Pijpe Et Al-2005-Arthritis & Rheumatism
11
ARTHRITIS & RHEUMATISM Vol. 52, No. 9, September 2005, pp 2740–2750 DOI 10.1002/art.21260 © 2005, American College of Rheumatology Rituximab Treatment in Patients With Primary Sjo ¨gren’s Syndrome An Open-Label Phase II Study J. Pijpe, 1 G. W. van Imhoff, 1 F. K. L. Spijkervet, 1 J. L. N. Roodenburg, 1 G. J. Wolbink, 2 K. Mansour, 1 A. Vissink, 1 C. G. M. Kallenberg, 1 and H. Bootsma 1 Objective. To investigate the safety and efficacy of B cell depletion treatment of patients with active pri- mary Sjo ¨gren’s syndrome of short duration (early pri- mary SS) and patients with primary SS and mucosa- associated lymphoid tissue (MALT)–type lymphoma (MALT/primary SS). Methods. Fifteen patients with primary SS were included in this phase II trial. Inclusion criteria for the early primary SS group were B cell hyperactivity (IgG >15 gm/liter), presence of autoantibodies (IgM rheu- matoid factor, anti-SSA/SSB), and short disease dura- tion (<4 years). Inclusion criteria for the MALT/ primary SS group were primary SS and an associated MALT-type lymphoma (Ann Arbor stage IE) localized in the parotid gland. Patients were treated with 4 infusions of rituximab (375 mg/m 2 ) given weekly after pretreatment with prednisone (25 mg) and clemastine. Patients were evaluated, using immunologic, salivary/ lacrimal function, and subjective parameters, at base- line and at 5 and 12 weeks after the first infusion. Results. Significant improvement of subjective symptoms and an increase in salivary gland function was observed in patients with residual salivary gland function. Immunologic analysis showed a rapid de- crease of peripheral B cells and stable levels of IgG. Human antichimeric antibodies (HACAs) developed in 4 of 15 patients (27%), all with early primary SS. Three of these patients developed a serum sickness–like dis- order. Of the 7 patients with MALT/primary SS, com- plete remission was achieved in 3, and disease was stable in 3 and progressive in 1. Conclusion. Findings of this phase II study sug- gest that rituximab is effective in the treatment of primary SS. The high incidence of HACAs and associ- ated side effects observed in this study needs further evaluation. Sjo ¨gren’s syndrome (SS) is a systemic auto- immune disease characterized by chronic inflammation of salivary and lacrimal glands, frequently accompanied by systemic symptoms. The presence of various autoan- tibodies such as rheumatoid factor (RF) and anti-SSA/ SSB antibodies, as well as hypergammaglobulinemia, is considered to reflect B cell hyperactivity. Five percent of patients with SS develop malignant B cell lymphoma, usually of the mucosa-associated lymphoid tissue (MALT) type and most frequently located in the major salivary glands (1). Currently, there is no evidence-based interven- tion therapy for SS. Corticosteroids and disease- modifying antirheumatic drugs (DMARDs) have no major effect on the disease course (2,3). Rituximab, a Presented in part at the 68th Annual Scientific Meeting of the American College of Rheumatology, San Antonio, TX, October 2004. Supported by the Innovation Fund of the University Medical Center Groningen. Part of the study medication was supplied by Roche, Woerden, The Netherlands. 1 J. Pijpe, MD, G. W. van Imhoff, MD, F. K. L. Spijkervet, DMD, PhD, J. L. N. Roodenburg, DMD, PhD, K. Mansour, MD, A. Vissink, MD, DMD, PhD, C. G. M. Kallenberg, MD, PhD, H. Bootsma, MD, PhD: University Medical Center Groningen, Gro- ningen, The Netherlands; 2 G. J. Wolbink, MD, PhD: Central Labora- tory of The Netherlands Red Cross Blood Transfusion Service, Amsterdam, The Netherlands. Address correspondence and reprint requests to J. Pijpe, MD, Department of Oral and Maxillofacial Surgery, University Medical Center Groningen, PO Box 30.001, 9700 RB Groningen, The Nether- lands. E-mail: [email protected]. Submitted for publication February 10, 2005; accepted in revised form June 3, 2005. 2740
description
Pijpe Et Al-2005-Arthritis & Rheumatism
Transcript of Pijpe Et Al-2005-Arthritis & Rheumatism

ARTHRITIS & RHEUMATISMVol. 52, No. 9, September 2005, pp 2740–2750DOI 10.1002/art.21260© 2005, American College of Rheumatology
Rituximab Treatment in Patients WithPrimary Sjogren’s Syndrome
An Open-Label Phase II Study
J. Pijpe,1 G. W. van Imhoff,1 F. K. L. Spijkervet,1 J. L. N. Roodenburg,1 G. J. Wolbink,2
K. Mansour,1 A. Vissink,1 C. G. M. Kallenberg,1 and H. Bootsma1
Objective. To investigate the safety and efficacy ofB cell depletion treatment of patients with active pri-mary Sjogren’s syndrome of short duration (early pri-mary SS) and patients with primary SS and mucosa-associated lymphoid tissue (MALT)–type lymphoma(MALT/primary SS).
Methods. Fifteen patients with primary SS wereincluded in this phase II trial. Inclusion criteria for theearly primary SS group were B cell hyperactivity (IgG>15 gm/liter), presence of autoantibodies (IgM rheu-matoid factor, anti-SSA/SSB), and short disease dura-tion (<4 years). Inclusion criteria for the MALT/primary SS group were primary SS and an associatedMALT-type lymphoma (Ann Arbor stage IE) localizedin the parotid gland. Patients were treated with 4infusions of rituximab (375 mg/m2) given weekly afterpretreatment with prednisone (25 mg) and clemastine.Patients were evaluated, using immunologic, salivary/
lacrimal function, and subjective parameters, at base-line and at 5 and 12 weeks after the first infusion.
Results. Significant improvement of subjectivesymptoms and an increase in salivary gland functionwas observed in patients with residual salivary glandfunction. Immunologic analysis showed a rapid de-crease of peripheral B cells and stable levels of IgG.Human antichimeric antibodies (HACAs) developed in4 of 15 patients (27%), all with early primary SS. Threeof these patients developed a serum sickness–like dis-order. Of the 7 patients with MALT/primary SS, com-plete remission was achieved in 3, and disease wasstable in 3 and progressive in 1.
Conclusion. Findings of this phase II study sug-gest that rituximab is effective in the treatment ofprimary SS. The high incidence of HACAs and associ-ated side effects observed in this study needs furtherevaluation.
Sjogren’s syndrome (SS) is a systemic auto-immune disease characterized by chronic inflammationof salivary and lacrimal glands, frequently accompaniedby systemic symptoms. The presence of various autoan-tibodies such as rheumatoid factor (RF) and anti-SSA/SSB antibodies, as well as hypergammaglobulinemia, isconsidered to reflect B cell hyperactivity. Five percent ofpatients with SS develop malignant B cell lymphoma,usually of the mucosa-associated lymphoid tissue(MALT) type and most frequently located in the majorsalivary glands (1).
