Severe Dengue: risk factors and management sharing/Severe... · Dengue fever without warning signs...
91
Severe Dengue: risk factors and management 高雄長庚 李允吉醫師
Transcript of Severe Dengue: risk factors and management sharing/Severe... · Dengue fever without warning signs...

Severe Dengue: risk factors and
management
高雄長庚
李允吉醫師

Outline
• Dengue case management
• Clinical manifestations and risk factors for
severe dengue
• Severe dengue in adults (KSCGMH
preliminary data)

Dengue case management

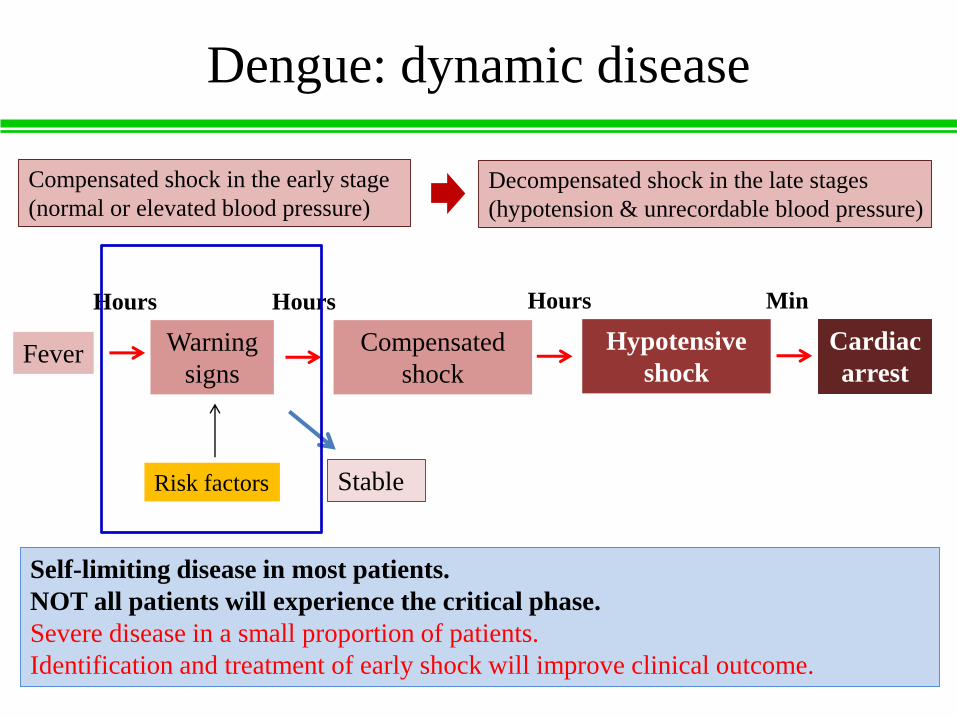
Dengue: dynamic disease
Compensated shock in the early stage
(normal or elevated blood pressure)
Decompensated shock in the late stages
(hypotension & unrecordable blood pressure)
Fever Warning
signs
Compensated
shock
Hypotensive
shock
Cardiac
arrest
Hours MinHours Hours
Self-limiting disease in most patients.
NOT all patients will experience the critical phase.
Severe disease in a small proportion of patients.
Identification and treatment of early shock will improve clinical outcome.
Risk factors Stable

Patient assessment
In which phase of disease is the patient? Day onset of illness
How much oral fluid intake ?
How much urine output ?
Fluid losses: diarrhea, vomiting
Presence of warning signs
Risk factors: infancy, pregnancy, diabetes mellitus, old age,
renal failure
What was the patient’s pulse volume?

Patient assessment
• Hemodynamic assessment is the foundation of dengue
clinical management
Parameters
Conscious level Organ perfusion (brain)
Capillary refill time
Peripheral perfusionExtremities (color, temp)
Peripheral pulse volume
Heart rate
Cardiac output Pulse pressure
Blood pressure
Respiratory rate Respirator compensation (tissue hypoxia)
Urine output Organ perfusion (kidney)
CCTV-R
1. Skin color
2. Capillary refill
3. Temperature
4. Pulse volume
5. Pulse rate
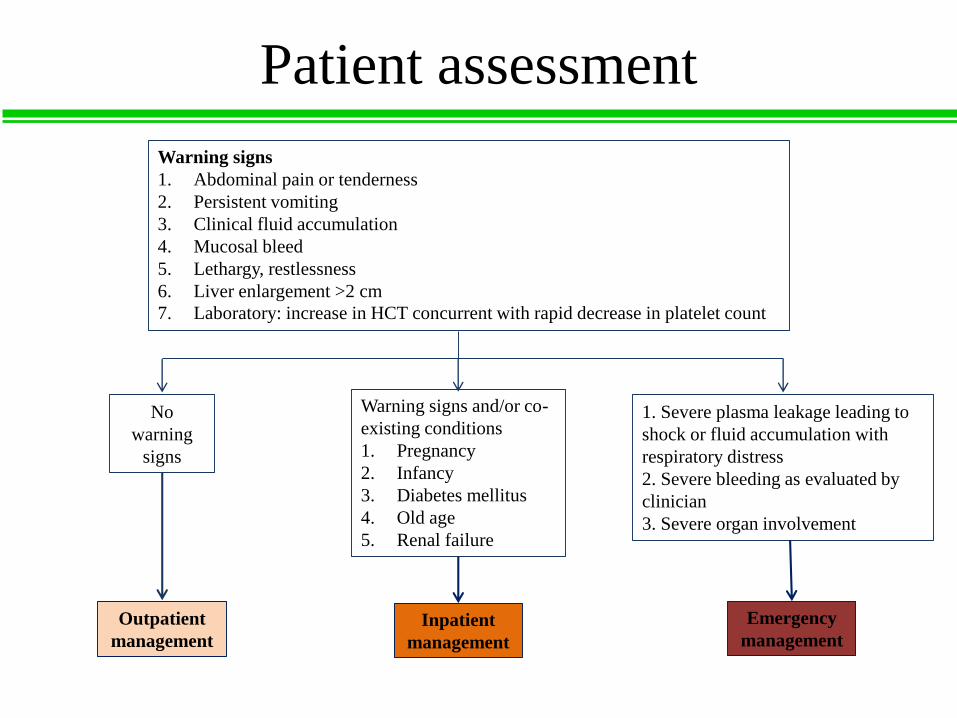
Patient assessment
Warning signs
1. Abdominal pain or tenderness
2. Persistent vomiting
3. Clinical fluid accumulation
4. Mucosal bleed
5. Lethargy, restlessness
6. Liver enlargement >2 cm
7. Laboratory: increase in HCT concurrent with rapid decrease in platelet count
No
warning
signs
Warning signs and/or co-
existing conditions
1. Pregnancy
2. Infancy
3. Diabetes mellitus
4. Old age
5. Renal failure
1. Severe plasma leakage leading to
shock or fluid accumulation with
respiratory distress
2. Severe bleeding as evaluated by
clinician
3. Severe organ involvement
Outpatient
management
Inpatient
management
Emergency
management

Principle of case management
DON’T use corticosteroids. They are not indicated and can increase the risk of
GI bleeding, hyperglycemia, and immunosuppression.
DON’T give platelet transfusions for a low platelet count. Platelet
transfusions do not decrease the risk of severe bleeding and may instead
lead to fluid overload and prolonged hospitalization.
DON’T give half normal (0.45%) saline. Half normal saline should not be
given, even as a maintenance fluid, because it leaks into third spaces and may
lead to worsening of ascites and pleural effusions.
DON’T assume that IV fluids are necessary. First check if the patient can take
fluids orally. Use only the minimum amount of IV fluid to keep the patient
well-perfused. Decrease IV fluid rate as hemodynamic status improves or
urine output increases.
DON’T give ibuprofen, aspirin, or aspirin-containing drugs, and intramuscular
injection.

