
Pineal Malignant B-cell Lymphoma with Lower Cranial Nerve ...
4
1205 □ CASE REPORT □ Pineal Malignant B-cell Lymphoma with Lower Cranial Nerve Involvement Takeshi Yoshida 1 , Yukio Tezuka 2 , Takanobu Hirosawa 2 , Hiroshi Umeki 3 , Haruo Obara 2 , Takeshi Sueyoshi 4 , Akimasa Yano 5 , Kazumitsu Tamaki 6 and Manabu Jonosono 1 Abstract A 62-year-old man was admitted to our hospital complaining of dysphagia and hoarseness that had per- sisted for five days. A neurological examination indicated bulbar palsy. Brain magnetic resonance imaging showed thickening of cranial nerves IX, X and XI, in addition to pineal body enlargement with diffuse con- trast enhancement. A tumor biopsy overriding the spinal root of the right XIth cranial nerve was performed. The histologic analysis confirmed a diagnosis of diffuse large B-cell lymphoma. Malignant lymphoma should be considered in the differential diagnosis of pineal region tumors. Furthermore, obtaining histological confir- mation is crucial for making proper management decisions. Key words: malignant lymphoma, pineal gland, bulbar palsy (Intern Med 53: 1205-1208, 2014) (DOI: 10.2169/internalmedicine.53.1002) Introduction Approximately 1-2% of patients with non-Hodgkin’s lym- phoma (NHL) present with primary central nervous system (CNS) disease at the initial diagnosis (1). Among them, the occurrence of malignant lymphoma in the pineal region is very rare, as only a few such cases have been re- ported (2-7). We herein report a case of pineal region malig- nant lymphoma with lower cranial nerve involvement and review the previous literature. Case Report A 62-year-old man was admitted to our hospital com- plaining of dysphagia and hoarseness that had persisted for five days. Most pronounced was a difficulty in swallowing liquids. He denied previously having similar episodes, fever, night sweats, weight loss, dizziness, altered vision, weakness or numbness. His past medical history was unremarkable, except for hypertension. His father had died of malignant lymphoma at 81 years of age. On a physical examination, there was no lymphadenopathy or abdominal organomegaly. A neurological examination revealed a positive curtain sign (uvula deviated to the left side), hoarseness and a decreased gag reflex. The remainder of the neurological exam, includ- ing assessments of other cranial nerves, the motor and sen- sory systems, the cerebellar function and gait, was normal. The patient was admitted to the neurology department for a further investigation of his symptoms. The results of labora- tory tests were as follows: white blood cell count=5.8×10 3 / μL (4.8-8.5×10 3 /μL); red blood cell count=4.53×10 6 /μL (3.70-5.00×10 6 /μL); hemoglobin=14.5 g/dL (12.0-16.0 g/ dL); platelet count=14.1×10 4 /μL (13-37×10 4 /μL); lactate de- hydrogenase (LDH)=175 IU/L (120-240 IU/L); angiotensin- converting enzyme (ACE)=6.0 IU/L (8.3-21.4 IU/L); cere- brospinal fluid (CSF) cell count=120/mm 3 (lymphocytes: 99%, neutrophils: 1%) (<5/mm 3 ); CSF protein=54 mg/dL (15-45 mg/dL); and CSF immunoglobulin G index=0.91. Blood and CSF cultures for bacteria and acid-fast bacilli were negative. The levels of serum beta-D-glucan as well as serum and CSF cryptococcal antigens were within the nor- mal limits. HIV antibodies were negative. Fiber optic laryn- goscopy showed a poor soft palate and vocal cord move- 1 Department of Neurology, Okinawa Chubu Hospital, Japan, 2 Department of Internal Medicine, Okinawa Chubu Hospital, Japan, 3 Department of Otolaryngology, Okinawa Chubu Hospital, Japan, 4 Department of Radiology, Okinawa Chubu Hospital, Japan, 5 Department of Neurosurgery, Okinawa Chubu Hospital, Japan and 6 Department of Hematology & Oncology, Okinawa Chubu Hospital, Japan Received for publication July 21, 2013; Accepted for publication January 13, 2014 Correspondence to Dr. Takeshi Yoshida, [email protected]
Transcript of Pineal Malignant B-cell Lymphoma with Lower Cranial Nerve ...

