Positron Emission Tomography-based Boron Neutron Capture ... · Pharmacokinetic analyses could be...
10
Vol. 4, 1833-1 841, August 1998 Clinical Cancer Research 1833 Advances in Brief Positron Emission Tomography-based Boron Neutron Capture Therapy Using Boronophenylalanine for High-Grade Gliomas: Part 111 Yoshio Imahori,2 Satoshi Ueda, Yoshio Ohmori, Kenji Sakae, Tsukasa Kusuki, Tooru Kobayashi, Masao Takagaki, Koji Ono, Tatsuo Ido, and Ryou Fujii Department of Neurosurgery, Kyoto Prefectural University of Medicine, Kyoto 602 [Y. I., S. U., Y. 0., K. S., T. Ku.]; Kyoto University Research Reactor Institute, Osaka 590-04 [T. Ko., M. T., K. 0.]; Cyclotron and RI Center, Tohoku University, Sendai [T. I.]; and Cyclotron Unit, Nishijin Hospital, Kyoto 602 [R. F.], Japan Abstract Based on pharmacokinetic findings of fluorine-18- labeled L-fluoroboronophenylalanine by positron emis- sion tomography (PET), methods for estimating tumor iOB concentration were devised. In clinical practice of boron neutron capture therapy (BNCT) for high-grade gliomas, a large amount of L-boronophenylalanine (LiOB BPA)-fructose solution is used. Under these conditions, a slow i.v. infusion of L-10B-BPA-fructose solution should be performed for BNCT; therefore, the changes over time in iOB concentration in the target tissue were estimated by convoluting the actual time course of changes in plasma ‘#{176}B concentration with a PET-based weight function in- cluding the proper rate constants [K1 (ml/g/min), k2 (min1), k3 (mint), and k4 (min’)]. With this method, the estimated values of ‘#{176}B concentration in gliomas were very close to the ioB levels in surgical specimens. This demonstrated the similarity in pharmacokinetics between fluorine-18-labeled L-fluoroboronophenylalanine and L-’#{176}B-BPA. This method, using the appropriate rate con- stant, permits the determination of tumor ioB concentra- tion and is widely suitable for clinical BNCT, because the averaged PET data are enough to use in future patients without individual PET study. Received 12/18/97; revised 5/22/98; accepted 7/1/98. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. I Supported in part by Grants-in-Aid for Science Research 06282254, 06671411, 07274259, 8671602, and 09671439 from the Ministry of Education, Science, Sports and Culture of Japan. 2 To whom requests for reprints should be addressed, at Department of Neurosurgery, Kyoto Prefectural University of Medicine, Kawarama- chi-Hirokoji, Kamigyo 602-0841, Kyoto, Japan. Phone: 075-251-5543; Fax: 075-251-5544; E-mail: [email protected]. Introduction BNCT3 requires selective delivery of a boron-containing drug to the tumor, followed by irradiation with neutrons (1-5). For estimation of the radiation dose to the tumor, it is essential to know the concentration of boron in the tumor at the time of BNCT. However, direct measurement at the time of BNCT is impossible; therefore, new approaches to the estimation of the boron content of tumors during BNCT are required. When actually performing BNCT, we must reconfirm the tumor level by measuring the L-’#{176}B-BPA in the arterial blood. We administered a large amount of L-’#{176}B-BPA-fructose solution i.v. before BNCT, admitted the patient to the irradiation room, and began neutron irradiation, but the collection of arterial blood was possible for at least 1-2 h, until the beginning of neutron irradiation. Thus, the input function of L-’#{176}B-BPA can be de- termined by blood sampling during this 1-2 h, and, finally, the neutron dose must be determined based on the tumor lO level. Under these conditions, estimation of ‘#{176}B level based on the incorporation constant (ic*) and the utilization ratio (Ur*; Refs. 6-8) is often inappropriate. In this study, our main purpose is to solve these actual problems. We evaluated the tumor pharma- cokinetics ofL-’8F-’#{176}B-FBPA based on comparison with L-’#{176}B- BPA using PET and assessed the similarity of L-’8F-’#{176}B-FBPA accumulation to that of L-’#{176}B-BPA. If the ‘#{176}B concentration calculated using the rate constant obtained by PET using L- ‘#{176}B-FBPA and the actually measured ‘#{176}B input function is close to that in the surgical specimens, similarity in pharmacokinetics between L-’8F-1#{176}B-FBPA and L-’#{176}B-BPA will be confirmed. We also designed a basic method for measuring the tumor concentration of L-’#{176}B-BPA using L-’8F-’#{176}B-FBPA for clinical BNCT. Patients and Methods Clinical Use of L-18F-’#{176}B-FBPA. The performance of L-’8F-’#{176}B-FBPA PET studies on humans and the quality control of L-’8F-’#{176}B-FBPA followed the guidelines established by the PET Committee of Nishijin Hospital (Kyoto, Japan) in January 1991. The synthesis method and purification of L-’8F-’#{176}B-FBPA are detailed in our previous report (9). Preparation of LiBBPAFructose Complex. L-’#{176}B- BPA is relatively insoluble in water. For i.v. administration, we prepared a L-’#{176}B-BPA fructose-complex solution as reported by Yoshino et a!. (10). This complex dissociates and reaches an 3 The abbreviations used are: BNCT, boron neutron capture therapy; PET, positron emission tomography; L-”F-1#{176}B-FBPA, fluorine-l8-la- beled L-fluoroboronophenylalanine; L-’#{176}B-BPA, L-boronophenylala- nine; GBM, glioblastoma multiforme; ROI, region of interest; All, anaplastic astrocytoma WHO grade II; Am, anaplastic astrocytoma WHO grade III. on April 9, 2021. © 1998 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Transcript of Positron Emission Tomography-based Boron Neutron Capture ... · Pharmacokinetic analyses could be...

