How To Quickly Write, Publish, And Profit From A Book That Will Grow Your Business

EditorialA light at the end of the tunnel 215Ildefonso Rodríguez-Leyva
Original Articles Hyperglycemia is independently associated with decreased survival after aneurysmal subarachnoid hemorrhage in Mexican patients 217Erwin Chiquete-Anaya, José L. Ruiz-Sandoval, Antonio Arauz-Góngora, Fernando Barinagarrementería, Luis M. Murillo-Bonilla, German López-Valencia, Fredy O. González-Pola, Amado Jiménez-Ruiz, Alejandro Gutiérrez-Castillo, Carlos Cantú-Brito, and the PREMIER Investigators
Epidemiological aspects of the risk factors needed to acquire the tapeworm/cysticercosis complex in Mexico 222Juan J. Gómez-Piña and Agnès Fleury
Clinical characteristics of Creutzfeldt-Jakob disease in Mexico: A retrospective analysis 228José A. Choreño-Parra, Francisco J. Pacheco-Sánchez, Alberto I. Rodríguez-Nava, Gabriela García-Quintero, Patricia E. Rodríguez-Muñoz, and Parménides Guadarrama-Ortiz
Review ArticlesEthical implications of shared decision-making in Parkinson’s disease treatment 235Ingrid Estrada-Bellmann and Jesús D. Meléndez-Flores
The time of COVID-19: Clinical approaches and research within 2 months of arriving in Mexico 240Gisela Vázquez-Flores and Marie Catherine Boll
PERMANYERwww.permanyer.com
VOLUME 21 - NUMBER 6 / November-December 2020 – ISSN: 1665-5044
eISSN: 2604-6180
www.revmexneurociencia.com
Revista Mexicana de
NeurocienciaPublicación oficial de la Academia Mexicana de Neurología A.C.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

215
A light at the end of the tunnelUna luz al final del túnel
Ildefonso Rodríguez Leyva*Editor in Chief
Department of Neurology, Faculty of Medicine, Hospital Central “Dr. Ignacio Morones Prieto”, Universidad Autónoma de San Luis Potosí, SLP, Mexico
Revista Mexicana de Neurociencia
EDITORIAL
Correspondence: Ildefonso Rodríguez Leyva
E-mail: [email protected]
Available online: 30-11-2020
Rev Mex Neuroci. 2020;21(6):215-216
www.revmexneurociencia.com
Date of reception: 30-10-2020
Date of acceptance: 03-11-2020
DOI: 10.24875/RMN.M20000081
This year has been very different from all the ones we have had the privilege of living for decades (no mat-ter how many, in the end, they end up being a few). The health situation we have been facing places us in front of multiple questions, some of them with no simple an-swer. Among these, whether this pandemic came from a virus that started spreading from a bat soup or a laboratory, where molecular manipulation generated a deadly weapon to reduce the world’s population. We wonder if the spreading occurred with the mobilization of individuals who crossed borders for family, social, or business travel and whether the possibility of such a problem was already known. The pandemic somehow happened to directly test how the different health-care systems around the world could demonstrate the ability to maintain the population’s health while facing this dis-ease. We questioned whether governments would be able to generate economic and public strategies to maintain security, education, infrastructure, develop-ment, and health in their communities.
This situation has not been straightforward, and its impact will be enormous and prolonged. However, it will be necessary to maintain a positive and adaptive atti-tude before the circumstances that have arisen since it seems that we will continue to face this situation in the new year that is about to begin.
Economically powerful nations are undergoing a need for reconstruction and reorganization, so other countries, such as Latin American, which are still look-ing for political models that will better allow for their development, are struggling even further.
In any case, it is in the medical sphere, to which we have the pleasure of belonging, wherein a daily and simple way that we can contribute to create a better society, albeit with a grain of sand within the ocean’s immensity.
As it turns out, each patient that we treat challenges us, not only in our approach to their diagnosis and treatment but also to educate them and their families to promote the education of other families with whom they have contact.
Those of us who have the opportunity to be university teachers can transmit knowledge that will logarithmical-ly impact society since each student can be a potential educator and shares with many others the knowledge that he or she is acquiring. Those of us who are curious to investigate and search for new realities for publish-ing, transmit new ideas to other generations, which can be evaluated, endorsed, and retransmitted to generate social changes.
It is, however, a massive effort on world’s neurologi-cal society’s side, and sometimes, it may seem as though this effort has little or no impact in a community
1665-5044/ © 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

216
Rev Mex Neuroci. 2020;21(6)
that appears to be more concerned with sports than with the improvements made in health and education. It may also seem like governments that are more con-cerned with having a society that does not question their policies and remains ignorant so that it conforms, and giving “bread and circus” continues to be the strat-egy to keep calm and not fall into social questioning.
We live in a time when we will lose brothers, friends, doctors, teachers, and researchers, in a society that is more concerned with labeling new sexual identities than scientific truths, new justifications for killing than opportunities for healing. Although empathy and soli-darity are maintained, they seem to be diluted in an authoritarian and perverse selfishness of those who hold power, as long as they continue to receive the canonies that come with it regardless of human, cultur-al, social, educational, and scientific losses.
This pandemic has revealed our fragility, but also our selfishness. We speak of defending the poor, but they are the most affected ones, we say to be compassion-ate, but we do not show empathy for the ones who suffer, we speak of sharing, but we continue to be egotistical.
In this year that would appear to be lost, we have had the opportunity to see ourselves, value our daily ac-tions, criticize our governments’ actions, our health-care
system, to compare the difference between public and private health care. We can see the injustice that pre-vails despite the constant offers that those in power profess and that stay that way: mere offerings. We have also had time to evaluate our actions, discover our strengths and accept our weaknesses, and see that plans are left at that, and goals are not being reached in our lives.
Life in the pandemic seems to be more critical be-cause even in social distancing and isolation, we have much left to do for others and ourselves, even if we are not physically near them. After all, digital media pro-vides us with the communication tools and strategies to educate, treat patients, and console when we have nothing more to offer than comfort.
We end a challenging year and begin another one that poses even more significant challenges. Those of us who work on this publication wish each of our readers a year of hope that will culminate in their goals being achieved, offering consolation that will comfort and relieve them, and teachings that will change their attitudes and lives.
This situation is not over yet. We will have to continue working together, even if from afar, to make each other better in generating happier families, a more solidary so-ciety, a more just, safe, healthy, and educated country.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

217
Hyperglycemia is independently associated with decreased survival after aneurysmal subarachnoid hemorrhage in Mexican patientsErwin Chiquete-Anaya1, José L. Ruiz-Sandoval2,3*, Antonio Arauz-Góngora4, Fernando Barinagarrementería5, Luis M. Murillo-Bonilla6, German López-Valencia2, Fredy O. González-Pola7, Amado Jiménez-Ruiz1, Alejandro Gutiérrez-Castillo8,9, Carlos Cantú-Brito1, and the PREMIER Investigators1Department of Neurology, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City; 2Department of Neurology, Hospital Civil de Guadalajara ‘‘Fray Antonio Alcalde’’, Guadalajara, Jalisco; 3Department of the Translational Neurosciences Institute, Centro Universitario de Ciencias de la Salud, Universidad de Guadalajara, Guadalajara, Jalisco; 4Department of Neurology, Stroke Clinic, Instituto Nacional de Neurología y Neurocirugía, Mexico City; 5Department of Neurology, Hospital Ángeles de Querétaro, Querétaro; 6Department of Neurology, Instituto Panvascular de Occidente, Guadalajara, Jalisco; 7Faculty of Human Medicine, Universidad Autónoma de Chiapas, Tuxtla Gutiérrez, Chiapas, Mexico; 8Department of Neurology, Hospital San José, Tecnológico de Monterrey, Nuevo León; 9School of Medicine, Instituto Tecnológico y de Estudios Superiores de Monterrey, Monterrey, Nuevo León, Mexico
Abstract
Background: Hyperglycemia at admission has been recognized as an independent predictor of poor outcome after aneurysmal subarachnoid hemorrhage (aSAH); however, it remains poorly characterized in multivariate models depicting representative population samples. Objective: The objective of the study was to identify if admission blood glucose can independently predict in-hospital mortality after subarachnoid hemorrhage in Mexican patients included in a nationwide multicenter registry. Design/methods: Consecutive patients with aSAH due to ruptured intracranial aneurysm confirmed by 4-vessel angiography were registered in 25 tertiary referral centers from 14 states in Mexico. Multivariate analyses were modeled to find indepen-dent predictors of in-hospital mortality, with adjustment for relevant confounders, using the Hunt-Hess and Fisher scales. Results: A total of 231 patients were studied (66% women; mean age 52 years, range 16-90). Length of hospital stay was a median of 23 days (range 2-98) with in-hospital mortality of 20%, 54% due to a neurological cause. Survival analyses showed a higher probability of death with admittance blood glucose levels in the higher quartile (glycemia > 150 mg/dl) (p < 0.001). Predictors of in-hospital mortality were the Hunt-Hess score > 2 (odds ratio [OR]: 3.79, 95% confidence interval [CI]: 1.43-10.06) and glycemia in the higher quartile (OR: 2.98, 95% CI: 1.12-7.96). Conclusions: Hyperglycemia is an impor-tant independent factor associated with in-hospital mortality. Its early detection and management should be a priority to improve outcomes.
Key words: Glucose, Hyperglycemia. Intracranial aneurysm. Subarachnoid hemorrhage. Outcome.
Correspondence: *José L. Ruiz-Sandoval
E-mail: [email protected]
Available online: 30-11-2020
Rev Mex Neuroci. 2020;21(6):217-221
www.revmexneurociencia.com
Date of reception: 18-03-2020
Date of acceptance: 22-05-2020
DOI: 10.24875/RMN.20000016
1665-5044/ © 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Revista Mexicana de Neurociencia
ORIGINAL ARTICLE
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

218
Rev Mex Neuroci. 2020;21(6)
Introduction
Hyperglycemia is a well-known poor prognostic factor associated with adverse outcomes in neurocritical con-ditions such as ischemic stroke, even in the absence of known diabetes mellitus. However, its contribution as an independent predictor in aneurysmal subarachnoid hemorrhage (aSAH) is limited1,2.
High blood glucose concentration can be present in one-third of patients with aSAH at any given time during hospitalization3-6. Retrospective studies have shown that for every mg increase in glucose over 140 mg/dL, there is an increase in mortality and adverse outcome7. In the present study, we aim to analyze the relationship between blood glucose level at admission and in-hos-pital mortality risk in patients with aSAH.
Materials and methods
Data were obtained from the prospective hospi-tal-based national multicenter RENAMEVASC registry (Registro Nacional de Enfermedad Cerebral Vascular) study where consecutive patients with all stroke types (ischemic and hemorrhagic) were registered over a 2-year period in 25 tertiary referral centers across the country. A total of 2000 patients were studied8,9. For the present analysis, only patients with a diagnosis of aSAH confirmed by 4-vessel angiography were included.
Demographic data, cardiovascular risk factors, clinical presentation at hospital admission (Glasgow Coma Scale and Hunt and Hess scale), radiological character-istics (aneurysm topography by angiography and Fisher score), medical and neurosurgical treatment, in-hospital complications, and final outcome at hospital discharge were also obtained from the original registry8,9.
Blood glucose was measured at hospital admission (using the first blood sample before any intervention) and patients were categorized into two groups depend-ing on blood levels: ≤ 150 mg/ml (≤ 8.3 mmol/l) and > 150 mg/ml (> 8.3 mmol/l). The primary outcome was the association of admission blood glycemia with in-hos-pital mortality. We used the prognostic Hunt-Hess scale, which classifies patients regarding their clinical features using a numbered scale (I to V, asymptomatic to coma-tose, respectively) and the Fisher scale which uses computed tomography scan findings to classify patients (I to IV, no visible blood in imaging study, diffuse or no subarachnoid blood with intracerebral or intraventricular hematoma, respectively) to predict the risk of develop-ing vasospasm as a basis to determine prognosis. Lower scores on the Hunt-Hess and the Fisher scales indicate better prognosis. The study was approved by the ethical committee of every participating center in the study, cataloged as a no risk study with no intervention. Patient information was obtained under previous autho-rization by written consent in all cases.
Hiperglicemia como factor predictor independiente de mayor mortalidad en pacientes mexicanos con hemorragia subaracnoidea aneurismática
Resumen
Antecedentes: La hiperglucemia al ingreso se ha reconocido como un predictor independiente de mal pronóstico después de una hemorragia subaracnoidea aneurismática (HSAA); sin embargo, este hallazgo aún está mal caracterizado en modelos multivariados de población representativa. Objetivo: Identificar si la glucosa en sangre al ingreso hospitalario puede pre-decir de forma independiente la mortalidad hospitalaria después de HSAA en pacientes mexicanos incluidos en un registro multicéntrico nacional. Diseño/métodos: Se registró a pacientes consecutivos con HSA secundaria a un aneurisma intra-craneal roto confirmado por angiografía de cuatro vasos en 25 centros de referencia terciarios de 14 estados en México. Los análisis multivariados se modelaron para identificar predictores independientes de mortalidad hospitalaria, con ajuste por factores de confusión relevantes, mediante las escalas de Hunt-Hess y Fisher. Resultados: Se estudió a un total de 231 pacientes (mujeres, 66%; edad media, 52 años; intervalo, 16-90). La duración de la estancia hospitalaria tuvo una mediana de 23 días (intervalo, 2-98) con una mortalidad hospitalaria del 20%, 54% debido a una causa neurológica. Los análisis de supervivencia mostraron una mayor probabilidad de muerte con los valores de glucosa en sangre en el cuartil superior (glucemia > 150 mg/dl; p < 0.001). Los predictores de mortalidad hospitalaria fueron la puntuación de Hunt-Hess > 2 (OR, 3.79; IC 95%, 1.43-10.06) y la glucemia en el cuartil superior (OR, 2.98; IC95%, 1.12-7.96). Conclusiones: La hiperglu-cemia es un importante factor independiente relacionado con la mortalidad hospitalaria. Su detección y gestión tempranas deben ser una prioridad para mejorar los resultados.
Palabras clave: Glucosa. Hiperglucemia. Aneurisma intracraneal. Hemorragia subaracnoidea. Pronóstico.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

