SIADH n DI
47
Disorders of Water Balance: Diabetes Insipidus and SIADH Louis J. Muglia, MD PhD Division of Pediatric Endocrinology and Metabolism Washington University School of Medicine
-
Upload
abel-brown -
Category
Documents
-
view
233 -
download
0
Transcript of SIADH n DI

Disorders of Water Balance: Diabetes Insipidus and SIADH
Louis J. Muglia, MD PhDDivision of Pediatric Endocrinology and
MetabolismWashington University School of Medicine

Physiology of Volume and Osmolarity Balance
• Renin-angiotensin-aldosterone system– Modulates sodium
retention by kidney – Serves to restore
intravascular volume status
– Once euvolemic will be suppressed and sodium will be lost in urine
• Vasopressin/thirst– Modulates water
ingestion/excretion– Serves to restore
normal osmolarity, activated to restore volume with severe hypovolemia

Normal Regulation of Body Water

Hypothalamic Nuclei in Water Regulation

Arginine Vasopressin Structure
Cys-Tyr-Phe-Gln-Asn-Cys-Pro-Arg-Gly-NH21 9
Cys-Tyr-Ile-Gln-Asn-Cys-Pro-Pro-Gly-NH21 9
Cys-Tyr-Phe-Gln-Asn-Cys-Pro-DArg-Gly-NH21 9
NH2-
NH2-
dDAVP
Oxytocin
AVP

Vasopressin Gene Structure
AVPSignal Neurophysin II Copeptin
Gly-Lys-Arg Arg
Exon A Exon B Exon C

Vasopressin Receptors
• V1a - localized to smooth muscle, hepatocytes, and platelets. Induces calcium flux and phosphatidyl inositol hydrolysis.
• V1b - localized to pituitary corticotrophs, augments ACTH release. Similar ligand binding and signaling to V1a.
• V2 - renal collecting ducts, periglomerular tubules, vascular endothelial cells. Activates adenylyl cyclase and stimulates vWF, VIIIa, and plasminogen activator.

QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture.
V2 Receptor Structure and Mutations
From Brenner and Rector's, The Kidney,Volume 2, A. Bonnardeaux and D.G. Bichet 2004


QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture.
Aquaporin-2 Structure and Mutations
From Brenner and Rector's, The Kidney,Volume 2, A. Bonnardeaux and D.G. Bichet 2004

Stimuli for Vasopressin Release
• Serum Osmolarity• Depleted Intravascular Volume• Nausea• Nicotine• Hypoglycemia

