 3 hours under occlusion prior to illumination
1 day 82-‐91
Peris et al. 2015, 2016; Pellacani 2015, Fargnoli 2015, Dirschka 2016

Factors that drive treatment choice in real life clinical practice
Number Thickness Distribution
Lesion characteristics

Factors that drive treatment choice
• Age (comorbidites)• Ability to perfom home-‐based treatment• Patient’s immune status• Adherence to the Tx regimen• History of previous treatment
Patient variables
• Availability of drugs/procedure• Dermatologist experience

REVIEW ARTICLE
Real-world approach to actinic keratosis management: practical treatmentalgorithm for office-based dermatology
Thomas Dirschkaa, Girish Guptab, Giuseppe Micalic, Eggert Stockflethd, Nicole Basset-S!eguine,V!eronique Del Marmolf, Reinhard Dummerg, Gregor B. E. Jemech, Josep Malvehyi,j, Ketty Perisk, Susana Puigi,j,Alexander J. Stratigosl, Iris Zalaudekm and Giovanni Pellacanin
aCentroderm Clinic, Wuppertal, and Faculty of Health, University of Witten-Herdecke, Witten, Germany; bDepartment of Dermatology,Monklands Hospital, Lanarkshire, and University of Glasgow, Glasgow, UK; cDermatology Clinic, University of Catania, Catania, Italy; dKlinik f€urDermatologie, Venerologie und Allergologie, St. Josef-Hospital, Ruhr-Universit€at Bochum, Bochum, Germany; ePoliclinique de Dermatologie,Hopital Saint-Louis, Paris, France; fDepartment of Dermatology, Hopital Erasme – Universit!e Libre de Bruxelles, Bruxelles, Belgium; gDepartmentof Dermatology Skin Cancer Unit, University Hospital Z€urich, Zurich, Switzerland; hDepartment of Dermatology, Zealand University Hospital,Roskilde; Health Sciences Faculty, University of Copenhagen, Copenhagen, Denmark; iDermatology Department, Melanoma Unit, Hospital Cl!ınicde Barcelona, IDIBAPS, Universitat de Barcelona, Barcelona, Spain; jCentro de Investigaci!on Biom!edica en Red en Enfermedades Raras (CIBERER),Valencia, Spain; kDepartment of Dermatology, Catholic University of Rome, Largo A. Gemelli 8, Rome, Italy; lFirst Department of Dermatology-Venereology, University of Athens Medical School, Andreas Sygros Hospital, Athens, Greece; mNon-Melanoma Skin Cancer Unit, Department ofDermatology and Venereology, Medical University of Graz, Graz, Austria; nDepartment of Dermatology, University of Modena and Reggio Emilia,Modena, Italy
ABSTRACTActinic keratosis (AK) is a chronic skin disease in which multiple clinical and subclinical lesions co-existacross large areas of sun-exposed skin, resulting in field cancerisation. Lesions require treatment becauseof their potential to transform into invasive squamous cell carcinoma. This article aims to provide office-based dermatologists and general practitioners with simple guidance on AK treatment in daily clinicalpractice to supplement existing evidence-based guidelines. Novel aspects of the proposed treatment algo-rithm include differentiating patients according to whether they have isolated scattered lesions, lesionsclustered in small areas or large affected fields without reference to specific absolute numbers of lesions.Recognising that complete lesion clearance is rarely achieved in real-life practice and that AK is a chronicdisease, the suggested treatment goals are to reduce the number of lesions, to achieve long-term diseasecontrol and to prevent disease progression to invasive squamous cell carcinoma. In the clinical setting,physicians should select AK treatments based on local availability, and the presentation and needs of theirpatients. The proposed AK treatment algorithm is easy-to-use and has high practical relevance for real-life,office-based dermatology.
ARTICLE HISTORYReceived 3 August 2016Accepted 23 October 2016Published online 11 Novem-ber 2016
KEYWORDSDiclofenac; fieldcancerisation; 5-fluorouracil;imiquimod; ingenolmebutate; photodynamictherapy
Introduction
Actinic keratosis (AK) is a chronic skin lesion, which principallyarises due to long-term sun-exposure (1–3). As ultraviolet radiationaffects the entire sun-exposed area of skin, clinically visible AKlesions are surrounded by subclinical or invisible lesions resultingin field cancerisation (Figure 1) (4,5). AK lesions can be consideredas early in situ squamous cell carcinoma (SCC) and part of a dis-ease continuum that can progress into invasive SCC (1–3).Furthermore, subclinical and early AK lesions may also be associ-ated with invasive SCC, suggesting that these lesions may also dir-ectly transform into invasive disease (6). Estimates from clinicalstudies indicate that 0.025–16% of AK lesions may progress toinvasive SCC per year (7), although there are currently no estab-lished biomarkers to predict which subclinical or clinical lesionswill progress and when this progression will occur. However,based on clinical experience, it is evident that there is an associ-ation between AK lesions and invasive SCC, which is stronger witha greater number of AK lesions, suggesting a risk of transform-ation (8). Consequently, guidelines recommend that all AKs needto be adequately treated (9).
The prevalence of AK and the clinical and economic burden ofthe disease are expected to rise substantially over the comingdecades (10,11). This is because AK mainly affects elderly peoplewho have had chronic lifetime sun exposure (with an estimatedprevalence of 34% of men and 18% of women in Europe agedover 70 years) (12), and due to the increasingly ageing globalpopulation. The prevalence of the disease varies widely betweendifferent countries with the highest prevalence seen in Australia(40–60% of adults) (13). In some countries, AK is considered to bean occupational disease for those who work outside (14). Otherrisk factors for the development of AK include male gender, fairskin type and immunosuppression (15–17).
The recently published global S3 guidelines from theInternational League of Dermatological Societies (ILDS) andEuropean Dermatology Forum (EDF) provide evidence-based rec-ommendations for the treatment of AK (9). Published data fromrandomised clinical trials (RCTs) are considered to be the “gold-standard” evidence to support the treatment recommendations.However, these RCTs typically include a highly selected homoge-neous population of patients due to their strict eligibility criteria
CONTACT T. Dirschka [email protected] CentroDerm GmbH, Heinz-Fangman-Straße 57, D-42287 Wuppertal, Germany! 2016 Informa UK Limited, trading as Taylor & Francis Group
JOURNAL OF DERMATOLOGICAL TREATMENT, 2016http://dx.doi.org/10.1080/09546634.2016.1254328
REVIEW ARTICLE
Real-world approach to actinic keratosis management: practical treatmentalgorithm for office-based dermatology
Thomas Dirschkaa, Girish Guptab, Giuseppe Micalic, Eggert Stockflethd, Nicole Basset-S!eguine,V!eronique Del Marmolf, Reinhard Dummerg, Gregor B. E. Jemech, Josep Malvehyi,j, Ketty Perisk, Susana Puigi,j,Alexander J. Stratigosl, Iris Zalaudekm and Giovanni Pellacanin
aCentroderm Clinic, Wuppertal, and Faculty of Health, University of Witten-Herdecke, Witten, Germany; bDepartment of Dermatology,Monklands Hospital, Lanarkshire, and University of Glasgow, Glasgow, UK; cDermatology Clinic, University of Catania, Catania, Italy; dKlinik f€urDermatologie, Venerologie und Allergologie, St. Josef-Hospital, Ruhr-Universit€at Bochum, Bochum, Germany; ePoliclinique de Dermatologie,Hopital Saint-Louis, Paris, France; fDepartment of Dermatology, Hopital Erasme – Universit!e Libre de Bruxelles, Bruxelles, Belgium; gDepartmentof Dermatology Skin Cancer Unit, University Hospital Z€urich, Zurich, Switzerland; hDepartment of Dermatology, Zealand University Hospital,Roskilde; Health Sciences Faculty, University of Copenhagen, Copenhagen, Denmark; iDermatology Department, Melanoma Unit, Hospital Cl!ınicde Barcelona, IDIBAPS, Universitat de Barcelona, Barcelona, Spain; jCentro de Investigaci!on Biom!edica en Red en Enfermedades Raras (CIBERER),Valencia, Spain; kDepartment of Dermatology, Catholic University of Rome, Largo A. Gemelli 8, Rome, Italy; lFirst Department of Dermatology-Venereology, University of Athens Medical School, Andreas Sygros Hospital, Athens, Greece; mNon-Melanoma Skin Cancer Unit, Department ofDermatology and Venereology, Medical University of Graz, Graz, Austria; nDepartment of Dermatology, University of Modena and Reggio Emilia,Modena, Italy
ABSTRACTActinic keratosis (AK) is a chronic skin disease in which multiple clinical and subclinical lesions co-existacross large areas of sun-exposed skin, resulting in field cancerisation. Lesions require treatment becauseof their potential to transform into invasive squamous cell carcinoma. This article aims to provide office-based dermatologists and general practitioners with simple guidance on AK treatment in daily clinicalpractice to supplement existing evidence-based guidelines. Novel aspects of the proposed treatment algo-rithm include differentiating patients according to whether they have isolated scattered lesions, lesionsclustered in small areas or large affected fields without reference to specific absolute numbers of lesions.Recognising that complete lesion clearance is rarely achieved in real-life practice and that AK is a chronicdisease, the suggested treatment goals are to reduce the number of lesions, to achieve long-term diseasecontrol and to prevent disease progression to invasive squamous cell carcinoma. In the clinical setting,physicians should select AK treatments based on local availability, and the presentation and needs of theirpatients. The proposed AK treatment algorithm is easy-to-use and has high practical relevance for real-life,office-based dermatology.
ARTICLE HISTORYReceived 3 August 2016Accepted 23 October 2016Published online 11 Novem-ber 2016
KEYWORDSDiclofenac; fieldcancerisation; 5-fluorouracil;imiquimod; ingenolmebutate; photodynamictherapy
Introduction
Actinic keratosis (AK) is a chronic skin lesion, which principallyarises due to long-term sun-exposure (1–3). As ultraviolet radiationaffects the entire sun-exposed area of skin, clinically visible AKlesions are surrounded by subclinical or invisible lesions resultingin field cancerisation (Figure 1) (4,5). AK lesions can be consideredas early in situ squamous cell carcinoma (SCC) and part of a dis-ease continuum that can progress into invasive SCC (1–3).Furthermore, subclinical and early AK lesions may also be associ-ated with invasive SCC, suggesting that these lesions may also dir-ectly transform into invasive disease (6). Estimates from clinicalstudies indicate that 0.025–16% of AK lesions may progress toinvasive SCC per year (7), although there are currently no estab-lished biomarkers to predict which subclinical or clinical lesionswill progress and when this progression will occur. However,based on clinical experience, it is evident that there is an associ-ation between AK lesions and invasive SCC, which is stronger witha greater number of AK lesions, suggesting a risk of transform-ation (8). Consequently, guidelines recommend that all AKs needto be adequately treated (9).
The prevalence of AK and the clinical and economic burden ofthe disease are expected to rise substantially over the comingdecades (10,11). This is because AK mainly affects elderly peoplewho have had chronic lifetime sun exposure (with an estimatedprevalence of 34% of men and 18% of women in Europe agedover 70 years) (12), and due to the increasingly ageing globalpopulation. The prevalence of the disease varies widely betweendifferent countries with the highest prevalence seen in Australia(40–60% of adults) (13). In some countries, AK is considered to bean occupational disease for those who work outside (14). Otherrisk factors for the development of AK include male gender, fairskin type and immunosuppression (15–17).
The recently published global S3 guidelines from theInternational League of Dermatological Societies (ILDS) andEuropean Dermatology Forum (EDF) provide evidence-based rec-ommendations for the treatment of AK (9). Published data fromrandomised clinical trials (RCTs) are considered to be the “gold-standard” evidence to support the treatment recommendations.However, these RCTs typically include a highly selected homoge-neous population of patients due to their strict eligibility criteria
CONTACT T. Dirschka [email protected] CentroDerm GmbH, Heinz-Fangman-Straße 57, D-42287 Wuppertal, Germany! 2016 Informa UK Limited, trading as Taylor & Francis Group
JOURNAL OF DERMATOLOGICAL TREATMENT, 2016http://dx.doi.org/10.1080/09546634.2016.1254328