219
E. Chiquete-Anaya, et al.: Hyperglycemia in subarachnoid hemorrhage
Statistical analysis
We grouped patients using quartiles with the following variables: Hunt-Hess scale, Fisher scale, Glasgow Coma Scale, and admission glycemia. Multivariable analyses were modeled to find independent predictors of in-hos-pital mortality, with adjustment for relevant confounders. All cases were evaluated by a neurologist using the Hunt and Hess score for aSAH to determine the mortality risk associated with the severity of the hemorrhage on imag-ing studies and their relation with other individual mortal-ity predictors (including glycemia).
Results
In the original registry, a total of 231 patients (153 [66%] women and 78 [34%] men) were included for analysis. Mean age was 51.8 years (median 51 years, range 16-90). A total of 42% of patients had a prior diagnosis of hypertension and 7% had a history of diabetes mellitus. History of tobacco use was a pres-ent in 35% of patients. Median duration of hospital stay was 23 days (range 2-98). In-hospital mortality oc-curred in 20% of cases; 54% were due to a neurological cause, 28% due to a systemic condition (including in-fection, deep vein thrombosis, pulmonary embolism, and cardiac arrhythmia), and 17% with both.
Of the total o patients, only 219 have a blood glucose test prior any intervention. A total of 55 (25%) patients had a blood glucose level in the upper quartile (> 8.3 mmol/l or > 150 mg/dL) compared with 164 patients (75%) with lower glucose level. Mortality occurred in 50% among patients
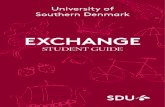
with hyperglycemia. Higher grades in the Hunt-Hess scale (Grades III-V) and Fisher scale (III-IV) were relat-ed to a higher mortality rate (60% and 100%, respec-tively) in comparison with lower grades. A lower score in the Glasgow scale was not related to mortality rate. These subanalyses are shown in table 1. Survival analyses and Kaplan–Meier curves showed a higher probability of in-hospital death with admittance blood glucose level in the higher quartile of the sample (p < 0.001) (Fig. 1). After a binary logistic regression model controlled for clinical and laboratory variables identified at hospital presentation, predictors of in-hos-pital mortality were Hunt-Hess score > 2 (odds ratio [OR]: 3.79, 95% confidence interval [CI]: 1.43-10.06) and glycemia in the higher quartile of the sample (OR: 2.98, 95% CI: 1.12-7.96) (Table 2).
Discussion
Hyperglycemia as a poor prognosis variable in pa-tients with aSAH was first mentioned in 192510. Since then, it has been related to non-neurological systemic complications, delayed vasospasm, cerebral infarction, prolonged in-hospital stay, poor functional outcome, and death. Admittance and perioperative blood glucose have been associated with a poor prognosis after aSAH11. Despite this early observation, the relationship has been scarcely investigated in other studies (Table S1). Hyperglycemia represents the metabolic response to stress12-14 and is associated with a higher risk of vasospasm and secondary ischemia15,16. It is
Table 1. In-hospital mortality based on clinical characteristics and cerebral imaging at hospital admission
Variable Total Gender p value Age (years) p value Intrahospital death p value Multivariate p value
Male Female ≤ 49 ≥ 50 Present Absent
Hunt-Hess scale Grade I-II, n (%)Grade III-V, n (%)
133 (66)69 (34)
51 (74)51 (38)
82 (62)18 (26)
0.09 72 (73)26 (27)
61 (59)43 (41)
0.04 14 (40)21 (60)
119 (71)48 (29)
< 0.001 0.046
Fisher scaleGrade I-II, n (%)Grade III-IV, n (%)
52 (26)149 (74)
17 (25)52 (75)
35 (26)97 (74)
0.8628 (29)68 (71)
24 (23)81 (77)
0.340 (0)
34 (100)52 (31)
115 (69)
< 0.001 0.997
Glasgow Coma Scale13-15, n (%)9-12, n (%)3-8, n (%)
149 (67)43 (19)32 (14)
61 (80)9 (12)6 (8)
88 (59)34 (23)26 (18)
0.00778 (76)12 (11)13 (13)
71 (59)31 (25)19 (16)
0.0117 (39)14 (33)12 (28)
132 (73)29 (16)20 (11)
< 0.001 0.026
Admission glycemia ≤ 150 mg/dl, n (%)> 150 mg/dl, n (%)
164 (75)55 (25)
55 (73)20 (27)
109 (76)35 (24)
0.7084 (43)20 (57)
65 (46)35 (54)
0.05620 (50)20 (50)
144 (80)35 (20)
< 0.001 0.026
aSAH: aneurysmal subarachnoid hemorrhage; CI: confidence interval.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

220
Rev Mex Neuroci. 2020;21(6)
difficult to determine if hyperglycemia is the cause, the consequence or an epiphenomenon related to medical complications such as pneumonia. Therefore, admit-tance blood glucose concentration (before several met-abolic and medical complications occur) could better define the role that hyperglycemia plays in the outcome of patients with SAH, particularly in those with ruptured aneurysms, after controlling for several factors known to affect the outcome in this condition.
Although in-hospital hyperglycemia has been accepted as a well-characterized contributing poor prognostic and death predictor in the neurosurgical critically ill patients, the role of admission glucose levels is not well described in aSAH, remaining poorly characterized in multivariate models of representative population samples13,17-19.
The relationship between hyperglycemia and poor outcomes has been well described in ischemic stroke
and is associated with infarct expansion, worse functional outcome, increased length of hospital stay, and death19-21. Multiple pathophysiological pathways including vascular inflammatory reactions and free rad-ical production lead to cell death and loss of viable brain tissue after stroke22-24. Vasospasm, one of the most feared complications in aSAH related to delayed ischemia and infarction, is present in up to 20% of patients25,26.
Recent studies have demonstrated that elevated blood glucose causes dysregulation of certain enzymes including endothelial nitric oxide (NO) synthase and induced NO synthase. The resulting endothelial dam-age promotes NO depletion and contributes to second-ary vasospasm27. Despite several studies describing the occurrence of hyperglycemia and negative out-comes in aSAH, the association of admission glucose with in-hospital mortality has not been described yet. Our study is the first of its kind in Mexican population to test this hypothesis2-5,7,12,14-20,24,25,28-31.
In our study, we found that the blood glucose levels at admission yield important information on mortality and prognosis. There are several useful scores avail-able that include clinical and radiological information (Hunt-Hess score and Fisher score) which are routinely used as a prognostic tool, but none of them include admission glucose levels. Glucose testing is cheap, readily available, and routinely performed in all centers. Based on these results and the available literature, hyperglycemia should be one of the most critical man-agement targets in patients with aSAH. Regarding the actual evidence, glucose control might help prevent vasospasm and subsequently brain infarct and other in-hospital complications that contribute to the currently poor outcome of this disease32. Early detection and management of hyperglycemia in patients with aSAH should be a primary target in the management of these patients in an effort to improve clinical outcomes.
Conclusions
Hyperglycemia is an important independent risk fac-tor associated with in-hospital mortality and adverse prognosis after aSAH. More prospective controlled studies are required to support these results and de-termine how glucose control might affect mortality and functional prognosis in patients with aSAH. The main limitation of this study is the lack of control of confound-ing factors as the diabetes mellitus disease control status and medication in patients with this diagnosis.
Figure 1. Kaplan–Meier cumulative survival curves in patients with aneurysmal subarachnoid hemorrhage with or without hyperglycemia.
Table 2. Multivariate analysis on factors predicting in-hospital mortality after aSAH: binary logistic regression model
Variable Multivariate odds ratios (95% CI)
p value
Glycemia > 8.3 mmol/l ( > 150 mg/dl) 2.98 (1.12-7.96) 0.03
Hunt-Hess > 2 3.80 (1.43-10.06) 0.007
aSAH: aneurysmal subarachnoid hemorrhage; CI: confidence interval.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

221
E. Chiquete-Anaya, et al.: Hyperglycemia in subarachnoid hemorrhage
Funding
This research has not received any specific grant from agencies in the public, commercial, or non-profit sectors.
Conflicts of interest
None to report.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The au-thors have obtained the written informed consent of the patients or subjects mentioned in the article. The cor-responding author is in possession of this document.
Supplementary data
A systematic review of studies about the association between glycemia and SAH is include in Table S1.
Supplementary data are available at Revista Mexicana de Neurociencia online (www.revmexneuro-ciencia.com/index.php). These data are provided by the corresponding author and published online for the ben-efit of the reader. The contents of supplementary data are the sole responsibility of the authors.
References 1. Hop JW, Rinkel GJ, Algra A, van Gijn J. Case-fatality rates and functio-
nal outcome after subarachnoid hemorrhage: a systematic review. Stroke. 1997;28:660-4.
2. Piironen K, Putaala J, Rosso C, Samson Y. Glucose and acute stroke: evidence for an interlude. Stroke. 2012;43:898-902.
3. Lanzino G, Kassell NF, Germanson T, Truskowski L, Alves W. Plasma glucose levels and outcome after aneurysmal subarachnoid hemorrhage. J Neurosurg. 1993;79:885-91.
4. Juvela S, Siironen J, Kuhmonen J. Hyperglycemia, excess weight, and history of hypertension as risk factors for poor outcome and cerebral infarction after aneurysmal subarachnoid hemorrhage. J Neurosurg. 2005;102:998-1003.
5. Alberti O, Becker R, Benes L, Wallenfang T, Bertalanffy H. Initial hyper-glycemia as an indicator of severity of the ictus in poor-grade patients with spontaneous subarachnoid hemorrhage. Clin Neurol Neurosurg. 2000;102:78-83.
6. Steiner T, Juvela S, Unterberg A, Jung C, Forsting M, Rinkel G. European Stroke Organization guidelines for the management of intracranial aneu-rysms and subarachnoid haemorrhage. Cerebrovasc Dis. 2013;35:93-112.
7. Sayantani G, Saugat D, Mitchell M, Vibbert M, Jallo J. Relationship be-tween serum and csf glucose in subarachnoid hemorrhage. Int J Collab Res Intern Med Public Health. 2012;4:813-8.
8. Ruiz-Sandoval JL, Cantú C, Chiquete E, León-Jiménez C, Arauz A, Muri-llo-Bonilla LM, et al, RENAMEVASC Investigators. Aneurysmal subarach-noid hemorrhage in a Mexican multicenter registry of cerebrovascular di-sease: the RENAMEVASC study. J Stroke Cerebrovasc Dis. 2009;18:48-55.
9. Cantú-Brito C, Ruiz-Sandoval JL, Chiquete E, León-Jimenez E, Muri-llo-Bonilla LM, Villarreal-Carreaga J, et al. Factores de riesgo, causas y pronóstico de los tipos de enfermedad vascular cerebral en México: estudio RENAMEVASC. Rev Mex Neuroci. 2011;12:224-34.
10. Nicolaysen L. Glykosurie bei meningealer blutung. Acta MedScan. 1925;62:392-4.
11. Macdonald RL, Pluta RM, Zhang JH. Cerebral vasospasm after subara-chnoid hemorrhage: the emerging revolution. Nat Clin Pract Neurol. 2007;3:256-63.
12. Mees SM, van Dijk GW, Algra A, Kempink DR, Rinkel GJ. Glucose levels and outcome after subarachnoid hemorrhage. Neurology. 2003;61:1132-3.
13. Helbok R, Schmidt JM, Kurtz P, Hanafy KA, Fernandez L, Stuart RM, et al. Systemic glucose and brain energy metabolism after subarachnoid hemorrhage. Neurocrit Care. 2010;12:317-23.
14. Pérez-Neri I. Relevance of hyperglycemia on the course and outcome of aneurysmal subarachnoid hemorrhage: evidence and mechanisms. In-vest Clin. 2014;55:278-88.
15. Kruyt ND, Roos YW, Mees SM, van den Bergh WM, Algra A, Rinkel GJ, et al High mean fasting glucose levels independently predict poor outco-me and delayed cerebral ischemia after aneurysmal subarachnoid hae-morrhage. J Neurol Neurosurg Psychiatry. 2008;79:1382-5.
16. McGirt MJ, Woodworth GF, Ali M, Than KD, Tamargo RJ, Clatterbuck RE. Persistent perioperative hyperglycemia as an independent predictor of poor outcome after aneurysmal subarachnoid hemorrhage. J Neurosurg. 2007;107:1080-5.
17. Badjatia N, Topcuoglu MA, Buonanno FS, Smith EE, Nogueria RG, Rordorf GA, et al. Relationship between hyperglycemia and symptomatic vasospasm after subarachnoid hemorrhage. Crit Care Med. 2005;33:1603-9.
18. Claassen J, Kreiter KT, Kowalski RG, Du EY, Ostapkovich N, Fitzsim-mons BF, et al. Effect of acute physiologic derangements on outcome after subarachnoid hemorrhage. Crit Care Med. 2004;32:832-8.
19. Frontera JA, Fernandez A, Claassen J, Schmidt M, Schumacher HC, Warternberg K, et al. Hyperglycemia after SAH: predictors, associated complications, and impact on outcome. Stroke. 2006;37:199-203.
20. Al-Khindi T, Macdonald RL, Schweizer TA. Cognitive and functional outco-me after aneurysmal subarachnoid hemorrhage. Stroke. 2010;41:e519-36.
21. Passier PE, Visser-Meily JM, Rinkel GJ, Lindeman E, Post MW. Life satisfaction and return to work after aneurysmal subarachnoid hemorrha-ge. J Stroke Cerebrovasc Dis. 2011;20:324-9.
22. Chan PH, Schmidley JW, Fishman RA, Longar SM. Brain injury, edema, and vascular permeability changes induced by oxygen-derived free radi-cals. Neurology. 1998;34:315-20.
23. Araki N, Greenberg JH, Sladky JT, Uematsu D, Karp A, Reivich M. The effect of hyperglycemia on intracellular calcium in stroke. J Cereb Blood Flow Metab. 1992;12:469-76.
24. Parsons MW, Barber PA, Desmond PM, Baird TA, Darby DG, Byrnes G, et al. Acute hyperglycemia adversely affects stroke outcome: a magnetic resonance imaging spectroscopy study. Ann Neurol. 2002;52:20-8.
25. Crowley RW, Medel R, Dumont AS, Ilodigwe D, Kassel NF, Mayer SA, et al. Angiographic vasospasm is strongly correlated with cerebral infarc-tion after subarachnoid hemorrhage. Stroke. 2011;42:919-23.
26. Nakae R, Yokota H, Yoshida D, Teramoto A. Transcranial Doppler ultra-sonography for diagnosis of cerebral vasospasm after aneurysmal suba-rachnoid hemorrhage: mean blood flow velocity ratio of the ipsilateral and contralateral middle cerebral arteries. Neurosurgery. 2011;69:876-83.
27. Huang YH, Chung CL, Tsai HP, Wu SC, Chang CZ, Chai CY, et al. Hyperglycemia aggravates cerebral vasospasm after subarachnoid he-morrhage in a rat model. Neurosurgery. 2017;80:809-15.
28. Kruyt ND, Biessels GJ, de Haan RJ, Vermeulen M, Rinkel GJ, Coert B, et al. Hyperglycemia and clinical outcome in aneurysmal subarachnoid hemorrhage: a meta-analysis. Stroke. 2009;40:e424-30.
29. Beseoglu K, Steiger HJ. Elevated glycated hemoglobin level and hyper-glycemia after aneurysmal subarachnoid hemorrhage. Clin Neurol Neu-rosurg. 2017;163:128-32.
30. Schmutzhard E, Rabinstein AA, Participants in the International Multi-dis-ciplinary Consensus Conference on the Critical care Management of Subarachnoid Hemorrhage. Spontaneous subarachnoid hemorrhage and glucose management. Neurocrit Care. 2011;15:281-6.
31. Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyper-glycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426-32.
32. Matano F, Fujiki Y, Mizunari T, Koketsu K, Tamaki T, Murai Y, et al. Serum glucose and potassium ratio as risk factors for cerebral vasos-pasm afteraneurysmal subarachnoid hemorrhage. J Stroke Cerebrovasc Dis. 2019;28:1951-7.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