1205
□ CASE REPORT □
Pineal Malignant B-cell Lymphoma with Lower CranialNerve Involvement
Takeshi Yoshida 1, Yukio Tezuka 2, Takanobu Hirosawa 2, Hiroshi Umeki 3, Haruo Obara 2,
Takeshi Sueyoshi 4, Akimasa Yano 5, Kazumitsu Tamaki 6 and Manabu Jonosono 1
Abstract
A 62-year-old man was admitted to our hospital complaining of dysphagia and hoarseness that had per-
sisted for five days. A neurological examination indicated bulbar palsy. Brain magnetic resonance imaging
showed thickening of cranial nerves IX, X and XI, in addition to pineal body enlargement with diffuse con-
trast enhancement. A tumor biopsy overriding the spinal root of the right XIth cranial nerve was performed.
The histologic analysis confirmed a diagnosis of diffuse large B-cell lymphoma. Malignant lymphoma should
be considered in the differential diagnosis of pineal region tumors. Furthermore, obtaining histological confir-
mation is crucial for making proper management decisions.
Key words: malignant lymphoma, pineal gland, bulbar palsy
(Intern Med 53: 1205-1208, 2014)(DOI: 10.2169/internalmedicine.53.1002)
Introduction
Approximately 1-2% of patients with non-Hodgkin’s lym-
phoma (NHL) present with primary central nervous system
(CNS) disease at the initial diagnosis (1). Among them, the
occurrence of malignant lymphoma in the pineal region is
very rare, as only a few such cases have been re-
ported (2-7). We herein report a case of pineal region malig-
nant lymphoma with lower cranial nerve involvement and
review the previous literature.
Case Report
A 62-year-old man was admitted to our hospital com-
plaining of dysphagia and hoarseness that had persisted for
five days. Most pronounced was a difficulty in swallowing
liquids. He denied previously having similar episodes, fever,
night sweats, weight loss, dizziness, altered vision, weakness
or numbness. His past medical history was unremarkable,
except for hypertension. His father had died of malignant
lymphoma at 81 years of age. On a physical examination,
there was no lymphadenopathy or abdominal organomegaly.
A neurological examination revealed a positive curtain sign
(uvula deviated to the left side), hoarseness and a decreased
gag reflex. The remainder of the neurological exam, includ-
ing assessments of other cranial nerves, the motor and sen-
sory systems, the cerebellar function and gait, was normal.
The patient was admitted to the neurology department for a
further investigation of his symptoms. The results of labora-
tory tests were as follows: white blood cell count=5.8×103/
μL (4.8-8.5×103/μL); red blood cell count=4.53×106/μL
(3.70-5.00×106/μL); hemoglobin=14.5 g/dL (12.0-16.0 g/
dL); platelet count=14.1×104/μL (13-37×104/μL); lactate de-
hydrogenase (LDH)=175 IU/L (120-240 IU/L); angiotensin-
converting enzyme (ACE)=6.0 IU/L (8.3-21.4 IU/L); cere-
brospinal fluid (CSF) cell count=120/mm3 (lymphocytes:
99%, neutrophils: 1%) (<5/mm3); CSF protein=54 mg/dL
(15-45 mg/dL); and CSF immunoglobulin G index=0.91.
