
Environmental Strategic Management Untuk Kawasan Industri ...
1
SEMBRAMKY ENVIRONMENTAL MANAGEMENT PVT LTD
Detailed Project Report with Specifications
For Development of Integrated Bio-Medical Waste
Management Facility in Patna & Surrounding areas.
Submitted to
Submitted By
SembRamky Environmental Management Pvt Ltd
304-307, Pankaj Arcade-3, Plot No-6, Pocket-4
Sector-11, Dwarka, New Delhi-110075
Tel: +91- 11 – 42770304, 42770305, Fax: 91-11-42770304
Email: [email protected]

SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
2
Chapter 1
1.0 Introduction
The rapid increase in population can be attributed to the industrial, commercial and location of
the city, which has opened vast employment to the nearby towns and villages. Rapid growth in
population, severe environmental degradation and increased awareness about the health care has
created a need for a wide variety of medical facilities.
In the service of a huge population, these hospitals are generating “Bio-Medical Wastes” that are
incompatible with the environment. These wastes need professional attention for effective
management as the infectious nature of the waste can cause irreparable damage to the human
health and the environment. It has become imperative to monitor and control the management
and handling of these wastes.
The concern about disposal of infectious wastes generated by the hospitals is increasing rapidly
due to the fear of the spread of viruses such as Acquired Immune Deficiency Syndrome (AIDS)
and Hepatitis B. These wastes (bio-medical wastes generated from health care establishments)
present a high risk of causing potential damage to the human health and the environment by way
of spreading. To prevent the spread of such infectious wastes that finds its genesis in bio-
medical wastes (from hospitals, clinics, laboratories, dispensaries etc.) a scientific approach is
required. From the beginning it is essential that professionally trained personnel should handle
the wastes.
To enable effective management and handling of the bio-medical wastes the Ministry of
Environment and Forests (MoEF) has issued Rules for the management and handling of these
wastes vis-à-vis Bio-Medical Wastes (Management and Handling) Rules 1998, under the aegis
of Environment (Protection) Act, 1986. In response of which, the Government and
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
3
Major Private Hospitals have made their own arrangements for treatment and disposal of bio-
medical wastes, however, the smaller nursing homes, clinics and other similar institutions which
do not have or can afford such facilities need alternate modalities and arrangements to dispose
their wastes, in accordance with the Rules.
Keeping in view the difficulties faced by private Hospitals, Nursing Homes and Clinics that
cannot make their own arrangements due to high cost involved in Treatment facilities, there was
need for centralized system for treatment. Later on, in September 2003, the Central Pollution
Control Board had made the guidelines for “Common bio-Medical Waste Treatment Facility” in
order to discourage the individual incineration facility by health care establishments and
strengthening CBWTF system.
To redress this problem and provide the health care establishments with a solution to their waste
disposal dilemma, SembRamky Environmental Management Pvt.Ltd has taken initiative and set
up and is operating 9 Common Treatment Facility in different cities of India
In need of professional attention for effective management to contain costs on the one hand and
enhance efficiencies on the other, M/S SembRamky Environmental Management Pvt. Ltd is
proposing Expression of Interest for Development of Integrated Bio-Medical Waste Management
Facilities for waste generated in Patna and other adjoining areas of Patna falling under the radius
of 150 K.M.

SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
4
A View of our Incinerator at Howrah
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
5
Chapter 2
2.0 Waste Quantities and Characteristics
2.1 Introduction
The primary purpose of waste quantification and characterization is to provide for an
economically viable option for treatment/ disposal of the wastes. This concept, if managed
properly reduces the quantity of infectious wastes to be handled under the Bio-Medical Waste
management rules and also enables for an efficient sorting/ segregation and collection into colour
coded bags/ containers.
2.2 Waste Classification and Characterization
Wastes generated by the hospitals can primarily be classified into 3 groups:
Conventional Wastes/ Municipal Solid Wastes: General refuse similar to the domestic/
municipal solid wastes and includes artificial linens, paper, food, cans, diapers, and plastic
cups. This waste is non-infectious if it is not brought in contact with the infectious wastes
and properly managed.
Hazardous Wastes: Laboratory and Pharmaceutical Chemicals and containers including off-
specification and other chemicals, alcohols, disinfectants, anti-neoplastic agents, heavy
metals (e.g. Mercury), etc. These wastes are hazardous in nature and if properly segregated
and managed can be transported to hazardous waste management facility for treatment/
storage/ disposal.
Infectious Wastes: Commonly referred to as Clinical and pathological Wastes and include:
isolation wastes (refuse associated with infectious patients), cultures and stocks of infectious
agents and associated biological, human blood and blood products, pathological wastes,
contaminated sharps, amputated body parts, placenta and others.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
6
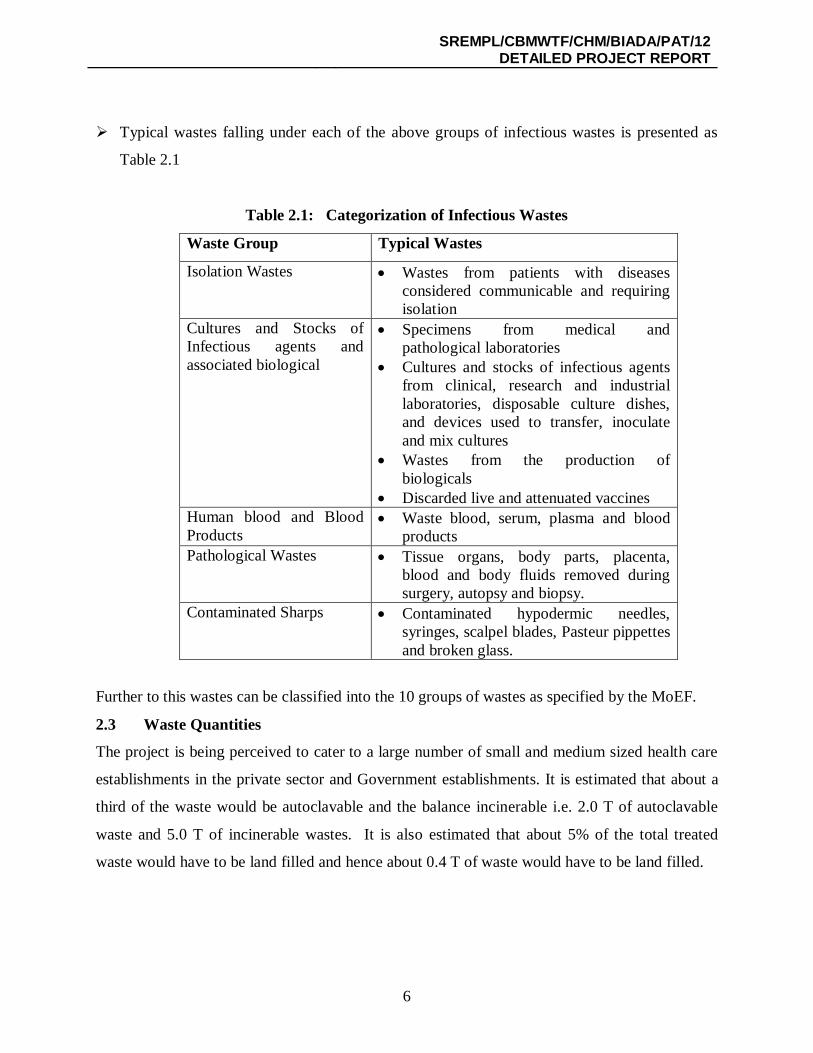
Typical wastes falling under each of the above groups of infectious wastes is presented as
Table 2.1
Table 2.1: Categorization of Infectious Wastes
Waste Group Typical Wastes
Isolation Wastes Wastes from patients with diseases considered communicable and requiring isolation
Cultures and Stocks of Infectious agents and associated biological
Specimens from medical and pathological laboratories
Cultures and stocks of infectious agents from clinical, research and industrial laboratories, disposable culture dishes, and devices used to transfer, inoculate and mix cultures
Wastes from the production of biologicals
Discarded live and attenuated vaccines Human blood and Blood Products
Waste blood, serum, plasma and blood products
Pathological Wastes Tissue organs, body parts, placenta, blood and body fluids removed during surgery, autopsy and biopsy.
