
Preliminary Analyses of Recruiting Centre for Mindfulness Research and Practice Elaine...
36
Staying Well after Depression Preliminary Analyses of Recruiting Centre for Mindfulness Research and Practice Elaine Weatherley-Jones & Mariel Jones Presentation for the ‘Mindfulness Now’ conference, Bangor, 10 th April, 2011
-
Upload
adrienne-duffell -
Category
Documents
-
view
213 -
download
0
Transcript of Preliminary Analyses of Recruiting Centre for Mindfulness Research and Practice Elaine...
Staying Well after Depression
Preliminary Analyses of Recruiting
Centre for Mindfulness Research and Practice
Elaine Weatherley-Jones & Mariel Jones
Presentation for the ‘Mindfulness Now’ conference, Bangor, 10th April, 2011
Research AimsTo explore the benefits of two new
psychological treatments for people who have been depressed and suicidal in the past:
Mindfulness-Based Cognitive Therapy (MBCT) – a group-based treatment programme that combines training in mindfulness meditation and yoga with cognitive therapy
Cognitive Psycho-Education (CPE) identical in content to MBCT, except there is no meditation component
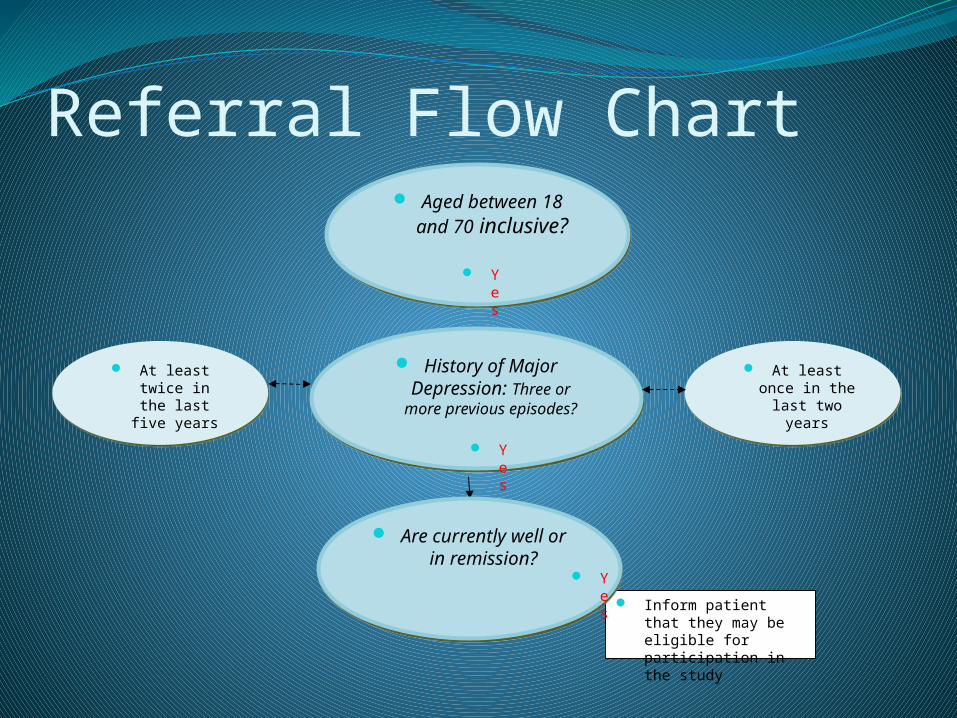
Referral Flow Chart Aged between 18 and
70 inclusive? Aged between 18 and
70 inclusive?
History of Major Depression: Three or more
previous episodes?
History of Major Depression: Three or more
previous episodes?
Inform patient that they may be eligible for participation in the study
Are currently well or in remission?
Are currently well or in remission?