Dengue fever without warning signs
(Outpatient Management)
• Prevent dehydration:
(1) Give plenty of fluids (not only water)
(2) Watch for signs of dehydration
▶ Decrease in urination
▶ Few or no tears when child cries
▶ Dry mouth, tongue or lips
▶ Sunken eyes
▶ Listlessness, agitation, or confusion
▶ Fast heartbeat (>100/min)
▶ Cold or clammy fingers and toes
▶ Sunken fontanel in an infant
• Watch for warning signs

Dengue fever with warning signs
(Inpatient Management)
Monitor fluid intake/output
and encourage oral fluid
intake
Obtain baseline complete
blood count
Monitor vital signs every 4
hours
Does patient
have adequate
oral fluid intake?
Adequate oral fluid
intake
Observe for warning
signs and early shock
Inadequate oral fluid
intake

Dengue fever with warning signs
(Inpatient Management)
Inadequate oral fluid
intake
Check HCT
Give isotonic crystalloids in stepwise manner:
1. 5-7ml/kg/h for 1-2 h
2. 3-5ml/kg/h for 2-4 h
Stable and no change or
minimal change in HCTWorsening vital signs
and increasing HCTContinue isotonic
crystalloids: 2-3ml/kg/h
for 2-4 h
Adequate fluid and urine
output (0.5 ml/kg/h); HCT
decreases to baseline.
Stop IVF therapy within
24–48 h
Isotonic crystalloids:
5-10ml/kg/h for 1-2 h
Recheck HCT
Reassess vital signs
Patient improving:
Reduce fluid (stepwise);
reassess before each change
1. 5-10 ml/kg/h for 1-2 h
2. 3-5 ml/kg/h for 2-4 h
3. 2-3 ml/kg/h for 2-4 h
Stop IV fluids at 48 h
Normal saline, Ringer’s lactate
No improved:
Emergency management

Parameters Compensated shock Hypotension shock
Conscious level Clear and lucid Restless
Capillary refill time > 2 sec Very prolonged, mottled
skin
Extremities (color, temp) Cool Cold, clammy
Peripheral pulse volume Weak Feeble, absent
Heart rate Tachycardia Severe tachycardia or
bradycardia in late shock
Blood pressure Normal systolic
pressure, rising diastolic
pressure
Hypotension;
unrecordable BP
Pulse pressure Narrowing, postural
hypotension
≤ 20mmHg
Respiratory rate Tachypnea Kussmaul breathing
Urine output Reduced Oliguria/anuria
How long does plasma leakage last?
24 – 48 hours

Compensated shock
Systolic pressure maintained but has
signs of reduced perfusion
Isotonic crystalloid§5–10 ml/kg/h over 1 h
Hemodynamic status improved Hemodynamic status
not improved (HCT)Reduce fluid (stepwise):
1. 5–7 ml/kg/h for 1–2 h
2. 3–5 ml/kg/h for 2–4 h
3. 2–3 ml/kg/h for 2–4 h
Recheck HCT; reassess
clinical status
If: adequate fluid intake and
urine output; HCT at baseline
or slightly below baseline,
Then: DC intravenous fluids
(stop at 48 hours)
Increasing HCT
Given isotonic
crystalloid10-
20ml/kg bolus 1h
Improving:
Reduce fluid to 7-
10ml/kg/h for 1-2 h
Then reduce further
Obtain HCT and organ
function tests
§Normal saline, Ringer’s
lactate
Decreasing HCT
Initiate transfusion
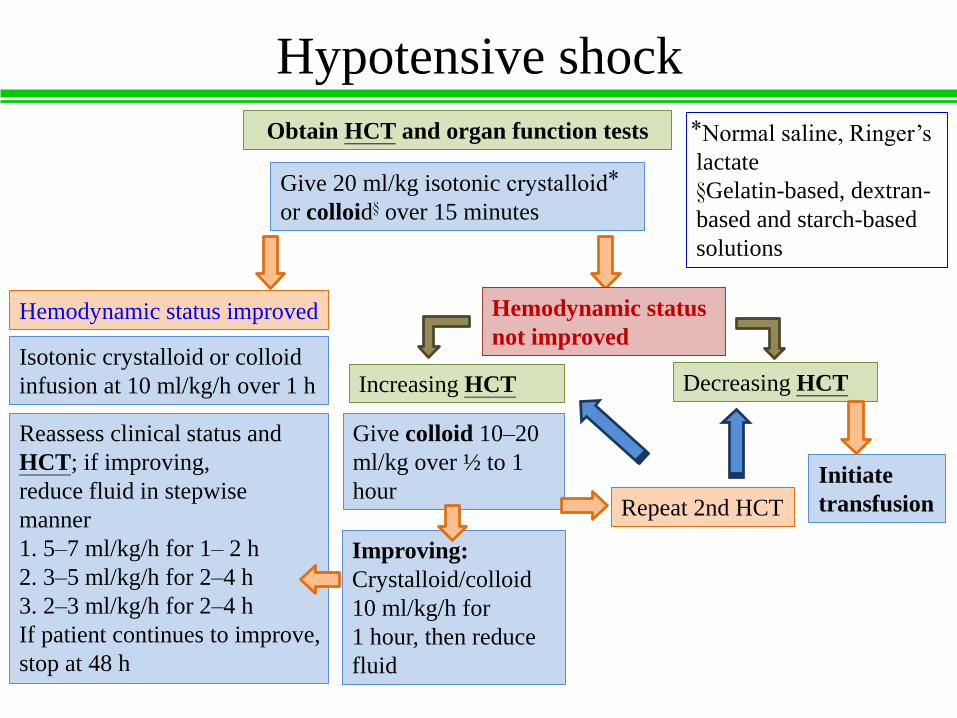
Hypotensive shock
Obtain HCT and organ function tests
Give 20 ml/kg isotonic crystalloid
or colloid§ over 15 minutes
Hemodynamic status improved Hemodynamic status
not improved Isotonic crystalloid or colloid
infusion at 10 ml/kg/h over 1 h
Reassess clinical status and
HCT; if improving,
reduce fluid in stepwise
manner
1. 5–7 ml/kg/h for 1– 2 h
2. 3–5 ml/kg/h for 2–4 h
3. 2–3 ml/kg/h for 2–4 h
If patient continues to improve,
stop at 48 h
Increasing HCT
Give colloid 10–20
ml/kg over ½ to 1
hour
Improving:
Crystalloid/colloid
10 ml/kg/h for
1 hour, then reduce
fluid
Decreasing HCT
Initiate
transfusionRepeat 2nd HCT
Normal saline, Ringer’s
lactate
§Gelatin-based, dextran-
based and starch-based
solutions

Hematocrit
levels
Increase Decrease NO change (or
minimal
change)
Disease
associated
Plasma leakage 1. Bleeding
2. Reabsorption
Plasma leak +
bleeding
Treatment
related
Blood
transfusion
1. Intravenous
fluid therapy
Disease +
treatment
Plasma leak +
IV fluids
or
Bleeding +
blood
transfusion
Phase of disease, day 2 vs. day 5
Hemodynamic state should be the principal driver of IV fluid therapy
HCT level should only be guide

Rising or high HCT + Unstable hemodynamic state
Active plasma leakage, fluid replacement
Decrease HCT + Unstable hemodynamic state
Bleeding, need for urgent transfusion
Rising or high HCT + Stable hemodynamic state
Does not require intravenous fluid, continue to monitor
Decrease HCT + Stable hemodynamic state
Hemodilution or reabsorption, reduced or DC intravenous fluid

When to start and stop intravenous
fluid therapy
Febrile phase: oral fluid advice
Critical phase: IV fluids are usually required for 24–48 hours
Recovery phase: IV fluids should be stopped so that
extravasated fluids can be reabsorbed

4 Intravenous Fluid Regimens for DSS
in the First Hour
Dextran 70
(n = 55)
Gelatin
(n = 56)
Lactated
Ringer’s
(n = 55)
Normal
saline
(n = 56)
P
“Reshock” rate, no. (%) of
patients
16 (29.1) 15 (26.8) 16 (29.1) 16 (28.6) .992
Decrease in hematocrit at 1 h,
% (mean)
11.5 (3.3) 9.7 (3.0) 5.7 (2.8) 6.5 (2.9) <.001
Decrease in pulse at 1 h,
beats/min (mean)
14.9 (9.9) 18.5 (11.3) 13.2 (9.2) 13.5 (8.9) .023
Total volume of iv fluid
infused, mL/kg (mean)
134.3 (22.1) 135 (23.5) 134.2 (19.9) 132.9 (16.6) 954
Required frusemide, no. (%)
of patients
5 (9.1) 10 (17.9) 8 (14.5) 12 (21.4) .328
Clin Infect Dis 2001; 32:204–13

Three Fluid Solutions for Resuscitation
in DSS
• Kaplan–Meier Curves for Time from Study Entry to Initial (Panel A) and Sustained (Panel B) Cardiovascular Stability among Children in Group 1, According to the Resuscitation Fluid Received.
N Engl J Med 2005; 353;9

Prophylaxis platelet transfusion in
Dengue Fever
• Platelet count, < 20 X 103 /uL
Clin Infect Dis 2009; 48:1262–5
Patients given
platelet transfusion
(n = 188)
Patients not given
platelet transfusion
(n = 68)
P
Age, years 40 (22–64) 39 (22–58) .54
Any bleeding 1 (1) 2 (3) .17
Platelet increment the
next day, x 103
platelets/mL
7(-7 to 50) 11 (-4 to 41) .26
Time to platelet count
≥50 x 103 platelets/mL,
days
3 (1–4) 3 (1–5) .59
Length of hospital stay,
days
6 (4–8) 5 (4–7) .09
Death 1 (1) 0 (0) 1.00
Preventive transfusion in dengue shock
syndrome
• Significant differences in the development of pulmonary
edema and length of hospitalization (P<.05) (in
preventive transfusions group) were observed.
• Preventive transfusions did not produce sustained
improvements in the coagulation status in DSS
J Pediatr. 2003 Nov; 143(5):682-4.