Clinical spectrum of AK
AK patients usually present with multiple clinical lesions ratherthan isolated individual lesions. The latest ILDS/EDF AK guidelinesclassify patients according to the number of AK lesions peraffected field or body region. Patients with single lesions have !1but "5 palpable or visible AK lesions, those with multiple lesionshave !6 distinguishable AK lesions, and those with field cancerisa-tion also have !6 distinguishable AK lesions together with con-tiguous areas of chronic actinic sun damage and hyperkeratosis(9). This classification is used to direct treatment choices.
The authors consider the ILDS/EDF patient classification tohave limited supporting evidence for the numerical thresholds ofAK lesions which separate the different categories of patients, aspreviously discussed by Pellacani et al. (28). Whilst the number ofAK lesions is useful to define patient eligibility criteria for RCTs, itdoes not provide useful information on the underlying biologicalcharacteristics of the disease process, in particular field cancerisa-tion. In addition, absolute lesion numbers do not take into consid-eration important factors, such as early recurrence after treatment,rapid increase in lesions, immunosuppression or other factors thatcan influence the risk of developing an invasive SCC.
The authors propose that AK patients should be classified asfollows without defining a specific number of AK lesions perpatient group: (1) Those with isolated individual lesions scatteredon separate body areas; (2) Those with multiple AK lesions clus-tered into a single small field; and (3) Those with multiple lesionsacross a large field such as the entire face or scalp (Figure 4).
The authors also consider it to be important to identifypatients who are at high risk of progression to invasive SCC or
metastatic disease so that they can be monitored more closely.Criteria suggestive of “high-risk” patients are shown in Table 1,although there is currently limited supporting evidence for identi-fying those most likely to progress to invasive disease.
Practical algorithm for AK management
A practical algorithm for the management of AK patients in real-life clinical practice is shown in Figure 5. Following a clinical diag-nosis of AK, it is advisable to remove any hyperkeratosis (e.g. withcurettage, laser ablation, keratolytic treatment) before initiatingtreatment. Curettage is preferred because it allows histologicalconfirmation of the diagnosis. Furthermore, the panel recom-mends taking biopsies and performing histopathology on residuallesions after topical treatment to explore the possibility ofmalignancy.
Treatment recommendations are provided for patients with iso-lated scattered lesions, those with small clusters of lesions andthose with involvement of large areas. Lesion-directed therapiesare those that are suitable for the treatment of single-scatteredlesions, but which do not treat the surrounding skin. Cluster-directed therapies are those that are suitable for the treatment ofsmall field cancerisation areas (usually "25 cm2) based on theirlicenced indication. Cluster-directed therapies may also be used totreat larger fields in successive treatment cycles, although thiscomes at the expense of an increased number of physician visitsand longer treatment durations as subsequent cycles can only bestarted after the initial cycle has been completed and a restperiod has been taken. Therapies for large-affected fields are
Figure 4. Classification of AK lesions: (A) isolated lesion; (B) multiple lesions clustered in a small field; (C) multiple lesions across a large field (entire scalp).
4 T. DIRSCHKA ET AL.
Clinical spectrum of AK
AK patients usually present with multiple clinical lesions ratherthan isolated individual lesions. The latest ILDS/EDF AK guidelinesclassify patients according to the number of AK lesions peraffected field or body region. Patients with single lesions have !1but "5 palpable or visible AK lesions, those with multiple lesionshave !6 distinguishable AK lesions, and those with field cancerisa-tion also have !6 distinguishable AK lesions together with con-tiguous areas of chronic actinic sun damage and hyperkeratosis(9). This classification is used to direct treatment choices.
The authors consider the ILDS/EDF patient classification tohave limited supporting evidence for the numerical thresholds ofAK lesions which separate the different categories of patients, aspreviously discussed by Pellacani et al. (28). Whilst the number ofAK lesions is useful to define patient eligibility criteria for RCTs, itdoes not provide useful information on the underlying biologicalcharacteristics of the disease process, in particular field cancerisa-tion. In addition, absolute lesion numbers do not take into consid-eration important factors, such as early recurrence after treatment,rapid increase in lesions, immunosuppression or other factors thatcan influence the risk of developing an invasive SCC.
The authors propose that AK patients should be classified asfollows without defining a specific number of AK lesions perpatient group: (1) Those with isolated individual lesions scatteredon separate body areas; (2) Those with multiple AK lesions clus-tered into a single small field; and (3) Those with multiple lesionsacross a large field such as the entire face or scalp (Figure 4).
The authors also consider it to be important to identifypatients who are at high risk of progression to invasive SCC or
metastatic disease so that they can be monitored more closely.Criteria suggestive of “high-risk” patients are shown in Table 1,although there is currently limited supporting evidence for identi-fying those most likely to progress to invasive disease.
Practical algorithm for AK management
A practical algorithm for the management of AK patients in real-life clinical practice is shown in Figure 5. Following a clinical diag-nosis of AK, it is advisable to remove any hyperkeratosis (e.g. withcurettage, laser ablation, keratolytic treatment) before initiatingtreatment. Curettage is preferred because it allows histologicalconfirmation of the diagnosis. Furthermore, the panel recom-mends taking biopsies and performing histopathology on residuallesions after topical treatment to explore the possibility ofmalignancy.
Treatment recommendations are provided for patients with iso-lated scattered lesions, those with small clusters of lesions andthose with involvement of large areas. Lesion-directed therapiesare those that are suitable for the treatment of single-scatteredlesions, but which do not treat the surrounding skin. Cluster-directed therapies are those that are suitable for the treatment ofsmall field cancerisation areas (usually "25 cm2) based on theirlicenced indication. Cluster-directed therapies may also be used totreat larger fields in successive treatment cycles, although thiscomes at the expense of an increased number of physician visitsand longer treatment durations as subsequent cycles can only bestarted after the initial cycle has been completed and a restperiod has been taken. Therapies for large-affected fields are
Figure 4. Classification of AK lesions: (A) isolated lesion; (B) multiple lesions clustered in a small field; (C) multiple lesions across a large field (entire scalp).
4 T. DIRSCHKA ET AL.
Clinical
spectrum
ofAK
AK
patie
ntsusua
llypresen
twith
multip
leclinical
lesion
srather
than
isolated
individu
allesion
s.Th
elatest
ILDS/ED
FAKgu
idelines
classify
patie
nts
according
tothe
numbe
rof
AK
lesion
spe
raffected
field
orbo
dyregion
.Patientswith
sing
lelesion
sha
ve!1
but"5pa
lpab
leor
visibleAKlesion
s,thosewith
multip
lelesion
sha
ve!6distingu
isha
bleAKlesion
s,an
dthosewith
field
canc
erisa-
tion
also
have
!6distingu
isha
bleAK
lesion
stoge
ther
with
con-
tiguo
usareasof
chronicactin
icsun
damag
ean
dhy
perkeratosis
(9).Th
isclassificationisused
todirect
treatm
entch
oices.
The
authors
consider
the
ILDS/ED
Fpa
tient
classification
toha
velim
itedsupp
ortin
geviden
ceforthenu
merical
thresholds
ofAKlesion
swhich
sepa
rate
thediffe
rent
catego
riesof
patie
nts,
aspreviously
discussedby
Pellacani
etal.(28
).Whilstthenu
mbe
rof
AKlesion
sis
useful
tode
finepa
tient
eligibility
crite
riaforRC
Ts,it
does
notprov
ideuseful
inform
ationon
theun
derly
ingbiolog
ical
characteristic
sof
thediseaseprocess,
inpa
rticular
field
canc
erisa-
tion.
Inad
ditio
n,ab
solute
lesion
numbe
rsdo
nottake
into
consid-
erationim
portan
tfactors,such
asearly
recurren
ceaftertreatm
ent,
rapidincrease
inlesion
s,im
mun
osup
pression
orothe
rfactorsthat
caninflu
ence
theriskof
developing
aninvasive
SCC.
Theau
thorsprop
osethat
AK
patie
ntsshou
ldbe
classifie
das
follo
ws
with
outde
fining
aspecific
numbe
rof
AK
lesion
spe
rpa
tient
grou
p:(1)Th
osewith
isolated
individu
allesion
sscattered
onsepa
rate
body
areas;
(2)Th
osewith
multip
leAKlesion
sclus-
teredinto
asing
lesm
allfie
ld;a
nd(3)Th
osewith
multip
lelesion
sacross
alargefie
ldsuch
astheen
tireface
orscalp(Figure4).
The
authors
also
consider
itto
beim
portan
tto
iden
tify
patie
ntswho
areat
high
riskof
prog
ression
toinvasive
SCC
or
metastatic
diseaseso
that
they
can
bemon
itored
moreclosely.
Crite
riasugg
estiv
eof
“high-risk”
patie
ntsare
show
nin
Table
1,althou
ghthereiscurren
tlylim
itedsupp
ortin
geviden
ceforiden
ti-fyingthosemostlikelyto
prog
ress
toinvasive
disease.
Practicalalgo
rithm
forAKman
agem
ent
Apractic
alalgo
rithm
fortheman
agem
entof
AKpa
tientsin
real-
lifeclinical
practic
eisshow
nin
Figu
re5.
Follo
wingaclinical
diag
-no
sisof
AK,
itisad
visableto
remov
ean
yhy
perkeratosis(e.g.w
ithcurettag
e,laserab
latio
n,keratolytic
treatm
ent)
before
initiating
treatm
ent.
Curettag
eis
preferred
because
itallowshistolog
ical
confirm
ation
ofthe
diag
nosis.
Furthe
rmore,
the
pane
lrecom-
men
dstaking
biop
sies
andpe
rforminghistop
atho
logy
onresidu
allesion
safter
topical
treatm
ent
toexplore
the
possibility
ofmaligna
ncy.
Treatm
entrecommen
datio
nsareprov
ided
forpa
tientswith
iso-
lated
scattered
lesion
s,those
with
smallclusters
oflesion
san
dthose
with
invo
lvem
entof
large
areas.
Lesion
-dire
cted
therap
ies
arethosethat
aresuita
bleforthetreatm
entof
sing
le-scattered
lesion
s,bu
twhich
dono
ttreatthe
surrou
nding
skin.Cluster-
directed
therap
iesarethosethat
aresuita
bleforthetreatm
entof
smallfie
ldcanc
erisation
areas(usually
"25
cm2)ba
sed
ontheir
licen
cedindicatio
n.Cluster-directed
therap
iesmay
also
beused
totreatlarger
fieldsin
successive
treatm
entcycles,althou
ghthis
comes
attheexpe
nseof
anincreasednu
mbe
rof
physicianvisits
andlong
ertreatm
entdu
ratio
nsas
subseq
uent
cycles
canon
lybe
started
afterthe
initial
cycle
has
been
completed
and
arest
perio
dha
sbe
entaken.
Therap
ies
forlarge-affected
fields
are
Figu
re4.
Classificationof
AKlesio
ns:(A)
isolatedlesio
n;(B)m
ultip
lelesio
nsclusteredin
asm
allfield;(C)
multip
lelesio
nsacross
alargefield
(entire
scalp).
4T.
DIRSC
HKA
ETAL.
MULTIPLE LESIONS CLUSTERED INTO A
SMALL FIELD
ISOLATED LESION MULTIPLE LESIONS ACROSS A LARGE FIELD (e.g ENTIRE FACE OR SCALP)
AK CLASSIFICATION
isolated individual lesionsscattered on separate body
areas