At least once in the last two
years
At least once in the last two
years
At least twice in the last five years
At least twice in the last five years
Yes
Yes
Yes
Potential Barriers IdentifiedStigma attached to depression and suicidality
Largely rural communities
Welsh socio-cultural ethos
Low population density
Low SES area
Large geographical area
Bangor site recruitment target/outcome figures
180 participants for each site (Bangor/Oxford)
771 contacted the trial in Bangor
519 screened
202 assessed
123 randomised
Strategy for Early Cohorts
Encouraging direct referral by primary and secondary care professionals
Encouraging self-referral using poster campaign, media and advertising

Strategy in later Cohorts
Direct referral, change in emphasis to searches of patient databases (managed by NISCHR CRC )
Media, increasing focus on TV and radio coverage to include an advert on a local radio station and use of Web based advertising
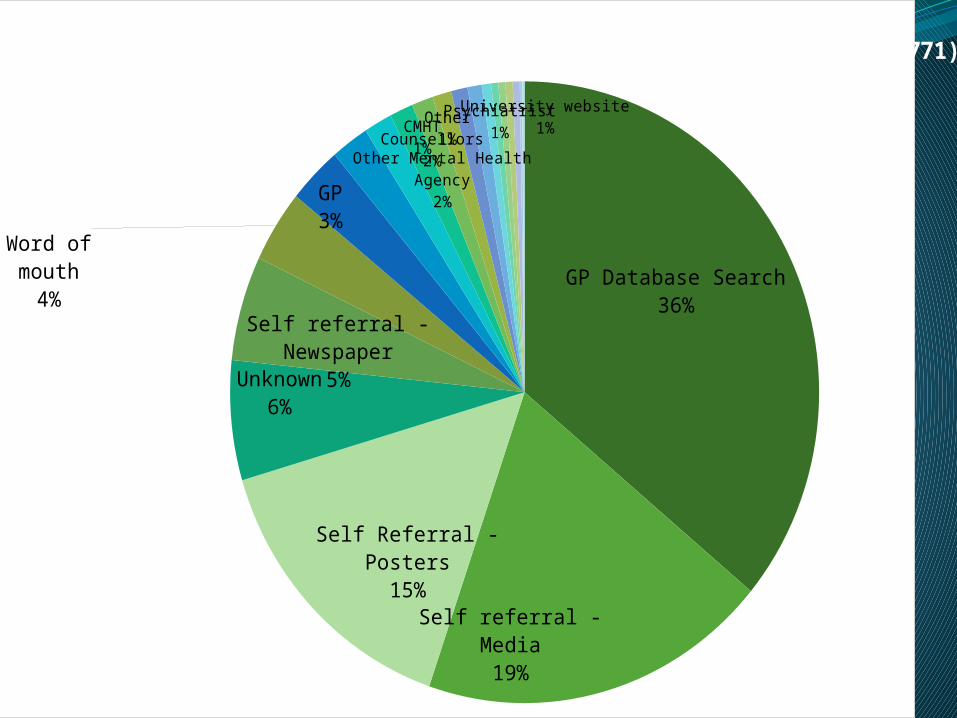
GP Database Search36%
Self referral - Media19%
Self Referral - Posters15%
Unknown6%
Self referral - Newspaper5%
Word of mouth
4%
GP3%
Other Mental Health Agency2%
Counsellors2%
CMHT1%
Other1%
Psychiatrist1%
University website1%
Source of recruiting (N=771)

GP Database Search33%
Self referral - Media11%
Self Referral - Posters24%
Unknown2%Self referral -
Newspaper7%
Word of mouth4%
GP7%
Other Mental Health Agency2%
Counsellors2%
CMHT1%
Other1%
Psychiatrist2%
University website2%
Source of people randomised (N=123)
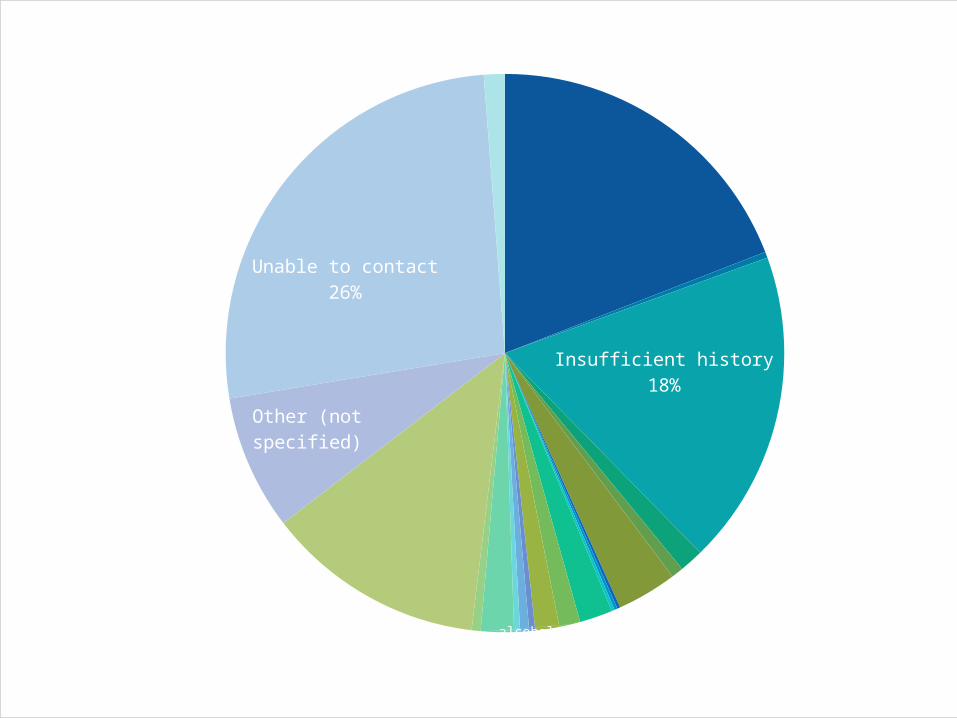
Currently depressed19% suicidal
0%
Insufficient history18%
no prior suicidaltiy1%
Current antidepressant1%
Recovered since CBT0%
current psychotherapy0%alcohol subst
2%eating disorder1%
bipolar1%
ocd1%
current meditation practice2%
unable to attend classes
13%
Other (not specified)
Unable to contact26%
Does not want to take part1%
Reasons for ineligibility at screening N=548

Currently depressed24%
suicidal2%
Insufficient history31%