Contaminated Sharps Contaminated hypodermic needles, syringes, scalpel blades, Pasteur pippettes and broken glass.
Further to this wastes can be classified into the 10 groups of wastes as specified by the MoEF.
2.3 Waste Quantities
The project is being perceived to cater to a large number of small and medium sized health care
establishments in the private sector and Government establishments. It is estimated that about a
third of the waste would be autoclavable and the balance incinerable i.e. 2.0 T of autoclavable
waste and 5.0 T of incinerable wastes. It is also estimated that about 5% of the total treated
waste would have to be land filled and hence about 0.4 T of waste would have to be land filled.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
7
Chapter 3
3.0 Alternate Options for Bio-Medical Waste Management
3.1 Introduction
Options considered for effective management and handling of the Bio-Medical Wastes need to
incorporate legal, technical and financial constraints that will be imposed on such practices. The
primary objective for providing such a system shall be to ensure safe, efficient and economic
collection incorporating segregation at source, transport, disinfection, destruction and disposal of
the residue, while ensuring that the system is reliable for now and for the foreseeable future.
The overall objective encompasses the following specific objectives:
To reduce the health effects/ risks associated with the proposed activities.
To minimise the environmental impacts.
To ensure the technical reliability of the adopted technology in terms of safety, flexibility and
sustainability under local conditions.
To maximise resource productivity.
To ensure the techno-economic feasibility of the proposed scheme.
3.2 Components of integrated Bio-Medical Waste Management
An integrated waste management system for bio-medical wastes must look into various stages of
the process. These key components can be broadly classified into the following:
Waste Segregation: As explained in chapter 2 wastes segregation will reduce the load of
bio-medical wastes from about 2 kgs/bed-day to about 0.2 kgs/bed-day and this also
minimize the environmental impacts associated with further processing. Waste will have to
be segregated into domestic refuse, hazardous wastes and infectious wastes separately.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
8
Further the infectious wastes will have to be segregated into plastics, metals, and other
infectious wastes generated. Segregation is done effectively if performed at source. MoEF
has issued clear guidelines for colour coded segregation.
Waste Collection and Transport: Facility / unit have to ensure that there are no
environmental or human health impacts while collecting & transporting Bio-Medical wastes.
Treatment/ Storage/ Disposal: Treatment/ Storage and disposal of the wastes have various
options available and are described in detail in section 3.3.
3.3 Treatment/ Storage/ Disposal Options
Waste treatment can be effectively performed by two operations running parallel to each other:
1 A Disinfecting Unit
2 A Destruction Unit
A Disinfecting unit is one that will effectively kill all the microorganisms. Autoclaving,
Microwaving, Hydroclaving and Chemical disinfection processes are the most prevalent
technologies used for disinfection of pathogens from the bio-medical wastes.
Autoclave used for the purpose of bio-medical waste management is expected to be dedicated for
the purpose and is expected to operate under standards specified by MoEF. Medical Wastes
shall not be considered treated unless the time, temperature and pressure indicated in the
standards are reached (for eg. 121o C, 15 psi for 1 hour for normal autoclave)
Microwave and Hydroclave disinfection units are similar in application to that of an autoclave.
Microwave technology cannot be applied for cytotoxins, hazardous or radioactive wastes,
contaminated animal carcasses, body parts and large metal items. Microwave should completely
and consistently kill the bacteria and other microorganisms.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
9
Chemical disinfection is a process of disinfection wherein chemical disinfectants like chlorine
and its derivatives or their disinfectants are used in a closed process to attain complete killing of
the pathogens.
A Destruction unit is one that will completely destroy the wastes into safe end products. High
temperature incinerators are used to achieve this. Incineration is a process by which combustible
materials are burnt, producing combustion gases and non-combustible residue and ash. The
combustible gases are vented into the air after treatment through air pollution control devices.
Ash and other non-combustible residue remain after the destruction/ incineration process is
disposed off securely into a landfill site.
Waste Storage is an applicable option for effective storage of certain hazardous wastes like
mercury and cytotoxins that do not have a cost-effective treatment technology as yet. Waste
Disposal is primary performed by deep burial of wastes into secure landfills.
Waste disposal is an option which remains to exist irrespective of the treatment options, incase
of disinfection waste material post-disinfection needs to be land filled and in case of incineration
the non-combustible residue and ash needs to be disposed off into a landfill and thus landfill
remains to be an integral part of an integrated bio-medical waste management facility.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
10
3.4 Alternate Options for Location of the facility
As discussed earlier, a Bio-Medical waste management facility would be most effective if
incorporated as an integrated facility with a disinfecting unit, a destruction unit and a disposal
unit. The options for locating such a unit shall be to have a centralised facility that will cater to a
group of hospitals or a localised facility with each of the hospital having an integrated
management system.
The advantages of centralised facility over localised facility in each of the components of waste
management are elaborated below:
Waste minimization would require the same effort in both the options.
Collection and Transportation of the wastes would be minimal for a localised facility
compared to that of a centralised facility.
Efficient management of treatment options would be low in localised facilities as this would
require a group of trained professionals to handle.
Disposal facility would be available at centralised facility while localised facilities would have
to send the residue to designated landfills.
Social Acceptability for a localised facility is very low, as most of the hospitals are located in
the heart of the residential areas with high population density. The prevalent concept of NIMBY
(Not in my Backyard) further decreases the level of social acceptability. As a centralised facility
would be located away from residential areas having low population density, it would be more
acceptable.
