Restraint and Seclusion Updates 2014 Annual Nursing Sandy Wade RN, CNS.
31
Restraint and Seclusion Updates 2014 Annual Nursing Sandy Wade RN, CNS
-
Upload
ashley-shepherd -
Category
Documents
-
view
212 -
download
0
Transcript of Restraint and Seclusion Updates 2014 Annual Nursing Sandy Wade RN, CNS.

Restraint and SeclusionUpdates
2014 Annual Nursing
Sandy Wade RN, CNS

Regulatory Reminders
• PRN restraint orders are not allowed.
When a restraint order is received, it is understood that restraint will be applied immediately, or has already been applied emergently. If the order is not carried out at that time, it becomes void.
• A “restraint break ” is not allowed, other than for patient care activities with a staff member in the room.– It is not permissible for family members to remove restraints for any
reason.– If the staff member leaves the room while the patient is un-restrained,
it is considered that restraints have been discontinued. A new order will be required if they are re-applied.

Indications for RestraintTerminology varies with the regulatory agency - The Joint Commission (TJC) or the
Centers for Medicare & Medicaid Services (CMS)
“Behavioral Health” (TJC) “Violent” (CMS)
Behavioral health care reasons for the use of restraint or seclusion are primarily to protect
the patient against injury to self or others because of an emotional or behavioral disorder.
“The use of restraint and seclusion for behavior management is not specific to the treatment
setting, but to the situation the restraint is being used to address.” (OLOL Policy OrgClin/036)
“Non-Behavioral Health” (TJC) “Non-violent” (CMS)
The restraint standards for medical or surgical purposes apply when the primary reason for use directly supports medical healing.
Commonly referred to as “Med-Surg” restraints

Tips for De-escalation of Aggressive/Disruptive Behavior
• Remain calm
• Speak in a soft voice
• Be aware of your body language (Where are your hands?)
• Position self in a supportive stance (Not confrontational)
• Set clear, concise & enforceable limits
• Be an empathetic listener (Not judgmental)
• Do not feign attention
• Practice silence
• Repeat & reflect on what was said

Alternatives to RestraintsAttempt these measures before applying restraints:
•Treat delirium•Offer distraction (eg, TV, toy to occupy hands, magazine to read) •Reorient patient •Reduce environmental noise •Offer pain relief •Have family or sitter with patient •Change environment (eg, room closer to nurses station, chair in hall) •Explain all procedures •Music offered •Routine ambulation •Offer toileting q2 hrs •Oral hygiene •Place in reclining chair
“Restraint or seclusion may only be used when less restrictive measures have been determined to be ineffective to protect the patient, a staff member or others from harm.” (CMS)

1 limb, 2 limbs, 3 limbs, 4 . . .Can be used on any floor
There is a misperception that the use of 4-point restraints constitutes “behavioral” restraints, and cannot be done on a typical med-surg unit. The facts are:• The number of restraints on a patient does not define the type of
restraint. It’s patient behavior -- the reason for restraint -- that determines the type: – Behavioral: For management of violent behavior that threatens to harm
the patient or others– Med-Surg: For management of non-violent behavior that is interfering
with med-surg care/treatments
• Though rare, behavioral restraints may be initiated for violent behavior on a non-behavioral (med-surg) unit. It must be remembered that this type of restraint requires constant 1:1 monitoring and frequent documentation of observations.

Tying Soft Limb Restraints• Annually, all clinical staff must demonstrate the
ability to secure and release restraint with a quick-release tie or bow.
Check-off will occur in your work area.
• Following are illustrations of acceptable quick-release tying methods.

The Simple Slip Knot

The Posey Quick-Release Tie
• This adds an extra step to the simple slip knot.• It makes the knot more secure while still being a
quick-release.

A Bow Is Also Acceptable

But This Knot . . . Is Not!

Points to Remember when Applying Restraints
• Secure the limb holder cuff tightly enough to prevent the patient from pulling the limb out of the cuff, but loose enough to allow adequate circulation. Allow a one-finger space between the cuff and the patient’s limb.
• Tie the straps to a movable part of the bed frame, out of the patient’s reach. Do not tie it to a side rail!
• Ensure that the bow/knot used can be released with a single pull on the tail of the straps.
• Maintain proper alignment of body and limbs, trying to allow enough slack to enable some limb movement without compromising the purpose for the restraint.

Enclosure Bed
This type of restraint may be used only on:
STUNeuro
RehabPICUPeds-4
• Annual competency demonstration is required for nurses and CNAs on these units.
• Managers of these units will notify their staff of the location and times for inservicing and check-off.

Restraint Documentation
in Powerchart

Obtain Initial Order from M.D.
• The physician should enter the Powerplan for restraints. The nurse may do so when necessary to obtain a telephone order.
• There are 4 restraint Powerplans:

Initiate the Powerplan
Be sure to leave these two boxes pre-checked!
They will trigger the necessary tasks as long as the Powerplan is active.
The physician may initiate the Powerplan or put it in a “planned” state. The nurse will then initiate the plan.

