sistemik - pedo

of 18
-
Upload
christine-widjaja -
Category
Documents
-
view
222 -
download
0
Transcript of sistemik - pedo
-
8/3/2019 sistemik - pedo
1/18
Congenital heart disease
Congenital heart disease refers to a problem with the heart's structure and function
due to abnormal heart development before birth. Congenital means present at
birth.
Causes
Congenital heart disease (CHD) can describe a number of different problems
affecting the heart. It is the most common type of birth defect. Congenital heart
disease is responsible for more deaths in the first year of life than any other birth
defects. Many of these defects need to be followed carefully. Some heal overtime, others will require treatment.
Congenital heart disease is often divided into two types: cyanotic (blue
discoloration caused by a relative lack of oxygen) and non-cyanotic. The
following lists cover the most common of the congenital heart diseases:
Cyanotic:
Tetralogy of Fallot
Transposition of the great vessels
Tricuspid atresia Total anomalous pulmonary venous return
Truncus arteriosus
Hypoplastic left heart
Pulmonary atresia
Some forms of total anomalous pulmonary venous return
Ebstein's anomaly
Non-cyanotic:
Ventricular septal defect (VSD)
Atrial septal defect (ASD) Patent ductus arteriosus (PDA)
Aortic stenosis
Pulmonic stenosis
Coarctation of the aorta
Atrioventricular canal (endocardial cushion defect)
These problems may occur alone or together. The majority of congenital heart
diseases occurs as an isolated defect and is not associated with other diseases.
However, they can also be a part of various genetic and chromosomal syndromes
such as Down syndrome,trisomy 13, Turner syndrome, Marfan syndrome,
Noonan syndrome, and DiGeorge syndrome.
http://www.nlm.nih.gov/medlineplus/ency/article/003215.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001567.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001568.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001110.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001115.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001111.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001106.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/007321.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001099.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000157.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001560.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000178.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001096.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000191.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/007324.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001660.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001660.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000379.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000418.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001656.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/003215.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001567.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001568.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001110.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001115.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001111.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001106.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/007321.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001099.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000157.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001560.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000178.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001096.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000191.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/007324.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001660.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000379.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000418.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001656.htm -
8/3/2019 sistemik - pedo
2/18
No known cause can be identified for most congenital heart defects. Congenital
heart diseases continue to be investigated and researched. Drugs such as retinoic
acid for acne, chemicals, alcohol, and infections (such asrubella) during
pregnancy can contribute to some congenital heart problems.
Symptoms
Symptoms depend on the specific condition. While congenital heart disease is
present at birth, the symptoms may not be immediately obvious. Defects such as
coarctation of the aorta may not cause problems for many years. Other problems,
such as a small ventricular septal defect(VSD), may never cause any problems,
and some people with a VSD have normal physical activity and a normal life
span.
Prevention
Avoid alcohol and other drugs during pregnancy. Doctors should be made aware
that a woman is pregnant before prescribing any medications for her. A blood test
should be done early in the pregnancy to see if the woman is immune to rubella. If
the mother is not immune, she must avoid any possible exposure to rubella and
should be immunized immediately following delivery.
Poorly controlled blood sugar levels in women who have diabetes during
pregnancy are also associated with a high rate of congenital heart defects during
pregnancy.
Experts believe that some prescription and over-the-counter medications and
street drugs used during pregnancy increase the risk of heart defects.
There may be some hereditary factors that play a role in congenital heart disease.
Genetics does appear to play a role in many diseases, and multiple family
members may be affected. Talk to your health care provider about screening.
Expectant mothers should receive good prenatal care. Many congenital defects
can be discovered on routine ultrasound examinations performed by an
obstetrician. The delivery can then be anticipated and the appropriate medicalpersonnel (such as a pediatric cardiologist, a cardiothoracic surgeon, and a
neonatologist) can be present, and ready to help as necessary. Such preparation
can mean the difference between life and death for some babies.
http://www.nlm.nih.gov/medlineplus/ency/article/001574.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001574.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000191.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001099.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001099.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/003778.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001574.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/000191.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/001099.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/003778.htm -
8/3/2019 sistemik - pedo
3/18
Rheumatic fever (RF) is a systemic illness that may occur following group A beta
hemolytic streptococcal (GABHS)pharyngitis in children. Rheumatic fever and
its most serious complication, rheumatic heart disease (RHD), are believed to
result from an autoimmune response; however, the exact pathogenesis remainsunclear. Studies in the 1950s during an epidemic on a military base demonstrated
3% incidence of rheumatic fever in adults with streptococcal pharyngitis not
treated with antibiotics.[1] Studies in children during the same period demonstrated
an incidence of only 0.3%. The current incidence of rheumatic fever after
GABHS infection is now thought to have decreased to less than 1%. Cardiac
involvement is reported to occur in 30-70% of patients with their first attack of
rheumatic fever and in 73-90% of patients when all attacks are counted.
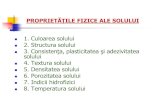
Clinical manifestations and time course of acute rheumatic fever are shown in the
image below.