Blood and CSF cultures for bacteria and acid-fast bacilli
were negative. The levels of serum beta-D-glucan as well as
serum and CSF cryptococcal antigens were within the nor-
mal limits. HIV antibodies were negative. Fiber optic laryn-
goscopy showed a poor soft palate and vocal cord move-
1Department of Neurology, Okinawa Chubu Hospital, Japan, 2Department of Internal Medicine, Okinawa Chubu Hospital, Japan, 3Department of
Otolaryngology, Okinawa Chubu Hospital, Japan, 4Department of Radiology, Okinawa Chubu Hospital, Japan, 5Department of Neurosurgery,
Okinawa Chubu Hospital, Japan and 6Department of Hematology & Oncology, Okinawa Chubu Hospital, Japan
Received for publication July 21, 2013; Accepted for publication January 13, 2014
Correspondence to Dr. Takeshi Yoshida, [email protected]
Intern Med 53: 1205-1208, 2014 DOI: 10.2169/internalmedicine.53.1002
1206
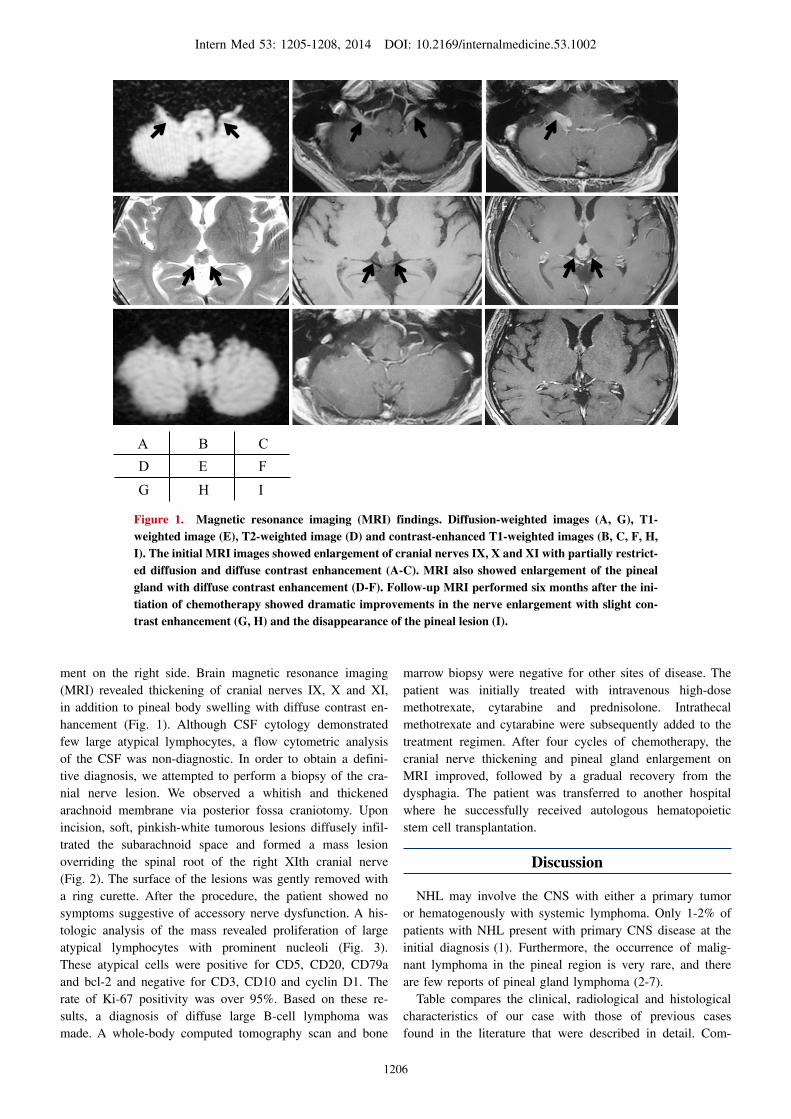
Figure 1. Magnetic resonance imaging (MRI) findings. Diffusion-weighted images (A, G), T1-weighted image (E), T2-weighted image (D) and contrast-enhanced T1-weighted images (B, C, F, H, I). The initial MRI images showed enlargement of cranial nerves IX, X and XI with partially restrict-ed diffusion and diffuse contrast enhancement (A-C). MRI also showed enlargement of the pineal gland with diffuse contrast enhancement (D-F). Follow-up MRI performed six months after the ini-tiation of chemotherapy showed dramatic improvements in the nerve enlargement with slight con-trast enhancement (G, H) and the disappearance of the pineal lesion (I).