Currently, there is no evidence-based interven-tion therapy for SS. Corticosteroids and disease-modifying antirheumatic drugs (DMARDs) have nomajor effect on the disease course (2,3). Rituximab, a
Presented in part at the 68th Annual Scientific Meeting of theAmerican College of Rheumatology, San Antonio, TX, October 2004.
Supported by the Innovation Fund of the University MedicalCenter Groningen. Part of the study medication was supplied byRoche, Woerden, The Netherlands.
1J. Pijpe, MD, G. W. van Imhoff, MD, F. K. L. Spijkervet,DMD, PhD, J. L. N. Roodenburg, DMD, PhD, K. Mansour, MD, A.Vissink, MD, DMD, PhD, C. G. M. Kallenberg, MD, PhD, H.Bootsma, MD, PhD: University Medical Center Groningen, Gro-ningen, The Netherlands; 2G. J. Wolbink, MD, PhD: Central Labora-tory of The Netherlands Red Cross Blood Transfusion Service,Amsterdam, The Netherlands.
Address correspondence and reprint requests to J. Pijpe, MD,Department of Oral and Maxillofacial Surgery, University MedicalCenter Groningen, PO Box 30.001, 9700 RB Groningen, The Nether-lands. E-mail: [email protected].
Submitted for publication February 10, 2005; accepted inrevised form June 3, 2005.
2740

chimeric murine/human anti-CD20 monoclonal anti-body that binds to the B cell surface antigen CD20, iscurrently used in the treatment of B cell lymphomas(4–6). It is also considered a promising agent for treat-ment of various autoimmune disorders, such as rheuma-toid arthritis (RA) and systemic lupus erythematosus(SLE) (7–9). It has been hypothesized that because Bcells appear to be involved in the pathogenesis of SS, Bcell depletion may lead to a decrease of disease activity.Progressive loss of salivary gland function occurs mainlyin early SS (i.e., the first 4 years after disease onset), andsalivary gland function stays relatively stable during thesubsequent course (10). Patients with residual exocrinegland function, i.e., those with early SS, may benefitmost from systemic therapy. Based on these consider-ations, this phase II study was undertaken to investigatethe safety and efficacy of rituximab in the treatment ofpatients with early, active primary SS and patients withprimary SS with associated MALT-type lymphoma.
PATIENTS AND METHODS
Study design. This was a prospective, single-center,open-label phase II study. The study protocol was approved bythe ethics committee of University Medical Center Groningen.All patients provided written informed consent.
Patients. All patients were at least 18 years old, and allfulfilled the American-European consensus criteria for pri-mary SS, including histopathologic criteria (11). Patients hadeither primary SS with active disease and short duration (earlyprimary SS group) or primary SS with associated MALT-typelymphoma (MALT/primary SS group). Inclusion criteria forthe early primary SS group were increased B cell activity (IgG�15 gm/liter) in combination with the presence of bothIgM-RF and anti-SSA or anti-SSB antibodies, short diseaseduration (maximum 4 years from the onset of oral symptoms),and absence of MALT-type lymphoma. Inclusion criteria forthe MALT/primary SS group were primary SS and associatedMALT-type lymphoma, localized in the parotid gland andconfirmed by incision biopsy (Ann Arbor stage IE). Patientswho had another known autoimmune disease or had beenpreviously treated with monoclonal antibodies were excluded.Treatment with DMARDS (e.g., hydroxychloroquine, metho-trexate, cyclosporine) and corticosteroids was not allowedduring the study and had to be discontinued at least 6 monthsbefore baseline, except in patients with severe extraglandularmanifestations necessitating continuation of their previoustreatment (with no change in dosage allowed) (patients 10, 13,and 14). The use of any type of systemic drug for the relief ofdryness-related symptoms (xerostomia, dry eyes) was notpermitted during the study.
Drug administration. Patients were treated with 4infusions of 375 mg/m2 rituximab (Roche, Woerden, TheNetherlands), given once weekly. To minimize infusion reac-tions, patients were pretreated with prednisone (25 mg intra-
venously), clemastine (2 mg intravenously), and acetamino-phen (1 gm orally) before each infusion. Prednisone at thisdose has been used as premedication in conjunction withrituximab treatment of patients with lymphoma (12).
Outcome measures. Patients were assessed for adverseevents and disease activity at baseline and at 5 weeks and 12weeks after initiation of rituximab treatment. Immunologic,salivary/lacrimal function, and subjective parameters were theresponse criteria. MALT-type lymphoma was restaged 12weeks after treatment initiation in the MALT/primary SSgroup.
Laboratory assessments. Laboratory assessments (in-cluding complete blood cell counts and serum biochemicalanalyses) were performed at baseline and at weeks 5 and 12.Levels of immunoglobulins (IgG, IgA, and IgM) and IgM-RFwere measured by nephelometry. Numbers of CD19� B cellsand CD3�, CD4�, CD8�, CD4�,CD25�, and CD8�,HLA–DR� T cells were measured by fluorescence-activated cellsorting. Rituximab-specific IgG (human antichimeric antibod-ies [HACAs]) was measured by an antigen binding test,essentially according to the procedure described by Aalberse etal (13). Briefly, serum (1 �l/test) was preincubated withagarose-immobilized protein A (1 mg/test; Pharmacia, Upp-sala, Sweden). Nonbound serum components were removed bywashing, after which 1 ng of 125I-labeled pepsin-treated ritux-imab was added. After overnight incubation, nonbound radio-label was washed away and agarose-bound radioactivity wasmeasured. Highly reactive samples were retested at appropri-ate dilutions (Central Laboratory of The Netherlands RedCross Blood Transfusion Service). Samples obtained from thepatients before treatment with rituximab were used as controls.
Functional parameters. Salivary gland. Whole and glan-dular saliva were collected in a standardized manner at base-line and at the 5-week and 12-week followup visits. Wholesaliva was collected as recommended in the revised American-European criteria (11). Unstimulated salivary secretions werecollected during a 15-minute period, followed by collection ofstimulated secretions (2% citric acid solution applied to thelateral border of the tongue every 30 seconds) during a periodof 10 minutes. Flow rates were calculated, and sialochemicalanalysis was performed. Glandular saliva specimens obtainedsimultaneously from both individual parotid glands and thesubmandibular/sublingual glands were collected with Lashleycups (placed on the orifices of the Stensen duct) and by syringeaspiration (from the orifices of the Wharton duct locatedanteriorly in the floor of the mouth), respectively (14). Sialo-chemical analysis focused on the concentration of sodium inparotid saliva, because an increase in sodium is indicative ofchronic sialadenitis (15).