Platelet Transfusion in Dengue Fever
• Acute lung injury after platelet transfusion in a
patient with dengue fever
Asian J Transfus Sci. 2014 Jul-Dec; 8(2): 131–134

Platelet Transfusion in Dengue Fever
• Prophylactic platelet transfusions are not required in
stable patients with platelet count below 20,000/μl.
J Indian Med Assoc. 2011 Jan; 109(1):30-5.
Blood component Indication
Platelet 1. In general there is no need to give prophylactic
platelets even at 20,000/μl.
2. Prophylactic platelet transfusion may be given at
level of <10,000/μl in absence of bleeding
manifestations.
3. Prolonged shock; with coagulopathy.
4. In case of massive bleeding, platelet transfusion
may be needed in addition to red cell transfusion.

Oral Corticosteroid
Therapy in Dengue Infection
• Randomized, Double-Blind Placebo Controlled Trial
Clin Infect Dis 2012;55(9):1216–24

Balapiravir therapy in Dengue
Infection
• Randomized, Double-Blind Placebo Controlled Trial
J Infect Dis 2013;207:1442–50
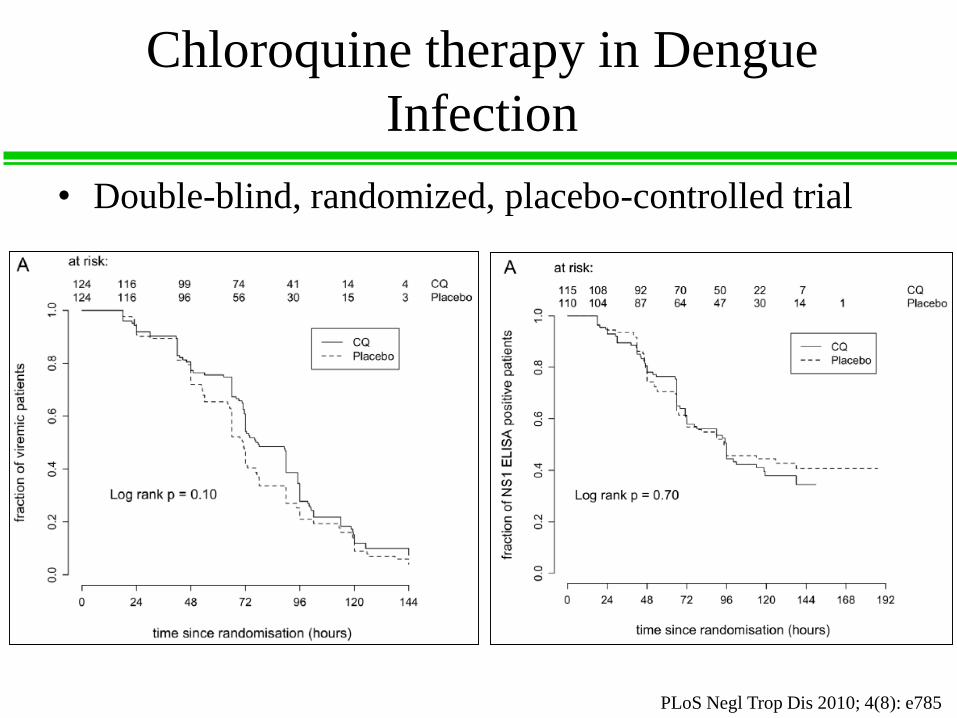
Chloroquine therapy in Dengue
Infection
• Double-blind, randomized, placebo-controlled trial
PLoS Negl Trop Dis 2010; 4(8): e785

Clinical manifestations and risk factors
for severe dengue

Global dengue burden
Source: From Global Strategy for Dengue Prevention and Control, 2012-2020
全球約25億人口生活在登革熱流行地區,每年發生約5000萬-2億登革熱病例,50萬人住院治療,2.5萬人死亡。

1997 WHO clinical classification of dengue
Dengue virus infection
Asymptomatic Symptomatic
Undifferentiated
fever
Dengue fever
syndromeDengue
hemorrhagic fever
Without
hemorrhage
With unusual
hemorrhage
Without
shock
Dengue shock
syndrome

1997 WHO clinical classification of dengue
Dengue
hemorrhagic
fever
Grade
Fever Tourniquet test Increased vascular
permeability
Thrombocytopenia
(<100 000×106
cells/l)
I
Hemorrhagic
manifestations
Rising hematocrit;
hypoproteinemia;
effusion
II
Hypovolemia,
weak pulse,
hypotension
Coagulopathy III (Dengue
shock syndrome)
Severe
bleeding
Profound shock Disseminated
intravascular
coagulopathy
IV (Dengue
shock syndrome)
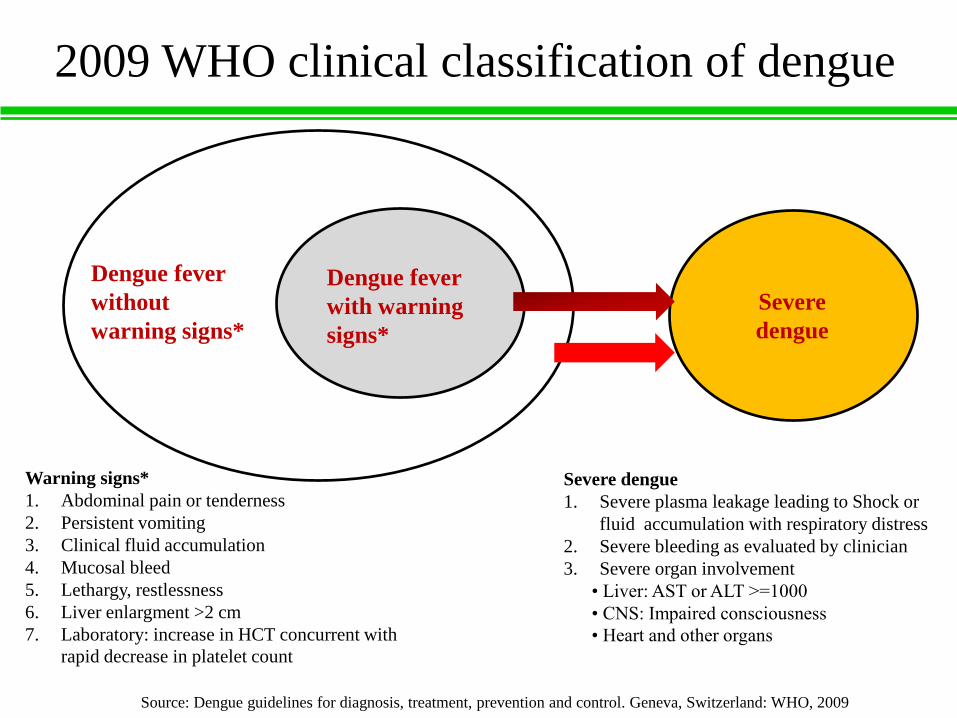
2009 WHO clinical classification of dengue
Severe
dengue
Dengue fever
with warning
signs*
Dengue fever
without
warning signs*
Severe dengue
1. Severe plasma leakage leading to Shock or
fluid accumulation with respiratory distress
2. Severe bleeding as evaluated by clinician
3. Severe organ involvement
• Liver: AST or ALT >=1000
• CNS: Impaired consciousness
• Heart and other organs
Warning signs*
1. Abdominal pain or tenderness
2. Persistent vomiting
3. Clinical fluid accumulation
4. Mucosal bleed
5. Lethargy, restlessness
6. Liver enlargment >2 cm
7. Laboratory: increase in HCT concurrent with
rapid decrease in platelet count
Source: Dengue guidelines for diagnosis, treatment, prevention and control. Geneva, Switzerland: WHO, 2009

