Prophylactic impact of endoscopic treatment for esophageal varices in liver resection: a prospective...
6
ORIGINAL ARTICLE—LIVER, PANCREAS, AND BILIARY TRACT Prophylactic impact of endoscopic treatment for esophageal varices in liver resection: a prospective study Shintaro Yamazaki • Tadatoshi Takayama • Masahiko Nakamura • Tokio Higaki • Shunichi Matsuoka • Shigeaki Mizuno • Mitsuhiko Moriyama Received: 15 March 2013 / Accepted: 21 May 2013 Ó Springer Japan 2013 Abstract Background Prophylactic treatment for esophageal vari- ces has been performed without adequate supporting evi- dence. We assessed the feasibility of prophylactic and follow-up treatment for high-risk esophageal varices in patients with hepatocellular carcinoma (HCC). Methods Patients with HCC were screened prospectively and followed up for esophageal varices and gastroduodenal ulceration. High-risk esophageal varices (huge F3 varices or intermediate F2 varices positive for red color signs) were treated prophylactically. Follow-up endoscopy was per- formed to assess the impact of prophylaxis and changes in varices at 1 week, 1 month, and 6 months after operation. If high-risk varices were found during follow-up, secondary prophylaxis was performed according to the same criteria. Results Among 251 patients with HCC, 81 (32.3 %) had esophageal varices on screening endoscopy. Prophylactic endoscopic treatment was required by 13 patients (1 with F3 varices and 12 with F2 varices positive for red color signs). Ten varices worsened, and 4 varices progressed to high-risk varices requiring endoscopic treatment. No F0 or F1 varices at screening endoscopy progressed to high-risk varices, and no bleeding event occurred during 6 months of preplanned follow-up. A preoperative platelet count of less than 10 9 10 4 /lL (odds ratio: 4.21, 95 % confidence interval 3.11–10.6; p \ 0.001), the presence of splenomegaly (2.87, 2.16–21.8; p = 0.011), and an indocyanine green retention rate at 15 min of greater than 30 % (2.31, 1.88–24.6; p = 0.026) were independent predictors of worsening varices. Conclusions Our protocol for prophylactic and follow-up treatment of high-risk esophageal varices was feasible in patients with HCC. Keywords Esophageal varices Á Liver resection Á Prophylactic treatment Introduction Improved outcomes of liver resection, partially attributed to the use of strict selection criteria, have broadened the indications for surgery in patients with advanced liver disease [1–3]. The presence of esophageal varices is strongly associated with the severity of cirrhosis and is an established risk factor for postoperative adverse events. Esophageal varices are found in 20–30 % of patients with chronic hepatitis and 30–50 % of those with liver cirrhosis [4–7]. Mortality rates of patients who have bleeding varices remain as high as 20–50 % [8–12]. Therefore, good evi- dence had been established for prophylactic intervention of high-risk varices in patients with liver cirrhosis. Perioperative variceal bleeding remains an important issue in patients who undergo liver resection. Portal hemodynamics may be altered by surgical procedures (e.g., liver mobilization and hepatic pedicle clamping during liver resection). Moreover, decreased parenchymal volume after liver resection leads to hyperperfusion of the remnant liver. These factors are thought to exacerbate or promote the development of portal hypertension. Preoperative S. Yamazaki (&) Á T. Takayama Á M. Nakamura Á T. Higaki Department of Digestive Surgery, Nihon University School of Medicine, 30-1 Oyaguchikami-machi, Itabashi-ku, Tokyo 173-8610, Japan e-mail: [email protected] S. Matsuoka Á S. Mizuno Á M. Moriyama Division of Gastroenterology and Hepatology, Department of Medicine, Nihon University School of Medicine, Tokyo, Japan 123 J Gastroenterol DOI 10.1007/s00535-013-0841-y
-
Upload
masahiko-nakamura -
Category
Documents
-
view
213 -
download
1
Transcript of Prophylactic impact of endoscopic treatment for esophageal varices in liver resection: a prospective...
ORIGINAL ARTICLE—LIVER, PANCREAS, AND BILIARY TRACT
Prophylactic impact of endoscopic treatment for esophagealvarices in liver resection: a prospective study
Shintaro Yamazaki • Tadatoshi Takayama •
Masahiko Nakamura • Tokio Higaki • Shunichi Matsuoka •
Shigeaki Mizuno • Mitsuhiko Moriyama
Received: 15 March 2013 / Accepted: 21 May 2013
� Springer Japan 2013
Abstract
Background Prophylactic treatment for esophageal vari-
ces has been performed without adequate supporting evi-
dence. We assessed the feasibility of prophylactic and
follow-up treatment for high-risk esophageal varices in
patients with hepatocellular carcinoma (HCC).