Impacts on Human Health and the Environment would be much higher in case of localised
facilities as the number of individuals exposed to the various pathways would be much higher,
while at the centralised facility it would be lower.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
11
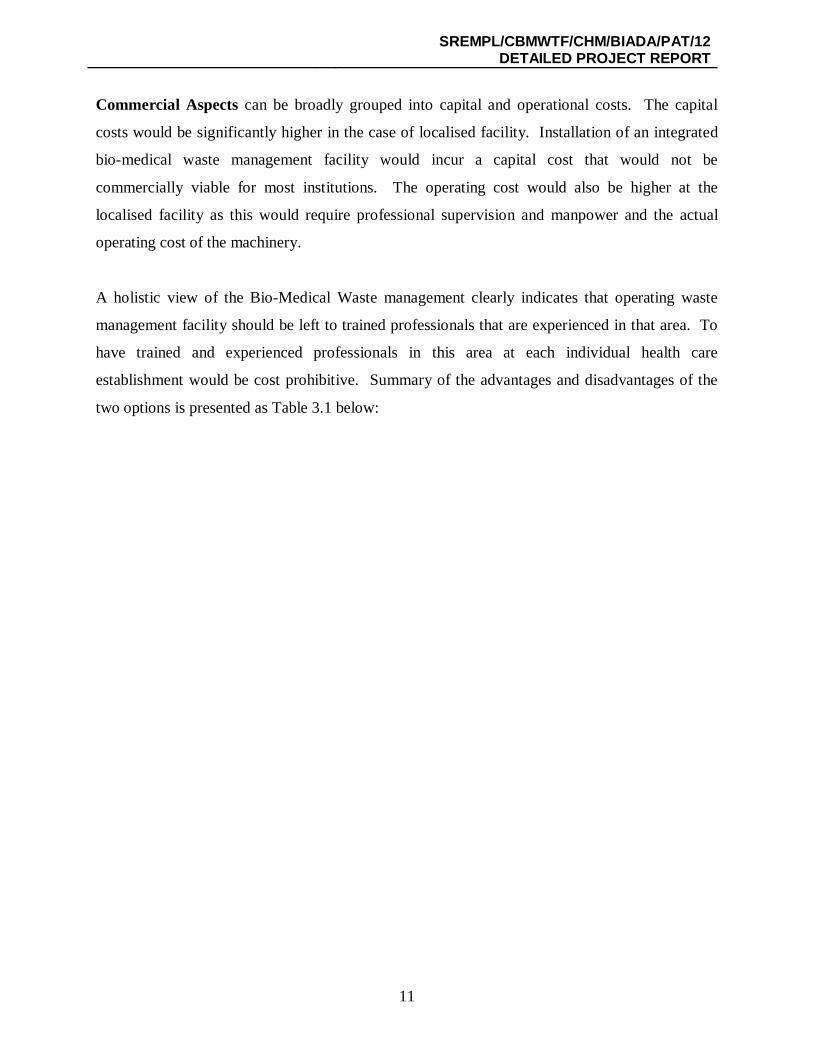
Commercial Aspects can be broadly grouped into capital and operational costs. The capital
costs would be significantly higher in the case of localised facility. Installation of an integrated
bio-medical waste management facility would incur a capital cost that would not be
commercially viable for most institutions. The operating cost would also be higher at the
localised facility as this would require professional supervision and manpower and the actual
operating cost of the machinery.
A holistic view of the Bio-Medical Waste management clearly indicates that operating waste
management facility should be left to trained professionals that are experienced in that area. To
have trained and experienced professionals in this area at each individual health care
establishment would be cost prohibitive. Summary of the advantages and disadvantages of the
two options is presented as Table 3.1 below:
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
12
Table 3.1 Localized facility Versus Centralised facility:
Aspect Localised facility Centralised facility
Waste Minimisation ND ND
Waste Segregation Efficient Higher Efficiency
Collection and
Transportation
Minimal Medium – High
Disinfection Variable Efficiency – Guaranteed
Thermal treatment Variable Efficiency – Guaranteed
Landfill ND ND
Social Acceptability Very Low Higher
Human Health Impacts High Low
Environmental Impacts High Low
Commercial Aspects
Capital Costs Very High Minimal
Operating costs High Low
ND – No Difference
3.5 Summary
In summary an efficient and an integrated waste management program shall comprise of various
components including waste minimization, segregation, collection and transport, disinfection,
destruction and disposal, which could be efficiently managed and handled by professionally
trained personnel. As this would be cost prohibitive for localised facilities a centralised facility
catering to group of hospitals would be more effective than localised ones.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
13
Chapter 4 4.0 The Proposal and Process Description
4.1 Introduction
As described in the earlier chapter hospital wastes once generated need to be segregated,
collected, transported and safely treated and disposed of without causing damage to the human
health and the environment. To redress this problem and provide the health care establishments
with a cost-effective solution to the waste disposal dilemma, SembRamky Environmental
Management Pvt. Ltd. proposes for the development of integrated Bio-Medical Waste
Management Facilities in Patna which will also cover the surrounding areas and strictly based on
the BMW (Management & Handling) Rules, 1998 and amendments of 2000 and 2003 published
by Ministry of Environment and Forest (MOEF).
SEMBRAMKY has identified the following as the major steps involved in making the system
efficient:
A Waste Audit
Training and Awareness – The Doctors, Nurses, Administrators and the ward boys.
Waste Minimization
Segregation at source
Collection and transport
Disinfection/ Destruction
Disposal.
4.1.1 Waste Audit
SEMBRAMKY shall undertake a waste audit to assess the waste quantities, present management
and handling practices and subsequent treatment and disposal of the wastes. The audit shall
include a survey of representative health care establishments and cover all aspects related to bio-
medical wastes including occupational health and safety.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
14
4.1.2 Training and Awareness
Our experiences indicate that, the awareness levels of most health care establishments in respect
to bio-medical waste management are very low. The health care workers are not completely
aware of the impacts of the improper waste handling and management. Our first step towards
our endeavor would be to create awareness among all the stakeholders involved in the subject.
Subsequent to this SEMBRAMKY shall provide a thorough training to all the members on
aspects of bio-medical waste Management. This training shall include segregation of wastes into
proper colour coded bags, identification of containers required for collecting the wastes,
precautions to be taken in respect of handling wastes with special reference to sharps
management. There shall be specific focus towards occupational safety of health care workers.
4.1.3 Waste Minimization
Waste minimization, though is a focus from the environmental angle, shall be recommended
only at point sources where there is no scope of cross-infection.
4.1.4 Segregation of Wastes at Source
Segregation of wastes is the key to the success of bio-medical waste management. As indicated
in chapter 2, though about 2 kg of hospital waste is generated per bed-day only about 0.2-0.25
kg/bed-day is the infectious portion of the waste. This is a clear indication that only about 10-
15% of the total waste generated at health care establishment is infectious in nature. Thus
segregation of wastes at source would firstly reduce the wastes management problem to 15%.
Further to this segregation of wastes (infectious) is integral in terms of further waste handling
and management.
Bio-Medical wastes would have to be managed by destruction, dis-infection and ultimate
disposal. With this in view, wastes would have to be segregated into incinerable wastes/
destructible wastes and dis-infectable wastes. SEMBRAMKY proposes to establish an
incinerator and an autoclave, thus wastes would have to be segregated into incinerable and
autoclavable wastes. Incinerable wastes include human anatomical wastes, animal carcasses,
placenta, cotton, bandage, soiled materials and other similar wastes that have come in contact
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
15
with the body fluids. Dis-infectable wastes include plastics, glass, metal, rubber and other similar
materials. These would include syringes, needles, ampoules, catathaters, blades and many more.
Focus during the training shall be made on segregation of wastes into colour coded bags ensuring
compliance with the MoEF rules as well as subsequent handling and management of wastes.
Segregation of wastes at source is very critical, as this would minimise further handling of the
wastes until treated.
4.1.5 Collection and Transportation
SEMBRAMKY shall collect the waste from each health care establishment on a regular basis.
Wastes shall be segregated as per the colour coding, properly packed and placed at a secure
designated point by the health care establishment from where SEMBRAMKY shall collect the
waste. Upon collection wastes shall be placed into closed containers enclosed in a containerized
vehicle. Transportation of the wastes shall also be the responsibility of SEMBRAMKY.
