OLADELE SIMEON OLATUNYA - Unicamprepositorio.unicamp.br/.../1/Olatunya_OladeleSimeon_D.pdf ·...
209
UNIVERSIDADE ESTADUAL DE CAMPINAS FACULDADE DE CIÊNCIAS MÉDICAS OLADELE SIMEON OLATUNYA ASSOCIATION BETWEEN HEMOLYSIS INTENSITY, GENETIC MARKERS AND CLINICAL EVOLUTION IN PATIENTS WITH SICKLE CELL DISEASE ASSOCIAÇÃO ENTRE A INTENSIDADE DA HEMÓLISE, MARCADORES GENETICOS E EVOLUÇÃO CLÍNICA EM PACIENTES COM DOENÇA FALCIFORME CAMPINAS 2018
Transcript of OLADELE SIMEON OLATUNYA - Unicamprepositorio.unicamp.br/.../1/Olatunya_OladeleSimeon_D.pdf ·...

UNIVERSIDADE ESTADUAL DE CAMPINAS
FACULDADE DE CIÊNCIAS MÉDICAS
OLADELE SIMEON OLATUNYA
ASSOCIATION BETWEEN HEMOLYSIS INTENSITY, GENETIC MARKERS
AND CLINICAL EVOLUTION IN PATIENTS WITH SICKLE CELL DISEASE
ASSOCIAÇÃO ENTRE A INTENSIDADE DA HEMÓLISE, MARCADORES
GENETICOS E EVOLUÇÃO CLÍNICA EM PACIENTES COM DOENÇA
FALCIFORME
CAMPINAS
2018

OLADELE SIMEON OLATUNYA
ASSOCIATION BETWEEN HEMOLYSIS INTENSITY, GENETIC MARKERS
AND CLINICAL EVOLUTION IN PATIENTS WITH SICKLE CELL DISEASE
ASSOCIAÇÃO ENTRE A INTENSIDADE DA HEMÓLISE, MARCADORES
GENETICOS E EVOLUÇÃO CLÍNICA EM PACIENTES COM DOENÇA
FALCIFORME
Thesis presented to the Faculty of Medical sciences of the University of Campinas in part-fulfilment of the requirement for the award of doctor in medical sciences, with area of concentration in clinical pathology.
Tese apresentada à Faculdade de Ciências Médicas da
Universidade Estadual de Campinas como parte dos
requisitos exigidos para a obtenção do título de doutor em
Ciências Médicas, área de concentração em Patologia
Clínica.
ORIENTADOR: PROF. DR. FERNANDO FERREIRA COSTA
ESTE EXEMPLAR CORRESPONDE À VERSÃO FINAL DA TESE DEFENDIDA PELO ALUNO OLADELE SIMEON OLATUNYA, E ORIENTADO PELO PROF. DR. FERNANDO FERREIRA COSTA
CAMPINAS
2018

FICHA CATALOGRÁFRICA:

BANCA EXAMINADORA DA DEFESA DE DOUTORADO
OLADELE SIMEON OLATUNYA
ORIENTADOR: PROF. DR. FERNANDO FERREIRA COSTA
MEMBROS:
1. PROF. DR. FERNANDO FERREIRA COSTA
2. PROFA. DRA. MARIA STELLA FIGUEIREDO
3. PROFA. DRA. SANDRA FATIMA MENOSI GUALANDRO
4. PROF. DR. ANDRE FATTORI
5. PROFA. DRA. MARINA PEREIRA COLELLA
Programa de Pós-Graduação em [PROGRAMA] da Faculdade de Ciências
Médicas da Universidade Estadual de Campinas.
A ata de defesa com as respectivas assinaturas dos membros da banca
examinadora encontra-se no processo de vida acadêmica do aluno.
Data: 16/01/2018

DEDICATION
This work is dedicated to Almighty God, the Alpha and Omega, beginning and the end,
who gave me the opportunity to start this research and to complete it, may His name be
praised forever.

ACKNOWLEDGEMENTS
My profound gratitude goes to the Almighty God for His sustaining grace,
protection, wisdom, good health and provision throughout the research work. My
undiluted gratitude goes to my amiable supervisor, Professor Fernando Ferreira Costa,
for his mentorship, guidance and supervision during the research work. Your simplicity
and hardwork have impacted me greatly. I am indeed very grateful sir.
I appreciate Drs Dulcinéia Martins de Albuquerque, Carolina Lanaro, Carla
Penteado, Ana Leda Longhini, Irene Santos and Flavia Leonardo Costa for their
inestimable supports during the research. God will continue to lift you up. My sincere
appreciations also go to Ana Luisa de Lorenzo for providing me with very huge and
inestimable administrative and secretariat supports. God bless you richly. To Daniela
Pinheiro, and my students` colleagues who assisted me in times of need, i say a big
thank you. My thanks to all the laboratory staffs at the Hemocentro (Unicamp), and a
host of others who has contributed to the success of this work. I also wish to appreciate
Prof (Mrs) Adeyinka Falusi, Mr Abayomi Odetunde, Mr Kayode Tolorunju Segun and
Mrs Benson Tolulope for providing laboratory supports for some analysis in Nigeria. I
also wish to greatly thank Drs Taiwo Adekunle, Faboya Ayodeji and Ajibola Ayo for
their great contributions. God bless you all.
My special appreciation to the sickle cell support society of Nigeria (SCSSN) for
nominating me for the programme that allowed me to undertake this study. I also wish to
specially appreciate Professor Adekunle Adekile for his mentorships, encouragements
and supports. God bless you sir. Also, my deep appreciations go to Professor Marilda of
FLOCRUZ foundation Bahia for her supports. I wish to specially thank my teachers at
the Ekiti State University for their inestimable roles at seeing me through this programme.

I need to make special mention of the vice chancellor of the Ekiti State University for
approving my study leave. Also, i greatly appreciate Professors GJF Esan, MA Araoye,
KS Oluwadiya, and OAO Oyelami for their timely supports, encouragements and strongly
recommending me for this programme. God bless you richly sirs!
To my father, His Highness Ojo James Olatunya, the Obalese of Oye Ekiti, who
has longed so much to see me complete this research and my wonderful ever supporting
mother Chief Mrs Margaret Modupe Olatunya, i say thank you so much i`m eternally
grateful to you both.
This section will not be complete if i fail to mention the supports of my friend,
my companion and God given wife, Dr Mrs Mercy Ayomadewa Olatunya for her
financial, moral, spiritual and academic supports. My love, you are wonderful! I pray
that God will protect us and help us to reap the fruits of our labour (Amen). Also, i want
to say a big thank you to our children Tijesunimi, Jesutimilehin, and Jesudarasimi who
were always praying and longing for me to complete this research work. I pray that
God will spare your lives and make you great in life in Jesus name. Amen.

RESUMO
Diversas hipóteses têm sido propostas para explicar a diversidade clínica da doença
falciforme (DF). Estas incluem a classificação de um sub-fenótipo hemolítico e sugerem
a potencial contribuição de marcadores genéticos. No entanto, estes não são explicam
totalmente as expressões fenotípicas observadas nos pacientes com DF, assim, há a
necessidade de buscar por mais marcadores candidatos para a DF. Este é um estudo de
correlação fenotípica com alguns marcadores hemolíticos conhecidos e desconhecidos
dentre os pacientes com DF. Este estudo avaliou a relação entre micropartículas
eritrocitárias e outros marcadores tradicionais de hemólise com os fenótipos clínicos de
138 brasileiros com DF, após consentimento, sendo 78 HbSS (63 em uso de hidroxiureia,
15 sem o uso da medicação), 12 HbS-Beta0 talassemia, 12 HbS-Beta+ talassemia e 36
HbSC sem uso de hidroxiurea e em estado estacionário da doença. Ainda, 110 crianças
nigerianas com DF, sendo 102 HbSS e 8 HbSC, foram avaliadas. Um total de 107
indivíduos, 39 do Brasil e 68 da Nigéria, fizeram parte do grupo controle. As
micropartículas eritrocitárias foram quantificadas em plasma por citometria de fluxo,
haptoglobina e hemopexina foram avaliadas por ELISA, e a hemoglobina plasmática e o
heme foram mensurados por ensaio colorimétrico. PCR foi utilizada para confirmar o
diagnóstico de DF. O perfil para alfa talassemia foi determinado por GAP-PCR multiplex,
os genótipos para UGT1A1 foram analisados por meio dos fragmentos gerados, e os
haplótipos βS e a deficiência de G6PD por meio de ensaio TaqMan. Os pacientes
apresentaram níveis elevados de micropartículas, hemoglobina plasmática e heme livre
na seguinte ordem: HbSS > HbSC > HbAA. Por outro lado, haptoglobina e hemopexina
estiveram mais elevadas no grupo controle: HbSS<HbSC<HbAA. As micropartículas
eritrocitárias mostraram correlações significantes com os marcadores tradicionais de
hemólise. Não foram observadas diferenças significantes nos níveis de micropartículas,

heme e hemoglobina plasmática entre os indivíduos HbSS tratados e não tratados com
hidroxiureia. Tanto as micropartículas quanto o heme estiveram associados com a
ocorrência de úlcera de perna e o risco para hipertensão pulmonar determinado pela
velocidade de regurgitação da tricúspide (TRV). Além disso, este estudo mostrou que a
coexistência de alfa talassemia foi significantemente associada com melhores índices
hematológicos, aumento de crises de dor óssea e proteção contra úlcera de perna. O
polimorfismo UGT1A1 foi significantemente associado com níveis mais altos de
bilirrubina e ocorrência de cálculo biliar dentre os pacientes nigerianos. Da deficiência de
G6PD nao foi associada com os eventos clinicos. Os SNPs do gene BCL11A
influenciaram significantemente os níveis de hemoglobina fetal desses pacientes e seus
haplótipos βS foram principalmente a homozigose do tipo Benin/Benin. Em conclusão,
este estudo mostrou que a alfa talassemia, e o polimorfismo UGT1A1 afetam os eventos
clínicos das crianças nigerianas com DF. Além disso, estabeleceu que as micropartículas
eritrocitárias são associadas com a hemólise e os eventos clínicos em brasileiros com DF.
Ambos RMP e heme foram associados com úlcera de perna e TRV (risco para hipertensão
pulmonar) elevado. Ainda, o heme esteve associado com microalbuminúria. Essas
observações sugerem que as micropartículas e o heme podem desempenhar importantes
papeis na fisiopatologia e nas manifestações clínicas da DF. Assim, RMP e heme como
alvo de terapias podem ser uma nova estratégia para tratar a DF.
Palavras chaves: doença falciforme, manifestações clínicas, hemólise, micropartículas
eritrocitárias, marcadores genéticos.

ABSTRACT
Several hypotheses have been proposed for the clinical diversity in SCD. These include
the classification of a sub-hemolytic phenotype and hints on the potential contributions
of genetic markers. However, these do not fully explain the phenotypic expressions
observed in SCD patients. Hence, the need to search for more candidate markers of SCD.
This is a study on phenotype correlation with some known genetic and newer candidate
hemolysis markers among SCD patients. This study evaluated the relationship between
red blood cell microparticles and other traditional markers of hemolysis in relation to
clinical phenotypes of 138 consenting adult Brazilians with SCD made up of 78 HbSS
(63-hydroxyurea treated &15-hydroxyurea naïve), 12 S-Beta0 thalassemia, 12 S-Beta+
thalassemia and 36 HbSC hydroxyurea naive patients in steady state. Also, 110 Nigerian
children with SCD made up of 102 SS and 8 HbSC were studied. A total of 107
individuals, 39 from Brazil and 68 from Nigeria, served as controls. The plasma red blood
cell microparticles were quantified by flow cytometer, haptoglobin and hemopexin by
ELISA, plasma hemoglobin and heme were measured by colorimetric assays. PCR was
used to confirm the diagnosis of SCD. Alpha thalassemia status was determined by
multiplex GAP-PCR, UGT1A1 genotypes by Fragment analysis, βS haplotype and G6PD
by TaqMan SNP genotyping assays. The patients had significant higher levels of red
blood microparticles, plasma hemoglobin, heme in the following order HbSS > HbSC >
HbAA. On the contrary, both haptoglobin and hemopexin were higher in controls than
the patients in the following reverse order HbSS<HbSC<HbAA.
Red blood cell microparticles showed significant correlations with traditional markers of
hemolysis. There were no significant differences in the red blood cell microparticles,
heme and plasma hemoglobin levels of hydroxyurea treated SS patients compared to
untreated patients. Both red blood cell microparticles and heme were associated with leg

ulcer and elevated trancuspid regurgitation velocity (TRV)-risk for pulmonary
hypertension. Also, this study established that coexistence of alpha thalassemia was
significantly associated with better hematologic indices, increased bone pain crisis and
protection against leg ulcer. The UGT1A1 polymorphism was significantly associated
with higher bilirubin levels and occurrence of gallstone among the Nigerian patients.
Similarly, G6PD deficiency was not associated with clinical events. The SNPs of the
BCL11A significantly influenced the fetal hemoglobin levels of the Nigerian patients and
their βS haplotypes were mainly of the homozygous Benin/Benin type. In conclusion,
this study established that alpha thalassemia, and UGT1A1 polymorphisms affect the
clinical events among Nigerian SCD children. It also established that the red blood cell
microparticles are associated with hemolysis and clinical events among Brazilian SCD
patients. Both RMP and heme were associated with leg ulceration and elevated TRV (risk
for pulmonary hypertension). Also, heme was associated with microabuminuria. These
observations suggest that red blood cell microparticle and heme may have important roles
in the pathophysiology and clinical manifestations of SCD. Hence, therapies targeting
RMP and heme could be another strategy to combat SCD.
Keywords: Sickle cell disease, Clinical manifestations, Hemolysis, Red blood cells
microparticles, Genetic Markers.