Methods Patients with HCC were screened prospectively
and followed up for esophageal varices and gastroduodenal
ulceration. High-risk esophageal varices (huge F3 varices or
intermediate F2 varices positive for red color signs) were
treated prophylactically. Follow-up endoscopy was per-
formed to assess the impact of prophylaxis and changes in
varices at 1 week, 1 month, and 6 months after operation. If
high-risk varices were found during follow-up, secondary
prophylaxis was performed according to the same criteria.
Results Among 251 patients with HCC, 81 (32.3 %) had
esophageal varices on screening endoscopy. Prophylactic
endoscopic treatment was required by 13 patients (1 with F3
varices and 12 with F2 varices positive for red color signs).
Ten varices worsened, and 4 varices progressed to high-risk
varices requiring endoscopic treatment. No F0 or F1 varices
at screening endoscopy progressed to high-risk varices, and
no bleeding event occurred during 6 months of preplanned
follow-up. A preoperative platelet count of less than
10 9 104/lL (odds ratio: 4.21, 95 % confidence interval
3.11–10.6; p \ 0.001), the presence of splenomegaly (2.87,
2.16–21.8; p = 0.011), and an indocyanine green retention
rate at 15 min of greater than 30 % (2.31, 1.88–24.6; p =
0.026) were independent predictors of worsening varices.
Conclusions Our protocol for prophylactic and follow-up
treatment of high-risk esophageal varices was feasible in
patients with HCC.
Keywords Esophageal varices � Liver resection �Prophylactic treatment
Introduction
Improved outcomes of liver resection, partially attributed
to the use of strict selection criteria, have broadened the
indications for surgery in patients with advanced liver
disease [1–3]. The presence of esophageal varices is
strongly associated with the severity of cirrhosis and is an
established risk factor for postoperative adverse events.
Esophageal varices are found in 20–30 % of patients with
chronic hepatitis and 30–50 % of those with liver cirrhosis
[4–7]. Mortality rates of patients who have bleeding varices
remain as high as 20–50 % [8–12]. Therefore, good evi-
dence had been established for prophylactic intervention of
high-risk varices in patients with liver cirrhosis.
Perioperative variceal bleeding remains an important
issue in patients who undergo liver resection. Portal
hemodynamics may be altered by surgical procedures (e.g.,
liver mobilization and hepatic pedicle clamping during
liver resection). Moreover, decreased parenchymal volume
after liver resection leads to hyperperfusion of the remnant
liver. These factors are thought to exacerbate or promote
the development of portal hypertension. Preoperative
S. Yamazaki (&) � T. Takayama � M. Nakamura � T. Higaki
Department of Digestive Surgery, Nihon University School of
Medicine, 30-1 Oyaguchikami-machi, Itabashi-ku,
Tokyo 173-8610, Japan
e-mail: [email protected]
S. Matsuoka � S. Mizuno � M. Moriyama
Division of Gastroenterology and Hepatology, Department of
Medicine, Nihon University School of Medicine, Tokyo, Japan
123
J Gastroenterol
DOI 10.1007/s00535-013-0841-y

endoscopic screening and prophylactic treatment of varices
are thus important issues in patients who undergo liver
resection [2, 13, 14].
The size, form, and color of varices are independent
predictors of bleeding [11–15]. However, standard proto-
cols for the prophylactic treatment of high-risk varices
before liver resection are unavailable, in part owing to the
lack of prospective studies providing a firm basis for cur-
rently used criteria [2, 16]. Moreover, no study has shown
which category of patients are at risk for the growth of
varices after surgical procedures. We therefore prospec-
tively assessed the impact of prophylactically treating
esophageal varices and studied postoperative changes in
such varices in patients with HCC who underwent liver
resection.
Methods
Inclusion criteria
The eligibility criteria included liver function of Child-
Pugh class A or B and curative hepatic resection for
hepatocellular carcinoma (HCC) without severe comor-
bidities. Exclusion criteria included a history of endo-
scopic, radiologic, or surgical treatment for esophageal
varices. Patients who had large gastric varices which
require balloon-occluded retrograde transvenous oblitera-
tion and who had active bleeding gastroduodenal ulceration
were excluded. Patients who had a history of esophageal or
gastric surgery or serious medical conditions that precluded
repeat endoscopy were also excluded.