Lesion-‐directed therapies for single or scattered lesions
those that are suitable for the treatment of sun-exposedfields>25cm2. These therapies may also be used for the treatmentof clustered lesions in small fields.
AK treatment goals
The goals of AK treatment are to eradicate as many clinical andsubclinical AK lesions as possible (i.e. to reduce the extent of fieldcancerisation), to achieve a time to relapse or disease-free intervalthat is as prolonged as possible, and to decrease the risk of apatient developing invasive SCC. Secondary aims are to improvethe quality of the patient’s skin and consequently their quality oflife. Since it is not always possible to clear each AK lesion in real-life practice, the main aim of therapy is to reduce the number oflesions and to achieve long-term disease control. As AK is amarker for chronic sun damage, another goal of AK treatment isto reduce the risk of other UV-dependent skin cancers.
In real-life clinical practice, treatment success should usually beevaluated using the absolute or percentage reduction in AKlesions, rather than by determining whether or not the patientachieves complete clearance. For example, a patient with 20 AKlesions on clinical presentation and one lesion remaining afterfield-directed treatment may be considered a treatment failurebased on the endpoint of complete lesion clearance, even thougha 95% reduction in lesions has been achieved. Treatment successparameters should ideally also take into consideration the abilityof a therapy to eliminate subclinical lesions, though this dependson these lesions becoming detectable during treatment, or theuse of specific imaging techniques for field cancerisation (whichare not usually available in dermatological offices) (26).
The authors do not specify a particular percentage reductionof lesions, which corresponds to treatment success in daily prac-tice, since this will depend on the number of lesions thepatient has on presentation and the individual clinical situation.
Figure 5. Practical algorithm for the treatment of AK. AK: actinic keratosis; iSCC: invasive squamous cell carcinoma. !Pre-treatment (e.g. curettage, laser ablation) toremove hyperkeratosis. †Discharge and follow-up patient if treatment success is achieved; move patient to different AK treatment if treatment success is not achieved.
Table 1. AK patients at high risk of progression to invasive squamous cell carcinoma or metastatic disease.
Supported by evidence Expert opinion
" AKs on body areas such as the ear and lip (29,30)" Early disease relapse following treatment (101)" Immunocompromised patients (29,30)
! Elderly! Organ transplant recipients! Rheumatological disease! Haematological disease! Inflammatory bowel disease! Chronic lymphocytic leukaemia
" Poor response to treatment" High cumulative lifetime sun exposure (occupational or recreational)" Personal history of skin cancer" Many AK lesions" Fair skin type" Smoking" Alcoholism" Other diseases affecting patients’ immunocompetence
AK: actinic keratosis.
JOURNAL OF DERMATOLOGICAL TREATMENT 5
• Cryotherapy• Topical active drugs• Laser (CO2; Er:Yag)• Curettage
Dirschka T et al JDT 2016