台灣登革熱疫情(1998-20150906)
Source: Taiwan CDC

Rash
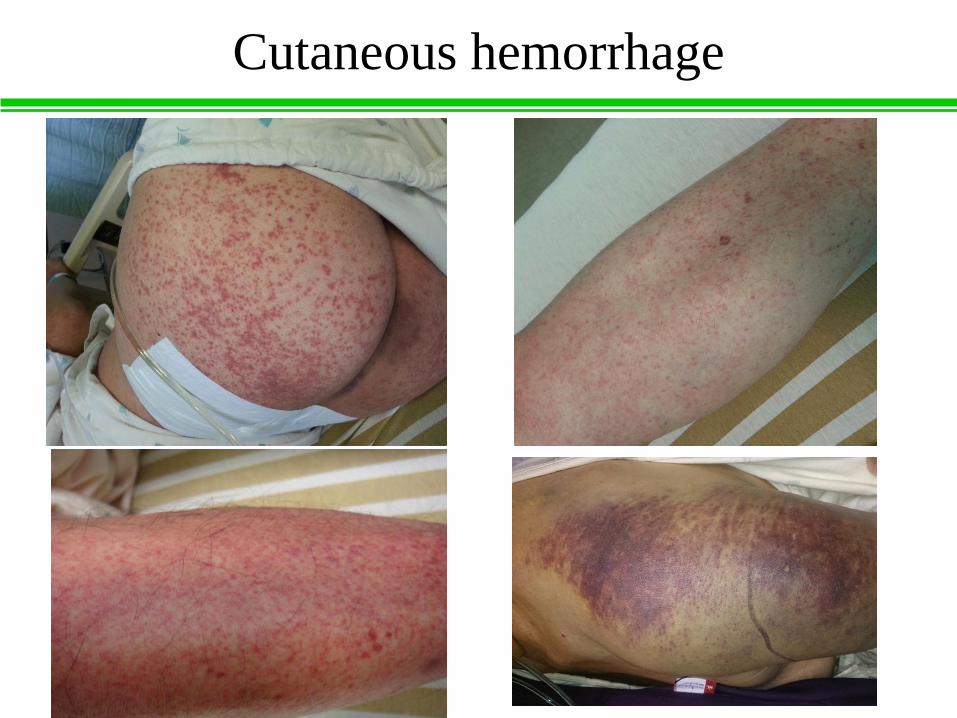
Cutaneous hemorrhage

Retinal hemorrhage

Gastrointestinal bleeding

Pleural effusion

Pulmonary congestion and acute
respiratory distress syndrome

Gallbladder swelling

Ascites

Acute abdomen in dengue
Acute abdomen
Acute cholecystitis
Non-specific peritonitis
Acute appendicitis
N=10
Am J Trop Med Hyg 2006; 74: 901
N= 3
N=1
The importance of differential diagnosis in patients with acute abdomen in a dengue-
endemic setting.

Hyperlipasemia and acute pancreatitis in
DHF
• Hyperlipasemia developed in 14 patients with DHF
• Pancreatitis was diagnosed in 3 patients
Pancreas 2007; 35: 381
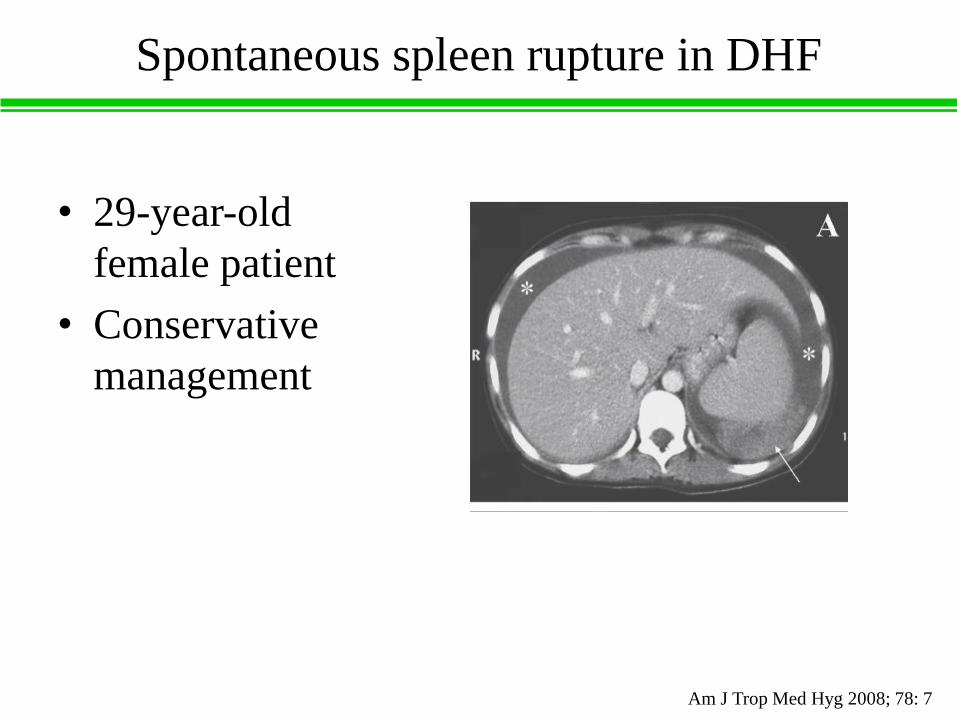
Spontaneous spleen rupture in DHF
• 29-year-old
female patient
• Conservative
management
Am J Trop Med Hyg 2008; 78: 7

Myocarditis in dengue
Int J Infect Dis. 2010 Oct;14(10):e919-22

Rhabdomyolysis in dengue
Am J Trop Med Hyg. 2015 Jan;92(1):75-81

Hemophagocytic Lymphohistiocytosis
MMWR / January 24, 2014 / Vol. 63 / No. 3

Acute transverse myelitis in dengue
J Clin Virol 2006; 35; 312

Concurrent bacteremia in dengue
Am J Trop Med Hyg 2005; 72: 221
Bacteria isolated
Klebsiella pneumoniae
Rosemonas spp.
Klebsiella ozaenae
Enterococcus faecalis
Moraxella lacunata
N=1
N=3
Clinicians should be alert to the potential for concurrent bacteremia when treating
patients with DHF/DSS

Case presentation
• 71-year-old woman
• Underlying: Senile dementia, hypertension, chronic
anemia
• Fever and malaise for 5 days
• She was evaluated by her family physician and was
prescribed some medication for a diagnosis of common
cold
• Gum bleeding and gross hematuria were found one
day before presentation at our emergency room

Case presentation
• On examination, the patient appeared clear
consciousness. She was febrile with a temperature of
38°C, pulse rate 100 beats/min, and blood pressure
126/66 mm Hg
• Laboratory data showed leukopenia and
thrombocytopenia
• She living in dengue endemic area; and dengue virus
infection was confirmed by serology test

Case presentation
Day 1 at ER
(day 7 after
illness onset)
Day 2 at ER
(day 8 after
illness onset)
Day 3 at ER
(day 9 after
illness onset)
White blood cell (×109 cells/L) 1.0 1.3 2.1
Hemoglobin g/dL 12.6 12.3 9.8
Hematocrit (%) 36.9 36.6 28.6
Platelet (×109 cells/L) 38 44 42
Creatinine mg/dL 0.71
GOT U/L 263
Platelet
transfusion
24 units
Platelet
transfusion
12 units
Admitted to
ward at night
time
Intravenous fluid: N/S run 60cc/h
(29%)
No more gum bleeding and hematuria
Haemodilution
Dengue fever with warning signs

Case presentation
Day 10 after
illness onset
Day 11 after
illness onset
Day 12 after
illness onset
White blood cell (×109 cells/L) 3.1 4.0 4.0
Hemoglobin g/dL 10.2 10.8 10.5
Hematocrit (%) 30.3 31.1 29.8
Platelet (×109 cells/L) 34 53 70
- The patient became drowsy on the next day after admission (day 10 after illness
onset). On examination she was unconsciousness with cold and clammy
peripheries. Her blood pressure was 60/40 mmHg and with a heart rate of
95/minute. Immediately rapid saline intravenously infusion 1000cc (within 30
minute). Her blood pressure was 110/80 after fluid replacement. Additional fluid
was given 500cc within 1 hour.
- Maintenance intravenous fluid of 60cc/h and monitor hematocrit, platelet count
and I/O.
- Improvement of patient’s consciousness. Reduced intravenous fluid on day 2
after shock.