Relationship of Vasopressin Release and Thirst
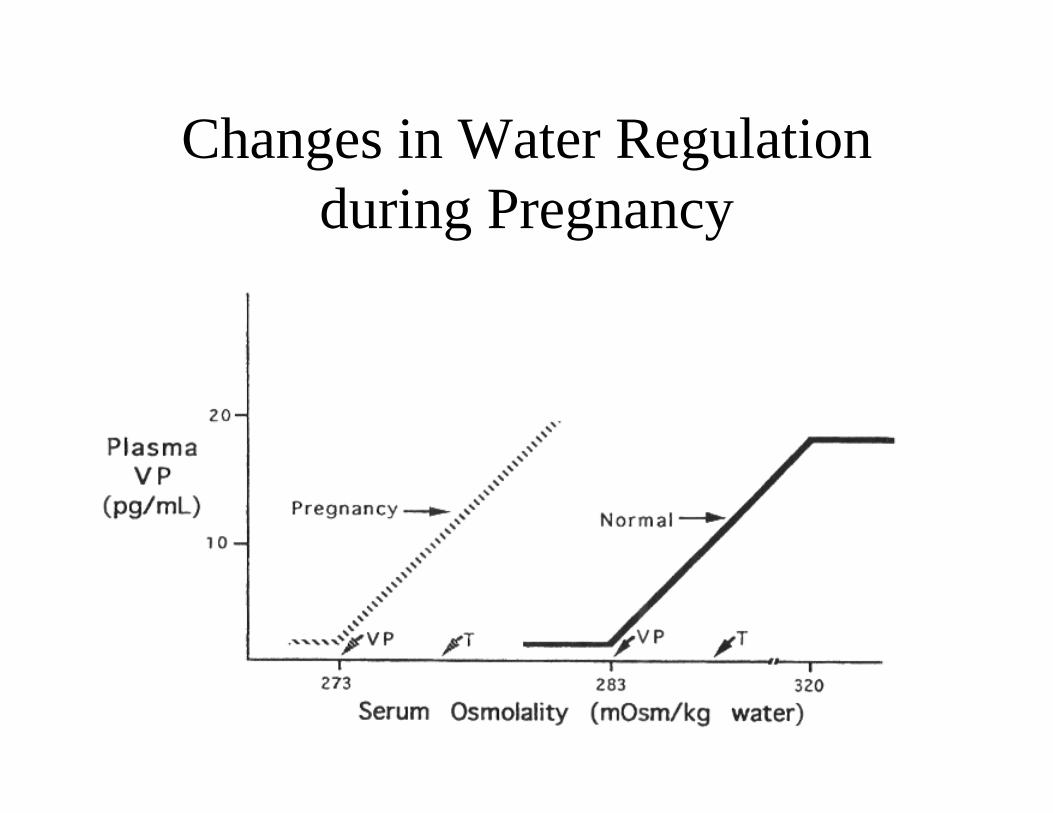
Changes in Water Regulation during Pregnancy

Effect of Volume Changes on Vasopressin Release
0 1 2 3 4 5 6 7 8 9 100
25
50
75
100
Age (years)
Bod
y W
ater
(% o
f bod
y w
eigh
t)
Total
Intracellular
Extracellular
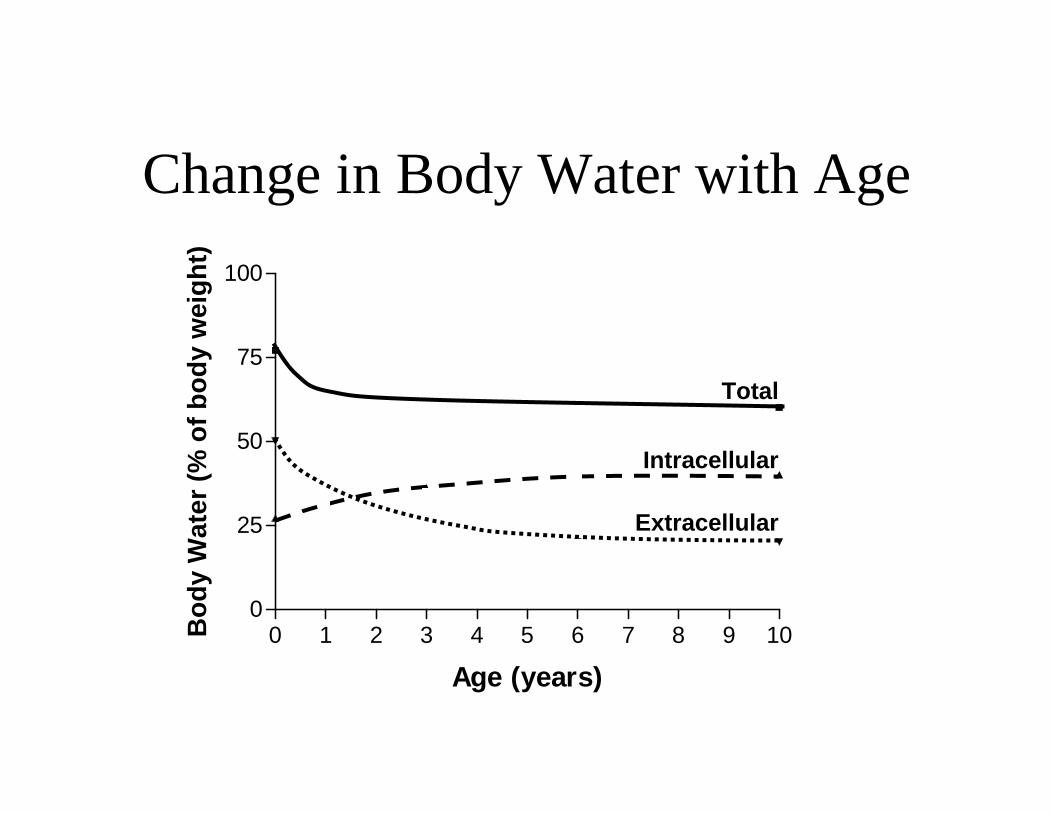
Change in Body Water with Age