Clustered-‐directed therapies (areas ≤25 cm2)
• Imiquimod 5%• 0.5% 5-‐FU / 10% salicylic acid• Ingenol Mebutate
those that are suitable for the treatment of sun-exposedfields>25cm2. These therapies may also be used for the treatmentof clustered lesions in small fields.
AK treatment goals
The goals of AK treatment are to eradicate as many clinical andsubclinical AK lesions as possible (i.e. to reduce the extent of fieldcancerisation), to achieve a time to relapse or disease-free intervalthat is as prolonged as possible, and to decrease the risk of apatient developing invasive SCC. Secondary aims are to improvethe quality of the patient’s skin and consequently their quality oflife. Since it is not always possible to clear each AK lesion in real-life practice, the main aim of therapy is to reduce the number oflesions and to achieve long-term disease control. As AK is amarker for chronic sun damage, another goal of AK treatment isto reduce the risk of other UV-dependent skin cancers.
In real-life clinical practice, treatment success should usually beevaluated using the absolute or percentage reduction in AKlesions, rather than by determining whether or not the patientachieves complete clearance. For example, a patient with 20 AKlesions on clinical presentation and one lesion remaining afterfield-directed treatment may be considered a treatment failurebased on the endpoint of complete lesion clearance, even thougha 95% reduction in lesions has been achieved. Treatment successparameters should ideally also take into consideration the abilityof a therapy to eliminate subclinical lesions, though this dependson these lesions becoming detectable during treatment, or theuse of specific imaging techniques for field cancerisation (whichare not usually available in dermatological offices) (26).
The authors do not specify a particular percentage reductionof lesions, which corresponds to treatment success in daily prac-tice, since this will depend on the number of lesions thepatient has on presentation and the individual clinical situation.
Figure 5. Practical algorithm for the treatment of AK. AK: actinic keratosis; iSCC: invasive squamous cell carcinoma. !Pre-treatment (e.g. curettage, laser ablation) toremove hyperkeratosis. †Discharge and follow-up patient if treatment success is achieved; move patient to different AK treatment if treatment success is not achieved.
Table 1. AK patients at high risk of progression to invasive squamous cell carcinoma or metastatic disease.
Supported by evidence Expert opinion
" AKs on body areas such as the ear and lip (29,30)" Early disease relapse following treatment (101)" Immunocompromised patients (29,30)
! Elderly! Organ transplant recipients! Rheumatological disease! Haematological disease! Inflammatory bowel disease! Chronic lymphocytic leukaemia
" Poor response to treatment" High cumulative lifetime sun exposure (occupational or recreational)" Personal history of skin cancer" Many AK lesions" Fair skin type" Smoking" Alcoholism" Other diseases affecting patients’ immunocompetence
AK: actinic keratosis.
JOURNAL OF DERMATOLOGICAL TREATMENT 5
Dirschka T et al JDT 2016
All large field-‐directed therapies can be used to treat clusters