Vol. 4, 1833-1 841, August 1998 Clinical Cancer Research 1833
Advances in Brief
Positron Emission Tomography-based Boron Neutron Capture
Therapy Using Boronophenylalanine for High-Grade
Gliomas: Part 111
Yoshio Imahori,2 Satoshi Ueda, Yoshio Ohmori,
Kenji Sakae, Tsukasa Kusuki, Tooru Kobayashi,
Masao Takagaki, Koji Ono, Tatsuo Ido, and
Ryou Fujii
Department of Neurosurgery, Kyoto Prefectural University ofMedicine, Kyoto 602 [Y. I., S. U., Y. 0., K. S., T. Ku.]; KyotoUniversity Research Reactor Institute, Osaka 590-04 [T. Ko., M. T.,
K. 0.]; Cyclotron and RI Center, Tohoku University, Sendai [T. I.];
and Cyclotron Unit, Nishijin Hospital, Kyoto 602 [R. F.], Japan
Abstract
Based on pharmacokinetic findings of fluorine-18-
labeled L-fluoroboronophenylalanine by positron emis-
sion tomography (PET), methods for estimating tumor
iOB concentration were devised. In clinical practice of
boron neutron capture therapy (BNCT) for high-grade
gliomas, a large amount of L-boronophenylalanine (L�iOB�
BPA)-fructose solution is used. Under these conditions, a
slow i.v. infusion of L-10B-BPA-fructose solution should be
performed for BNCT; therefore, the changes over time iniOB concentration in the target tissue were estimated by
convoluting the actual time course of changes in plasma‘#{176}Bconcentration with a PET-based weight function in-
cluding the proper rate constants [K1 (ml/g/min), k2
(min1), k3 (mint), and k4 (min’)]. With this method,
the estimated values of ‘#{176}Bconcentration in gliomas werevery close to the ioB levels in surgical specimens. Thisdemonstrated the similarity in pharmacokinetics between
fluorine-18-labeled L-fluoroboronophenylalanine and
L-’#{176}B-BPA. This method, using the appropriate rate con-
stant, permits the determination of tumor ioB concentra-
tion and is widely suitable for clinical BNCT, because the
averaged PET data are enough to use in future patientswithout individual PET study.
Received 12/18/97; revised 5/22/98; accepted 7/1/98.The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to
indicate this fact.
I Supported in part by Grants-in-Aid for Science Research 06282254,06671411, 07274259, 8671602, and 09671439 from the Ministry of
Education, Science, Sports and Culture of Japan.2 To whom requests for reprints should be addressed, at Department of
Neurosurgery, Kyoto Prefectural University of Medicine, Kawarama-chi-Hirokoji, Kamigyo 602-0841, Kyoto, Japan. Phone: 075-251-5543;
Fax: 075-251-5544; E-mail: [email protected].
Introduction
BNCT3 requires selective delivery of a boron-containing
drug to the tumor, followed by irradiation with neutrons (1-5).
For estimation of the radiation dose to the tumor, it is essential
to know the concentration of boron in the tumor at the time of
BNCT. However, direct measurement at the time of BNCT is
impossible; therefore, new approaches to the estimation of the
boron content of tumors during BNCT are required. When
actually performing BNCT, we must reconfirm the tumor
level by measuring the L-’#{176}B-BPA in the arterial blood. We
administered a large amount of L-’#{176}B-BPA-fructose solution i.v.
before BNCT, admitted the patient to the irradiation room, and
began neutron irradiation, but the collection of arterial blood
was possible for at least 1-2 h, until the beginning of neutron
irradiation. Thus, the input function of L-’#{176}B-BPA can be de-
termined by blood sampling during this 1-2 h, and, finally, the
neutron dose must be determined based on the tumor lO� level.
Under these conditions, estimation of ‘#{176}Blevel based on the
incorporation constant (ic*) and the utilization ratio (Ur*; Refs.
6-8) is often inappropriate. In this study, our main purpose is to
solve these actual problems. We evaluated the tumor pharma-
cokinetics ofL-’8F-’#{176}B-FBPA based on comparison with L-’#{176}B-
BPA using PET and assessed the similarity of L-’8F-’#{176}B-FBPA
accumulation to that of L-’#{176}B-BPA. If the ‘#{176}Bconcentration
calculated using the rate constant obtained by PET using L-
‘#{176}B-FBPA and the actually measured ‘#{176}Binput function is close
to that in the surgical specimens, similarity in pharmacokinetics
between L-’8F-1#{176}B-FBPA and L-’#{176}B-BPA will be confirmed.
We also designed a basic method for measuring the tumor
concentration of L-’#{176}B-BPA using L-’8F-’#{176}B-FBPA for clinical
BNCT.
Patients and Methods
Clinical Use of L-18F-’#{176}B-FBPA. The performance ofL-’8F-’#{176}B-FBPA PET studies on humans and the quality control
of L-’8F-’#{176}B-FBPA followed the guidelines established by the
PET Committee of Nishijin Hospital (Kyoto, Japan) in January
1991. The synthesis method and purification of L-’8F-’#{176}B-FBPA
are detailed in our previous report (9).
Preparation of L�i�B�BPA�Fructose Complex. L-’#{176}B-
BPA is relatively insoluble in water. For i.v. administration, we
prepared a L-’#{176}B-BPA fructose-complex solution as reported by
Yoshino et a!. (10). This complex dissociates and reaches an
3 The abbreviations used are: BNCT, boron neutron capture therapy;PET, positron emission tomography; L-”F-1#{176}B-FBPA, fluorine-l8-la-
beled L-fluoroboronophenylalanine; L-’#{176}B-BPA, L-boronophenylala-nine; GBM, glioblastoma multiforme; ROI, region of interest; All,anaplastic astrocytoma WHO grade II; Am, anaplastic astrocytoma
WHO grade III.
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

k3 �
k4!uI�
i81?.jO�fl3pA
in tumor
A Ki
‘8F-’#{176}B-FBPAin plasma _______
. k2
metabolitesIn plasma
B
r
r��i�BPAI in plasma
1(4
complex
Ki
k2
....x
k3 �
k4.I�
lSFJOB4�pA
in tumor
1834 PET-based BNCT Using L-’#{176}B-BPA: Part II
the mean value. Using this as a criterion, we limited macro-
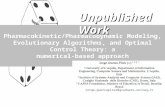
Fig. 1 Modified three-compartment model of
L-’8F-’#{176}B-FBPA and L-’#{176}B-BPA. A, this model is
adapted to a four-parameter model by adding anadditional serial tissue compartment with anabolic
and reverse process rate constants k3 and k4, re-spectively. K1 and k2 refer to forward and reversetransport of L-”F-’#{176}B-FBPA across the blood-
brain barrier, respectively. The pharmacokinetics
of L�ISF�tt�B�FBPA were analyzed using the three-
compartment model by K, (mllg/min), k, (min’),
k3 (min’), and k4 (min ‘).B,this model was also
adopted to analyze the pharmacokinetics of L-’#{176}B-
BPA described here. The L-’#{176}B-BPA-fructosecomplex is dissociative and reaches an equilibriumbetween free molecule and the complex in the
diluted condition in plasma. Kd and Ka representthe dissociation and association process of thecomplex, respectively.