Three-phase, contrast-enhanced, dynamic computed
tomographic (CT) scanning was performed in all patients
preoperatively. The diameter of the spleen was measured
on abdominal CT scans, and a major diameter of more than
12 cm was defined as splenomegaly [17]. Written informed
consent was obtained from all patients. An English-lan-
guage summary of the protocol is available at the Clinical
Trials Registry managed by the University Hospital Med-
ical Information Network in Japan (http://www.umin.ac.jp/
ctr/index.htm: UMIN000008616).
Screening and follow up endoscopy
Upper gastrointestinal endoscopy was performed at 4 dif-
ferent times (before operation and at 1 week, 1 month, and
6 months after operation). Preoperative endoscopy was
done to assess the need for prophylactic treatment of
esophageal varices [11, 12]. At follow-up endoscopy, the
change in form, color, and presence of red-color (RC) signs
of varices were evaluated [10–12, 18]. The effectiveness of
prophylactic therapy and the need for additional treatment
were assessed at the same times as follow-up endoscopy.
Liver resection was scheduled to be performed after an
interval of at least 2 weeks in patients who underwent
esophageal variceal ligation (EVL) or endoscopic clipping
of ulcers.
Indications and treatment protocol
Prophylactic treatment of esophageal varices was per-
formed according to the General Rules for Recording
Endoscopic Findings of Esophagogastric Varices (The
Japan Society for Portal Hypertension), based on the
Beppu’s classification [11]. EVL was indicated for the
management of F3 varices (largest size) or F2 varices
(enlarged tortuous) or blue varices positive for red color
signs. EVL was performed using an endoscopic ligation
device (Pneumatic EVL Device; Sumitomo Bakelite,
Tokyo, Japan). The ligation band was placed around the
varix in a spiral fashion, starting from the proximal side
and then progressing superiorly at 1-cm intervals. Addi-
tional sessions of EVL were performed every 2 weeks
using the same method until the varices were eradicated. At
follow-up endoscopy, secondary prophylaxis was per-
formed as required according to the same criteria as pri-
mary prophylaxis in patients who had signs of worsening
varices, ulceration, or both [18].
Proton-pump inhibitors were given to patients in whom
ulcers were diagnosed. Otherwise, the study protocol
required that all patients receive a proton-pump inhibitor
for 3 days after liver resection to prevent operation-related
stress ulcers and portal hypertensive gastropathy.
Surgical procedure
The indications for surgical resection and the operative
procedures were in accordance with Makuuchi’s criteria
[19]. Anatomic resection of Couinaud’s segment was the
first-line operative procedure for hepatocellular carcinoma.
Minor hepatectomy was defined as limited resection or
resection of up to two Couinaud’s segments, and major
hepatectomy was defined as resection of more than two
segments. Hepatic parenchymal transection was guided
ultrasonographically and performed by the clamp-crushing
method with the inflow-blood-occlusion technique, and
Glisson’s pedicle was tied and divided with silk thread, as
described previously [20].
Statistical analysis
Data are expressed as medians and ranges or as absolute
values and percentages. Student’s t test, the v2 test, and
Fisher’s exact test were used for univariate analysis as
required. Multivariate analysis was performed by logistic
J Gastroenterol
123
regression. Odds ratios (OR) with 95 % confidence intervals
(CI) were derived from logistic regression analysis. The per-
iod to the onset of infection was analyzed using the Kaplan–
Meier method and compared by the log-rank test. p values of
\0.05 were considered to indicate statistical significance. All
analyses were performed using a statistical software package
(JMP v.9.0; SAS Institute, Cary, NC, USA).
Results
Patients
Between 2008 and 2010, a total of 371 consecutive patients
were studied prospectively (Fig. 1). Preoperative endos-
copy performed in all patients. The underlying diagnosis
was HCC in 269 patients, metastatic liver cancer in 87,
gallbladder cancer in 8, bile duct cancer in 5, and others in
2. We excluded the non-HCC patients from this study
because the risk of esophageal varices was obviously low
(Table 1). Also, a total of 18 patients with HCC were
excluded: 9 patients had a history of esophageal or gastric
surgery, 4 had a history of variceal treatment, 3 had large
gastric varices that required preoperative treatment, and 2
were excluded for other reasons. At screening endoscopy
of 253 HCC patients, gastroduodenal ulceration was pres-
ent in 29 patients (11.6 %), including 2 who required
endoscopic treatment. Thus, two patients were excluded
from this study. Finally, 251 HCC patients were included
and followed in this study.