Large field-‐directed therapies for multiple lesions
• IMQ 3.75%• 5-‐FU• Diclofenac gel• PDT
those that are suitable for the treatment of sun-exposedfields>25cm2. These therapies may also be used for the treatmentof clustered lesions in small fields.
AK treatment goals
The goals of AK treatment are to eradicate as many clinical andsubclinical AK lesions as possible (i.e. to reduce the extent of fieldcancerisation), to achieve a time to relapse or disease-free intervalthat is as prolonged as possible, and to decrease the risk of apatient developing invasive SCC. Secondary aims are to improvethe quality of the patient’s skin and consequently their quality oflife. Since it is not always possible to clear each AK lesion in real-life practice, the main aim of therapy is to reduce the number oflesions and to achieve long-term disease control. As AK is amarker for chronic sun damage, another goal of AK treatment isto reduce the risk of other UV-dependent skin cancers.
In real-life clinical practice, treatment success should usually beevaluated using the absolute or percentage reduction in AKlesions, rather than by determining whether or not the patientachieves complete clearance. For example, a patient with 20 AKlesions on clinical presentation and one lesion remaining afterfield-directed treatment may be considered a treatment failurebased on the endpoint of complete lesion clearance, even thougha 95% reduction in lesions has been achieved. Treatment successparameters should ideally also take into consideration the abilityof a therapy to eliminate subclinical lesions, though this dependson these lesions becoming detectable during treatment, or theuse of specific imaging techniques for field cancerisation (whichare not usually available in dermatological offices) (26).
The authors do not specify a particular percentage reductionof lesions, which corresponds to treatment success in daily prac-tice, since this will depend on the number of lesions thepatient has on presentation and the individual clinical situation.
Figure 5. Practical algorithm for the treatment of AK. AK: actinic keratosis; iSCC: invasive squamous cell carcinoma. !Pre-treatment (e.g. curettage, laser ablation) toremove hyperkeratosis. †Discharge and follow-up patient if treatment success is achieved; move patient to different AK treatment if treatment success is not achieved.
Table 1. AK patients at high risk of progression to invasive squamous cell carcinoma or metastatic disease.
Supported by evidence Expert opinion
" AKs on body areas such as the ear and lip (29,30)" Early disease relapse following treatment (101)" Immunocompromised patients (29,30)
! Elderly! Organ transplant recipients! Rheumatological disease! Haematological disease! Inflammatory bowel disease! Chronic lymphocytic leukaemia
" Poor response to treatment" High cumulative lifetime sun exposure (occupational or recreational)" Personal history of skin cancer" Many AK lesions" Fair skin type" Smoking" Alcoholism" Other diseases affecting patients’ immunocompetence
AK: actinic keratosis.
JOURNAL OF DERMATOLOGICAL TREATMENT 5
Dirschka T et al JDT 2016
Clustered-‐directed therapies may be used to treat large fields in successive treatment cycles