Table 1 Rate constants of L-”F-’#{176}B-FBPA in patients with gliomas
Rate constants of L-’8F-’#{176}B-FBPA in patients with gliomas, including 17 cases of high-grade gliomas and 4 cases of Al!. The values of the rate
constants (K,, k2, k3, and k4) are given as the mean ± SD. Control was established at the corresponding region in contralateral brain in each case.
Grade n K, (mug/mm) k2 (min’) k3 (mm’) k4 (mm’)
GBM 1 1 0.040 ± 0.007 0.034 ± 0.009 0.018 ± 0.007 0.01 1 ± 0.005
Alil 6 0.039 ± 0.025 0.030 ± 0.013 0.025 ± 0.014 0.01 1 ± 0.007All 4 0.021 ± 0.006 0.030 ± 0.005 0.025 ± 0.005 0.009 ± 0.009Control 21 0.01 1 ± 0.003 0.025 ± 0.009 0.033 ± 0.015 0.009 ± 0.0 10
equilibrium between free molecules and the complex in the
diluted condition present in the plasma (Fig. 1B; Ref. I 1 ). The
solution of L- ‘#{176}B-BPA-fructose complex consisted of L-
BPA (1 g):D-(-)-fructose (2.22 g):H20 (30 ml):lN NaOH (5.55
ml). Thereafter, the solution was slowly added to 0.8 ml of iN
HC1, and the pH value was adjusted to 7.5. To buffer the
solution, 7% NaHCO3 was added. The molar concentration of
the final solution was 1 15 m�vi, and the ‘#{176}Bconcentration was
5.52 mrsi. The molar ratio of L-’#{176}B-BPA:fructose was 1:2.57.
Finally, the fructose complex was prepared by filtration using a
Millipore filter (MILLEX-GS; 0.22 p.m; Waters). The L-’#{176}B-
BPA solution was then tested for a pH value of 8.5. The i.v.
infusion rate was 10 mI/mm.
Patients. The subjects were the same group of patients
described in part I (6). Pharmacokinetic analyses could be
performed for 17 patients with high-grade gliomas and 4 pa-
tients with All in the group, and the rate constants were calcu-
lated (Table 1). Seven of the patients (the same set of patients
described in Table 2 of part I; Ref. 6) underwent resection of the
tumor after PET studies using L�ISF�i�B�FBPA, and the ‘#{176}B
concentration estimated using PET data was compared with that
in the tissue obtained at surgery (Table 2). Surgery was per-
formed for all patients, and in each case, the diagnosis was
confirmed histologically. The degree of malignancy was classi-
fled histologically using the WHO grading criteria (All, Alli,
and GBM).
Dynamic PET Method. The spatial resolution in PET
imaging was 8.2 mm at full-width half-maximum with plane
resolution, whereas the average axial resolution was 12.8 mm.
X-ray computed tomography and magnetic resonance imaging
were also performed for all patients. Dynamic images of L-’8F-
‘#{176}B-FBPA were obtained using PET in all cases. PET scans
were conducted with a tomograph using a HEADTOME III
(Shimadzu Co., Kyoto, Japan). The planes of the PET scans
were the same as those in the parallel computed tomography
studies. Local cerebral blood volume was measured after bolus
inhalation of ‘5O-labeled carbon monoxide gas (12). A dose of
1-1 .5 mCi/lO kg body weight of L-’8F-’#{176}B-FBPA was injected
i.v. over 40 s. Dynamic PET study was begun when whole brain
activity reached a value greater than that of the background
activity. PET data were collected continuously for nine 2-mm
periods and six 4-mm periods, making a total of 15 periods over
a total of 42 mm (Fig. 2, A and B). The four initial arterial blood
samples were obtained at 5-s intervals; subsequent samples were
obtained at gradually longer intervals (0.5-10 mm), making a
total of 21 samples over a period of 42 mm (Fig. 3A). The time
course changes in plasma L-’5F-’#{176}B-FBPA levels were fitted
using Equation A (see “Appendix”).
Choice of ROIs. All regions of macroscopically necrotic
tumor were excluded when ROIs were designated. The variation
in radioactivity associated with each pixel was less than 1 8% of
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

A B
p.9-6 Tumor area
/
70’
I Fitting result K(1) .0306075
c� K(2) .0206767I K(3) .020022I K(4) .0084036
Normal area,t5
9,I
p/ Fitting result K(l) .0093911
1 K(2) .0257794c� K(3) .024827
K(4).01l0718
Clinical Cancer Research 1835
Table 2 Segmental convolution method for estimation of the tumor ‘#{176}Blevel
The values shown under “Estimated ‘#{176}B�’were obtained by the segmental convolution method using rate constants obtained by PET (EquationsC-H, see “Appendix”). These ‘#{176}Blevels were estimated according to the resection time on operation (see Fig. 6). L-’#{176}B-BPA solution (3.38-I 13.6
mg/kg body weight) was infused for 20-45 mm. “Tumor ‘#{176}B��shows the ‘#{176}Blevels in tumor tissue resected after an infusion of L-’#{176}B-BPA, as
measured using the prompt -y method.
Grade, total injection Rate constants
dose of L-’#{176}BPA
Case (mg/kg body weight) K, (ml/g/min) k2 (mm ‘) k1 (min ‘) k4 (mm ‘) Estimated ‘#{176}B(p.g/ml) Tumor “B (pg/ml)
1 All!, 51.0 0.031 0.034 0.025 0.009 4.66 (71 mm) 2.1
2 GBM, 33.8 0.043 0.022 0.004 0.015 3.72 (50 mm) 2.3
3 All!, I 13.6 0.027 0.038 0.025 0.023 7.15 (60 mm) 5.4
4 GBM, 71.4 0.039 0.045 0.018 0.013 7.48 (77 mm) 6.0-8.0
5 GBM, 83.3 0.027 0.039 0.01 1 0.013 5.13 (76 mm) 3.5-4.06 GBM, 76.9 0.035 0.034 0.018 0.010 5.77 (1 12 mm) 5.4
7 GBM, 76.9 0.041 0.037 0.019 0.01 1 10.63 (82 mm) 9.5
Fig. 2 Time-activity data ofL-’8F-’#{176}B-FBPA and the fitting results. A, time-activity data in the tumor region. B, time-activity data in the normal brain
region. Fine dotted lines represent the fitting results obtained by the nonlinear least squares best regression method. The pharmacokinetics of
IS�IOi�p�p� were analyzed using a three-compartment model. as shown in Fig. IA. The equation (Equation B in “Appendix”) proposed by Huang
et al. (20) is a generalized model of the theorem on which the three-compartment model is based. The nonlinear least squares best regression method
was used to obtain the rate constants (K,, k,, k3, and k4). For the nonlinear least squares best regression method. an appropriate initial value is required.The method for obtaining this initial value is described in our previous report (9).
scopic heterogeneity to a minimum when designating ROIs.
