Rationale of Antibiotic Smart Use - ศูนย์ข้อมูล...
91
Rationale of Antibiotic Smart Use รศ. นพ. ภิรุญ มุตสิกพันธุ หนวยโรคติดเชื้อ ภาควิชาอายุรศาสตร คณะแพทยศาสตร มหาวิทยาลัยขอนแกน
Transcript of Rationale of Antibiotic Smart Use - ศูนย์ข้อมูล...

Rationale of Antibiotic Smart Use
รศ. นพ. ภิรุญ มุตสิกพันธุหนวยโรคติดเชื้อ ภาควิชาอายุรศาสตร
คณะแพทยศาสตร มหาวิทยาลัยขอนแกน

Targeted diseases
• Upper respiratory tract infection
• Acute diarrhea
• Lacerated wounds

Upper respiratory tract infection (URI)

Sinusitis
Rhinitis
Pharyngitis
Glottitis
Laryngitis
Tracheobronchitis
Bronchiolitis
Pneumonia
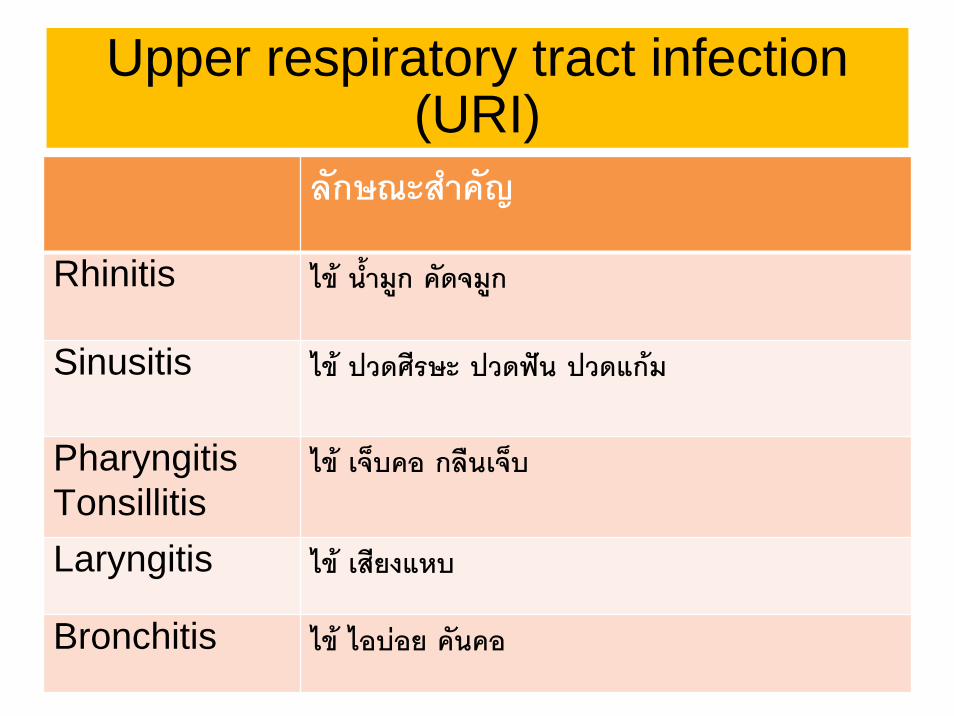
Upper respiratory tract infection (URI)
ลักษณะสําคญั
Rhinitis ไข น้ํามูก คัดจมูก
Sinusitis ไข ปวดศีรษะ ปวดฟน ปวดแกม
PharyngitisTonsillitis
ไข เจ็บคอ กลืนเจ็บ
Laryngitis ไข เสียงแหบ
Bronchitis ไข ไอบอย คนัคอ
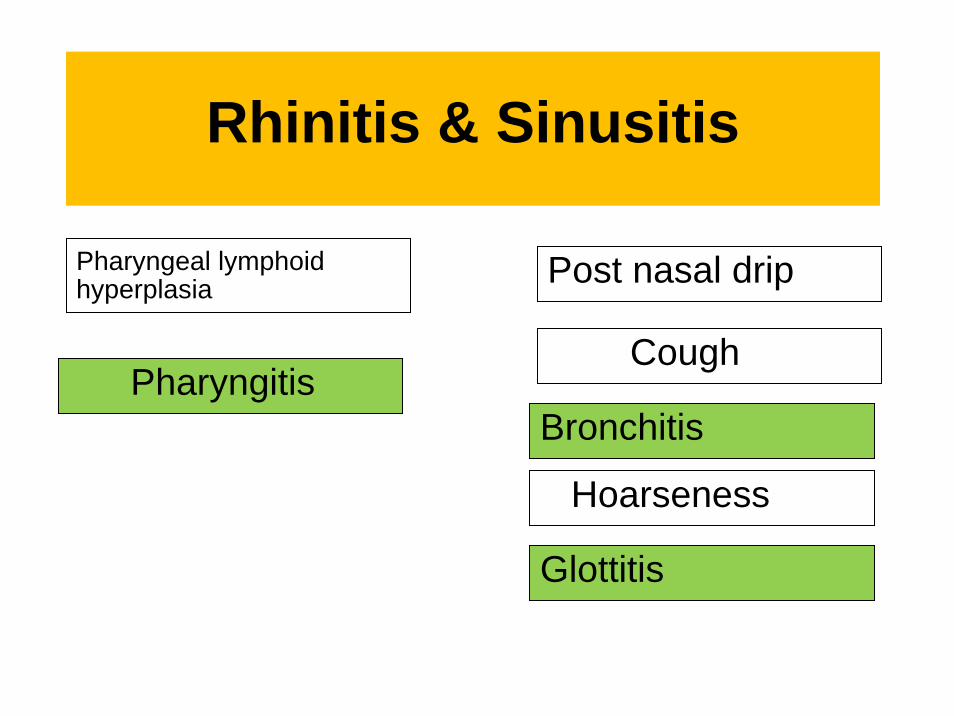
Rhinitis & Sinusitis
Post nasal drip
Bronchitis
Glottitis
Pharyngeal lymphoid hyperplasia
Cough
Hoarseness
Pharyngitis