Lacrimal gland. Parameters included in the revisedAmerican-European criteria (11) were evaluated by the sameophthalmologist at baseline and during the 5-week and 12-week followup visits. Schirmer’s test was carried out with afilter paper strip, which was placed in the lower fornix of theconjunctiva of the nonanesthetized eye. The amount of wettingwas measured after 5 minutes. The rose bengal test wasperformed by instillation of a 1% rose bengal solution in botheyes. After 1 or 2 full blinks, the intensity of staining of bothmedial and lateral bulbar conjunctiva and the cornea was
RITUXIMAB IN SS 2741

scored (up to 3 points for each section [1 � sparsely scattered;2 � densely scattered; 3 � confluent]), such that a maximum of9 points could be obtained (16). To determine the tearbreak-up time (interval between a complete blink and theappearance of the first randomly distributed dry spots), a 1%fluorescein solution was instilled in the inferior fornix of botheyes. The patient was asked to blink a few times, after whichthe interval in seconds between the last blink and the firstbreak in the tear film was measured (17).
Subjective assessments. At baseline and at weeks 5 and12, patients rated oral dryness during the day, oral drynessduring the night, difficulty in swallowing dry food without anyadditional liquids, and dryness of eyes, on a 100-mm visualanalog scale. Patients also completed the MultidimensionalFatigue Inventory (MFI) (18) and the Short Form 36 (SF-36)(19). The MFI is a 20-item self-report scale, which has beenvalidated for SS (20) and is designed to objectively measurefatigue, including the following dimensions: 1) general fatigue,2) physical fatigue, 3) mental fatigue, 4) reduced motivation,and 5) reduced activity. A higher score (possible range 4–20)indicates a higher level of fatigue. The SF-36 questionnaire,which has been used for measuring subjective well-being, has
also been validated for SS (21). A higher score indicates ahigher level of well-being.
MALT-type lymphoma staging. Prior to treatment, allpatients with MALT-type lymphoma underwent staging pro-cedures including history, physical examination, completeblood cell counts, chemistry profile, computed tomography ofthe chest, abdomen, and pelvis, magnetic resonance imaging ofthe head and neck, and bone marrow biopsy. The effect ofrituximab treatment on MALT-type lymphoma was evaluatedby complete clinical restaging 12 weeks after treatment initia-tion. Restaging included repeat administration of all stagingtests for which results were previously abnormal. Tumorresponses were classified as complete response, partial re-sponse, stable disease, or relapsing/progressive disease, ac-cording to the standardized response criteria for non-Hodgkin’s lymphoma (22).
Statistical analysis. Data are presented as the mean ormedian and range, and were analyzed on an intent-to-treatbasis. The statistical significance of the change from baselinewas measured by Wilcoxon’s signed rank test. The Mann-Whitney U test (in SPSS version 10.0) was used to analyze the
Table 1. Characteristics of the patients at baseline*
Patient Age/sex
Diseaseduration,months
Anti-SSA/SSBpositivity
IgG,gm/liter
IgM-RF,KIU/liter
Monoclonalprotein
Parotid glandswelling Extraglandular manifestations
Early primary SS1† 41/F 36 SSA/SSB 18.2 125 � No Raynaud’s phenomenon, fatigue,
arthralgia2 56/F 30 SSA/SSB 21.4 168 � Yes Raynaud’s phenomenon, fatigue,
arthralgia3 50/F 18 SSA/SSB 18.9 741 � No Raynaud’s phenomenon, fatigue4 65/F 48 SSA/SSB 15.8 108 � Yes Raynaud’s phenomenon, fatigue,
arthralgia5† 39/F 24 SSA/SSB 15.4 16 � No Raynaud’s phenomenon, fatigue,
arthralgia6 49/F 12 SSA/SSB 15.6 32 � No Fatigue, arthralgia7 43/F 18 SSA 15.2 647 � No Raynaud’s phenomenon, fatigue,
arthralgia, myalgia8† 27/F 36 SSA 30.2 569 � Yes Arthralgia, pulmonary
involvementMALT/primary SS
9 62/M 24 SSA/SSB 22.1 267 � No Fatigue, arthralgia10‡ 52/F 120 SSA 6.8 101 � Yes Fatigue, pulmonary, hepatic, and
renal involvement, vasculitis11 48/F 108 SSA/SSB 12.4 80 � Yes None12 71/F 84 SSA/SSB 14.8 98 � Yes Fatigue, arthralgia13‡ 49/F 12 SSA/SSB 5.9 342 � Yes Raynaud’s phenomenon, fatigue,
arthritis, vasculitis andesophageal involvement
14‡ 40/F 120 SSA/SSB 14.7 124 � (IgG�) Yes Raynaud’s phenomenon, fatigue,arthralgia
15 55/F 84 SSA 15.1 25 � No Fatigue
* IgM-RF � IgM rheumatoid factor; SS � Sjogren’s syndrome; MALT � mucosa-associated lymphoid tissue–type lymphoma.† Patient in whom a serious adverse event developed after rituximab treatment.‡ Patient continued immunosuppressive treatment (patient 10 prednisone 15 mg/day, patient 13 prednisone 7.5 mg/day and methotrexate 15mg/week, patient 14 prednisone 5 mg/day and azathioprine 75 mg/day).
2742 PIJPE ET AL

differences between patient groups. P values less than 0.05were considered significant.