LIST OF ABBREVIATIONS
SCD – Sickle cell disease
SCA – Sickle cell anaemia
RBC – Red blood cells
WBC – White blood cells
RMP – Red blood cell microparticles
TRV – Trancuspid regurgitation velocity
UACR – Urinary albumin creatinine ratio
VOC – Vaso occlusive crisis
ACS – Acute chest syndrome
NO – Nitric oxide
TLR4 – Toll-like receptor 4
DAMPs – Damage associated molecular pattern molecules
LDH – Lactate dehydrogenase
MCV – Mean corpuscular volume
HU – Hydroxyurea
HbF – Fetal haemoglobin
SNP – Single nucleotide polymorphism
Hp - Haptoglobin
HPX – Hemopexin
Plasma Hb- Plasma Hemoglobin
G6PD – Glucose 6 phosphate dehydrogenase
UGT1A1- Uridine diphosphate glucuronosyl transferase 1A

LIST OF TABLES
Table 1: Summary of parameters among hemolysis study cohorts
Table 2: Effects of hydroxyurea treatment on biologic markers of HbSS patients
Table 3: Effects of hydroxyurea treatment on biologic markers of HbS-β thalassemia patients
Table 4: Associations between acute chest syndrome and biologic markers
Table 5: Associations between acute bone pain crisis (VOC) and biologic markers
Table 6: Associations between leg ulcer and biologic markers
Table 7: Associations between elevated tricuspid regurgitation velocity/risk for
pulmonary hypertension and biologic markers
Table 8: Associations between stroke and biologic markers
Table 9: Associations between sickle cell retinopathy and biologic markers
Table 10: Associations between osteonecrosis and biologic markers
Table 11: Associations between priapism and biologic markers
Table 12: Associations between microalbuminuria and biologic markers
Table 13: Distribution of βs-haplotypes and G6PD deficiency among Nigerian cohorts
Table 14 : Associations between G6PD deficiency and biologic markers of Nigerian SS
cohorts
Table 15: Co-inheritance of sickle cell anemia with G6PD deficiency and clinical events
Table 16: Allele and genotype frequencies of UGT1A1 promoter polymorphism among
participants
Table 17: Comparison of laboratory markers between patients and controls UGT1A1
study cohort
Table 18: Influence of UGT1A1 genotype on laboratory parameters of SS cohort
Table 19: Influence of UGT1A1 genotype on clinical events of SS patients
Table 20: Comparison of parameters in patients with and without gallstones
Table 21: Biodata and frequencies of alpha thalassemia alleles
Table 22: Laboratory parameters of patients and controls of the thalassemia study cohort
Table 23: Alpha thalassemia Alleles and laboratory parameters
Table 24: Co-inheritance of sickle cell anemia with Alpha Thalassemia and clinical events
Table 25: Comparison of parameters in patients with or without leg ulcer in the absence
of Alpha thalassemia

Table 26: Associations between Haptoglobin genotypes and biologic markers of SS cohorts
Table 27: Influence of Haptoglobin genotype on clinical events of SS cohorts
Table28: Table of BCL11A SNPs examined
Table 29: Descriptive statistics and comparisons of BCL11A SNPs between the patients and controls
Table 30: Measures of fetal hemoglobin by allele combination and comparison in Patients group
Table 31: Measures of fetal hemoglobin by allele combination and regression analysis.
Table 32: Linkage disequilibrium between the SNPs pairs.

LIST OF FIGURES
Figure 1: Pathophysiology of sickle cell disease
Figure 2: Sickle cell disease and hemolysis products
Figure 3: The βs-haplotypes
Figure 4: Comparison of red blood cell microparticles across groups
Figure 5: Comparison of plasma hemoglobin across groups
Figure 6: Comparison of heme across groups
Figure 7: Comparison of haptoglobin across groups
Figure 8: Comparison of hemopexin across groups
Figure 9: Comparison of LDH across groups
Figure 10: Comparison of total serum bilirubin across groups
Figure 11: Comparison of unconjugated bilirubin across groups
Figure 12: Comparison of reticulocyte count across groups
Figure 13: Comparison of RBC concentration across groups
Figure 14: Comparison of haemoglobin concentration across groups
Figure 15: Comparison of fetal hemoglobin across groups
Figure 16: Red blood cell correlation plots
Figure 17: Glucose 6 phosphate dehydrogenase agarose gel by restriction analysis
Figure 18: UGT1A1 promoter genotypes found among Nigerian groups
Figure 19: Agarose gel analysis showing α 3.7 deletion by PCR.
Figure 20: Illustration of modeled Red blood cells microparticles in the lumen and endothelial regions of blood vessels
Figiure 21: Illustration of the predictive value of tricuspid regurgitant velocity on functional outcomes and mortality risk in sickle cell disease
Figure 22: Mechanisms of hemolytic anemia in reducing NO bioavailability and association with vasculopathic sub-phenotypes of sickle cell disease

TABLE OF CONTENTS
PAGE
Introduction…………………………………………………………………...17 – 28
Justification……………………………………………………………………29
Objectives……………………………………………………………………..30
Patients and methods………………………………………………………….32 – 44
Results…………………………………………………………………………45 – 101
Discussion……………………………………………………………………..102 – 118
Conclusions……………………………………………………………………119 – 120
References…………………………………….……………………………….121 – 133
Appendices………………………………………………………………… 134 – 201
Annexes……………………………………………………………………. 202 - 209

17
1. INTRODUCTION
Sickle cell disease (SCD) is a common genetic disorder of man that is caused by
a mutation in the β-globin gene1,2. SCD is a disorder of public health importance,
especially in sub-Saharan Africa where the largest burden of the disease exists with about
6 million people affected. Nigeria is the country with the highest burden of the disease
where approximately 2 to 3% of all newborns are born with the disorder3. Due to slave
trade and people migration, the disease has spread from Africa to the other parts of the
world. In Brazil, the prevalence of SCD varies between 0.8 and 60 per 100,000 live births
in different regions of the country and most of those affected are Brazilians of African
descent4,5.
Pathophysiologic basis of SCD
The proximate cause of SCD is a single gene mutation resulting in a single base
change from adenine to thymine (GAG to GTG) in the codon for amino acid. This
mutation results in the replacement of the hydrophilic glutamate by hydrophobic valine
at the sixth amino acid residue of the β-globin polypeptide chain and HbS (Hemoglobin
S) β-globin chain substitute for normal HbA β-globin chain. The HbS can undergo
reversible polymerization when deoxygenated. However, following repeated sickling and
un-sickling cycles, the HbS becomes irreversibly polymerized and injures the RBC (Red
blood cell) by causing irreversible damage to the RBC membrane. The damaged RBCs
have a shortened life span and are removed thus forming the basis for chronic anemia in
SCD. The intravascular component of hemolysis depletes nitric oxide thereby causing
disruption in its balance and this leads to some vascular complications. In addition, other
complex interactions with endothelial cells and some molecules lead to cellular injuries,
inflammation, and other cascades of downstream events.and injuries seen in SCD1,2.
Some aspects of the pathophysiology and complicating events are summarized in Figure
1 below.

18
Figure 1: The Glu6Val mutation leads to HbS formation which polymerises at low O2
tension causing damage to RBC membrane, ↓RBC life span, Hemolysis, NO depletion,
and vasoocclusion. Steinberg MH, 2008. The Scientific World Journal2
Studies have shown that SCD is clinically pleiotropic both within an individual
and among groups of patients. The clinical spectrum ranges from asymptomatic or mild
course to persistent, severe or life-threatening situations often requiring frequent hospital
visits and admissions1,2. These inter- and intra-patient variability and unpredictable
phenotypic expression pose significant management challenges to physicians and
caregivers1,4.
Several hypotheses have been proposed for the phenotypic diversity in SCD with
environmental influences as well as sociodemographic characteristics playing major roles
in tropical Africa2,3,6. Others have attributed the clinical variability to the roles of some
genetic modifiers such as the presence of α-thalassemia, and Glucose 6 phosphatase
dehydrogenase deficiency (G6PD). Also, fetal hemoglobin production which is thought
to be influenced by β-globin gene haplotype and some other factors, has been
implicated6,7,8. In addition, other non-globin genetic factors like the uridine diphosphate
glucuronosyl transferase 1A (UGT1A1) promoter polymorphism has also been found to

19
modify the clinical course of SCD7. However, these factors do not fully explain the
phenotypic diversity observed in SCD patients. Hence, researchers continue to search for
more markers of the SCD clinical expression8,9. Studies on markers of hemolysis such as
reticulocyte count, lactate dehydrogenase, aspartate transaminase, serum bilirubin, heme,
haptoglobin, hemopexin, cell-free plasma haemoglobin and red blood cell micro particles,
have shown some promise in elucidating the clinical course of SCD9-11. Hemolysis,
though considered traditionally as the cause of anemia and gallstone formation in SCD,
has now been shown to cause more than these complications in SCD. Some
pathophysiological processes, such as, endothelial dysfunction, chronic inflammation and
vascular injury have been linked to hemolysis via the release of cell free plasma
haemoglobin, heme, and other toxic products during hemolysis. This leads to a cascade
of downstream events and complications in SCD patients12-15. Due to the damages and
injuries caused by these products of hemolysis, circulating cell free haemoglobin and
heme are now being referred to as erythrocytic damage associated molecules
(eDAMPS)12,15. This is further explained and simplified in figure 2 below. As shown, in
the figure, although the human body has innate mechanisms to neutralise products of
intravascular hemolysis, these endogenous mechanisms are often overwhelm in SCD
patients thus leading to circulating eDAMPS12,15.
Figure 2: Hemolysis releases erythroid DAMP molecules to drive vascular injury and
sterile inflammation, which contribute to the pathogenesis of sickle cell disease.
Hemolysis releases cell free hemoglobin (Hb), which is normally scavenged by
haptoglobin and CD163. Free hemoglobin reacts with and scavenges NO via the
dioxygenation reaction and also reacts with hydrogen peroxide to generate hydroxyl
radicals via the Fenton reaction. This process leads to endothelial dysfunction and

20
pathological vascular remodeling. Oxidized hemoglobin releases free heme, which can
trigger a sterile inflammatory reaction involving TLR4 activation, and stimulates
neutrophils to release NETs. These inflammatory events are proposed to cause
vasoocclusion and acute chest syndrome in sickle cell disease. There are several potential
therapies using the indicated agents (shown in red text) that target multiple stages of this
proposed pathophysiological pathway. RBC=red blood cell (Gladwin MT et al12).
Furthermore, although the impacts of genetic modifiers of SCD are relatively
known in the developed world, there is paucity of information on this from Africa.
Moreover, because of genetic variability in different populations, it is pertinent that more
studies are carried out among cohorts from different ethnic backgrounds to fully
understand the impact of genetic modifiers on SCD.
These observations underscore the inherent potentials of hemolysis and genetic
markers contributions to the clinical course of SCD and fuells the need for search for
more markers of SCD expression that could help to fully understand the disease.
Therefore, putting more focus on some hypothesised markers may help in elucidating
more facts on predictors of SCD phenotypes.
1.2. REVIEW OF SOME HYPOTHESISED SCD PHENOTYPE MARKERS OF
INTEREST
HEMOLYSIS MARKERS
1.2.1 Haptoglobin: This is a protein produced mainly by the liver and regarded
as an acute phase protein because it is elevated in inflammatory conditions. It is an α-
sialoglycoprotein found in mammals but in humans it exhibits polymorphism through two
dominant alleles (Hp1 and Hp2) located on the long arm of chromosome 16q22 and 3
phenotypes have been recognised (HP1-1, HP2-2, & HP2-1)16,17. The HP1-1 allele is
found commonly among Africans and South Americans. It is least prevalent in South east
Asia and it is the most biologically active of the three haplotypes with regards to binding
free plasma Hb (plasma hemoglobin) and suppressing inflammation16. The HP2-2 variant
has the least biological activities with respect to binding free plasma HB and suppressing
inflammation16,17. The HP2-1 variant has intermediate biological and anti-inflammatory
abilities compared to the first two variants. Although haptoglobin has antioxidant and
antibacterial properties, their most striking roles are generally in modulating acute phase