7
Rhino-sinusitis นาจะเรียกรวมกันมากกวาเพราะ
• Allergic or non-allergic rhinitis มักจะเกิดนํามากอน sinusitis เสมอ
• Sinusitis ที่ไมมี rhinitis พบนอยมาก
• อาการคัดจมูกและมีน้ํามูกเปนอาการเดนของ sinusitis เชนกัน
• Nasal mucosa และ sinus mucosa มีลักษณะ
เดียวกันและตอเนื่องกัน

8
Non-infectious Causes of Rhinosinusitis
• Non-allergic cause• Tobacco smoke• Perfumes• Cleaning solutions• Burning candles• Cosmetics
• Car exhaust, diesel fumes
• Hair spray
• Auto exhaust, Gas, diesel fuel
• Cold air, Dry air
• Allergic cause• Pollen
• House dust
• Animal danders
• Food & Beverages

Common cold

Common cold
• Really a viral rhinosinusitis
• 87% of common cold have CT evidence of sinus cavity disease
• Maxillary sinus is commonly affected
CID 1996;23:1209


Common cold
• 0.5 -2% will progress to acute bacterial sinusitis
• 1 ใน 200 คน ถึง 1 ใน 50 คนที่เปนหวัดจะมีโอกาสเปน
acute bacterial sinusitis
• หมายถึงวาถาใหยาปฏิชีวนะแกผูปวยที่มีอาการของหวัด 50-200
รายมีโอกาสรักษา ABRS เพียง 1 ราย





ปจจัยบงชี้วาเปน bacterial sinusitis
JAMA 1993;270:1242-6
ลักษณะทางคลินิก ความเปนไปได
Maxillary toothache 2.5 (1.2-5.0)
Purulent secretion by exam 2.1 (1.5-3.0)
Poor response to decongestion
2.1 (1.4-3.1)
Abnormal transillumination 1.6 (1.3-2.0)
Hx of colored nasal discharge
1.5 (1.2-1.9)

ความเปนไปไดวาเปน bacterial sinusitis
JAMA 1993;270:1242-6
จํานวน predictor ความเปนไปได (%)0 9
1 21
2 40
3 63
4 81
5 92

Antibiotic for acute sinusitis
• Indicated only in patients with persistent symptoms more than 7 days

Causative organisms (ABRS)PEDIATRIC
(%)
ADULT
(%)
S.pneumoniae 35-42 20-43
H.Influenzae 21-28 22-35
M.Catarrhalis 21-28 2-10
Other streptococci 3-7 3-9
Anaerobe 3-7 0-9
S.aereus 0 0-8

Are antibiotics effective in resolving symptoms and preventing complications in
ABRS
Antibiotics were significantly more effective than placebo, reducing treatment failures by almost one-half. However, symptoms improved or were cured in 69 percent of patients without any antibiotic treatment at all (95 percent CI, 57 to 79 percent).