Pathophysiology
Rheumatic fever develops in children and adolescents following pharyngitis with
GABHS (ie, Streptococcus pyogenes). The organisms attach to the epithelial cells
of the upper respiratory tract and produce a battery of enzymes, which allows
them to damage and invade human tissues. After an incubation period of 2-4 days,
the invading organisms elicit an acute inflammatory response, with 3-5 days of
sore throat, fever, malaise, headache, and elevated leukocyte count. In a small
percent of patients, infection leads to rheumatic fever several weeks after the sore
throat has resolved. Only infections of the pharynx initiate or reactivate rheumaticfever.
Direct contact with oral (PO) or respiratory secretions transmits the organism, and
crowding enhances transmission. Patients remain infected for weeks after
symptomatic resolution of pharyngitis and may serve as a reservoir for infecting
others. Penicillin treatment shortens the clinical course of streptococcal
pharyngitis and more importantly prevents the major sequelae.
GABHS organisms are gram-positive cocci, which frequently colonize the skin
and oropharynx. These organisms may cause suppurative diseases (eg,
pharyngitis, impetigo, cellulitis, myositis,pneumonia, puerperal sepsis). GABHS
http://emedicine.medscape.com/article/967384-overviewhttp://emedicine.medscape.com/article/891897-overviewhttp://emedicine.medscape.com/article/965254-overviewhttp://emedicine.medscape.com/article/967822-overviewhttp://emedicine.medscape.com/article/967822-overviewhttp://refimgshow%281%29/http://emedicine.medscape.com/article/967384-overviewhttp://emedicine.medscape.com/article/891897-overviewhttp://emedicine.medscape.com/article/965254-overviewhttp://emedicine.medscape.com/article/967822-overview -
8/3/2019 sistemik - pedo
4/18
organisms also may be associated with nonsuppurative diseases (eg, rheumatic
fever, acute poststreptococcal glomerulonephritis). Group A streptococci (GAS)
elaborate the cytolytic toxins, streptolysins S and O. Of these 2 toxins,
streptolysin O induces persistently high antibody titers that provide a useful
marker of GAS infection and its nonsuppurative complications.
GAS, as identified using the Lancefield classification, has a group A carbohydrate
antigen in the cell wall that is composed of a branched polymer of L-rhamnose
and N-acetyl-D-glucosamine in a 2:1 ratio. Surface proteins on the cell wall of the
organism may subserotype GAS. The presence of the M protein is the most
important virulence factor for GAS infection in humans. More than 120 M protein
serotypes or M protein genotypes have been identified,[20] some of which have a
long terminal antigenic domain (ie, epitopes) similar to antigens in various
components of the human heart.
Rheumatogenic strains are often encapsulated mucoid strains, rich in M proteins,and resistant to phagocytosis. These strains are strongly immunogenic, and anti-M
antibodies against the streptococcal infection may cross-react with components of
heart tissue (ie, sarcolemmal membranes, valve glycoproteins). Currently, emm
typing is felt to be more discriminating than M typing.[20]
Acute RHD often produces a pancarditis, characterized by endocarditis,
myocarditis, and pericarditis. Endocarditis is manifested as mitral and aortic valve
insufficiency. Severe scarring of the valves develops during a period of months to
years after an episode of acute rheumatic fever, and recurrent episodes may cause
progressive damage to the valves. The mitral valve is affected most commonly
and severely (65-70% of patients); the aortic valve is affected second most
commonly (25%).
The tricuspid valve is deformed in only 10% of patients, almost always in
association with mitral and aortic lesions, and the pulmonary valve is rarely
affected. Severe valve insufficiency during the acute phase may result in
congestive heart failure (CHF) and even death (1% of patients). Whether
myocardial dysfunction during acute rheumatic fever is primarily related to
myocarditis or is secondary to CHF from severe valve insufficiency is not known.
When pericarditis is present, it rarely affects cardiac function or results in
constrictive pericarditis.
Chronic manifestations occur in adults with previous RHD from residual and
progressive valve deformity. RHD is responsible for 99% of mitral valve stenosis
in adults, and it may be associated with atrial fibrillation from chronic mitral
valve disease and atrial enlargement.
Epidemiology
-
8/3/2019 sistemik - pedo
5/18
Frequency
United States
Rheumatic fever is now uncommon among children in the United States.Incidence of rheumatic fever and RHD has decreased in the United States and
other industrialized countries during the past 80 years. Prevalence of RHD in the
United States is now less than 0.05 per 1000 population, with rare regional
outbreaks reported in Tennessee in the 1960s and in Utah, Ohio, and Pennsylvania
in the 1980s. In the early 1900s, incidence was reportedly 5-10 cases per 1000
population. Decreased incidence of rheumatic fever has been attributed to the
introduction of penicillin or a change in the virulence of the streptococci.
International
In contrast to trends in the United States, rheumatic fever and RHD have not
decreased in developing countries. Retrospective studies in developing countries
demonstrate the highest figures for cardiac involvement and the highest
recurrence rates of rheumatic fever. Worldwide, an estimated 5-30 million
children and young adults have chronic RHD, and 90,000 patients die from this
disease each year.
A study using echocardiographic screening in schoolchildren in Cambodia and
Mozambique suggests that RHD prevalence may be as much as 10 times that
detected using clinical examination with echocardiographic verification.[2]
Mortality/Morbidity
RHD is the major cause of morbidity from rheumatic fever and is the major cause
of mitral insufficiency and stenosis in the United States and the world. Variables
that correlate with severity of valve disease include the number of previous
attacks of rheumatic fever, the length of time between the onset of disease and
start of therapy, and sex (the prognosis for females is worse than for males).
