Self-Assessment Tool for Pilot Implementation CEEQNET...
31
CEEQNET (Central and Eastern Europe Quality Network) Unified Central and Eastern European surveillance/monitoring system for healthcare quality and efficiency indicators National Health Information Center (Národné centrum zdravotníckych informácii – Slovak Republic), 26, Lazaretská ulica, 811 09 Bratislava, Slovak Republic. Project partners: SEMMELWEIS University The following material has been produced to provide insight of ongoing activities and interim results of the CEEQNET project in June 2006 It contains examples of outputs of this project at the current phase of implementation. CEEQNET goals Objective Administrative healthcare data based system for healthcare quality performance evaluation – Austria, Czech Republic, Hungary, Poland and Slovakia. Cataloging and description of currently used systems of performance measurement, methodologies, data sets Performance defined as composed of: •Clinical production (Volume & Product Portfolio) •Clinical productivity (Human & Financial Inputs / Outputs) •Quality of care Methodology National data audit in areas:
Transcript of Self-Assessment Tool for Pilot Implementation CEEQNET...

CEEQNET (Central and Eastern Europe Quality Network)
Unified Central and Eastern European surveillance/monitoring system for healthcare quality and efficiency indicators
National Health Information Center (Národné centrum zdravotníckych informácii – Slovak Republic), 26, Lazaretská ulica, 811 09 Bratislava, Slovak Republic.
Project partners:
SEMMELWEIS University The following material has been produced to provide insight of ongoing activities and interim results of the CEEQNET project in June 2006 It contains examples of outputs of this project at the current phase of implementation. CEEQNET goals Objective Administrative healthcare data based system for healthcare quality performance evaluation – Austria, Czech Republic, Hungary, Poland and Slovakia. Cataloging and description of currently used systems of performance measurement, methodologies, data sets Performance defined as composed of: •Clinical production (Volume & Product Portfolio) •Clinical productivity (Human & Financial Inputs / Outputs) •Quality of care Methodology National data audit in areas:

Clinical, Capacity, Human resources, Accounting Questionnaire: Systems of performance measurement, methodologies and data sets used in each participating country Results For every tested QI the CEEQNET project identifies: •If National MBDS enables to define the indicator •If Common MBDS enables to define the indicator to be coherent across countries •What are the know factors of indicator distortion in individual countries •If indicator is “trans-culturally compatible” (measures or reflects in another country what was meant to be reflected or measured in the country of origin of the indicator) Common data model enabling formation of a universal data-base for 5 countries QI setsCEEQNET accessible data sets are cross-matched against inter-national QI sets (OECD-HCQI, iQUIP, AHRQ-HUCP, NHS 2001) to find out if HC data in Central Europe can be used for constructing some indicators defined in the above named QI systems. Reporting - Set of Oracle Discoverer® worksheets online via Internet. Conclusions Challenges of consistency of data sources (for Common MBDS needs) Complex mapping is only partly possible. Challenges of transformation of data for data model needs The only country with transparent, logical and complex data model is Austria First known factors limiting benchmarking between countries • Different ways of organizing acute inpatient care • Different descriptions of hospital and care types • Absence of common coding of list of procedures • Low level of reliability of procedures and diagnoses coding in some countries
Project aims at forming a „community of excellence“ of institutions using their data for quality performance improvement compatible with various quality management models. The end result is seen in strengthening the role of health care consumer of Europe facilitating appropriate informed choice of health care service providers, policy-makers and consumers
List of dimensions used in CEEQNET to provide “views” of collected data
• PERIOD • COUNTRY • HOSPITAL (ZZ) • PRIMARY CASE DIAGNOSIS • GENDER

• URGENCY (CASE PLANNING) • TYPE OF CASE ADMISSION • TYPE OF CASE ENDING • TURNOVER TYPES • PROFESSION TYPES • Clinical field • Type of expenses (costs) center • Operational procedures • Secondary case diagnosis
List of characteristics used in CEEQNET
Primary characteristics • Number of cases • Age • Length of stay (LOS) • Costs and revenues (turnovers) • Number of employees („heads/human resources“) • Weighted number of employees („duties“) • Working hours • Salaries
Secondary characteristics • Average age • Average length of stay (ALOS).
OUTPUT No. 1
The first output of the project is detailed description of primary data used in health care (HC) systems of all collaborating countries. It is expected, that this material could prove helpful to any project based on HC data utilization.

OUTPUT No. 2
Tabulated overview of indicators (extractable from data administrated in the 5 countries of the project) proposed for testing in the CEEQNET database (June 2006, Hungarian data not included) Clinical group Mortality
Rate Annual Volume
Utilization Rate ALOS Transfer
Rate AMI PQI A A A HIP Fracture PQI A A A Congestive Heart Failure (CHF) PQI A A A Gastrointestinal (GI) Hemorrhage PQI A A A Acute Stroke PQI A A A Pneumonia PQI A A A PTCA PQI A A A Pancreatic Resection Mortality Rate PQI PQI A A Esophageal Resection PQI PQI A A Abdominal Aortic Aneurysm (AAA) Repair PQI A A A Carotid endarterectomy (CEA) PQI A A A CABG PQI A A A Hip Replacement PQI A A A Craniotomy PQI A A A Laparoscopic Cholecystectomy Rate A A PQI A A Primary Cesarean Delivery Rate A A PQI A A
A = Additional Information