no prior suicidaltiy2%
Recovered since CBT2%
current psychotherapy2%
alcohol/substance
misuse6%
bipolar4%
mania present2%
current meditation practice2%
unable to attend classes4%
DNA assessments2%
Other (not specified)
10%
Unable to contact6%
Reasons for ineligibility at assessment (N=79)
Back to what we learned
ConclusionsThe high level of interest in this trial suggests that many
people in North Wales are suffering with depression and experience a gap in service provision
The feasibility of recruiting in a largely rural, bilingual, low SES area is promising despite the barriers to recruitment
Posters campaigns and media coverage are the most effective means for generating self-referrals
Radio advertising is recommended as being very effective in generating high levels of interest, however it requires careful orchestrating to avoid an influx of ineligible people as well as people who cannot be contacted back
Recruiting via direct referral from primary or secondary mental health services is poorly indicated for people who are currently well
Data base searches and self-referrals have proven to be the most effective strategy for this population
Collaborative working with NISCHR CRC plays a key role in facilitating Primary Care data searches
Recruitment in culturally diverse areas such as North Wales requires a flexible recruitment strategy that is responsive
Collaboration between (similarly oriented) research teams that concurrently liaise with GP surgeries and other health care professionals is indicated to reduce confusion and competition, as well as to share support and expertise

MBCT in Primary care
A pilot of feasibility and effectiveness
Sholto Radford (CMRP)[email protected]
MBCT within a Primary care setting
WaMH in PC funding to deliver MBCT in GP surgery (Victoria Doc Caernarfon)
Presentation to GP’s and information packs given
GP’s referred patients for past depression, current mild to moderate depression, anxiety disorders and CFS.