F
A B CD E F G H I
ment on the right side. Brain magnetic resonance imaging
(MRI) revealed thickening of cranial nerves IX, X and XI,
in addition to pineal body swelling with diffuse contrast en-
hancement (Fig. 1). Although CSF cytology demonstrated
few large atypical lymphocytes, a flow cytometric analysis
of the CSF was non-diagnostic. In order to obtain a defini-
tive diagnosis, we attempted to perform a biopsy of the cra-
nial nerve lesion. We observed a whitish and thickened
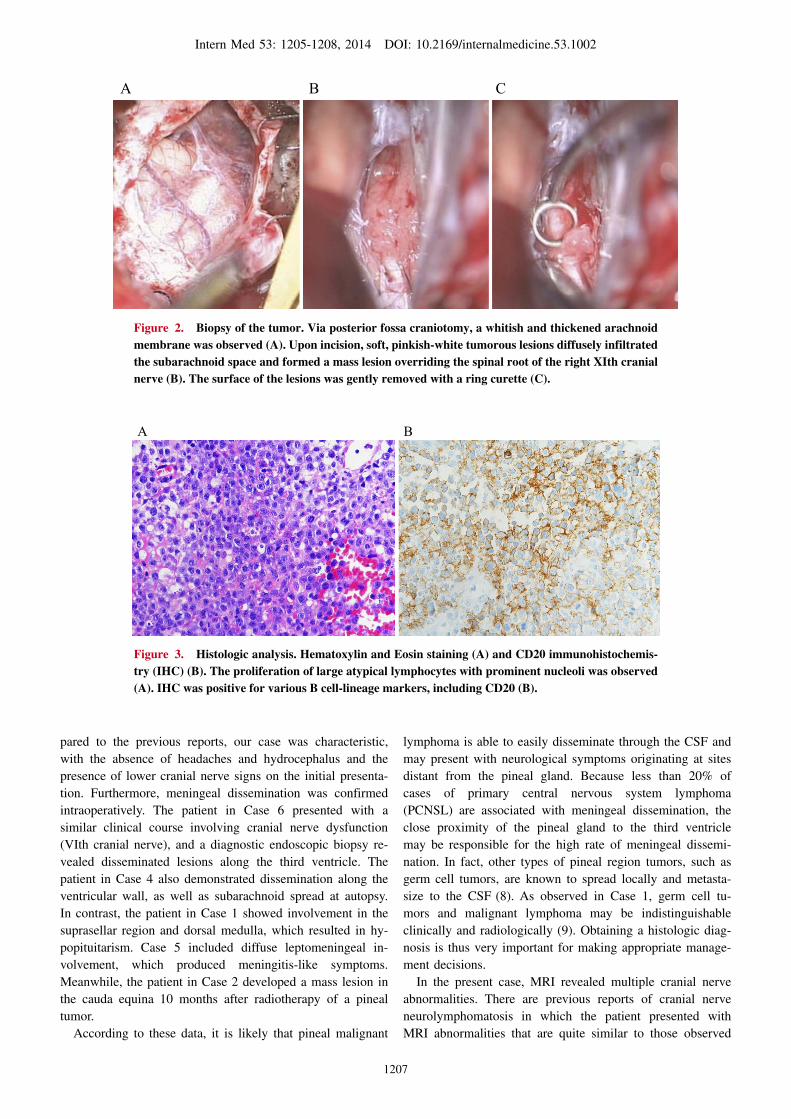
arachnoid membrane via posterior fossa craniotomy. Upon
incision, soft, pinkish-white tumorous lesions diffusely infil-
trated the subarachnoid space and formed a mass lesion
overriding the spinal root of the right XIth cranial nerve
(Fig. 2). The surface of the lesions was gently removed with
a ring curette. After the procedure, the patient showed no
symptoms suggestive of accessory nerve dysfunction. A his-
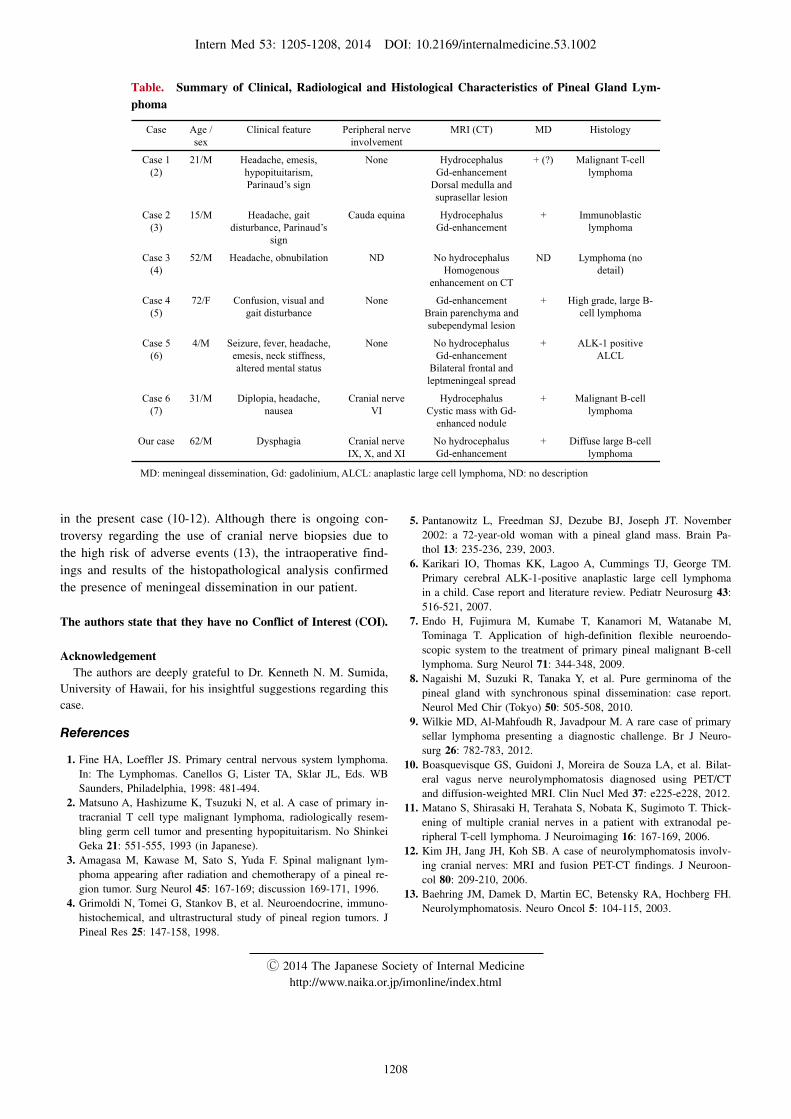
tologic analysis of the mass revealed proliferation of large
atypical lymphocytes with prominent nucleoli (Fig. 3).
These atypical cells were positive for CD5, CD20, CD79a
and bcl-2 and negative for CD3, CD10 and cyclin D1. The
rate of Ki-67 positivity was over 95%. Based on these re-
sults, a diagnosis of diffuse large B-cell lymphoma was
made. A whole-body computed tomography scan and bone
marrow biopsy were negative for other sites of disease. The
patient was initially treated with intravenous high-dose
methotrexate, cytarabine and prednisolone. Intrathecal
methotrexate and cytarabine were subsequently added to the
treatment regimen. After four cycles of chemotherapy, the
cranial nerve thickening and pineal gland enlargement on
MRI improved, followed by a gradual recovery from the
dysphagia. The patient was transferred to another hospital
where he successfully received autologous hematopoietic
stem cell transplantation.
Discussion
NHL may involve the CNS with either a primary tumor
or hematogenously with systemic lymphoma. Only 1-2% of
patients with NHL present with primary CNS disease at the
initial diagnosis (1). Furthermore, the occurrence of malig-
nant lymphoma in the pineal region is very rare, and there
are few reports of pineal gland lymphoma (2-7).