222
Epidemiological aspects of the risk factors needed to acquire the tapeworm/cysticercosis complex in Mexico
Juan J. Gómez-Piña1,2* and Agnès Fleury2,3
1Department of Neurology and Psychiatry, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán; 2Neuroinflammation Unit, Instituto de Investigaciones Biomédicas - UNAM/Instituto Nacional de Neurología y Neurocirugía; 3Neurocysticercosis consultation, Instituto Nacional de Neurología y Neurocirugía. Mexico City, Mexico
Revista Mexicana de Neurociencia
ORIGINAL ARTICLE
Abstract
Introduction: Cysticercosis is still an endemic disease in Mexico, because our country has the main unhealthy conditions to acquire this microorganism, such as the lack of drainage, water, sanitation, and the coexistence with pigs of rustic breeding. Objective: The objective of the study was to evaluate the current prevalence (2015 INEGI database) of risk factors necessary to develop tapeworm/cysticercosis complex and to compare them with the 2010 situation. Materials and methods: The last INEGI database were consulted and compared with the 2010 data, these dates were obtained per state to evaluate the risk factors of states and townships. Results: The current distribution of the 32 Mexico’s states, showed an improvement of water, toilet, drainage, and pigs in housing, compared to the previous data from 2010 database. Conclusions: There was an impro-vement in Mexico’s states, lowering risk factors to acquire tapeworm/cysticercosis complex, although unhealthy conditions still remain in 20 of 32 states of Mexico.
Key words: Cysticercosis. Unhealthy. Mexico. Prevention. Risk factor.
Aspectos epidemiológicos de los factores de riesgo necesarios para adquirir el complejo teniasis/cisticercosis en México
Resumen
Introducción: La cisticercosis sigue siendo una enfermedad endémica en México porque nuestro país cumple con las principales condiciones insalubres para adquirir este microorganismo, como por ejemplo, la falta de drenaje, agua, instalaciones sanitarias y la convivencia con cerdos de cría rústica. Objetivo: Evaluar la prevalencia actual (base de datos INEGI 2015) de los factores de riesgo necesarios para desarrollar el complejo teniasis/cisticercosis y compararlos con la situación de 2010. Métodos: Se consultó la última base de datos INEGI y se comparó con los datos de 2010. Estas fechas se obtuvieron por estado para evaluar los factores de riesgo de los estados y municipios. Resultados: La distribución actual de los 32 estados de México mostró una mejora del agua, el inodoro, el drenaje y los cerdos en las viviendas, en comparación con los datos anteriores de la base de datos de 2010. Conclusiones: Hubo una mejora en los estados de México, disminuyendo los factores de riesgo para adquirir el complejo de teniasis/cisticercosis, aunque aún se mantienen condiciones insalubres en 20 de los 32 estados de México.
Palabras clave: Cistercosis. Insalubre. México. Prevención. Factor de riesgo.
*Correspondence: Juan J. Gómez-Piña
E-mail: [email protected]
Available online: 30-11-2020
Rev Mex Neuroci. 2020;21(6):222-227
www.revmexneurociencia.com
Date of reception: 18-04-2020
Date of acceptance: 11-08-2020
DOI: 10.24875/RMN.20000020
1665-5044/ © 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

223
J.J. Gómez-Piña, A. Fleury: Epidemiological risk factors in México
Introduction
Neurocysticercosis is the most frequent central nervous system (CNS) parasitic disease, being human the only definitive host, while pig is the main interme-diate. Taenia solium causes taeniasis, when adult par-asite is lodged in the small bowel, and cysticercosis, when larval form is lodged in CNS and skeletal muscle.
Neurocysticercosis is still diagnosed frequently in Mexican patients; the Instituto Nacional de Neurología y Neurocirugía, attended 429 new cases from 2000 to 2014, which means 28-29 patients per year in the hospital1-3.
According to the 2005 Sistema Nacional de Vigilan-cia Epidemiológica (SUIVE), the national incidence of taeniasis is up to 0.37%4. Studies made in Mexico sug-gest that 8-13% of pigs are infected with cysticercosis, predominately in Puebla and Guerrero5.
Main risk factors to acquire this infection in Mexico are lack of water, drainage, toilet, and pigs in housing, which are prevalent in most of Mexico’s communities; however, lack of water and/or low quality of it are most important factors to acquire tapeworm/cysticercosis complex in our country, feature which keeps in marginal and rural areas6.
According to the last GLAAS report (UN-Water Global Analysis and Assessment of Sanitation and Drinking-Water) is needed to increase public and free access to quality water, increasing the use of toilet and population`s hygiene in Mexico, especially in marginal, rural or farer areas, where there are susceptible population7.
Previously, we applied the same methodology to 2010 Instituto Nacional de Estadística y Geografía (INEGI) database, considering lack of water, sanitary, drainage, and pigs in housing, obtaining 21 affected states corre-sponding to the 100 first townships affected. Although there was significant correlation between all national townships and Human Development Index (HDI), no significant correlation between just 100 townships and HDI8.
Materials and methods
We consulted the population and housing 2015 IN-EGI census, and agricultural INEGI census, to obtain number of inhabitants, houses with lack of water, houses without drainage, houses without toilet, and number of houses with pigs in housing. These data were considered during the period of 2010-2015,
considering as an inclusion criteria, states, and town-ships with high number of houses with lack of water, houses without drainage, houses without toilet, and houses with pigs in housing. We selected states and townships with highest number or percentage of hous-es meeting these criteria, to be compared with HDI, hypothesizing the highest risk factors the lower HDI. Hence, states and townships were classified to obtain a percentage per township and state, these data were ordered from higher to lower frequency to get risky areas according to Pearson correlation. Moreover, re-sults were graphic in a national map to check the most affected areas in 2015, and compare with 2010 INEGI previous results.
Results
The main townships which meet high risk factors and a low HDI were located in the first quartile of all Mexican townships. This township belongs to all Mexicans states, but just the first 100 townships belonged to 20 of 32 states of Mexico (Table 1), with 2,360,752 (14,074-220,000, IC 95%) of risked habitants, representing a 1.968 % of national population, and 3.094% of risked states population.
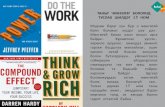
In the other hand, we found that population grown an 8.064% (n = 8,920,678) between 2010 and 2015 ac-cording to INEGI database, representing a 0.154% (n = 13,738) grown of risked population, compared to 2010 analysis (Fig. 1)8. Moreover, the HDI of Mexican states were from 0.667 to 0.79 with a medium HDI of 0.73 (Fig. 2). The state with the higher HDI was Nuevo Leon with 0.79, and the lower HDI was Chiapas with 0.667.
Finally, we compared the HDI with risk factors, hy-pothesized that the higher HDI the lower risk factors, obtaining a significant Pearson correlation with p = 0.01 (R = 0.529), concluding that the most affected state was Guerrero with 7.55% of risked population, and the less affected state was Puebla, with 0.04% of risked popu-lation (Fig. 3).
Discussion
According to our results, the risk factors keeps in the most of areas in Mexico, unfortunately between 2010 and 2015 there were and increasing of 0.154% of risked population, corresponding to 978,834 habitants. These data suggest that risk factors are still remaining in Mexico, but some areas have shown an improve-ment while others did not. The distribution of these
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

224
Rev Mex Neuroci. 2020;21(6)
data (2005-2015) shows us that risk factors to acquire tapeworm/cysticercosis complex are common and prevalent in the most of states of Mexico, which rep-resents the need to implement preventive measures in these states to reduce the incidence of this infection in our country.
Mohit et al. explored Nottinghamshire County Council’s (NCC’s) risk factors, including patients with NCC who used water from unsafe drinking sources, or whom
disposed garbage close to water source, obtaining that there were more slaughter houses and pigs around the houses of NCC patients than the control group9.
We suggest preventive measures as improving the health and hygiene of these areas, as well as imple-menting vaccination in pigs in the areas of greatest impact to eradicate this epidemic, taking into consider-ation that the main risky states are the main states with low population affiliated to health system (Fig. 4).
Table 1. Results of main risked factor’s states, HDI, and population in Mexican analysis
State Municipal population State population Percentage of risk population HDI
Oaxaca 4365 3,967,889 0.110 0.681
Puebla 3084 6,168,883 0.049 0.717
Baja California Sur 1496 712,029 0.210 0.776
Hidalgo 3429 2,858,359 0.119 0.723
Michoacán 46,762 4,584,471 1.020 0.7
Nayarit 6731 1,181,050 0.569 0.733
Querétaro 18,954 2,038,372 0.929 0.76
Chiapas 35,482 5,217,908 0.680 0.667
Aguascalientes 9583 1,312,544 0.730 0.76
Chihuahua 19,207 3,556,574 0.540 0.734
Estado de México 100,366 16,187,608 0.620 0.745
Zacatecas 17,688 1,579,209 1.120 0.72
Colima 18,428 711,235 2.590 0.763
Veracruz 930,019 8,112,505 0.370 0.713
Campeche 17,634 899,931 1.959 0.749
Tamaulipas 84,322 3,441,698 2.450 0.758
Nuevo Leon 160,755 5,119,504 3.140 0.79
Tabasco 453,157 2,395,272 4.306 0.742
San Luis Potosi 162,528 2,717,820 5.980 0.726
Guerrero 266,762 3,533,251 7.550 0.679
Total 2,360,752 76,296,112 1.752 0.7318
Percentage of risk factors according to national population 2015 1.968
Increased of risked population from 2010 to 2015 0.154
Percentage of risked population according to risked states 3.094
Medium HDI 0.731
2015 population (INEGI) 119,938,473
Increased of population in 5 years 8.064N
o p
art
of
this
pu
blic
atio
n m
ay b
e re
pro
du
ced
or
ph
oto
cop
yin
g w
ith
ou
t th
e p
rio
r w
ritt
en p
erm
issi
on
of
the
pu
blis
her
.
© P
erm
anye
r 20
20

225
J.J. Gómez-Piña, A. Fleury: Epidemiological risk factors in México
Figure 2. National Human Development Index (HDI) per states and ascending form (PNUD).
Figure 1. Comparison between 2010 and 2015 analysis, pictured the most affected states in Mexico, as well as transition in dispersion graphics of affected township areas.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

226
Rev Mex Neuroci. 2020;21(6)
Figure 3. Association between HDI and risk factors, showing significant relation between high risk factors with low HDI.
Figure 4. Relationship between population affiliated to health system and risk factors according to our methodology, with no direct relations between the higher risk factor the higher population affiliated to health systems, p = 0.000, Regression, R=0.159.
Conclusions
Comparing the 2010 and 2015 results according to our methodology, we obtained an improvement in risk factors, with a low increasing of affected population, and
a maintenance of HDI in the past 5 years. There were
20 of 32 affected states, compared to the previous anal-
ysis from 2010, with 21 of 32 affected states. Although
there are less affected states, the population in them
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

227
J.J. Gómez-Piña, A. Fleury: Epidemiological risk factors in México
keeps risk factors and unhealthy conditions, which are necessary to acquire tapeworm/cysticercosis complex.
Funding
None.
Conflicts of interest
None.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The au-thors have obtained the written informed consent of the
patients or subjects mentioned in the article. The corre-sponding author is in possession of this document.
References 1. Del Brutto OH, Sotelo J. Neurocysticercosis: an update. Rev Infect Dis.
1988;10:1075-87. 2. Flisser A. Neurocysticercosis in Mexico. Parasitol Today. 1988;4:131-7. 3. Marcin Sierra M, Arroyo M, Cadena Torres M, Ramírez Cruz N, García
Hernández F, Taboada D, et al. Extraparenchymal neurocysticercosis: demographic, clinicoradiological, and inflammatory features. PLoS Negl Trop Dis. 2017;11:e0005646.
4. Sistema Único de Información. Sistema Nacional de Vigilancia Epidemio-lógica Semana 42. Aspectos Relevantes Sobre el Binomio Teniasis/Cisticercosis. México: Sistema Único de Información; 2007.
5. Sciutto CE, Martínez JJ, Villalobos NM, Hernández M, José MV, Beltrán C, et al. Limitations of current diagnostic procedures for the diagnosis of Taenia solium cysticercosis in rural pigs. Vet Parasitol. 1998;79: 229-313.
6. Morales J, Martínez JJ, Rosetti M, Fleury A, Maza V, Hernandez M, et al. Spatial distribution of Taenia solium porcine cysticercosis within a rural area of Mexico. Trop Dis. 2008;2:e284.
7. WHO/UNICEF. Investing in Water and Sanitation: Increasing Access, Reducing Inequalities, UN-Water Global Analysis and Assessment of Sanitation and Drinking-Water (GLAAS) 2014-Report. Geneva: World Health Organization; 2014.
8. Gómez-Piña JJ, Fleury A. Situación actual de los factores de riesgo para el complejo teniosis/cisticercosis en México. Rev Mex Neuroci. 2017;18:34-48.
9. Girotra M, Gera C, Abraham RR, Kaur P, Gauba R, Singh Y, et al. Risk factors for neurocysticercosis: a study from Northwest India. CHRISMED J Health Res. 2014;1:21-4.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