RESULTS
Characteristics of the patients. Baseline charac-teristics of the individual patients are summarized inTable 1. Between July 2003 and September 2004, 15consecutive patients with early primary SS (n � 8) orMALT/primary SS (n � 7) were prospectively enrolledin the study and treated with rituximab. The group ofpatients with early primary SS differed significantly (P �
0.05) at baseline from the group with MALT/primary SSwith regard to disease duration, flow rate of stimulatedwhole saliva, stimulated parotid flow, level of IgG, levelof CD4� T cells, and physical functioning (Tables 1 and2). In particular, the MALT/primary SS group wascharacterized by longer disease duration, and the major-ity of patients in this group had very low stimulatedsalivary secretion levels. Of the 7 patients with MALT/primary SS, 3 (patients 10, 13, and 14) had longstandingprimary SS (time since diagnosis of primary SS 13, 9, and4 years, respectively) complicated by recent persistent
Table 2. Laboratory, subjective, and functional assessments in the 14 patients who completed the study*
Early primary SS group MALT/primary SS group
Week 0 Week 5 Week 12 Week 0 Week 5 Week 12
Laboratory testsWBCs, 109/liter 4.8 (3.2–8.7) 4.2 (2.9–7.4) 4.6 (2.7–8.7) 4.5 (2.4–10.7) 4.9 (2.3–10.7) 6.0 (2.6–10.7)�2-microglobulin, gm/liter 2.5 (2–4.7) 2.8 (1.8–3.3) 2.4 (2.2–3.2) 2.5 (1.8–3.7) 2.8 (1.7–24) 2.4 (1.9–3.5)CD19� cells, 109/liter 0.17 (0.11–0.32) 0 (0–0)† 0 (0–0.11)† 0.10 (0.01–0.18) 0 (0–0)† 0 (0–0)†CD4� cells, 109/liter 0.53 (0.25–1.12)‡ 0.58 (0.29–1.03) 0.57 (0.27–1.25)† 0.33 (0.21–0.61) 0.33 (0.24–0.67) 0.30 (0.09–0.73)CD8� cells, 109/liter 0.20 (0.13–0.66) 0.20 (0.13–0.83) 0.21 (0.14–0.89) 0.23 (0.07–0.39) 0.25 (0.09–0.59) 0.21 (0.05–0.55)CD4�, CD25� cells, 109/liter 0.04 (0.02–0.06) 0.03 (0.02–0.05) 0.04 (0.02–0.07) 0.03 (0.01–0.13) 0.03 (0–0.19) 0.02 (0.01–0.55)CD8�, HLA–DR� cells,
109/liter0.02 (0.01–0.06) 0.02 (0.01–0.06) 0.02 (0.01–0.08) 0.03 (0–0.26) 0.12 (0–0.55) 0.02 (0.01–0.56)
Salivary testsUWS, ml/minute 0.04 (0–0.19) 0.07 (0.02–0.15) 0.08 (0.02–0.34) 0 (0–0.5) 0.01 (0–0.09) 0.01 (0–0.14)SWS, ml/minute 0.38 (0.2–1.38)‡ 0.62 (0.27–0.80) 0.58 (0.14–1.21) 0.01 (0–0.47) 0.01 (0–0.48) 0.02 (0.01–0.35)Parotid stimulated secretion,
ml/minute0.15 (0.01–0.5)‡ 0.21 (0.05–0.25) 0.21 (0.02–0.38) 0 (0–0.07) 0 (0.09) 0.01 (0–0.4)
Na in parotid saliva, mmoles/liter
19 (4–63) 11 (3–30) 8 (3–43)† 4 (4–4) 5 (5–5) 4 (3–4)
Eye testsSchirmer’s, mm/5 minutes 5 (1–33) 9 (2–30) 10 (2–34) 2 (0–5) 3 (1–6) 3 (2–4)Rose bengal score 6 (1–9) 5 (0–7)† 4 (0–6)† 7 (5–8) 6 (3–7)§ 5 (4–7)†Tear break-up time, seconds 2 (0–9) 7 (1–10)§ 7 (1–10)† 4 (0–6) 3 (0–8) 3 (0–5)
SubjectiveMFI
General fatigue 18 (11–20) 14 (8–18) 9 (4–20)† 17 (15–20) 16 (9–19) 14 (8–20)Physical fatigue 15 (6–18) 13 (9–19) 8 (6–19)† 17 (12–19) 16 (8–19) 17 (4–20)Reduced activity 13 (7–16) 12 (6–16) 6 (4–16)† 14 (9–20) 13 (7–17) 15 (5–20)Reduced motivation 11 (6–16) 12 (6–19) 6 (4–16)† 11 (6–16) 8 (7–19) 11 (5–17)Mental fatigue 14 (4–19) 9 (5–20) 12 (4–17) 12 (8–20) 12 (4–18) 12 (8–20)
SF-36Physical functioning 1 (1–90)‡ 72 (55–90)† 85 (40–100)† 55 (15–75) 50 (20–90) 50 (20–95)Social functioning 63 (13–100) 63 (50–75) 75 (13–100) 25 (0–75) 50 (0–88)§ 63 (13–100)Role physical 13 (0–100) 25 (0–100) 11 (0–100)§ 0 (0–50) 0 (0–100) 0 (0–100)Role emotional 100 (100–100) 100 (33–100) 100 (0–100) 66 (0–100) 0 (0–100)§ 1 (0–100)Mental health 80 (40–88) 80 (60–92) 84 (40–100) 64 (36–80) 64 (16–72) 72 (12–84)Vitality 38 (20–80) 45 (25–80) 65 (20–80)† 30 (10–50) 45 (20–50) 40 (15–70)Bodily pain 56 (32–100) 58 (45–100) 78 (67–90)§ 45 (20–100) 78 (33–100)§ 45 (33–100)General health perception 43 (15–70) 50 (25–65) 60 (10–65) 30 (0–70) 40 (20–75)§ 35 (15–75)Health change 25 (0–100) 50 (0–100)§ 75 (0–100)† 0 (0–50) 50 (0–75) 50 (0–100)
* Values are the median (range). WBCs � white blood cells; UWS � unstimulated whole saliva; SWS � stimulated whole saliva; MFI �Multidimensional Fatigue Inventory (range 4–20; higher score indicates higher level of fatigue); SF-36 � Short Form 36 (higher score indicateshigher level of well-being) (see Table 1 for other definitions).† P � 0.05 versus baseline value in the same patient group, by Wilcoxon’s signed rank test.‡ P � 0.05 versus baseline value in the MALT/primary SS group, by Mann-Whitney U test.§ 0.05 � P � 0.10 versus baseline value in the same patient group, by Wilcoxon’s signed rank test.
RITUXIMAB IN SS 2743

parotid gland swelling, prompting performance of aparotid gland biopsy which showed MALT-type lym-phoma. The other 4 patients in the MALT/primary SSgroup (patients 9, 11, 12, and 15) had been referred forevaluation for possible SS, and routine diagnostic pa-rotid gland biopsy revealed SS and concomitant MALT-type lymphoma. Of the latter patients, patients 11 and 12also had swelling of the right parotid gland.
Efficacy. Three patients with early primary SS(patients 1, 5, and 8) did not complete the treatmentprotocol because of a serious adverse event. Each ofthese 3 patients received only 2 infusions of rituximab.All but 1 of them (patient 1) completed the studyassessments. The latter patient refused further followup.There were no serious adverse events in the MALT/primary SS group, and all 7 patients with MALT/primary SS completed the study. Analysis of efficacycould therefore be performed in 14 patients. Treatmentwith rituximab resulted in improvement in various mea-sures of primary SS disease activity in the patients withearly primary SS. Of the 7 patients with MALT/primarySS, complete clinical remission was achieved in 3 (pa-tients 11, 12, and 14), and disease remained stable in 3(patients 9, 10, and 15) and progressed in 1 (patient 13).After an initial improvement of the extraglandular man-ifestations, patient 10 had an exacerbation at 24 weeksafter her SS had become active, necessitating additionalimmunosuppressive treatment.