Among the various ATB, what is their comparative efficacy in ABRS?
The pooled failure rate in patients treated with amoxicillin was low (11 percent; 95 percent CI, 8-14), and the further decrease in clinical failures with broad-spectrum antibiotics was not clinically important. Treating 100 patients with amoxicillin would lead to only 0.85 more failures (95 percent CI, 3.1 more to 1.4 fewer failures).

Recommendation of ATB
• First line ATB for ABRS -> Amoxycillin• Duration of Rx – 10-14 days
• Alternative or different class ATB if
• - Penicillin allergy
• - fail to improve by 7 days of initial Rx
• - Prior use of ATB 4-6 wks before (risk of drug resistant bacteria)
• - chronic or recurrent acute rhinosinusitis

Sinus and Allergy Health Partnerships 2004
• Alternative ATB
• Fluoroquinolones• High dose amoxycillin/clavulanate (4/250 mg/d)
• No evidence of difference in clinical outcome regard to different dose and duration
• However, adherence of once daily ATB and short duration is better and greater completion of full course

Recommendation of treatment failure after 7 days
• Alternative ATB• Fluoroquinolones
• High dose amoxy/clav (4gm/250 mg/d)
• Large number of reduced susceptibility to original ATB
• Most common – PRSP, MRSP, BLP H. influenzae
• Optimal ATB not studied-> based on prior ATB
• Cephalosporins, macrolides may not adequate

Sinusitis – Primary Care RCT• Amox 500 mg3 x 7 days• Block randomized (ITT)• Healthy >15 yr• Median 7 days symptoms• No difference at day ≥10
– Symptom duration– Symptom severity
• No severe complications at 6 wks
• No interactions– Factorial trial with nasal
steroids
Williamson et al. JAMA 2007; 298(12):2487-2496
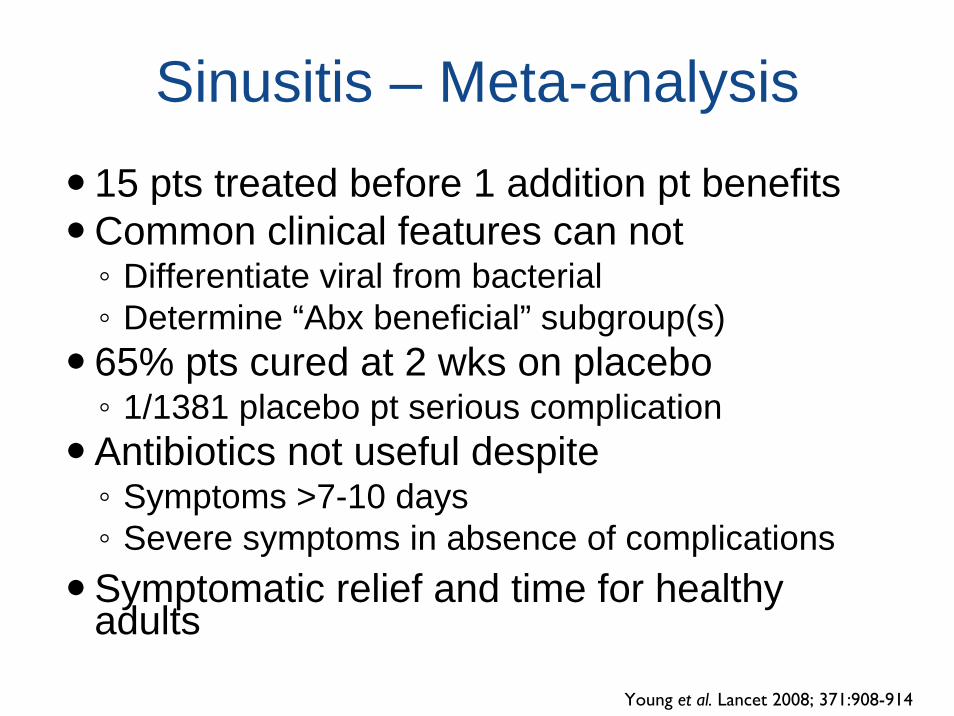
Sinusitis – Meta-analysis15 pts treated before 1 addition pt benefitsCommon clinical features can not◦ Differentiate viral from bacterial◦ Determine “Abx beneficial” subgroup(s)65% pts cured at 2 wks on placebo◦ 1/1381 placebo pt serious complication Antibiotics not useful despite◦ Symptoms >7-10 days◦ Severe symptoms in absence of complicationsSymptomatic relief and time for healthy adults
Young et al. Lancet 2008; 371:908-914