The proposed vehicles shall be dedicated for the purpose and shall adopt the conditions specified
in the BMW (Management & Handling) Rules-1998.
waste Collection Vehicles
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
16
4.1.6 Disinfection and Destruction
Upon receipt at the facility, wastes containers shall be unloaded. Wastes based on their colour
codes shall be separated and properly treated and disposed off. Categories 1, 2, 3 and 6 (as per
MoEF rules) shall be directly loaded into the incinerator while categories 4 and 7 shall be loaded
into the autoclave for dis-infection. Residue from these units shall be disposed into a landfill.
Detailed process description of the treatment technologies is presented in the subsequent
sections.
4.1.7 Disposal
Ash, residue from high temperature incineration and other material residues from the process
shall be collected into containers and shall be disposed into a secure landfill.
4.2 Treatment Technologies
4.2.1 Incineration
Incineration incorporates the right technology featuring for a complete destruction of the waste
into completely safe end products. A process combination of pyrolysis and controlled air
combustion, where heat and air for combustion is regulated in such a way as to first volatalise/
gasify the waste in conditions of inadequate air, i.e., below stochiometric air conditions and heat,
and then totally destroy it in adequate heat and excess air, thereby making the end products
environmentally safe. The process is not only safe but is also today’s answer to the rampant
problem of hospital waste management and pollution.
The primary purpose of incineration is to burn the waste to ashes through a combustion process.
SEMBRAMKY intends to setup a 5.0 T/ Day incinerator. The unit shall be a dual chambered
incinerator. The primary chambers primary purpose would be combustion of the
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
17
waste materials into safe end products (ash). The temperature of the primary chamber would be
850o C and above wherein, wastes shall be completely destroyed. The primary chamber would
have an attached burner with auxiliary fuel supply to augment the fuel requirements and ensure
maintenance of temperatures. The purpose of the secondary chamber would be to burn the off-
gases and ensure safe end products (gaseous). The secondary chamber would operate at a
temperature of 1050o C and above. The gases would be completely burnt and safe gases then
shall be let out of the incinerator unit.
Both the primary and secondary burners used by us at our existing plants and proposed at Patna
are imported Italian burners. The incinerator is completely automated with control panel and
continuous recording of temperatures. The entire system is very simple and is easy to operate.
The system is environmentally safe without any hazard.
4.2.2 Air Pollution Control System
The gases after being burnt at 1050o C shall be run into a ventury scrubber followed by a flooded
scrubber with water quenching arrangement. The scrubber shall be an alkaline scrubber to
neutralise the gases and ensure trapping of any pollutants escaping into the environment. The
purpose of water quenching is to reduce the temperature of the gases which are at high
temperature. The clean gases are let out into the environment. The scrubbed water shall be
collected into a sump, where the water is neutralised, and then sent into a cooling tower from
where the water is recirculated into the scrubber after cleaning them of their particulates by way
of pressure sand filter and activated carbon filter. The system is thus a zero discharge system in
terms of water discharges and is pollution free.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
18
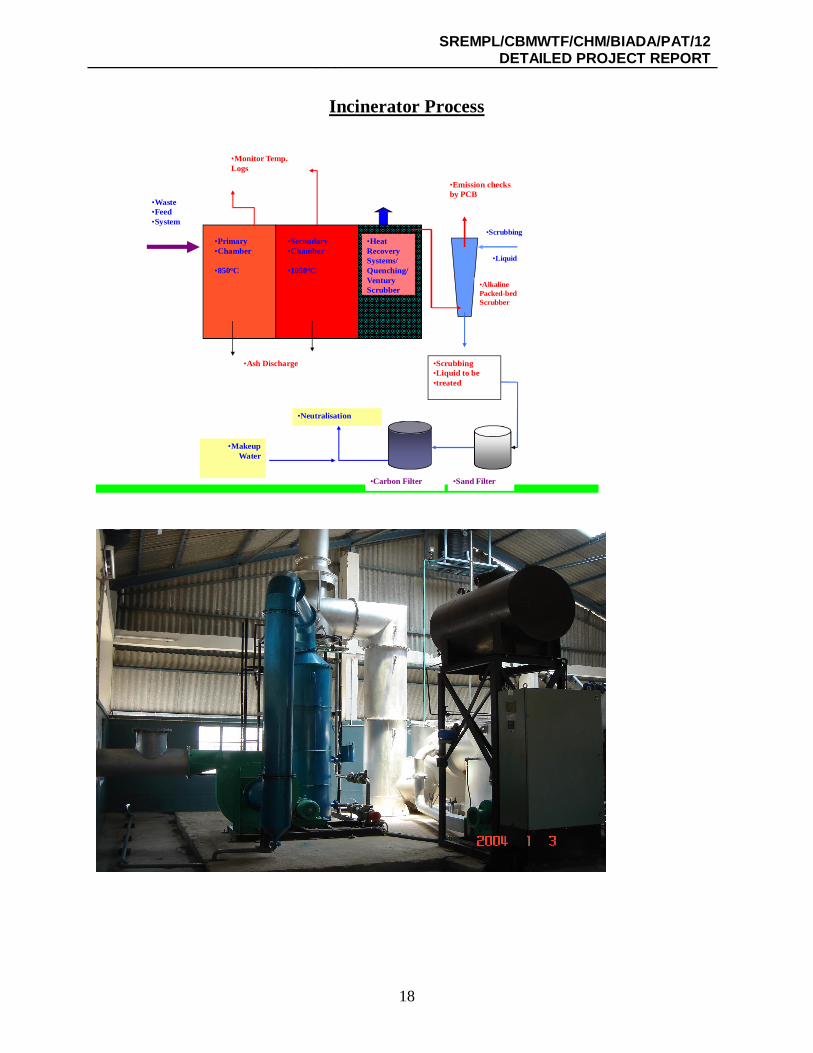
Incinerator Process
•Primary•Chamber
•850oC
•Secondary•Chamber
•1050oC
•Heat Recovery Systems/ Quenching/ Ventury Scrubber
•Waste•Feed•System
•Ash Discharge •Scrubbing •Liquid to be•treated
•Alkaline Packed-bed Scrubber
•Emission checks by PCB
•Scrubbing
•Liquid
•Sand Filter•Carbon Filter
•Neutralisation
•Makeup Water
•Monitor Temp. Logs
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
19
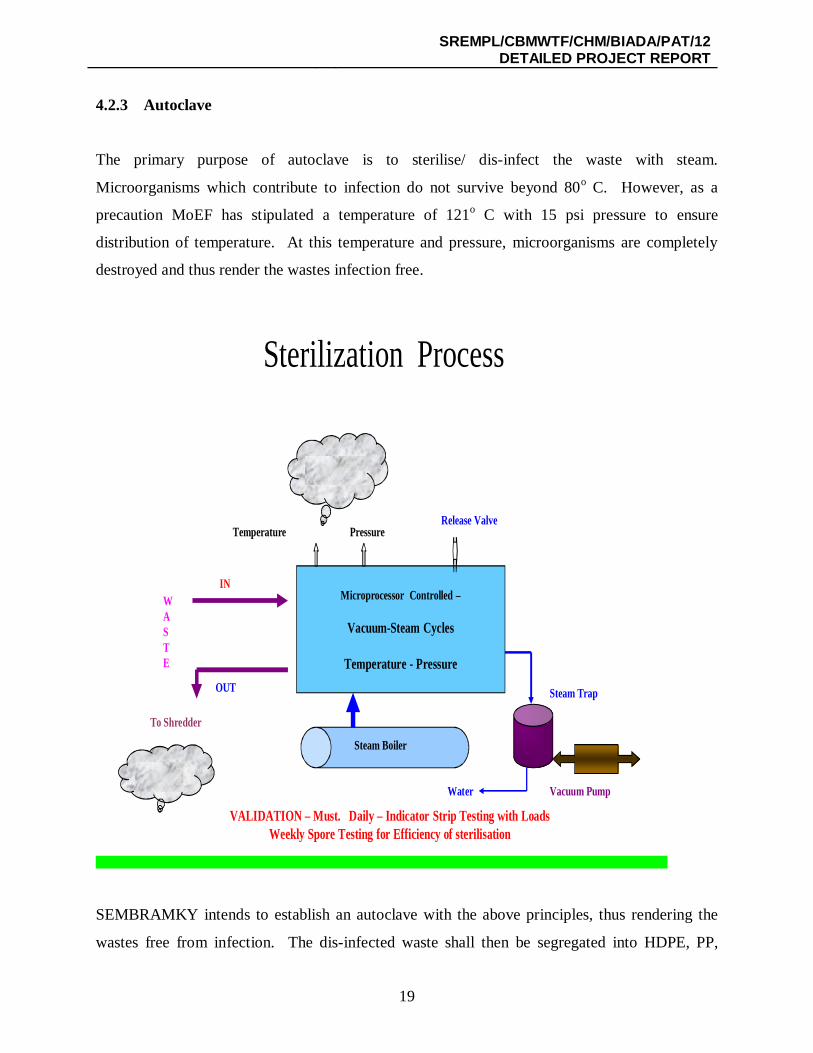
4.2.3 Autoclave
The primary purpose of autoclave is to sterilise/ dis-infect the waste with steam.