Laboratory assessments in the 14 patients whocompleted the study. Rapid decrease of peripheral Bcells, lasting for 12 weeks, occurred in all but 2 patients
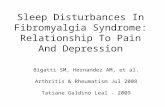
(patients 5 and 8). The latter patients had received only2 infusions of rituximab. B cell depletion was accompa-nied by a significant decrease in IgM-RF levels at week5 in patients with MALT/primary SS (Figure 1). In the 7patients with early primary SS, a small but significantincrease in the number of CD4� T cells was seen atweek 12 (P � 0.05) (Table 2). No changes in T cell subsetswere observed in patients with MALT/primary SS. Levelsof IgG, IgA, IgM, and �2-microglobulin did not change ineither group of patients. Monoclonal protein disappearedfollowing treatment in the only patient who was positive forthis protein at baseline (patient 14).
Functional assessments in the 14 patients whocompleted the study. Salivary gland. Although no signif-icant changes were seen in whole saliva, stimulatedsubmandibular/sublingual salivary secretion increasedsignificantly in patients whose stimulated salivary flowwas �0.10 ml/minute at baseline (all patients with earlyprimary SS and 2 with MALT/primary SS). No changewas seen in patients who had a stimulated salivary flowof �0.10 ml/minute at baseline (5 patients with MALT/primary SS) (Figures 2A and B). Furthermore, a signif-icant decrease in sodium levels in parotid saliva frombaseline to week 12 was observed in the patients with anincrease in salivary function (Table 2).
Lacrimal gland. Results of the Schirmer’s test didnot change significantly, but significant improvements inthe rose bengal score in the group with early primary SSand the group with MALT/primary SS, and in tearbreak-up time in the group with early primary SS, wereobserved (Table 2).
Figure 1. Levels of IgM rheumatoid factor (IgM-RF) at weeks 0, 5, and 12 in individual patientswith early primary Sjogren’s syndrome (pSS) (patients 2–8) and patients with primary SS withmucosa-associated lymphoid tissue (MALT)–type lymphoma (patients 9–15).
2744 PIJPE ET AL

Subjective assessments in the 14 patients who com-pleted the study. Significant improvement was observedin patients’ assessment of mouth dryness (Figure 3),arthralgia, physical functioning, vitality, and most do-
mains of the MFI in the group with early primary SS. Inpatients with MALT/primary SS, these features re-mained stable or showed a tendency toward slight im-provement (Table 2).
Long-term followup data were available on 7patients. Peripheral blood B cell counts returned tonormal after 6–9 months, followed by an increase inIgM-RF levels and a concomitant increase in fatigue. In3 of 4 patients with an initial increase in salivary glandfunction (3 with early primary SS and 1 with MALT/primary SS), this increase persisted up to 48 weeks aftertreatment. In 2 patients with MALT/primary SS (pa-tients 10 and 13), increases in IgM-RF levels precededexacerbation of disease activity (vasculitis and respira-tory insufficiency at week 24 [patient 10]) or progressionof MALT-type lymphoma (suggested by parotid glandswelling and confirmed by parotid gland biopsy at week12 [patient 13]). In 1 of these patients (patient 13),peripheral blood B cells were not yet detectable at thetime of increase in the IgM-RF level.
Adverse events. Two patients with primary SS(patients 2 and 7) had a mild infusion reaction, i.e., feverand headache, after the first infusion. No additionaltreatment for the reaction was necessary. In patient 3,herpes zoster developed 10 days after the last infusion.She was treated by her general practitioner with acyclo-vir, which led to full recovery.
HACAs developed in 4 of the 8 patients withearly primary SS (50%) (patients 1, 2, 5, and 8), and innone of the patients with MALT/primary SS. In 3 of thepatients in whom HACAs developed (patients 1, 5, and
Figure 2. Mean � SEM stimulated submandibular/sublingual (SM/SL) salivary secretion at weeks 1 (baseline), 5, and 12 in A, patients with earlyprimary SS (n � 7) versus patients with MALT/primary SS (n � 7) and B, patients with primary SS whose stimulated whole saliva secretion (SWS)was �0.10 ml/minute at baseline (n � 9) versus patients with primary SS whose SWS secretion was �0.10 ml/minute at baseline (n � 5). � � P� 0.05 versus baseline, by Wilcoxon’s signed rank test. See Figure 1 for other definitions.
Figure 3. Mean and SEM scores of the severity of dry mouth and dryeyes at baseline, week 5, and week 12, assessed by patients on a100-mm visual analog scale, in patients with early primary SS (n � 7)and patients with MALT/primary SS (n � 7). � � P � 0.05 versusbaseline, by Wilcoxon’s signed rank test. See Figure 1 for definitions.
RITUXIMAB IN SS 2745

8), rituximab treatment was discontinued after 2 infu-sions, because of a serious side effect. These patientspresented 5–7 days after the second infusion of ritux-imab with fever (38–39°C), arthritis, serious arthralgia,and myalgia. Two of them also presented with purpuraon the extremities (Figure 4A). Skin biopsy of a purpuriclesion revealed moderate perivascular lymphocytic infil-tration in the dermis and subcutis, with nuclear debrisbut without leukocytoclastic vasculitis (Figure 4B). Di-rect immunofluorescence showed deposition of IgA,
IgM, and complement in the subepidermal vessel walls,but no deposition of IgG. There were no signs of viral orbacterial infections. Laboratory investigations revealedincreases in the erythrocyte sedimentation rate (ESR)and C-reactive protein (CRP) level in all 3 patients, andelevated complement C3d levels in patients 5 and 8. Adecreased level of complement C4 was observed inpatient 5 (Table 3).Proteinuria was not detectable in anyof the 3 patients. No significant changes in the ESR or inlevels of leukocytes, thrombocytes, or CRP were ob-
Figure 4. A, Purpura, which developed after the second infusion of rituximab, on the lower legs of patient8. B, Biopsy of a purpuric lesion from patient 8, showing perivascular lymphocytic infiltration in the dermisand subcutis, with nuclear debris (hematoxylin and eosin stained; original magnification � 40).
Table 3. Laboratory findings in the 3 patients with early primary Sjogren’s syndrome who experienced a serious adverse event of the treatmentwith rituximab*
Patient 1 Patient 5 Patient 8
Week0
DuringSAE
2–4 weeksafterSAE
48 weeksafterSAE
Week0
DuringSAE
2–4 weeksafterSAE
24 weeksafterSAE
Week0
DuringSAE
2–4 weeksafterSAE
24 weeksafterSAE
WBCs, 109/liter 3.5 2.4 4.2 NA 5.0 8.1 3.1 NA 4.5 3.1 4.2 NAThrombocytes, 109/liter 205 124 262 NA 217 109 286 NA 183 272 280 NAESR, mm/hour 32 82 45 NA 15 59 26 NA 70 89 80 NACRP, mg/liter �3 41 �3 NA �3 42 �3 NA �3 41 6 NAC3, gm/liter 0.94 1.25 1.07 NA 0.73 1.05 0.94 NA 0.93 1.43 1.15 NAC4, gm/liter 0.10 0.16 0.10 NA 0.15 0.06 0.15 NA 0.17 0.14 0.10 NAC1q, gm/liter NA NA NA NA 0.21 0.24 0.20 NA 0.34 0.22 0.34 NAC3d, gm/liter NA NA NA NA 3.30 9.30 3.40 NA 4.00 7.20 NA NAB cells, 109/liter 0.15 NA NA NA 0.16 NA 0.10 NA 0.32 NA 0 NAHACA response, % of
agarose-boundradioactivity
�1 NA �1 1.16 1.05 1.32 1.73 7.54 �1 �1 �1 9.35
* SAE � serious adverse event; WBCs � white blood cells; NA � not available; ESR � erythrocyte sedimentation rate; CRP � C-reactive protein;HACA � human antichimeric antibodies (values of �1% are negligible).