ROl images consisted of 49-171 pixels on the tumor center and
a nontumor control area; hence, they had a minimum voxel
volume of 2.94 cm3. Patients with a hot area (active area)
smaller than the above-mentioned area were excluded from the
evaluation. The tumor areas of all 2 1 cases presented in this
study satisfied this voxel volume requirement. No partial vol-
ume corrections were performed for any patient. We designated
several ROIs from tumor-affected areas and used the region
with the highest values as a representative ROI. In pharmaco-
kinetic analyses, we corrected the time-activity curve for over-
estimation of ‘8F-’#{176}B-FBPA incorporation by cerebral blood
volume to obtain accurate values of the rate constants [K,
(mL/g/min), k2 (min’), k3 (min’), and k4 (min’)] in the
three-compartment model, as reported in our previous study (9).
Correction of Blood Concentration Data. Generally,plasma:whole blood ratios of ‘8F radioactivity and ‘0B level are
1.3 for both L-’8F-’#{176}B-FBPA and L-’#{176}B-BPA. We determined
the time course changes in both ratios. The plasma:whole blood
ratios of ‘8F radioactivity and ‘#{176}Blevels changed little over
time. Based on these results, we judged it reasonable to treat the
ratio as a constant. When ‘#{176}Blevels of whole blood are meas-
ured by the prompt �l’ method, they should be corrected by
multiplication using a factor of 1 .3, because the input function is
based only on plasma concentrations. Ishiwata et a!. ( I 3) re-
ported that the amounts of labeled metabolites of L-’8F-’#{176}B-
FBPA in arterial plasma were small during the 1-h animal
experiments. In our human PET studies, the metabolic fractions
were negligible during the 42-mm period after injection, be-
cause we observed that more than 95% of the total radioactivity
in plasma was due to the free ‘8F-’#{176}B-FBPA fraction during the
42-mm arterial sampling. These findings suggest that plasma
metabolite correction is not necessary, and that the metabolism
of L- ‘#{176}B-BPAcan be treated like that of ‘ 8F- ‘#{176}B-FBPA.
Three-Compartment Model of L�iSF�i�B�FBPA and
L�iOB�BPA. Our previous data obtained by dynamic PET
studies using ‘8F-’#{176}B-FBPA suggested that the time-activity
curves reveal a characteristic accumulation of ‘8F activity. After
a rapid increase to a quasi-steady state, accumulation remained
stable (Fig. 2, A and B). When the dynamic PET data were
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

A B
40000
30000
20000
1 0000
Iplasma
whole blood
40 60 80
mm
0 tj.i tj
1836 PET-based BNCT Using L-’#{176}B-BPA: Part II
, I;
� . �0
Fig. 3 Input functions of L-’8F-’#{176}B-FBPAon two differential iv. administrations. A, all pharmacokinetic analyses were performed by using the input
function administered by a bolus injection for 40 s and arterial blood sampling for 42 mm after the injection. X axis, time course; Y axis, ‘8Fradioactivity of plasma or whole blood. Radioactivity in the blood increased rapidly until I mm after the bolus injection and subsequently decreased
rapidly, permitting three-exponential fittings, as shown in Equation A (see “Appendix”). Plasma:whole blood ratios of ‘8F radioactivity and the ‘#{176}Blevel are 1 .3. We determined the time course changes in ratios. The plasma:whole blood ratios of ‘8F radioactivity changed little over time. Basedon these results, we judged it reasonable to treat the ratio as a constant (6). B, with slow infusion of L-’8F-’#{176}B-FBPA over 20 mm, radioactivity in
the blood increased gradually and then decreased rapidly after discontinuation of the infusion. In this case, the input function permits two-exponentialfunction, but we adopted the segmental convolution method to obtain the accurate C�’t).
#{163}�iCij(t)
Fig. 4 Segmental convolution method for estimation of the tumor ‘#{176}B
level. The input function [C�(t)] was obtained by arterial blood sam-pling.j, segment number; t, time (minutes); C(t), the estimated ‘#{176}Blevelat time t; G�, slope of the first order function, Cpj(t); K�, Y axis interceptof Cpj(t).
represented as Gjedde-Patlak plots (14, 15), a positive slope was
obtained, suggesting the involvement of the putative metabolic
pool of this tracer in tumor cells (9). We used a compartment
model that is adapted to a four-parameter model by adding an
additional serial tissue compartment with anabolic and reverse
process rate constants k3 and k4, respectively; the incorporation
into proteins is then described by rate constant k5, but it should
be ignored because of less incorporation into proteins (13). This
method has already been established as an analytical model of
amino acids by Wienhard et a!. (16); a similarity in the model
analysis between the characteristics of ‘ 8F)fluorotyrosine
in their report and the characteristics of ‘8F-’#{176}B-FBPA was
found (9, 17-19). Therefore, the pharmacokinetics of ‘8F-’#{176}B-
FBPA were analyzed using a modified three-compartment
model by K, (mug/mm), k, (min ‘), k3 (min ‘), and k4 (min ‘)
as shown in Fig. 1A. The equation (Equation B in “Appendix”)
proposed by Huang et al. (20) is a generalized model of the
theorem on which the three-compartment model is based. The
nonlinear least squares best regression method was used to
obtain the rate constants (K, , k2, k3, and k4). Using this method
of analysis, the rate constants were determined in each glioma
patient. Details of the relationship between each rate constant
and malignancy were presented in our previous study (9).