Body Fluids
• Total body water: 80% of body weight in infants, 60% in children and adults– Extracellular: 40% of BW in infants, 20% later
(15% interstitial and 5% intravascular)– Intracellular: 40% of BW
• Sodium is the principal volume regulator, exerting effects over TBW

Water Requirements
• What is maintenance fluid volume?• Losses per day:
– Respiratory and skin: 500 ml/m2/d– Gastrointestinal: 100 ml/m2/d– Urine (at 400-500 mOsm/kg): 1150 ml/m2/d
• Sources:– Water of oxidation: 250 ml/m2/d
• Net: 1,500 ml/m2/d

Calculation of Water Deficit
• Water deficit = usual BW - current BW• Usual BW = current weight x 0.6 x current
Osm/normal Osm

Electrolyte Requirements
• Sodium: 20 - 50 mEq/m2/d• Potassium: 20 - 50 mEq/m2/d• Calcium (elemental):
– Newborns 50-75 mg/kg/d (term)– Infants 600 mg/d– Children 800 mg/d– Adolescents 1200 mg/d– Acute treatment of hypocalcemia: 10 mg/kg IV
followed by 50 mg/kg/d IV

Glucose Requirements
• Providing 5% dextrose-containing solutions normally adequate to stop ketone production in normal individuals, but still catabolic
• Important to prevent catabolism in patients with inborn errors of metabolism, so provide at least hepatic glucose production rate = 0.0014x3 -0.214x2 + 10.411x - 9.084 (x is body weight in kg; glucose prodution rate in mg/min)
• For children, this is approximately 6-8 mg/kg/min

Determination of Ongoing Losses
• Measure volume of output site - emesis, stool, ostomy drainage, etc.
• Know general electrolyte composition of drainage from that site (e.g., sodium in gastric contents = 50 mEq/l; bile 130 mEq/l; stool 50 mEq/l) to determine best replacement fluid

What determines urine volume?
• Solute excretion - usually 500 mOsm/m2/d• Urine concentration
– If maximally concentrated = 1200 mOsm/kg– If minimally concentrated = 100 mOsm/kg
• So, for SIADH you need to provide 500/1200 + 0.5 + 0.1 - 0.25 = 0.8 l/m2/d
• For DI, same calculations lead to 5 l/m2/d -don’t try and replace urine output!
Acute Fluid Resuscitation
• Weigh the patient• For signs of cardiovascular compromise,
volume expand with isotonic saline (0.9% NaCl or Ringer’s lactate) in 10-20 cc/kg boluses
• Consider including 5% dextrose (if only acutely hypoglycemic, 2-4 cc/kg D25)

Isotonic Dehydration
• Most common form of dehydration (80%)• Proportional loss of water and solute, thus no
redistribution from ECF to ICF• Typically replace half the deficit over 8 h and
remainder over next 16 h• Alternatively, can provide 3 l/m2/d in replacement
phase• D5 1/4-1/2 NS appropriate depending upon
ongoing sodium losses

Hyponatremia with Dehydration(Na+ < 130 mEq/L)
• With appropriate increase in vasopressin– Severe dehydration– Decreased effective circulating volume
• CHF, cirrhosis, nephrotic syndrome, positive pressure ventilation
• Therapy: rehydration with salt-containing fluid for dehydration.