Interview with teacher to assess suitability
Methodology Single sample repeated measures design
(pre/post & six month follow up)
Primary outcomes - depression (HADS, PHQ-9) and anxiety (HADS)
Secondary outcomes - rumination (RRS), self compassion (SCS) and well being (WBI-5).
GP survey (posted to 52 GPs in Arfon and South Anglesey)
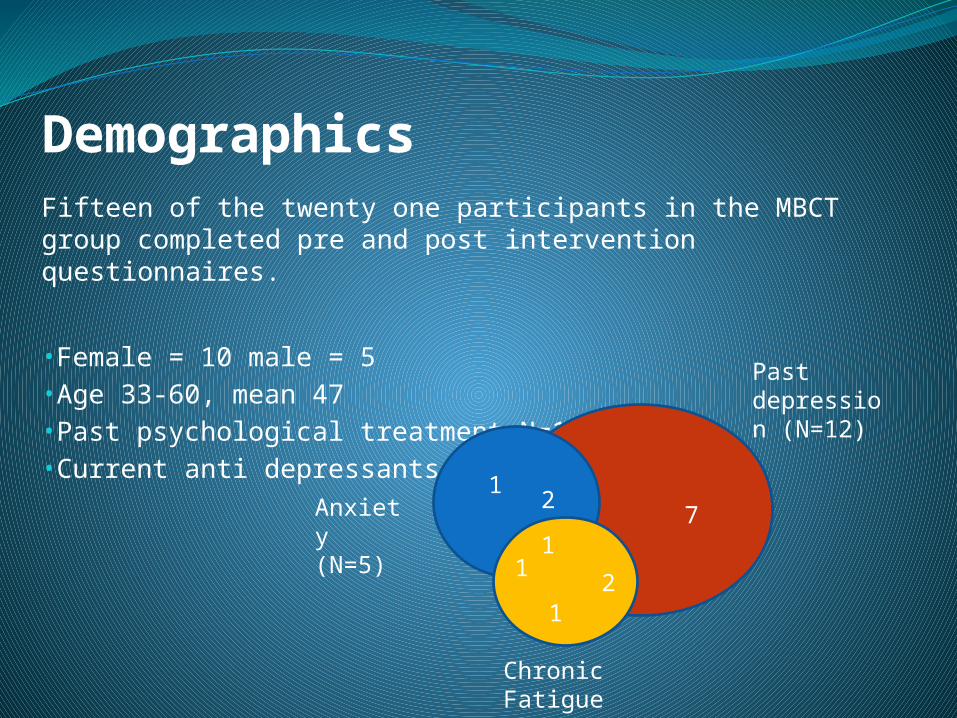
DemographicsFifteen of the twenty one participants in the MBCT group completed pre and post intervention questionnaires.
•Female = 10 male = 5•Age 33-60, mean 47•Past psychological treatment N=10•Current anti depressants N=9
71
1
2
12
1
Past depression (N=12)
Chronic Fatigue Syndrome (N=5)
Anxiety (N=5)
Appropriate referral Low drop out (two of the twenty one MBCT participant's)High attendance Positive feedback from participant's (high ratings of
importance and positive comments)
Survey revealed GP’s (N=10) Supported a shift to more preventative methods for dealing with mental
health problems Felt that Primary care was the most suitable setting for MBCT Would regularly refer patients if it was routinely available (6-30 per year M=
