Rapidly Progressive Respiratory Failure in Mixed ...
5
3415 □ CASE REPORT □ Rapidly Progressive Respiratory Failure in Mixed Connective Tissue Disease: Report of an Autopsy Case Yasutaka Watanabe 1 , Shinichiro Koyama 1 , Masato Moriguchi 2 , Chihiro Miwa 1 , Mamoru Shiraishi 1 , Motoko Nomura 1 , Mitsuhiro Nokubi 3 , Chihiro Terai 2 and Yoshinori Kawabata 4 Abstract A 64-year-old woman presented with exertional dyspnea. The case was diagnosed as mixed connective tis- sue disease (MCTD) due to presence of swollen fingers, Raynaud’s phenomenon, muscle weakness, positive anti-U1RNP antibody, pericarditis and interstitial pneumonia. Although the histology from a transbronchial lung biopsy (TBLB) indicated organizing pneumonia, corticosteroid therapy was postponed for two months at the patient’s request. She died 8 weeks later from acute progressive interstitial pneumonia in spite of the ad- ministration of intravenous cyclophosphamide combined with prednisolone. The autopsy revealed exudative and organizing diffuse alveolar damage (DAD). Previous reports have shown that DAD is an extremely rare pulmonary complication in MCTD. This report presents a case of MCTD with acute respiratory failure. This case thus suggests that this therapy should be administered as soon as possible. Key words: mixed connective tissue disease, diffuse alveolar damage, interstitial pneumonia, cytomegalo- virus (Intern Med 51: 3415-3419, 2012) (DOI: 10.2169/internalmedicine.51.8728) Introduction Mixed connective tissue disease (MCTD) is characterized by the combined features of systemic lupus erythematosus (SLE), scleroderma and polymyositis, and high titers of a serum antibody to ribonucleoprotein antigen (anti-RNP- antibody). Pulmonary involvement, such as pleuritis, usual interstitial pneumonia (UIP), and pulmonary hypertension, occurs in 20 to 85% of patients with MCTD (1-3). This re- port presents an autopsy case of MCTD in a patient that died from acute progressive interstitial pneumonia (IP). Or- ganizing pneumonia was diagnosed by a transbronchial lung biopsy (TBLB) before therapy; however, an autopsy showed diffuse alveolar damage (DAD). The rare association of MCTD and DAD is discussed in the pathological findings. Case Report A 64-year-old woman presented with a one-month history of exertional dyspnea. She was a housewife, with a BMI of 20.2 and was an ex-smoker with a 45 pack-year history. The patient had an eight-year history of diabetes mellitus, hyper- tension and hyperlipidemia. She was diagnosed with IP 3 weeks after the first visit based on fine crackles on chest auscultation, and chest computed tomography (CT) showing a reticular pattern at bilateral lower lung fields (Fig. 1a, b). The case was also diagnosed as scleroderma or MCTD be- cause she had swollen fingers, Raynaud’s phenomenon, positive anti-nuclear-antibody and a single high titer of anti- RNP-antibody. She was admitted for the TBLB one month later, and the pathological examination showed findings that suggested organizing pneumonia with plug formation and a 1 Division of Pulmonary Medicine, Jichi Medical University, Saitama Medical Center, Japan, 2 Division of Reumatology, Jichi Medical University, Saitama Medical Center, Japan, 3 Division of Pathology, Jichi Medical University, Saitama Medical Center, Japan and 4 Division of Pathology, Saitama Cardiovascular and Respiratory Center, Japan Received for publication August 1, 2012; Accepted for publication September 11, 2012 Correspondence to Dr. Yasutaka Watanabe, [email protected]
Transcript of Rapidly Progressive Respiratory Failure in Mixed ...