Case presentation
• Pleural effusion,
ascites and
gallbladder swelling

Case presentation
• Day from onset illness to shock: 10th day
• Plasma leak: pleural effusion, ascites, hemoconcentration
• Critical phase: between 7th and 11th day after onset illness
• Warning signs: mucosal bleeding (gum bleeding, hematuria),
increase hematocrit concurrent decrease platelet count, drowsy
(onset to shock: hours)
Day 7 after
illness onset
Day 17 after
illness onset
White blood cell (×109 cells/L) 1.0 3.0
Hemoglobin g/dL 12.6 9.0
Hematocrit (%) 36.9 26.6
Platelet (×109 cells/L) 38 145
Day
discharge
from
hospital
Hemoconcentration
(39%)

Risk for severe dengue
1. Strain virulence
2. Serotype
Viral
factors
Epidemiological
risk factors
Individual
risk factors
1. Number of
susceptible
2. Vector high
density
3. Wide viral
circulation
4. Hyperendemicity
1. Age
2. Sex
3. Race
4. Nutritional
status
5. Secondary
infection
6. Host
response
Lancet Infectious Disease 2001: 2: 33
Antibody-Dependent
Enhancement
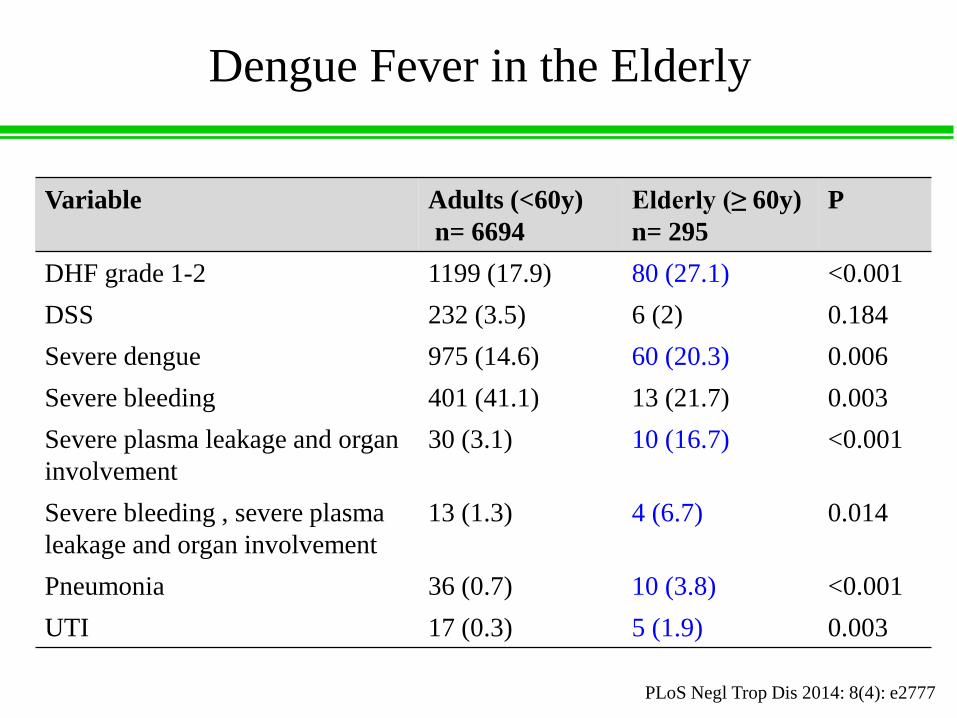
Dengue Fever in the Elderly
Variable Adults (<60y)
n= 6694
Elderly (≥ 60y)
n= 295
P
DHF grade 1-2 1199 (17.9) 80 (27.1) <0.001
DSS 232 (3.5) 6 (2) 0.184
Severe dengue 975 (14.6) 60 (20.3) 0.006
Severe bleeding 401 (41.1) 13 (21.7) 0.003
Severe plasma leakage and organ
involvement
30 (3.1) 10 (16.7) <0.001
Severe bleeding , severe plasma
leakage and organ involvement
13 (1.3) 4 (6.7) 0.014
Pneumonia 36 (0.7) 10 (3.8) <0.001
UTI 17 (0.3) 5 (1.9) 0.003
PLoS Negl Trop Dis 2014: 8(4): e2777

DHF in the Elderly (KSCGMH)
Variable Elderly (≥ 65 years)
(N=66)
Non-elderly (19–64
years) (N=241)
P
Fever, n (%) 60 (90.9) 239 (99.2) 0.002
Bone pain, n (%) 24 (36.4) 147 (61) < 0.001
Acute renal failure, n (%) 8 (12.1) 4 (1.7) 0.001
Concurrent bacteremia, n/N
(%)
4/23 (17.4) 2/59 (3.4) 0.049
Pleural effusion (bilateral or
unilateral), n/N (%)
26/46 (56.5) 60/173 (34.7) 0.010
Gastrointestinal bleeding, n
(%)
21 (32) 47 (19.5) 0.044
Length of hospital stay (day;
mean ± SD)
7.9 ± 4.9 6.3 ± 2.9 0.049
Fatality (%) 5 (7.6) 2 (0.8) 0.006
Am J Trop Med Hyg 2008;79:149
Atypical and more complicated clinical presentation in elderly patients with dengue

In vitro Diabetes’ Mononuclear Cells
Infected with Dengue Virus
Biomed Res Int. 2013;2013:965853
Third post-infection day in an in vitro infection model.
Our result suggest that patients with T2DM are at higher risk for development of
DHF/severe dengue

Diabetes: Risk Factor for Severe
dengue
PLoS Negl Trop Dis 2015; 9(4): e0003741

Warning signs associated with disease
progression
Trop Med Int Health. 2011 Aug;16(8):936-48.
These warning signs were derived in part from a dataset describing 1587 patients
with dengue across Asia and Latin America. Only a small number of subjects (5%)
progressed to severe disease while under observation; several warning signs were
identified.

Warning signs before severe dengue (n=65)
in adult dengue
• 1. Abdominal pain
• 2. Persistent vomiting
• 3. Hepatomegaly
• 4. Hematocrit rise and
rapid platelet count drop
• 5. Clinical fluid
accumulation
• 6. Mucosal bleeding
• 7. Lethargy
(%)
PLoS Negl Trop Dis 2013; 7(1): e2023.
0
5
10
15
20
25
30
1 2 3 4 5 6 7
15
8
03 2
10
26
Before severe dengue (n=65)
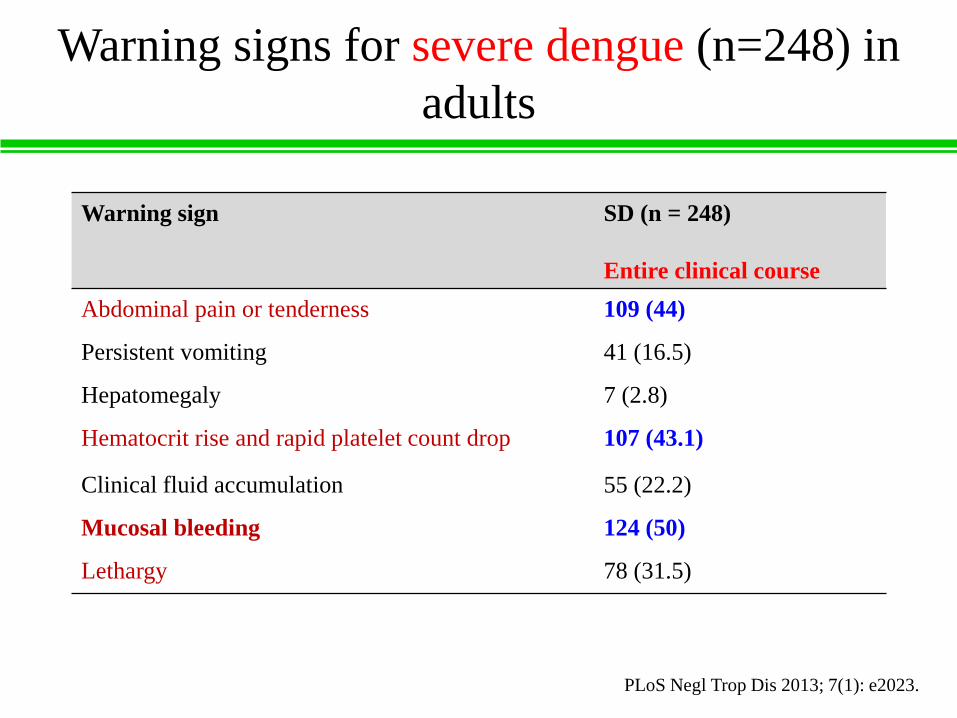
Warning signs for severe dengue (n=248) in
adults
Warning sign SD (n = 248)
Entire clinical course
Abdominal pain or tenderness 109 (44)
Persistent vomiting 41 (16.5)
Hepatomegaly 7 (2.8)
Hematocrit rise and rapid platelet count drop 107 (43.1)
Clinical fluid accumulation 55 (22.2)
Mucosal bleeding 124 (50)
Lethargy 78 (31.5)
PLoS Negl Trop Dis 2013; 7(1): e2023.