Recommendation of Management
• - pain relief with analgesic – paracet, NSAIDs
• - nasal decongestant – local or systemic
• - topical steroid nasal spray
• - nasal saline irrigation
• - antihistamine if allergic component present
• - guaifenesin expectorant – no evidence
• - Antibiotic

Acute Otitis Media











Otitis MediaMeta analysis favour Abx◦ Clinical cure (RR = 1.13)◦ Symptoms at day 2 to 4 of Tx (RR = 0.68)◦ More diarrhea (RR = 1.5)◦ No difference in severe complicationsMargin of benefit very narrow◦ Parental relief & less absenteeism◦ Side effects & resistant bacteriaRCT F/U Amox vs. placebo◦ 20% more recurrences in Abx group
Vouloumanou et al. JAC 2009; 64:16-24Bezakova et al. BMJ 2009; 339:b2525

Acute Bronchitis
• 9th most common outpatient issue– 5% of adults annually
• Viral etiology predominates• Antibiotics not recommended
– Reduce cough by 0.6 of a day– Trend towards Abx adverse events– B. pertussis an exception
• Reduce transmission• Decrease cough duration (given) in 1st week
Wenzel & Fowler. NEJM 2006; 355:2125-2130

Pharyngitis

Causes of pharyngitis
Rhinovirus 20%
Coronavirus > 5%
Adenovirus 5%
Herpes simplex virus 4%
Group A streptococcus 15-30%
Group C streptococcus 5-10%
Unknown 30%
Gwaltney 1995

Group A streptococcal pharyngitis
• 50% of pharyngitis in high school children (6-17 yrs) but less than 10% in adult
• Typical feature include sudden onset of fever, chill, severe sore throat, dysphagia, malaise, headache
• Exam – pharyngeal erythema, exudativepharyngitis, and anterior cervical LN
• Strept pharyngitis usually improve in 3 days, even not treated.




ถาไมสามารถเพาะเชื้อ GASได จะวินจิฉัยอยางไร และตองรักษานานถงึ 14 วันหรือไม
• ใชเกณฑการวินิจฉัย 3 ขอ• ไขมากกวา 39 C• Exudative phayngotonsillitis• Tender cervical LN• รักษานาน 10 วันเพียงพอ เพื่อปองกัน rheumatic fever



Therapy for streptococcal pharyngitis
In children:
• - penicillin 250 mg BID or TID X 10 d (amoxy OK)
• - Erythromycin 20-40 mg.kg/d x 10 d
In adult:
• - penicillin 250 mg TID (500 mg BID) X 10d
• - erythromycin 250 mg QID X 10 d

Persistent or recurrent pharyngitis
• Recurrent or persistent symptoms usually due to co-infection with beta-lactamaseproducing organism
• Alternatives• - clindamycin 20-30 mg/kg/d x 10 d• - clindamycin 150 mg TID X 10 d




Acute diarrhea

Common causes of acute diarrhea
• Non-infectious• Osmotic • Laxative
• Infectious• Inflammatory• Non-inflammatory• - viral• - protozoa• - bacterial toxin• - S. aureus• - B. cereus• - ETEC• - V. cholerae
• Bacteria• - Shigella• -Salmonella• - Campylobacter• - Plesiomonas• - V. parahemolyticus