Table compares the clinical, radiological and histological
characteristics of our case with those of previous cases
found in the literature that were described in detail. Com-
Intern Med 53: 1205-1208, 2014 DOI: 10.2169/internalmedicine.53.1002
1207
Figure 2. Biopsy of the tumor. Via posterior fossa craniotomy, a whitish and thickened arachnoid membrane was observed (A). Upon incision, soft, pinkish-white tumorous lesions diffusely infiltrated the subarachnoid space and formed a mass lesion overriding the spinal root of the right XIth cranial nerve (B). The surface of the lesions was gently removed with a ring curette (C).
BA C
Figure 3. Histologic analysis. Hematoxylin and Eosin staining (A) and CD20 immunohistochemis-try (IHC) (B). The proliferation of large atypical lymphocytes with prominent nucleoli was observed (A). IHC was positive for various B cell-lineage markers, including CD20 (B).
A B
pared to the previous reports, our case was characteristic,
with the absence of headaches and hydrocephalus and the
presence of lower cranial nerve signs on the initial presenta-
tion. Furthermore, meningeal dissemination was confirmed
intraoperatively. The patient in Case 6 presented with a
similar clinical course involving cranial nerve dysfunction
(VIth cranial nerve), and a diagnostic endoscopic biopsy re-
vealed disseminated lesions along the third ventricle. The
patient in Case 4 also demonstrated dissemination along the
ventricular wall, as well as subarachnoid spread at autopsy.
In contrast, the patient in Case 1 showed involvement in the
suprasellar region and dorsal medulla, which resulted in hy-
popituitarism. Case 5 included diffuse leptomeningeal in-
volvement, which produced meningitis-like symptoms.
Meanwhile, the patient in Case 2 developed a mass lesion in
the cauda equina 10 months after radiotherapy of a pineal
tumor.
According to these data, it is likely that pineal malignant
lymphoma is able to easily disseminate through the CSF and
may present with neurological symptoms originating at sites
distant from the pineal gland. Because less than 20% of
cases of primary central nervous system lymphoma
(PCNSL) are associated with meningeal dissemination, the
close proximity of the pineal gland to the third ventricle
may be responsible for the high rate of meningeal dissemi-
nation. In fact, other types of pineal region tumors, such as
germ cell tumors, are known to spread locally and metasta-
size to the CSF (8). As observed in Case 1, germ cell tu-
mors and malignant lymphoma may be indistinguishable
clinically and radiologically (9). Obtaining a histologic diag-
nosis is thus very important for making appropriate manage-
ment decisions.
In the present case, MRI revealed multiple cranial nerve
abnormalities. There are previous reports of cranial nerve
neurolymphomatosis in which the patient presented with
MRI abnormalities that are quite similar to those observed
Intern Med 53: 1205-1208, 2014 DOI: 10.2169/internalmedicine.53.1002
1208
Table. Summary of Clinical, Radiological and Histological Characteristics of Pineal Gland Lym-phoma
Case Age / sex
Clinical feature Peripheral nerve involvement
MRI (CT) MD Histology
Case 1(2)
21/M Headache, emesis,hypopituitarism, Parinaud’s sign
None HydrocephalusGd-enhancement
Dorsal medulla and suprasellar lesion
+ (?) Malignant T-cell lymphoma
Case 2(3)
15/M Headache, gait disturbance, Parinaud’s
sign
Cauda equina HydrocephalusGd-enhancement
+ Immunoblasticlymphoma
Case 3(4)
52/M Headache, obnubilation ND No hydrocephalusHomogenous
enhancement on CT
ND Lymphoma (no detail)
Case 4(5)
72/F Confusion, visual and gait disturbance
None Gd-enhancementBrain parenchyma and subependymal lesion
+ High grade, large B-cell lymphoma
Case 5(6)
4/M Seizure, fever, headache, emesis, neck stiffness, altered mental status
None No hydrocephalusGd-enhancement
Bilateral frontal and leptmeningeal spread
+ ALK-1 positiveALCL
Case 6(7)
31/M Diplopia, headache, nausea
Cranial nerveVI
HydrocephalusCystic mass with Gd-
enhanced nodule
+ Malignant B-cell lymphoma
Our case 62/M Dysphagia Cranial nerve IX, X, and XI
No hydrocephalusGd-enhancement
+ Diffuse large B-cell lymphoma
MD: meningeal dissemination, Gd: gadolinium, ALCL: anaplastic large cell lymphoma, ND: no description
in the present case (10-12). Although there is ongoing con-
troversy regarding the use of cranial nerve biopsies due to
the high risk of adverse events (13), the intraoperative find-
ings and results of the histopathological analysis confirmed
the presence of meningeal dissemination in our patient.