Laboratory background in presence or absence
of esophageal varices
The following laboratory variables differed significantly
according to the presence (n = 81) or absence (n = 170)
of esophageal varices (Table 2): platelet count [median:
10.8 9 104/lL, (range 5.6–27.9) vs. 15.9, (4.2–54.9),
p \ 0.001], albumin [3.6 g/dL, (2.7–5.7) vs. 3.9, (2.8–6.1),
p = 0.031], total bilirubin [0.84 mg/dL, (0.28–1.75) vs.
0.61, (0.19–1.60), p \ 0.001], cholinesterase [200 IU/L,
(39–382) vs. 241, (19–481), p \ 0.001], ammonia [49 lg/
dL, (16–155) vs. 42, (15–121), p = 0.005], and indocya-
nine green retention rate at 15 min [15.4 %, (3.7–46.0) vs.
10.9 %, (2.1–37.7), p \ 0.001]. The prevalences of Child
class B disease (21.8 vs. 7.6 %; p = 0.004) and spleno-
megaly (79.5 vs. 45.7 %; p \ 0.001) were significantly
higher among patients with varices.
Screening endoscopy and prophylactic treatment
On screening endoscopy, esophageal varices were found in
81 patients (32.3 %) (Table 3). There were 49 cases of
color blue varices. One patient had a huge varix (F3), and
19 had intermediate varices (F2). Twelve of the F2 patients
had RC signs on varices, but 5 had no RC signs. Conse-
quently, a total of 13 high-risk varices (1 of F3 varix and 12
of F2 varices with RC signs) were prophylactically treated
by the present protocol. EVL was effective in all patients.
There was no bleeding event related to prophylactic