228
Clinical characteristics of Creutzfeldt-Jakob disease in Mexico: A retrospective analysisJosé A. Choreño-Parra1,2, Francisco J. Pacheco-Sánchez1,3,4, Alberto I. Rodríguez-Nava1,3,4, Gabriela García-Quintero1,3,4, Patricia E. Rodríguez-Muñoz1, and Parménides Guadarrama-Ortiz1*1Department of Neurosurgery, Centro Especializado en Neurocirugía y Neurociencias México (CENNM); 2Escuela Nacional de Ciencias Biológicas, Instituto Politécnico Nacional; 3Internado Médico de Pregrado, CENNM; 4Escuela Nacional de Medicina y Homeopatía, Instituto Politécnico Nacional. Mexico City, Mexico
Revista Mexicana de Neurociencia
ORIGINAL ARTICLE
Abstract
Background: Little is known about the clinical characteristics and significance of Creutzfeldt-Jakob disease (CJD) in Mexi-co. Objective: This study aimed to conduct a retrospective revision and analysis of the clinical cases of Mexican patients with CJD available in the literature. Methods: We systematically searched electronic databases for studies in English and Spanish conducted in Mexico over the period of 1990-2020 that involved Mexican patients with any of the clinical forms of CJD. Clinical variables were extracted from the selected studies that met eligibility criteria. Descriptive statistics were used to characterize the study population. Results: A total of seven studies were included in the analysis. From these, 29 cases were revised, and their clinical characteristics analyzed. The median age at the time of diagnosis was 54 years (range 23-75 years). CJD was more frequent among females than male patients (male:female ratio 1:1.41). Most patients resided in Mex-ico City and the State of Mexico, and 93% attended public hospitals. The most frequent form of CJD was sporadic, with only two probable cases of familiar disease. The most common clinical symptoms observed in order or frequency were rapidly progressive dementia (68.9%), cerebellar signs (51.7%), neuropsychiatric symptoms (51.7%), akinetic mutism (51.7%), myoc-lonus (44,8%), extrapyramidal signs (44.8%), visual disturbances (41.3%), pyramidal signs (31%), and sleep disorders (17.2%). Only 20% of the cases were confirmed by histopathological analysis of brain biopsy or autopsy specimens. Conclusions: Our study provides an overview of the main clinical characteristics of CJD in Mexican patients.
Key words: Creutzfeldt-Jakob disease. Prion. Cognitive decline. Rapidly progressive dementia. Spongiform encephalopathy.
Características clínicas de la enfermedad de Creutzfledt-Jakob en México: un análisis retrospectivo
Resumen
Antecedentes: Se sabe poco sobre las características clínicas y la importancia de la enfermedad de Creutzfeldt-Jakob (ECJ) en México. Objetivo: Este estudio tuvo como objetivo realizar una revisión y análisis retrospectivo de los casos clíni-cos de pacientes mexicanos con ECJ disponibles en la literatura. Métodos: Se hizo una búsqueda sistemática en bases de datos electrónicas de estudios en inglés y español realizados en México durante el período de 1990 a 2020, que involucraron
Correspondence: *Parménides Guadarrama-Ortiz
E-mail: [email protected],
Available online: 30-11-2020
Rev Mex Neuroci. 2020;21(6):228-234
www.revmexneurociencia.com
Date of reception: 14-09-2020
Date of acceptance: 14-10-2020
DOI: 10.24875/RMN.20000099
1665-5044/ © 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

229
J.A. Choreño-Parra, et al.: Creutzfeldt-Jakob disease in Mexico
Introduction
Creutzfeldt-Jakob disease (CJD) is the most frequent variant among human spongiform encephalopathies (SE). This rare and invariably fatal neurological disorder is characterized clinically by rapidly progressive dementia, myoclonus, and periodic activity in the elec-troencephalogram (EEG). Such clinical features are as-sociated with a global loss of cerebral tissue due to the spread of an alternative-folded “scrapie prion protein” (PrPSc) within the central nervous system (CNS)1,2. No-tably, CJD is a unique condition that can occur as a sporadic (sCJD), familiar (fCDJ), contagious (vCJD), or iatrogenic (iCJD) disorder depending on the underlying causative mechanism. Nonetheless, the variety of sCJD accounts for about 85% of all CJD cases3,4.
The natural variant of the prion protein (PrPC) has a longitude of 209 amino acids and is codified by the PRNP gene on chromosome 20. This protein, anchored to the surface of neurons, plays several essential roles in the homeostasis of neural cell functions5. PrPC is characterized by a C-terminal region containing a more significant proportion of α–helices than β–sheet struc-tures. This feature provides the protein the properties of being monomeric, soluble, and protease-sensitive. However, several alterations can lead to PrPC to acquire an alternative folding that consists of a gain of β–sheet structures and results in the conversion of PrPC into PrPSc6. In fCJD cases, a wide range of autosomal dom-inant inherited mutations in the PRNP gene makes PrPC more prone to acquire an alternative-folding. In contrast, in the iCJD and vCJD forms, the abnormal PrPSc is transmitted by consumption of contaminated food or iatrogenic exposure to infectious nervous tis-sue, respectively. Once in the brain, PrPSc induces its
self-replication by template conversion of PrPC. On the other hand, the specific cause of spontaneous conver-sion of PrPC into PrPSc in sCJD remains unknown, but a failure of the mechanisms controlling protein folding may be implicated3,7.
At present, the definitive confirmation of CJD is by histopathological analysis of brain biopsy or autopsy specimens. This analysis must show amyloid deposits of PrPSc, astrogliosis, spongiform degeneration, and vacuolization of the neuropil8. In Mexico, there are few reports of CJD, and the real incidence of this and other forms of SE remain unknown. This is due to the clinical heterogeneity of CJD and the lack of awareness of the disease among physicians. Furthermore, the absence of laboratories technically capable of conducting spe-cial cerebrospinal fluid (CSF) studies, and the dimin-ished performance of autopsies has complicated the surveillance concerning CJD. Furthermore, the preva-lence of the distinct forms of CJD and the clinical man-ifestations that more frequently affect Mexican patients with this disorder are unknown.
Here, we performed a comprehensive review of the literature looking for studies of the clinical characteris-tics of Mexican patients with CJD. Our study shows a high frequency of the classic cognitive deficits of CJD in Mexicans, as well as a high frequency of cerebellar manifestations. Furthermore, our analysis reveals a low incidence of this disease in our country that perhaps is underestimated due to several deficiencies in the diag-nostic approach to CJD in health institutions of Mexico. This review may contribute to improving our under-standing of the clinical features of CJD in Mexican patients, which ultimately can generate improvements in the diagnostic approach to this disorder.
a pacientes mexicanos con cualquiera de las formas clínicas de ECJ. Se extrajeron variables clínicas de los estudios selec-cionados que cumplieron con los criterios de elegibilidad. Se utilizó estadística descriptiva para caracterizar la población de estudio. Resultados: Se incluyó un total de siete estudios en el análisis. De estos, se revisaron 29 casos y se analizaron sus características clínicas. La mediana de edad en el momento del diagnóstico fue de 54 años (rango de 23 a 75 años). La ECJ fue más frecuente entre las mujeres que entre los hombres (proporción hombre: mujer 1: 1.41). La mayoría de los pacientes residían en la Ciudad de México y el Estado de México y el 93% acudía a hospitales públicos. La forma más frecuente de ECJ fue esporádica, con solo dos casos probables de enfermedad familiar. Los síntomas clínicos más comunes observados en orden o frecuencia fueron demencia rápidamente progresiva (68.9%), signos cerebelosos (51.7%), síntomas neuropsiquiátricos (51.7%), mutismo acinético (51.7%), mioclonías (44.8%), signos extrapiramidales. (44.8%), alteraciones visuales (41.3%), signos piramidales (31%) y trastornos del sueño (17.2%). Solo el 20% de los casos fueron confirmados por análisis histopatológico de biopsias cerebrales o muestras de autopsias. Conclusiones: En conclusión, nuestro estudio ofrece una visión general de las principales características clínicas de la ECJ en pacientes mexicanos.
Palabras clave: Enfermedad de Cretuzfeldt-Jakob. Prion. Deterioro cognitivo. Demencia rápidamente progresiva. Encefalo-patía espongiforme.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

230
Rev Mex Neuroci. 2020;21(6)
Materials and methods
Search strategy
We systematically searched for studies conducted in Mexico involving non-Caucasian Hispanic patients with any of the clinical forms of CJD. The following electron-ic databases were searched for both published and unpublished studies in the English and Spanish lan-guage over the period of 1990-2020: PubMed, EM-BASE, Web of Science, Scientific Electronic Library Online (SciELO), and Google Scholar. The following terms were used to generate a search: Creutzfeldt-Ja-kob disease, prion, clinical characteristics, clinical fea-tures, Mexico, and Mexican. The selection criteria for papers included: (a) primary research; (b) full-text pa-per in English or Spanish; (c) a general population (e.g., not a single age group or gender); and (d) letters to editor, case reports, case series, cross-sectional, and longitudinal studies. Two reviewers independently per-formed the literature search and screened the abstracts and full text according to these eligibility criteria. The reference list of the included studies was checked to reduce literature omissions.
Data retrieval
The two reviewers who performed the literature search also independently extracted the data from the selected studies. Microsoft Excel (MS Excel 365) was used for data collection. We extracted the following variables: age, gender, state of residence in Mexico, comorbidities, family history of rapidly progressive de-mentia, the clinical variant of CJD (sCJD, fCJD, iCJD, and vCJD), neurological manifestations, the interval between symptoms onset to hospital admission, type of medical care received (public or private), diagnostic tests employed, and category of diagnosis according to the clinical probability of disease (possible, probable, or definitive). Categories of diagnosis were defined fol-lowing the 2018 diagnostic criteria for CJD of the Cen-ters for Disease Control and Prevention (CDC)9, as shown in Table 1.
Data analysis
Descriptive statistics were used to characterize the study population clinically. Frequencies and propor-tions were calculated for categorical data. Means, medians, standard deviations (SD), and interquartile ranges (IQR) were used for continuous variables.
Results
Fifty articles were identified from the searched elec-tronic databases. From these, seven studies met the inclusion criteria and were selected in this review (Table 2)10-16. A total of 29 cases of CJD were reported over the period of 1990-2020 in Mexico. The clinical and demographic data of these cases are summarized in Table 3. The median age reported was 54 years. The youngest and oldest Mexican patients with CJD had 23 and 75 years old, respectively. The disease was more frequent in females (58.62%) than in male (41.37%) patients, with a male to female ratio of 1:1.41. Mexico City and the State of Mexico were the mean regions of patients’ residency, probably reflecting the centraliza-tion of the health-care services rather than the real distribution of CJD in Mexico. The relevant comorbidi-ties most frequently observed among CJD patients were diabetes and hypertension, two medical condi-tions highly prevalent in the Mexican population.
The most common neurological findings of frequency were rapidly progressive dementia, cerebellar signs, neuropsychiatric symptoms, akinetic mutism, myoclo-nus, extrapyramidal signs, visual disturbances, pyrami-dal signs, and sleep disorders. Median of days between disease onsets, defined as the moment when the pa-tients reported the first symptoms, to hospital admis-sion was 64. However, this interval varied from 9 days to 2 years. The most frequent clinical form of CJD was sporadic, with only two cases of probable fCJD. These cases were not confirmed by the demonstration of an inherited mutation in the PRNP gene, but they reported a family history of similar cases in first-degree relatives. There were no reports of iCJD and vCJD in the litera-ture searched. The survival of Mexican patients with CJD could not be estimated since a fraction of the cases was not further followed until death.
According to the 2018 CDC’s criteria for CJD (9), 44.82% of the cases reported in Mexico met the criteria for probable CJD. Meanwhile, 34.48% of patients re-ported can be categorized as possible CJD, and only six patients (20.68%) were considered as definitive cas-es, as they were confirmed by histopathological analy-sis of autopsy brain specimens (Table 4). The majority of Mexican patients with CJD attended public health institutions (93.1%), whereas only two cases received private medical care. EEG was the most frequent diag-nostic tool employed for the diagnostic approach of CJD in Mexican patients, followed by brain magnetic resonance imaging (MRI), CSF levels of 14-3-3 protein, brain single-photon emission computed tomography
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

231
J.A. Choreño-Parra, et al.: Creutzfeldt-Jakob disease in Mexico
Table 2. Studies of CJD in Mexican patients
Author Year Type of study
Number of cases
Reference
Martínez Barros, et al.
1995 Case series 3 10
Calderón-Garcidueñas, et al.
2001 Case report 1 11
Reyes, et al. 2002 Case report 1 12
Velásquez-Pérez, et al.
2007 Case series 15 13
González-Duarte, et al.
2011 Case series 7 14
Restrepo-Martínez, et al.
2019 Letter to editor
1 15
Guadarrama-Ortíz, et al.
2020 Case report 1 16
Table 1. CDC’s Diagnostic criteria for CJD, 2018
Form of CJD Diagnostic subtype
Criteria
Sporadic CJD Definite Diagnosed by standard neuropathological techniques; and/or immunocytochemically; and/or Western blot confirmed protease-resistant PrP; and/or presence of scrapie-associated fibrils.
Probable Neuropsychiatric disorder plus positive RT-QuIC in cerebrospinal fluid (CSF) or other tissuesORRapidly progressive dementia; and at least two out of the following four clinical features:
1. Myoclonus2. Visual or cerebellar signs3. Pyramidal/extrapyramidal signs4. Akinetic mutism
AND a positive result on at least one of the following laboratory tests:− A typical EEG (periodic sharp wave complexes) during an illness of any duration; and/or− A positive 14-3-3 cerebrospinal fluid (CSF) assay in patients with a disease duration of less than 2 years− Magnetic resonance imaging (MRI) high signal abnormalities in caudate nucleus and/or putamen
on diffusion-weighted imaging (DWI) or fluid attenuated inversion recovery (FLAIR)AND without routine investigations indicating an alternative diagnosis.
Possible Progressive dementia; and at least two out of the following four clinical features:1. Myoclonus2. Visual or cerebellar signs3. Pyramidal/extrapyramidal signs4. Akinetic mutismAND the absence of a positive result for any of the four tests above that would classify a case as “probable”AND duration of illness < 2 yearsAND without routine investigations indicating an alternative diagnosis.
Iatrogenic CJD
-- Progressive cerebellar syndrome in a recipient of human cadaveric-derived pituitary hormone; or sporadic CJD with a recognized exposure risk, for example, antecedent neurosurgery with dura mater implantation.
Familiar CJD -- Definite or probable CJD plus definite or probable CJD in a first degree relative; and/or neuropsychiatric disorder plus disease-specific PrP gene mutation.
(SPECT), and histopathological analysis. Only one case was tested for special CSF studies, such as levels of T-tau protein16. Furthermore, 18-fluorodeoxyglucose
positron emission tomography (18FDG-PET) was per-formed in one patient15. Finally, only one case was confirmed by a real-time quaking-induced conversion (RT-QuIC) test16, a novel technique with the highest diagnostic performance to detect minimal amounts of PrPSc in CSF samples17.
Discussion
The knowledge about the incidence, clinical charac-teristics, and epidemiological significance of CJD in Mexico is limited. Our study aimed to retrospectively revise and analyze available reports about the main manifestations of CJD in Mexican patients. A striking finding of our analysis was the low amount of cases from Mexico formally described in the literature. Indeed, only 29 patients with CJD have been reported over the past three decades in our country, which is <1 case/year. This finding undoubtedly reflects a high grade of underreporting and sub-diagnosis of CJD cases in Mexicans. For instance, if we took the global incidence of sCJD as a reference (1 case per million people per
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

