Physiotherapy management for rheumatoid arthritis
28
Senthilkumar Thiyagaran, M.P.T(ortho) Physiotherapist Rheumatoid Arthritis Physiotherapy management
-
Upload
senphysio -
Category
Health & Medicine
-
view
183 -
download
1
Transcript of Physiotherapy management for rheumatoid arthritis

Senthilkumar Thiyagaran, M.P.T(ortho)
Physiotherapist
Rheumatoid Arthritis
Physiotherapy management

Objectives To know about definition, causes, pathology
and clinical features
To know about pathomechanics of RA
To know about the medical management
To know about the physiotherapist role in RA
management

Definition
RA /rheumatic disease
It’s a autoimmune disease
Chronic inflammatory disease
Crippling and disabling disorder which
affects connective tissues in the whole
body

Incidence
More commonly affects women
Ratio 2:1
In the world population 1% to 2%
affected
Age – 16 years and above

Pathology
Uncontrolled
inflammation
Exuberant proliferatio
n of synovium
PannusFormation Consequent
bone and cartilage
destruction
Involvment of tendons,
ligaments, blood vessels

Clinical manifestations
Stiffness
Tenderness
Pain on motion
Swelling
Deformity
Limitation of motion
Extra-articular manifestations
Rheumatoid nodules

American College of Rheumatology uses this list of
criteria:
1. Morning stiffness in and around the joints for at least one hour.
2. Swelling or fluid around three or more joints simultaneously.
3. At least one swollen area in the wrist, hand, or finger joints.
4. Arthritis involving the same joint on both sides of the body (symmetric arthritis).
5. Rheumatoid nodules, which are firm lumps in the skin of people with rheumatoid arthritis. These nodules are usually in pressure points of the body, most commonly the elbows.
6. Abnormal amounts of rheumatoid factor in the blood.
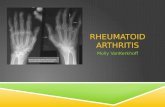
7. X-ray changes in the hands and wrists typical of rheumatoid arthritis, with destruction of bone around the involved joints. However, these changes are typical of later-stage disease.

PATHOMECHANICS Genu valgum, hallux valgus, pronationof the foot, depression of the metatarsal heads, hammer or claw toes, and tendocalcaneal bursitis or subplantar spur formation.
decreased velocity, cadence, and stride length; poor heel-toe pattern; and abnormal patterns of weight bearing.
Gait deviations

Conservative managment
NonSteroidal Anti-Inflammatory Drugs
(NSAIDs),
Disease-Modifying Antirheumatic Drugs
(DMARDs),
Immunosuppressants, and
Corticosteroids.

Surgical management
• Persistent pain (from, for example, joint damage or
other soft tissue cause).
• Worsening joint function.
• Progressive deformity.
• Persistent localised synovitis.
Deformity becomes irreversible:
• Imminent or actual tendon rupture.
• Nerve entrapment (for example, carpal tunnel
syndrome).
• Any stress fracture.

Physical therapy Management

Assessment/ Evaluation
Assessment of posture
Testing muscle strength and power
Measuring joint movement
Gait analysis
Functional test
such as balance, walking, dressing, toileting(ADL),
etc..

Treatment Goals To protect the joint from further damages
Provide pain relief
Prevent deformity
Prevent disabilities
Increase functional capacity
Improve flexbility and strength
Encourage regular exercise
Improve general fitnes

Management
Cold therapy in acute phases
Dosage
10 – 20 min/ 1-2 times a day

Heat Therapy (chronic phases)
Dosage
20 – 30 mins 1 to 2 times a
day

TENS
Short term pain relief (6 to 18
hours)

Exercise for Acute phase
Performed at least once a day
Gentle assisted movement through normal range
(joint Mobilisation)
Isometric “ static muscle contraction” helps to
maintain muscle tone without increasing
inflammation


Exercises for the Chronic Phase
Can progress the above exercises to include use
of light resistance
Postural / core stability exercises
Swimming / walking / cycling to maintain
cardiovascular fitness
Gentle stretches for areas that become tight,
such as knees & calves


Regular Exercises
Maintaining muscle strength is important for joint
stability & preventing injury
Muscles can become weak following reduced
activity
Pain signals from your nerves and swelling can
both inhibit muscles
Muscle length can be affected by prolonged
positions & immobilization and tightness can limit
daily activities

General Body Stretching

Joint Protection
Try to avoid prolonged positions
Balance activity with rest periods rest should
come before you get fatigued or sore
Look at your work or home desk set up
During the acute phase activities such as stair
climbing can put stress through your knees
ankles & hips try to keep the number of trips up &
down to a minimum

Common deformities


ALTERNATIVE THERAPIES
THI CHI
MUSCIAL THERAPY
YOGA THERAPY
RELAXATION TECHNIQUES
PILATES

References
http://ptjournal.apta.org/content/62/8/1148.abstrac
t
http://www.webmd.com/rheumatoid-
arthritis/guide/diagnosing-ra
http://rawarrior.com/new-criteria-for-rheumatoid-
arthritis/
http://emedicine.medscape.com/article/331715-
overview#aw2aab6b2b3

http://www.patient.co.uk/doctor/management-of-
rheumatoid-arthritis
http://morphopedics.wikidot.com/physical-
therapy-management-of-rheumatoid-arthritis