those that are suitable for the treatment of sun-exposedfields>25cm2. These therapies may also be used for the treatmentof clustered lesions in small fields.
AK treatment goals
The goals of AK treatment are to eradicate as many clinical andsubclinical AK lesions as possible (i.e. to reduce the extent of fieldcancerisation), to achieve a time to relapse or disease-free intervalthat is as prolonged as possible, and to decrease the risk of apatient developing invasive SCC. Secondary aims are to improvethe quality of the patient’s skin and consequently their quality oflife. Since it is not always possible to clear each AK lesion in real-life practice, the main aim of therapy is to reduce the number oflesions and to achieve long-term disease control. As AK is amarker for chronic sun damage, another goal of AK treatment isto reduce the risk of other UV-dependent skin cancers.
In real-life clinical practice, treatment success should usually beevaluated using the absolute or percentage reduction in AKlesions, rather than by determining whether or not the patientachieves complete clearance. For example, a patient with 20 AKlesions on clinical presentation and one lesion remaining afterfield-directed treatment may be considered a treatment failurebased on the endpoint of complete lesion clearance, even thougha 95% reduction in lesions has been achieved. Treatment successparameters should ideally also take into consideration the abilityof a therapy to eliminate subclinical lesions, though this dependson these lesions becoming detectable during treatment, or theuse of specific imaging techniques for field cancerisation (whichare not usually available in dermatological offices) (26).
The authors do not specify a particular percentage reductionof lesions, which corresponds to treatment success in daily prac-tice, since this will depend on the number of lesions thepatient has on presentation and the individual clinical situation.
Figure 5. Practical algorithm for the treatment of AK. AK: actinic keratosis; iSCC: invasive squamous cell carcinoma. !Pre-treatment (e.g. curettage, laser ablation) toremove hyperkeratosis. †Discharge and follow-up patient if treatment success is achieved; move patient to different AK treatment if treatment success is not achieved.
Table 1. AK patients at high risk of progression to invasive squamous cell carcinoma or metastatic disease.
Supported by evidence Expert opinion
" AKs on body areas such as the ear and lip (29,30)" Early disease relapse following treatment (101)" Immunocompromised patients (29,30)
! Elderly! Organ transplant recipients! Rheumatological disease! Haematological disease! Inflammatory bowel disease! Chronic lymphocytic leukaemia
" Poor response to treatment" High cumulative lifetime sun exposure (occupational or recreational)" Personal history of skin cancer" Many AK lesions" Fair skin type" Smoking" Alcoholism" Other diseases affecting patients’ immunocompetence
AK: actinic keratosis.
JOURNAL OF DERMATOLOGICAL TREATMENT 5
those that are suitable for the treatment of sun-exposedfields>25cm2. These therapies may also be used for the treatmentof clustered lesions in small fields.
AK treatment goals
The goals of AK treatment are to eradicate as many clinical andsubclinical AK lesions as possible (i.e. to reduce the extent of fieldcancerisation), to achieve a time to relapse or disease-free intervalthat is as prolonged as possible, and to decrease the risk of apatient developing invasive SCC. Secondary aims are to improvethe quality of the patient’s skin and consequently their quality oflife. Since it is not always possible to clear each AK lesion in real-life practice, the main aim of therapy is to reduce the number oflesions and to achieve long-term disease control. As AK is amarker for chronic sun damage, another goal of AK treatment isto reduce the risk of other UV-dependent skin cancers.
In real-life clinical practice, treatment success should usually beevaluated using the absolute or percentage reduction in AKlesions, rather than by determining whether or not the patientachieves complete clearance. For example, a patient with 20 AKlesions on clinical presentation and one lesion remaining afterfield-directed treatment may be considered a treatment failurebased on the endpoint of complete lesion clearance, even thougha 95% reduction in lesions has been achieved. Treatment successparameters should ideally also take into consideration the abilityof a therapy to eliminate subclinical lesions, though this dependson these lesions becoming detectable during treatment, or theuse of specific imaging techniques for field cancerisation (whichare not usually available in dermatological offices) (26).
The authors do not specify a particular percentage reductionof lesions, which corresponds to treatment success in daily prac-tice, since this will depend on the number of lesions thepatient has on presentation and the individual clinical situation.
Figure 5. Practical algorithm for the treatment of AK. AK: actinic keratosis; iSCC: invasive squamous cell carcinoma. !Pre-treatment (e.g. curettage, laser ablation) toremove hyperkeratosis. †Discharge and follow-up patient if treatment success is achieved; move patient to different AK treatment if treatment success is not achieved.
Table 1. AK patients at high risk of progression to invasive squamous cell carcinoma or metastatic disease.
Supported by evidence Expert opinion
" AKs on body areas such as the ear and lip (29,30)" Early disease relapse following treatment (101)" Immunocompromised patients (29,30)
! Elderly! Organ transplant recipients! Rheumatological disease! Haematological disease! Inflammatory bowel disease! Chronic lymphocytic leukaemia
" Poor response to treatment" High cumulative lifetime sun exposure (occupational or recreational)" Personal history of skin cancer" Many AK lesions" Fair skin type" Smoking" Alcoholism" Other diseases affecting patients’ immunocompetence
AK: actinic keratosis.
JOURNAL OF DERMATOLOGICAL TREATMENT 5
those that are suitable for the treatment of sun-exposedfields>25cm2. These therapies may also be used for the treatmentof clustered lesions in small fields.
AK treatment goals
The goals of AK treatment are to eradicate as many clinical andsubclinical AK lesions as possible (i.e. to reduce the extent of fieldcancerisation), to achieve a time to relapse or disease-free intervalthat is as prolonged as possible, and to decrease the risk of apatient developing invasive SCC. Secondary aims are to improvethe quality of the patient’s skin and consequently their quality oflife. Since it is not always possible to clear each AK lesion in real-life practice, the main aim of therapy is to reduce the number oflesions and to achieve long-term disease control. As AK is amarker for chronic sun damage, another goal of AK treatment isto reduce the risk of other UV-dependent skin cancers.
In real-life clinical practice, treatment success should usually beevaluated using the absolute or percentage reduction in AKlesions, rather than by determining whether or not the patientachieves complete clearance. For example, a patient with 20 AKlesions on clinical presentation and one lesion remaining afterfield-directed treatment may be considered a treatment failurebased on the endpoint of complete lesion clearance, even thougha 95% reduction in lesions has been achieved. Treatment successparameters should ideally also take into consideration the abilityof a therapy to eliminate subclinical lesions, though this dependson these lesions becoming detectable during treatment, or theuse of specific imaging techniques for field cancerisation (whichare not usually available in dermatological offices) (26).
The authors do not specify a particular percentage reductionof lesions, which corresponds to treatment success in daily prac-tice, since this will depend on the number of lesions thepatient has on presentation and the individual clinical situation.
Figure 5. Practical algorithm for the treatment of AK. AK: actinic keratosis; iSCC: invasive squamous cell carcinoma. !Pre-treatment (e.g. curettage, laser ablation) toremove hyperkeratosis. †Discharge and follow-up patient if treatment success is achieved; move patient to different AK treatment if treatment success is not achieved.
Table 1. AK patients at high risk of progression to invasive squamous cell carcinoma or metastatic disease.
Supported by evidence Expert opinion
" AKs on body areas such as the ear and lip (29,30)" Early disease relapse following treatment (101)" Immunocompromised patients (29,30)
! Elderly! Organ transplant recipients! Rheumatological disease! Haematological disease! Inflammatory bowel disease! Chronic lymphocytic leukaemia
" Poor response to treatment" High cumulative lifetime sun exposure (occupational or recreational)" Personal history of skin cancer" Many AK lesions" Fair skin type" Smoking" Alcoholism" Other diseases affecting patients’ immunocompetence
AK: actinic keratosis.
JOURNAL OF DERMATOLOGICAL TREATMENT 5
SCATTERED LESIONS CLUSTERED LESIONS IN A SMALL FIELD
CLUSTERED LESIONS IN A LARGE FIELD
TREATMENT SUCCESS EVALUATION AFTER 3 TO 6 MONTHS
Lesion-‐directed therapies Cluster-‐directed therapies Large field-‐directed therapies
Dirschka T et al. JDT 2016