232
Rev Mex Neuroci. 2020;21(6)
Table 3. Demographic and clinical characteristics of CJD cases reported in Mexico
Characteristic n = 29 (%)
Age (years), median (range) 54 (23-75)
Gender MaleFemaleMale: female ratio
12 (41.37)17 (58.62)
1: 1.41
Place of residenceMexico CityState of MexicoOther States*Not reported
11 (37.93)6 (20.68)7 (24.13)4 (13.79)
Type of diagnosisDefinitiveProbablePossible
6 (20.68)13 (44.82)10 (34.48)
Clinical CJD formsCJDfCJD**iCJDvCJD
26 (89.65)2 (6.89)
00
Clinical featuresRapidly progressive dementiaMyoclonusAkinetic mutismVisual disturbancesCerebellar signsPyramidal signsExtrapyramidal signsSleep disordersNeuropsychiatric symptoms(depression, anxiety, behavioral changes)Symptoms onset to hospital admission interval (days), median (range)Family history of rapidly progressive dementia
20 (68.96)13 (44.82)15 (51.72)12 (41.37)15 (51.72)9 (31.03)
13 (44.82)5 (17.24)
15 (51.72)
64 (9-730)
2 (6.89)
Relevant comorbiditiesDiabetesHypertensionCancer
3 (10.34)4 (13.79)1 (3.44)
Type of medical carePublic carePrivate care
27 (93.1)2 (6.89)
*Hidalgo, Sonora, Veracruz, Michoacán, Morelos, Jalisco, Coahuila. **Individuals with a family history of rapidly progressive dementia but no confirmation of inherited mutations in the PRNP gene (probable fCJD).
Table 4. Diagnostic approach to CJD in Mexico
Public hospital care(n = 27) (%)
Private hospital care
(n = 2) (%)
Total(n = 29) (%)
MRI 20 (74.07) 2 (100) 22 (75.86)
EEG 26 (96.29) 2 (100) 27 (93.1)
SPECT 7 (25.92) 0 7 (24.13)
18FDG-PET 1 (3.7) 0 1 (3.44)
CSF 14-3-3 protein 14 (51.85) 2 (100) 16 (55.17)
CSF Tau protein 0 1 (50) 1 (3.44)
CSF RT-QuIC 0 1 (50) 1 (3.44)
Histopathological analysis
6 (22.22) 0 6 (20.68)
CSF: cerebrospinal fluid, EEG: electroencephalogram, MRI: magnetic resonance imaging, RT-QuIC: real time quaking-induced conversion test, SPECT: single photon emission computed tomography, 18-fluorodeoxyglucose positron emission tomography.
year)3, then the expected number of CJD cases occur-ring in Mexico would be much higher.
These data are in part due to the rarity and unspecific manifestations of CJD. In this sense, it is well recog-nized that rapidly progressive dementia is not a unique characteristic of this disease. In fact, many other neu-rological disorders can be confused with CJD, including some variants of Alzheimer disease (AD), dementia with Lewy bodies (DLB), frontotemporal dementia
(FTD), viral, bacterial, parasitic, or autoimmune meningoencephalitis (e.g., Hashimoto’s encephalitis, and limbic encephalitis), corticobasal degeneration, progressive supranuclear palsy, paraneoplastic en-cephalomyelitis, and even vascular dementia18,19. Fur-thermore, a wide range of other clinical manifestations, such as pyramidal/extrapyramidal dysfunction, ataxia, cerebellar signs, psychiatric symptoms, visual distur-bances, sleep disorders, akinetic mutism, and per-sistent painful sensory symptoms, may be present among patients with CJD1, adding complexity to the clinical spectrum of the disease. This fact led physi-cians to subclassify various forms of CJD according to the mean symptoms, including the classic (dyskinetic), Heidenhain (visual), myoclonic, cerebellar (ataxic), tha-lamic, amyotrophic, and panencephalopathic forms4,7.
Furthermore, it is, currently, well known that, in the specific case of sCJD, the clinical heterogeneity is also associated with some genetic and molecular features of the pathogenic PrPSc. Specifically, methionine (M) or valine (V) polymorphism at codon 129 of the PRNP gene20, as well as the type of electrophoretic mobility pattern of PrPSc after protease digestion (type 1 and 2), are used to classify patients into several phenotypes separated into three categories: sCJD cognitive sub-types (MM1, MV1, MM2, and VV1), ataxic subtypes (VV2 and MV2), and other non-sCJD subtypes (types 3 and 4 electrophoretic mobility for sporadic fatal in-somnia (sFI) and variably protease-sensitive prionopa-thy (VPSPr), respectively)4,7. Each category has unique
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

233
J.A. Choreño-Parra, et al.: Creutzfeldt-Jakob disease in Mexico
characteristics differing from the others in age at onset, duration of the disease, dominant neurological findings, and among others. However, the age at onset of all CJD cases ranges from 50 to 70 years with no predi-lection for any gender.
The polymorphisms in the PRNP gene that determine the susceptibility for the development of sCJD are dif-ferentially distributed among various populations around the world21-24. However, the frequency of M129V genotypes and alleles in the Mexican population has not been addressed. Our results confirm that sCJD is the most frequent variant of this disease in Mexicans. Furthermore, there are only two cases of probable fCJD not confirmed by the demonstration of an inher-ited mutation in the PRNP gene. There is no registry of any case of acquired CJD through iatrogenic expo-sure or contagion, but there are cases in very young patients, and the wide range of interval between dis-ease onset to hospital admission opens the possibility of the occurrence of vCJD/iCJD among Mexican indi-viduals. We also observed that rapidly progressive de-mentia, akinetic mutism, and myoclonus were among the most common symptoms observed in Mexican CJD patients. Furthermore, neuropsychiatric symptoms were frequently reported, although only one case was formally categorized as a Heidenhain variant of CJD15. These data indicate that the sCJD cognitive subtypes are common in Mexicans with this disease. Thus, we can predict that the underlying genetic and molecular traits of these phenotypes (MM1, MV1, MM2, and VV1) would be frequent in our population.
Interestingly, we found a high number of patients with CJD that presented cerebellar symptoms (51.72%), in-cluding ataxia. The frequency of cerebellar affection in CJD patients from other regions has not been compre-hensively estimated. In a study conducted in the United Kingdom, cerebellar ataxia occurred as the only clinical manifestation in 5% of patients with CJD25. In contrast, in a study of Chinese patients with CJD, up to 51.9% of affected individuals presented cerebellar ataxia26, which coincides with our findings. Thus, based on our results, we also predict that the genetic and molecular characteristics of the PrPSc underlying ataxic subtypes of sCJD (VV2 and MV2) may have a high incidence in Mexico.
The variable clinical characteristics of CJD compli-cate the diagnostic approach and opportune detection of positive cases. Furthermore, the low level of clinical suspicion among physicians and the absence of a for-mal surveillance strategy may further contribute to the underestimation of the burden of CJD in the Mexican
population. To improve the diagnosis and global surveillance of CJD, the CDCs have established sev-eral diagnostic criteria that classify each case accord-ing to the likelihood of the disease based on clinical features and the results of different laboratory and im-aging tests9. Possible and probable categories are based on clinical symptoms and positive results in EEG, MRI, and CSF 14-3-3. Most such studies have high specificity but low sensitivity, and it is important to mention that their diagnostic reliability varies according to the CJD form and even to the sCJD subtype27.
EEG recording in patients with sCJD typically shows pseudo-periodic sharp-wave complexes (PSWC) with diffuse slowly background activity at the middle and late stages of the disease. The diagnostic value of EEG is due to its 64% sensitivity and 91% specificity28. On the other hand, MRI has shown to have better diagnostic performance due to improvements in the DWI se-quence29. MRI does not allow to distinguish between clinical forms of CJD, but in cases of vCJD, a posterior thalamus involvement (pulvinar sign) supports the di-agnosis30. CSF levels of neuron-specific enolase (NSE) and T-tau protein have also been proposed as biomark-ers of CJD. From these, T-tau protein has the highest sensitivity and specificity with a cutoff of 1150pg/mL31. However, CSF levels of T-tau protein have not been integrated into the 2018 CDC’s diagnos-tic criteria for CJD.
Notably, in the last decade, RT-QuIC has emerged as a novel alternative for premortem diagnosis of CJD with better performance compared with other CSF tests. This assay relies on the in vitro template conver-sion of recombinant PrPC into PrPSc, evidenced through a fluorescent indicator, allowing to detect minute amounts of PrPSc in biological samples with high sen-sitivity and specificity17. Indeed, we recently reported the first case of a Mexican patient with sCJD confirmed by a complete battery of diagnostic tests, including EEG, MRI-DWI, CSF levels of T-tau, and 14-3-3 protein, as well as CSF RT-QuIC, which allowed us to detect this case premortem (16). In such a report, we demon-strated an excellent correlation between the results of the RT-QuIC test and other clinical and laboratory pa-rameters. Despite this, RT-QuIC is not considered as a diagnostic tool that can classify a patient as a defin-itive case of CJD by the CDCs. Thus, the definitive diagnosis of CJD is still based on the histopathological analysis of brain biopsy and autopsy specimens.
Our study reveals concerning data about the diag-nostic approach to CJD in our country. First, we ob-served that only 20% of cases were confirmed by
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