Segmental Convolution Method for Estimation of theTumor ioB LeveL In clinical practice of BNCT, 600-800 ml
of L-’#{176}B-BPA-fructose solution are used, and infusion requires
about 60-80 mm. Under these conditions, convolution of the
time course changes in plasma ‘#{176}Bconcentration in the form of
L-’#{176}B-BPA determined by Equation D (in “Appendix”), as
shown in Fig. 4, can be used in Equation C (in “Appendix”). In
the segmental convolution method, the estimated values of
tissue ‘#{176}Bconcentration of L-’#{176}B-BPA can be calculated from
the values of K,, k2, k3, and k4 obtained by PET using L-’8F-
‘#{176}B-FBPA for each patient or the mean values shown in Table
1 . If the ‘ #{176}Bconcentration calculated using the rate constant
obtained by L-’8F-’#{176}B-FBPA PET and the actually measured
‘#{176}Binput function is close to that in surgical specimens, simi-
larity in pharmacokinetics between L-’8F-’#{176}B-FBPA and L-’#{176}B-
BPA will be confirmed. Using this method, we also preopera-
tively compared the estimated values with the ‘#{176}Blevels in
seven patients with high-grade gliomas (anaplastic astrocytoma
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

A
I
B
E
0 40 80 120 160 200
mm
Plasma 18F-level
Estimated tumor 18F-level
0 20 40 60 80
mm
brain 18F-level
and GBM). The estimated ‘#{176}Blevels were obtained using Equa-
tions B-H (in “Appendix”).
Results
Input Function of L�i$F�i�B�FBPA Obtained by Arte-rial Sampling To facilitate the evaluation of pharmacokinet-
ics, a bolus injection of L-’8F-’#{176}B-FBPA over 40 s was used for
dynamic PET studies. Radioactivity in the blood increased rap-
idly until 1 mm after the bolus injection and subsequently
decreased rapidly, permitting three-exponential fittings, as
shown in Equation A (Fig. 3A). With the slow infusion of
L-’8F-’#{176}B-FBPA, radioactivity in the blood increased gradually
and then decreased rapidly after discontinuation of the infusion
(Fig. 3B). These findings suggest that L-’8F-’#{176}B-FBPA is
cleared immediately from the blood. Fig. 3B shows the changes
in blood radioactivity after a slow infusion of L-’8F-’#{176}B-FBPA
Clinical Cancer Research 1837
Fig. 5 Assessment of the suitabil-
ity of the segmental convolution
method. Representative images (A
and B) are of patients with glioblas-toma. As shown in both A and B,the estimated values by the segmen-tat convolution corresponded wellwith the actual measurements by
PET in each case. The estimatedcurves were plotted by the convo-lution of the input function [C�*(t)]of ‘8F radioactivity obtained by
continual arterial blood specimen
collection at the same time, with themean values of K,-k4 shown in Ta-
ble 1 substituted into the weight
function. #{149},C.*(t) of tumor lesionbased on actual PET study (tumor
‘8F level on PET); �, the estimatedci *(t) (the estimated tumor ‘ 8F 1ev-ci). #{149},C*(t) of the normal brainbased on actual PET study (normal
brain ‘8F level on PET); 0, the es-
timated C. *(t) (estimated normal
brain ‘8F level).
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

Plasma 10B-level
Estimated 10B-level
20
16’
12
Plasma 10B-level
Estimated 10B-level
0
8
4
50 100 150 200
mm25 50
mm
Fig. 6 Segmental convolution method for the estimation of the tumor ‘#{176}Blevel. A comparison between the estimated values and the ‘#{176}Blevels of
surgical specimens in case 6 (A) and case 7 (B) in Table 2 are shown. We used the proper rate constants as a weight function obtained by PET in
each patient. The estimated curves were calculated by the input function of the ‘#{176}Blevel obtained by continuous arterial blood sampling.
75 100 125
1838 PET-based BNCT Using L-’#{176}B-BPA: Part II
A B
Case 6 Case 710�
8
� 4.
2
over 20 mm. It shows a time-activity curve for L-’8F-’#{176}B-FBPA
obtained under conditions similar to those used for BNCT. In
BNCT, a large amount of L-’#{176}B-BPA-fructOse solution is in-
fused over 60 mm. Segmental convolution using Equations C-H
therefore seems to be appropriate for slow iv. infusion.
Pharmacokinetics of L�lSF�iOB�FBPA Determined byPET. Based on the results of dynamic studies, we calculated
the rate constants (K, , k2, k3, and k4) for the three-compartment
model in Fig. iA. Radioactivity in tumor tissue increased rapidly
for 20 mm after bolus injection and increased gradually there-
after (Fig. 2, A and B). The rate constants obtained are shown in
Table 1. When BNCT is performed clinically, L-’#{176}B-BPA is
infused at 170-280 mg/kg body weight, and the tumor ‘#{176}Blevel
during BNCT is 20-35 p�g/ml (in ppm). In this case, estimation
of the ‘#{176}Blevel based on Ur* and lc* is often inappropriate, but
segmental convolution of the serially determined plasma ioB
concentrations in Equation D yields accurate estimations (Fig.
4). To use Equation E, K,, k2, k3, and k4 should be obtained
beforehand by PET using L-’8F-’#{176}B-FBPA for each patient, or
the mean values shown in Table 1 can be used. The input
function of L-’#{176}B-BPA in plasma, C�(t), was obtained by the
prompt “�‘ measurement connected with the reactor.
Fig. 5, A and B, shows examples of a PET study to assess
the suitability of the segmental convolution method. Both im-
ages are of patients with glioblastoma. These two patients un-
derwent slow infusions of L-’8F-’#{176}B-FBPA, and we performed
a continual measurement by PET and plotted C1*(t). In this PET
measurement, slow infusions of L-’8F-’#{176}B-FBPA were per-
formed under conditions of administration quite similar to those
of clinical BNCT. The closed squares show values of C� *(t) for
the tumor obtained from the PET study, and the open squares
show the estimated curves, which were plotted by convolution
of the input function [C�*(t)] of ‘8F radioactivity obtained by
continual arterial blood specimen collection at the same time,
with the mean values of K,-k4 shown in Table 1 substituted into
the weight function. As shown, the values estimated by the
segmental convolution method corresponded well with the PET
measurements in each case, confirming the suitability of the
segmental convolution method.