treatment by EVL. Ulceration of the esophagus was found
after EVL in only 1 patient, in whom surgery was post-
poned for 2 weeks.
Follow-up endoscopy and additional treatment
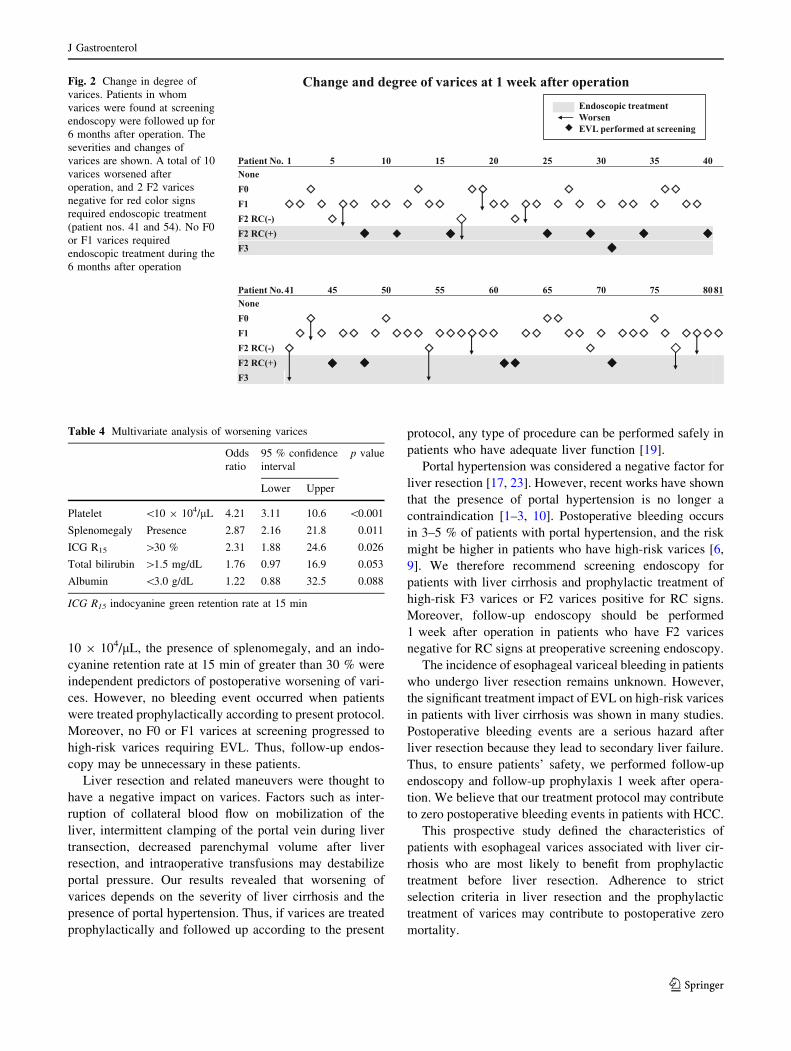
The 81 varices found on screening endoscopy were fol-
lowed up for 6 months (Fig. 2). One week after operation,
269 Hepatocellular carcinoma patients
371 Liver tumor patients102 Excluded
87 Metastatic liver cancer8 Gallbladder cancer5 Bile duct cancer2 Others
18 Excluded9 Esophageal or gastric operation4 History of esophageal varices treatment 3 Gastric varices which required treatment2 Others
2 Excluded2 Endoscopic clipping for gastric ulceration
251 Follow-up endoscopy1 week, 1 month, 6 month
Flow of patients
253 Screening endoscopyProphylactic treatment performed: F3 or F2 red color signs
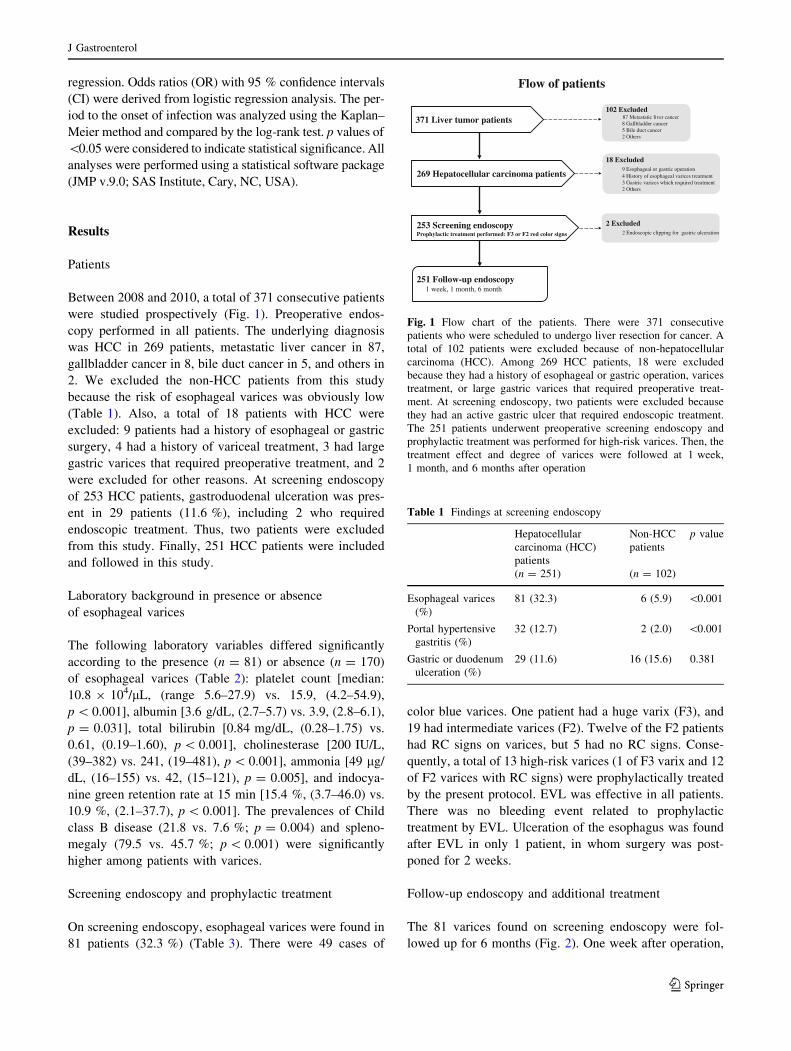
Fig. 1 Flow chart of the patients. There were 371 consecutive
patients who were scheduled to undergo liver resection for cancer. A
total of 102 patients were excluded because of non-hepatocellular
carcinoma (HCC). Among 269 HCC patients, 18 were excluded
because they had a history of esophageal or gastric operation, varices
treatment, or large gastric varices that required preoperative treat-
ment. At screening endoscopy, two patients were excluded because
they had an active gastric ulcer that required endoscopic treatment.