234
Rev Mex Neuroci. 2020;21(6)
histopathology. The definitive confirmation of CJD in Mexicans was exclusively performed in public health-care institutions. More specific and sophisticated imaging and CSF tests were rarely performed in public hospital care, and they were carried out in laboratories outside Mexico, even in cases diagnosed at private hospitals. These facts must claim the attention of na-tional health-care authorities to make the efforts need-ed to create laboratories with the technical capacity to perform special CSF studies and to introduce new tests that allow confirming CJD in Mexico, such as the RT-QuIC test.
Conclusions
Our study provides an overview of the main clinical characteristics of CJD in Mexican patients. Also, our study reveals that the incidence of CJD in our country could be higher than supposed. Finally, we remarked several deficiencies in the diagnostic approach to this neurological disorder in our country that needs the attention of the Mexican authorities of health. Our findings should motivate Mexican physicians and researchers to get involved in the surveillance and im-provement of diagnosis of the disease
Funding
The current study did not receive financial support.
Conflicts of interest
The authors declare that they have not conflicts of interest.
Acknowledgments
The authors would like to thank the medical and nursing staff of our center, for their critical reading and comments on our manuscript.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The au-thors declare that no patient data appear in this article.
References 1. Prusiner SB. The prion diseases. Brain Pathol. 1998;8:499-513. 2. Prusiner SB. Novel proteinaceous infectious particles cause scrapie.
Science. 1982;216:136-44. 3. Chen C, Dong XP. Epidemiological characteristics of human prion disea-
ses. Infect Dis Poverty. 2016;5:47. 4. Imran M, Mahmood S. An overview of human prion diseases. Virol J.
2011;8:559. 5. Castle AR, Gill AC. Physiological functions of the cellular prion protein.
Front Mol Biosci. 2017;4:19. 6. Prusiner SB. Prions. Proc Natl Acad Sci U S A. 1998;95:13363-83. 7. Kovacs GG, Budka H. Molecular pathology of human prion diseases. Int
J Mol Sci. 2009;10:976-99. 8. Budka H. Neuropathology of prion diseases. Br Med Bull. 2003;66:121-30. 9. Centers for Disease Control and Prevention. CDC’s Diagnostic Criteria
for Creutzfeldt-Jakob Disease (CJD); 2018. Available from: https://www.cdc.gov/prions/cjd/diagnostic-criteria.html.
10. Barros MM, Peek JR, Vega R, Escobar A. Creutzfeldt-Jakob disease. Clinical, electrophysiological and histopathological correlations. Gac Med Mex. 1995;131:591-6.
11. Calderón-Garcidueñas AL, Sagastegui-Rodríguez JA, Canales-Ibarra C, Fa-rías-García R. A case of Creutzfeldt-Jakob in the Mexican North-East and review of current concepts on prion disease. Gac Med Mex. 2001;137:589-94.
12. Reyes MT, Aguilar S, Corona R, Vega I, Colón CM, Ramos GG. Enfer-medad de Creutzfeldt-Jakob: reporte de un caso y revisión de la litera-tura. Med Sur. 2002;9:79-87.
13. Velásquez-Pérez L, Rembao-Bojorquez D, Guevara J, Guadarrama-To-rres RM, Trejo-Contreras A. Creutzfeldt-Jakob disease in Mexico. Neu-ropathology. 2007;27:419-28.
14. González-Duarte A, Medina Z, Balaguer RR, Calleja JH. Can prion di-sease suspicion be supported earlier? Clinical, radiological and laboratory findings in a series of cases. Prion. 2011;5:201-7.
15. Restrepo-Martínez M, Chacón-González J, Oñate-Cadena N, Bayliss L. Neuropsychiatric symptoms in the Heidenhain variant of Creutzfel-dt-Jakob’s disease mistaken for major depression and functional neuro-logical disorder. Aust N Z J Psychiatry. 2019;53:1222-3.
16. Guadarrama-Ortíz P, Choreño-Parra JA, Carnalla-Cortés M, Rodrí-guez-Muñoz PE, Ángeles-Castellanos M. A complete and state of the art pre-mortem diagnostic approach to Creutzfeldt-Jakob disease: a case report. Neurol India. 2020;68:1-3.
17. Orrú CD, Groveman BR, Hughson AG, Zanusso G, Coulthart MB, Cau-ghey B. Rapid and sensitive RT-QuIC detection of human Creutzfel-dt-Jakob disease using cerebrospinal fluid. mBio. 2015;6:e02451-14.
18. Paterson RW, Torres-Chae CC, Kuo AL, Ando T, Nguyen EA, Wong K, et al. Differential diagnosis of Jakob-Creutzfeldt disease. Arch Neurol. 2012;69:1578-82.
19. Mead S, Rudge P. CJD mimics and chameleons. Pract Neurol. 2017;17:113-21. 20. Saba R, Booth SA. The genetics of susceptibility to variant Creutzfel-
dt-Jakob disease. Public Health Genomics. 2013;16:17-24. 21. Lee SM, Ju YR, Choi BY, Hyeon JW, Park JS, Kim CK, et al. Genotype
patterns and characteristics of PRNP in the Korean population. Prion. 2012;6:375-82.
22. Saetta AA, Michalopoulos NV, Malamis G, Papanastasiou PI, Mazmanian N, Karlou M, et al. Analysis of PRNP gene codon 129 poly-morphism in the Greek population. Eur J Epidemiol. 2006;21:211-5.
23. Yu SL, Jin L, Sy MS, Mei FH, Kang SL, Sun GH, et al. Polymorphisms of the PRNP gene in Chinese populations and the identification of a novel insertion mutation. Eur J Hum Genet. 2004;12:867-70.
24. Erginel-Unaltuna N, Peoc’h K, Komurcu E, Acuner TT, Issever H, Laplan-che JL. Distribution of the M129V polymorphism of the prion protein gene in a Turkish population suggests a high risk for Creutzfeldt-Jakob disea-se. Eur J Hum Genet. 2001;9:965-8.
25. Cooper SA, Murray KL, Heath CA, Will RG, Knight RS. Sporadic Creut-zfeldt-Jakob disease with cerebellar ataxia at onset in the UK. J Neurol Neurosurg Psychiatry. 2006;77:1273-5.
26. Qi C, Zhang JT, Zhao W, Xing XW, Yu SY. Sporadic Creutzfeldt-Jakob disease: a retrospective analysis of 104 cases. Eur Neurol. 2020;83:65-72.
27. Forner SA, Takada LT, Bettcher BM, Lobach IV, Tartaglia MC, Torres-Chae C, et al. Comparing CSF biomarkers and brain MRI in the diagnosis of spora-dic Creutzfeldt-Jakob disease. Neurol Clin Pract. 2015;5:116-25.
28. Wieser HG, Schindler K, Zumsteg D. EEG in Creutzfeldt-Jakob disease. Clin Neurophysiol. 2006;117:935-51.
29. Fujita K, Harada M, Sasaki M, Yuasa T, Sakai K, Hamaguchi T, et al. Multicentre multiobserver study of diffusion-weighted and fluid-attenuated inversion recovery MRI for the diagnosis of sporadic Creutzfeldt-Jakob disease: a reliability and agreement study. BMJ Open. 2012;2:e000649-e.
30. Zeidler M, Sellar RJ, Collie DA, Knight R, Stewart G, Macleod MA, et al. The pulvinar sign on magnetic resonance imaging in variant Creutzfel-dt-Jakob disease. Lancet. 2000;355:1412-8.
31. Hamlin C, Puoti G, Berri S, Sting E, Harris C, Cohen M, et al. A compa-rison of tau and 14-3-3 protein in the diagnosis of Creutzfeldt-Jakob di-sease. Neurology. 2012;79:547-52.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

235
Ethical implications of shared decision-making in Parkinson’s disease treatmentIngrid Estrada-Bellmann1* and Jesús D. Meléndez-Flores2
1Department of Internal Medicine, Movement Disorders Clinic, Neurology Division, University Hospital “Dr. José E. González”; 2Faculty of Medicine. Universidad Autónoma de Nuevo León, Nuevo León, Monterrey, Mexico
Revista Mexicana de Neurociencia
REVIEW ARTICLE
Abstract
Shared decision-making (SDM) involves an active participation of the patient in deciding treatment choice, based on his/her preferences, beliefs, and values. In the context of Parkinson’s disease (PD), physicians encounter limitations in applying this model related to cognitive decline and other disease-related complications. Discussing the ethics of this approach on the context of these limitations the PD patient suffers is thus of great importance. This review intends to analyze ethical challen-ges of SDM in PD related to decision-making capacity, surrogates’ role in patient’s identity, and patients’ and physicians’ preferences. Although skepticism could arise when dealing with surrogates’ decisions, a key for flourishing the patient’s autonomy is acknowledging its relational context, as relatives’ beliefs and values are imprinted in the patient’s identity. To do so, empathy should be encouraged in physicians, recognizing the different value attribution that patients and their relatives have in the decision process.
Key word: Cognition. Parkinson disease. Shared decision-making. Surrogate decision maker.
Implicaciones éticas de la toma de decisiones compartida en el tratamiento de la enfermedad de Parkinson
Resumen
La toma de decisiones compartida (TDC) implica una participación activa del paciente en la decisión del tratamiento, en función de sus preferencias, creencias y valores. En el contexto de la enfermedad de Parkinson (EP), los médicos encuentran limitaciones al aplicar este modelo relacionado con el deterioro cognitivo y otras complicaciones relacionadas con la enfer-medad. Discutir la ética de este enfoque en el contexto de estas limitaciones que sufre el paciente con EP es, por lo tanto, de gran importancia. Esta revisión tiene la intención de analizar los desafíos éticos de la TDC en la EP relacionados con la capacidad de toma de decisiones, el rol del tomador de decisiones sustituto en la identidad del paciente y las preferencias de los pacientes y médicos. Aunque podría surgir escepticismo al tratar con las decisiones de los sustitutos, una clave para el florecimiento de la autonomía del paciente es reconocer su contexto relacional, ya que las creencias y valores de los familiares están impresos en la identidad del paciente. Para hacerlo, se debe alentar la empatía en los médicos, or recono-ci-endo la diferente atribución de valor que los pacientes y sus familiares tienen en el proceso de decisión.
Palabras clave: Cognición. Enfermedad de Parkinson. Toma de decisiones compartida. Tomador de decisiones sustituto.
Correspondence: *Ingrid Estrada-Bellmann
E-mail: [email protected]
Available online: 30-11-2020
Rev Mex Neuroci. 2020;21(6):235-239
www.revmexneurociencia.com
Date of reception: 21-04-2020
Date of acceptance: 28-09-2020
DOI: 10.24875/RMN.20000022
1665-5044/ © 2020. Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

236
Rev Mex Neuroci. 2020;21(6)
Introduction
Shared decision-making (SDM) has been a topic broadly discussed in medicine, where ultimately the shift from paternalistic toward more patient-centered care is being more encouraged. The ideal of SDM in-volves patients and physicians discussing treatment options based on patients’ values, beliefs, and prefer-ences, reaching a consensual decision1,2. The ethical guidelines of this approach rely on the principles of bioethics: patient’s autonomy, beneficence, non-malef-icence, and justice. In the neurology field, especially Parkinson’s disease (PD), physicians encounter limita-tions when trying to apply this approach, this related to the cognitive decline and other complications that most PD patients suffer in advanced stages3. This leads to physicians questioning SDM applicability in reassuring what is best for the patient, tending to revert to a pa-ternalistic approach4.
This review aims to analyze ethical challenges relat-ed to SDM in the context of PD patients through anal-ysis of decision-making capacity, autonomy, and surro-gates, and medical and patients’ preferences in the treatment context.
Decision-making capacity in PD patients: an obstacle for SDM
For a decision to be made, this must have been con-sent. This implies that patients had to be informed, choose voluntary, and had the competence to decide5. Problems arise with the population suffering neurode-generative diseases, such as Alzheimer’s and PD, as the cognitive decline over years makes physicians question their decision-making capacity. In fact, studies evaluating this capacity in PD patients with cognitive impairment have found that, compared to controls, this population has deficits in this decision-making pro-cess3,6-10. Furthermore, within this capacity, domains affected mostly are understanding, reasoning, and ap-preciation, but no differences arise from choice8,11. This means that a patient later on advanced stages could express a decision that is against his former way of reasoning and be additionally detrimental, thus making the physician, who has followed him/her along the pro-gression of the disease, question, and put aside his/her preferences and consider weighing the principle of non-maleficence over autonomy.
On the other side, a study on non-demented nor cognitive impaired PD patients showed no differences in decision capacity compared to healthy controls12.
The main problem regarding this study lies on the prevalence of cognitive impairment in newly diagnosed PD patients, which is over 20%13. Hence, to ensure SDM in all stages of the disease, this implies the ethical need of awareness and screening for decision capacity in patients even at the first stages of the disease. More-over, as the cognitive decline in PD follows a progres-sive course14,15, focus has been attributed on determin-ing the existence of a window period of maximum decision capacity16. This is critical in the SDM process as this period can be used for (1) the physician to get to know the patients’ preferences, values, and beliefs related to treatment and (2) the family could be educat-ed in the process of becoming a surrogate deci-sion-maker alongside patient and physicians to ensure preferences are aligned.
PD patients with cognitive impairment or dementia suffer problems in understanding, reasoning, and ap-preciation areas of decision capacity. However, not all decisions are based on reasoning or logic. Some are made by applying values, emotions, needs, and hab-its17,18. Moreover, critics on the traditional approach of decision capacity assessment argue that this is more cognitive based, whereas emotional factors are left aside19-21. This has ethical considerations, as emotions and values are basic for human experience and for the acquisition of knowledge22, so a question arises: is it ethical to accept a cognitive impaired PD patient’s de-cision when this is based only on values or emotions? As these non-cognitive factors form part of the patient’s identity, if the non-maleficence principle is not infringed, autonomy principle must be respected. Nonetheless, this has two considerations (1) this might collide with what the physician thinks is best for the patient (benef-icence principle). Here is where SDM and physicians’ empathy toward patients’ values comes into play, as this increases participation23, and acknowledges differ-ences in value attributions. Moreover, (2) as the patient is a social being, his/her identity is influenced by his interactions with others, implicating a role of a third party in the decision-making process.
Surrogate decision-making in advanced PD: the role of the third party
As the disease progresses, and PD patients are in-competent to decide for themselves, the individual ap-proach to autonomy urges for advance care directives to be implemented24,25, where explicit patient wishes are heard and taken into consideration, and no interference of third parties is desired. However, problems arise with
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

237
I. Estrada-Bellmann, J. D. Meléndez-Flores: Shared decision-making in Parkinson’s
this approach. Only a few percentage of patients under-take these directives26, and it may seem impossible to foresee all the possible clinical scenarios in practice27. Moreover, a patient’s literal statement may be vague or prompt to different interpretations from relatives or phy-sicians28. Nonetheless, the main problem with this view-point of autonomy is that it views a patient as an isolated individual making an isolated decision, when he/she forms part of a social context, where interactions and interdependency with others are inevitable. Thus, surro-gate decision-makers come into play, keeping PD pa-tient’s preferences at the center of the process.
When contemplating the patient as a social being, his/her identity is thus seen as being influenced by others in a social trade-off. In this manner, the society’s and family’s values, beliefs, and preferences are im-printed in this identity. Van Nistelrooij et al. expressed this view as relatives being coeditors of the patient’s identity, shifting the concept of autonomy to a relational context29. Consequently, choices regarding health problems are not to be seen as individual, but rather involving the help of the third parties, as these may aid the patient in showing an insight into his/her past, and present, being thus part of the decision-making pro-cess25,30. Following this logic, surrogate decision-mak-ers, when being close relatives to the patient, constitute a door to patient’s values and preferences, making a substituted judgment. However, a systematic review on accuracy of surrogates’ decisions showed that these incorrectly predict patient’s preferences in one-third of cases31. Furthermore, another study showed that sur-rogates rely on other factors such as their best interest or mutual interest32, making physicians question the validity of the decision taken by these substitutes.
Nonetheless, a study showed that patients, when be-ing unable to decide for themselves, weighed more heavily the loved ones’ input than physicians’ input33. This could be understood as patients acknowledging relatives’ influence on their decision, as they share mu-tual interests, values, and beliefs. In fact, some articles share the idea that one’s personal interests are not only self-centered, but other’s centered34-37, adapting prefer-ences according to intimates’ wishes38. Rather than seeing this as a threat to the intrinsic value of autonomy, physicians should be aware of the relational context of this concept and aid surrogates on taking the best de-cision for the patient, pledging at all time to the benefi-cence principle. This implies that the decision, instead of being delegated completely to the family, is being shared by physicians and the latter, in a substituted interests model39, where the clinical expertise and
experience of the physicians, along with the knowledge of the PD patient’s values and preferences from the surrogates’ viewpoint, aid define the particular interests of the patient in a particular clinical scenario, fulfilling the patient’s full autonomy and fulfilling the beneficence principle. Sharing this decision implies from an ethical view that medical judgment reassures all bioethical prin-ciples are being considered, while relieving the emotion-al burden that surrogates may experience.
Physicians and patients’ preferences: the need for empathy
As new treatment modalities arise in PD, a physician might feel necessary to change to device-aided thera-peutics, such as deep brain stimulation, subcutaneous apomorphine pump, or levodopa-carbidopa intestinal gel infusion, to improve motor or non-motor function, weighing harms, and benefits for their implementation. However, physicians may weigh these differently com-pared to patients40, and their pledge toward maximizing benefit might impede listening what patients really want. A study showed that some PD patients focused more on optimizing the process of care, while others focused on improving motor symptoms41. Furthermore, another study concluded that PD patients might not want to un-dergo advanced treatments to obtain health improve-ments, as they might feel adapted to their current situ-ation42. The latter could surprise physicians, and these could be prompted to question this decision, trying to convince patients of a specific treatment based on po-tential benefits, tending to an unwarranted paternalistic approach. The key to change this urge of paternalism dressed in the physician’s mind as beneficence is em-pathy. That is, in the SDM process, the physician should try to understand what the patient wants and what is more important for him/her based on his/her needs, placing his/her autonomy, in a relational context as dis-cussed previously, as central for the decision process. Moreover, involving the patient in the decision-making process goes beyond ethical issues, as a study showed that PD patients who are involved have more treatment adherence43. In this manner, interventions aimed at as-sessing and improving empathy process should be im-plemented not only in neurological residencies, but rath-er in all medical residency programs throughout all years, as a study showed that self-evaluated empathy in medical residents declines at the end of their training programs44. By implementing educational programs that have proven useful in increasing empathy levels among medical residents and students45,46, the formation of
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