21
responses. They are the first line scavenger of free plasma Hb where they combine and
bind free hemoglobin in the blood stream to form an hemoglobin-haptoglobin (Hb-HP)
complex which is quickly recognised by the scavenger receptor CD163 located on the
surfaces of circulating monocytes and liver macrophages16,17. Haptoglobin disappears
faster than being created when large amounts of RBC are destroyed in the intravascular
compartment due to excess amount of free Hb released into the blood stream. This leads
to reduction in the blood level of haptoglobin. As a result of this, haptoglobin has high
sensitivity and specificity in the diagnosis of hemolytic anemia16,17. Hence, in conjunction
with other markers of hemolysis, and in the absence of other factors like liver disease,
infections, drugs and other inflammatory diseases that may cause alterations in
haptoglobin, blood levels of haptoglobin could be used to ascertain the degree of
hemolysis in chronic hemolytic anemia condition like SCD16,17. Although previous
studies showed the predominance of Hp 1-1 and Hp 2-1 haplotypes among Brazilian and
Nigerian SCD patients respectively,16,18 till date, the influence of Hp polymorphism on
the phenotypic expressions of the SCD patients in the two countries has not yet been
studied. A study of Haptoglobin genotypes’ behaviour among SCD patients will help to
further understand how this parameter influences the clinical outcome of SCD bearing in
mind that haptoglobin is now being used for acute severe haemolytic conditions in some
parts of the world19. This will help to answer the question as to whether the proposition
for its use as an adjunct therapy in the treatment of SCD is justifiable20.
1.2.2 Hemopexin (HPX): Hemopexin is a heme-binding plasma glycoprotein
which is the second line of defense against hemolysis mediated oxidative damage by
mopping up the liberated free plasma heme. It is produced primarily in the liver but in
addition, other parenchymal cells produce it. The heme-hemopexin complex that is
formed is subsequently delivered to the liver cells through receptor- mediated endocytosis
after which the heme is taken off and the HPX is recycled. Decreased plasma level of
HPX indicates higher degree of hemolysis from RBC destruction reflective of increased
hemolysis severity in patients with associated heme toxicities and/or SCD19,21,22,23. To this
end, researchers are currently exploring therapeutic roles for hemopexin infusion in
SCD19,21,22. Hence, further studies are needed to throw more light on the influence of
hemopexin on the clinical expression of SCD in order to justify or dispel the need to
incorporate hemopexin therapy into the care of SCD patients.

22
1.2.3 Lactate dehydrogenase (LDH): Lactate dehydrogenase is an intracellular
enzyme that abounds in many cells and tissues of human body where it plays crucial roles
in generating energy for the cells through two key processes (glycolysis and
gluconeogenesis)24. Different isoenzymes of it have been recognised based on their cells
or tissues of origin. LD1 and LD2 are primarily derived from the red blood cells, heart
and the kidney while LD3 is mainly from lymphoid cells and platelet. LD4 and LD5 are
primarily from the liver and skeletal muscles. The concept about the mechanisms of LDH
as marker of SCD severity is still debatable. While some authors have argued that the
elevated levels of LDH in SCD is due to hemolysis24,25, others have linked the elevation
to tissue destruction26. However, more studies are in agreement with the hemolysis theory
as the primary source of the LD1 and LD2 isoenzymes in patients with SCD as they
strongly correlate with known markers of hemolysis in these patients24,25,27. As a result of
this, LDH serum levels especially the LD1 & LD2 isoenzymes, are now been considered
useful markers of intravascular hemolysis and disease severity in patients with
SCD24,25,27. It is now being considered as parts of routine tests for SCD in most developed
parts of the world as markers of SCD severity based on new findings that it also correlates
well with other complications of SCD9,24,25,27. Kato et al24, found high correlation of
elevated LDH with ntiric oxide insufficiency, increased rates of leg ulcers, pulmonary
hypertension, priapisms and deaths among SCD patients in the USA. Similarly, Mikobi
et al28 found increased disease severity among SCD patients with elevated LDH in Congo.
But of more interest is the suggestion by Mecabo et al27, that LDH levels in SCD could
be used to monitor response to hydroxyurea following their study of LDH behaviour
among the Brazilian cohorts of SCD patients. However, due to lack of resources and
tools, testing for LDH is seldomly performed in most developing countries of Africa
including Nigeria28,29. This is a paradox given the huge burden of SCD in these parts of
the world. Drawing from these, the yield of information that could be obtained from such
studies is therefore huge. Hence, further correlational studies on LDH could unravel more
potentials for this marker in the various aspects of care for the SCD patients and help to
further clarify its roles in SCD expression.
1.2.4 Red blood cell derived microparticles (RMP): These are small
biologically active plasma membrane vesicles released by red blood cells into the blood
stream either as a result of their aging and self preservation processes or as a result of
cellular injuries and destruction of the red blood cell30,31. They are generally less than

23
1µm in size and they have been implicated in some pathological processes where they
exert sundry roles which include: immune modulation, transfer of messages between
cells, activation of coagulation cascade and endothelial injury30,31. In SCD, levels of RMP
have been shown to be elevated both in steady state and in vaso-occlusive crisis31,32. In
addition, they concentrate plasma heme and transfer it to vascular endothelium where it
mediate oxidative stress, vascular dysfunction and vaso-occlussions in SCD31,32,33. Also,
the degree of RMP elevation has also been speculated to be closely related to known
markers of SCD complications/severity like nitric oxide (NO) depletion, generation of
thrombin, rise of plasma free plasma Hb, and increased rate of intravascular
hemolysis30,31,32,33. These deleterious synergies between the RMP and known markers of
SCD disease severity raises a possibility of using the RMP levels of SCD patients to
categorise them into clinical sub-phenotype groups and possibly prognosticate the disease
outcome. Most current studies on RMP in SCD were conducted on patients in the
developed parts of the world. A further study of RMP in SCD patients will help to
explore more on the roles of this biomarker in the clinical expressions of SCD patients.
1.2.5 Free plasma haemoglobin: Although majority (≥70%) of total hemolysis
in SCD occurs in the extravascular space (monocytic-phargocytic systems in spleen and
liver), while approximately ≤30% takes place within the intravascular compartment. In
SCD patients, polymerization of HbS leads to the destabilisation of the RBC membrane
and excessive premature destruction of the erythrocytes. The rate of destruction can be
up to 10% of their total erythrocytes in every 24 hours19,23,34. This process can lead to the
release of as much as 30g of free (decompartmentalised or plasma hemoglobin) per day
and this amount is enough to saturate the endogenous scavenging mechanisms comprising
the plasma haptoglobin and CD163 scavenging receptor. Hence, may result in substantial
amount of free circulating plasma Hb19,23. Free plasma Hb has been found to significantly
scavenge the nitric oxide (NO) levels because of its high affinity for NO. An experimental
study has observed rapid depletion of NO levels in SCD patients by up to 1000 fold by
free plasma Hb and noted that the release of plasma free haemoglobin and its role in
depleting the NO levels may be the main reason for the vascular complications seen in
SCD34. In addition, there is a catastrophic synergy in NO depletion between free plasma
Hb and arginase enzyme released by destroyed RBC during hemolysis in SCD
patients35,36. Nitric oxide is required for the maintenance of vascular integrity and
relaxation to prevent vascular events in SCD patients24,34,35,36. These roles have been

24
found to be totally abrogated when the plasma free haemoglobin level rises up to 6µM
leading to serious vascular complications like systemic and pulmonary hypertensions24,34.
In view of this, some authorities have hinted on the possible need to administer
Haptoglobin (the scavenger of free plasma Hb) to SCD patients in order to ameliorate the
disease complications19,20,23. Therefore, there is need for more studies on the free plasma
Hb of SCD patients in order to unravel more of its roles in the pathophysiology of SCD
as this could help to further strengthen or dispel its roles in the sequaelae of SCD.
1.2.6 Heme: Heme is synthesised in all human cells including the RBC. This
process involves eight enzymatic reactions that take place either within the cells’
mitochondria or their cytosols37. Upon formation, the heme is maintained in constant
equilibrium within the RBC through three regulatory mechanisms. These include
diffusion though the cell membrane, binding to the RBC cell membrane or cytoskeleton
and intracellular degradation by glutathione38. The first two mechanisms are
concentration dependent while the third mechanism requires the presence of adequate
glutathione at a concentration not ˂ 2mM within the RBC otherwise, excess heme could
accumulate and or escape to injure the RBC or other cells38. However, as the RBCs
become senescent they become denatured and some of them undergo autoxidation to
methemoglobin leading to the release of free heme into the plasma. In SCD patients, it
has been shown that sickled HbS has an exaggerated rate of autoxidation compared to
normal HbA leading to excess free heme in these patients38. In addition, the high rate of
destruction of sickled RBC also contributes to excessive amount of free heme in them38.
Free heme has been implicated in the pathophysiology and clinical expression of SCD
through two key methods. Firstly, it is implicated as a co-factor in the promotion of HbS
polymerization (the primary event in the pathophysiology of SCD) causing cascades of
pathological processes. Secondly, it has also been implicated in damaging the RBC
membrane thereby contributing to the increased rate of endothelium adhesion, hemolysis,
RBC removal by monocytic-phargocytic system and these lead to shorter life span of
RBC in SCD patients38. Recently, some researchers found that administration of
hemopexin (a known heme scavenger), prevents these unwanted events in animal
models22. This observation has led to others proposing the possibility of administering
hemopexin to SCD patients in order to ameliorate their disease19. It is therefore pertinent
that, more studies be conducted on SCD patients to further highlight the roles of plasma
free heme as a marker of disease severity in SCD. The major complications attributed to
heme and plasma hemoglobin in the SCD hemolysis phenotypes appear to be mediated

25
through complex and mixed processes involving vascular injuries, inflammation
promotion, oxidative injuries, and networking to signal the activation of other mediatory
molecules like the toll like receptors39-42. Given the impacts of these effects on SCD
patients, researchers are now suggesting that using the scavengers of heme and plasma
hemoglobin on patients with SCD could ameliorate their disease20,42. This raise the need
for more studies to further explore the relationships between these markers as well their
contributions to the clinical manifestations of SCD.
GENETIC MARKERS
1.2.7 Thalassemia syndromes: The thalassaemia syndromes are a group of
inherited disorders in which there is absence or reduced rate of synthesis of one of the
globin chains: either the alpha or the beta-globin chains of hemoglobin A (α2β2), which
is the major human adult haemoglobin approximately 97%. The other minor adult
haemoglobins are haemoglobin A2 (α2δ2) comprising 2.5% and fetal haemoglobin (α2γ2)
comprising less than 1% of the total hemoglobins. The involvement of either globin chain
causes imbalanced globin chain production, ineffective erythropoesis, microcytosis,
hemolysis and various degrees of anaemia43,44. The alpha (α) thalassaemia is usually due
to gene deletion, and is caused by loss of one (αα/-α) or two (-α/-α) of the normal
complement of four alpha genes (αα/αα) leading to a decrease in or absence of α chains.
Alpha thalassaemia is common in Africa where it is believed to offer some protection
against malaria in addition to ameliorating some clinical features of SCD patients43. The
beta (β) thalassaemia is usually due to a point mutation, may be beta (βo) or beta (β+). A
βo thalassaemia is one in which there is no β gene expression and, therefore, no β chain
synthesis and consequently no haemoglobin A (HbA) production. A β+ thalassaemia is
one in which the β gene is expressed but at a reduced rate so that there is some β chain
synthesis and some production of HbA. Beta thalassaemia trait has been found among
2.1% of Nigerian SCD patients44. Beta thalassaemia has been classified into three main
clinical subtypes based on the severity of the clinical manifestations and these include:
(a) Beta thalassaemia major otherwise known as Cooley’s anaemia in which case patients
have severe symptoms and blood transfusion dependent. (b) Beta thalassaemia trait this
is direct opposite of Cooley’s anaemia here patient is usually not symptomatic and the
diagnosis is usually made by chance when patients manifest very mild symptoms upon
the exposure of the patients to extreme stress. (c) Beta thalassaemia intermedia represents