Correction of Hyponatremic Dehydration
• Similar management as isotonic dehydration except for calculation of additional sodium replacement
• Extra Na+ = (135-measured Na) x total body water
• Example: 10% dehydration in 30 kg child with Na 128 mEq/l = (135-128) x 0.6 x 30 = 126 mEq; water deficit 0.6*30*0.1= 1.8 L
• Therefore, to replace half deficit over 12 h give 63 mEq in 0.9 L or D5 .45 NS at 75 cc/h above maintenance
Symptomatic Hyponatremia
• Mental status changes, seizures• Rapid correction of sodium up to level that
stops seizure activity• Use 3% NaCl to deliver approximately 5
mEq/kg/hr. If due to SIADH, give lasix to prevent sodium dumping with volume expansion.

Adaptation to Hyponatremia
Limitations in Correction of Hyponatremia
• Acute changes can probably be safely corrected in a rapid fashion
• Chronic (more than 24 h) hyponatremia should be corrected slowly (< 0.5 mEq/L/hr) to avoid central pontine myelinolysis

Hyponatremia without Dehydration(Na+ < 130 mEq/L)
• With inappropriate increase in vasopressin (SIADH)– Uncommon, but many etiologies.
• Therapy: Fluid restriction - restrict to volume required for excretion of solute with maximally concentrated urine (0.4 l/m2/d) plus insensible loss (0.4 l/m2/d). If mental status changes, 3% normal saline and lasix.
Hyponatremia(Na+ < 130 mEq/L)
• Due to sodium chloride loss– Renal disease– Mineralocorticoid deficiency– Diuretic use– Gastrointestinal disease– Cystic fibrosis– Increased secretion of ANP (cerebral salt-wasting)
• Therapy: salt supplementation

The Natriuretic Peptides
Cys
Cys
NH2
NH2
NH2
HOOC
HOOC
HOOC
ANP
BNP
CNP
NPR-A, C
NPR-B, C
LIGAND RECEPTOR
Cys
Cys
Cys
Cys

Findings in Cerebral Salt-Wasting
SIADH CSW CDIPlasma volume ↑ ↓ ↓Clinical evidence of volume depletion − + +Serum sodium/osmolality ↓ ↓ ↑Urine sodium/osmolality ↑ ↑↑ ↓Urine flow rate ↓ ↑↑ ↑Plasma renin activity ↓ ↓ ↑Plasma aldosterone concentration ↓ or → ↓ ↑Plasma AVP concentration ↑ ↑ or → ↓BUN/Creatinine ↓/↓ ↑/↑ ↓/↑Hematocrit ↓ ↑ ↑Albumin concentration ↓ ↑ ↑Serum uric acid concentration ↓ ↓ or → ↑Plasma ANP or BNP concentration ↑ ↑ ↓
Treatment Fluid restrictionSalt and fluidreplacement
Salt poor fluidreplacement

Hyponatremia without Dehydration(Na+ < 130 mEq/L)
• With normal regulation of vasopressin– Primary polydipsia– Decreased free water clearance
• Adrenal (glucocorticoid) deficiency• Hypothyroidism• Drugs
– Cyclophosphamide, tegretol, cis-platinum
• Therapy at underlying cause

Hyponatremia(Na+ < 130 mEq/L)
• With normal osmolarity– Hyperglycemia
• Decrease in serum sodium 1.6 mEq/L for each 100 mg/dl increase in glucose above 100 mg/dl
– Hyperlipidemia - “factitious”

Evaluation of Hyponatremia

Hypertonic Dehydration
• Volume loss with serum sodium above 150 mEq/L• Goal is to lower sodium not more rapidly than 0.5
mEq/L/h and correct fluid deficit over 48 - 72 h• To calculate water deficit:
– Deficit = ((Nameasured - 140)/140)0.6 Weightnow
• Can also begin therapy with fluids at 2 l/m2/d and monitor rate of correction
• D5 0.2NS or D5W (diabetes insidipus) appropriate rehydration fluids