OUTPUT No. 3
A functional database of data „extracted and transformed into a standard format“ from primary data sources of collaborating HC systems. OUTPUT No. 4 Reporting tool (based on Oracle Discoverer technology) enabling different views of database using the „DIMENSIONS“ of CEEQNET
Oracle Discoverer Viewer - examples Oracle Discoverer Viewer is used for CEEQNET analysis reporting. It gives immediate access to all information in data storages, data marketplaces and OLAP systems. With Discoverer Viewer users can easily transform data into information using well known and intuitive interface – online accessible by means of a web browser.
The database of “comparable” measures is produced and allows online access to all participants to their data and visualization in relation to other CEEQNET participating hospitals.

Chapter ICD-10 selection
Chapter selection is made by choice of objects from the DIAGNOSIS dimension. This dimension has the following levels:
• (All) • Chapter ICD-10 (first letter selection, e.g. I = blood circulation) • Three-letters diagnosis (e.g. acute myocardial infarction) • Four-letters diagnosis (e.g. acute transmural myocardial infarction of lower layer)

Indicator: number of cases
Indicator is always present in the „data area“. Besides the total number (COUNT) it is also possible to select average, maximum or minimum value.
Indicator: length of hospitalization and age Other characteristics are Age (average age is shown here) and Length of hospitalization (average length is shown here).

Proportional indicators (including AVG values) allow easy comparison. E.g. - for the selected diagnosis average lengths of hospitalization are different, however average age is very similar in all three compared countries (see red frame).

OUTPUT No. 5
Comparative analysis of the way indicators extractable from administrated HC data in 5 countries of the CEEQNET are being used (e.g. QI for AIM)
INPATIENT PROCESS OF CARE (PHARMACOLOGICAL) INDICATORS
CCORT (Canada)
CCP/HCFA (US)1
WESTCOP (Australia)2
1. Aspirin prescribed within six hours of hospital arrival X X X 2. Aspirin prescribed at hospital discharge X X X 3. Reperfusion with thrombolytics during hospitalization X X 4. Median “door to needle” time for thrombolysis X 5. Beta-blocker within 12 hours of admission X X 6. Beta-blocker at hospital discharge X X 7. ACEI prescribed at hospital discharge X X X 8. Lipid sample obtained within 24 hours of admission X 9. Statin prescribed at hospital discharge X X
INPATIENT PROCESS OF CARE (NON-PHARMACOLOGICAL) INDICATORS
1. Reperfusion using primary PCI X X 2. Median time from door to 1st balloon inflation in primary PCI X
3. Coronary angiography in-hospital or referral for angiography (test indicator*) X X
4. Median length of stay in ED X 5. Median length of CCU/ICU stay X 6. Median length of in-hospital stay X X
OUTPATIENT PROCESS OF CARE (PHARMACOLOGICAL) INDICATORS
1. Beta-blocker prescription filled within 30 days post-discharge X X† X† 2. Beta-blocker prescription within 90 days post-discharge X X† X† 3. Beta-blocker 1 year adherence post-discharge X X† 4. ACEI prescription filled within 30 days post-discharge X 5. ACEI prescription filled within 90 days post-discharge X 6. ACEI 1 year adherence post-discharge X 7. Statin prescription filled within 30 days post-discharge X 8. Statin prescription filled within 90 days post-discharge X 9. Statin 1 year adherence post-discharge X
OUTPATIENT PROCESS OF CARE (NON-PHARMACOLOGICAL) INDICATORS
1. Physician visit within 4 weeks post-discharge X 2. Median waiting time (days) for catheterization post-MI X 3. Median waiting time (days) for PCI post-MI X 4. Median waiting time (days) for CABG post-MI X

OUTCOME INDICATORS CCORT
(Canada)CCP/HCFA
(US)1 WESTCOP (Australia)2
1. In-hospital mortality X X X 2. 30 day mortality X X X 3. 1 year mortality X 4. AMI readmission rate at 30 days post-discharge X X† 5. AMI readmission rate at 1 year post-discharge X X† 6. CHF readmission rate at 30 days post-discharge X X† 7. CHF readmission rate at 1 year post-discharge X X† 8. Unstable angina readmission rate at 30 days post-discharge X X† 9. Unstable angina readmission rate at 1 year post-discharge X X† * Test indicator: quality indicator which has not been incorporated in published guidelines or for which it is uncertain whether the process of care can be feasibly and reliably assessed or uncertain whether it is amenable to quality improvement efforts † no time line was specified DETAILED EXPLANATION RELATING TO INDICATOR: INDICATOR : ACUTE MYOCARDIAL INFARCTION (AMI) MORTALITY RATE Indicator Provider level mortality rate for AMI. Relationship to Quality Better processes of care may reduce mortality for AMI.
As such lower rates represent better quality care. Benchmark
State, regional, or peer group average.
Method: Quality Measure Number of deaths per 100 discharges with diagnosis code
for AMI. Outcome of Interest Number of deaths with diagnosis code for AMI (see
Appendix 6) in any field. Population at Risk All discharges with diagnosis codes for AMI in any field.
(see Appendix 6) Age 18 years and older. Exclude transfers to other institution. Exclude MDC 14 (pregnancy, childbirth, and puerperium) and MDC 15 (newborns and other neonates).
Evidence from the literature Face validity. Acute myocardial infarction (AMI) affects…. Precision. The precision of AMI mortality rate estimates may be problematic… Minimum bias. Starting in 1990, ICD-9-CM included a fifth digit for AMI codes… Risk adjustment. Numerous studies have established the importance of risk Construct validity. Numerous randomized controlled trials have conclusively… Fosters true quality improvement. In general, physicians and hospitals… Prior use. Inpatient AMI mortality, based on administrative data, has …