Insufficiency from acute rheumatic valve disease resolves in 70-80% of patients if
they adhere to antibiotic prophylaxis.
Race
Native Hawaiians and Maori (both of Polynesian descent) have a higher incidence
of rheumatic fever. Incidence of rheumatic fever in these patients is 13.4 per
100,000 hospitalized children per year, even with antibiotic prophylaxis of
streptococcal pharyngitis. Otherwise, race (when controlled for socioeconomic
variables) has not been documented to influence the disease incidence.
-
8/3/2019 sistemik - pedo
6/18
Sex
Rheumatic fever occurs in equal numbers in males and females. Females with
rheumatic fever fare worse than males and have a slightly higher incidence of
chorea.
Age
Rheumatic fever is principally a disease of childhood, with a median age of 10
years; However, GABHS pharyngitis is uncommon in children younger than 3
years, and acute rheumatic fever is extremely rare in these younger children in
industrialized countries. Although less commonly seen in adults compared with
children, rheumatic fever in adults accounts for 20% of cases.
HistoryAcute rheumatic fever (RF) is a systemic disease. Thus, patients may present with
a large variety of symptoms and complaints.
History of an antecedent sore throat 1-5 weeks prior to onset is present in
70% of older children and young adults. Only 20% of younger children
can recall an antecedent sore throat.
Other symptoms on presentation may include fever, rash, headache,
weight loss, epistaxis, fatigue, malaise, diaphoresis, and pallor.
Patients also may have chest pain with orthopnea or abdominal pain and
vomiting. Finally, history may reveal symptoms more specific to rheumatic fever.
o Migratory joint pain
o Nodules under the skin
o Increased irritability and shortened attention span with personality
changes, such as pediatric autoimmune neuropsychiatric disorder
associated with streptococcal infections (PANDAS)
o Motor dysfunction
o History of previous rheumatic fever
Patients with previous rheumatic fever are at a high risk of recurrence.
o
Highest risk of recurrence within 5 years of the initial episodeo Greater risk of recurrence with younger age at the time of the
initial episode
o Generally, recurrent attacks similar to the initial attack (however,
risk of carditis and severity of valve damage increase with each
attack)
Physical
Revised in 1992, the modified Jones criteria provide guidelines for making the
diagnosis of rheumatic fever.[3] The Jones criteria require the presence of 2 major
or 1 major and 2 minor criteria for the diagnosis of rheumatic fever. Having
-
8/3/2019 sistemik - pedo
7/18
evidence of previous group A streptococci (GAS) pharyngitis is also necessary.
These criteria are not absolute, and the diagnosis of rheumatic fever can be made
in patients with only confirmed streptococcal pharyngitis and chorea.
Major diagnostic criteriao Carditis
o Polyarthritis
o Chorea
o Subcutaneous nodules
o Erythema marginatum
Minor diagnostic criteria
o Fever
o Arthralgia
o Prolonged PR interval on electrocardiography
o Elevated acute-phase reactants (APRs), which are erythrocyte
sedimentation rate and C-reactive protein
Three notable exceptions to strict adherence to the Jones criteria
o Chorea: It may occur late and be the only manifestation of
rheumatic fever.
o Indolent carditis: Patients presenting late to medical attention
months after the onset of rheumatic fever may have insufficient
support to fulfill the criteria.
o Newly ill patients with a history of rheumatic fever, especially
rheumatic heart disease (RHD), who have supporting evidence of a
recent GAS infection and who manifest either a single major or
several minor criteria: Distinguishing recurrent carditis frompreexisting significant RHD may be impossible.
Evidence of previous GAS pharyngitis (One of the following must be
present):
o Positive throat culture or rapid streptococcal antigen test
o Elevated or rising streptococcal antibody titer
Major clinical manifestations
o Arthritis
Polyarthritis is the most common symptom and is
frequently the earliest manifestation of acute rheumatic
fever (70-75%).
Characteristically, the arthritis begins in the large joints ofthe lower extremities (ie, knees, ankles) and migrates to
other large joints in the lower or upper extremities (ie,
elbows, wrists).
Affected joints are painful, swollen, warm, erythematous,
and limited in their range of motion. The pain is out of
proportion to clinical findings.
The arthritis reaches maximum severity in 12-24 hours and
persists for 2-6 days (rarely more than 4 wk, but has been
reported to persist 44 d) at each site and is migratory but
not additive.
-
8/3/2019 sistemik - pedo
8/18
The arthritis responds rapidly to aspirin, which decreases
symptoms in affected joints and prevents further migration
of the arthritis.
Polyarthritis is more common and more severe in teenagers
and young adults than in younger children. Patients suffering multiple attacks may exhibit destructive
arthritis (Jaccoud arthritis).
o Carditis
Pancarditis is the most serious complication and the second
most common complication of rheumatic fever (50%).
In advanced cases, patients may experience of dyspnea,
mild-to-moderate chest discomfort, pleuritic chest pain,
edema, cough, or orthopnea.