Therefore, as shown in Table 2, we administered subthera-
peutic doses of L-’#{176}B-BPA to seven patients and plotted the
estimated curves of the ‘#{176}Blevels using the method of calcula-
tion described above. The estimated curves were calculated by
the input function of the ‘#{176}Blevel obtained by continuous
arterial blood sampling. Typical examples are shown in Fig. 6,
A and B. In the seven cases shown in Table 2, we were able to
substitute the proper rate constants determined by PET in Equa-
tion C. We compared the estimated values with the ‘#{176}Blevels in
surgical specimens for these seven cases. As shown in Table 2,
the estimated values tended to be higher than those for surgical
specimens but were similar to them, except in cases 1 and 2. On
PET, the highest radioactivity area can be set as the concerned
area. As a result, the highest value will be the representative
value. On the other hand, in the case of the surgical sample,
selection of only a high area of ‘#{176}Bis impossible. For this
simple reason, a discrepancy develops between them. However,
in patients from whom a homogenous tumor sample was ob-
tamed, the surgical sample is close to the estimated value, and
the data are considered as validating the adequacy of the present
method.
Discussion
In Vivo L-’#{176}B-BPAPharmacokinetics Determined withL-’8F-10B-FBPA PET. In the treatment of gliomas, L-’8F-
‘#{176}B-FBPA uptake permits clear visualization of the main part
of the tumor and helps to determine the extent of tumor
resection required. Infiltrating cells are present around the
main part of the tumor, and treatment of this area with BNCT
is considered to be the most reasonable approach. We as-
sumed that infiltrating cells have the same biochemical prop-
erties as cells in the main part of the tumor, which could be
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

E
3
Plasma iSFIevel
Tumor 18F4evel on PET
20 40 60 80 100 120
mm
140
Clinical Cancer Research 1839
Fig. 7 Differences in the courses of time-activity
curves between tumor lesion and normal brain
tissue. The time-activity curves of ‘�F (in cps/ml)
were real data obtained in a patient with GBM.
When PET scans were performed 1-2 h after theinjection, we found a decrease in radioactivity inthe tumor region after a while. This seemed to bedue to the catabolic process, as suggested by theaction of k4 in the tumors. X axis, time (minutes):
Y axis, ‘8F activity.
macroscopically observed by PET, and planned the use of
thermal neutron irradiation in BNCT. With this concept for
PET-based BNCT, clinical application ofBNCT using L-’#{176}B-
BPA was successful. L-’#{176}B-BPA is cleared rapidly from the
blood but is retained in tumor tissue and actively taken up by
proliferating cells. Its accumulation in tumors was demon-
strated by dynamic PET using L-’8F-’#{176}B-FBPA (6, 9). An
important factor in BNCT is the determination of the ‘#{176}B
concentration in both the tumor tissue and normal brain. An
increase in the tumor:normal ratio increases the efficacy of
BNCT, because it allows a greater tumor dose to be delivered
per dose administered to normal tissue, and the tumor dose is
limited by normal tissue tolerance (4). Appropriate indica-
tions for BNCT include a tumor:normal ratio above 2.5 (21).
We studied the factors contributing to accumulation. An
increase in K, is the principal factor affecting the accumula-
tion of L-’8F-’#{176}B-FBPA (6, 9). As described above, L-’5F-
‘#{176}B-FBPA accumulation is accomplished within 42 mm after
bolus i.v. injection in dynamic PET studies. The rapid
achievement of equilibrium (within 42 mm) was attributed to
K,. When PET scans were performed in patients with high-
grade gliomas during 1-2 h after injection, we found a
decrease in radioactivity in the tumor region after a while
(Fig. 7). This seemed to be due to catabolism, as suggested by
the action of k4 in tumors. Kabalka et a!. (22) recently
showed that the four-compartment model can be used for the
evaluation of the tracer kinetics of L-’8F-’#{176}B-FBPA. They
obtained the arterial blood concentration input function from
a ROl representing vascular activity in the internal carotid
artery. Although their method is different from our compart-
ment model, the results of the kinetics were essentially sim-
ilar to ours. Assessment based on these characteristics of
� suggests that accurate ‘#{176}Blevels can be
estimated within 1-2 h after iv. infusion of L-’#{176}B-BPA.
Furthermore, the � concentration in normal tissue must be
considered. Briefly, a rapid increase in the tumor ‘#{176}Blevel is
promoted by K, and suppressed by k, until blood ‘#{176}Blevels
decrease rapidly after the end of the iv. infusion; then the ‘#{176}B
level is maintained by k3 and decreased by k4 in tumor tissue
after a while. Although a similar process occurs in normal
tissue, normal tissue has a higher k3 (0.033 ± 0.015) than
does tumor tissue (GBM, 0.018 ± 0.007; AIlI, 0.025 ±
0.014). Fig. 7 shows that differences between tumor and
normal tissue in time course changes decreased with time in
the L-’5F-’#{176}B-FBPA study. This suggests that ‘#{176}Blevels in
normal tissue gradually approach the tumor ‘#{176}Blevel as a
result of the higher k3 value in normal tissue. It may be
appropriate to start BNCT when the difference in ‘#{176}Bcon-
centration between normal tissue and tumor is marked.
Pathological Features and Pharmacokinetics. There
are some important problems regarding pathological features
and pharmacokinetics in gliomas. One of them is whether the
cellularity of the tumor sample relates to the boron content. In
general, the cellularity of tumors is the standard of malignancy.
The detailed comparison of malignancy and L-’8F-’#{176}B-FBPA
uptake was described in our previous report (9). Elowitz et a!.
(23) also referred the correlation. However, because micro-
scopic heterogeneity is observed in tumor tissues, a numerical
determination of the tumor cellularity using a part of the tumor
tissues is generally difficult, although the cellularity can be
classified into various stages based on the evaluation of pathol-
ogists. Therefore, we did not compare the cellularity with the
boron contents. We also recognize that classifying the cellularity
by certain numerical indices is an important subject to under-
stand the detailed mechanism of ‘#{176}B-BPAuptake and the pro-
tection of the brain. Regarding these subjects, future experi-
ments should be performed to solve this problem, including the
administration of a compound, a cell population marker as a
positron tracer, and a simultaneous scan by L-’8F-’#{176}B-FBPA.
Then, discussion comparing the results of positron tracer ad-
ministration with scanning data is thought to be necessary.
Another problem is that if only a relatively small percent-
age of the tumor cells are undergoing mitosis at any one time,
then the uptake of L-’8F-’#{176}B-FBPA would significantly under-
estimate the true size of the tumor. When we investigated the
relationship between the malignancy of the tumor and L- ‘ 8F-
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

1840 PET-based BNCT Using L-’#{176}B-BPA: Part II
�Ci3(t) = Ci�(t) - C�_,(t) (G)
‘#{176}B-FBPA uptake, it was clinically found that the malignancy is
greatly dependent on the capacity of amino acid transport by
tumors. However, we have encountered cases of low-grade
tumors with marked amino acid uptake. It was considered that
these low-grade tumors might correspond to metabolically ac-
tive nonproliferating cells. Furthermore, although these tumors
were pathohistologically classified as low grade, the prognoses
of the patients were unsatisfactory (9). In general, however,
macroscopic analysis is the objective level for the methodology
described here, and it is difficult to differentiate the small
percentage of metabolically active cells included in the entire
tumor mass. Because there is the possibility of underestimating
regions with the proliferating potential, treatment of this area
with BNCT should be considered as a concept of the target area.