Microorganisms which contribute to infection do not survive beyond 80o C. However, as a
precaution MoEF has stipulated a temperature of 121o C with 15 psi pressure to ensure
distribution of temperature. At this temperature and pressure, microorganisms are completely
destroyed and thus render the wastes infection free.
Sterilization Process
Steam Boiler
Temperature Pressure
WASTE
IN
OUT
Release Valve
Steam Trap
Vacuum PumpWater
VALIDATION – Must. Daily – Indicator Strip Testing with LoadsWeekly Spore Testing for Efficiency of sterilisation
Microprocessor Controlled –
Vacuum-Steam Cycles
Temperature - Pressure
To Shredder
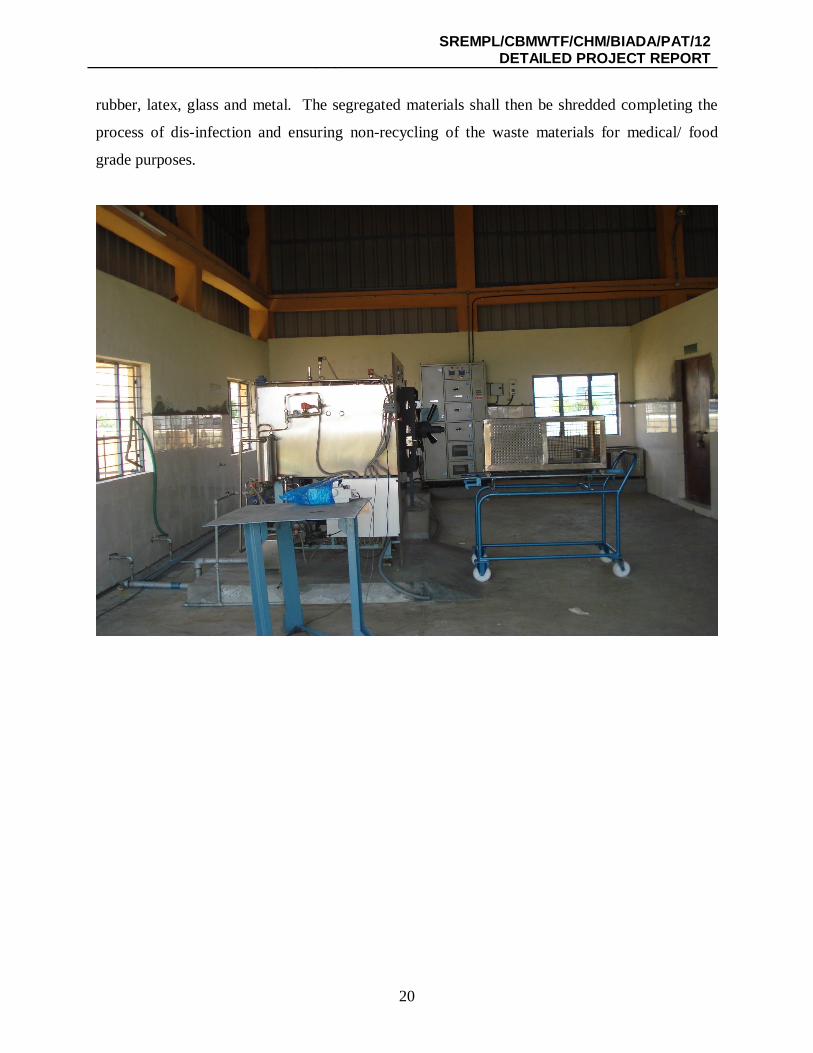
SEMBRAMKY intends to establish an autoclave with the above principles, thus rendering the
wastes free from infection. The dis-infected waste shall then be segregated into HDPE, PP,
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
20
rubber, latex, glass and metal. The segregated materials shall then be shredded completing the
process of dis-infection and ensuring non-recycling of the waste materials for medical/ food
grade purposes.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
21
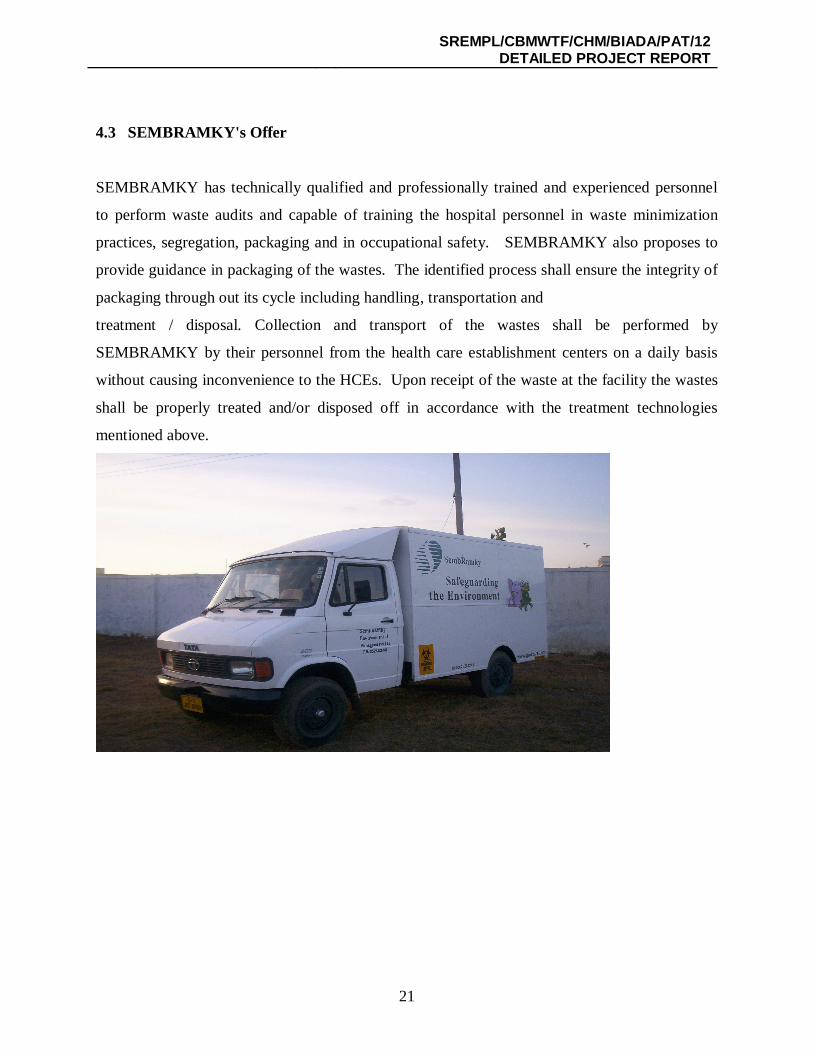
4.3 SEMBRAMKY's Offer
SEMBRAMKY has technically qualified and professionally trained and experienced personnel
to perform waste audits and capable of training the hospital personnel in waste minimization
practices, segregation, packaging and in occupational safety. SEMBRAMKY also proposes to
provide guidance in packaging of the wastes. The identified process shall ensure the integrity of
packaging through out its cycle including handling, transportation and
treatment / disposal. Collection and transport of the wastes shall be performed by
SEMBRAMKY by their personnel from the health care establishment centers on a daily basis
without causing inconvenience to the HCEs. Upon receipt of the waste at the facility the wastes
shall be properly treated and/or disposed off in accordance with the treatment technologies
mentioned above.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
22
4.4 Infrastructure and Specifications proposed for the Project
SEMBRAMKY intends to establish the following infrastructure:
Incinerator: A mechanical loading dual chambered incinerator to cater for disposal of 5.0 T of
medical wastes per day, with the primary chamber operating at 850°C and the secondary
operating at 1050°C. The flue gases shall be run through a ventury and flooded scrubber and
then vented through a 30-m height stack. The temperatures of the incinerator shall be
continuously monitored through a strip chart recorder/data logger for effective recording of
temperatures.