Upon physical examination, carditis is most commonly
revealed by a new murmur and tachycardia that is out of
proportion to the fever. New or changing murmurstraditionally have been considered necessary for a diagnosis
of rheumatic valvulitis. The murmurs of acute rheumatic
fever are from valve regurgitation, and the murmurs of
chronic rheumatic fever are from valve stenosis.
Frequently examine patients in whom the diagnosis of
acute rheumatic fever is made due to the progressive nature
of the disease. Some cardiologists have proposed that
evidence of new mitral regurgitation from Doppler
echocardiography, even in the absence of accompanying
auscultatory findings, may be sufficient for making the
diagnosis of carditis, particularly if the echocardiography
findings resolve along with other manifestations of
rheumatic fever. This criterion for carditis is not uniformly
accepted and remains specifically excluded in the 1992
revised Jones criteria because of insufficient data at the
time of publication.
Congestive heart failure (CHF) may develop secondary to
severe valve insufficiency or myocarditis. Physical findings
associated with heart failure include tachypnea, orthopnea,
jugular venous distention, rales, hepatomegaly, a gallop
rhythm, and peripheral swelling and edema. A pericardialfriction rub indicates that pericarditis is present. Increased
cardiac dullness to percussion, muffled heart sounds, and a
paradoxical pulse are consistent with pericardial effusion
and impending pericardial tamponade. Confirm this clinical
emergency with ECG, and evacuate the effusion by
pericardiocentesis if it is producing hemodynamic
compromise.
o Chorea: In the absence of a family history of Huntington chorea or
findings consistent with systemic lupus erythematosus, the
diagnosis of acute rheumatic fever is almost certain. A long latency
period exists between streptococcal pharyngitis (1-6 mo) and the
-
8/3/2019 sistemik - pedo
9/18
onset of chorea, and a history of an antecedent sore throat
frequently is not obtained. Patients with chorea often do not
demonstrate other Jones criteria. Chorea is slightly more common
in females than males. Chorea is also known as rheumatic chorea,
Sydenham chorea, chorea minor, and St Vitus dance.o Poststreptococcal movement disorders
Described poststreptococcal movement disorders have
included pediatric autoimmune neuropsychiatric disorder
associated with streptococcal infections (PANDAS) and
Tourette syndrome.
Daily handwriting samples can be used as an indicator of
progression or resolution of disease. Complete resolution of
the symptoms typically occurs, with improvement in 1-2
weeks and full recovery in 2-3 months; however, incidents
have been reported in which symptoms wax and wane for
several years. The PANDAS disorder appears to have a relapsing-
remitting symptom complex characterized by obsessive-
compulsive personality disorder. Patients with Sydenham
chorea and obsessive-compulsive symptoms tend to show
aggressive, contamination, and somatic obsessions and
checking, cleaning, and repeating compulsions. Neurologic
abnormalities include cognitive defects and motoric
hyperactivity. The symptoms may also include emotional
lability, separation anxiety, and oppositional behaviors, and
they are prepubertal in onset.
Some have proposed that the streptococcal infection
triggers the formation of antibodies that cross-react with the
basal ganglia of genetically susceptible hosts in a manner
similar to the proposed mechanism for Sydenham chorea
and causes the symptom complex.
o Erythema marginatum: This characteristic rash, also known as
erythema annulare, occurs in 5-13% of patients with acute
rheumatic fever. Erythema marginatum begins as 1-cm to 3-cm
diameter, pink-to-red nonpruritic macules or papules located on the
trunk and proximal limbs but never on the face. The lesions spread
outward to form a serpiginous ring with erythematous raisedmargins and central clearing. The rash may fade and reappear
within hours and is exacerbated by heat. Thus, if the lesions are not
observed easily, they can be accentuated by the application of
warm towels, a hot bath, or the use of tangential lighting. The rash
occurs early in the course of the disease and remains long past the
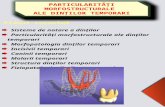
resolution of other symptoms. Erythema marginatum (shown in the
image below) has also been reported in association with sepsis,
drug reactions, and glomerulonephritis.
-
8/3/2019 sistemik - pedo
10/18
Erythema marginatum, the
characteristic rash of acute rheumatic fever.
o Subcutaneous nodules: Subcutaneous nodules are now an
infrequent manifestation of rheumatic fever. The frequency has
declined during the past several years to 0-8% of patients with
rheumatic fever. When present, the nodules appear over the
extensor surfaces of the elbows, knees, ankles, knuckles, scalp, and
spinous processes of the lumbar and thoracic vertebrae (attached to
the tendon sheath). The nodules are firm, nontender, and free from
attachments to the overlying skin, and they range from a few
millimeters to 1-2 cm. The nodules number from 1 to dozens, with
a mean of 3-4. Histologically, the nodules contain areas resembling
the Aschoff bodies observed in the heart. Subcutaneous nodules
generally occur several weeks into the disease and resolve within a
month. They are strongly associated with severe rheumatic carditis,
and in the absence of carditis, question the diagnosis of
subcutaneous nodules.
Other clinical manifestations
o Abdominal pain: Abdominal pain usually occurs at the onset of
acute rheumatic fever, resembles other conditions with acutemicrovascular mesenteric inflammation, and may mimic acute
appendicitis.
o Arthralgias: Patients may report arthralgias upon presentation. In
the history, determining if the patient has taken aspirin or
nonsteroidal anti-inflammatory drugs (NSAIDs) is important
because these may suppress the full manifestations of the disease.