The 251 patients underwent preoperative screening endoscopy and
prophylactic treatment was performed for high-risk varices. Then, the
treatment effect and degree of varices were followed at 1 week,
1 month, and 6 months after operation
Table 1 Findings at screening endoscopy
Hepatocellular
carcinoma (HCC)
patients
Non-HCC
patients
p value
(n = 251) (n = 102)
Esophageal varices
(%)
81 (32.3) 6 (5.9) \0.001
Portal hypertensive
gastritis (%)
32 (12.7) 2 (2.0) \0.001
Gastric or duodenum
ulceration (%)
29 (11.6) 16 (15.6) 0.381
J Gastroenterol
123

65 patients (25.9 %) had varices, and 23 (9.2 %) had
ulcerations. A total of 10 varices worsened 1 week after
operation. Two F2 varices progressed to F3 varices (patient
nos. 41 and 54), and RC signs were found on two F2
varices (patient nos. 17 and 77) 1 week after operation. An
additional session of EVL was thus performed in 4 patients.
At 1 month and 6 months, no varices progress to high-risk
varices during 6 months’ follow-up. Then, there was no
need for additional endoscopic treatment. No F0 or F1
varices progressed to high-risk varices requiring endo-
scopic treatment during the 6 months after treatment.
There was no postoperative bleeding event, and the
effect of treatment according to the study protocol con-
tinued for 6 months. There were two duodenal ulcers that
required endoscopic clipping 1 week after operation.
Risk analysis of worsening esophageal varices
Multivariate analysis revealed 3 independent predictors of
worsening varices (Table 4). A platelet count of less than
10 9 104/lL was the strongest predictor (OR: 4.21, 95 %
CI 3.11–10.6; p \ 0.001). The presence of splenomegaly
(OR: 2.87, 95 % CI 2.16–21.8; p = 0.011) and an indo-
cyanine retention rate at 15 min of greater than 30 % (OR:
2.31, 95 % CI 1.88–24.6; p = 0.026) were also significant
predictors of worsening esophageal varices.
Discussion
None of the 276 patients with HCC who were consecu-
tively enrolled in this prospective study had bleeding
events. Our results indicated that F3 varices or F2 varices
positive for RC signs should undergo prophylactic EVL.
The treatment effect continued for 6 months after liver
resection in accordance with our protocol. In contrast, F0
or F1 varices at screening endoscopy did not progress to
high-risk varices requiring additional EVL.
The feasibility of prophylactic EVL has been demon-
strated in patients who have liver cirrhosis with or without
HCC [18, 21, 22]. Therefore, prophylactic EVL has been
performed in patients scheduled to undergo liver resection
for HCC [2, 15, 18]. However, postoperative changes in the
severity of varices for patients who receive prophylactic
treatment is not well understood. To date, no study has
confirmed these changes in varices or prospectively eval-
uated the characteristics of varices that require prophylactic
treatment. Our study was designed to address these unan-
swered questions.
Our results showed that the prophylactic therapy of high-
risk varices according to our protocol was feasible and may
minimize the risk of postoperative bleeding events. Our risk
analysis demonstrated that a platelet count of less than
Table 2 Preoperative characteristics of esophageal varices
Varices p value
Presence
(n = 81)
Absence
(n = 170)
Hepatitis viral infection
(%)
62 (79.5) 142 (82.1) 0.411
Tumor diameter (mm) 24 (11–105) 28 (10–205) 0.344
Number of tumors 1 (1–3) 1 (1–4) 0.974
Phenotype (expansive
growth) (%)
17 (22.1) 40 (25.5) 0.569
Vascular invasion (%) 16 (20.5) 45 (26.0) 0.311
Platelets (104/lL) 10.8
(5.6–27.9)
15.9
(42–54.9)
\0.001
Albumin (g/dL) 3.6 (2.7–5.7) 3.9 (2.8–6.1) 0.031
Total bilirubin (mg/dL) 0.84
(0.28–1.75)
0.61
(0.19–1.60)
\0.001
Aspartate
aminotransferase (IU/L)
38 (11–96) 34 (5–296) 0.523
Cholinesterase (IU/L) 200 (39–382) 241 (19–481) \0.001
Ammonia (lg/dL) 49 (16–155) 42 (15–121) 0.005
Prothrombin time (INR) 1.00
(0.83–1.19)
0.97
(0.86–1.08)
0.508
ICG R15 (%) 15.4
(3.7–46.0)
10.9
(2.1–37.7)
\0.001
Child-Pugh B (%) 17 (21.8) 13 (7.6) 0.004
Splenomegaly (%) 62 (79.5) 79 (45.7) \0.001
ICG R15 indocyanine green retention rate at 15 min, INR international
normalized rate
Table 3 Endoscopic screening and prophylactic treatment in 251
patients with HCC
Screening Follow-up
1 week 1 month 6 months
Esophageal
varices
81
(32.3 %)
65
(25.9 %)
59
(23.5 %)
58
(23.1 %)
Form (F0/F1/F2/
F3)
12/51/17/
1
17/39/7/2 12/37/7/0 9/40/9/0
Blue color
varices
49 52 32 29
Presence of red
color signs
12 2 0 0
Endoscopic
treatment
13 4 0 0
Ulcerationa 29
(11.6 %)
23
(9.2 %)
14
(5.6 %)
6 (2.4 %)
Gastric 25 21 18 4
Endoscopic
treatment
2 0 0 0
Duodenum 6 5 3 2
Endoscopic
treatment
0 2 0 0
a Total number of patients
J Gastroenterol
123
10 9 104/lL, the presence of splenomegaly, and an indo-
cyanine retention rate at 15 min of greater than 30 % were
independent predictors of postoperative worsening of vari-
ces. However, no bleeding event occurred when patients
were treated prophylactically according to present protocol.