3415
□ CASE REPORT □
Rapidly Progressive Respiratory Failure in MixedConnective Tissue Disease: Report of an Autopsy Case
Yasutaka Watanabe 1, Shinichiro Koyama 1, Masato Moriguchi 2, Chihiro Miwa 1,
Mamoru Shiraishi 1, Motoko Nomura 1, Mitsuhiro Nokubi 3,
Chihiro Terai 2 and Yoshinori Kawabata 4
Abstract
A 64-year-old woman presented with exertional dyspnea. The case was diagnosed as mixed connective tis-
sue disease (MCTD) due to presence of swollen fingers, Raynaud’s phenomenon, muscle weakness, positive
anti-U1RNP antibody, pericarditis and interstitial pneumonia. Although the histology from a transbronchial
lung biopsy (TBLB) indicated organizing pneumonia, corticosteroid therapy was postponed for two months at
the patient’s request. She died 8 weeks later from acute progressive interstitial pneumonia in spite of the ad-
ministration of intravenous cyclophosphamide combined with prednisolone. The autopsy revealed exudative
and organizing diffuse alveolar damage (DAD). Previous reports have shown that DAD is an extremely rare
pulmonary complication in MCTD. This report presents a case of MCTD with acute respiratory failure. This
case thus suggests that this therapy should be administered as soon as possible.
Key words: mixed connective tissue disease, diffuse alveolar damage, interstitial pneumonia, cytomegalo-
virus
(Intern Med 51: 3415-3419, 2012)(DOI: 10.2169/internalmedicine.51.8728)
Introduction
Mixed connective tissue disease (MCTD) is characterized
by the combined features of systemic lupus erythematosus
(SLE), scleroderma and polymyositis, and high titers of a
serum antibody to ribonucleoprotein antigen (anti-RNP-
antibody). Pulmonary involvement, such as pleuritis, usual
interstitial pneumonia (UIP), and pulmonary hypertension,
occurs in 20 to 85% of patients with MCTD (1-3). This re-
port presents an autopsy case of MCTD in a patient that
died from acute progressive interstitial pneumonia (IP). Or-
ganizing pneumonia was diagnosed by a transbronchial lung
biopsy (TBLB) before therapy; however, an autopsy showed
diffuse alveolar damage (DAD). The rare association of
MCTD and DAD is discussed in the pathological findings.
Case Report
A 64-year-old woman presented with a one-month history
of exertional dyspnea. She was a housewife, with a BMI of