Arthralgia cannot be considered a minor manifestation if arthritis is
present.
o Epistaxis: Epistaxis may be associated with severe protracted
rheumatic carditis.
o Fever: Fevers greater than 39C with no characteristic pattern arepresent initially in almost every patient with acute rheumatic fever.
The fever may be low grade (38-38.5C) in children with mild
carditis or absent in patients with pure chorea. The fever decreases
without antipyretic therapy in approximately 1 week, but low-
grade fevers persist for 2-3 weeks.
o Rheumatic pneumonia: Patients present with the same signs as an
infectious pneumonia. Differentiate rheumatic pneumonia from
respiratory distress related to CHF.
Causes
http://refimgshow%283%29/ -
8/3/2019 sistemik - pedo
11/18
Rheumatic fever is believed to result from an autoimmune response; however, the
exact pathogenesis remains unclear.
Rheumatic fever only develops in children and adolescents following
group A beta hemolytic streptococcal (GABHS) pharyngitis, and onlyinfections of the pharynx initiate or reactivate rheumatic fever.
At least some rheumatogenic strains of GAS have antigenic domains
similar to antigens in components of the human heart, and some authors
have proposed that anti-M antibodies against the streptococci may cross-
react with heart tissue, causing the pancarditis that is observed in
rheumatic fever. So-called molecular mimicry between streptococcal and
human proteins is felt to involve both the B and T cells of peripheral
blood, with infiltration of the heart by T cells. Some believe that an
increased production of inflammatory cytokines is the final mechanism of
the autoimmune reaction that causes damage to cardiac tissue in RHD. An
insufficiency of interleukin-4 (IL-4)producing cells in the valve tissuemay also contribute to the valve lesions.
Streptococcal antigens, which are structurally similar to those in the heart,
include hyaluronate in the bacterial capsule, cell wall polysaccharides
(similar to glycoproteins in heart valves), and membrane antigens that
share epitopes with the sarcolemma and smooth muscle.
Medical Care
Prevention of rheumatic fever in patients with group A beta
hemolytic streptococci (GABHS) pharyngitis
For patients with GABHS pharyngitis, a meta-analysis supported a protective
effect against rheumatic fever (RF) when penicillin is used following the
diagnosis.[4]
Oral (PO) penicillin V remains the drug of choice for treatment of
GABHS pharyngitis, but ampicillin and amoxicillin are equally effective.
When PO penicillin is not feasible or dependable, a single dose of
intramuscular benzathine penicillin G, or benzathine/procaine penicillin
combination is therapeutic.
For patients who are allergic to penicillin, administer erythromycin or a
first-generation cephalosporin. Other options include clarithromycin for 10
days, azithromycin for 5 days, or a narrow-spectrum (first-generation)
cephalosporin for 10 days. As many as 15% of penicillin-allergic patients
are also allergic to cephalosporins.
Do not use tetracyclines and sulfonamides to treat GABHS pharyngitis.
For recurrent group A streptococci (GAS) pharyngitis, a second 10-day
course of the same antibiotic may be repeated. Alternate drugs include
narrow-spectrum cephalosporins, amoxicillin-clavulanate, dicloxacillin,
erythromycin, or other macrolides.
Control measures for patients with GABHS pharyngitis are as follows:
-
8/3/2019 sistemik - pedo
12/18
o Hospitalized patients: Place hospitalized patients with GABHS
pharyngitis of pneumonia on droplet precautions, as well as
standard precautions, until 24 hours after initiation of appropriate
antibiotics.
o Exposed persons: People in contact with patients havingdocumented cases of streptococcal infection first should undergo
appropriate laboratory testing if they have clinical evidence of
GABHS infection and should undergo antibiotic therapy if
infected.
o School and childcare centers: Children with GABHS infection
should not attend school or childcare centers for the first 24 hours
after initiating antimicrobial therapy.
GABHS carriage is difficult to eradicate with conventional penicillin
therapy. Thus, PO clindamycin (20 mg/kg/d PO in 3 divided doses for 10
d) is recommended.
In general, antimicrobial therapy is not indicated for pharyngeal carriers ofGABHS. Exceptions include the following:
o Outbreaks of rheumatic fever or poststreptococcal
glomerulonephritis
o Family history of rheumatic fever
o During outbreaks of GAS pharyngitis in a closed community
o When tonsillectomy is considered for chronic GABHS carriage
o When multiple episodes of documented GABHS pharyngitis occur
within a family despite appropriate therapy
o Following GAS toxic shock syndrome or necrotizing fasciitis in a
household contact
Treatment for patients with rheumatic fever
Therapy is directed towards eliminating the GABHS pharyngitis (if still present),
suppressing inflammation from the autoimmune response, and providing
supportive treatment of congestive heart failure (CHF).
Treat residual GABHS pharyngitis as outlined above, if still present.
Treatment of the acute inflammatory manifestations of acute rheumatic
fever consists of salicylates and steroids. Aspirin in anti-inflammatory
doses effectively reduces all manifestations of the disease except chorea,and the response typically is dramatic.
o If rapid improvement is not observed after 24-36 hours of therapy,
question the diagnosis of rheumatic fever.
o Attempt to obtain aspirin blood levels from 20-25 mg/dL, but
stable levels may be difficult to achieve during the inflammatory
phase because of variable GI absorption of the drug. Maintain
aspirin at anti-inflammatory doses until the signs and symptoms of
acute rheumatic fever are resolved or residing (6-8 wk) and the
acute phase reactants (APRs) have returned to normal.