Warning signs for predicting severe dengue
in adult dengue
Warning signs Sn Sp PPV NPV
Abdominal pain or tenderness 0.21 0.72 0.09 0.87
Persistent vomiting 0.08 0.93 0.18 0.85
Hepatomegaly 0.00 0.99 0.06 0.84
Hematocrit rise and rapid platelet
count drop
0.05 0.94 0.09 0.89
Clinical fluid accumulation 0.02 0.98 0.16 0.87
Mucosal bleeding 0.17 0.82 0.10 0.89
Lethargy 0.34 0.56 0.17 0.76
PLoS Negl Trop Dis 2013; 7(1): e2023.
Sn = sensitivity, Sp = specificity, PPV = positive predictive value, NPV = negative
predictive value

Onset of warning signs to DHF and severe
dengue in adult dengue
Warning signs Days to severe
dengue
Abdominal pain or tenderness 2 (8–2)
Persistent vomiting 2 (1–5.7)
Hepatomegaly 1.5 (1–2)
Hematocrit rise and rapid platelet count drop 3 (1–7.6)
Clinical fluid accumulation 3 (1–8)
Mucosal bleeding 2 (1–8.5)
Lethargy 3 (1–8)
Warning signs occurred at median of two days before severe dengue
PLoS Negl Trop Dis 2013; 7(1): e2023.
Dengue shock
syndrome in 1719 Vietnamese children
• Shock occurred commonly between days 4 and 6 of illness.
• Warning signs (at the onset of shock):
lethargy (1490/1719 [87%]);
vomiting (1199/1713 [70%]);
abdominal pain (932/1709 [55%]);
liver enlargement (1478/1696 [87%])
• Two-third had bleeding; 31 (2%) patients developed severe bleeding, primarily from the gastrointestinal tract
• 8 patients died; the interval from admission to death was short (median, 34 hours [range, 11–87 hours])
Clin Infect Dis 2013;57(11):1577
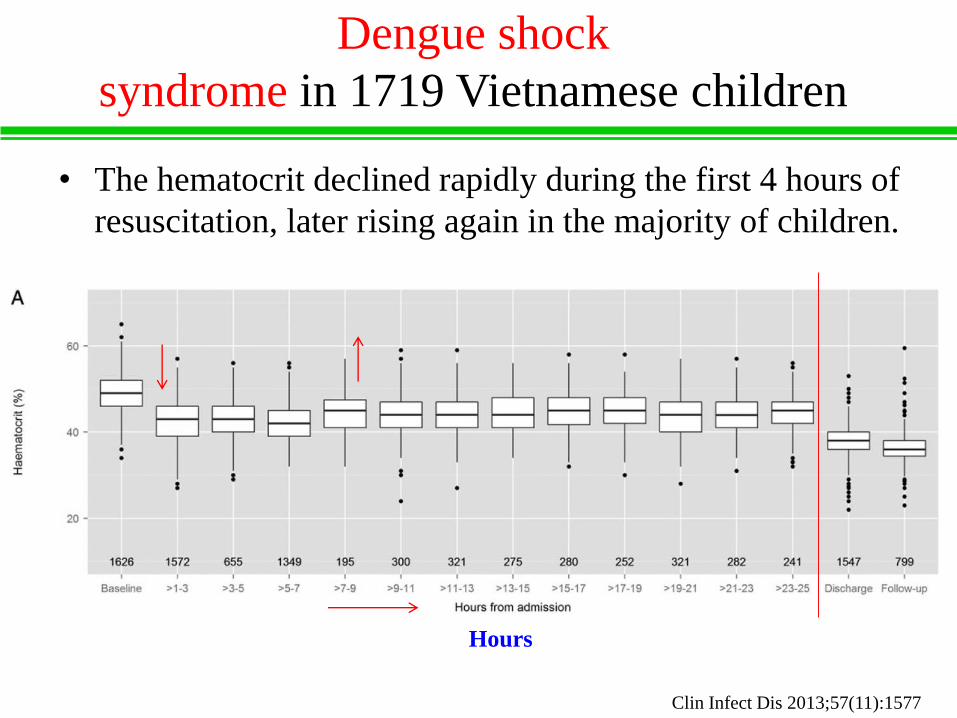
Dengue shock
syndrome in 1719 Vietnamese children
• The hematocrit declined rapidly during the first 4 hours of
resuscitation, later rising again in the majority of children.
Clin Infect Dis 2013;57(11):1577
Hours

Factors associated with dengue shock
syndrome: meta-analysis (all ages)
Variable Total sample size
(DSS/DHF)
P Odds ratio (95% CI)
Malnutrition 1689/3449 0.05 1.19 (1.00-1.41)
Neurological signs 859/1891 0.01 4.66 (1.70-12.8)
Vomiting/nausea 839/1891 0.01 1.43 (1.15-1.78)
Abdominal pain 2340/4986 <0.001 2.26 (1.76-2.89)
Gastrointestinal bleeding 786/1317 <0.001 1.84 (1.42-2.39)
Hemoconcentration 2847/5214 <0.001 2.61 (2.02-3.37)
Pleural effusion 1757/3860 <0.001 10.4 (5.47-19.6)
Ascites 373/763 <0.001 5.92 (5.42-14.5)
Hypoalbuminemia 1662/3461 <0.001 4.34 (2.51-7.52)
Hepatomegaly 4130/8906 <0.001 3.10 (2.18-4.41)
Thrombocytopenia (low platelet count) 2801/7172 <0.001 2.08 (1.39-3.12)
Prothrombin time 1661/3713 <0.001 2.83 (1.84-4.37)
PLoS Negl Trop Dis 2013; 7(9): e2412

Plasma Leakage in Dengue: daily Bedside
Ultrasonography (N=158)
Pediatr Infect Dis J 2007; 26: 283

C-Reactive Protein Levels for Early
Prediction
Median CRP (range)/no, mg/L
Phase of illness Non-severe dengue Severe dengue P
Febrile phase (days 1–3) 14.4 (0.6–69)/87 36.2 (3.3–205.5)/10 0.025
Critical phase (days 4–6) 8 (0.5–215.5)/81 29.2 (6.9–144)/4 0.053
Convalescent phase (days 7–10) 3.3 (1.6–10.7)/8 1.2 (—)/1 -
BioMed Research International 2015; 2015: 936062
In the febrile phase of illness, similarly, a CRP cutoff level of 24.2
mg/L (0.717 AUC) was obtained with 70% sensitivity and 71.3%
specificity for differentiating between non-severe dengue and severe
dengue.

Fatal DHF in adults (Malaysia): clinical
features
Variable Fatal (n=9)
Abdominal pain, N (%) 6 (67)
Vomiting/nausea, N (%) 9 (100)
Lethargy, N (%) 3 (33)
Liver enlargement, N (%) 3 (33)
Any bleeding, N (%) 8 (89)
GI bleeding, N (%) 5 (56)
Ascites, N (%) 5 (56)
Pleural effusion, N (%) 7 (78)
Hypoalbuminemia, n/ N (%) 7/7 (100)
Platelet < 50,000/uL, n/ N (%) 7/7 (100)
PLoS Negl Trop Dis 2013; 7(5): e2194.
2006-2007; 10 fatal cases (median age, 32 years)
The mean duration of illness prior to hospitalization was 4.7 days and
deaths occurred at an average of 2.4 days post-admission.

Fatal DHF in adults (Malaysia): cause of
death
Cause of death No.
DHF 1
DSS 1
DSS with severe GI bleeding and acute renal failure 1
DSS with severe GI bleeding and multi-organ failure 3
DSS with severe GI bleeding 1
DSS with myocarditis and cardiogenic shock 1
DSS with pulmonary edema and sepsis 1
PLoS Negl Trop Dis 2013; 7(5): e2194.