26
the group of patients between the first two groups. They have mild to moderate
intermediate symptoms and are not blood transfusion dependent. The combination of
sickle cell mutation and beta-thalassaemia mutation gives rise to varying heterogenous
groups known as Hb S/β thalassaemia (Hb S/β-Thal). Patients with Hb S/β-Thal exhibit
heterogeneity in their clinical manifestations ranging from nearly asymptomatic state to
severe symptoms depending on the types of mutations involved and the amount β globin
synthesis which is reflected by the amount of HbA produced45. Currently, there is no
consensus about the classification of Hb S/β-Thal. However, two types namely: (Hb S/βo-
Thal and Hb S/β+-Thal) have been recognised generally45. The Hb S/βo-Thal has no
production of HbA and its clinically indistinguishable from sickle cell anaemia.
Therefore, it tend to exhibit a more severe course compared to the Hb S/β+-Thal in which
there is production of variable amounts of HbA which dilute the polymerisation of HbS
thus resulting in milder phenotypic expression. It is however important to note that the
influence of other genetic modifiers of SCD also affect this phenotypic expression45. To
this end, while increased hypercoagulability have been associated with coinheritance of
thalassaemia with SCD46, others have found very mild SCD phenotypic expressions with
Hb S/β+-Thal47 and alpha thalassaemia43 respectively. These observations suggest that the
exact pathophysiologic mechanisms and or influence of the thalassaemias on the
phenotypic expression of SCD are not yet fully elucidated hence, the need for more
studies.
1.2.8 Fetal hemoglobin (HbF) AND BCL11A ,HBS1L-MYB polymorphisms:
HbF has emerged as a central modifier of the several phenotypes like anemia, stroke,
infections and others seen in SCD patients48,49,50. The presence of HbF limits the rate of
polymerisation of HbS which is the primary event that leads to the cascades of both
pathological and clinical manifestations in SCD48,49,50. Luckily, the expression of HbF is
amenable to therapeutic manipulation. To this end, clinicians have used hydroxyurea to
increase the proportion of HbF in SCD patients with the aim of making the patients benefit
from its ameliorative effects on their disease phenotypes51,52. Interestingly, genetic
variations at three principal loci (BCL11A, HBS1L-MYB and HBB) each on chromosomes
2, 6 and 11 respectively, have been shown to account for increased expression of 10-20%
HbF variation among SCD patients in the USA, Brazilian and United Kingdom50. Of
these, only the BCL11A locus has been studied among the African SCD patients. Initial
studies in Tanzania 53 and Cameroon 54,55 have shown that single-nucleotide

27
polymorphism (SNPs) in the BCL11A are prevalent among SCD patients in both
countries with significant association of these SNPs with HbF. Researchers have hinted
on the high degree of variations in the micro allele frequency (MAF) of SNPs of other
genetic variants among the African SCD patients thus making extrapolation of findings
from one African country to another difficult50. These findings suggest that studies of
multiple SCD populations are needed especially from Africa, to further improve the
understanding of the impact of human diversity on HbF expression in SCD.
1.2.9 Glucose 6 phosphate dehydrogenase (G6PD): G6PD is a cytosolic
enzyme in the pentose phosphate pathway which supplies reducing energy to cells by
maintaining the level of the co-enzyme nicotinamide adenine dinucleotide phosphate
(NADPH). G6PDH reduces nicotinamide adenine dinucleotide phosphate (NADP) to
NADPH while oxidizing glucose-6-phosphate (G6PD)56. Humans with a genetic
deficiency of G6PD are predisposed to non-immune hemolytic anaemia and this
deficiency is highly prevalent in sub-Saharan Africa where it is believed that both HbS
and G6PD deficiency confer partial protection against malaria hence, its predominance
in Africa where malaria is endemic57,58. The prevalence of G6PD among the Nigerian
population is between 15-25%59 while that among the Brazilian population varies
between 1-13% depending on the region of the country.56 The most prevalent variant in
the two countries is the G6PD A-variant56,59. There have been conflicting reports about
the genetic polymorphisms of G6PD A-variants in Africa 60,61,62. De-Araujo et al60 and
Capelini et al61 found a predominance of G6PD genotypes with G6PD 202A and G6PD 376G
alleles in Senegal and other parts of Africa similar to the genotypes in Brazil56. However,
Clark et al62 found a predominant of G6PD968C and G6PD376G alleles among the Gambian
population also from the West Africa sub-region like Senegal. This suggests
heterogeneity in the patterns of G6PD A-variants among the African population and this
factor could affect the clinical events in patients with G6PD deficiency. Till date, only
few studies investigated the potential effects of G6PD deficiency on SCD and the studies
have shown conflicting reports. While studies from Saudi Arabia and Burkina Faso, found
no effect of G6PD deficiency on the clinical manifestations and laboratory parameters of
SCD patients63,64, studies from the USA and France found association with increased
cerebral blood flow velocity, increased rate of acute anaemic events, blood transfusions,
vaso-occlussive crisis, and decreased steady state haemoglobin levels58,65,66. The mixed
reports from these studies concerning the effects of G6PD deficiency co-inheritance on

28
the clinical events or laboratory parameters of the SCD raise the need for further studies
to dispel or establish if the co-inheritance impact any influence on SCD manifestations.
1.2.10 Uridine diphosphate glucuronyltransferase 1A (UGT1A)
Polymorphism: Patients with Gilbert's syndrome (GS) have a defect in the uridine
diphosphate glucoronosyl transferase 1A gene that encodes for uridine diphosphate
glucuronyltransferase 1A (UGT1A) enzyme which is the main enzyme responsible for
bilirubin conjugation among the uridine diphosphate glucuronosyl transferase (UGT)
family67,68. Polymorphisms in the UGT1A gene results in a 60-70% reduction in the
enzyme and by extension, the liver's ability to conjugate bilirubin leading to unconjugated
hyperbilirubinemia.69 Bilirubin is an endogenous antioxidant and some authors have
postulated that, Gilbert's syndrome may actually reduce the risk of various age-related
diseases because of the antioxidant properties of bilirubin67,69. One recent study found
that mortality rates observed for people with Gilbert's syndrome in the general population
were shown to be almost half those of people without evidence of Gilbert's syndrome70
and the occurrence of GS had also been thought to give protection to Africans against
malaria among other benefits71. Reports on co-inheritance of SCD with GS have shown
increased rates of cholelithiasis, need for cholecystectomy and increased morbidity72,73,74.
In addition, the response to hydroxyurea treatment was found to be blunted by the
presence of GS in some SCD patients75. These further highlight the deleterious roles GS
could play in modulating the SCD phenotypic expression. Studies on GS behaviour
among Africans and Brazilians are scanty and no specific study has been found from
Nigeria. However, a brief report by Fertrin et al76 found increased rate of
hyperbilrubinemia and possible risk for early onset of symptomatic gallstone disease that
may warrant cholecystectomy among Brazilian SCD patients. These observations raise
the need for more studies to explore the roles of GS in the clinical expression of SCD
patients.

29
2. JUSTIFICATION
Although several hypotheses have been proposed for the phenotypic diversity found
in sickle cell disease, these factors do not fully explain the clinical heterogeneity observed
in SCD patients. Therefore, efforts are on-going in search of new markers that can be
used to better characterize sickle cell disease. The present study aims to establish a link
between markers of hemolysis and some genetic modifiers, and clinical phenotypes of
patients with sickle cell disease. These may be useful for predicting severity as well as
influencing therapeutic decisions in SCD.

30
3. OBJECTIVES
3.1. General objective
To determine the influence of some hemolysis and genetic markers on the
phenotypic expression of patients with sickle cell disease.
3.2 Specific objectives are to:
• Quantify red blood cell microparticles, plasma hemoglobin, heme, hemopexin,
and haptoglobin in plasma samples from Brazillian adult patients with sickle cell
disease treated with or without hydroxyurea, and control subjects
• To correlate the clinical, hematologic and biochemical results of patients with
sickle cell disease with the above quantified markers.
• To evaluate the influence of hydroxyurea treatment on the levels of free plasma
hemoglobin, heme, hemopexin, haptoglobin, and red blood cell microparticles of
SCD patients.
• Identify and try to establish any association between the polymorphisms of G6PD,
UGT1A1, BCL11A, haptoglobin genes and alpha thalassemia trait with clinical
events and laboratory markers of Nigerian children with SCD.

31
4. HYPOTHESIS
Some recent studies have shown that hemolysis and genetic markers play important
roles in the progression of sickle cell disease. The aim of this study is to establish whether
some hypothesized biologic and genetic markers have any link with the laboratory and
clinical expressions of patients with sickle cell disease as these may be useful in predicting
severity as well as influencing therapeutic decisions in SCD.

32
5. PATIENTS AND METHODS
5.1. Type of study
This was a cross-sectional descriptive study
5.2. Place of research
The research was carried out at the Hemoglobin and Genome Laboratory of the
Hematology and Hemotherapy Center of UNICAMP and the pediatrics hematology unit
of the Ekiti State University Teaching Hospital (EKSUTH) Ado Ekiti, Ekiti State Nigeria.
Institutional ethical approvals were obtained (EKSUTH/A67/2016/03/003 and
UNICAMP CAAE 54031115.9.0000.5404).
5.3. Selection of patients and control subjects
The study included patients with sickle cell disease treated at the hematology and
hemotherapy centre, UNICAMP and EKSUTH with diagnostic testing by high pressure
liquid chromatography (HPLC) (Bio-Rad, Hercules, CA, USA) and genetic studies.
UNICAMP
For the hematology and hemotherapy centre arm of the study, the study participants
included patients of both sexes, aged 18 – 60 years and are on regular follow up. The
patients were stable state, i.e, absence of any acute event such as painful crisis, and or
infection, within a month and without blood transfusion for at least three months to
recruitment period. 12mL of each participant's blood were collected for plasma separation
and other analyses.The control group consisted of healthy volunteers, and staff members
at the Hemoglobin and Genome Laboratory of the Hematology and Hemotherapy Center
of UNICAMP, aged 18-60 years. All the controls had HbAA genotype and this was
confirmed by high performance liquid chromatography (HPLC). The determination of
clinical sequale and complications of sickle cell disease in all patients, were as previously
described by Ballas et al77
EKSUTH
The EKSUTH participants consisted of children and adolescents diagnosed with
SCD and aged 2 -21 years of both sexes in steady state. Children who accompanied their
siblings to the EKSUTH to the outpatients` well-child clinic served as controls.