-
8/3/2019 sistemik - pedo
13/18
o Anti-inflammatory doses of aspirin may be associated with
abnormal liver function tests and GI toxicity, and adjusting the
aspirin dosage may be necessary.
o When discontinuing therapy, withdraw aspirin gradually over
weeks while monitoring the APRs for evidence of rebound. Choreamost frequently is self-limited but may be alleviated or partially
controlled with phenobarbital or diazepam.
If moderate to severe carditis is present as indicated by cardiomegaly,
third-degree heart block, or CHF, add PO prednisone to salicylate therapy.
o Continue prednisone for 2-6 weeks depending on the severity of
the carditis, and taper prednisone during the last week of therapy.
o Discontinuing prednisone therapy after 2-4 weeks, while
maintaining salicylates for an additional 2-4 weeks, can minimize
adverse effects.
Include digoxin and diuretics, afterload reduction, supplemental oxygen,
bed rest, and sodium and fluid restriction as additional treatment forpatients with acute rheumatic fever and CHF. The diuretics most
commonly used in conjunction with digoxin for children with CHF
include furosemide and spironolactone.
o Initiate digoxin only after checking electrolytes and correcting
abnormalities in serum potassium.
o The total loading dose is 20-30 mcg/kg PO every day, with 50% of
the dose administered initially, followed by 25% of the dose 8
hours and 16 hours after the initial dose. Maintenance doses
typically are 8-10 mcg/kg/d PO in 2 divided doses. For older
children and adults, the total loading dose is 1.25-1.5 mg PO, andthe maintenance dose is 0.25-0.5 mg PO every day. Therapeutic
digoxin levels are present at trough levels of 1.5-2 ng/mL.
Afterload reduction (ie, using ACE inhibitor captopril) may be effective in
improving cardiac output, particularly in the presence of mitral and aortic
insufficiency. Start these agents judiciously. Use a small, initial test dose
(some patients have an abnormally large response to these agents), and
administer only after correcting hypovolemia.
When heart failure persists or worsens during the acute phase after
aggressive medical therapy, surgery is indicated to decrease valve
insufficiency.
Treatment for patients following rheumatic heart disease (RHD)
Preventive and prophylactic therapy is indicated after rheumatic fever and RHD to
prevent further damage to valves.
Primary prophylaxis (initial course of antibiotics administered to eradicate
the streptococcal infection) also serves as the first course of secondary
prophylaxis (prevention of recurrent rheumatic fever and RHD).
An injection of 0.6-1.2 million units of benzathine penicillin G
intramuscularly every 4 weeks is the recommended regimen for secondary
prophylaxis for most US patients. Administer the same dosage every 3
-
8/3/2019 sistemik - pedo
14/18
weeks in areas where rheumatic fever is endemic, in patients with residual
carditis, and in high-risk patients.
o Although PO penicillin prophylaxis is also effective, data from the
World Health Organization indicate that the recurrence risk of
GABHS pharyngitis is lower when penicillin is administeredparentally.
o The duration of antibiotic prophylaxis is controversial. Continue
antibiotic prophylaxis indefinitely for patients at high risk (eg,
health care workers, teachers, daycare workers) for recurrent
GABHS infection. Ideally, continue prophylaxis indefinitely,
because recurrent GABHS infection and rheumatic fever can occur
at any age; however, the American Heart Association currently
recommends that patients with rheumatic fever without carditis
receive prophylactic antibiotics for 5 years or until aged 21 years,
whichever is longer.[5] Patients with rheumatic fever with carditis
but no valve disease should receive prophylactic antibiotics for 10years or well into adulthood, whichever is longer. Finally, patients
with rheumatic fever with carditis and valve disease should receive
antibiotics at least 10 years or until aged 40 years.
o Patients with RHD and valve damage require a single dose of
antibiotics 1 hour before surgical and dental procedures to help
prevent bacterial endocarditis. Patients who had rheumatic fever
without valve damage do not need endocarditis prophylaxis. Do
not use penicillin, ampicillin, or amoxicillin for endocarditis
prophylaxis in patients already receiving penicillin for secondary
rheumatic fever prophylaxis (relative resistance of PO streptococci
to penicillin and aminopenicillins). Alternate drugs recommended
by the American Heart Association for these patients include PO
clindamycin (20 mg/kg in children, 600 mg in adults) and PO
azithromycin or clarithromycin (15 mg/kg in children, 500 mg in
adults). Additional guidelines for endocarditis prophylaxis in
patients who are allergic to penicillin or who are unable to receive
PO antibiotics are discussed in the Bacterial Endocarditis article.
o A recent study investigated the difference in clinical manifestations
and outcomes between first episode and recurrent rheumatic fever.[6] The study concluded that subclinical carditis occurred only in
patients experiencing the first episode, and that all deaths occurredin patients with recurrent rheumatic fever, emphasizing the need
for secondary prophylaxis.