238
Rev Mex Neuroci. 2020;21(6)
future specialists that acknowledge the need of placing the patient’s preferences, needs, and interests on the front line could be reassured.
Conclusion
From the diagnosis and first encounter of a PD patient, assessing his or her decision capacity must be an eth-ical imperative for physicians, as in SDM, patient’s pref-erences are determining in modeling the conduct physi-cians would take for future encounters. That being said, medical judgments and patients’ preferences are not two opposing poles, where the physician calls on his/her expertise and experience, and questions decisions that diverge from his/her viewpoint, as this is implicitly an act of paternalism that leaves the patient’s autonomy aside. Rather, through empathy, these two should align toward the same direction from the first encounter, as this goes beyond ethical manners, improving quality of patient care. Moreover, in PD, as the patient’s decision capacity decreases, the inclusion of family members as surro-gates is vital, as they provide an insight into the patient’s preferences, beliefs, and interests, being part of the patient’s identity. In this manner, the physicians, bearing into mind the patient’s beliefs and preferences, discuss with family members and share their expertise toward what’s best for the patient in a circumstance, and by doing so, fulfill the patients’ autonomy at all time.
This review proposes that it is not about questioning the patient’s autonomy in PD and considering the phy-sicians’ judgment as better grounded, but rather, with the help of the family members, promote the under-standing of the preferences and interests of the patient, reaching to a shared decision that places autonomy in the center of the decision.
Funding
This research has not received any specific grant from agencies in the public, commercial, or non-profit sectors.
Conflicts of interest
None.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The au-thors declare that no patient data appear in this article.
References 1. Charles C, Gafni A, Whelan T. Shared decision-making in the medical
encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44:681-92.
2. Barry MJ, Edgman-Levitan S. Shared decision making-the pinnacle of patient centered care. N Engl J Med. 2012;366:780-1.
3. Herz DM, Bogacz R, Brown P. Neuroscience: impaired decision-making in Parkinson’s disease. Curr Biol. 2016;26:R671-3.
4. Driever EM, Stiggelbout AM, Brand PL. Shared decision making: physi-cians’ preferred role, usual role and their perception of its key compo-nents. Patient Educ Couns. 2020;103:77-82.
5. Grisso T, Appelbaum P. Assessing Competence to Consent to Treat-ment: a Guide for Physicians and Other Health Professionals. New York: Oxford University Press; 1998.
6. Karlawish J, Cary M, Moelter ST, Siderowf A, Sullo E, Xie S, et al. Cog-nitive impairment and PD patients’ capacity to consent to research. Neu-rology. 2013;81:801-7.
7. Martin RC, Okonkwo OC, Hill J, Griffith HR, Triebel K, Bartolucci A, et al. Medical decision-making capacity in cognitively impaired Parkinson’s disease patients without dementia. Mov Disord. 2008;23:1867-74.
8. Griffith HR, Dymek MP, Atchison P, Harrell L, Marson DC. Medical de-cision-making in neurodegenerative disease: mild AD and PD with cog-nitive impairment. Neurology. 2005;65:483-5.
9. Brand M, Labudda K, Kalbe E, Hilker R, Emmans D, Fuchs G, et al. Decision-making impairments in patients with Parkinson’s disease. Behav Neurol. 2004;15:77-85.
10. Dymek MP, Atchison P, Harrell L, Marson DC. Competency to consent to medical treatment in cognitively impaired patients with Parkinson’s disease. Neurology. 2000;56:17-24.
11. Abu Snineh M, Camicioli R, Miyasaki JM. Decisional capacity for advan-ced care directives in Parkinson’s disease with cognitive concerns. Par-kinsonism Relat Disord. 2017;39:77-9.
12. Eygelshoven S, van den Hout A, Tucha L, Fuermaier A, Bangma D, Thome J, et al. Are non-demented patients with Parkinson’s disease able to decide about their own treatment? Parkinson Relat Disord. 2017; 38:48-53.
13. Muslimovic D, Post B, Speelman JD, Schmand B. Cognitive profile of patients with newly diagnosed Parkinson disease. Neurology. 2005;65:1239-45.
14. Stepkina DA, Zakharov VV, Yakhno NN. Cognitive impairments in pro-gression of Parkinson’s disease. Neurosci Behav Physiol. 2010;40:61-7.
15. Muslimovic D, Post B, Speelman JD, De Haan RJ, Schmand B. Cogniti-ve decline in Parkinson’s disease: a prospective longitudinal study. J Int Neuropsychol Soc. 2009;15:426-37.
16. Okonkwo OC, Griffith HR, Copeland JN, Belue K, Lanza S, Zamrini EY, et al. Medical decision-making capacity in mild cognitive impairment: a 3-year longitudinal study. Neurology. 2008;71:1474-80.
17. Mozley CG, Huxley P, Sutcliffe C, Bagley H, Burns A, Challis D, et al. Not knowing where I am doesn’t mean I don’t know what I like: cognitive impairment and quality of life responses in elderly people. Int J Geriatr Psychiatry. 1999;14:776-83.
18. Karel MJ, Gurrera RJ, Moye H, Moye J. Reasoning in the capacity to make medical decisions: the consideration of values. J Clin Ethics. 2010;21:58-71.
19. Hermann H, Trachsel M, Elger BS, Biller-Andorno N. Emotion and value in the evaluation of medical decision-making capacity: a narrative review of arguments. Front Psychol. 2016;7:765.
20. Charland LC. Is Mr. Spock mentally competent? Competence to consent and emotion. Philos Psychiatr Psychol. 1998b;5:67-81.
21. Banner NF. Can procedural and substantive elements of decision-making be reconciled in assessments of mental capacity? Int J Law Context. 2013;9:71-86.
22. van de Lagemaat R. Theory of Knowledege for the IB Diploma. 2nd ed. Cambridge: Cambridge University Press; 2015.
23. Kirkscey R. Bioethical communication: shared decision-making and rela-tional empathy. J Commun Healthc. 2018;11:164-74.
24. Silveira MJ, Kim SY, Langa KM. Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362: 1211-8.
25. Donchin A. Understanding autonomy relationally: toward a reconfigura-tion of bioethical principles. J Med Philos. 2001;26:365-86.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

239
I. Estrada-Bellmann, J. D. Meléndez-Flores: Shared decision-making in Parkinson’s
26. Perkins HS. Controlling death: the false promise of advance directives. Ann Intern Med. 2007;147:51-7.
27. Sudore RL, Fried TR. Redefining the planning in advance care planning: preparing for end-of-life decision making. Ann Intern Med. 2010;153:256-1.
28. Fagerlin A, Schneider CE. Enough: the failure of the living will. Hastings Cent Rep. 2004;34:30.
29. Van Nistelrooij I, Visse M, Spekkink A, de Lange J. How shared is shared decision-making? A care-ethical view on the role of partner and family. J Med Ethics. 2017;43:637-44.
30. Dove ES, Kelly SE, Lucivero F, Machirori M, Dheensa S, Prainsack B. Beyond individualism: is there a place for relational autonomy in clinical practice and research? Clin Ethics. 2017;12:150-65.
31. Shalowitz DI, Garrett-Mayer E, Wendler D. The accuracy of surrogate decision makers: a systematic review. Arch Intern Med. 2006;166:493-7.
32. Vig EK, Taylor JS, Starks H, Hopley EK, Fryer-Edwards K. Beyond substituted judgment: how surrogates navigate end-of-life decision-ma-king. J Am Geriatr Soc. 2006;54:1688-93.
33. Nolan MT, Hughes M, Narendra DP, Sood JR, Terry PB, Astrow AB, et al. When patients lack capacity: the roles that patients with terminal diagnoses would choose for their physicians and loved ones in making medical decisions. J Pain Symptom Manage. 2005;30:342-53.
34. Ho A. Relational autonomy or undue pressure? Family’s role in medical decision-making. Scand J Caring Sci. 2008;22:128-35.
35. Walter JK, Ross LF. Relational autonomy: moving beyond the limits of isolated individualism. Pediatrics. 2014;133:S16-23.
36. Lolich L, Lynch K. No choice without care: palliative care as a relational matter, the case of Ireland. Soundings. 2017;100:353-74.
37. Gómez-Vírseda C, de Maeseneer Y, Gastmans C. Relational autonomy: what does it mean and how is it used in end-of-life care? A systematic review of argument-based ethics literature. BMC Med Ethics. 2019;20:76.
38. Azoulay E, Chaize M, Kentish-Barnes N. Involvement of ICU families in decisions: fine-tuning the partnership. Ann Intensive Care. 2014;4:37.
39. Sulmasy D, Snyder L. Substituted interests and best judgments: an inte-grated model of surrogate decision making. JAMA. 2010;304:1946-7.
40. Mühlbacher AC, Juhnke C. Patient preferences versus physicians’ jud-gement: does it make a difference in healthcare decision making? Appl Health Econ Health Policy. 2013;11:163-80.
41. Weernink MG, van Til JA, van Vugt JP, Movig KL, Groothuis-Oudshoorn CG, IJzerman MJ. Involving patients in weighting benefits and harms of treat-ment in Parkinson’s disease. PLoS One. 2016;11:e0160771.
42. Weernink MG, van Til JA, Groothuis-Oudshoorn CG, IJzerman MJ. Pa-tient and public preferences for treatment attributes in Parkinson’s disea-se. Patient. 2017;10:763-72.
43. Grosset KA, Grosset DG. Patient-perceived involvement and satisfaction in Parkinson’s disease: effect on therapy decisions and quality of life. Mov Disord. 2005;20:616-9.
44. Foreback J, Kusz H, Lepisto BL, Pawlaczyk B. Empathy in internal me-dicine residents at community-based hospitals: a cross-sectional study. J Med Educ Curric Dev. 2018;5:1-4.
45. Kelm Z, Womer J, Walter JK, Feudtner C. Interventions to cultivate physician empathy: a systematic review. BMC Med Educ. 2014;14:219.
46. Batt-Rawden SA, Chisolm MS, Anton B, Flickinger TE. Teaching empathy to medical students: an updated, systematic review. Acad Med. 2013; 88:1171-7.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

240
The time of COVID-19: Clinical approaches and research within 2 months of arriving in MexicoGisela Vázquez-Flores and Marie Catherine Boll*Clinical Research Laboratory, Ataxias, Choreas and Other Rare Diseases, Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez”, Mexico City, Mexico
Revista Mexicana de Neurociencia
REVIEW ARTICLE
Abstract
By the end of 2019, a peculiar epidemic appeared in China; it was of the flu-type and revealed a lethal zoonosis caused by a beta coronavirus. In this study, we review the history of this new pandemic starting from its origin; we describe how COVID-19 spread its symptoms, especially the neurological ones, and the investigations currently underway.
Key words: COVID-19. SARS-CoV-2. Symptoms. Diagnostic tests. Clinical trials.
Tiempos de COVID-19: aproximaciones clínicas e investigaciones en dos meses desde su llegada en México
Resumen
A finales del 2019 surgió en China una peculiar epidemia de tipo gripal, que reveló ser una zoonosis letal causada por un betacoronavirus. Revisamos en este artículo la historia de la ahora pandemia desde su origen, describimos los síntomas, especialmente los neurológicos, y las investigaciones actualmente en curso.
Palabras claves: COVID-19. SARS-CoV-2. Síntomas. Pruebas diagnósticas. Ensayos clínicos.
Correspondence: *Marie Catherine Boll
E-mail: [email protected]
Available online: 30-11-2020
Rev Mex Neuroci. 2020;21(6):240-244
www.revmexneurociencia.com
Date of reception: 27-05-2020
Date of acceptance: 29-07-2020
DOI: 10.24875/RMN.20000049
Introduction
By the end of 2019 in Wuhan, pneumonia of unknown etiology emerged. A new kind of betacoronavirus was identified when only two beta-coronaviruses were asso-ciated with respiratory syndromes in humans: Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV). The new virus was called SARS-CoV-2 by the International Committee of Virus Taxonomy. Howev-er, significant differences were found in transmission,
pathogenesis, and clinical presentation between the new virus and the other SARS-CoV.
The surge of a new strain
The attendance to the Chinese Spring Festival im-plied the rapid mobilization of infected persons. The first five studied patients presented high fever and dry cough and four developed respiratory distress. Subsequently, a study in 137 patients concluded that middle-aged and
1665-5044/ © 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