33
To qualify for inclusion, the SCD patients must have been on regular follow up at
the pediatric hematology unit. The determination of clinical sequale and complications of
sickle cell disease in all patients, were as previously described by Ballas et al77.
5.4. Exclusion Criteria:
1. Lack of consent of the patient, or parents or accompanying family members /
caregivers.
2. Patients in crisis or pain crisis in the last month before the study.
3. Patients hospitalized for any medical condition in the last three months prior to the
study.
4. Patients on chronic blood transfusion or those who have received blood transfusion in
the last three months.
5. Patients with other chronic medical conditions.
6. Pregnancy
5.5. Sample size:
A total of 358 people participated in the study. They comprised of 138 patients
with SCD and 39 controls from hematology and hemotherapy centre, UNICAMP, Brazil
and 110 children with SCD alongside 68 controls from the EKSUTH in Nigeria.
5.6. Study Procedure and data collection
After obtaining the consent of participants, parents and or assent as applicable,
peripheral venous blood samples approximately 12 mL (4ml into EDTA tube for
hematological and DNA studies, 4ml into EDTA tube for plasma extraction, and 3.5ml
into Sodium citrate tube for red blood cell microparticle studies), were collected by
venipuncture from the patients.
Blood samples were processed to obtain plasma and stored in freezer at -80 ° C until
analysis as applicable.
5.7. Clinical history and events
A detailed history with special attention to the frequency of acute events such as
pain episodes, and acute chest syndrome in the past 12 months were obtained from the
records. In addition, frequency of other chronic events complicating SCD such as,
cerebrovascular disease, avascular necrosis of the head of femur, leg ulcers, priapism,

34
SCD retinopathy, pulmonary complications and kidney disease, were verified through
past hospital records, and were defined according the SCD co-operative study group77.
A brief description of few of the events by Ballas et al are as follows77.
1. Painful crisis: Acute significant painful episode will be described as painful
event(s) requiring a hospital visit or disruption of normal daily activities and
requiring the use of oral or parenteral analgesics.
2. Avascular necrosis: This will be defined as osteonecrosis or aseptic necrosis of
the head of femur or humerus confirmed by radiography as irregularity of the
articular surfaces of the head of femur/humerus
3. Severe bacterial infections: These will be defined by the presence of one or more
of pneumonia, sepsis, meningitis, osteomyelitis, septic arthritis, confirmed by
positive blood culture and or radiograph as appropriate.
4. Acute chest syndrome: An acute illness characterised by fever, and respiratory
symptoms (dyspnea, chest pain) accompanied by low pulse oxymetry and new
pulmonary infilterates on chest radiodragh
5. Stroke (cerebro-vascular disease): Acute neurologic symptoms or signs
secondarytoocclussion of and orhemorrhage from cerebral vessels confirmed on
computerized tomography (CT) scan or magnetic resonance imaging (MRI)
6. Chronic leg ulcer: Ulceration of the skin and underlying tissue of the lower
extremeties, especially the media or lateral surface of the ankle.
7. Priapism: Sustained, unwanted and painful penile erection.
8. Cholelithiasis: Confirmed cholelithiasis on abdominal USS with or without
abdominal pain.
However, due to the lack of right heart catetherisation to diagnose pulmonary
hypertension the tricuspid regurgitation velocity (TRV) obtained from Doppler
echocardiography was used to categorise patients into two groups based on risk
for pulmonary hypertension. Patients with TRV < 2.5m/sec were categorised as
having normal TRV and those with TRV ≥2.5m/sec were categorised as having
elevated TRV and at risk of pulmonary hypertension78. Urinary albumin-
creatinine ratio (UACR) of less than 30mg/g was taken as no albuminuria (i.e.
normal), between 30mg/g and 300mg/g as microalbuminuria and greater than
300mg/g was classified as macroalbuminuria79. Patients were also classified into

35
two groups based on whether they had presence or absence of proliferative SCD
retinopathy.
Routine laboratory investigations: All laboratory tests were done by standard
procedures.
5.8. Haematological tests:
These included haematocrit; haemoglobin concentration; WBC - total and differential
counts; MCV; MCHC, RDW, reticulocyte count and platelet count and fetal
Haemoglobin level measurements using automated hematology analyzer and HPLC
respectively.
5.9. Biochemical tests: These were done by standard laboratory procedures and they
included serum bilirubin – total and unconjugated, lactate dehydrogenase (LDH) and
urinalysis to determine microalbuminuria.
5.10. Colorimetric Assays:
5.10.1. Plasma hemoglobin: This was done on frozen plasma samples with the
QuantiChromTM Hemoglobin Assay Kit (DIHB-250), BioAssay Systems
USA. This assay is based on an improved Triton/NaOH method, in which
the haemoglobin present in a sample is concerted to a uniform coloured end-
product, and the intensity of colour measured at 400nM is directly
proportional to the haemoglobin concentration present in the plasma80.
5.10.2. Heme: This was done on frozen plasma samples with the QuantiChromTM
Heme Assay Kit (DIHM-250), BioAssay Systems USA. The Assay Kit is
based on an improved aqueous alkaline solution method, in which the heme
is converted into a uniform coloured form. The intensity of colour, measured
at 400 nm, is directly proportional to the heme concentration in the sample81.
5.11. ELISA Tests:
5.11.1. Hemopexin: This was done on frozen plasma samples with the Abcam
Human Hemopexin (ab171576) ELISA kit. This assay employs an affinity
tag labelled capture antibody and a reporter conjugated detector antibody
which immunocaptured the samples analyte in solution. This entire complex

36
(capture antibody/analyte/detector antibody) is in turn immobilised via
immunoaffinity of an anti-tag antibody coating the well. Briefly, to perform
the assay, a Hemopexin specific antibody has been precoated onto 96-well
plates. Standards or test samples were added to the wells and subsequently
biotinylated Hemopexin (antibody mix) was added and incubated on a plate
shaker then followed by washing with wash buffer. After washing away any
unbound substances, an enzyme linked polyclonal antibody specific for
hemopoxin was added to the wells and a substrate solution was then added to
the wells and colour change develops in proportion to the amount of
hemopexin bounded by in the initial step. The development of colour was
stopped by adding stop solution. The density of yellow coloration was
proportional to the amount of Hemopexin captured in the plate. The intensity
was measured at 450nM82. The minimal detectable limit of the kit is
1.44ng/ml.
5.11.2. Haptoglobin: This was done on frozen plasma samples with the Quantikine
Human Haptoglobin (DHAPGO) ELISA kit, R & D Systems USA. The assay
employs the quantitative sandwich enzyme immune assay technique in which
a Haptoglobin specific antibody has been precoated onto 96-wellplates and
immobilised. Standards or test samples were added to the wells and any
Haptoglobin present was bounded by the immobilised antibody. After
washing away any unbound substances, an enzyme linked polyclonal
antibody specific for haptoglobin was added to the wells. This was followed
by a repeat wash to remove any unbound antibody-enzyme reagent, a
substrate solution was then added to the wells and colour develops in
proportion to the amount of haptoglobin bounded by in the initial step. The
development was stopped by adding stop solution. The density of coloration
was proportional to the amount of Haptoglobin captured in the plate. The
intensity of the colour was measured at 450nM83. The minimum detectable
limit of the kit ranged from 0.031 – 0.529ng/ml and the mean minimal
detectable limit is 0.192ng/ml.
5.12. Flow Cytometry:
5.12.1. Red blood cell microparticles quantification: Flow cytometry was used
to characterise and quantify the red blood cells microparticles (RMP). The
processes involved differential centrifugation followed by staining and

37
fluorescence flow cytometry analysis as previously described84. The
processes are briefly described below.
5.12.2. Sample collection and plasma separation for RMP analysis: 3.5ml of
citrated venous sample collected by 21gauge syringe were drawn from each
participants after taking the first 8ml of blood into two EDTA sample tubes
(4mL each) for plasma separation and the other for hematological analysis
with very light tourniquets applied. The citrate samples were not mixed or
rocked and were transported securely in upright positions inside the sample
carrier to the laboratory immediately and the plasma separation was done
within 30 minutes of collection. To obtain the plasma, the topmost 1ml of the
citrated whole blood sample was pipetted out and discarded and the remaining
was processed through a two stage centrifuging, the first at 2,500g x 15min
at 22 °C thereafter the topmost 1ml of the plasma from this first centrifugation
was pipetted out and the remaining discarded. A second centrifugation at
13,000g x 5mins at 22 °C was done for the topmost 1ml plasma obtained from
the first centrifugation. The topmost 700µl of the product of the second
centrifugation was pipetted out into a separate polypropylene tube and the
platelet count of the plasma was checked using Beckman Coulter hematologic
counter (Model 8246-EN, SN- AN37824), USA, to ensure it was platelet
depleted. Thereafter, the samples were aliquoted into polypropylene tubes
and frozen at -80 °C until analysis.
5.12.3. Red blood cell microparticle staining and quantification: The staining
reagents (a. Calcein violet AM (Molecular probes-Invitrogen: 3,125µg (5µL),
b. Bovine Lactadherin FITC (Haematologic Technologies, Inc. 0.83µg
(10µL), c. Anti-CD235a R-PE (Life Technologies: 2µL), d. Sterile filtered
PBS 2 x 0.22 µm membrane) and aliquoted frozen platelet poor plasma were
brought to room temperature. The reagents were prepared according to
manufacturers` specifications. The antibodies (Calcein AM, Anti-CD235a
and Lactadherin were also subjected to a high speed centrifugation at 20,000g
x 5minutes at room temperature to remove false positive events at analysis.
After preparing fresh polypropylene tubes, 10µl of each sample was stained
with 5µL, 10µL, 2µL & 5µL of calcein, lactadherin, anti-CD235a and filtered
sterile PBS buffer respectively. The resultant solution was gently vortexed
and incubated in the dark at 37 ° C, -5%CO2 for 60mins initially. Thereafter,

38
500µL of sterile filtered PBS was added and then incubated for the second
time in the dark at 37 ° C, -5%CO2 for 30mins. Immediately after the second
incubation, the resultant solution was further diluted with 3,468µL of sterile
filtered PBS to make a final dilution of 1:400 with a resultant solution totaling
4000µL. This resultant solution was immediately analysed on a calibrated
flow cytometer, the Beckman Coutler`s CytoFLEX Flow Cytometer, (Model
A00 -1-1102) USA, using the staining buffer as negative control. Each sample
was aspirated and read for 10mins by the Cytoflex machine. The RMP events
were expressed per mL.
5.13. Genetic Studies:
The DNA of the Nigerian patients extracted from each participant by Qiagen
QIAamp DNA (Blood Mini Kit Cat No. 51104 Germany), was used to confirm the
diagnosis of SCD by polymerase chain reaction (PCR) at the genetic laboratory at the
Hematology and Hemotherapy centre, Hemocentro-Universidade Estadual de Campinas
(UNICAMP) Brazil. All DNA studies were carried out blinded regarding the clinical and
laboratory parameters of the participants.
5.13.1. Alpha thalassemia determination: Alpha-thalassemia (α3.7Kb deletion)
was investigated by GAP-PCR according to Dodé et al., 1993. The PCR was
performed in 25 μL reaction volume containing 100ng of DNA sample; 1X
α- Buffer (Tris-HCl 2M (pH 8.6), (NH4)2 SO4 1M, MgCl2 1M, Na2EDTA
0.2M, BSA and β-mercaptoetanol 14.3M); 1X DMSO; 0.3mM of dNTP mix;
0.2 µM of each primer (C2:CCATGCTGGCACGTTTCTGAandC10:
GATGCACCCACTGGACTCCT); 1U of GoTaq® Flexi DNA Polymerase
(Promega Corporation, Madison, USA). Thermal cycle conditions were as
follows: preheating at 94°C by 5 minutes, followed by 35 cycles of 94°C for
45 seconds, 56°C for 1 minute, and 72°C for 2 minutes and a final extension
at 72°C for 7 minutes was performed. After electrophoresis in a 1.2% agarose
gel a fragment of 2.1Kb could be observed for normal alleles and 1.9Kb
fragment for deleted alleles (-α3.7Kb).
Alpha-thalassemia (α4.2Kb deletion) was investigated by Multiplex-PCR.
The PCR was performed in 25 μL reaction volume containing 100ng of DNA
sample; 1X α- Buffer (Tris-HCl 2M (pH 8.6), (NH4)2 SO4 1M, MgCl2 1M,

39
Na2EDTA 0.2M, BSA and β-mercaptoetanol 14.3M); 1X DMSO; 0.3mM of
dNTP mix; 0.4 µM of primer (P71: TACCCATGTGGTGCCTCCATG and
0.3 µM of each of primer P72:TGTCTGCCACCCTCTTCTGAC and P52:
CCTCCATTGTTGGCACATTCC; 1U of Taq DNA Polymerase (Invitrogen,
Carlsbad,CA). Thermal cycle conditions were as follows: preheating at 94°C
by 5 minutes, followed by 35 cycles of 94°C for 45 seconds, 60°C for 1
minute, and 72°C for 2 minutes and a final extension at 72°C for 7 minutes
was performed. After electrophoresis in a 1.2% agarose gel a fragment of
1596 bp could be observed for deleted alleles (-α4.2Kb) and 233 bp as an
internal control to verify the quality of DNA sample.
5.13.2. Uridine diphosphate glucuronosyl transferase 1A (UGT1A1)
promoter polymorphism (rs8175347): DNA samples were used for
genotyping of the (TA)nTAA UGT1A1 promoter polymorphism (GenBank
accession NG_002601). The rs8175347 identification was performed by
Polymerase Chain Reaction (PCR) using a forward primer 5'- (6-FAM)
labelled (*) for detection by fragment analysis in capillary electrophoresis
system. The PCR reaction was prepared in 30 µL volume with 100ng of
genomic DNA; 1X Reaction Buffer (BIOTOOLS B&M Labs, Spain);
2.16mM MgCl2; 1.33 mM of dNTP mix; 133 nM of each primer (Integrated
DNA Technologies, Coralville, Iowa) named: UGT1A1_*F:
GTCACGTGACACAGTCAAAC and UGT1A1_R:
CAACAGTATCTTCCCAGCATG; and 1 U Taq DNA Polymerase
(BIOTOOLS B&M Labs, Spain). Thermal cycle conditions were as follows:
preheating at 96°C by 2 minutes, followed by 25 cycles of 96°C for 30
seconds, 58°C for 40 seconds, and 72°C for 40 seconds. An ended step at
72°C for 30 min was performed to promote adenylation of the PCR products.
The PCR product (1 μL) was added to 8.7 μL Hi-Di Formamide (Applied
Biosystems, Carlsbad, CA) and 0.3 μL of a GeneScan™ 500 LIZ™ size
standard (Applied Biosystems, Carlsbad, CA) and the fragments ranged from
197 - 203 bp, corresponding to (TA)5 - (TA)8 repeats, respectively, were
separated by capillary electrophoresis on a ABI3500 Genetic Analyzer and
analysed by Gene Mapper v 4.1 Software (both Applied Biosystems,
Carlsbad, CA). The UGT1A1 genotypes were further classified into three