Diet
Advise nutritious diet without restrictions except in patients with CHF, who
should follow a fluid-restricted and sodium-restricted diet. Potassium
supplementation may be necessary because of the mineralocorticoid effect of
corticosteroid and the diuretics, if used.
http://emedicine.medscape.com/article/896540-overviewhttp://emedicine.medscape.com/article/896540-overview -
8/3/2019 sistemik - pedo
15/18
Medication Summary
Treatment and prevention of group A streptococci (GAS) pharyngitis outlined
here are based on the current recommendations of the Committee on Infectious
Disease (American Academy of Pediatrics). Medical therapy is directed toward
elimination of GAS pharyngitis (if still present), suppression of inflammation
from the autoimmune response, and supportive treatment of congestive heart
failure (CHF). Attempts are being made to produce vaccines against GAS
infection, but the vaccines will not be available for years.
Antibiotics for endocarditis prophylaxis are administered to patients with certain
cardiac conditions, such as carditis caused by rheumatic fever, before procedures
that may causebacteremia are performed. For more information, see Antibiotic
Prophylactic Regimens for Endocarditis.
Antibiotics
Class Summary
The roles for antibiotics are to (1) initially treat GABHS pharyngitis, (2) prevent
recurrent streptococcal pharyngitis, rheumatic fever (RF), and rheumatic heart
disease (RHD), and (3) provide prophylaxis against bacterial endocarditis.
View full drug information
Penicillin VK (Beepen-VK, Pen.Vee K, V-Cillin K, Veetids)
DOC for treatment of GABHS pharyngitis. Although ampicillin or amoxicillin
may be used instead, they have no microbiologic advantage. Do not use
tetracyclines and sulfonamides to treat GABHS pharyngitis. For recurrent
GABHS pharyngitis, a second 10-d course of same antibiotic may be repeated.
Alternate drugs include narrow-spectrum cephalosporins, amoxicillin-clavulanate,
dicloxacillin, erythromycin, or other macrolides.
Penicillin benzathine (Bicillin L-A) or penicillin procaine(Crysticillin A.S., Wycillin)
Used when PO administration of penicillin is not feasible or dependable. IM
therapy with penicillin is painful, but discomfort may be minimized if penicillin G
is brought to room temperature before injection or combination of benzathine
penicillin G and procaine penicillin G is used. Initial course of antibiotics
administered to eradicate streptococcal infection also serves as first course of
prophylaxis. An injection of benzathine penicillin G IM q4wk is recommended
regimen for secondary prevention for most United States patients. Administer
http://emedicine.medscape.com/article/961169-overviewhttp://web.archive.org/web/20060209093103/http/master.emedicine.com/drugs/Endocarditis_Prophylaxis.htmhttp://web.archive.org/web/20060209093103/http/master.emedicine.com/drugs/Endocarditis_Prophylaxis.htmhttp://reference.medscape.com/drug/pen-vee-k-penicillin-v-penicillin-vk-342483#1http://reference.medscape.com/drug/pen-vee-k-penicillin-v-penicillin-vk-342483#1http://emedicine.medscape.com/article/961169-overviewhttp://web.archive.org/web/20060209093103/http/master.emedicine.com/drugs/Endocarditis_Prophylaxis.htmhttp://web.archive.org/web/20060209093103/http/master.emedicine.com/drugs/Endocarditis_Prophylaxis.htmhttp://reference.medscape.com/drug/pen-vee-k-penicillin-v-penicillin-vk-342483#1http://reference.medscape.com/drug/pen-vee-k-penicillin-v-penicillin-vk-342483#1 -
8/3/2019 sistemik - pedo
16/18
same dosage q3wk in areas where RF is endemic, in patients with residual
carditis, and in high-risk patients.
View full drug information
Erythromycin (E.E.S., E-Mycin, Eryc, Ery-Tab, Erythrocin)
Used for patients who are allergic to penicillin. Other options include
clarithromycin, azithromycin, or a narrow-spectrum cephalosporin (ie,
cephalexin). As many as 15% of penicillin-allergic patients are also allergic to
cephalosporins.
View full drug information
Clarithromycin (Biaxin)
Alternate antibiotic for treating GAS pharyngitis in patients allergic to penicillin.
View full drug information
Azithromycin (Zithromax)
Alternate antibiotic for treating GAS pharyngitis in patients allergic to penicillin.
View full drug information
Cephalexin (Keflex, Biocef, Keftab)
Alternate antibiotic for treating GAS pharyngitis in patients allergic to penicillin.
View full drug information
Amoxicillin (Amoxil, Biomox, Trimox)
DOC used for bacterial endocarditis prophylaxis. Administered as single PO dose
1 h before dental work or surgery.