Empirical Evidence
Test Statistic Rating Precision Raw provider level rate/standard deviation 24.4%, 16.1% Systematic provider -level standard deviation** 3.4% High Provider variation as a percentage of total
variation** 0.8% High
Signal ratio** 42.8% Moderate R-Square** 59.0% Moderate **APR-DRG, age-, gender- adjusted Minimum Bias – APR-DRG risk adjustment Signal variance change with risk adjustment Decreases Fair Absolute impact:
Average absolute change (in %) 32.4%
Fair
Relative impact: Rank correlation Percent remaining in high decile/low decile Percent changing more than 2 deciles
0.747 36.3% / 67.3% 29.0%
Fair Fair Fair
Precision. This indicator is precise, with a raw provider level… Bias. Signal variance decreases by over 25% with risk adjustment… Construct validity. AMI mortality does not load substantially on any of… Discussion Reductions in the mortality rate for acute myocardial infarction on both the patient level and the provider level has been related to better processes of care. Timely and…

OUTPUT No. 6 Description of quality management in collaborating HC institutions – for obtaining a view of initial conditions before use of the CEEQNET dBase. Self-Assessment Tool for Pilot Implementation CEEQNET – quality and efficiency evaluation. based on HPH framework
1. - Relevant improvement of quality and efficiency of healthcare in selected institutions, acceptance and development of principles of quality management and Excellence – is one of the criteria of evaluation of the CEEQNET project by the EC.
In order to document the status of Quality management and efficiency of the hospital, please use either this self-assessment tool, or provide the CEEQNET project leader with any structured self-evaluation (in English in order to be included in the final report of CEEQNET to DG SANCO)
Function Country Manager - Austria Date May 2006 One person has to take the overall responsibility (project leader). Additional responsibilities may be distributed for the various standards, according to the hospital's structure and human resources available Standard 1: Management Policy The organization has a written policy for quality management. The policy is implemented as part of the overall organization quality improvement system, aiming at improving health outcomes. This policy is aimed at patients, relatives and staff. To describe the framework for the organization's activities concerning the organization's quality management system. The MBDS Hospital data provided to the CEEQNET-Project are data from Hospitals of Upper Austria. Following the description will mirror the situation, policy and management System of those hospitals.
1.1. The organization identifies responsibilities for the process of implementation, evaluation and regular review of the policy.
Based on legal rules all hospitals of Upper Austria have to take part in an international QI-Project – clinical outcome measuring system. Goal is the Self Assessment to force continous quality improvement strategies. Structure and process-indicators (within the MBDS-data) are only used for planning. Each hospital has a so called Q-Commission, responsible for all Quality issues within the hospital-Quality targets and each hospital has a Quality plan. Hospitals state missions in regard to administration, resources, staff and performance are available.

No Partly Yes The hospital's stated aims and mission include quality management [Evidence: time-table for the action or list of activities]. Comments: Strategic goals and the use of internal and external indicators are part of the Q-management system. No Partly Yes Minutes of the governing body reaffirm agreement within the past year to participate in the CEEQNET project [Evidence: date for the decision or for payment of the annual fee]. Comments: No Partly Yes The hospital´s current quality and business plans include QUALITY ASSURANCE. [Evidence: quality management explicitly in the plan of action] Yes (see above) No Partly Yes The hospital´s QUALITY ASSURANCE policy has been formally adopted or revised by the executive management within the past two years. [Evidence: minutes or instructions from the CEO or other responsible member of the management] Yes No Partly Yes The policy explicitly refers to QUALITY ASSURANCE for patients, staff and community [Evidence: guidelines for action for patients, specific plan for staff and community]. Yes (see above) No Partly Yes
1.2. The organization allocates resources to the processes of implementation, evaluation and regular review of the policy. A programme for quality assessment of the promoting activities is established.
As mentioned above quality self assessment has to be established by law. Partly there are defined budget and/or staff resources for Quality Management. Operational procedures concerning the Organisation are available. Clinical guidelines for Hygiene, for instance. Pathways are partly esablished and/or in development. [Evidence: time schedule for surveys is available] Comments: No Partly Yes There is an identifiable budget for the evaluation of QUALITY ASSURANCE services and materials . [Evidence: budget or staff resources] Comments: No Partly Yes Operational procedures (e.g. clinical practice guidelines or pathways) available in clinical departments incorporate QUALITY ASSURANCE. [Evidence: check guidelines] Comments: No Partly Yes
1.3. Staff is aware of the quality management policy and it is included in induction programmes for new staff. The hospital organization structure identifies personnel and functions for the coordination of QUALITY ASSURANCE

Each hospital has established an interdisciplinary Quality commission (by law). The Q-commission is responsible for “information, coordination” in regard to Quality issues. The Q-commission initiates Quality circles for improvement projects. [Evidence: staff member nominated for the coordination of QUALITY ASSURANCE]. Comments: No Partly Yes
1.4. The organization ensures the availability of procedures for collection and evaluation of data in order to monitor the quality of quality management activities. Data are routinely captured on QUALITY ASSURANCE interventions and available to staff for evaluation.
Within the international performance measuring system each organisation of Upper Austria collects data for each implemented indicator routinely (monthly and quarterly) and receives feedback in comparision with aggregated data (Austrian, European, US) quarterly.