14) Felt that counsellors would be the most suitable professional group to deliver
MBCT in primary care Were not generally enthusiastic about receiving training in MBCT themselves
Feasibility
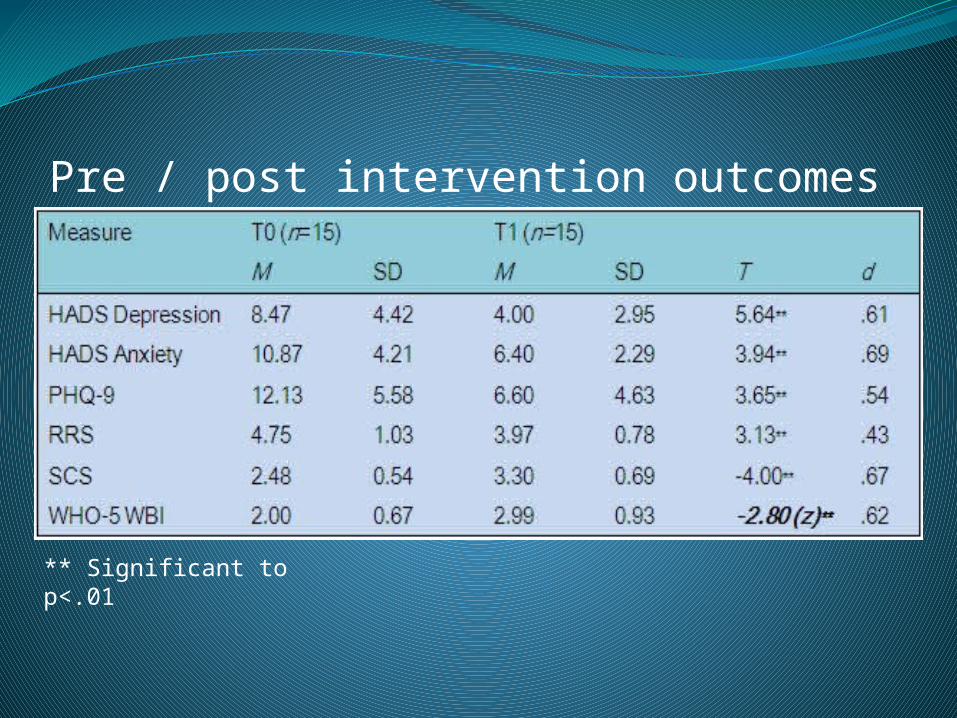
Pre / post intervention outcomes
** Significant to p<.01

Depression – HADS
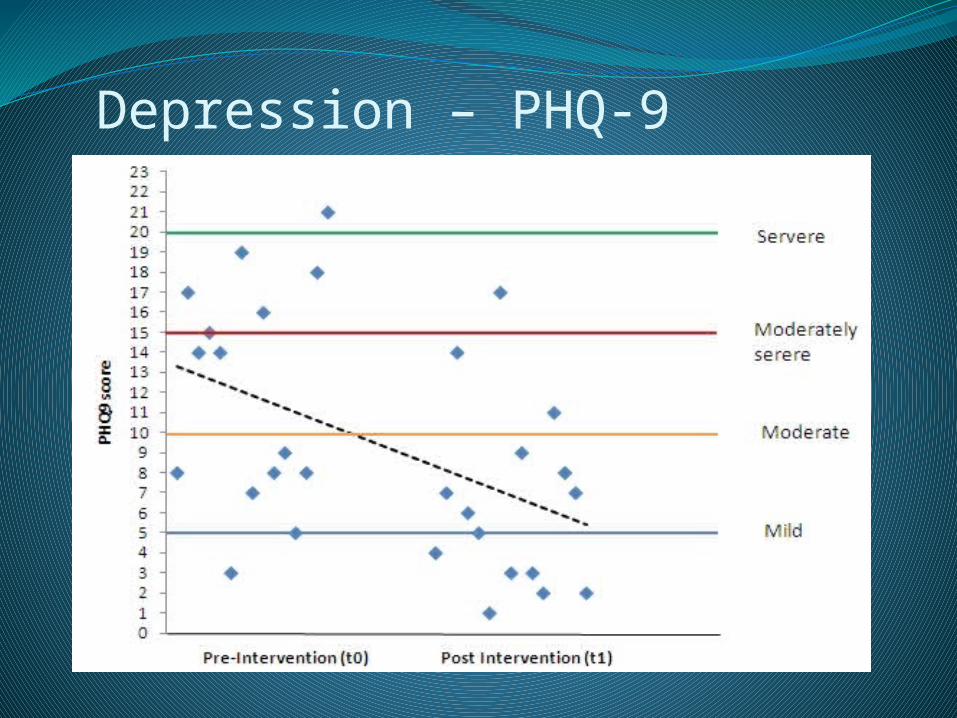
Depression – PHQ-9

Anxiety – HADS
Encouraging preliminary findings
Appears to be effective for individuals with mild and moderate depression
Leads to positive changes in Rumination, Self compassion and well being
Six month follow up data will confirm if outcomes are maintained
Limitations (sample size , absence of control group)
Conclusions
Acknowledgements
Eluned GoldDr Gareth OwenRebecca CraneCatrin EamesStephanie HopwoodSophie PodmoreKatrina DrewHannah Owen

Evaluating mindfulness-based interventions for the general
population Catrin Eames
Centre for Mindfulness Research and [email protected]
Presentation for the ‘Mindfulness Now’ conference, Bangor, 10th April, 2011.