20.2 and was an ex-smoker with a 45 pack-year history. The
patient had an eight-year history of diabetes mellitus, hyper-
tension and hyperlipidemia. She was diagnosed with IP 3
weeks after the first visit based on fine crackles on chest
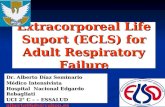
auscultation, and chest computed tomography (CT) showing
a reticular pattern at bilateral lower lung fields (Fig. 1a, b).
The case was also diagnosed as scleroderma or MCTD be-
cause she had swollen fingers, Raynaud’s phenomenon,
positive anti-nuclear-antibody and a single high titer of anti-
RNP-antibody. She was admitted for the TBLB one month
later, and the pathological examination showed findings that
suggested organizing pneumonia with plug formation and a
1Division of Pulmonary Medicine, Jichi Medical University, Saitama Medical Center, Japan, 2Division of Reumatology, Jichi Medical University,
Saitama Medical Center, Japan, 3Division of Pathology, Jichi Medical University, Saitama Medical Center, Japan and 4Division of Pathology,
Saitama Cardiovascular and Respiratory Center, Japan
Received for publication August 1, 2012; Accepted for publication September 11, 2012
Correspondence to Dr. Yasutaka Watanabe, [email protected]
Intern Med 51: 3415-3419, 2012 DOI: 10.2169/internalmedicine.51.8728
3416
Table 1. Laboratory Data on Admission
ygoloreSCBCWBC 6800 / L CRP 0.77 mg/dL
Neu 75.3 % ESR 62 mm Lym 16.2 % MPO-ANCA <10 EU Mono 5.4 % RF <10 IU/L
RBC 426×104 / L ANA 1:40960 Hb 12.3 g/dL Anti-RNP-Ab 256 Index Ht 41.5 % Anti-SSA-Ab (-) Plt 26.9×104 / L Anti-Jo1-Ab (-)
bA-AND-itnAyrtsimehC (-) HbA1c 5.9 % KL-6 3140 U/mL TP 8.3 g/dL SP-D 250 ng/mL Alb 3.3 g/dL IC 1.5 pg/mL T.Bil 0.53 mg/dL CH50 40.9 U/mL AST 30 IU/L C3 87 mg/dL ALT 10 IU/L C4 22 mg/dL LDH 379 IU/L Arterial blood gas analysis ; room air CK 382 IU/L pH 7.422 Aldolase 7.6 IU/L PaO2 60.5 mmHg ALP 216 mU/mL PaCO2 35.3 mmHg BUN 7 mg/dL HCO3
- 22.5 mmol/L Cre 0.43 mg/dL Na 142 mEq/L K 3.3 mEq/L Cl 107 mEq/L
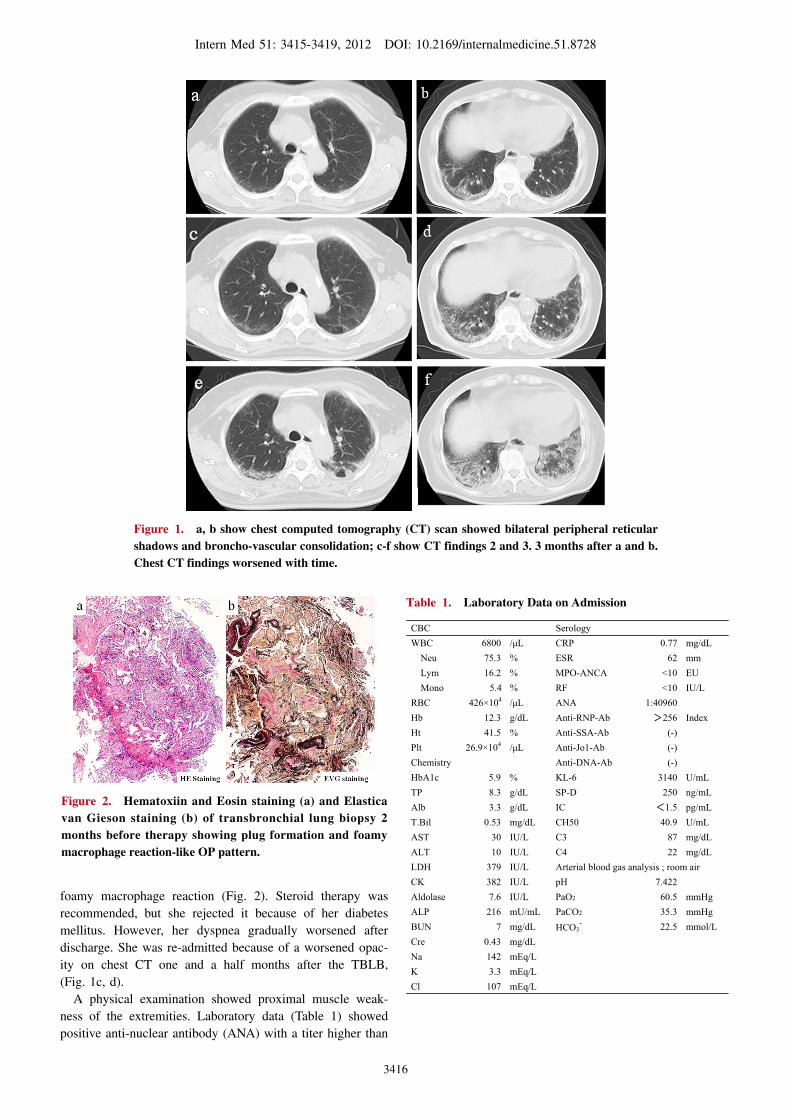
Figure 1. a, b show chest computed tomography (CT) scan showed bilateral peripheral reticular shadows and broncho-vascular consolidation; c-f show CT findings 2 and 3. 3 months after a and b. Chest CT findings worsened with time.