Conditions for Quantitative Measurement of Tissue ‘#{176}BLevels in Clinical BNCT. We found that the segmental con-
volution method is appropriate for clinical BNCT. This method
uses two different modalities. Equation E involves data from
PET and the prompt ‘y method. The rate constants obtained by
PET are used in the weight function in Equation C. The input
function describing changes over time in i% levels, C�(t), is
also involved in Equation C. In the present study, when we
compared the ‘#{176}Bvalues estimated by PET with those of sur-
gical specimens, the estimated values were found to be very
close to the iO� levels in the surgical specimens, as shown in
Table 2. The similarity between L�i8F�i�B�FBPA and L-’#{176}B-
BPA in their pharmacokinetics was thus verified. Therefore, the
proper rate constants for L-’#{176}B-BPA in each subject were re-
garded as similar to those for L-’8F-’#{176}B-FBPA obtained by PET
(Fig. 1, A and B).
When actually performing BNCT, we must reconfirm the
tumor 10B level by measurement of L-’#{176}B-BPA in arterial blood.
As mentioned above, the input function of L-’#{176}B-BPA can be
determined by blood sampling during this 1-2 h. The tumor iOi�
level can be more precisely determined by convoluting the input
function of C�(t) to Equations B-E using K1, k2, k3, and k4. In
evaluating indications for BNCT, Ic* and Ur* are useful for
estimating the dose of L-10B-BPA required (6), but the tumor
10B level calculated by the segmental convolution method based
on the prompt -y measurement is more reliable for the perform-
ance of BNCT.
In the former (6) and the present studies, we evaluated two
different methods ofestimating i% concentration. The first method
permits estimation by PET alone and is useful for determining the
indications for BNCI’. In the second method, the proper rate
constant for brain tumors is used, and the i0J3 concentration in
tumor tissue is obtained using the input function for plasma ‘#{176}B
concentration. This method is useful for the performance of clinical
BNCT, and with it, tissue concentration can be measured even after
slow infusion. Systematic PET-based BNCT is possible using one
or the other of those two methods according to the purpose. With
the first method, the administered dose of L-’#{176}B-BPA can be
estimated for individual patients by PET, and patients can be
selected for future BNCT. With the second method, the concentra-
tion in the tumor can be accurately determined at the time of
neutron irradiation using L-’#{176}B-BPA, and the method is widely
suitable for clinical BNCT, because the averaged PET data as
shown in Table 1 are enough to use in future patients without
individual PET study. The development of this PET-based BNCT
system has made it possible for us to perform BNCT accurately
using reliable objective data. Using this system, we have performed
BNCT with thermal neutrons on patients with high-grade gliomas
(24, 25).
In conclusion, tumor � #{176}Blevels can be more accurately
determined by convoluting the input function to the weight
function using rate constants. The similarity in pharmacokinet-
ics between L�i8F�iOB�FBPA and L�i�B�BPA was also con-
firmed. Using the PET-based BNCT system described here,
clinical performance of BNCT using L-’#{176}B-BPA is possible.
Acknowledgments
We acknowledge the technical support and effort of Kazuo Wakita
and Hitoshi Horii (Cyclotron Unit, Nishijin Hospital, Kyoto, Japan). We
gratefully thank Dr. Kiichi Ishiwata (PET Center, Tokyo MetropolitanInstitute of Gerontology, Tokyo, Japan) for helpful advice regarding‘8F’o��PA synthesis and its biological properties.
Appendix
Cp*(t) = �
i= I
K,Ci(t) = [(k3 + k4 -
( a2 �I)
with
+ (a2 k3 - k4)e_a2h] #{174}Cp(t)
a, [(k2 + k3 + k4) - �(k2 + k3 + k4)2 - 4k2k4]/2
(A)
a2 [(k2 + k3 + k4) + �(k2 + k3 + k4)2 - 4k2k4]12 (B)
Ci(t) = (Ae�’ + Be�2) #{174}Cp(t)
with
K,A= (k3+k4-a,)
(a2 - a,)
K,B=
(a2 - a,)
tJ � 1 < t <
Cp�(t) G�t + K�
C�(t) = f’(Ae�_� + Be�2(T)) X (G�T +
AGCi�(t) - -y�(e’” + a,t - 1) + � + a2t - 1)
a, a2
(C)
(D)
(E)
AK BK.- -�(e” - 1) - � 1) (F)
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 1841
References
Ci(t) = � �Ci�(t)
I . Sweet, W. H. Early history of development of boron neutron capturetherapy of tumors. J. Neuro-Oncol., 33: 19-26. 1997.
2. Asbury, A. K., Ojemann, R. G., Nielsen, S. L., and Sweet, W. H.
Neuropathologic study of fourteen cases of malignant brain tumor
treated by boron-lO slow neutron capture radiation. J. Neuropathol. Exp.Neurol., 31: 278-303. 1972.
3. Hatanaka, H. Experience of boron neutron capture therapy for ma-
lignant brain tumors with special reference to the problems of postop-
erative CT follow-ups. Acta Neurochir. Suppl., 42: 187-192, 1988.
4. Barth, R. F., Soloway, A. H., and Fairchild, R. G. Boron neutron
capture therapy of cancer. Cancer Res., 50: 1061-1070, 1990.
5. Soloway, A. H., Barth, R. F., Gahbauer, R. A., Blue, T. E., and
Goodman, J. H. The rationale and requirements for the development ofboron neutron capture therapy of brain tumors. J. Neuro-Oncol., 33:
9-18, 1997.
6. lmahori, Y., Ueda, S., Ohmori, Y., Sakae, K., Kusuki, T., Kobayashi.T., Takagaki, M., Ono, K., Ido, T., and Fujii, R. Positron emissiontomography-based boron neutron capture therapy using boronophenyl-alanine for high-grade gliomas: part I. Clin. Cancer Res., 4: 1825-1832,1998.