Acknowledgements
• Prof. Richard Bentall, Filippo Varese, Alisa Udachina• Dr. Val Morrison, Polly Barr• Judith Soulsby, Anne Douglas, Rebecca Crane, Sholto Radford
Research aims• Increasing evaluations of mindfulness in clinical settings • CMRP deliver 3 eight-week courses annually• Increasing interest (and waiting lists!) but no formal evaluation of the CMRP courses• Systematic evaluation of courses delivered to general population groups
• assessing the psychological factors believed to be influenced by mindfulness training
• Routine assessment of response to mindfulness training
Methodology• Pre- (T0) and post- (T1) intervention, 6 (T2) and 12 (T3) month follow-up • Intervention and waiting-list control• No exclusion criteria• Measures
• Demographic questionnaire (T0)• Hospital Anxiety Depression Questionnaire (HADS; Zigmond &
Snaith, 1983)• Perceived Stress Scale (Cohen, Kamarck & Mermelstein, 1983)• Well-Being Index 5 (World Health Organization, 1996)• Five Factor Mindfulness Questionnaire (Baer et al., 2006)• Ruminative Responses Scale (Nolen-Hoeksema, 1991)• Self Compassion Scale (Neff, 2003)
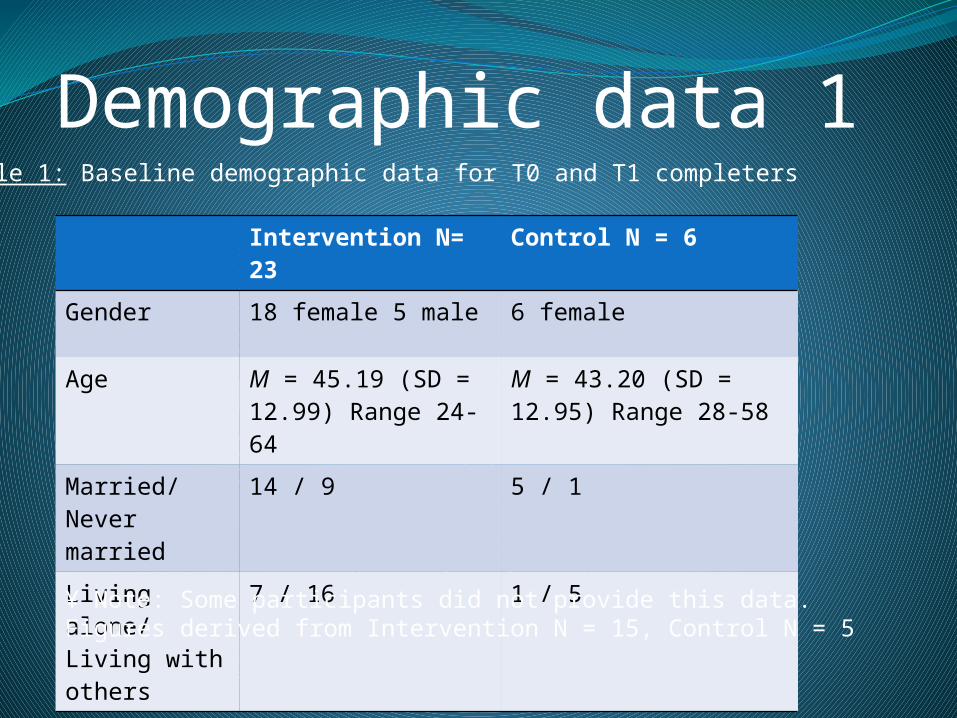
Demographic data 1
Intervention N= 23
Control N = 6
Gender 18 female 5 male 6 female
Age M = 45.19 (SD = 12.99) Range 24-64