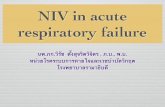
Figure 2. Hematoxiin and Eosin staining (a) and Elastica van Gieson staining (b) of transbronchial lung biopsy 2 months before therapy showing plug formation and foamy macrophage reaction-like OP pattern.
foamy macrophage reaction (Fig. 2). Steroid therapy was
recommended, but she rejected it because of her diabetes
mellitus. However, her dyspnea gradually worsened after
discharge. She was re-admitted because of a worsened opac-
ity on chest CT one and a half months after the TBLB,
(Fig. 1c, d).
A physical examination showed proximal muscle weak-
ness of the extremities. Laboratory data (Table 1) showed
positive anti-nuclear antibody (ANA) with a titer higher than
Intern Med 51: 3415-3419, 2012 DOI: 10.2169/internalmedicine.51.8728
3417
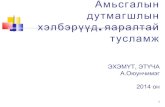
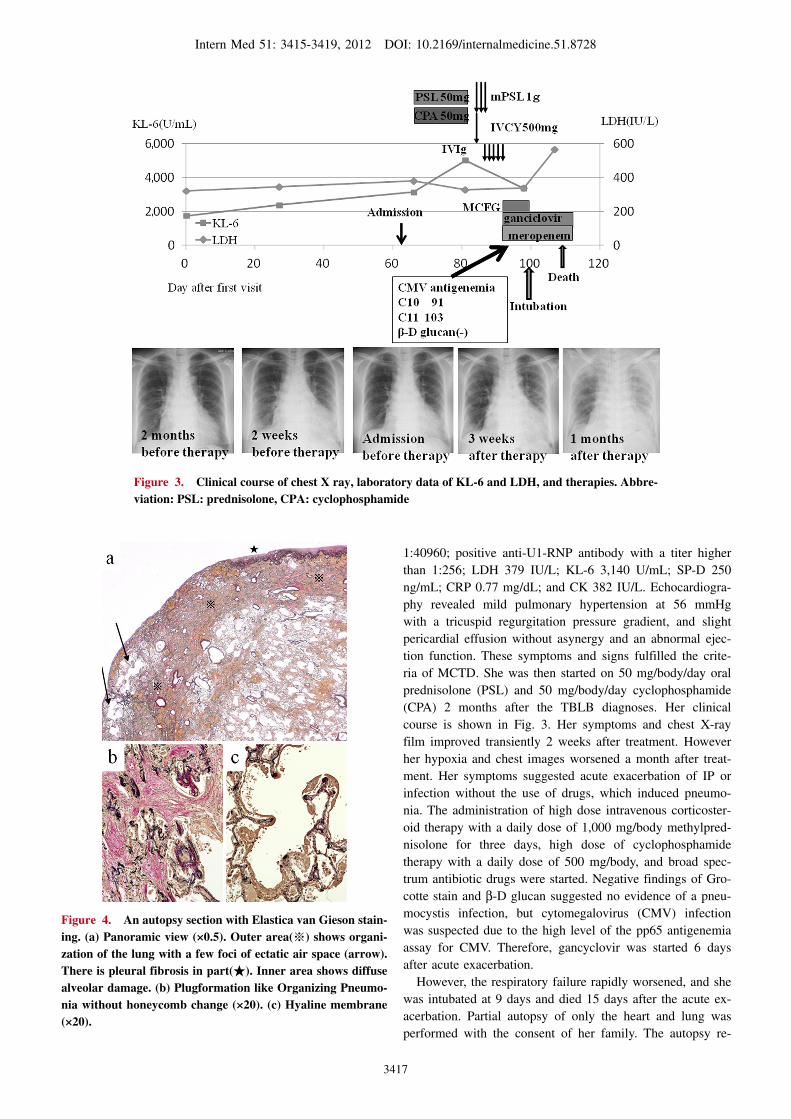
Figure 3. Clinical course of chest X ray, laboratory data of KL-6 and LDH, and therapies. Abbre-viation: PSL: prednisolone, CPA: cyclophosphamide
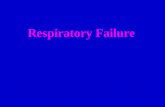
Figure 4. An autopsy section with Elastica van Gieson stain-ing. (a) Panoramic view (×0.5). Outer area(※) shows organi-zation of the lung with a few foci of ectatic air space (arrow). There is pleural fibrosis in part(★). Inner area shows diffuse alveolar damage. (b) Plugformation like Organizing Pneumo-nia without honeycomb change (×20). (c) Hyaline membrane (×20).