40
subgroups namely: low, intermediate and high activity group based on their
activities and number of TA repeats.
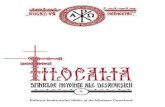
5.13.3. Haplotypes (β globin chain): The βs-haplotypes were determined by by
TaqMan SNP genotyping assay of three single nucleotide polymorphisms
(SNPs); Xmn I-rs7482144, Hinc II-rs968857, and Hinf I-rs16911905 as
follows.
Haplotypes linked to the βS mutation provided important anthropological
information regarding the multiple origins of the HbS allele. TaqMan®
Genotyping Assays (Applied Biosystems, Carlsbad, CA) were used for
screening of 3 polymorphic sites located at β-globin gene cluster and to
determine the different haplotypes: SENEGAL, BENIN, CAR (Central
African Republic), ARAB-INDIAN, CAMEROON. The assays related to
restriction sites were analysed: Xmn I (customized - rs7482144) at position
- 158 of the γG gene promoter; Hinc II (C_9599121_10 - rs968857 ) located
at 3' region of ψβ gene; and Hinf I (C_32838989_10 - rs16911905) at 5’ to
the β gene. DNA samples were prepared at 50ng/μL of concentration and the
SNP Genotyping assay was diluted to 5X concentrated, then the reaction
mixture contained: 2.5 μL TaqMan Genotyping MasterMix (2X); 1.0 μL of
diluted assay (5X) and 1.5 μL of DNA sample. The reaction was carried out
using allelic discrimination protocol in ABI7500 FAST and StepOne Plus
Real Time PCR systems (Applied Biosystems, Carlsbad, CA), following the
cycling conditions: 30 seconds at 60°C, 10 minutes at 95°C followed by 45
cycles of 15 seconds at 95°C and 1 minute at 60°C, and a final step named
post-PCR at 60°C for 30 seconds with automated allele calling settings for
the SDS 2.1 software (Applied Biosystems, Carlsbad, CA). The figure below
shows how the haplotypes could be identified.

41
Figure 3: The βs-haplotypes.
5.13.4. Glucose 6 phosphate dehydrogenase deficiency (G6PD): The
Identification of mutations: G6PD G202A - African (rs1050828), G6PD
A376G-(rs1050829), G6PD A542T-(rs5030872), G6PD G680T-
(rs137852328) and C563T - Mediterranean (rs5030868) was as follows.
TaqMan® Genotyping Assays (Applied Biosystems, Carlsbad, CA) were
used for screening of African and Mediterranean mutations of G6PD,
respectively identified as rs1050828 and rs5030868 DNA samples were
prepared at 50ng/μL of concentration and the SNP Genotyping assay was
diluted to 5X concentrated, then the reaction mixture contained: 2.5 μL
TaqMan Genotyping MasterMix (2X); 1.0 μL of diluted assay (5X) and 1.5
μL of DNA sample. The reaction was carried out using allelic discrimination
protocol in ABI7500 FAST and StepOne Plus Real Time PCR systems
(Applied Biosystems, Carlsbad, CA), following the cycling conditions: 30
seconds at 60°C, 10 minutes at 95°C followed by 45 cycles of 15 seconds at
95°C and 1 minute at 60°C, and a final step named post-PCR at 60°C for 30
seconds with automated allele calling settings for the SDS 2.1 software
(Applied Biosystems, Carlsbad, CA). PCR-RFLP was performed in aleatory
samples to confirm G6PD G202A genotypes. The PCR reaction was prepared
in 25 µL volume with 100ng of genomic DNA; 1X Colorless GoTaq® Flexi
Reaction Buffer (Promega Corporation, Madison, USA); 2 mM MgCl2; 0.2
mM of dNTP mix; 0.2 µM of each primer (Integrated DNA Technologies,
Haplotype Name Xmn I (1)
rs7482144
Hinc II (2)
rs968857
Hinf I (3)
rs16911905
Sequence
Senegal + (A) + (T) + (G) ATG
Arab-Indian + (A) + (T) - (C) ATC
CAR - (G) - (C) - (C) GCC
Benin - (G) + (T) - (C) GTC
CAM - (G) + (T) + (G) GTG

42
Coralville,Iowa) named G6PD-202_F:CAAGGGTGGAGGATGATGTATG
and G6PD-202_R: AACGCAGCAGAGCACAGCAG; and 1U of GoTaq®
Flexi DNA Polymerase (Promega Corporation, Madison, USA). Thermal
cycle conditions were as follows: preheating at 96°C by 2 minutes, followed
by 35 cycles of 96°C for 30 seconds, 60°C for 30 seconds , 72°C for 1 minute
and a final extension at 72°C for 5 minutes was performed. The PCR
amplicon corresponding to 527 bp was digested with the restriction enzyme
Nla III and it was possible to observe the following fragments: 376 and 151
bp for wild allele and 253, 151 and 123 bp for mutant alleles. Identification
of other G6PD mutations: G6PD A376G (rs1050829), A542T (rs5030872)
and G680T (rs137852328) was done by direct Sanger sequencing using an
ABI 3500 Genetic Analyzer (Applied Biosystems) from genomic DNA to
screen the others mutations in the G6PD gene. The region that include the
SNPs G6PD A376G (rs1050829), A542T (rs5030872) and G680T
(rs137852328) was amplified followed these conditions in 30 µL volume:
150ng of genomic DNA; 1X Colorless GoTaq® Flexi Reaction Buffer
(Promega Corporation, Madison, USA); 2 mM MgCl2; 0.2 mM of dNTP mix;
0.2 µM of each primer (Integrated DNA Technologies, Coralville,Iowa)
named G6PD-1_F: ACCTGGCCAAGAAGAAGATCTACandG6PD-1_R:
TGATAGCTCAGACACTTAGGTTTTG; and 1,5U of GoTaq® Flexi DNA
Polymerase (Promega Corporation, Madison, USA). Thermal cycle
conditions were as follows: preheating at 96°C by 2 minutes, followed by 35
cycles of 96°C for 30 seconds, 60°C for 40 seconds , 72°C for 2 minutes and
a final extension at 72°C for 5 minutes was performed. The PCR product
(2273bp) was submitted to sequencing reaction by following conditions: 40ng
PCR product purified by ammonium acetate and ethanol method, 1,0 µL
BigDye Terminator v3.1 Ready Reaction Mix (AppliedBiosystems, Foster
City, CA, USA), 1X BigDye Reaction Buffer, 2µM of each primer, in
separated reaction (G6PD-2F:
GAGAAGCTCAAGCTGGAGGACTandG6PD_Seq_R:
GCAGGACTCGTGAATGTTCTTG). After thermal cycling (preheating at
96°C by 2 minutes, followed by 25 cycles of 96°C for 15 seconds, 58°C for
5 seconds, 60°C for 4 minutes and a final extension at 72°C for 5 minutes)

43
the sequencing reaction product was purified by ammonium acetate and
ethanol method, dried at 65ºC and ressuspending in 10 µL of Hi-Di
Formamide for electrophoresis. Resulting sequence data were compared with
the reference NM_000402.
5.13.5. Haptoglobin Genotypes determination: The haptoglobin genotypes of
the patients were determined according to Santos et al16 technique using
the selective amplification of the different alleles.
5.13.6. BCL11A Polymorphism and HbF quantification: The HbF quantitation
was done using HPLC (Bio-Rad Variant D10, USA) based on
manufacturer`s specifications. The BCL11A polymorphisms of rs
4671393, rs11886868, rs766432, rs1427407, rs 7606173, rs 6706648, rs
7557939, rs 6738440, rs 6732518 and rs 13019832 were determined by
real time PCR as described below.
DNA samples were prepared at 50ng/μL of concentration and the SNP
Genotyping assay was diluted to 5X concentrated, then the reaction
mixture contained: 2.5 μL TaqMan Genotyping MasterMix (2X); 1.0 μL
of diluted assay (5X) and 1.5 μL of DNA sample. The reaction was carried
out using allelic discrimination protocol in ABI7500 FAST and StepOne
Plus Real Time PCR systems (Applied Biosystems, Carlsbad, CA),
following the cycling conditions: 30 seconds at 60°C, 10 minutes at 95°C
followed by 45 cycles of 15 seconds at 95°C and 1 minute at 60°C, and a
final step named post-PCR at 60°C for 30 seconds with automated allele
calling settings for the SDS 2.1 software (Applied Biosystems, Carlsbad,
CA).
5.14. Data analysis: Data were analyzed with the GraphPad Prism version 5.0 statistical
software for windows (San Diego, California, USA) and STATA Statistical Software
release 12. (College Station, TX: STATACorp LP; 2011, USA), using both descriptive
and comparative statistics. The frequencies of variables were described and the
significance of differences between groups of participants was assessed using the
Kruskal-Wallis analysis of variance (ANOVA), chi-square, Mann-Whitney or Fisher`s
exact tests as appropriate. For the correlation studies, data were normalised by taking

44
logarithms of the various variables and correlating them with other variables of interest
using the Pearson correlation and the scatter diagrams were plotted as applicable. The
correlational studies were done with STATA Statistical Software. The logarithm of the
variables was used for the correlations because data were not normally distributed and
had some outliers. The level of significance was set at P < 0.05 for all statistical tests.

45
6. RESULTS
HEMOLYSIS STUDIES
6.1. Parameters in patients and controls
Table 1 shows the summary of participants and parameters (UNICAMP)
Parameters a. SS (N=78)
Median (Range)
b. SBeta0
(N=12)
Median (Range)
P Value
(a vs b)
c. SBeta+
(N=12)
Median (Range)
P Value
(a vs c)
d. SC
(N=36)
Median
(Range)
P Value
(a vs d)
e. AA
(N=39)
Median (Range)
P Value
(a vs b vs c d
vs e)
Age in years 41 (18 – 60) 38 (18 – 60) 0.754 39 (21 – 58) 0.501†
45 (27 – 60) 0.08†
35 (20 – 60) 0.0237
*1
Red blood cell
microparticles
(Events/ML)
200000.0 (0 –
17840000.0)
120000.0 (0 -
440000) 0.168
† 40000 (0 –
160000) 0.0002
† 80000.0 (0 –
1320000.0) 0.0006
† 0.0 (0 – 12000.0)
<0.0001 *2
Plasma Hemoglobin
(mg/dL)
84.6 (28.2 – 257.5) 77.5 (42.0 – 134.0) 0.479†
58.7 (34.0 –
196.0) 0.015
† 63.5 (33.4 –
158.9) 0.0001
† 42.7 (27.1 – 90.0)
<0.0001 *3
Haptoglobin
(ng/mL)
1937.0 (279.0 –
17520.0)
2342.0 (540.0 –
5290.0) 0.939
† 5417.0 (480.0 –
18180.0) 0.04
† 2832.0 (424.0
– 29670.0) 0.0381
† 986000.0 (656800.0
– 2455000.0) <0.0001
*4
Heme (µM) 55.6 (15.8 – 206.0) 53.2 (31.6 – 94.0) 0.479†
45.0 (22.9 –
119.0) 0.048
† 42.4 (19.5 –
165.0) 0.0025
† 28.5 (12.9 – 86.6)
<0.0001 *5
Hemopexin (µg/mL) 469.0 (76.7 – 1937.0) 448.0 (227.0 –
1221.0) 0.542
† 704.0 (127.0 –
1805.0) 0.803
† 761.4 (114.0 –
1930.0) 0.045
† 988.0 (800.0 –
1409.0) <0.0001
*6
HbF (%) 13.1 (1.7 – 31.0) 13.9 (2.8 – 35.2) 0.433†
11.7 (0.6 – 27.9) 0.554†
0.8 (0.2 –
12.7) <0.0001
† 0.2 (0.1 – 0.9)
<0.0001 *7
Hb Conc (g/dL) 8.5 (4.2 – 12.9) 8.5 (6.8 – 9.7) 0.680†
9.8 (8.4 – 11.5) 0.0009†
11.3 (9.3 –
15.2) <0.0001
† 13.5 (11.7 – 16.3)
<0.0001 *8