[Evidence: availability assessed in staff survey] Comments: No Partly Yes There is documented evidence of ongoing systematic audit including implementation of the QUALITY ASSURANCE policy in each department. [Evidence: time schedule for the audit] see above No Partly Yes Staff in all departments are aware of the content of the policy. [Evidence: annual performance evaluation or staff's participation in the QUALITY ASSURANCE programme] partly No Partly Yes The hospital´s induction program for new staff specifies health promotion activities. [Evidence: the program includes introduction to the QUALITY ASSURANCE plan] no No Partly Yes The policy is accessible to staff in all departments and all shifts. [Evidence: newsletters, posters or brochures] yes No Partly Yes The organization ensures that staff has relevant competences to perform quality management activities and supports the acquisition of further competences as required. [Evidence: Comments: No Partly Yes
1.5. Job descriptions for all staff members specify relevant quality improvement activities.
All members of the Q-commission have to be trained in quality management. [Evidence: for individuals or well-defined groups. Familiarity with job description documented by survey or interview] Comments: No Partly Yes Continuing professional development program includes education in quality asurance. [Evidence: training program on QUALITY ASSURANCE attended] partly No Partly Yes
1.6. The organization ensures the availability of the necessary infrastructure, including resources, space, equipment, etc. in order to implement quality management activities. Specific structures and facilities can be identified.
Resouces are partly available (like equipment) There exists no policy document which covers issues like training or resources.

[Evidence: facilities available] No Partly Yes Comments: % of staff aware of quality management policy % of patients aware of standards of quality management
26 Standard 1 Management Policy Complementary indicators Additional Indicators (local indicators you may want to consider for the action plan) e.g. % budget dedicated to staff QUALITY ASSURANCE activities
27 The organization ensures procedures to assess specific needs for quality management for diagnosis-related patient-groups. Guidelines are present on how to identify needs for QUALITY ASSURANCE for groups of patients (e.g. asthma patients, diabetes patients, chronic obstructive pulmonary disease, surgery, rehabilitation). [Evidence: for groups of patients specifically treated in the clinical department] Comments: Management Policy In principle clinical guidelines are available and used; developed by physician association and/or organisations (e.g. asthma patients, diabetes patients). Education and training possibilities are given. Procedures and Guidelines are developed by multidisciplinary teams. No training assessment will take place. No Partly Yes The organization ensures the establishment and implementation of a comprehensive Human Resources Strategy that includes the development and training of staff in quality management skills Comments: Only for the members of the Q-commission. No Partly Yes A performance appraisal system and continuing professional development exists. [Evidence: documented by review of staff files or interview] Comments: No Partly Yes New staff receive an induction training. [Evidence: interviews with new staff] Comments: No Partly Yes Training plans are set up and fulfilled by the end of the year. [Evidence: check with staff] partly No Partly Yes Working practices (procedures and guidelines) are developed by multidisciplinary teams. [Evidence: check procedures, check with staff] partly (see above) No Partly Yes Staff's knowledge on quality management is assessed through surveys. [Evidence: check questionnaire used for and results of staff survey] no No Partly Yes

Readmission rate for ambulatory care sensitive conditions within 5 days Comments: Cannot see the relation to the other questions. No Partly Yes Number of guidelines developed or revised with collaboration of external users and care providers Comments: No Partly Yes

OUTPUT No. 7 NEWSLETTER (quarterly) – To prime and facilitate the use of performance measurement and benchmarking in everyday life in HC facilities. Benchmarking culture is interpreted not as a mean to “see your relative position in a league-list”, but as a tool (means / platform) for discussions and collaboration for improvement – benchmarking is implemented as an enabler to become best.