1:40960; positive anti-U1-RNP antibody with a titer higher
than 1:256; LDH 379 IU/L; KL-6 3,140 U/mL; SP-D 250
ng/mL; CRP 0.77 mg/dL; and CK 382 IU/L. Echocardiogra-
phy revealed mild pulmonary hypertension at 56 mmHg
with a tricuspid regurgitation pressure gradient, and slight
pericardial effusion without asynergy and an abnormal ejec-
tion function. These symptoms and signs fulfilled the crite-
ria of MCTD. She was then started on 50 mg/body/day oral
prednisolone (PSL) and 50 mg/body/day cyclophosphamide
(CPA) 2 months after the TBLB diagnoses. Her clinical
course is shown in Fig. 3. Her symptoms and chest X-ray
film improved transiently 2 weeks after treatment. However
her hypoxia and chest images worsened a month after treat-
ment. Her symptoms suggested acute exacerbation of IP or
infection without the use of drugs, which induced pneumo-
nia. The administration of high dose intravenous corticoster-
oid therapy with a daily dose of 1,000 mg/body methylpred-
nisolone for three days, high dose of cyclophosphamide
therapy with a daily dose of 500 mg/body, and broad spec-
trum antibiotic drugs were started. Negative findings of Gro-
cotte stain and β-D glucan suggested no evidence of a pneu-
mocystis infection, but cytomegalovirus (CMV) infection
was suspected due to the high level of the pp65 antigenemia
assay for CMV. Therefore, gancyclovir was started 6 days
after acute exacerbation.
However, the respiratory failure rapidly worsened, and she
was intubated at 9 days and died 15 days after the acute ex-
acerbation. Partial autopsy of only the heart and lung was
performed with the consent of her family. The autopsy re-

Intern Med 51: 3415-3419, 2012 DOI: 10.2169/internalmedicine.51.8728
3418
Table 2. Reports of Acute Courses of Pulmonary Diseases Except Pulmonary Hypertension Complicated with MCTD
Reference number Age, Sex Histopathology(type of specimen)
Therapy Prognosis
5 37, M Modest interstitial fibrosis(TBLB, open lung biopsy & autopsy)
PSL&CPA dead
5 66, M Distortion of alveolar architecture by patchy interstitial fibrosis, recently organizing(open lung biopsy)
chlorambucil & PSL
alive
6 43, F unknown mPSL alive
7 33, F UIP&OP(open lung biopsy)
PSL & CsA Y UT
alive
8 49, F DAD(open lung biopsy)
mPSL & CPA alive
Abbreviations. TBLB: transbronchial lung biopsy, UIP: usual interstitial pneumonia, OP: organizingpneumonia, UIP: usual interstitial pneumonia, DAD: diffuse alveolar damage, PSL: Prednisolone, CPA: oral cyclophosphamide, CsA: cyclosporine A, Y: intravenous cyclophosphamide, UT: Ulinastatin, mPSL: methylprednisolone, : intravenous immunoglobulin, MC micafungin,
megalovirus
vealed the occlusion of alveoli, hyaline membranes, mem-
branous organization in the alveoli, and dilation of the al-
veolar ducts. Some lesions were associated with subpleural
fibrosis, but no honeycombing was found. In addition, an in-
traluminal organizing process was noted (Fig. 4). Her autop-
sied lung revealed acute or exudative DAD. There were no
features associated with DAD caused by CMV pneumonia,
although there were a few CMV inclusion bodies. There
were no findings to implicate other organisms such as bacte-
ria, pneumocystis jirovecii, and fungus. In addition, no vas-
cular changes of pulmonary hypertension with plexiform le-
sion were found, although there were a few arterializations
of small blood vessels. She was clinically diagnosed with
fatal interstitial pneumonia associated with MCTD.