Antimicrobial Rx in acute diarrhea







สามารถใช co-trimoxazole ในการรักษา acute diarrhea ไดหรือไม
• ขอมูลของความไวของเชื้อ shigella, salmonella ตอ
Cotrimoxazole พบวามีความไวเพียงรอยละ 3-26 และ
77 ตามลําดับ จึงมีความเสี่ยงสูงที่อาจจะรักษาไมไดผล ยกเวนมี
ขอมูลของโรงพยาบาลนั้นๆวาเชื้อยังไวตอยามากกวารอยละ 80 ขึ้น
ไป
• การที่ใช cotrimoxazole ไดผลอาจเนื่องจากไมไดเปนการติด
เชื้อ shigella หรืออาการไมรุนแรง หายเอง

โรคทองรวงในเดก็อายเุทาไรที่ให co-trimoxazole ไดและอายุเทาไรให norfloxacin ได
• Cotrimoxazole ในเด็กสามารถใหไดตั้งแต 6 สัปดาหขึ้นไป
อาศัยหลักฐานจากคําแนะนําการใช cotrimoxazole ในการ
ปองกนั OI ในเด็กติดเชื้อ HIV
• สําหรับการใช quinolone มีขอมูลการใชใน preterm,
infant, children มากขึ้น และมีความปลอดภัย จึงสามารถ
ใชไดเมื่อจําเปนตองใช

โรคทองรวงในเดก็เล็กๆสามารถใช ceftriaxone หรือ cotrimoxazole suspensionไดหรือไม
• ใชได




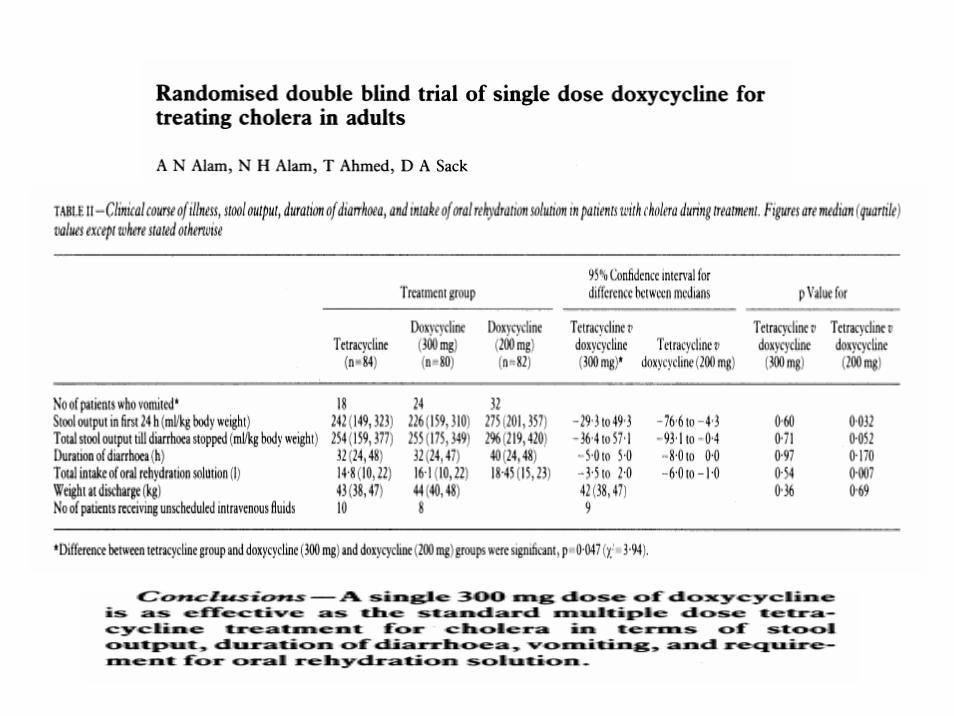
Guideline การรักษาอหิวาต ไมตรงกับของกระทรวง
Antimicrobial agents play a secondary role in the treatment of cholera.
Clinical trials have shown that, when patients with severe dehydration are
given antibiotics, the duration of diarrhea is decreased and the volume of
stool is reduced by nearly half.
Early discharge and lessened hydration decrease hospital expense. These
benefits are critical in epidemic conditions.
Oral tetracycline and doxycycline are the agents of choice in areas of the

การใช quinolone ในคนทอง


แนวทางการใหยาปฏิชีวนะในแผลเลือดออก(guidelines of ATB use in lacerated
wounds)