Fatal DHF in adults (Singapore): cause of
death
• 2004; 7 fatal cases
International Journal of Infectious Diseases (2007) 11, 263
Cause of death
Gastrointestinal bleeding; ketoacidosis (DM); multi-organ failure
Myocarditis with cardiogenic shock; ARDS
Gram-negative septicemia; myocarditis with cardiogenic shock; ARDS
Gastrointestinal bleeding; septicemia; multi-organ failure; ARDS
Disseminated intravascular coagulopathy; multi-organ failure
Severe bilateral pneumonia; disseminated intravascular coagulopathy; multi-
organ failure
Acute renal failure; septicemia; ARDS
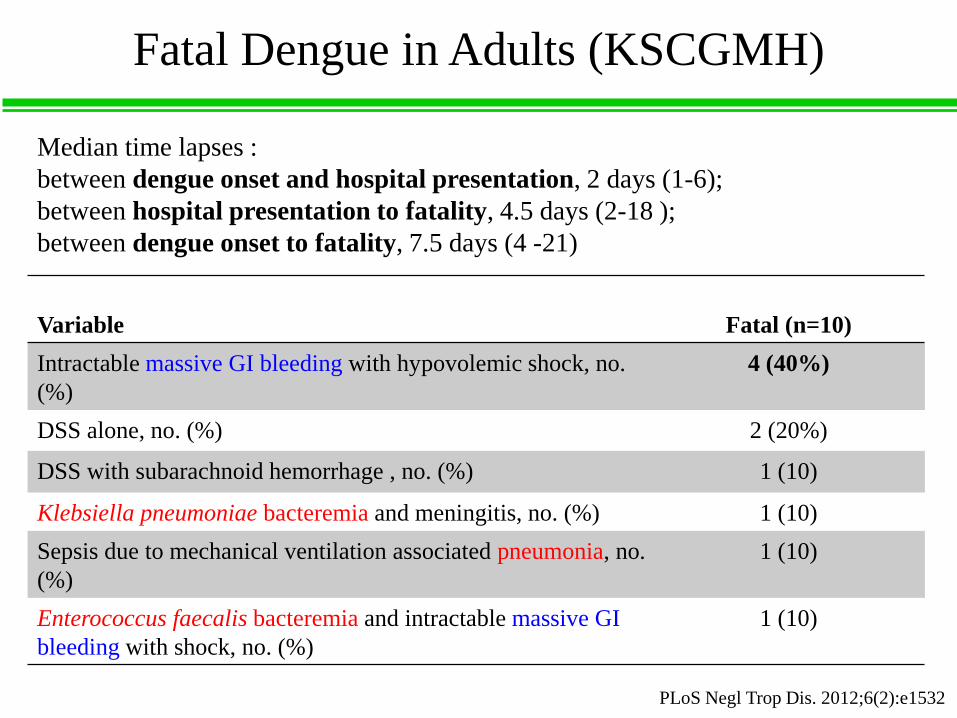
Fatal Dengue in Adults (KSCGMH)
Variable Fatal (n=10)
Intractable massive GI bleeding with hypovolemic shock, no.
(%)
4 (40%)
DSS alone, no. (%) 2 (20%)
DSS with subarachnoid hemorrhage , no. (%) 1 (10)
Klebsiella pneumoniae bacteremia and meningitis, no. (%) 1 (10)
Sepsis due to mechanical ventilation associated pneumonia, no.
(%)
1 (10)
Enterococcus faecalis bacteremia and intractable massive GI
bleeding with shock, no. (%)
1 (10)
PLoS Negl Trop Dis. 2012;6(2):e1532
Median time lapses :
between dengue onset and hospital presentation, 2 days (1-6);
between hospital presentation to fatality, 4.5 days (2-18 );
between dengue onset to fatality, 7.5 days (4 -21)

Fatal Dengue in Adults (KSCGMH)
Variable
Initial
laboratory data
(fatal group)
(A)
Initial
laboratory data
(non-fatal group)
(B)
Pre-fatal
laboratory data
(48h before
fatality)
(fatal group)
(C)
P
(A vs. B)
P
(C vs. A)
Leukocytosis
(WBC>12000/mL),
n/N (%)
1/10 (10) 4/293 (1.4) 6/9 (66.7) NS 0.020
Bandemia, n/N (%) 3/8 (37.5) 5/277 (1.8) 4/6 (66.7) 0.001 NS
Median platelet
count (mL) (range)
35000 (3000–
157000)
(N = 10)
93000 (1000–
303000)
(N = 299)
17000 (9000–
108000)
(N = 10)
NS <0.001
PLoS Negl Trop Dis. 2012;6(2):e1532

Detection of DENV antigens in tissue
SpleenKidney
HeartLung
Liver

Pathology of fatal dengue (Brazil)
Liver sections of dengue cases,
stained with HE, showing hepatic
injuries, edema (E) and
hemorrhage (He) near central vein
(CV).
PLoS ONE 2014; 9(4): e83386
Lung sections of dengue cases, stained with HE, showing
pulmonary alterations, including septal thickening (St), edema
(E), hemorrhage (He), presence of mononuclear infiltrate (Inf),
hyaline membrane formation (HM) and hypertrophy of alveolar
macrophages (AM) and type II pneumocytes (PcyII)

Pathology of fatal dengue
Heart sections of dengue
cases, stained with HE,
showing hemorrhage (He),
edema (E), presence of
mononuclear infiltrate (Inf)
and degeneration of muscle
fibers (black star).
Kidney sections of dengue
cases, stained with HE,
showing hemorrhage (He),
and edema (E)
PLoS ONE 2014; 9(4): e83386
Spleen sections of dengue
cases, stained with HE,
showing edema (E)

Severe dengue in adults
(KSCGMH preliminary data)
• Period: 2002 ~ 2014–07

Dengue cases (n=1063)
Age group
No. pat
ient
0
50
100
150
200
250
300
350
18-39 40-49 50-59 60-69 >70
Non-severe dengue
Severe dengue
Incidence of severe dengue:
Age, 18-59 yr (2%) vs. ≥ 60 yr (15%); P<0.001
Based on 2009
WHO dengue
classification
scheme.
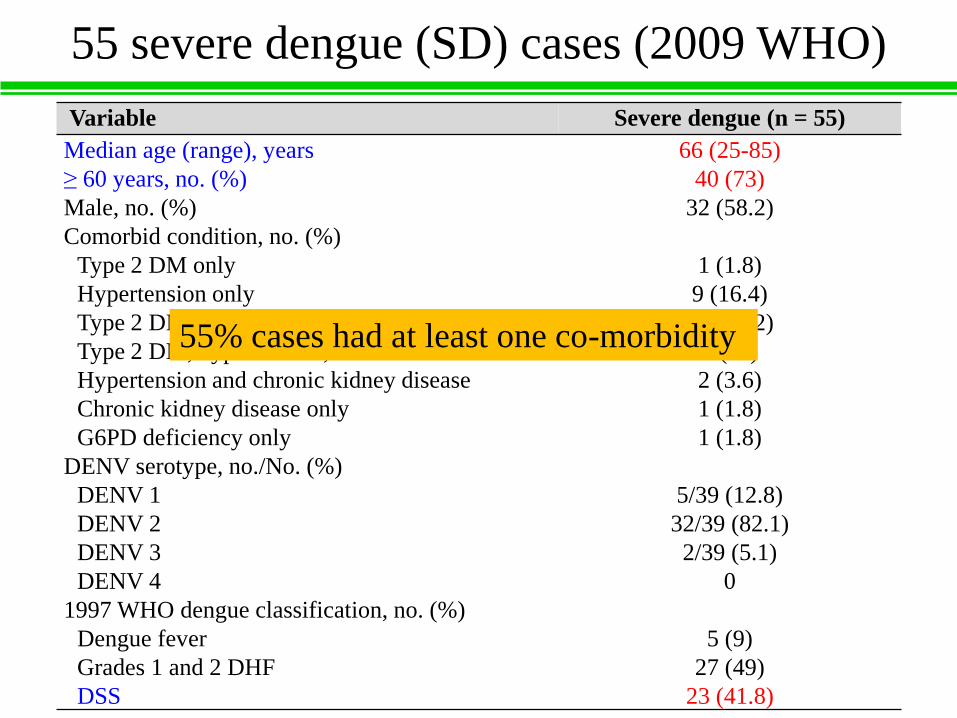
55 severe dengue (SD) cases (2009 WHO)
Variable Severe dengue (n = 55)
Median age (range), years 66 (25-85)
≥ 60 years, no. (%) 40 (73)
Male, no. (%) 32 (58.2)
Comorbid condition, no. (%)
Type 2 DM only 1 (1.8)
Hypertension only 9 (16.4)
Type 2 DM and hypertension 10 (18.2)
Type 2 DM, hypertension, and others 6 (11)
Hypertension and chronic kidney disease 2 (3.6)
Chronic kidney disease only 1 (1.8)
G6PD deficiency only 1 (1.8)
DENV serotype, no./No. (%)
DENV 1 5/39 (12.8)
DENV 2 32/39 (82.1)
DENV 3 2/39 (5.1)
DENV 4 0
1997 WHO dengue classification, no. (%)
Dengue fever 5 (9)
Grades 1 and 2 DHF 27 (49)
DSS 23 (41.8)
55% cases had at least one co-morbidity

55 SD cases (2009 WHO)
Variable Severe dengue
Median time from illness onset to hospital presentation
(range), days (n = 55)
3 (1-7)
Median time from illness onset to severe dengue (range),
days (n = 55)
5 (2-10)
Median time from illness onset to shock (range), days (no.)
(n = 23)
6 (2-10)
Median time from hospital presentation to severe dengue
(range), days (n = 55)
1 (1-5)
Median time from hospital presentation to shock (range),
days (no.) (n = 23)
1 (1-5)