The authors state that they have no Conflict of Interest (COI).
AcknowledgementThe authors are deeply grateful to Dr. Kenneth N. M. Sumida,
University of Hawaii, for his insightful suggestions regarding this
case.
References
1. Fine HA, Loeffler JS. Primary central nervous system lymphoma.
In: The Lymphomas. Canellos G, Lister TA, Sklar JL, Eds. WB
Saunders, Philadelphia, 1998: 481-494.
2. Matsuno A, Hashizume K, Tsuzuki N, et al. A case of primary in-
tracranial T cell type malignant lymphoma, radiologically resem-
bling germ cell tumor and presenting hypopituitarism. No Shinkei
Geka 21: 551-555, 1993 (in Japanese).
3. Amagasa M, Kawase M, Sato S, Yuda F. Spinal malignant lym-
phoma appearing after radiation and chemotherapy of a pineal re-
gion tumor. Surg Neurol 45: 167-169; discussion 169-171, 1996.
4. Grimoldi N, Tomei G, Stankov B, et al. Neuroendocrine, immuno-
histochemical, and ultrastructural study of pineal region tumors. J
Pineal Res 25: 147-158, 1998.
5. Pantanowitz L, Freedman SJ, Dezube BJ, Joseph JT. November
2002: a 72-year-old woman with a pineal gland mass. Brain Pa-
thol 13: 235-236, 239, 2003.
6. Karikari IO, Thomas KK, Lagoo A, Cummings TJ, George TM.
Primary cerebral ALK-1-positive anaplastic large cell lymphoma
in a child. Case report and literature review. Pediatr Neurosurg 43:
516-521, 2007.
7. Endo H, Fujimura M, Kumabe T, Kanamori M, Watanabe M,
Tominaga T. Application of high-definition flexible neuroendo-
scopic system to the treatment of primary pineal malignant B-cell
lymphoma. Surg Neurol 71: 344-348, 2009.
8. Nagaishi M, Suzuki R, Tanaka Y, et al. Pure germinoma of the
pineal gland with synchronous spinal dissemination: case report.
Neurol Med Chir (Tokyo) 50: 505-508, 2010.
9. Wilkie MD, Al-Mahfoudh R, Javadpour M. A rare case of primary
sellar lymphoma presenting a diagnostic challenge. Br J Neuro-
surg 26: 782-783, 2012.
10. Boasquevisque GS, Guidoni J, Moreira de Souza LA, et al. Bilat-
eral vagus nerve neurolymphomatosis diagnosed using PET/CT
and diffusion-weighted MRI. Clin Nucl Med 37: e225-e228, 2012.
11. Matano S, Shirasaki H, Terahata S, Nobata K, Sugimoto T. Thick-
ening of multiple cranial nerves in a patient with extranodal pe-
ripheral T-cell lymphoma. J Neuroimaging 16: 167-169, 2006.
12. Kim JH, Jang JH, Koh SB. A case of neurolymphomatosis involv-
ing cranial nerves: MRI and fusion PET-CT findings. J Neuroon-
col 80: 209-210, 2006.
13. Baehring JM, Damek D, Martin EC, Betensky RA, Hochberg FH.
Neurolymphomatosis. Neuro Oncol 5: 104-115, 2003.
Ⓒ 2014 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imonline/index.html


