ORIGINAL ARTICLE
Real-life efficacy and safety of ingenol mebutate for the treatment of actinickeratosis of the face and scalp: A single arm retrospective study
Francesco Riccia, Sara Tamboneb, Luca Neric, Luca Faniaa, Antonella Piccionib, Cristina Guerrieroa,Maria Concetta Fargnolib and Ketty Perisa
aInstitute of Dermatology, Catholic University of the Sacred Heart, Rome, Italy; bDepartment of Dermatology, University of L’Aquila, L’Aquila Italy;cOutcomes Research Consulting, Milano, ItalyQ1
ABSTRACTBackground: The efficacy and safety of ingenol mebutate versus placebo have been proven in fourrandomized controlled trials (RCTs), although there is a lack of real-life studies corroborating such promisesin routine clinical practices. In our study, we sought to describe real-life effectiveness, safety and regimenadherence among patients with multiple AKs on the face treated with ingenol mebutate and evaluate cor-relates of clinical outcomes in this population. Methods: We reviewed the clinical charts of adult patientswith multiple (!3) AK grade I and II of the face and scalp, treated with ingenol mebutate from April 2014to April 2015. All subjects received the medication according to ingenol mebutate standard of care.Results: We enrolled 88 patients during the study period and carried out 122 treatment cycles. Theunadjusted lesion clearance rate per treated field was 81.3% and the average local skin reactions score atday 4 was 6.06 2.8 (range: 0–18). Conclusions: We observed an excellent rate (>99%) of adherence toingenol mebutate. This was mirrored by the fact that our clinical outcomes broadly confirmed resultsobtained in RTCs. Our study showed that the efficacy and safety of ingenol mebutate observed in RCTscan be reliably translated in real-world practice.
ARTICLE HISTORYReceived 1 February 2016Accepted 28 February 2016Published online 2 2 2
KEYWORDSingenol mebutate; actinickeratosis; field-directedtreatment
Introduction
Actinic keratosis (AK) is a common keratinocytic neoplasm typic-ally occurring in photodamaged skin of elderly individuals, whichcan potentially progress to invasive squamous cell carcinoma(iSCC) (1). Available data indicate that there are no clues to pre-dict which AK lesions may progress to iSCC. Therefore, currentguidelines recommend treating all clinically visible AK lesionsand the underlying cancerization field (2–7). A number of effect-ive lesion-directed and field-directed treatments are available.Ingenol mebutate is the most recent advancement in a fast-growing field with several newly developed drugs or procedurestill awaiting for approval from health care authorities in Europeand USA. Ingenol mebutate is extracted and purified fromEuphorbia peplus and formulated as a gel for topical application.Ingenol mebutate is self-applied by the patients over two con-secutive days for AK lesions on the trunk or extremities andover three consecutive days on the face or scalp. The efficacyand safety of ingenol mebutate versus placebo have been pro-ven in four randomized controlled trials (RCTs) reported in onepooled analysis (8). Patients treated with the drug achieved 83%reduction rates for lesions on the face or scalp and 75% forlesions on the trunk or extremities at two-month follow-up (8).Long-term efficacy studies demonstrated that patients treatedwith ingenol mebutate approximately achieve a 90% 12-monthsustained clearance rates (lesion count) of initially cleared lesions(9). Evidence from RCTs shows extremely high adherence rates(i.e. over 95%) in patients receiving ingenol mebutate (8), as wellas improvement of patients’ quality of life (10); however, there is
a lack of real-life studies corroborating such promises in routineclinical practices. Additionally, no study has evaluated sociode-mographic and clinical predictors of treatment response for field-directed therapies so far. Such information might help profilepatients and tailor interventions to those most likely to benefitfrom specific treatments. In the present study, we sought todescribe real-life effectiveness, safety and regimen adherenceamong patients with multiple AKs on the face treated withingenol mebutate and evaluate correlates of clinical outcomes inthis population.
Methods
Study design, patients and treatment
We conducted a single arm, observational historical cohort studyof clinical outcomes among AK patients treated with ingenolmebutate. Patients were enrolled from two dermatological out-patient clinics (Catholic University of Sacred Heart of Rome andUniversity of L’Aquila). We reviewed the clinical charts of adultpatients with multiple (!3) AK grade I and II (11) of the faceand scalp, treated with ingenol mebutate from April 2014 toApril 2015. We excluded patients if they received any othertreatment in the target area in the three months prior toingenol mebutate treatment or concurrent immunosuppressivemedications. Patients were also excluded if the target treatmentarea was within 5 cm of an incompletely healed wound orwithin 10 cm of a suspected basal cell carcinoma (BCC) or squa-mous cell carcinoma (SCC), or if the target treatment area
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263
646566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126
CONTACT Ketty Peris [email protected] Institute of Dermatology, Catholic University of the Sacred Heart, Largo A. Gemelli 8 - 00168 Rome, Italy! 2016 Informa UK Limited, trading as Taylor & Francis Group
JOURNAL OF DERMATOLOGICAL TREATMENT, 2016http://dx.doi.org/10.3109/09546634.2016.1161162
ORIGINAL ARTICLE
Real-life efficacy and safety of ingenol mebutate for the treatment of actinickeratosis of the face and scalp: A single arm retrospective study
Francesco Riccia, Sara Tamboneb, Luca Neric, Luca Faniaa, Antonella Piccionib, Cristina Guerrieroa,Maria Concetta Fargnolib and Ketty Perisa
aInstitute of Dermatology, Catholic University of the Sacred Heart, Rome, Italy; bDepartment of Dermatology, University of L’Aquila, L’Aquila Italy;cOutcomes Research Consulting, Milano, ItalyQ1
ABSTRACTBackground: The efficacy and safety of ingenol mebutate versus placebo have been proven in fourrandomized controlled trials (RCTs), although there is a lack of real-life studies corroborating such promisesin routine clinical practices. In our study, we sought to describe real-life effectiveness, safety and regimenadherence among patients with multiple AKs on the face treated with ingenol mebutate and evaluate cor-relates of clinical outcomes in this population. Methods: We reviewed the clinical charts of adult patientswith multiple (!3) AK grade I and II of the face and scalp, treated with ingenol mebutate from April 2014to April 2015. All subjects received the medication according to ingenol mebutate standard of care.Results: We enrolled 88 patients during the study period and carried out 122 treatment cycles. Theunadjusted lesion clearance rate per treated field was 81.3% and the average local skin reactions score atday 4 was 6.06 2.8 (range: 0–18). Conclusions: We observed an excellent rate (>99%) of adherence toingenol mebutate. This was mirrored by the fact that our clinical outcomes broadly confirmed resultsobtained in RTCs. Our study showed that the efficacy and safety of ingenol mebutate observed in RCTscan be reliably translated in real-world practice.
ARTICLE HISTORYReceived 1 February 2016Accepted 28 February 2016Published online 2 2 2
KEYWORDSingenol mebutate; actinickeratosis; field-directedtreatment
Introduction
Actinic keratosis (AK) is a common keratinocytic neoplasm typic-ally occurring in photodamaged skin of elderly individuals, whichcan potentially progress to invasive squamous cell carcinoma(iSCC) (1). Available data indicate that there are no clues to pre-dict which AK lesions may progress to iSCC. Therefore, currentguidelines recommend treating all clinically visible AK lesionsand the underlying cancerization field (2–7). A number of effect-ive lesion-directed and field-directed treatments are available.Ingenol mebutate is the most recent advancement in a fast-growing field with several newly developed drugs or procedurestill awaiting for approval from health care authorities in Europeand USA. Ingenol mebutate is extracted and purified fromEuphorbia peplus and formulated as a gel for topical application.Ingenol mebutate is self-applied by the patients over two con-secutive days for AK lesions on the trunk or extremities andover three consecutive days on the face or scalp. The efficacyand safety of ingenol mebutate versus placebo have been pro-ven in four randomized controlled trials (RCTs) reported in onepooled analysis (8). Patients treated with the drug achieved 83%reduction rates for lesions on the face or scalp and 75% forlesions on the trunk or extremities at two-month follow-up (8).Long-term efficacy studies demonstrated that patients treatedwith ingenol mebutate approximately achieve a 90% 12-monthsustained clearance rates (lesion count) of initially cleared lesions(9). Evidence from RCTs shows extremely high adherence rates(i.e. over 95%) in patients receiving ingenol mebutate (8), as wellas improvement of patients’ quality of life (10); however, there is
a lack of real-life studies corroborating such promises in routineclinical practices. Additionally, no study has evaluated sociode-mographic and clinical predictors of treatment response for field-directed therapies so far. Such information might help profilepatients and tailor interventions to those most likely to benefitfrom specific treatments. In the present study, we sought todescribe real-life effectiveness, safety and regimen adherenceamong patients with multiple AKs on the face treated withingenol mebutate and evaluate correlates of clinical outcomes inthis population.
Methods
Study design, patients and treatment
We conducted a single arm, observational historical cohort studyof clinical outcomes among AK patients treated with ingenolmebutate. Patients were enrolled from two dermatological out-patient clinics (Catholic University of Sacred Heart of Rome andUniversity of L’Aquila). We reviewed the clinical charts of adultpatients with multiple (!3) AK grade I and II (11) of the faceand scalp, treated with ingenol mebutate from April 2014 toApril 2015. We excluded patients if they received any othertreatment in the target area in the three months prior toingenol mebutate treatment or concurrent immunosuppressivemedications. Patients were also excluded if the target treatmentarea was within 5 cm of an incompletely healed wound orwithin 10 cm of a suspected basal cell carcinoma (BCC) or squa-mous cell carcinoma (SCC), or if the target treatment area
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263
646566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126
CONTACT Ketty Peris [email protected] Institute of Dermatology, Catholic University of the Sacred Heart, Largo A. Gemelli 8 - 00168 Rome, Italy! 2016 Informa UK Limited, trading as Taylor & Francis Group
JOURNAL OF DERMATOLOGICAL TREATMENT, 2016http://dx.doi.org/10.3109/09546634.2016.1161162
Lesion clearance rate: 81.3% (vs 78% in RCT)
Week 8Day 0
• Scalp lesions had a higher clearance rate compared to RCT (80% vs 53%)