46
Platelet ( X 103/uL) 339.0 (99.0 – 682.0) 377.0 (172.0 –
755.0) 0.413
† 375.0 (76.0 –
458.0) 0.546
† 264.0 (61.0
557.0) 0.04
† 257.0 (171.0 –
453.0) 0.002
*9
WBC ( X 103/uL) 6.4 (3.2 – 14.0) 7.8 (4.2 – 16.4) 0.960†
5.4 (4.1 – 11.8) 0.227†
7.8 (3.9 –
14.7) 0.039
† 6.8 (4.5 – 11.3)
0.174 *
Reticulocyte count
(x 109/L)
271 (23.2 – 755.0) 264.0 (161.0 –
455.0) 0.794
† 261.0 (52.0 –
561.0) 0.785
† 233.0 (57.0 –
467.0) 0.191
† NA
0.574 *
Total bilirubin
(mg/dL)
1.7 (0.4 – 6.8) 1.4 (1.0 – 5.1) 0.315†
1.2 (0.6 – 3.2) 0.031†
1.1 (0.4 – 2.4) <0.0001†
NA <0.0001
*10
Unconjugated
bilirubin(mg/dL)
1.4 (0.3 – 6.0) 1.1 (0.8 – 4.2) 0.210†
0.8 (0.4 – 2.6) 0.029†
0.9 (0.3 – 1.8) <0.0001†
NA <0.0001
*10
LDH (IU) 384.0 (164.0 – 938.0) 311.0 (195.0 –
531.0) 0.046
† 200.0 (128.0 –
496.0) 0.0001
† 237.0 (136.0 –
642.0) <0.0001
† NA
<0.0001*11
RBC count (×1012/L) 2.3 (1.0 – 4.0) 2.8 (2.3 – 4.2) 0.005†
4.0 (2.8 – 6.1) <0.0001†
4.0 (2.2 – 6.3) <0.0001†
4.8 (4.0 – 5.5) <0.0001
*12
NB: Significant P values are indicated in bold fonts, †-Mann-Whitney Test, RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb
Hemoglobin concentration, WBC-White blood cell count, LDH-Lactate dehydrogenase, *- Kruskal-Wallis Test with Dunn`s multiple comparison post-hoc
tests with differences in *1= SC vs AA only; *2= (SS vs SBeta+), (SS vs SC), (SS vs AA), (SBeta0 vs AA), (SC vs AA); *3= (SS vs SC), (SS vs AA), (SBeta0 vs AA),
(SC vs AA); *4= (SS vs AA), (SBeta0 vs AA), (SBeta+ vs AA), (SC vs AA); *5= (SS vs AA), (SBeta0 vs AA); *6= (SS vs AA), (SBeta0 vs AA), (SC vs AA); *7= (SS vs
SC), (SS vs AA), (SBeta0 vs SC), (SBeta vs AA), (SBeta+ vs SC), (SBeta+ vs AA); *8=(SS vs SC), (SS vs AA), (SBeta0 vs SC), (SBeta0 vs AA), (SBeta+ vs AA), (SC vs
AA); *9=SS vs AA only; *10=SS vs SC only; *11=(SS vs SBeta+), (SS vs SC); *12=(SS vs SBeta+), (SS vs SC), (SS vs AA), (SBeta0 vs AA).
SS= Sickle cell anemia, SBeta+=Sickle β+- thalassemia, SBeta0=Sickle β0-thalassemia, SC=HbSC disease, AA= Healthy HbAA controls

47
6.2. Comparison of biologic markers across different categories of SCD patients
6.2.1. RBC Microparticles (RMP)
The levels of red blood cell microparticles of the patients were significantly
different across the SCD patients’ groups with HbSS having the highest levels
(p<0.05) Figure 4.
SS SB0 SB+ SC AA0
50000100000150000200000
400000600000800000
1000000
20000003000000
4000000
P1<0.0001
P2=0.0006
P3=0.0002
P4=0.168
RM
P (
even
ts/m
L)
Figure 4: Comparison of red blood cell microparticles across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.
6.2.2. Plasma hemoglobin (PHb)
The levels of plasma hemoglobin of the patients were significantly different across
the SCD patients’ groups in the following order (HbSS>SC>AA) with HbSS having
the highest levels (p<0.05) Figure 5.

48
SS SB0 SB+ SC AA0
20
40
60
80
100
150
200
250
300
P1<0.0001
P2=0.0001
P3=0.015
P4=0.47
Pla
sm
a H
b (
mg
/dL
)
Figure 5: Comparison of plasma hemoglobin across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.
6.2.3. Plasma heme
The levels of plasma heme of the patients were significantly different across the
groups in the following order, (HbSS>SC>AA) with HbSS having the highest
levels (p<0.05) Figure 6.

49
SS SB0 SB+ SC AA0
20
40
60
100
150
200
250
P1<0.0001
P2=0.0025
P3=0.04
P4=0.479
He
me
(µµ µµ
M)
Figure 6: Comparison of heme across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.
6.2.4. Haptoglobin
The levels of plasma haptoglobin of the patients were significantly different
across the groups in the following order, (AA>SC>>SS) with HbSS having the
lowest levels (p<0.05) Figure 7.

50
SS SB0 SB+ SC AA0
500
1000
1500
10000
20000
1000000
2000000
3000000
P1<0.0001
P2=0.038
P3=0.04
P4=0.93
Ha
pto
glo
bin
(n
g\m
l)
Figure 7: Comparison of haptoglobin across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.
6.2.5. Hemopexin
The levels of plasma hemopexin of the patients were significantly different across
the groups in the following order, (AA>SC>>SS) with HbSS patients having the
lowest levels (p<0.05) Figure 8.

51
SS SB0 SB+ SC AA0
100
200
300
400
500
1000
1500
2000
P1<0.0001
P2=0.045
P3=0.80
P4=0.54
He
mo
pe
xin
(µµ µµ
g\m
l)
Figure 8: Comparison of hemopexin across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.

52
6.2.6. Lactate dehydrogenase (LDH)
The levels of LDH of the patients were significantly different across the SCD
patients’ groups with HbSS having the highest levels (p<0.05) Figure 9.
SS SB0 SB+ SC0
200
400
600
800
1000
P1<0.0001
P2=0.0001
P3=0.046
LD
H (
IU/L
)
Figure 9: Comparison of LDH across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC), P2=Mann-Whitney Test (SS vs SB+),
P3= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), and RMP=Red blood cells microparticles.
6.2.7. Total bilirubin
The levels of total serum bilirubin of the patients were significantly different across the
SCD patients` groups with HbSS having the highest levels (p<0.05) Figure 10.

53
SS SB0 SB+ SC0
2
4
6
8
P1<0.0001
P2=0.031
P3=0.315
To
tal b
ilir
ub
in (
mg
/dL
)
Figure 10: Comparison of total serum bilirubin across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC), P2=Mann-Whitney Test (SS vs SB+),
P3= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), and RMP=Red blood cells microparticles.
6.2.8. Unconjugated bilirubin
The levels of unconjugated serum bilirubin of the patients were significantly
different across the SCD patients` groups with HbSS having the highest levels
(p<0.05) Figure 11.

54
SS SB0 SB+ SC0
2
4
6
8
P1<0.0001
P2=0.029
P3=0.210
Un
co
nju
bilir
ub
in (
mg
/dL
)
Figure 11: Comparison of unconjugated bilirubin across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC), P2=Mann-Whitney Test (SS vs SB+),
P3= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), and RMP=Red blood cells microparticles.
6.2.9. Reticulocyte count
There were no significant differences across the patients groups regarding their
reticulocytes counts (p>0.05) Figure 12.

55
SS SB0 SB+ SC0
200
400
600
800
P1=0.574
P2=0.785
P3=0.794
Reti
cu
locyte
co
un
t (X
10
9/L
)
Figure 12: Comparison of reticulocyte count across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC), P2=Mann-Whitney Test (SS vs SB+),
P3= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), and RMP=Red blood cells microparticles.
6.2.10. Red blood cell (RBC) count
The levels of RBC counts of the patients were significantly different across the
groups with HbSS having the lowest levels (p<0.05) Figure 13.

56
SS SB0 SB+ SC AA0
2
4
6
8
P1<0.0001
P2<0.0001
P3<0.0001
P4=0.005
RB
C c
ou
nt
(x 1
01
2/L
)
Figure 13: Comparison of RBC concentration across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.
6.2.11. Hemoglobin concentration (Hb conc)
The levels of RBC counts of the patients were significantly different across the
groups with HbSS having the lowest levels (p<0.05) Figure 14.

57
SS SB0 SB+ SC AA0
5
10
15
20
P1<0.0001
P2<0.0001
P3=0.0009
P4=0.68
Hb
co
nc
(g
\dL
)
Figure 14: Comparison of haemoglobin concentration across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.
6.2.12. Fetal hemoglobin (HbF)
There were significant differences in the levels of HbF between the patients and
controls, the SS patients HbF were significantly higher that of the SC patients and

58
AA respectively p<0.05) with HbSS having the highest levels Figure 15.
SS SB0 SB+ SC AA0
10
20
30
40
P1<0.0001
P2<0.0001
P3=0.554
P4=0.43
Hb
F(%
)
Figure 15: Comparison of fetal hemoglobin across groups
KEY: P1=Kruskal-Wallis ANOVA (SS vs SB0 vs SB+ vs SC vs AA), P2=Mann-Whitney Test (SS vs
SC), P3= Mann-Whitney Test (SS vs SBeta+), P4= Mann-Whitney Test (SS vs SBeta0)
SS= Sickle cell anemia (n=78), SB+=Sickle β+- thalassemia (n=12), SB0=Sickle β0-thalassemia
(n=12), SC=HbSC disease (n=36), AA= Healthy HbAA controls (n=39) and RMP=Red
blood cells microparticles.
6.3. Effects of hydroxyurea on patients’ parameters
None of the HbSC patients was on hydroxyurea treatment. However, 63 (80.7%)
out of the 78 HbSS patients and 12 (50%) of the 24 S-Beta patients comprising
eight (67.0%) S-Beta0, and four (33.0%) S-Beta+, were on hydroxyurea.
HbSS patients on hydroxyurea had significantly higher HbF, MCV, haptoglobin
and hemopexin. On the contrary, they had significantly lower bilirubin, red blood
count, reticulocyte counts, HbS levels, and white blood cell counts. Although the
blood levels of red blood cell microparticles, plasma hemoglobin, and heme were
lower in the HbSS patients on hydroxurea treatment, these values did not reach
statistical significance (Table 2).

59
Table 2: Effects of hydroxyurea treatment on biologic markers of HbSS patients
Parameters HbSS treated with hydroxyurea (N=63)
NO hydroxyurea treatment (N=15)
P values
RMP(events/mL) 160,000.0 (0.0 -17840000.0)
440,000 (0 – 3760000)
0.08
Plasma Hb (mg/dL) 83.9 (28.2 – 169.0) 98.4 (32.6 – 257.5) 0.103
Haptoglobin (ng/mL) 2001.0 (280.0 – 17520)
1013 (543.0 – 8400)
0.023
Heme (µM) 53.3 (15.8 – 206.0) 68.9 (23.5 – 155.6) 0.177
Hemopexin (µg/mL) 686.0 (76.7 – 1937.0)
242.0 (117.0 – 1607)
0.0021
HbF (%) 14.2 (1.7 – 29.5) 5.6 (2.1 – 31.0) 0.014
HbS (%) 76.8 (36.4 – 92.2) 84.7 (54.0 – 92.0) 0.0043
RBC ( million cells/uL)
2.3 (1.0 – 3.7) 2.6 (2.3 – 4.0) 0.006
MCV (fL) 123.7 (85.7 – 147.0) 96.8 (78.6 – 120.0) <0.0001
Total bilirubin (mg/dL)
1.7 (0.6 – 6.1) 3.1 (0.4 – 6.8) 0.0072
Unconjugated bilirubin (mg/dL)
1.3 (0.4 – 5.4) 2.4 (0.3 – 6.0) 0.0073
Hb (g/dL) 8.3 (4.2 – 10.8) 8.5 (7.4 – 12.9) 0.599
Reticulocyte (×109/L) 223.9 (23.2 – 755) 369.6 (76.9 – 548) 0.023
LDH (IU) 384.0 (210.0 – 938.0)
487.0 (164.0 – 683.0)
0.222
Platelet ( X 103/uL) 338.0 (99.0 – 682.0) 372.0 (208.0 – 525.0)
0.368
WBC ( X 103/uL) 5.7 (3.3 – 13.1) 10.3 (8.2 – 14.0) <0.0001
NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test, RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-Hemoglobin concentration, HbS- Hemoglobin S, MCV- Mean corpuscular volume, WBC-White blood cell count, LDH-Lactate dehydrogenase.
For the S-Beta thalassemia patients, the only parameters affected by hydroxyurea
treatment were the RBC and the MCV which were significantly reduced and increased
respectively (Table in Annex 1).