How do you evaluate polyuria and polydipsia?
• History • Objective assessment• Random labs• Additional outpatient laboratories• Water deprivation test• Imaging studies
Laboratory Confirmation of DI
• Polyuria and polydipsia with serum Osm above 300 mOsm/kg and urine Osm less than 300 mOsm/kg
• Not usually achieved with random screening labs
• Proceed to water deprivation

Water Deprivation TestingWater Deprivation Phase
• Obtain initial weight, vitals and document duration of pretest water restriction (ifany)
• Place intravenous line to assist with repeated blood drawing, and place foleycatheter in children too young to provided hourly voided urine specimens
• Obtain baseline serum Na, vasopressin, urine osmolality and urine specificgravity.
• Begin (or continue) water deprivation• Measure and record hourly a flow sheet:
o Weight, HR, BP, urine output and urine specific gravity.o Stat laboratory testing: serum sodium and urine osmolality.
• If Na < 145, urine osmolality<600, and there is no clinical evidence of significant,symptomatic hypovolemia, continue water deprivation.
• If urine osmolality is above 1000, or above 600 and stable over 2 measures, stoptest. Patient does not have diabetes insipidus.
• If serum osmolality is above 300 and urine osmolality is below 600, the patienthas diabetes insipidus. Proceed to Vasopressin response phas e
Vasopressin Response Phase
• Collect blood for vasopressin level.• Administer Pitressin, 1 unit/m2, SQ• Allow the patient to eat, and drink, limiting fluid intake to the volume of urine
produced during the entire testing period (water deprivation and vasopressinresponse)
• 30 and 60 minutes after Pitressin, measure vital signs, urine output, and urinespecific gravity, and send urine to lab for osmolality.
• A two fold increase in urine osmolality indicates central diabetes insipidus.• An increase of less then 2 fold in urine osmolality is consistent with nephrogenic
diabetes insipidus.

Causes of Diabetes Insipidus
• Central DI– Genetic: Familial Autosomal Dominant, Wolfram
(DIDMOAD), Septo-optic Dysplasia– Trauma– Iatrogenic– Anatomical defects in hypothalamus– Neoplasms– Infiltrative,autoimmune, infectious diseases– Increased vasopressin metabolism

Causes of Diabetes Insipidus• Nephrogenic DI
– Genetic: X-linked vasopressin V2 receptor mutations; Autosomal recessive aquaporin 2 mutations
– Acquired• Drugs: demeclocycline, lithium• Electrolyte disturbance: hypercalcemia,
hypokalemia• Renal damage

Triphasic Response after Pituitary Stalk Damage
Postoperative Days
Urin
e V
olum
e 3-7 days

Perioperative Fluid Management for Hypothalamic/Pituitary Surgery
• Provide basal fluids to replace insensible losses and obligate urine output assuming maximally concentrated urine = 1 L/m2/d with D5 1/4NS
• Replace urine output to a maximum of 4 L/m2/d with D5W
• If patient has DI, expect serum sodium to run about 150 mEq/L
• Alternatively, can restrict fluids to 1 L/m2/d and give Pitressin intravenously at 1.5 mU/kg/h

Chronic Management of Central Diabetes Insipidus
• With intact thirst mechanism, fluids based upon thirst and dDAVP dosed to allow 1-2 hours of polyuria per day to minimize risk for hyponatremia
• Relative potency: Oral 1, Nasal 20-100, subQ 200-1000
• With disrupted thirst, both fluids and dDAVP need to be prescribed.

Treatment of Nephrogenic DI
• Identify underlying disorder and treat• Minimize solute load for excretion (foods
with the highest caloric/osmotic load ratio)• Thiazides to decrease GFR and distal tubule
water delivery– With amiloride or indomethacin