CEEQNET Health Care Quality Newsletter 2004
Dear partners of the CEEQNET project. As you are all aware of, the main aim of our project is to share best practices for the improvement of all the health care services our respective facilities provide to our patients. There is a multitude of activities targeted on improvement of quality, accessibility, efficiency, efficacy, safety and timeliness of the services we are providing. The core product of our efforts (the identification and appropriate use of some core measures which can be extracted from the already used databases of our respective health care facilities) would be useless, unless we are able to interpret the measures in the context of our health care systems and assure appropriate processes leading to improvement in the work we are doing. In order to facilitate the process of reflection and reorientation of some of our everyday efforts, please accept the following newsletter (which will be produced periodically) as a service to all members of our community – „ to find out what's going on in other places and organizations“. We sincerely hope, that you will (if you have lists of significant links relating to performance and quality management in health care, or if you can provide or point to significant documents) all actively collaborate in the production of our future newsletters. We are more than eager to receive any of your comments, that will help us develop this newsletter into a useful resource not only for you, but also for any health care facilities you may be collaborating with. Sincerely yours Michaela Taborska (assistant to CEEQNET Project Leader) Ales Bourek (Project leader) Please be so kind and send your comments and suggestions to [email protected] This newsletter keywords: health care indicators, reports, hospitals, EHR (electronic health records), surveys, European, spending
JULY – SEPTEMBER 2004 ..........................................................................................................................20 New tool of the National Committee for Quality Assurance................................................................20 New Jersey releases first annual report on hospital care....................................................................20 URAC plans to convene a research and focus group to explore new quality benchmarks..................20 New JCAHO web site regarding quality checks ..................................................................................20 NCQA releases Quality Compass®2004 and Updated Quality Dividend Calculator.........................21 A few medical conditions account for large share of health spending growth ....................................21 The results of the Sixth Annual MRI Survey of EHR Trends and Usage for 2004 are now available .21 Health monitoring programme : Funded project 2002 : "European Emergency Data Project - EMS-Data-Based health surveillance system".......................................................................................................22

Health monitoring programme : Funded project 2001 : "ECHI 2 - European Community Health Indicators (Phase 2)"...........................................................................................................................22
July – September 2004
New tool of the National Committee for Quality Assurance http://www.ncqa.org/PhysicianQualityReports.htm NCQA’s Recognized Physician Directory allows you to identify physicians in your area who demonstrate a high level of performance in providing care NCQA announced that a new online tool and a new arrangement with the GeoAccess division of Ingenix, a leading supplier of physician directory information, will make NCQA-supplied information about doctor quality readily available to tens of millions of consumers. The forthcoming data on doctor quality are drawn from physician recognition programs in the areas of diabetes and cardiac/stroke care. To earn recognition, physicians must meet rigorous quality and performance standards. Historically, little such information has been available.
New Jersey releases first annual report on hospital care http://web.doh.state.nj.us/hpr/ The New Jersey Department of Health and Senior Services unveiled the state's first annual hospital quality report, which rates hospitals' performance on eight measures of care for heart attack and pneumonia. The measures are among those used in the national Quality Initiative led by the AHA and others, and among those required for a full Medicare payment update starting next year through the Medicare Modernization Act. The report is based on data from 82 hospitals, which treated 16,000 heart attack patients and 28,000 pneumonia patients over a nine-month period last year. New Jersey Hospital Association President and CEO Gary Carter said the report will complement hospitals' ongoing quality improvement efforts and urged consumers to use the report along with information from hospital Web sites, friends and neighbors, and physicians to learn about their hospitals' quality of care. "As valuable as this data is, no single study should be used to judge the overall quality of health care in New Jersey," he said.
URAC plans to convene a research and focus group to explore new quality benchmarks http://www.urac.org/default.asp?navid=home&pagename=default URAC plans to convene a research and focus group to explore new quality benchmarks for health information technology (HIT), including the possible development of standards addressing electronic health records and HIT systems infrastructure. URAC, an independent, nonprofit organization, is well-known as a leader in promoting health care quality through its accreditation and certification programs. URAC offers a wide range of quality benchmarking programs and services that keep pace with the rapid changes in the health care system, and provide a symbol of excellence for organizations to validate their commitment to quality and accountability. Through its broad-based governance structure and an inclusive standards development process, URAC ensures that all stakeholders are represented in establishing meaningful quality measures for the entire health care industry.
New JCAHO web site regarding quality checks http://www.qualitycheck.org/ The Joint Commission has had a longstanding commitment to providing meaningful information about the comparative performance of accredited organizations to the public. In 1994, the Joint Commission

first published organization-specific Performance Reports. In 1997, Quality Check®, a directory of Joint Commission accredited organizations and performance reports, became available on the website. In 2004, Quality Reports ― containing merit badge achievements, Hospital Quality Measures and other core measure data ― replaced Performance Reports, although historical Performance Reports are still available. The improvements continued in 2005 with a redesign of Quality Check. The process included extensive testing and input from consumer focus groups and stakeholders, including four advisory groups and state hospital associations. An online survey was also posted on the Joint Commission website. The feedback was used to refine and clarify Quality Reports for both health care professionals and the public.
NCQA releases Quality Compass®2004 and Updated Quality Dividend Calculator http://www.ncqacalculator.com The National Committee for Quality Assurance (NCQA) has released the latest update to its comprehensive database of health plan performance information, Quality Compass® 2004. The database includes information on NCQA Accreditation and plan-specific results on HEDIS® and CAHPS® measures, data sets that measure clinical performance and member satisfaction, respectively. A measure of flu shot rates for adults is included in this year's edition of Quality Compass for the first time. This year's data was reported by 262 health plans that cover more than 60 million Americans collectively.
A few medical conditions account for large share of health spending growth http://www.healthaffairs.org/ The 15 most costly medical conditions accounted for about half of the growth in health care spending between 1987 and 2000, largely due to more people being treated for those conditions and to more expensive and effective drugs and technologies, according to a study published by Health Affairs. Five conditions -- mental disorders, cerebrovascular disease (such as stroke and cerebral ischemia), pulmonary disease and diabetes -- accounted for 31% of the growth. "If we really want to get a handle on rising health care costs, we need to analyze what it is we're spending money on, instead of where we're spending the money," said lead author and economist Kenneth Thorpe. "By focusing on a disease-based analysis of spending, we can compare the medical benefits we are purchasing."
The results of the Sixth Annual MRI Survey of EHR Trends and Usage for 2004 are now available http://www.medrecinst.com/pages/latestNews.asp?id=115 The results of the MRI Survey of EHR Trends and Usage are available to download (see below) at no cost. A total of 808 individuals responded to the survey. However, to increase relevancy and reduce bias, responses from vendors, consultants, and payers are not included in the results. Therefore, the results that follow include only provider responses with a total database size of 436. The data includes responses from April 30th through June 11th, 2004. The EHR Survey includes the results from all sixteen questions in the survey, including the first four demographic questions. The MRI Survey of EHR Trends and Usage reveals insights into the:
• Motivations driving the need for Electronic Health Record systems • EHR applications and functions being implemented or planned • IT platforms used to support EHR applications • EHR configurations for different environments • Data capture methods being employed • Major barriers to implementing EHR systems