Summary of the Features of the Proposed Incinerator are:
Dual Chambered Incinerator, with MS outer shell and Internal lining using high
alumina refractory.
Loading shall be mechanical.
Interconnected ducting shall also be lined system.
They shall be connected with fully automatic spark ignited burners to be run using
HSD with all necessary interlocks like the cut-off systems.
The system shall be supported with combustion air supply through an FD fan.
Temperatures in both the chambers shall be continuously recorded,
graphically/through a data logger.
Autoclave: A vacuum type (programmable) autoclave which can operate at all the
specifications mentioned by MoEF with a capacity to handle 2 T of medical waste per day. The
autoclave shall have continuous and automatic recording of temperature, pressure, date, time and
batch of loading. Every batch shall be monitored with a strip chart recorder and once in a month
the spore validation test and/or spore monitoring shall be done. Following are the key features of
the proposed autoclave:
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
23
Type: Vacuum Type, automatic with documentation.
Capacity: 2 Ton per day
Temperature: 135° C
Pressure: 35 psi
Automation: PLC with MMI (Man-Machine interface)
Documentation/ Recording: Computerized recording
Effluent Treatment Plant: An ETP to treat the scrubbing water, floor washings and
other wastewater from the plant and send the same for circulation into the scrubber. The
system shall be cooling, followed by pressure sand filter and activated carbon filter
assembly followed by neutralization before recirculation into the scrubber.
Shredder: A mechanical shredder to make the waste unrecognizable as medical waste
shall be installed with a capacity to handle about 3.3 T of medical wastes per day.
Landfill: The residue will be sent to authorize landfill site.
Transport Vehicles: vehicles meeting the specifications mentioned in the tender
document shall be put in place for collection and transport of medical wastes. 10 Nos.
shall be purchased.
Administrative Infrastructure: Administrative, electrical and mechanical infrastructure
like office, rest rooms, roads, generator and other infrastructure shall be developed to
support the waste management activities.

SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
24
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
25
Chapter 5
Environmental Management Plan 5.0 Summary
Bio-Medical Waste Management plant is an environmentally friendly project and the project
itself is an environmental management plan for the effective management of bio-medical wastes
for the project area. However, the emissions from the project also need to be considered and
addressed and this chapter addresses these issues in brief.
5.1 Air Environment
Air environment in the project can broadly be divided into two, firstly the odour emanating from
the wastes and secondly the emissions from the incinerator.
Bio-Medical Wastes are very putriscible and have the potential to degrade very fast and in the
process generate odour nuisance if they are not managed properly. To address the issue
effectively, MoEF has issued rules whereby the wastes will have to be collected, transported,
treated and disposed off effectively. SEMBRAMKY abides to adopt this to ensure that odour
nuisance is eliminated. In addition to the above, SEMBRAMKY undertakes to collect wastes on
a daily basis
The other impact on air environment from the air emissions from the incinerator stack.
However, the impacts are minimal. To minimize the air impacts from the incinerator the flue
gases from the secondary chamber shall be run through a water quenching and ventury scrubber,
where in the high temperature gases shall be rapidly cooled in the water quenching and ventury
scrubber and then the gases shall be run-into a counter current packed bed alkaline scrubber
wherein the gases shall be completely cleaned and then ejected into the atmosphere through a 30-
m high chimney with the aid of an ID fan (10 HP).
The cleaned gases shall be well within the limits specified under the Bio-Medical Wastes
(Management and Handling) Rules 1998. The statement is backed by the emissions measured
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
26
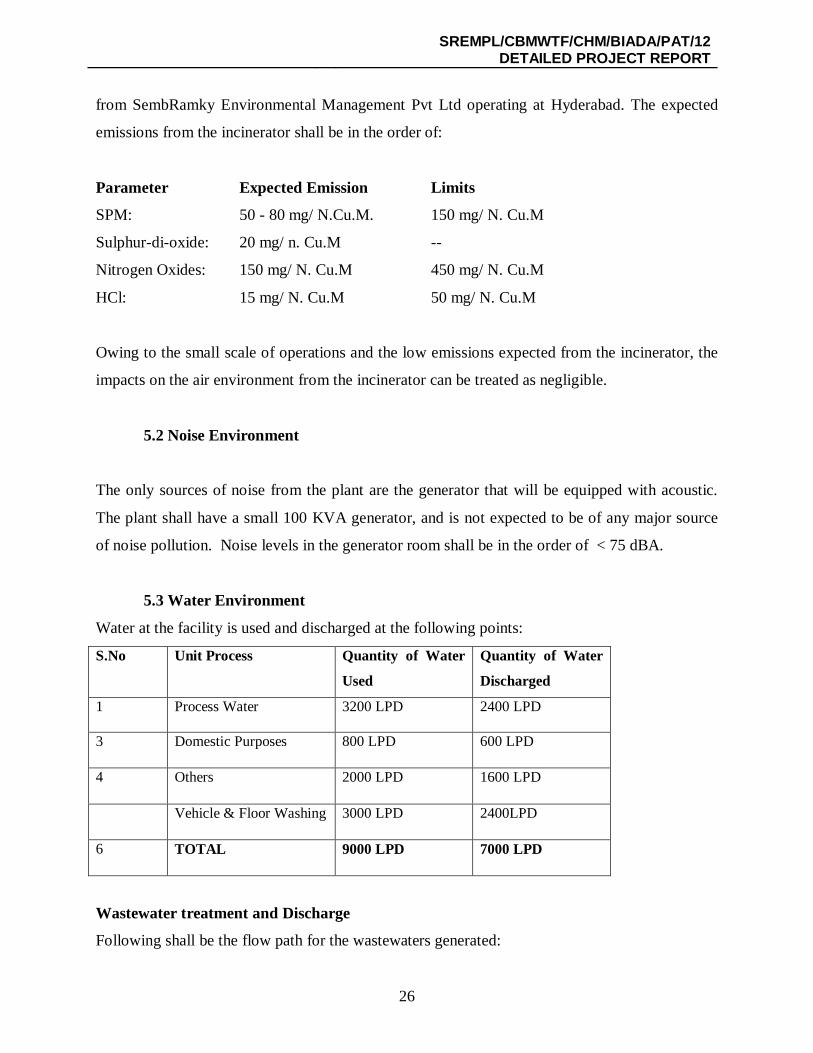
from SembRamky Environmental Management Pvt Ltd operating at Hyderabad. The expected
emissions from the incinerator shall be in the order of:
Parameter Expected Emission Limits
SPM: 50 - 80 mg/ N.Cu.M. 150 mg/ N. Cu.M
Sulphur-di-oxide: 20 mg/ n. Cu.M --
Nitrogen Oxides: 150 mg/ N. Cu.M 450 mg/ N. Cu.M
HCl: 15 mg/ N. Cu.M 50 mg/ N. Cu.M
Owing to the small scale of operations and the low emissions expected from the incinerator, the
impacts on the air environment from the incinerator can be treated as negligible.