Discussion
This report presented a MCTD case with rapidly fatal res-
piratory failure showing DAD at autopsy. IP is the most
common pulmonary manifestation of MCTD. The reported
frequency of IP in MCTD is between 21 and 50% (1, 4).
Sullivan et al. described chest X-ray abnormalities in 10 of
34 MCTD patients (3). However, rapid pulmonary complica-
tions associated with MCTD, other than pulmonary hyper-
tension, are very rare and there are few previous reports, as
shown in Table 2 (5-8). Patients with DAD generally have a
poor prognosis in comparison to other histopathological pat-
terns of IP. DAD can be seen in patients with UIP, pneumo-
nias, sepsis, drug-induced lung disease, inhalation injuries,
and various other conditions (9). Although the current pa-
tient received oxygen treatment, it was difficult to regard
oxygen therapy as the most probable origin of DAD because
her severe respiratory failure occurred before intubation. In
addition, there were no findings induced by drugs, sepsis
and so on in her clinical course and there were few CMV
inclusions or other pathogens found in the autopsy. There-
fore, the origin of DAD was first suspected to have been
caused by MCTD itself. Parambil et al. reported that DAD
can occasionally occur as a presenting manifestation of con-
nective tissue diseases (CTDs) (8). Their study population
indicated that DAD occurs in patients with or without preex-
isting CTD-related chronic IP and is a de novo manifesta-
tion of CTD in some patients. The CTD-related IP findings
prior to the onset of DAD showed organizing pneumonia
(OP) in 3 of 9 patients. The current patient’s TBLB finding
before therapy showed OP-like findings with plugs of granu-
lation tissue filling airspaces. It was possible that the first
pathological finding was not accurate for a diagnosis of IP
because very small samples were obtained by the TBLB. In
other words, her TBLB sample might be a part of DAD
showing granulation tissue in both the airspace and intersti-
tium (organizing pattern) (10). The pathological findings
might have progressed during the two months after the
TBLB. Another possibility is that acute exacerbation was su-
perimposed on the preexisting OP (8, 11). The TBLB speci-
men showed organizing pneumonia, and the autopsy find-
ings were DAD. Therefore, the cause of DAD seems most
likely to be related to her underlying MCTD.
On the other hand, this case had a high titer of CMV an-
tigenemia. Hanaoka et al. reported that CMV reactivation in-
dicates poor prognosis in CTD patients and might cause
subclinical CMV pneumonia in CTD patients that die by ex-
acerbation of IP (12). CMV infection could have caused
DAD in the current patient, because there was a high CMV
antigen titer. In addition, there were few CMV inclusions in
her autopsy, although previous reports said that their pres-
ence at autopsy might be a secondary phenomenon during
the terminal episode following treatment with high-dose cor-
ticosteroids (10). It is difficult to entirely exclude a viral in-
fection as a trigger for her course of DAD.
Case reports have described successful therapeutic use of
cyclosporine A combined with PSL or CPA, or human uri-

Intern Med 51: 3415-3419, 2012 DOI: 10.2169/internalmedicine.51.8728
3419
nary trypsin inhibitor (5-7). Cyclophosphamide combined
with prednisolone was administered in the present case, but
was not effective.
IP associated with CTD can be fatal even in patients
treated with high-dose corticosteroids (13, 14). In particular,
DAD has been described most commonly in patients with
polymyositis (PM)-dermatomyositis (DM) in whom DAD
implies a poor prognosis. Most of these patients die within a
few months of the onset of DAD despite corticosteroid ther-
apy (15). However, the drug seems to be effective for IP in
PM-DM, particularly when used early in the course of the
disease (16, 17). MCTD has features of PM or DM. DAD
might be related to PM or DM in the current patient. The
only therapy that might have helped this patient before exac-
erbation was to intervene earlier. Early immunosuppressive
therapy might have improved the clinical course of this pa-
tient although the autopsy finding suggested that her condi-
tion was irreversible and refractory.
It is sometimes difficult to determine whether the clinical
manifestations related to pulmonary involvement are due to
CTD or to an infectious process under immunosuppressive
therapy. However, early therapeutic intervention may be
preferable to avoid the deterioration of pulmonary lesions
associated with MCTD.