Ricci et al JDT 2016
• No differences in clearance rate for patients who werepreviously treated compared to naïve patients
• No differences according to patients’ age, sex and baseline number of AK lesions
• No difference of efficacy across treatment cycles

IMIQUIMOD 3.75%• Can be used to treat small clusters of
lesions in a 25 cm2 area• Self-‐applied 3 times/week for 4 wks; 4
wks free interval, II 4wks course• Can detect and treat both clinical and
subclinical lesions• Clearance rate: 75%• Used to treat large affected fields (i.e.
full face or balding scalp) in sequentialtreatment courses (high cost)
IMIQUIMOD 5%• Can be used to treat large affected
fields (i.e. full face or balding scalp) in one treatment course
• Self-‐applied once daily for 2 wkstreatment cycles separated by a 2-‐wks free interval
• Can detect and treat both clinical and subclinical lesions
• 81.8% median percentage reductionin AK lesions from baseline
• Sustained clinical response over long-‐term
Stockfleth E Arch Dermatol 2004; Alomar A BJD 2007; Jorizzo J JAAD 2007; Ulrich M Dermatology 2010; Swanson N JAAD 2010; StockflethE EJD 2014; Hanke CW J Drugs Dermatol 2011; Gupta G JEADV 2015, Tambone S GIDV 2015

Diclofenac 3% in 2.5% hyaluronic acid
• NSAD which inhibits cyclooxygenase 2• Treat clustered lesions and field cancerisation• Overall lesion clearance rates reported in RCTs: 54–63% • Advantage: good tolerability with only mild irritant side effects
(pruritus, erythema and dry skin; rare: contact dermatitis)• Treatment duration is long (60-‐90days): difficult for many patients
to fully comply
Wolf JE IJD 2001; Rivers JK BJD 2002; Gebauer K AJD 2003, Nelson CG TCRM 011

Before any specific treatment
• Urea 10-‐30% cream
• Salicylic acid 10%
• Gentle curettage
Hyperkeratotic AK

TREATMENT OF ACTINIC CHEILITIS
• Cryosurgery
• 5% 5-‐FU
• MAL-‐PDT followed by IMQ
• Ingenol Mebutate
• Surgical vermilionectomy
Sotiriou E BJD 2011; Tzika E Dermatology 2016; Florez A JDT 2016; Chaves YN Photodermatol Photoimmunol Photomed 2016;
NO RCT !

• Cryotherapy• Curettage and electrodessication• PDT• Imiquimod*• Ingenol mebutate**• Diclofenac 3%• Systemic retinoids
AK treatment in OTR
*off label**no studies

Diclofenac 3%
Imiquimod
Photodynamictherapy
5-Fluorouracil
Cryotherapy
SURGERY
Laser
Combined or sequential treatments

Combined or sequential treatments
• Field-‐treatment followed by cryo to target individual, resistantlesions
• Lesion-‐directed treatment followed by field-‐directed therapy, used to treat the actinic damage in the surrounding area
-‐ Cryosurgery followed by imiquimod 3.75%
-‐ Cryosurgery followed by 5-‐fluorouracil
-‐ PDT followed by imiquimod 5%
-‐ 5-‐FU followed by ALA-‐PDT
-‐ Diclofenac 3% followed by PDT
Gilbert DJ 2005;; Price NM 2007;; van der Geer S 2009;; Shaffelburg M 2009;; Jorizzo JL 2010;; Sotiriou E 2011;; Ondo AL 2012;; Held L 2012, Serra-Guillen C 2012;; Hoover WD 2014

CONCLUSIONS
• Deliver simple yet complete information about the modality of self-‐administration (apply to the target area or the whole area, e.g. full scalp or face) and the expected course of therapy
• Routine follow-‐up evaluation (every 3-‐6 months) to examineskin carefully and identify new, early AK lesions as well asother skin cancers
• Sunprotection! Instruct the patient to avoid excessive sun-‐exposure and to use sunscreen daily