M = 43.20 (SD = 12.95) Range 28-58
Married/Never married
14 / 9 5 / 1
Living alone/ Living with others
7 / 16 1 / 5
Table 1: Baseline demographic data for T0 and T1 completers
¥ Note: Some participants did not provide this data. Figures derived from Intervention N = 15, Control N = 5
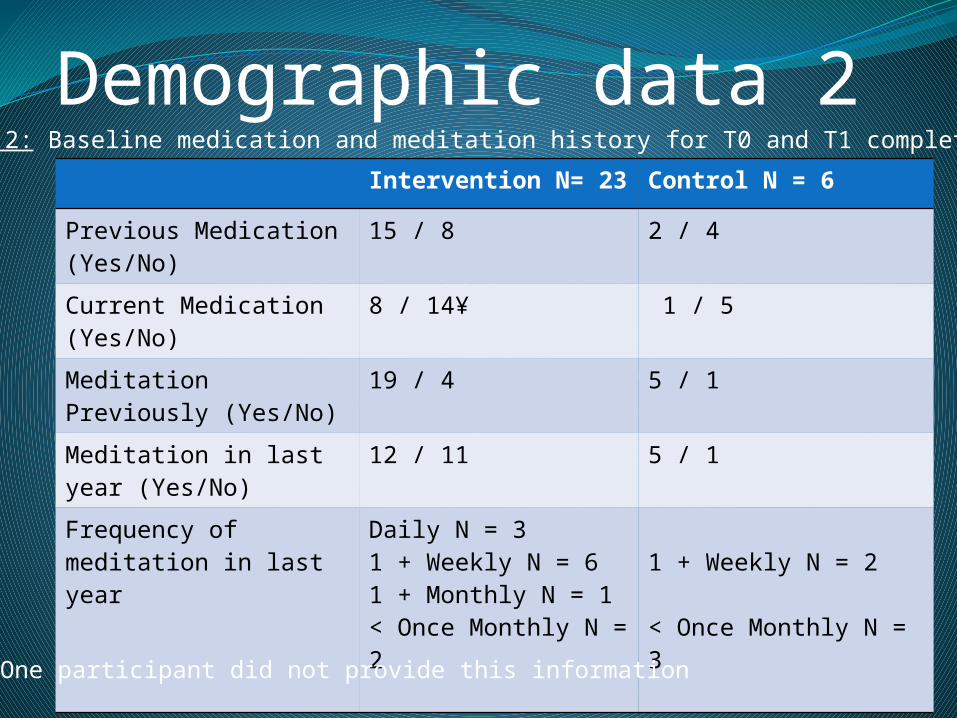
Demographic data 2Intervention N= 23 Control N = 6
Previous Medication (Yes/No)
15 / 8 2 / 4
Current Medication (Yes/No)
8 / 14¥ 1 / 5
Meditation Previously (Yes/No)
19 / 4 5 / 1
Meditation in last year (Yes/No)
12 / 11 5 / 1
Frequency of meditation in last year
Daily N = 31 + Weekly N = 61 + Monthly N = 1< Once Monthly N = 2
1 + Weekly N = 2
< Once Monthly N = 3
Table 2: Baseline medication and meditation history for T0 and T1 completers
¥ One participant did not provide this information

Figure 1: Psychological disorders history (percentages by group) N = 29

Figure 2: Reported reasons for wishing to attend course (percentage by group) N = 29
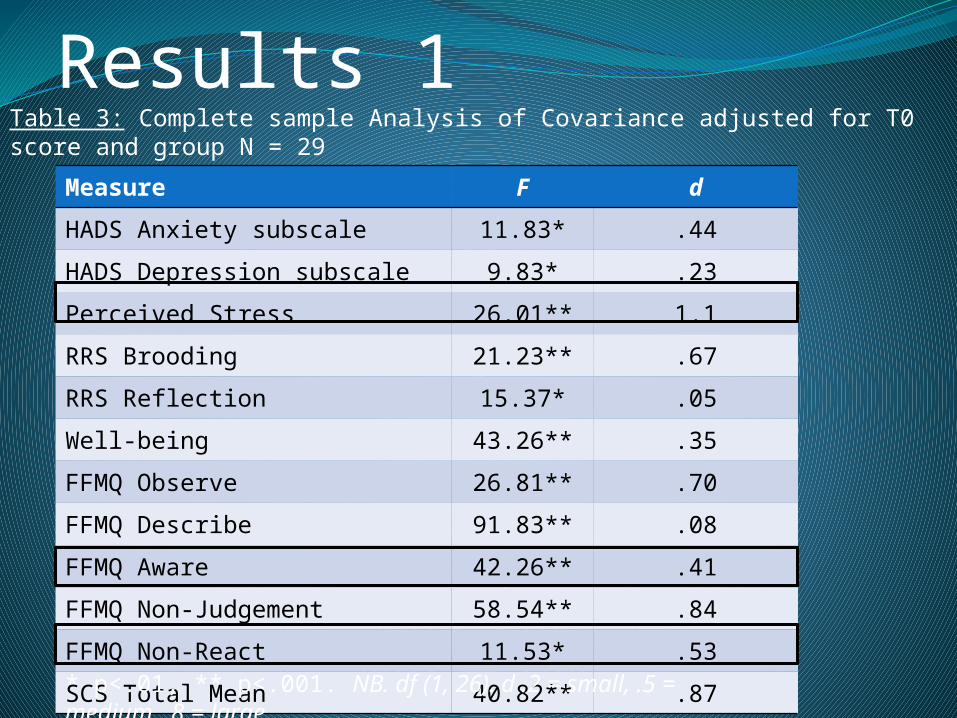
Results 1Measure F d
HADS Anxiety subscale 11.83* .44
HADS Depression subscale 9.83* .23
Perceived Stress 26.01** 1.1
RRS Brooding 21.23** .67
RRS Reflection 15.37* .05
Well-being 43.26** .35
FFMQ Observe 26.81** .70
FFMQ Describe 91.83** .08