Moreover, no F0 or F1 varices at screening progressed to
high-risk varices requiring EVL. Thus, follow-up endos-
copy may be unnecessary in these patients.
Liver resection and related maneuvers were thought to
have a negative impact on varices. Factors such as inter-
ruption of collateral blood flow on mobilization of the
liver, intermittent clamping of the portal vein during liver
transection, decreased parenchymal volume after liver
resection, and intraoperative transfusions may destabilize
portal pressure. Our results revealed that worsening of
varices depends on the severity of liver cirrhosis and the
presence of portal hypertension. Thus, if varices are treated
prophylactically and followed up according to the present
protocol, any type of procedure can be performed safely in
patients who have adequate liver function [19].
Portal hypertension was considered a negative factor for
liver resection [17, 23]. However, recent works have shown
that the presence of portal hypertension is no longer a
contraindication [1–3, 10]. Postoperative bleeding occurs
in 3–5 % of patients with portal hypertension, and the risk
might be higher in patients who have high-risk varices [6,
9]. We therefore recommend screening endoscopy for
patients with liver cirrhosis and prophylactic treatment of
high-risk F3 varices or F2 varices positive for RC signs.
Moreover, follow-up endoscopy should be performed
1 week after operation in patients who have F2 varices
negative for RC signs at preoperative screening endoscopy.
The incidence of esophageal variceal bleeding in patients
who undergo liver resection remains unknown. However,
the significant treatment impact of EVL on high-risk varices
in patients with liver cirrhosis was shown in many studies.
Postoperative bleeding events are a serious hazard after
liver resection because they lead to secondary liver failure.
Thus, to ensure patients’ safety, we performed follow-up
endoscopy and follow-up prophylaxis 1 week after opera-
tion. We believe that our treatment protocol may contribute
to zero postoperative bleeding events in patients with HCC.
This prospective study defined the characteristics of
patients with esophageal varices associated with liver cir-
rhosis who are most likely to benefit from prophylactic
treatment before liver resection. Adherence to strict
selection criteria in liver resection and the prophylactic
treatment of varices may contribute to postoperative zero
mortality.
Fig. 2 Change in degree of
varices. Patients in whom
varices were found at screening
endoscopy were followed up for
6 months after operation. The
severities and changes of
varices are shown. A total of 10
varices worsened after
operation, and 2 F2 varices
negative for red color signs
required endoscopic treatment
(patient nos. 41 and 54). No F0
or F1 varices required
endoscopic treatment during the
6 months after operation
Table 4 Multivariate analysis of worsening varices
Odds
ratio
95 % confidence
interval
p value
Lower Upper
Platelet \10 9 104/lL 4.21 3.11 10.6 \0.001
Splenomegaly Presence 2.87 2.16 21.8 0.011
ICG R15 [30 % 2.31 1.88 24.6 0.026
Total bilirubin [1.5 mg/dL 1.76 0.97 16.9 0.053
Albumin \3.0 g/dL 1.22 0.88 32.5 0.088
ICG R15 indocyanine green retention rate at 15 min
J Gastroenterol
123

Acknowledgments This study was supported by the grant from
2013 Hagiwara fund, Nihon University School of Medicine.
Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Capussotti L, Ferrero A, Vigano L, et al. Portal hypertension:
contraindication to liver surgery? World J Surg. 2006;30:992–9.
2. Ishizawa T, Hasegawa K, Aoki T, et al. Neither multiple tumors
nor portal hypertension are surgical contraindications for hepa-
tocellular carcinoma. Gastroenterology. 2008;134:1908–16.