2746 PIJPE ET AL

served in the remaining 12 patients who did not haveserious clinical side effects.
Two of the 3 patients were treated with methyl-prednisolone (500 mg and 1,000 mg intravenously, re-spectively) and a nonsteroidal antiinflammatory drug(NSAID); the third patient was treated with an NSAIDonly, because her symptoms had begun to resolve spon-taneously. Treatment resulted in complete resolution ofall clinical side effects, and laboratory results returned tonormal (Table 3). It was of interest that HACAs andserum sickness–like symptoms occurred in patients withearly primary SS only, and in none of those withMALT/primary SS.
DISCUSSION
In this phase II study, selective depletion of Bcells led to improvement of subjective and objectiveparameters of disease activity, including salivary andlacrimal gland function, in patients with early primary SSas well as patients with MALT/primary SS with residualgland function. In parallel, B cell depletion occurredquickly and B cells remained undetectable at 12 weeks inall patients except the 2 who received only 2 infusions ofrituximab due to the occurrence of a serious adverseevent. Rituximab, with or without additional chemo-therapy, seems to be effective in the treatment ofMALT-type lymphoma (5). This was confirmed in ourstudy, in which complete remission was achieved in 3 ofthe 7 patients with MALT/primary SS, and diseaseremained stable in 3.
Anti–B cell monoclonal antibody treatment is apromising therapeutic modality in autoimmune disor-ders. Initial data have shown rituximab to be efficaciousand relatively safe in the treatment of systemic diseasessuch as RA, Wegener’s granulomatosis, and SLE (7,9,23).Although SS is considered to be a T cell–mediateddisease, its systemic complications are associated withincreased B cell activity. A positive effect of rituximabon clinical parameters of both SS and MALT-typelymphoma in SS patients has been described in case-reports (24–26), as well as in a report of a case series of4 patients with aggressive lymphoma and SS treated withrituximab combined with chemotherapy (cyclo-phosphamide/doxorubicin/vincristine/prednisone) (27).Recently, Gottenberg et al reported on 6 patients withprimary SS treated with rituximab (23). Extraglandularsymptoms and cryoglobulinemia-related vasculitis re-sponded to rituximab in all but 1 patient, but data on thesubjective and objective parameters of mouth and eye
dryness were not recorded for all patients, so no conclu-sion could be drawn regarding the effect of rituximab onsalivary/lacrimal gland function in the patients in thatstudy.
The objective of this open-label phase II studywas to evaluate the efficacy and safety of rituximab inpatients with primary SS with active disease and shortdisease duration and in patients with primary SS withlocalized MALT-type lymphoma. Since there are novalidated disease activity criteria for SS, active diseasewas arbitrarily defined as the presence of hypergamma-globulinemia (�15 gm/liter), and most components ofthe outcome criteria for clinical trials in SS as proposedby Pillemer et al (28) were used. Both patient groups hadincreased levels of IgM-RF. Levels of circulatingIgM-RF correlate positively with the number of extra-glandular disease manifestations (29). Most myoepithe-lial sialadenitis–associated B cell clones, and subse-quently, lymphomas, express RF (30). Moreover, serioussystemic complications of primary SS, such as vasculitisand nephritis, occur mainly in patients with elevatedIgM-RF levels (29). We observed a slight decrease inIgM-RF levels after treatment in 12 of 15 patients. A risein IgM-RF levels soon after treatment was seen in 2patients with MALT/primary SS, preceding an exacer-bation of their disease (patients 10 and 13; Figure 1).IgM-RF is probably produced by short-lived plasma cellsand might be a good surrogate marker for SS activity(31), e.g., an increase in the IgM-RF level might indicatethe need for retreatment.
In patients with primary SS, progressive reduc-tion of salivary gland function is observed early in thecourse of the disease, with the submandibular andsublingual glands being the first to be affected. This isusually accompanied by a change in the composition ofparotid and submandibular/sublingual saliva (10,14,32).These parameters were the first to improve in ourpatients with early primary SS. Systemic therapy isprobably most beneficial in patients who manifest sub-stantial residual exocrine gland function. This is sup-ported by the finding in this study that patients withlongstanding primary SS (most of those with MALT-type lymphoma), who had no salivary secretion at base-line, did not exhibit any improvement in salivary secre-tion (Figure 2B), while patients with MALT/primary SSwho had some residual salivary gland function did showimprovement.
Analysis of parotid saliva revealed a decrease insodium concentration, indicating normalization of so-dium readsorption by the salivary gland ductal system.
RITUXIMAB IN SS 2747

This was especially prominent in patients with early SS,who had high concentrations of sodium at baseline(Table 2). In healthy subjects, most of the sodium isreabsorbed from primary saliva during its transportthrough the ductal system (15). The increase in salivarysecretion and the normalization of sodium concentra-tion might indicate recovery or regeneration of salivarygland tissue. This regeneration probably occurs only inpatients with residual salivary gland tissue (24). Further-more, high concentrations of salivary sodium are relatedto more severe disease manifestations (33). This high-lights the need for early and aggressive treatment ofprimary SS of short duration, which is often character-ized by residual salivary gland function and high levels ofsalivary sodium. Physical functioning in these patients isfrequently severely impaired, and B cell depletion maylead to improved quality of life as well as preservation oflacrimal and salivary gland function.
An unexpected finding was the high incidence ofserious adverse events in patients with early primary SSwithout MALT-type lymphoma. Three patients devel-oped serum sickness–like symptoms, with HACAs. Only6 cases of serum sickness after rituximab treatment havebeen reported to date in the literature (23,34–36),including 1 case in a patient with primary SS andassociated MALT-type lymphoma (23). Most of thetoxicities associated with rituximab are infusion related,presumably due to cytokine release (37). To our knowl-edge, serum sickness or a similar adverse event has neverbeen reported to occur in association with rituximabtreatment of lymphoma patients without autoimmunedisease. Our patients had a clinical presentation com-patible with serum sickness. An acute-phase responsewas observed in all 3 patients, accompanied by anincrease in the level of C3d, which is indicative ofcomplement consumption, in 2 (Table 3). The presenceof HACAs makes a type III hypersensitivity reactionvery likely. Surprisingly, skin biopsy did not reveal theclassic findings of leukocytoclastic vasculitis (Figure 4B).Recent reports on rituximab treatment of SLE and RAdo not mention similar adverse events (9,38,39). How-ever, patients in the latter studies also received cyclo-phosphamide, methotrexate, or high-dose corticoste-roids, which may account for the lack of these events.