Severe dengue in KSCGMH
Variable Severe dengue
(n=55)
Non-severe
dengue (n=1008)
P
Mean age (±SD), yrs 63 (13.4) 48.7 (15.5) <0.001
Male, no. (%) 32 (58.2) 464 (46) 0.095
Comorbid condition, no. (%)
Type 2 DM only 1 (1.8) 53 (5.3) 0.520
HTN only 19 (16.4) 110 (11) >0.99
Type 2 DM with HTN 16 (29) 75 (7.4) >0.99
Type 2 DM with HTN and others 6 (11) 16 (1.6) >0.99
G6PD only 1 (1.8) 1 (0.1) >0.99
Dengue virus serotype, no./No. (%)
DENV 1 1/39 (2.6) 12/699 -
DENV 2 32/39 (82.1) 607/699 -
DENV 3 2/39 (5.1) 79/699 -
DENV 4 0 1/699 -
1997 dengue classification, no. (%)
Dengue fever 5 (9) 909 -
DHF, grades 1-2 27 (49) 99 -
DSS 23 (41.8) 0 -
Mean day from onset illness to hospital
presentation (±SD)
3.8 (1.9) 3.7 (2.2) 0.427
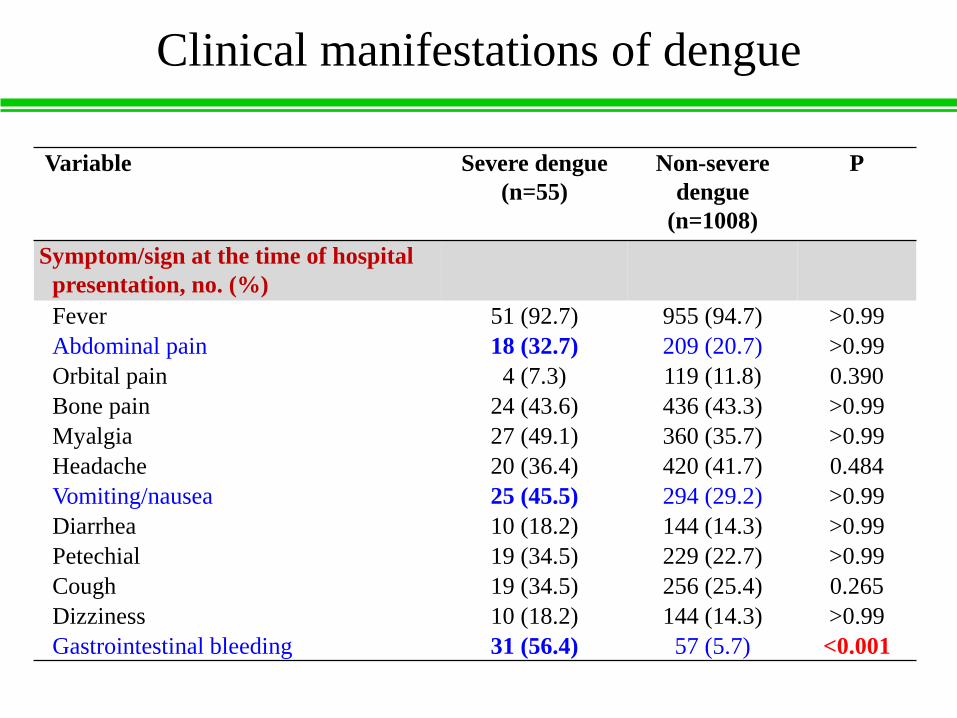
Clinical manifestations of dengue
Variable Severe dengue
(n=55)
Non-severe
dengue
(n=1008)
P
Symptom/sign at the time of hospital
presentation, no. (%)
Fever 51 (92.7) 955 (94.7) >0.99
Abdominal pain 18 (32.7) 209 (20.7) >0.99
Orbital pain 4 (7.3) 119 (11.8) 0.390
Bone pain 24 (43.6) 436 (43.3) >0.99
Myalgia 27 (49.1) 360 (35.7) >0.99
Headache 20 (36.4) 420 (41.7) 0.484
Vomiting/nausea 25 (45.5) 294 (29.2) >0.99
Diarrhea 10 (18.2) 144 (14.3) >0.99
Petechial 19 (34.5) 229 (22.7) >0.99
Cough 19 (34.5) 256 (25.4) 0.265
Dizziness 10 (18.2) 144 (14.3) >0.99
Gastrointestinal bleeding 31 (56.4) 57 (5.7) <0.001

Laboratory features of dengue
Variable
Severe dengue
(n =55)
Non-severe dengue
(n=1008)
P
Data during the
entire clinical
course
Data at the time of
hospital
presentation
Data at the time of
hospital
presentation
Leukopenia (WBC <3.0 × 109
cells/L), no./ total no. (%)
15/55 (27.3) 6/55 (10.9) 333/977 (34) <0.001
Leukocytosis (WBC >10 ×109 cells/L), no./ total no. (%)
15/55 (27.3) 10/55 (18.2) 3/977 (0.3) <0.001
Mean hematocrit, % (± SD)
(no.)
38.6 (7.4)
(n=55)
36.1 (7.6)
(n=55)
39.3 (5.6)
(n=975)
<0.001
Mean platelet count (± SD)
(× 109 cells/L) (no.)
23.8 (25.3)
(n=55)
56.8 (56.5)
(n=55)
102 (62.1)
(n=984)
<0.001
Severity of thrombocytopenia
Platelet count >150 × 109
cells/L, no./total no. (%)
1/55 (1.8) 7/55 (12.7) 203/984 (20.6) 1
Platelet count 100-149 ×109 cells/L, no./total no. (%)
0 3/55 (5.5) 297/984 (30.2) 0.078
Platelet count 50-99 × 109
cells/L, no./total no. (%)
5/55 (9.1) 13/55 (23.6) 261/984 (26.5) 0.442
Platelet count <50 × 109
cells/L, no./total no. (%)
49/55 (89.1) 32/55 (58.2) 223/984 (22.7) 0.001

Laboratory features according to day
onset of illness
SD Day
1-2
(n=14)
Non-SD
Day 1-2
(n=221)
SD Day
3-4
(n=22)
Non-SD
Day 3-4
(n=347)
SD Day
5-7
(n=18)
Non-SD
Day 5-7
(n=376)
Maxi 10.3 10 17.3 19.1 12 17.4
Mini 1.8 1.3 1.8 0.6 1 0.7
Median 4.5 4.2 5.45 3.7 5.95 3.5
0
5
10
15
20
25
White blood cell count
10
9ce
lls/
L
P<0.001P<0.001
P=0.573

Laboratory features according to day
onset of illness
SD Day
1-2
(n=14)
Non-SD
Day 1-2
(n=219)
SD Day
3-4
(n=22)
Non-SD
Day 3-4
(n=347)
SD Day
5-7
(n=17)
Non-SD
Day 5-7
(n=372)
Maxi 45.1 49.6 50.4 51 49.9 57.2
Mini 21.9 21.4 24.7 27.8 22.3 23.7
Median 32.9 39.3 38.1 39 36.9 39.8
0
10
20
30
40
50
60
70
Hematocrit
%
P <0.001 P=0.266 P=0.040

Laboratory features according to day
onset of illness
SD Day
1-2
(n=14)
Non-SD
Day 1-2
(n=221)
SD Day
3-4
(n=23)
Non-SD
Day 3-4
(n=351)
SD Day
5-7
(n=18)
Non-SD
Day 5-7
(n=379)
Maxi 170 374 190 413.3 191 344
Mini 29 3 1.5 2 3 1
Median 96.5 118 24 102 22 87
0
50
100
150
200
250
300
350
400
450
Platelet count
10
9ce
lls/
L
P=0.260 P<0.001 P<0.001

Severe dengue in KSCGMH
Severe
dengue
n =55
Non-severe
dengue
n = 973
Odds
ratio 95% CI P
Mean age (±SD), yrs 63 (13.4) 48.9 (15.5) 1.071 1.041-1.102 <0.001
Gastrointestinal bleeding,
no. (%)
31 (56.4) 56 (5.7) 12.811 6.549-25.061 <0.001
Leukocytosis (WBC >10
× 109 cells/L), no. (%)
10 (18.2) 3 (0.3) 33.329 4.464-248.838 0.001
Thrombocytopenia <50 ×109 cells/L, no. (%)
32 (58.2) 216 (22.1) 2.181 1.123-4.236 0.021

Parameters
Phase of illness: day 4-7
Host factor
1. Age: Infant (< 1 y/o) and elderly (> 60 y/o)
2. Pregnant
3. Diabetes mellitus
4. Chronic kidney disease
Warning signs
1. Abdominal pain
2. Persistent vomiting
3. Fluid accumulation
4. Mucosal bleeding (gastrointestinal bleeding)
Evaluation of hemodynamic status: BP CCTV-R
Laboratory data
1. Increase hematocrit concurrent drop platelet count
2. WBC (leukocytosis) and CRP (> 30 mg/L)

Thanks