3. Kawano Y, Sasaki A, Kai S, et al. Short- and long-term outcomes
after hepatic resection for hepatocellular carcinoma with con-
comitant esophageal varices in patients with cirrhosis. Ann Surg
Oncol. 2008;15:1670–6.
4. Brocchi E, Caletti G, Brambilla G, et al. Prediction of the first
variceal hemorrhage in patients with cirrhosis of the liver and
esophageal varices. A prospective multicenter study. North Ital-
ian Endoscopic Club for the Study and Treatment of Esophageal
Varices. N Engl J Med. 1988;319:983–9.
5. D’Amico G, Pagliaro L, Bosch J. The treatment of portal
hypertension: a meta-analytic review. Hepatology. 2003;22:
332–54.
6. de Franchis R. Evolving consensus in portal hypertension. Report
of the Baveno IV consensus workshop on methodology of diag-
nosis and therapy in portal hypertension. J Hepatol. 2005;43:
167–76.
7. Bambha K, Kim WR, Pedersen R, et al. Predictors of early re-
bleeding and mortality after acute variceal haemorrhage in
patients with cirrhosis. Gut. 2008;57:814–20.
8. Spina GP, Arcidiacono R, Bosch J, et al. Gastric endoscopic
features in portal hypertension: final report of a consensus con-
ference, Milan, Italy, September 19, 1992. J Hepatol. 1994;21:
461–7.
9. del Olmo JA, Pena A, Serra MA, et al. Predictors of morbidity
and mortality after the first episode of upper gastrointestinal
bleeding in liver cirrhosis. J Hepatol. 2000;32:19–24.
10. Nidegger D, Ragot S, Berthelemy P, et al. Cirrhosis and bleeding:
the need for very early management. J Hepatol. 2003;39:509–14.
11. Beppu K, Inokuchi K, Koyanagi N, et al. Prediction of variceal
hemorrhage by esophageal endoscopy. Gastrointest Endosc.
1981;27:213–8.
12. Merkel C, Zoli M, Siringo S, et al. Prognostic indicators of risk
for first variceal bleeding in cirrhosis: a multicenter study in 711
patients to validate and improve the North Italian Endoscopic
Club (NIEC) index. Am J Gastroenterol. 2000;95:2915–20.
13. Tomikawa M, Shimabukuro R, Okita K, et al. Propranolol alone
may not be acceptable to prevent first esophageal variceal
bleeding in Japanese cirrhotic patients: randomized controlled
trial. J Gastroenterol Hepatol. 2004;19:576–81.
14. Carbonell N, Pauwels A, Serfaty L, et al. Improved survival after
variceal bleeding in patients with cirrhosis over the past two
decades. Hepatology. 2004;40:652–9.
15. Snady H, Feinman L. Prediction of variceal hemorrhage: a pro-
spective study. Am J Gastroenterol. 1988;83:519–25.
16. Yeo W, Sung JY, Ward SC, et al. A prospective study of upper
gastrointestinal hemorrhage in patients with hepatocellular car-
cinoma. Dig Dis Sci. 1995;40:2516–21.
17. Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carci-
noma: the BCLC staging classification. Semin Liver Dis.
1999;19:329–38.
18. Chen WC, Hou MC, Lin HC, et al. Feasibility and potential
benefit of maintenance endoscopic variceal ligation in patients
with unresectable hepatocellular carcinoma and acute esophageal
variceal hemorrhage: a controlled trial. Gastrointest Endosc.
2001;54:18–23.
19. Makuuchi M, Kosuge T, Takayama T, et al. Surgery for small
liver cancers. Semin Surg Oncol. 1993;9:298–304.
20. Takayama T, Makuuchi M, Kubota K, et al. Randomized com-
parison of ultrasonic vs clamp transection of the liver. Arch Surg.
2001;136:922–8.
21. Chalasani N, Kahi C, Francois F, et al. Improved patient survival
after acute variceal bleeding: a multicenter, cohort study. Am J
Gastroenterol. 2003;98:653–9.
22. Imperiale TF, Chalasani N. A meta-analysis of endoscopic vari-
ceal ligation for primary prophylaxis of esophageal variceal
bleeding. Hepatology. 2001;33:802–7.
23. Bruix J, Castells A, Bosch J, et al. Surgical resection of hepato-
cellular carcinoma in cirrhotic patients: prognostic value of pre-
operative portal pressure. Gastroenterology. 1996;111:1018–22.
J Gastroenterol
123