• Mobile/Wireless healthcare priorities, applications, platforms, and concerns
Health monitoring programme: Funded project 2002 : "European Emergency Data Project - EMS-Data-Based health surveillance system" http://ec.europa.eu/comm/health/ph_projects/2002/monitoring/fp_monitoring_2002_exs_07_en.pdf Related project from the emergency care area, final report available As the principle result, there were five key indicators defined and recommended to be included in the European Community Health Indicators (ECHI) short list:
• Unit hours ELS + BLS + ALS per 100,000 inhabitants (with 3 sub-indicators for ELS, BLS and ALS) Indicator for Health System/ Resources
• Response time (with 2 sub-indicators: 90% percentile and percentage ≤ 480 sec) Indicator for Health System / Performance
• Rate of highest priority responses per 100,000 inhabitants Indicator for Health System/ Utilisation
• Rate of FHQ diagnoses per 100,000 inhabitants (with 5 sub-indicators: cardiac arrest incidents,
severe trauma incidents, severe breathing difficulties, cardiac chest pain incidents and stroke incidents) Indicator for Health Status / Mortality; Morbidity
• Rate of ALS interventions per 100,000 inhabitants (with 3 sub-indicators: assisted ventilation, intubation and iv drug administration) Indicator for Health System/ Performance Additional indicators that can be applied universally were identified as future recommendations. An outstanding example of a clearly identified, defined and essential indicator is “Time to First Shock”. It marks the interval between collapse after cardiac arrest and application of the first defibrillatory shock in patients suffering from ventricular fibrillation. The time period determines the chances of good neurological recovery and/or survival after cardiac arrest and is therefore considered to be one of the most crucial indicators for EMS performance. The pilot study revealed significant limitations regarding availability and comparability of this key indicator, so it was not included in the list of recommended EMS key indicators. Unless there is a focus on prevention and public health for FHQ conditions, EMS demand will rise due to demographics and morbidity and the health-care burden will increase. A European declaration of emergency care rights needs to be made and supported by a template for minimum standards for a European EMS system.
Health monitoring programme: Funded project 2001: "ECHI 2 - European Community Health Indicators (Phase 2)" http://ec.europa.eu/comm/health/ph_projects/2001/monitoring/fp_monitoring_2001_frep_08_en.pdf Related project aimed at healhcare indicators, final report available As a follow-up of ECHI-1, the ECHI-2 project has expanded the indicator list, with input from many projects under the Health Monitoring Programme and recently the Public Health Programme. This has resulted in (1) the ‘long list’, which consists of an inventory of indicators structured within a robust conceptual frame, but with recognized imbalances reflecting specific areas covered by HMP projects; (2) the concept of ‘user-windows’ which allows for the interest-oriented selection of subsets of indicators; (3) the shortlist, which is selected as a subset from the long list for first priority implementation; and (4) a web-based application (ICHI-2, International Compendium of Health Indicators) in which the ECHI indicators are listed, with their definitions, along with the indicators used by Eurostat (rather as ‘statistical indicators’), WHO-Europe (in the HFA database) and the OECD (OECD health data). Thus, the project has served two functions:

first to develop a list of items and indicators for more comparable data collection among EU Member States, and second, to act as a sort of co-ordinating momentum or ‘umbrella’, integrating the results of a variety of projects into a common structure.