เมื่อไหรที่ควรจะใชยาปฏิชีวนะในแผลเลือดออก
• เพื่อปองกันการติดเชื้อ
• แผลที่เสี่ยงตอการติดเชื้อ และ
• ถามีการติดเชื้อมีโอกาสลุกลามไดรุนแรง
• เพื่อรักษาการติดเชื้อ





การใช Penicillin V ในกรณีสัตวกดั สามารถใชไดหรือไม
• เชื้อที่พบจากแผลที่ถูกสัตวกัด • Pasteurella species were found in 75% of cat bite wound
infections and 50% of dog bite infections. • Staphylococcus species and Streptococcus species were commonly
found in bites wounds from dogs, cats, and humans • anaerobes such as Prevotella, Fusobacterium, Bacteroides, and
Peptosteptococcus.• Eikenella corrodens was found in 30% of human bite wound
infections.
• Pasteurella species are susceptible to penicillin, ampicillin, amoxicillin, second- and third-generation cephalosporins, azithromycin, and the fluoroquinolones. First-generation cephalosporins, erythromycin, and dicloxacillin are not recommended.

การใช Penicillin V ในกรณีสัตวกดั สามารถใชไดหรือไม
• Penicillin ไมสามารถ cover เชื้อ S. aureus, anaerobes gram negative, gram negative ได
• จึงไมเพียงพอสําหรับการปองกันการติดเชื้อจากสัตวกัด
• ในกรณีไมมี co-amoxyclav สามารถใชยา 2 ชนิดรวมกัน เชน cloxacillin + ofloxacin หรือ cotrimoxazole
• clindamycin + ofloxacin หรือ cotrimoxazole

แผลปนเปอน ถาไมมี co-amoxyclav สามารถใช high dose penicillin ไดหรือไม
• Penicillin ไมสามารถ cover เชื้อ S. aureus, anaerobes gram negative, gram negative
• จึงไมเพียงพอสําหรับการปองกันการติดเชื้อจากแผลปนเปอน
• ในกรณีไมมี co-amoxyclav สามารถใชยา 2 ชนิดรวมกัน เชน clindamycin + ofloxacin หรือ cotrimoxazole
Clear evidence and recommendations regarding the use of prophylactic antibiotics after bite wounds have been lacking. Randomized studies are few, contain small numbers of patients, and utilize dissimilar antibiotics, many of which have subsequently been determined to be poor empiric choices. Meta-analysis reviews have been done but are limited by the same paucity of original research. A review by Medirios et al. looked at eight of the randomized studies and found little evidence that prophylactic antibiotics changed the outcome in wounds other than those to the hand or those resulting from human or cat bite (7). Lack of evidence of the efficacy of prophylactic antibiotics after dog bite wounds to nonhand areas found in this study was not found in an earlier meta-analysis study by Cummings. In this study, there was a statistically significant relative risk reduction of 44% in the use of antibiotics after dog bites (8).

แผลเปด การใช dicloxacillin เพียง 2 วันเพียงพอหรือไม จะทําใหเพิ่มโอกาสการดื้อยาหรือไม
• แผลสะอาด ไมมีเนื้อเนาตาย ไมมี DM, PVD เชื้อสวนใหญที่อาจปนเปอนที่แผลจากการเดินที่เทา หรือจากผิวหนังผูปวยเองเกือบทั้งหมดเปนเชื้อ S. aureus, Streptococci ดังนั้น การใช dicloxacilin เพียงพอในการปองกันการติดเชื้อเชนเดียวกับในการปองกนัการติดเชื้อจากการผาตัด
• 2 วันเพียงพอ ถาแผลดูอักเสบมากขึ้น ควรจะใหเปนการรักษาไปแทน• การดื้อยาขึ้นกับปริมาณเชื้อในแผล และระดับยาที่เพียงพอในเนื้อเยื่อ









![Rational Antibiotic Use in the Management of … Antibiotic...Rational Antibiotic Use in the Management of Respiratory Tract [RTI] and Urinary Tract [UTI] Infections Noe B. Mateo,](https://static.fdocument.pub/doc/165x107/5ae2540a7f8b9ad47c8cf9fb/rational-antibiotic-use-in-the-management-of-antibioticrational-antibiotic.jpg)