Because prednisone can influence salivary flow inselected patients (40), we decided to use a relatively low,single dose of prednisone as premedication in our study,based on safety data from a large trial of rituximabtreatment in patients with relapses of low-grade lym-phoma (6). In addition to the premedication, 3 of the 7
patients with MALT/primary SS continued to receiveprednisone 7.5–15 mg/day in combination with metho-trexate or azathioprine, which might have contributed tothe lack of serious adverse events in this group.
HACAs have been reported to occur at a higherrate in patients with autoimmune disease than in pa-tients with lymphoma (27% in our study of patients withSS, 4.3% in patients with RA, 35% in SLE patients, and0.6% in patients with lymphoma) (6,9,41). In patientswith RA, SLE, or lymphoma, HACAs have not beenreported to result in clinical manifestations. It seemsthat monoclonal antibodies are more immunogenic inactive autoimmune disease, independent of the type ofdisease. It is not known why HACAs did not lead toinfusion reactions in the RA and SLE patients in theabove studies, but the additional use of immunosuppres-sive medication in those studies might be explanatory.This is supported by the findings of Gottenberg et al(23). Although no information about HACA formationis available in their report, they present data on tolera-bility and short-term efficacy of rituximab in 43 patientswith systemic autoimmune disease, including 6 withprimary SS. Two patients with SLE and 1 patient withprimary SS had serum sickness–like reactions. In total,15 of their 43 patients received rituximab alone, withoutother immunosuppressive agents. Of the 6 patients withprimary SS, all but the 1 who developed a serum sickness–like reaction were receiving concomitant prednisone orother immunosuppressive treatment. This patient had thehighest level of IgM-RF (499 IU/liter) (23).
Steinfeld et al treated 16 patients with primary SSwith infliximab, another chimeric monoclonal antibody(42). Infliximab was well tolerated, and all patientscompleted the study. There were no serious adverseevents. These SS patients also had an increased ESRand/or hypergammaglobulinemia, comparable with ourfindings. Use of DMARDs and corticosteroids was notallowed during the study. No details on development ofHACAs among Steinfeld and colleagues’ patients areavailable, and no serious adverse events were reported.The only difference between their patients and ours,apart from the type of antibody treatment, was theproportion of patients who were positive for IgM-RF(50% in their study versus 100% in ours). Although wecannot exclude a possible role of an intrinsic factorrelated to SS, we hypothesize that the combination ofhigh B cell activity (as reflected by high levels ofIgM-RF) and lack of concomitant immunosuppressivetherapy might be responsible for the development of
2748 PIJPE ET AL

serum–sickness like reactions after treatment with ritux-imab in our SS patients.
In conclusion, the findings of this open-labelphase II study in 15 patients with primary SS suggest thatrituximab is efficacious in the treatment of SS with orwithout MALT-type lymphoma. Early initiation of ther-apy may lead to a decrease in disease activity and mayprevent irreversible chronic damage of the salivaryglands. The occurrence of serum sickness, a previouslyrarely observed side effect of rituximab, in 3 of 8 patientswith early primary SS with high disease activity butwithout MALT-type lymphoma warrants further study.Based on our preliminary results, we would recommendthat concomitant corticosteroid treatment be given at ahigher dosage and/or for a longer period of time in orderto prevent development of serum sickness–like disordersin rituximab-treated patients with SS.
ACKNOWLEDGMENTS
We are grateful to Philip M. Kluin, Jacqueline E. vander Wal, and Caroline Roozendaal for their support andmeaningful discussions.
REFERENCES
1. Voulgarelis M, Dafni UG, Isenberg DA, Moutsopoulos HM, andthe Members of the European Concerted Action on Sjogren’ssyndrome. Malignant lymphoma in primary Sjogren’s syndrome: amulticenter, retrospective, clinical study by the European Con-certed Action on Sjogren’s Syndrome. Arthritis Rheum 1999;42:1765–72.
2. Jonsson R, Haga HJ, Gordon TP. Current concepts on diagnosis,autoantibodies and therapy in Sjogren’s syndrome. Scand J Rheu-matol 2000;29:341–8.
3. Van der Reijden WA, Vissink A, Veerman EC, Nieuw Amer-ongen AV. Treatment of oral dryness related complaints (xe-rostomia) in Sjogren’s syndrome. Ann Rheum Dis 1999;58:465–74.
4. Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, BouabdallahR, et al. CHOP chemotherapy plus rituximab compared withCHOP alone in elderly patients with diffuse large-B-cell lym-phoma. N Engl J Med 2002;346:235–42.
5. Conconi A, Martinelli G, Thieblemont C, Ferreri AJ, Devizzi L,Peccatori F, et al. Clinical activity of rituximab in extranodalmarginal zone B-cell lymphoma of MALT type. Blood 2003;102:2741–5.
6. McLaughlin P, Grillo-Lopez AJ, Link BK, Levy R, Czuczman MS,Williams ME, et al. Rituximab chimeric anti-CD20 monoclonalantibody therapy for relapsed indolent lymphoma: half of patientsrespond to a four-dose treatment program. J Clin Oncol 1998;16:2825–33.
7. Silverman GJ, Weisman S. Rituximab therapy and autoimmunedisorders: prospects for anti–B cell therapy [review]. ArthritisRheum 2003;48:1484–92.
8. Virgolini L, Marzocchi V. Rituximab in autoimmune diseases.Biomed Pharmacother 2004;58:299–309.
9. Edwards JC, Szczepanski L, Szechinski J, Filipowicz-Sosnowska A,
Emery P, Close DR, et al. Efficacy of B-cell-targeted therapy withrituximab in patients with rheumatoid arthritis. N Engl J Med2004;350:2572–81.
10. Pijpe J, Kalk WW, Vissink A. Clinical and immunological factorsassociated with low lacrimal and salivary flow rate in patients withprimary Sjogren’s syndrome. J Rheumatol 2003;30:206–7.
11. Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alex-ander EL, Carsons SE, et al. Classification criteria for Sjogren’ssyndrome: a revised version of the European criteria proposed bythe American-European Consensus Group. Ann Rheum Dis2002;61:554–8.
12. Maloney DG, Grillo-Lopez AJ, White CA, Bodkin D, Schilder RJ,Neidhart JA, et al. IDEC-C2B8 (rituximab) anti-CD20 monoclo-nal antibody therapy in patients with relapsed low-grade non-Hodgkin’s lymphoma. Blood 1997;90:2188–95.
13. Aalberse RC, Dieges PH, Knul-Bretovla V, Vooren P, Aalbers M,van Leeuwen J. IgG4 as a blocking antibody. In: Halpern GM,editor. Clinical reviews in allergy. vol. I. New York: ElsevierBiomedical; 1983. p. 289–302.