3 nursing tasks will be triggered when the Powerplan is initiated and signed:
• “Restraint Initiate” (Activity View) – This task is only charted once.
• “Restraint Observe/NV/ROM” (Activity View)– The frequency of this task is every 2 hours. – For Med Surg restraints, this task will continue until the Powerpan is
discontinued. Behavioral restraint tasks have a duration associated with the order.
• “Check with MD regarding new orders for restraints if appropriate” – A one-time reminder the next day, charted as “done/not done”.
Tasks Triggered by the Powerplan
See screen prints on the following slides

“Restraint Initiate”
Chart pre-restraint assessment and actions as well as education.

“Restraint Observe/NV/ROM”
• Use a dynamic group to create the appropriate label for the restraints being used.
• If bilateral limb restraints are in use, a dynamic group for each limb is required.
• Creating the label is only needed with the first documentation or if the location of the restraint is changed.

“Check with MD regarding new orders for restraints if appropriate”
• The task will fire at 0900 the next day to remind the nurse to obtain a new order if restraints are still necessary.
• This task only serves as a one-time reminder and is charted as “done/not done”.
• If restraints are no longer needed, the nurse should:– Document their discontinuation– Discontinue the Powerplan

Restraint Continuation beyond Day 1• The next day, and each day thereafter, the MD must evaluate the need for
restraint and enter an order if indicated. (The nurse may do so only when necessitated by telephone order)
• The order to use is “Restraint Apply (Post Initiation)”. • Enter this order by using “Add to Phase” on the previously initiated
Powerplan for Restraints - Med Surg/Non Violent. • Do not discontinue the initial Powerplan and enter a new one each
day!
See next slide for Post-Initiation steps

Post-Initiation Steps

“Post-Initiation” Tasks
• When signed, the Post-Initiation order will generate “Check with MD regarding new orders” again at 0900 the following morning.
• Since the Post-Initiation order is a continuation of the original restraint order, the q2hr tasks for “Restraint Observe/NV/ROM” will continue uninterrupted until the original order is D/C’d.

Advantages of Using “Post-Initiation” Orders
• It is not necessary to discontinue the previous day’s restraint orders when the new “Post-Initiation” orders are entered each day.
• All the restraint orders for all days of the current restraint episode will be in one location in a single Powerplan.
• By simply clicking on the Powerplan, you can view all the restraint orders for that episode, rather than having to scroll through the list of “Patient Care Orders” to locate them.
• This helps to streamline the documentation audit process!

And speaking of documentation audits …
The following slides compare OLOL’s 2012 & 2013 restraint documentation compliance.

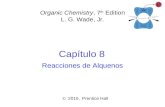
Documentation ComplianceICU
Audit Item 2012Compliance
2013 (thru Oct)Compliance
Timely initial order 98% 97%Documentation of restraint application 95% 98%Order obtained each subsequent day 95% 94%Documentation q 2hrs
Observe 97% 92% ROM 97% 92% NV check 97% 92%Plan of Care addressed daily 96% 91%Restraint removal documented 91% 90%

Documentation ComplianceNon-ICU
Audit Item 2012Compliance
2013 (thru Oct)Compliance
Timely initial order 96% 99%Documentation of restraint application 92% 96%Order obtained each subsequent day 91% 91%
Documentation q 2hrs
Observe 83% 87% ROM 84% 85% NV check 83% 83%
Plan of Care addressed daily 88% 90%Restraint removal documented 83% 68%
Note: Minimum acceptable Joint Commission compliance is 90% Scores below 90% are in red

Documentation ComplianceECU/PECU (Med-Surg)
Audit Item 2012Compliance
2013 (thru Oct)Compliance
Timely initial order 95% 85%Documentation of restraint application 84% 96%Order obtained each subsequent day n/a n/a
Documentation q 2hrs
Observe 89% 89%
ROM 89% 83% NV check 89% 79%Plan of Care addressed daily 63% 69%
Restraint removal documented 88% 76%
Note: Minimum acceptable Joint Commission compliance is 90% Scores below 90% are in red

Documentation ComplianceBehavioral Restraints
ECU/PECU M&BH Units
Audit Item 2012 2013(thru Oct)
Audit Item 2012 2013(thru Oct)
Timely order 89% 86% Timely order 100% 100%
Time-limited order 74% 81% Time-limited order 100% 87%
Documentation of application
84% 98% Documentation of application
100% 100%
Documentation q 15 min 84% 82% Documentation q 15 min 100% 91%
POC Revision 100% 84% POC Revision 100% 70%
Post-restraint debriefing 82% 70% Post-restraint debriefing 100% 87%
Note: Minimum acceptable Joint Commission compliance is 90% Scores below 90% are in red

But don’t let these results keep you uptight . . .
Simply make a commitment to doing
it RIGHT!

You are finished!
• Close out of this document.• Click REFRESH• Take Test