OUTPUT No. 8 Detailed descriptions of HC quality approach in all 5 collaborating countries (provided by Country Leaders of CEEQNET). A detailed description of HC QM systems of CEEQNET countries was produced: e.g. Czech Rep. approach:
The System of Quality Management and Information on Quality in Health Care in the Czech Republic
1. International aspects There is no specific uniform concept of management and assessment of quality and efficiency in health care and its international acknowledgement within the EU to date. Accordingly, the quality of health care is managed directly at national levels of the respective countries. The current activities in the health sector in the Czech Republic are based on the basic conceptual requirements of the EU and WHO, which means that the health sector must be focused on results and the provision of medical services should correspond to the needs of society. The concrete approach to the solution is implemented, however, within the powers of the Czech medical institutions and specialists. The common international goal acknowledged by the CR today is quality, safety and efficiency of the provided medical services including the progressive provision of international comparability of the standard of the provided care.
Within the concept of quality in health care, the CR now prefers an internationally coordinated comprehensive model of professional and managerial qualification of the medical facility to provide quality, efficient and safe care at adequate scientific level which is perceived as quality care also by the clients and which is economically effective as well. This model was defined globally by the International Society for Quality in Health Care (ISQua) in cooperation with WHO and the World Bank. This model of accreditations of medical facilities contains the basic international principles of the approach to quality and efficiency in care that should be elaborated in the national accreditation standards of individual countries. The National Health Accreditation System is expected to be established in the CR to ensure a uniform access to the accreditation activity in health care in accordance with the ISQua international accreditation principles. The accreditation evaluation must be ensured by accreditation commissions, i.e. commissions of specialists with long-standing experience in the field, knowledge of management principles and a high level of professional and personal …………………….(the original document has 25 pages)

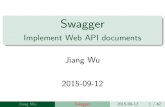
REGISTRACE
STANDARDIZACE
SYSTÉMY MANAGEMENTUISO 9000, ISO 14000, BS8800
AKREDITACE ZDRAV. ZAŘÍZENÍ,KLINICKÝCH LABORATOŘÍ
(JCIA, ISO 15189 + ISO 15190)
EFQMEXCELLENCE MODEL
Odbornázpůsobilost
FIGURE: Hierarchical structure of the QMS of Czech HC Slovak Republic:
Quality and efficiency of health care in Slovakia and
selected health care providers
Improvement of the health status of the population, extension of the life expectancy
and improvement of life conditions belong to the priorities of the Government of Slovak Republic. Carrying out of tasks is covered by several Departments; however the pilot Department is the Ministry of Health. One of the measuring tools of these priorities is assessment, monitoring and evaluation of quality indicators at the providers of health care. The sense of the quality indicators has several dimensions:
- Quality of the provider - Health status of the population - Patient safety - Economy of the health care - International standardization Quality indicators were initiated by the Ministry of Health and built in the Directive of
Government No: 752/2004. The aim of the Directive is the improvement of evaluation of health care providers in range of those diseases, which occurrence in the population is globally severe, i.e. oncologic, cardiovascular, and surgical and others. This Directive is updated on demand and a group of experts actively cooperates on the revision of the documents in sense of getting updated set of indicators in Slovak health care closer to the range and structure of HCQI by OECD.
Evaluation of the stipulated quality indicators in Slovak Republic is assured by the Health Insurance Companies. These indicators concern mainly availability of the care, their efficiency, fairness, health care results and opinions of the patients.

Quality indicators are subject to interest of the Government, together with WHO, OECD and World Bank. Slovak Republic became a regular member of OECD in 2004 and started to work in selected expert groups. One of those groups was the HCQI Expert Group – the group for Health Care Quality Indicators. The goal of the Group is to identify and harmonize indicators of health care provision, to enable collection of selected statistical data, followed by evaluation and final ranking among the member countries of OECD. First phase of the project was to choose indicators available for the majority of member countries. ……………………….
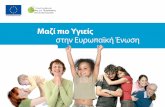
Figure 2: Basic model of quality management system in health care services
(Aplication of ISO 9000:2000 on health care)
•
QUALITY MANAGEMENT SYSTEMCONTINUAL IMPROVEMENT
Managementresponsibility
HEALTHCARE PERFORMANCE
Measuring, analysing, improving
Managingsources
INVOLVED
PARTIES
-
SATISFIED
CL I ENT
REQUIREMENTS
Quality of life
OUTPUTVSTUPY
Internal environment of care facility
Defined environment with clear authorisation (the right for choice of physician mainained), economy of care providerfocused on QH and QL staff of the care provider
- People (their QL and QH)- medicaments, disposables, devices, ...
Added value – return, maintain and/or
improve QH
Conditions for increasingGDP/1 inhabitant

TASKS TO BE PERFORMED: TASK FOR EXTERNAL EXPERTS OF CEEQNET: Finally I am able (on behalf of people from the STAPRO company) to present you with a concise table of the most promising candidates of indicators, which seem to be reasonably constructible from data administered in hospitals of the above countries. We are all totally aware of the biggest draw back, namely the fact that most of these indicators relate to larger hospital facilities on the level of teaching hospitals. Each indicator (measure) in the following table has a vast documentation available on the World Wide Web. All of them have been explicitly defined as well as having the definition of their „construct validity“, strong and weak points, possibilities of distortion, possibility of false motivation and recommendations regarding their use. The following table containing the PQI measures defined in the database of the CEEQNET project should now be submitted to testing. With some of the indicators it should be relatively simple, some will probably present problems relating to mapping of procedures (for example a craniotomy). Performance „Quality“ Indicator SET OF THE CEEQNET PROJECT (5 collaborating countries)
Mortality Rate
Annual Volume
Utilisation Rate ALOS Transfer
Rate AMI PQI A A A HIP Fracture PQI A A A Congestive Heart Failure (CHF) PQI A A A Gastrointestinal (GI) Hemorrhage PQI A A A
Acute Stroke PQI A A A Pneumonia PQI A A A PTCA PQI A A A Pancreatic Resection Mortality Rate PQI PQI A A
Esophageal Resection PQI PQI A A Abdominal Aortic Aneurysm (AAA) Repair PQI A A A
Carotid endarterectomy (CEA) PQI A A A CABG PQI A A A Hip Replacement PQI A A A Craniotomy PQI A A A Laparoscopic Cholecystectomy Rate A A PQI A A Primary Cesarean Delivery Rate A A PQI A A
A = Additional Information Please, start building a repository with materials that will be able to help you produce an „expert volume of text“ relating to the above mentioned measures with regards to: Their construct validity: (this is something we are unable to verify in the CEEQNET project and we will have to rely on literature)