5.2 Noise Environment
The only sources of noise from the plant are the generator that will be equipped with acoustic.
The plant shall have a small 100 KVA generator, and is not expected to be of any major source
of noise pollution. Noise levels in the generator room shall be in the order of < 75 dBA.
5.3 Water Environment
Water at the facility is used and discharged at the following points:
S.No Unit Process Quantity of Water
Used
Quantity of Water
Discharged
1 Process Water 3200 LPD 2400 LPD
3 Domestic Purposes 800 LPD 600 LPD
4 Others 2000 LPD 1600 LPD
Vehicle & Floor Washing 3000 LPD 2400LPD
6 TOTAL 9000 LPD 7000 LPD
Wastewater treatment and Discharge
Following shall be the flow path for the wastewaters generated:
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
27
Scrubbing Effluent – Collected in Hot Water Sump
Autoclave Effluent – Collected into the Hot Water Sump.
Floor and Reactor Washings – Collected into the Hot Water Sump
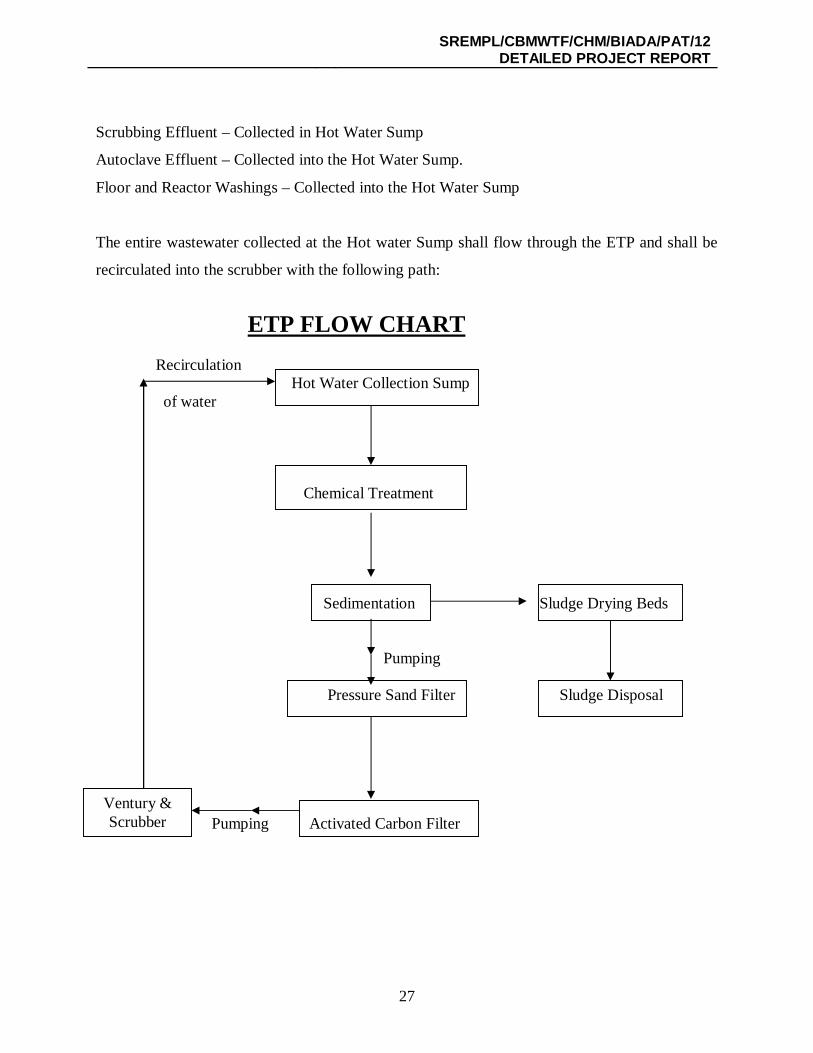
The entire wastewater collected at the Hot water Sump shall flow through the ETP and shall be
recirculated into the scrubber with the following path:
ETP FLOW CHART Recirculation Hot Water Collection Sump of water Chemical Treatment Sedimentation Sludge Drying Beds Pumping Pressure Sand Filter Sludge Disposal Pumping Activated Carbon Filter
Ventury & Scrubber
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
28
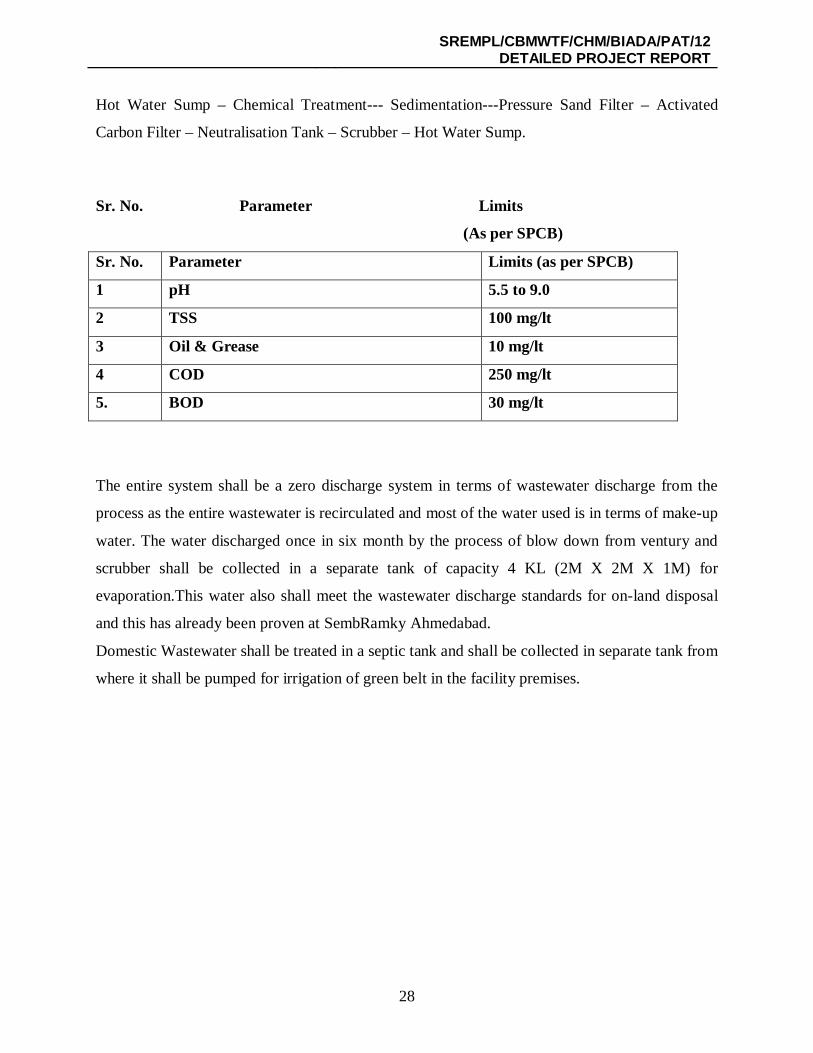
Hot Water Sump – Chemical Treatment--- Sedimentation---Pressure Sand Filter – Activated
Carbon Filter – Neutralisation Tank – Scrubber – Hot Water Sump.