241
G. Vázquez-Flores, M.C. Boll: The time of COVID-19
elderly subjects with comorbidities have a poorer prog-nosis1. Next, angiotensin-converting enzyme-2 (ACE2) was identified as a SARS-CoV-2 receptor. ACE2 ex-pression has been found in kidneys, intestines, gallblad-der, nervous system, and placenta. In lungs, the target organ, it was much lower. On the other hand, ACE2 was strongly expressed in proximal tubules. Thirty-six of 536 patients presented acute renal failure 20 days after the onset, even though baseline creatinine levels were normal2.
Clinical manifestations
Mainly respiratory, a dry cough accompanied by fever and mild constitutional symptoms is present in the first phase of the viral response (stage I). Then, shortness of breath without or with hypoxia corresponds to the moderate phase or pulmonary involvement, when pa-tients develop viral pneumonia and when an abnormal chest computed tomography (CT) scan can be useful for rapid diagnosis to optimize management. A 3-stage classification and establishment of a standardized no-menclature were recently proposed for reporting the disease and orienting therapeutic interventions. In-deed, in stage II, the host’s inflammatory response in-creases until it reaches hyper inflammation in stage III with acute respiratory distress syndrome, systemic in-flammatory response syndrome, and cardiac failure ac-companied by the peak of pro-inflammatory cytokines, troponin, and NT-proBNP elevation. At this time, corti-coid or immunomodulatory treatments can be beneficial3.
SARS-CoV-2 can affect other systems and cause abdominal pain, diarrhea, vomit, anorexia, acute renal failure, and a series of symptoms considered as neu-rological: dizziness, headache, consciousness impair-ment, acute cerebrovascular disease, ataxia, seizures, peripheral nervous system damage consisting of ocu-lomotor palsy, the frequent anosmia/ageusia, other neuropathies, and also myalgias. In the mild phase of coronavirus disease (COVID)-19, an interplay between pro-inflammatory cytokines and chemokine release, in-creased endothelial damage, and potential sepsis in-duces coagulopathy development. It is known that the cytokine storm, macrophage activation, leukocyte ad-hesion molecule overexpression, together with the marked expression of ACE2 in the vascular endotheli-um, makes it a clear target of the disease. Therefore, COVID-patients are at risk of thrombogenesis due to both biochemical hypercoagulable state and direct vas-cular damage. A major neurological manifestation is
ischemic stroke involving large vessels, often in multi-ple vascular territories and associated with elevated D-dimer, ferritin, anticardiolipin, and phospholipid antibodies4.
The mechanism of neuroinvasion has not been elucidated, though it could be due to a direct infec-tion by SARS-CoV-2 as part of acute toxic encepha-litis or by axonal transport through the olfactory sys-tem. The presence of viral particles in olfactory epithelium has been related to anosmia, an initial symptom that can persist until the moderate phase. The most severe phase of hyper inflammation threats the integrity of the blood-brain barrier. Toll-like recep-tors activation in microglia and astrocytes may ex-plain the association with encephalitis, encephalomy-elitis, acute necrotizing encephalopathy, meningitis, transverse myelitis, and acute cerebellar inflamma-tion. Furthermore, post-infectious and immune medi-ate neurological complications are described, includ-ing Guillain-Barré syndrome and its variants that usually appear in the moderate and severe phases and some rare cases of acute disseminated enceph-alomyelitis-like encephalomyelitis4.
SARS-CoV-2 was isolated in cerebrospinal fluid from two patients with meningoencephalitis but not in nasal swabbing. One of them underwent severe dis-order of consciousness; the other presented seizures. Previously, pediatric cases with Kawasaki-type vascu-litis have been reported in New York. The first case, a 6-month infant had fever, tachycardia, tachypnea, irritability, conjunctivitis, and cracked lips. On day 5, the infant exhibited maculopapular exanthema and edema in limbs. Diagnosed with Kawasaki disease (KD) and immunoglobulin therapy was initiated. Eight pediatric English patients with KD showed shock signs; one died after ischemic strokes, and seven ex-hibited right heart ventricular failure. These latter im-proved after Immunoglobulin therapy and antibiotic treatment5.
The arrival of the pandemic in Mexico
The first case of COVID-19 in Mexico, a 35-year-old male subject returning from Bergamo, Italy, was con-firmed on February 28, while an increase in the number of cases in Western Europe was evident. Subsequently, preventive measures were taken such as avoiding physical contact and massive events (Table 1). On March 24, 405 cases were confirmed and phase 2 im-plemented with homeschooling and home-office during the quarantine (Fig. 1). At the beginning of April, a
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

242
Rev Mex Neuroci. 2020;21(6)
sharp rise in the contagion curve took place, but it was until April 21 that phase 3 of the pandemic was de-clared so as 857 deaths (Fig. 2).
Current research (Table 2)
After sequencing genetic material of SARS-CoV-2 (RNA), the first RT-polymerase chain reaction (PCR) diagnostic tests were developed. It has a sensitivity range of 56%-83% and specificity of 95%. The pres-ence of the virus in aerosols and surfaces was then studied. SARS-CoV-2 remains in aerosols for 3 h and 8 h in copper; it is not found in carton after 24 h, but it is more stable on stainless steel for 48 h and on plastic with a viability of 72 h6. After PCR diagnostic test, se-rological tests were settled. A French laboratory devel-oped a fast one called NG-Test IgG-IgM COVID-19 All-in-One that detects and differentiates antibodies against SARS-CoV-2 in blood. This test was carried out in 101 patients with COVID-19 and rendered a positive result in 95% on day 157.
In Mexico, the laboratory Lansbiodyt at the UNAM University is developing a biomarker detecting magnet-ic pearls that bind to the RNA of SARS-CoV-2 virus and send a fluorescent signal measured with a versatile biomolecule sensor. This method can detect a small viral load and is currently under validation.
Research on the control of hypoxic complications led to a clinical study in France on Arenicola marina, given that hemoglobin from this marine worm can transport 40 times more oxygen than the human one and is compatible with all human blood groups. The company Hemarina intends to use this hemoglobin for treating COVID-19. The study began in 10 patients with severe COVID-19 and on ventilators, but on April 19, the trial was stopped by the French Security
Agency of Medicaments. In this same country, a study using hydroxychloroquine administered with azithromycin was carried out in 36 COVID-subjects when admitted to hospital. It was an open clinical trial. Main criticisms on this research are the risk of QT lengthening in the electrocardiogram and the low level of evidence, though the outcome was rather promising8.
Another therapeutic possibility is ivermectin, an anti-parasitic with potent antiviral activity toward HIV and dengue. In a study in Vero/hSLAM cells infected with SARS-CoV-2, a 5 mM of ivermectin treatment showed after 24 h, that viral RNA was reduced by 93% in the supernatant. At 72 h, no remnant could be detected9. However, the dose utilized in Vero cells is 35 times higher than the Cmax allowed in human plasma after oral administration of the approved dose of ivermectin. At present, there is still no evidence of the efficacy of this drug in treating patients with COVID-19.
In the UK, RECOVERY, a randomized controlled trial, announced preliminary results in 2104 patients that showed that dexamethasone reduced significantly the 28-day mortality rate with the greatest benefit among those patients requiring mechanical ventilation but also in patients who only received oxygen therapy.
Among other therapeutic options, mesenchymal stem cells are expected to control the exacerbated immune response exhibited by patients. After cell transplantation, ten patients improved significantly in 2-4 days, PCR levels were low, also inflammatory cy-tokines diminished and chest CT showed a reduction in lung infiltration on the 9th day10. Meanwhile, an epi-demiologic study in 175 countries shows a significant reduction in morbidity and mortality from COVID-19 in countries with BCG vaccine as part of their individual policy13.
Figure 1. Empty avenue in Mexico City during April 2020 contingency. Photo bequeathed by DRONERO.MX.
Figure 2. Global death curves starting after the 6th death. Record as far as May 12, 2020 in ciencias.unam.mx/lansbiodyt/contacto with permission.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

243
G. Vázquez-Flores, M.C. Boll: The time of COVID-19
Table 2. Relevant ongoing research in March and April 2020
Type of study Sample size References
NG-Test IgM-IgG COVID All-in-One detects specific antibodies anti-SARS-CoV-2 of IgG and IgM types in blood, serum, or plasma, producing results in 15 min. Positive outcome from day of infection to day 15 (p = 0.001)
Development of serologic test
101 patients Dortet et al. 20207
Lansbiodyt Laboratory at the University of Mexico (UNAM) develops a biomarker that binds to SARS-CoV-2 virus and emits a quantifiable fluorescent signal at low cost. Project UNAM-INDRE-001
Diagnostic test 40 patients. On hold until financing is available
UNAM 202012
Hydroxychloroquine and azithromycin as treatment for COVID-19 patients. It reduces viral load in PCR assay in nasopharyngeal swabbing (p < 0.001)
Non-randomized clinical trial
36 patients Gautret et al. 20208
Countries with BCG vaccine as part of their individual policy show reduction in morbidity and mortality in patients with COVID-19 (p = 0.0001, and p = 0.05, respectively)
Epidemiologic study in cases and controls
175 countries Ozdemir et al. 202013
Antiparasitic Ivermectin reduces the viral load in Vero cells infected with SARS-CoV-2 assayed by RT-PCR
In vitro study 10 simulations Caly et al. 20209
Transplant of mesenchymal stem cells ACE2 reduces inflammation in patients with pneumonia caused by COVID-19 (p < 0.05)
Clinical trial 10 patients Leng et al. 202010
Patients administered Remdesivir show a 2-point clinical improvement on a 1-6 scale after 10 days, with viral load reduction
Randomized clinical trial (pilot study)
237 patients Wang et al. 202014
Patients treated with 200 mL of plasma from convalescent patients of COVID-19 show significant clinical, biochemical, and radiologic improvement
Open trial 10 patients Duan et al. 202015
IgG and IgM antibodies target receptor S binding dominion (S-RBD) of SARS-CoV-2 and select it as humoral immunity target to become the aim for the development of vaccines
Pre-clinical phase and Phase 1
12 patients Ni et al. 202016
Table 1. Control and prevention interventions of COVID-19 in different scenarios11
Scenarios 1. Viral importDozens of cases
2.-Community dispersionHundreds of cases
3.- EpidemicThousands of cases
Greeting between people No restriction No kiss, no hug No kiss, no hug
Closed public spaces (theaters, stadiums, cinemas, etc.)
Not necessary Suspension of events before outbreaks
Suspension of events before outbreaks
Open public spaces (malls, parks, beaches)
Not necessary Suspension of events before outbreaks
Suspension of events before outbreaks
Schools, high schools and universities
Dissemination of preventive messages
School filter Suspension of classes in schools during active outbreak
Workplaces Dissemination of preventive messages
Sanitary filter Suspension of work activities in workplaces during active outbreak
Another study in 10 severely ill COVID-19 patients explored the administration of plasma from recovered patients. This procedure significantly improved symp-tomatology and viral load15.
Vaccine research has been undertaken in different countries, reaching relatively advanced stages such as
the recently published clinical trial with AD5-nCOV. One hundred eight healthy individuals received low (0.5 mL), medium (1.0 mL), or high (1.5 mL) doses of Ad5 vec-tored COVID-19 vaccine; 83% in low and medium doses and 75% in high doses reported mild or moderate ad-verse reactions consisting of pain in the injection site,
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

244
Rev Mex Neuroci. 2020;21(6)
fever, fatigue, headache, and myalgia. ELISA and neu-tralizing antibodies increased significantly from day 14 and specific T-cell response was rapidly reached17.
In Mexico, ten patients with COVID-19 were partici-pating in a clinical study to test the efficacy of remde-sivir. On May 12, 9 out of 10 patients had been discharged and the antiviral clearly showed significant shortening in the course of the disease.
Conclusion
Similarly to COVID-19, research to fight the mortal agent will take quite a while. This pandemic has shown that we are facing a virus capable of disrupting global economy in a few months and draws attention to human fragility as was experienced in the big epidemics of antiquity, Middle ages, or the more recent Spanish Flu. Within a vicious circle, the economic and health repercussions slow down research progress at the risk of having to live the effects of SARS-CoV-2 for a long time. The whole world awaits the teachings of mass testing and the arrival of a vaccine. Furthermore, neurological manifestations that could be classified as early and systemic, neuroinvasion, and post-infectious immune-mediated have very diverse pre-sentations and mechanisms that remain to be clarified.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The au-thors declare that no patient data appear in this article.
References 1. Liu K, Fang YY, Deng Y, Liu W, Wang MF, Ma JP, et al. Clinical charac-
teristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin Med J. 2020;133:1025-31.
2. Deng YY, Zheng Y, Cai GY, Chen XM, Hong Q. Single-cell RNA sequen-cing data suggest a role for angiotensin-converting enzyme 2 in kidney impairment in patients infected with 2019-nCoV. Chin Med J. 2020;133:1129-31.
3. Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppres-sed states: a clinical-therapeutic staging proposal. J Heart Lung Trans-plant. 2020;39:405-7.
4. Koralnik IJ, Tyler KL. COVID-19: a global threat to the nervous system. Ann Neurol. 2020;88:1-11.
5. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. 2020;395:1607-8.
6. Van Doremalen N, Bushmarker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020;382:1564-67.
7. Dortet L, Emeraud C, Vauloup-Fellous C, Khecharem M, Ronat JB, Fortineau N, et al. Rapid determination of SARS-CoV-2 antibodies using a bedside, point-of-care, serological test. Emerg Microbes Infect. 2020; 24:1-32.
8. Gautret P, Lagier JC, Parola P, Hoang VT, Meddeb L, Mailhe M, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: re-sults of an open-label non-randomized clinical trial. Int J Antimicrob Agents. 2020;2020:105949.
9. Caly L, Druce JD, Catton MG, Jans DA, Wagstaff KM. The FDA approved drug Ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antiviral Res. 2020;178:104787.
10. Leng Z, Zhu R, Hou W, Feng Y, Yang Y, Han Q, et al. Transplantation of ACE2-mesenchymal stem cells improves the outcome of patients with COVID-19 pneumonia. Aging Dis. 2020;11:216-28.
11. Secretaría de Salud. COVID-19 Comunicado Técnico Diario. Lunes 9 de marzo de 2020. Available at: https://www.gob.mx/cms/uploads/attachment/file/540170/COVID-19_-_Comunicado_Tecnico_Diario_2020.03.09.pdf
12. Desarrollan en la UNAM biosensor para detección rápida de COVID-19. Boletín UNAM-DGCS-343/2020. Accessed March 17, 2020. Available at https://www.dgcs.unam.mx/boletin/bdboletin/2020_343.html.
13. Ozdemir C, Kucuksezer UC, Tamay ZU. Is BCG vaccination effecting the spread and severity of COVID-19? Allergy. 2020;75:1824-7.
14. Wang Y, Zhang D, Du G, Du R, Zhao J, Jin, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020;395:1569-78.
15. Duan K, Liu B, Li C, Zhang H, Yu T, Qu J, et al. Effectiveness of conva-lescent plasma therapy in severe COVID-19 patients. Proc Natl Acad Sci USA. 2020;117:9490-96.
16. Ni L, Ye F, Cheng ML, Feng Y, Deng, YQ, et al. Detection of SARS-CoV-2-specific humoral and cellular immunity in COVID-19 convalescent indi-viduals. Immunity. 2020;52:971-77.
17. Zhu FC, Li YH, Guan XH, Hou LH, Wang WJ, Li JX, et al. Safety, tole-rability, and immunogenicity of a recombinant adenovirus Type-5 vecto-red COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial. Lancet. 2020;395:1845-54.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020