Anti-inflammatory agents
http://reference.medscape.com/drug/ees-eryped-erythromycin-ethylsuccinate-999596#1http://reference.medscape.com/drug/ees-eryped-erythromycin-ethylsuccinate-999596#1http://reference.medscape.com/drug/biaxin-xl-clarithromycin-342524#1http://reference.medscape.com/drug/biaxin-xl-clarithromycin-342524#1http://reference.medscape.com/drug/zithromax-azithromycin-342523#1http://reference.medscape.com/drug/zithromax-azithromycin-342523#1http://reference.medscape.com/drug/keflex-cephalexin-342490#1http://reference.medscape.com/drug/keflex-cephalexin-342490#1http://reference.medscape.com/drug/amoxil-moxatag-amoxicillin-342473#1http://reference.medscape.com/drug/amoxil-moxatag-amoxicillin-342473#1http://reference.medscape.com/drug/ees-eryped-erythromycin-ethylsuccinate-999596#1http://reference.medscape.com/drug/ees-eryped-erythromycin-ethylsuccinate-999596#1http://reference.medscape.com/drug/biaxin-xl-clarithromycin-342524#1http://reference.medscape.com/drug/biaxin-xl-clarithromycin-342524#1http://reference.medscape.com/drug/zithromax-azithromycin-342523#1http://reference.medscape.com/drug/zithromax-azithromycin-342523#1http://reference.medscape.com/drug/keflex-cephalexin-342490#1http://reference.medscape.com/drug/keflex-cephalexin-342490#1http://reference.medscape.com/drug/amoxil-moxatag-amoxicillin-342473#1http://reference.medscape.com/drug/amoxil-moxatag-amoxicillin-342473#1 -
8/3/2019 sistemik - pedo
17/18
Class Summary
Manifestations of acute rheumatic fever (including carditis) typically respond
rapidly to therapy with anti-inflammatory agents. Aspirin, in anti-inflammatory
doses, is DOC. Prednisone is added when evidence of worsening carditis andheart failure is noted.
View full drug information
Aspirin (Anacin, Ascriptin, Bayer Aspirin)
Begin administration immediately after diagnosis of RF. Initiation of therapy may
mask manifestations of disease.
View full drug information
Prednisone (Deltasone, Orasone)
If moderate-to-severe carditis is present as indicated by cardiomegaly, CHF, or
third-degree heart block, use 2 mg/kg/d PO prednisone in addition to or in lieu of
salicylate therapy. Continue prednisone for 2-4 wk depending on severity of
carditis and taper during last week of therapy. Discontinuing prednisone therapy
after 2 wk while adding or maintaining salicylates for additional 2-4 wk may
minimize adverse effects.
Therapy for congestive heart failure
Class Summary
Heart failure in RHD probably is related in part to severe insufficiency of the
mitral and aortic valves and in part to pancarditis. Therapy traditionally has
consisted of an inotropic agent (digitalis) in combination with diuretics
(furosemide, spironolactone) and afterload reduction (captopril).
View full drug information
Digoxin (Lanoxin, Lanoxicaps)
Inotropic agent widely used in past. Its efficacy in CHF is under review. Potential
for toxicity is present. Therapeutic levels and clinical effects are observed more
quickly if loading doses of digitalis are administered before routine maintenance
doses. Acts directly on cardiac muscle, increasing myocardial systolic
contractions. Indirect actions result in increased carotid sinus nerve activity and
http://reference.medscape.com/drug/zorprin-bayer-buffered-aspirin-343279#1http://reference.medscape.com/drug/zorprin-bayer-buffered-aspirin-343279#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/lanoxin-digoxin-342432#1http://reference.medscape.com/drug/lanoxin-digoxin-342432#1http://reference.medscape.com/drug/zorprin-bayer-buffered-aspirin-343279#1http://reference.medscape.com/drug/zorprin-bayer-buffered-aspirin-343279#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/lanoxin-digoxin-342432#1http://reference.medscape.com/drug/lanoxin-digoxin-342432#1 -
8/3/2019 sistemik - pedo
18/18
enhanced sympathetic withdrawal for any given increase in mean arterial
pressure. Therapeutic digoxin levels are present at trough levels of 1.5-2 ng/mL.
View full drug information
Captopril (Capoten)
Systemic afterload reduction may be helpful in improving cardiac output,
particularly in setting of mitral and aortic valve insufficiency. Some patients have
unusually large hypotensive response. Use small starting dose, particularly with
hypovolemia.
View full drug information
Furosemide (Lasix)
Diuretics frequently are used in conjunction with inotropic agents for patients
with CHF. When used aggressively, may result in hypokalemia and hypovolemia.
Risk of hearing loss in premature infants.
Increases excretion of water by interfering with chloride-binding cotransport
system, which, in turn, inhibits sodium and chloride reabsorption in ascending
loop of Henle and distal renal tubule.
View full drug information
Spironolactone (Aldactone)
Used in conjunction with furosemide as potassium-sparing diuretic.
Competes with aldosterone for receptor sites in distal renal tubules, increasing
water excretion while retaining potassium and hydrogen ions.
http://reference.medscape.com/drug/capoten-captoril-captopril-342315#1http://reference.medscape.com/drug/capoten-captoril-captopril-342315#1http://reference.medscape.com/drug/lasix-furosemide-342423#1http://reference.medscape.com/drug/lasix-furosemide-342423#1http://reference.medscape.com/drug/aldactone-spironolactone-342407#1http://reference.medscape.com/drug/aldactone-spironolactone-342407#1http://reference.medscape.com/drug/capoten-captoril-captopril-342315#1http://reference.medscape.com/drug/capoten-captoril-captopril-342315#1http://reference.medscape.com/drug/lasix-furosemide-342423#1http://reference.medscape.com/drug/lasix-furosemide-342423#1http://reference.medscape.com/drug/aldactone-spironolactone-342407#1http://reference.medscape.com/drug/aldactone-spironolactone-342407#1