Their transferability: (all of the above measures have been used by AHRQ, we are able to compute them from the data sets of the five collaborating countries, but a very significant volume of the text of the final report has to be devoted to an expert discussion if a measure constructed from data in one healthcare system - and having a certain meaning there - can be used in other healthcare systems, to what extent and with what meaning). The existing threat of bias or distortion: (it would be nice, if you could find examples from your own respective countries relating to the CEEQNET selected measures, documenting that they performed differently (or the same) is in the country where the measures were initially produced. Their potential for “false motivation”: (with respect to quality management systems you work with or you for comfortable with) At this point we would also like you to expertly comment on two other issues:
1. How much do you “feel” – we know this cannot be statistically documented or measured, this is the reason for expert work - that the above defined core measures of the CEEQNET (measures for which we found enough already existing data to construct them) are able to give their “testimony” about the efficiency or quality of provided healthcare in healthcare institutions (hospitals) or how much (and based on what arguments) you might consider such a data set having only the value of “scattered biopsies” from an otherwise obscure and unknown healthcare facility. In other words, how much can such a “bag of measures” be used for assessment and for decisionmaking in the process of management of quality - what could the measures mean for the omnipresent uncertainty of healthcare organization.
2. provide as many as possible examples of potential errors, confounding factors relating
to interpretation, chances for distortion, risks relating to the data collection etc. Finally, please be so kind and provide as with a list of your QUESTIONS that come onto your mind when looking at the result of the list of PQI that form the intersection of data already administered in the hospitals forming a part of the CEEQNET project. We will not be able to produce a thorough analysis for all the measures in the above table, but after the meeting in Budapest this year, we feel, that we will have to make a „extensive comment“ on at least one of the measures – Acute myocardial infarction as is suggested in the following (PLEASE broaden this framework if you have ideas) : As PETER TUMA WROTE Dear CEEQNET colleagues, I am sending you the structure of the formal measurement description. It is a draft, which will be altered, adjusted, explained and completed according your reactions and replies. Please find in attachment also 3 other documents which
1. • might elucidate the sense of some items, listed in the „Formal description“. 2. • could serve as the basis for our later discussions
I’d like to remind that the purpose of this activity is

3. • to find the consensus about the formal description and evaluation of the performance measurement
4. • to describe AMI mortality as a „model description“ 5. • to test then the capacity of the CEEQNET database to meet requirements, issued
from this consensual description Regards Petr Tuma
CEEQNET
Intra-hospital mortality –Acute Myocardial Infarction –
Structured description - DRAFT – 23.4. 2006
Importance; Face validity - Country AMI morbidity a mortality - Country cardiovascular programs - Cross-Country cardiovascular programs
Precision AMI coding - Country instruction for AMI coding - Country practice in AMI coding - Other consideration about AMI coding? Intra-hospital versus time-frame mortality - What is the best time time-frame definition? e.g. 6 month - Is the country difference between intra-hospital and <30 days known?
Country diagnosis coding quality - What is carried out to improve (or maintain) the coding quality?
- Is the coding quality audited? - Other consideration about the diagnosis coding?
Country case principal diagnosis (PD) specification - What is the definition? ...if any - If the correctness of the PD choice audited? Bias Selection bias - Referral and admission criteria bias - Discharge and transfer policy related bias

Risk Adjustment - Any model tested? See attachments Construct validity - Does national AMI standard exist? - Some procedural standards AMI related in use? - Are there some country based pieces of evidence which could contribute to the AMI mortality construct validity?
Prior use - Is the AIM mortality rate used for hospital comparison?
....in whatever form
- Was there an critical attempt to do the international comparison in AIM mortality?
See attachments
Prior use - Is the AIM mortality rate used for hospital comparison?
....in whatever form
- Was there an critical attempt to do the international comparison in AIM mortality?
See attachments
The main result of the CEEQNET project should be a material towards the Commission informing about how a „number“ has to be well defined, how the collection must be scrutinized etc. in order to turn the data into exact information, then how to find relationships between such information clusters to extract any level of KNOWLEDGE to make decisions. Hoping to stay in touch with you and waiting for your reactions Ales Bourek [email protected]

This report was produced by a contractor for Health & Consumer Protection Directorate General and represents the views of thecontractor or author. These views have not been adopted or in any way approved by the Commission and do not necessarilyrepresent the view of the Commission or the Directorate General for Health and Consumer Protection. The EuropeanCommission does not guarantee the accuracy of the data included in this study, nor does it accept responsibility for any use madethereof.