14. Kalk WW, Vissink A, Stegenga B, Bootsma H, Nieuw AmerongenAV, Kallenberg CG. Sialometry and sialochemistry: a non-invasiveapproach for diagnosing Sjogren’s syndrome. Ann Rheum Dis2002;61:137–44.
15. Mandel ID, Baurmash H. Sialochemistry in Sjogren’s syndrome.Oral Surg Oral Med Oral Pathol 1976;41:182–7.
16. Bijsterveld O. Diagnostic tests in the Sicca syndrome. ArchOphthalmol 1969;82:10–4.
17. Kalk WW, Mansour K, Vissink A, Spijkervet FK, Bootsma H,Kallenberg CG, et al. Oral and ocular manifestations in Sjogren’ssyndrome. J Rheumatol 2002;29:924–30.
18. Smets EM, Garssen B, Bonke B, de Haes JC. The multidimen-sional fatigue inventory (MFI) psychometric qualities of an instru-ment to assess fatigue. J Psychosom Res 1995;39:315–25.
19. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form healthsurvey (SF-36). I. Conceptual framework and item selection. MedCare 1992;30:473–83.
20. Barendregt PJ, Visser MR, Smets EM, Tulen JH, van denMeiracker AH, Boomsma F, et al. Fatigue in primary Sjogren’ssyndrome. Ann Rheum Dis 1998;57:291–5.
21. Strombeck B, Ekdahl C, Manthorpe R, Wikstrom I, Jacobsson L.Health-related quality of life in primary Sjogren’s syndrome,rheumatoid arthritis and fibromyalgia compared to normal popu-lation data using SF-36. Scand J Rheumatol 2000;29:20–8.
22. Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI,Connors JM, et al, and the NCI Sponsored International WorkingGroup. Report of an international workshop to standardize re-sponse criteria for non-Hodgkin’s lymphomas. J Clin Oncol 1999;17:1244–53.
23. Gottenberg J, Guillevin L, Lambotte O, Combe B, Allanore Y,Cantagrel A, et al. Tolerance and short-term efficacy of rituximabin 43 patients with systemic autoimmune diseases. Ann Rheum Dis2005;64:913–20.
24. Pijpe J, van Imhoff GW, Vissink A, van der Wal JE, Kluin PM,Spijkervet FK, et al. Changes in salivary gland immunohistologyand function after rituximab mono-therapy in a patient withSjogren’s syndrome and associated MALT-lymphoma. AnnRheum Dis 2005;64:958–60.
25. Shih WJ, Ghesani N, Hongming Z, Alavi A, Schusper S, Mozley D.F-18 FDG positron emission tomography demonstrates resolutionof non- Hodgkin’s lymphoma of the parotid gland in a patient withSjogren’s syndrome: before and after anti-CD20 antibody ritux-imab therapy. Clin Nucl Med 2002;27:142–3.
26. Somer BG, Tsai DE, Downs L, Weinstein B, Schuster SJ. Improve-ment in Sjogren’s syndrome following therapy with rituximab formarginal zone lymphoma. Arthritis Rheum 2003;49:394–8.
27. Voulgarelis M, Giannouli S, Anagnostou D, Tzioufas AG. Com-
RITUXIMAB IN SS 2749

bined therapy with rituximab plus cyclophosphamide/doxorubicin/vincristine/prednisone (CHOP) for Sjogren’s syndrome-associatedB-cell aggressive non-Hodgkin’s lymphomas. Rheumatology (Ox-ford) 2004;43:1050–3.
28. Pillemer SR, Smith J, Fox PC, Bowman SJ. Outcome measures forSjogren’s syndrome, April 10-11, 2003, Bethesda, Maryland, USA.J Rheumatol 2005;32:143–9.
29. Oxholm P. Primary Sjogren’s syndrome: clinical and laboratorymarkers of disease activity. Semin Arthritis Rheum 1992;2:114–26.
30. Martin T, Weber JC, Levallois H, Labouret N, Soley A, Koenig S,et al. Salivary gland lymphomas in patients with Sjogren’s syn-drome may frequently develop from rheumatoid factor B cells.Arthritis Rheum 2000;43:908–16.
31. Dorner T, Egerer K, Feist E, Burmester GR. Rheumatoid factorrevisited. Curr Opin Rheumatol 2004;16:246–53.
32. Vissink A, Panders AK, Nauta JM, Ligeon EE, Nikkels PG,Kallenberg CG. Applicability of saliva as a diagnostic fluid inSjogren’s syndrome. Ann N Y Acad Sci 1993;694:325–9.
33. Pederson AM, Reibel J, Nordgarden H, Bergem HO, Jensen JL,Nauntofte B. Primary Sjogren’s syndrome: salivary gland functionand clinical oral findings. Oral Dis 1999;5:128–38.
34. D’Arcy CA, Mannik M. Serum sickness secondary to treatmentwith the murine–human chimeric antibody IDEC-C2B8 (ritux-imab). Arthritis Rheum 2003;44:1717–8.
35. Hellerstedt B, Ahmed A. Delayed-type hypersensitivity reaction
or serum sickness after rituximab treatment [letter]. Ann Oncol2003;14:1792.
36. Herishanu Y. Rituximab-induced serum sickness [letter]. Am JHematol 2002;70:329.
37. Winkler U, Jensen M, Manzke O, Schulz H, Diehl V, Engert A.Cytokine-release syndrome in patients with B-cell chronic lympho-cytic leukemia and high lymphocyte counts after treatment with ananti-CD20 monoclonal antibody (rituximab, IDEC-C2B8). Blood1999;94:2217–24.
38. Leandro MJ, Edwards JC, Cambridge G, Ehrenstein MR, Isen-berg DA. An open study of B lymphocyte depletion in systemiclupus erythematosus. Arthritis Rheum 2002;46:2673–7.
39. Leandro MJ, Edwards JC, Cambridge G. Clinical outcome in 22patients with rheumatoid arthritis treated with B lymphocytedepletion. Ann Rheum Dis 2002;61:883–8.
40. Fox PC, Datiles M, Atkinson JC, Macynski AA, Scott J, FletcherD, et al. Prednisone and piroxicam for treatment of primarySjogren’s syndrome. Clin Exp Rheumatol 1993;11:149–56.
41. Looney RJ, Anolik JH, Campbell D, Felgar RE, Young F, ArendLJ, et al. B cell depletion as a novel treatment for systemic lupuserythematosus: a phase I/II dose-escalation trial of rituximab.Arthritis Rheum 2004;50:2580–9.
42. Steinfeld SD, Demols P, Salmon I, Kiss R, Appelboom T. Inflix-imab in patients with primary Sjogren’s syndrome: a pilot study.Arthritis Rheum 2001;44:2371–5.
2750 PIJPE ET AL