Sr. No. Parameter Limits
(As per SPCB)
Sr. No. Parameter Limits (as per SPCB)
1 pH 5.5 to 9.0
2 TSS 100 mg/lt
3 Oil & Grease 10 mg/lt
4 COD 250 mg/lt
5. BOD 30 mg/lt
The entire system shall be a zero discharge system in terms of wastewater discharge from the
process as the entire wastewater is recirculated and most of the water used is in terms of make-up
water. The water discharged once in six month by the process of blow down from ventury and
scrubber shall be collected in a separate tank of capacity 4 KL (2M X 2M X 1M) for
evaporation.This water also shall meet the wastewater discharge standards for on-land disposal
and this has already been proven at SembRamky Ahmedabad.
Domestic Wastewater shall be treated in a septic tank and shall be collected in separate tank from
where it shall be pumped for irrigation of green belt in the facility premises.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
29
5.4 Occupational Health and safety
The projects key focus area shall be in terms of occupational safety and health as the employees
dealing with infectious wastes with potential for cross contamination and/or infection.
SEMBRAMKY shall take the following steps to ensure that the occupational health is protected:
While Transportation, the collection boys shall wear gloves, masks, rubber gum boots
While unloading the same PPE shall be used.
While loading the wastes into incinerators, the staff shall wear helmet, goggles, masks,
asbestos temperature resistant gloves, and boots.
While segregation, they shall ensure protection from needle pricking and shall use hard
gloves.
Any needle stick injury shall be attended to immediately; they shall thoroughly wash the
injured area using soap/ detergent and then apply disinfectant to the area. Further to this
they shall get checked up for infections.
Health check-up and vaccination will be done as per standard prescribed by health
department.
Note:
1. We have already got the certificates of ISO 9001, 14001 and OSHAS 18001.
2. We are ready to comply with all pollution control measures as suggested by you in
addition to various means proposed in our DPR.
SREMPL/CBMWTF/CHM/BIADA/PAT/12 DETAILED PROJECT REPORT
30
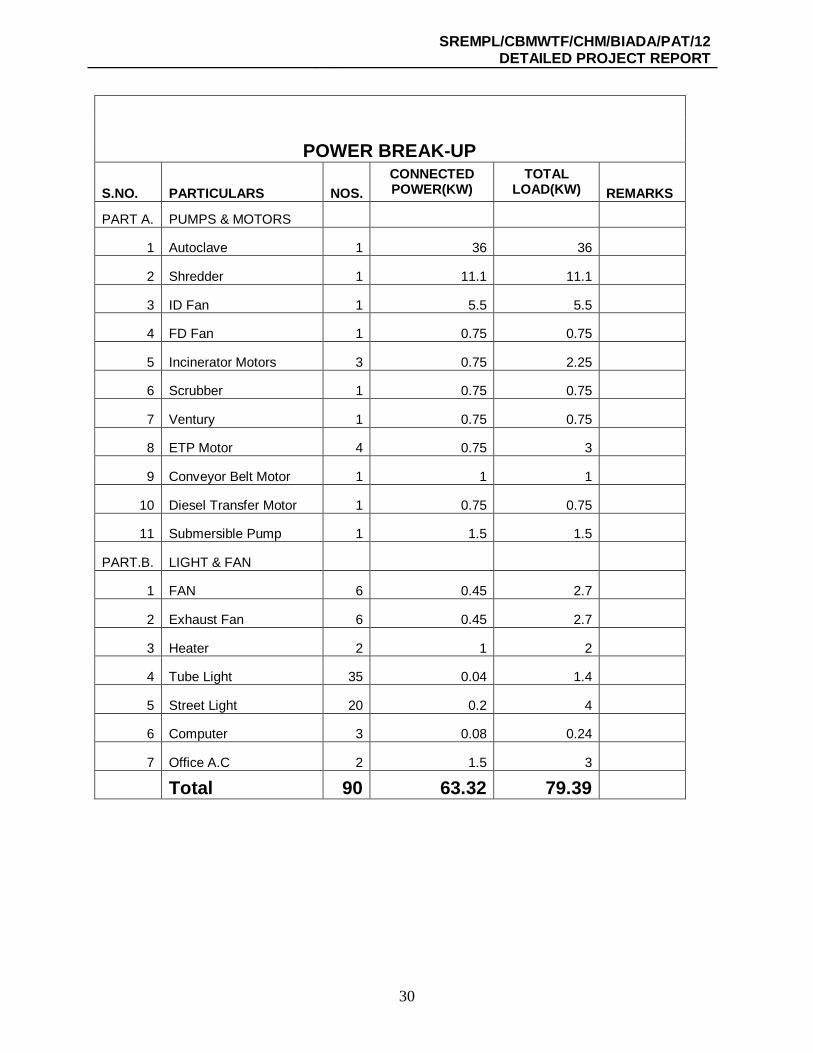
POWER BREAK-UP
S.NO. PARTICULARS NOS. CONNECTED POWER(KW)
TOTAL LOAD(KW) REMARKS
PART A. PUMPS & MOTORS
1 Autoclave 1 36 36
2 Shredder 1 11.1 11.1
3 ID Fan 1 5.5 5.5
4 FD Fan 1 0.75 0.75
5 Incinerator Motors 3 0.75 2.25
6 Scrubber 1 0.75 0.75
7 Ventury 1 0.75 0.75
8 ETP Motor 4 0.75 3
9 Conveyor Belt Motor 1 1 1
10 Diesel Transfer Motor 1 0.75 0.75
11 Submersible Pump 1 1.5 1.5
PART.B. LIGHT & FAN
1 FAN 6 0.45 2.7
2 Exhaust Fan 6 0.45 2.7
3 Heater 2 1 2
4 Tube Light 35 0.04 1.4
5 Street Light 20 0.2 4
6 Computer 3 0.08 0.24
7 Office A.C 2 1.5 3
Total 90 63.32 79.39















![[Organisation’s Title] Environmental Management System [Staff Awareness Training]](https://static.fdocument.pub/doc/165x107/551b5916550346dd1a8b634a/organisations-title-environmental-management-system-staff-awareness-training.jpg)