MCTD patients could be further compromised by respira-
tory deterioration and need early examination to determine
the optimal therapy. The duration of remission is uncertain.
The authors state that they have no Conflict of Interest (COI).
AcknowledgementThe authors thank Dr. Jack Hildebrandt and Wayne Lamm at
the University of Washington in Seattle, for their editorial assis-
tance.
References
1. Prakash UBS. Respiratory complications in mixed connective tis-
sue disease. Clin Chest Med 19: 733-746, 1998.
2. Prakash UBS. Lungs in mixed connective tissue disease. J Thorac
Imaging 7: 55-61, 1992.
3. Sullivan WD, Hurst DJ, Harmon CE, et al. A prospective evalu-
ation emphasizing pulmonary involvement in patients with mixed
connective tissue disease. Medicine 63: 92-107, 1984.
4. Sharp GC, Singsen BH. Mixed connective tissue disease. In: Ar-
thritis and Allied Conditions: A Textbook of Rheumatology. 11th
ed. McCarty DJ, Ed. Lea and Febiger, Philadelphia, 1989: 1080-
1091.
5. Wiener-Kronish JP, Solinger AM, Warnock ML, et al. Severe pul-
monary involvement in mixed connective tissue disease. Am Rev
Respir Dis 124: 499-503, 1981.
6. Takeda T, Tsutsumi A, Ogura N, et al. A case of mixed connective
tissue disease with acute interstitial pneumonitis. Jpn J Clin Im-
mun 18: 303-307, 1995 (in Japanese).
7. Tsujimura S, Saito K, Nakayamada S, et al. Human urinary tryp-
sin inhibitor bolus infusion improved severe interstitial pneumonia
in mixed connective tissue disease. Mod Rheumatol 15: 374-380,
2005.
8. Parambil JG, Myers JL, Ryu JH. Diffuse alveolar damage: uncom-
mon manifestation of pulmonary involvement in patients with con-
nective tissue diseases. Chest 130: 553-558, 2006.
9. Kaarteenaho R, Kinnula VL. Diffuse alveolar damage: a common
phenomenon in progressive interstitial lung disorders. Pulm Med
2011: 531302, 2011.
10. Rice AJ, Wells AU, Bouros D, et al. Terminal diffuse alveolar
damage in relation to interstitial pneumonias. An autopsy study.
Am J Clin Pathol 119: 709-714, 2003.
11. Churg A, Müller NL, Silva CI, et al. Acute exacerbation (acute
lung injury of unknown cause) in UIP and other forms of fibrotic
interstitial pneumonias. Am J Surg Pathol 31: 277-284, 2007.
12. Hanaoka R, Kurasawa K, Maezawa R, et al. Reactivation of cy-
tomegalovirus predicts poor prognosis in patients on intensive im-
munosuppressive treatment for collagen-vascular diseases. Mod
Rheumatol Online FirstTM 13 September 2011.
13. Lynch JP 3rd, Hunninghake GW. Pulmonary complications of col-
lagen vascular disease. Ann Rev Med 43: 17-35, 1992.
14. Maeda K, Kimura R, Komura K, et al. Cyclosporine treatment for
polymyositis/dermatomyositis: is it possible to rescue the deterio-
rating cases with interstitial pneumonitis? Scand J Rheumatol 26:
24-29, 1997.
15. Douglas WW, Tazelaar HD, Hartman TE, et al. Polymyositis-
dermatomyositis-associated interstitial lung disease. Am J Respir
Crit Care Med 164: 1182-1185, 2001.
16. Miyazaki E, Ando M, Muramatsu T, et al. Early assessment of
rapidly progressive interstitial pneumonia associated with
amyopathic dermatomyositis. Clin Rheumatol 26: 436-439, 2007.
17. Shimojima Y, Ishii W, Kato T, et al. Intractable skin necrosis and
interstitial pneumonia in amyopathic dermatomyositis, successfully
treated with cyclosporin A. Intern Med 42: 1253-1258, 2003.
Ⓒ 2012 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imonline/index.html