7. Mishima, Y., Imahori, Y., Honda, C., Hiratsuka, J., Ueda, S., and
ldo, T. in vivo diagnosis of human malignant melanoma with positron
emission tomography using specific melanoma-seeking ‘8F-DOpA an-
alogue. J. Neuro-Oncol., 33: 163-169, 1997.
8. Imahori, Y., Ueda, S., Ohmori, Y., Yoshino, E., Ono, K., Kobayashi,
T., Ido, T., and Mishima, Y. A basic concept for PET-BNCT system. In:
Y. Mishima (ed), Cancer Neutron Capture Therapy, pp. 691-696. New
York: Plenum Press, 1996.
9. Imahori, Y., Ueda, S., Ohmori, Y., Kusuki, T., Ono, K., Fujii, R., andIdo, T. Fluorine-l8-labeled fluoroboronophenylalanine and PET in pa-tients with glioma. J. Nucl. Med., 39: 325-333, 1998.
10. Yoshino, K., Suzuki, A., Mon. Y., Kakihana, H., Honda, C..Mishima, Y., Kobayashi, T., and Kanda, K. Improvement of solubility
ofp-boronophenylalanine by complex formation with monosaccharides.
Strahlenther. Onkol., 165: 127-129, 1989.
I 1. Kakihana, H., Yoshino, K., and Mod, Y. Relation between struc-tures of p-boronophenylalanine related compounds and their usefulnessfor boron neutron capture therapy. In: A. H. Soloway et al. (eds.),Advances in Neutron Capture Therapy, pp. 257-260. New York: Plc-num Press, 1993.
12. Phelps, M. E., Huang, S-C., Hoffman, E. J., and Kuhl, D. E.
Validation of tomographic measurement of cerebral blood volume withC-l 1-labeled carboxyhemoglobin. J. Nucl. Med., 20: 328-334, 1979.
13. Ishiwata, K., Ido, T., Kawamura, M., Kubota, K., Ichihashi, M.,
and Mishima, Y. 4-Borono-2-[’8F]fluoro-D,L-phenylalafline as a tar-
get compound for boron neutron capture therapy: tumor imaging
(H) potential with positron emission tomography. Nucl. Med. Biol., 18:745-751, 1991.
14. Gjedde, A. High- and low-affinity transport of o-glucose from
blood to brain. J. Neurochem., 36: 1463-1471, 1981.
15. Patlak, C. S., Blasberg, R. G., and Fenstmacher. J. D. Graphical
evaluation of blood-to-brain transfer constants from multiple-time up-take data. J. Cereb. Blood Flow Metab., 3: 1-7, 1983.
16. Wienhard, K., Herholz, K., Coenen, H. H., Rudolf, J., Kling, P.,Stocklin, G., and Heiss, W. D. Increased amino acid transport into brain
tumors measured by PET of L-(2-’8F)fluorotyrosine. J. Nucl. Med.. 32:
1338-1346, 1991.
17. Coenen, H. H., Kling, P., and Stocklin, G. Cerebral metabolism ofL-[2-l8F]fluorotyrosine, a new PET tracer of protein synthesis. J. Nucl.Med., 30: 1367-1372, 1989.
18. Willemsen, A. 1. M., van Waarde, A., Paans, A. M. J., Pruim, J.,
Luurtsema, G., Go, K. G., and Vaalburg, W. in vivo protein synthesisrate determination in primary or recurrent brain tumors using L-[l-’ ‘C]-
tyrosine and PET. J. Nucl. Med., 36: 41 1-419, 1995.
19. Keen, R. E., Barrio, J. R., Huang, S-C., Hawkins, R. A., and Phelps,M. E. In vivo cerebral protein synthesis rates with leucyl-transfer RNAused as a precursor pool: determination of biochemical parameters tostructure tracer kinetics models for positron emission tomography.J. Cereb. Blood Flow Metab., 9: 429-445, 1989.
20. Huang, S-C., Phelps, M. E., Hoffmann, E. J., Sideris, K., Selin,
C. J., and Kuhl, D. E. Non-invasive determination of local cerebral
metabolic rate of glucose in man. Am. J. Physiol., 238: E69-E82, 1980.
2 1 . Laramore, G. E., and Spence, A. M. Boron neutron capture therapy
(BNCT) for high-grade gliomas of the brain: a cautionary note. Int. J.Radiat. Oncol. Biol. Phys., 36: 241-246, 1996.
22. Kabalka, G. W., Smith, G. T., Dyke, J. P., Reid, W. S., Longford,
C. P. D., Roberts, T. 0., Reddy, N. K., and HUbner, K. F. Evaluation offluorine- 18-BPA-fructose for boron neutron capture treatment planning.J. Nucl. Med., 38: 1762-1767, 1997.
23. Elowitz, E. H., Bergland, R. M., Coderre, J. A., Joel, D. D., Chadha,
M., and Chanana, A. D. Biodistribution of p-boronophenylalanine inpatients with glioblastoma multiforme for use in boron neutron capture
therapy. Neurosurgery (Baltimore), 42: 463-469, 1998.
24. Ueda, S., Imahori, Y., Ohmori, Y., Yoshino, E., Ono, K.,
Kobayashi, T., Takagaki, M., Oda, Y., Ido, T., and Mishima, Y. Positronemission tomography and boron neutron capture therapy system to the
patient with malignant brain tumor: the first clinical trial using ‘#{176}B-
BPA. in: Y. Mishima (ed), Cancer Neutron Capture Therapy, pp.
823-827. New York: Plenum Press, 1996.
25. Ueda, S., Imahori, Y., Ohmori, Y., Kusuki. T., Yoshino, E.,Takagaki, M., Kobayashi, T., Ono, K., Fujii, R., and Ido, 1. Positronemission tomography boron neutron capture therapy system and clinical
application to patients with malignant glioma. In: B. Larsson, J.Crawford, and R. Weinreich (eds.), Advances in Neutron Capture Ther-
apy, Vol. II, Chemistry and Biology, pp. 280-285. Amsterdam: ElsevierScience Publishers, B. V., 1997.
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from

1998;4:1833-1841. Clin Cancer Res Y Imahori, S Ueda, Y Ohmori, et al. II.
parttherapy using boronophenylalanine for high-grade gliomas: Positron emission tomography-based boron neutron capture
Updated version
http://clincancerres.aacrjournals.org/content/4/8/1833
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/4/8/1833To request permission to re-use all or part of this article, use this link
on April 9, 2021. © 1998 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from