FFMQ Aware 42.26** .41
FFMQ Non-Judgement 58.54** .84
FFMQ Non-React 11.53* .53
SCS Total Mean 40.82** .87
Table 3: Complete sample Analysis of Covariance adjusted for T0 score and group N = 29
* p<.01, ** p<.001. NB. df (1, 26). d .2 = small, .5 = medium, .8 = large

Results 2Measure F d
HADS Anxiety subscale 15.22** .08
HADS Depression subscale 7.77* .50
Perceived Stress 14.56** .79
RRS Brooding 19.61*** .33
RRS Reflection 7.97* .81
Well-being 36.96*** 1.3
FFMQ Observe 18.31*** .85
FFMQ Describe 64.97*** .77
FFMQ Aware 25.65*** 1.2
FFMQ Non-Judgement 35.66*** .78
FFMQ Non-React 7.62* .67
SCS Total Mean 22.22*** .82
Table 4: Intervention only Analysis of Covariance adjusted for T0 score and Current Meditation N = 23
* p<.05, ** p<.01. ***p<.001 NB. df (1,20). d .2 = small, .5 = medium, .8 = large
Conclusions• Global improvements for intervention vs control• Improvements demonstrated when take into account existing meditation practice • A feasible intervention for the general population to enhance well-being, reduce stress, anxiety, depression• Follow-up data will indicate whether changes are maintained

Key messages from three studies• Differing designs, differing barriers• Referrals/ Accessibility• Feasibility• Transition into routine practice


