60
6.4. Correlational studies of measured parameters in patients
6.4.1. Red blood cell microparticles
The correlations of RMP with other biologic markers are shown in Figure 16. It showed
that, RMP had positive correlations with total serum bilirubin (r=0.45, p<0.000, figure
16.1), unconjugated bilirubin (r=0.46, p<0.0001, figure 16.2), LDH (r=0.57, p<0.0001),
figure 16.3), plasma hemoglobin (r=0.48, p<0.0001, figure 16.4), heme (r=0.60,
p<0.0001, figure 16.6), and absolute reticulocyte counts (r=0.31, p=0.002, figure 16.8),
of the patients. It also showed a modest significant positive correlation with TRV (r=0.42,
p=<0.0001, figure 16.9), and MCV (r=0.23, p=0.024, figure 16.10). On the contrary, a
modest significant negative correlation was observed between RMP and haptoglobin (r=
-0.228, p=0.039, figure 16.5), hemopexin (r= -0.37, p<0.0001, figure 16.7, red blood cell
count (r= -0.28, p=0.003, figure 16.11) and Hb concentration (r= -0.232, p=0.017, figure
16.12). Also, the HbF of the patients showed a negative correlation with red blood cells
microparticles (r= -0.33, p=0.001), figure 16.13).

61
Figure.16.1
Fig 16.2
r = 0.45, p= 0.000H
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(RM
P)
(eve
nts/
mL)
-1 0 1 2logTotal bilirubin (mg/dL)
logRMPeventsml Fitted values
r=0.46, p= 0.000N
1012
1416
18
log
RB
C m
icro
part
icle
s (R
MP
) (e
vent
s/m
L)
-2 -1 0 1 2log Unconjugated bilirubin (mg/dL)
logRMPeventsml Fitted values

62
Fig 16.3
Fig 16.4
1012
1416
18lo
g R
MP
(ev
ents
/mL)
5 5.5 6 6.5 7log LDH (IU)
logRMPeventsml Fitted values
B r = 0.57 p=0.000
r = 0.48, p = 0.000M
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(RM
P)
(eve
nts/
mL)
3.5 4 4.5 5 5.5log Plasma Hemoglobin (mg/dL)
logRMPeventsml Fitted values

63
Fig 16.5
Fig 16.6
K r= -0.228, p=0.039
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(RM
P)
(eve
nts/
mL)
6 7 8 9 10logHaptoglobin (ng/mL)
logRMPeventsml Fitted values
1012
1416
18lo
g R
MP
(ev
ents
/mL)
3 4 5 6log HemeM (µM)
logRMPeventsml Fitted values
A r = 0.60 p=0.000

64
Fig 16.7
Fig 16.8
r = -0.37, p=0.000
1012
1416
18lo
gRM
Pev
ents
ml (
RM
P)
(eve
nts/
mL)
4 5 6 7 8logHemopexingml (µg/ml)
logRMPeventsml Fitted values
r=0.305, p=0.002A
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(RM
P)
(eve
nts/
mL)
3 4 5 6 7log Absolute Reticulocyte count (x10^9/L)
logRMPeventsml Fitted values

65
Fig 16.9
Fig 16.10
r = 0.42, p=0.000
1012
1416
18lo
gRM
Pev
ents
ml (
RM
P)
(eve
nts/
mL)
.6 .8 1 1.2 1.4 1.6logTRVmsec (m/sec)
logRMPeventsml Fitted values
r = 0.23, p= 0.024G
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(RM
P)
(eve
nts/
mL)
4.2 4.4 4.6 4.8 5log MCV (fl)
logRMPeventsml Fitted values

66
Fig 16.11
Fig 16.12
r = -0.28, p = 0.003F
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(RM
P)
(eve
nts/
mL)
0 .5 1 1.5 2log RBCCount (10^12/L)
logRMPeventsml Fitted values
r = -0.232, p = 0.017I
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(RM
P)
(eve
nts/
mL)
1.5 2 2.5 3log Hb Conc (g/dL)
logRMPeventsml Fitted values

67
Fig 16.13
6.4.2 Plasma haemoglobin
Plasma hemoglobin showed significant positive correlations with total bilirubin (r=0.45,
p<0.0001), unconjugated bilirubin (r=0.43, p<0.0001), LDH (r=0.42, p<0.0001), absolute
reticulocyte counts (r=0.45, p<0.0001), HbS (r=0.357, p=0.0001), of the SCD cohorts.
On the contrary plasma haemoglobin showed significant negative correlations with
haptoglobin (r= -0.35, p <0.0001), modestly with red blood cell count (r= -0.25, p=0.011),
Hb concentration (r= -0.196, p=0.02) and HbF (r= -0.23), p=0.017).
6.4.3 Plasma heme
Heme also showed showed significant positive correlations with total bilirubin (r=0.45,
p<0.0001), unconjugated bilirubin (r=0.44, p<0.0001), (LDH r=0.47, p<0.0001), HbS (r=
0.228, p=0.007), and absolute reticulocyte count (r=0.46, p<0.0001).
It showed significant negative correlations with hemopexin (r= -0.42, p<0.0001), red
blood cell count (r= -0.195, p=0.02) Hb concentration (r= -0.187, p=0.03) and HbF (r= -
0.25, p=0.013).
6.4.4 Plasma hemopexin
1012
1416
18lo
g R
BC
mic
ropa
rtic
les
(eve
nts/
mL)
-1 0 1 2 3 4log HBF (%)
logRMPeventsml Fitted values
r = - 0.33 p=0.001

68
Hemopexin showed modest negative correlations with total bilirubin r= -0.38, p=0.001,
unconjugated bilirubin r= -0.390, p=0.001, reticulocyte count (r= -0.397, p<0.0001),
LDH (r= -0.186, p=0.028) and HbS (r= -0.235, p=0.005).
6.4.5 Plasma haptoglobin
Haptoglobin showed modest negative correlations with total bilirubin r= -0.268, p=0.001,
unconjugated bilirubin r= -0.256, p=0.002, and reticulocyte counts (r= -0.28, p=0.001)
and LDH (r= -0.23, p=0.007).
6.4.6 Tricuspid regurgitation velocity (TRV) and markers of hemolysis
The TRV showed significant positive correlations with RMP (r= 0.42, p<0.0001), heme
(r= 0.25, p=0.004), Total bilirubin (r=0.19, p=0.03), Unconjugated bilirubin (r=0.21,
p=0.019), and LDH (r= 0.32, p=0.001). It however showed no significant correlation with
plasma haemoglobin (r= 0.114, p=0.253) and reticulocyte count (r=0.086, p=0.333). On
the contrary, it showed significant negative correlations with the red blood cell count (r =
-0.43, p<0.0001) and haemoglobin concentration (r= 0.33, p<0.0001).
6.5 Clinical events among the patients
Regarding the acute symptoms or complications of SCD within the last 12 months, 14
(10.1%) patients had acute chest syndrome, and 48 (34.8%) had bone pain crisis.
However, the cumulative and longtime complications found among the patients included:
leg ulcer in 17 (12.3%), stroke 12 (8.6%), proliferative SCD retinopathy 33 (23.9%),
Osteonecrosis 32 (23.2%), elevated tricuspid regurgitation velocity in 53 (38.4%),
priapism in 4 males (3.6%), and albuminuria in 37 (26.8%) out of which 34 (24.6%)
patients were cases of microalbuminuria while the remaining three patients had
macroalbuminuria. In general, the cumulative and longtime complications were more
common among the patients with the HbSS and S-Beta0 genotypes. However, the
occurrence of proliferative SCD associated retinopathy was more among the HbSC
patients (Table 3).

69
Table 3: Clinical events among Brazilian patients
Acute clinical
events and
chronic
complications
(N=138), n (%)
Number
with SS
genotype
N=78
n (%)
Number
with SBeta0
genotype
N=12
n (%)
Number
with SBeta+
genotype
N=12
n (%)
Number
with SC
genotype
N=36
n (%)
Number of
patients (n) and
percentage (%) on
hydroxyurea
therapy per clinical
event and chronic
complications
Bone pain crisis
48 (34.8)
30 (38.4) 5 (41.6) 5 (41.6) 8 (22.2) 32 (66.7)
Osteonecrosis
32 (23.2)
14 (17.9) 1 (8.3) 7 (58.3) 10 (27.7) 15 (46.8)
Acute chest
syndrome
14 (10.1)
12 (15.3) 2 (16.6) 0 (0) 0 (0) 9 (64.2)
Elevated
Tricuspid
regurgitant
velocity (Risk for
pulmonary
hypertension)
53 (38.4)
44 (56.4) 5 (41.6) 1 (8.3) 4 (11.1) 40 (75.5)
Sickle leg ulcer
17 (12.3)
14 (17.9) 3 (25.0) 0 (0) 0 (0) 16 (94.1)
Stroke
12 (8.6)
9 (11.5) 1 (8.3) 2 (16.6) 0 (0) 12 (100)
Proliferative
retinopathy
33 (23.9)
10 (12.8) 0 (0) 1 (8.3) 22 (61.1) 10 (30.3)
Microalbuminuria
34 (24.6)
24 (30.7) 2 (16.6) 2 (16.6) 6 (16.7) 26 (76.5)
Priapism (Male
only N=51)
5 (9.8)
5 (9.8) 0 (0) 0 (0) 0 (0) 5 (100)
NB: SS= Sickle cell anemia, SBeta+=Sickle β+- thalassemia, SBeta0=Sickle β0-thalassemia,
SC=HbSC disease
6.6 Relationships between clinical events and biologic parameters of patients
6.6.1 Acute chest syndrome (ACS)
None of the measured parameters was associated with the occurrence of acute chest
syndrome among the patients (Table 4)

70
Table 4: Associations between acute chest syndrome and biologic markers
Parameters ACS present (N=14) ACS absent (N=124)
P values
RMP(events/mL) 140,000.0 (0.0 -17840000.0)
80,000 (0 – 3760000)
0.3568
Plasma Hb (mg/dL) 99.8 (28.5 – 168.4) 76.8 (31.7 – 257.5) 0.0688
Haptoglobin (ng/mL) 2154.0 (280.0 – 29670) 2275 (279.0 – 11536)
0.826
Heme (µM) 69.8 (15.8 – 177.0) 50.5 (16.0 – 206.0) 0.1309
Hemopexin (µg/mL) 361.1 (76.7 – 1843.0) 648.5 (100.0 – 1937)
0.257
HbF (%) 5.5 (1.7 – 24.6) 9.1 (0.2 – 35.2) 0.969
HbS (%) 69.5 (44.8 – 92.1) 70.3 (23.4 – 92.2) 0.636
RBC ( million cells/uL) 2.9 (1.0 – 4.2) 2.8 (1.2 – 6.3) 0.5319
Total bilirubin (mg/dL) 1.6 (0.6 – 5.4) 1.4 (0.4 – 6.8) 0.2927
Unconj. bilirubin (mg/dL) 1.2 (0.5 – 4.3) 1.1 (0.3 – 6.0) 0.3023
Hb (g/dL) 9.2 (4.2 – 10.8) 9.3 (4.8 – 15.2) 0.599
Reticulocyte (×109/L) 328.0 (23.2 – 755) 225.0 (47.2 – 561) 0.2911
LDH (IU) 334.0 (166.0 – 938.0) 331.0 (128.0 – 907.0)
0.997
Platelet ( X 103/uL) 310.0 (152.0 – 497.0) 339.0 (61.0 – 755) 0.7336
WBC ( X 103/uL) 8.5 (3.2 – 13.1) 6.9 (3.4 – 16.4) 0.3610
NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test, RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-Lactate dehydrogenase.
6.6.2 Vaso occlusive crisis (VOC) / Bone pain crisis
None of the measured parameters was associated with the occurrence of bone pain crisis
among the patients (Table 5)
Table 5: Associations between acute bone pain crisis (VOC) and biologic markers
Parameters VOC present (N=48) VOC absent (N=90) P values
RMP(events/mL) 100,000(0.0 -17840000) 100,000 (0 – 3760000) 0.8594
Plasma Hb (mg/dL) 77.3 (28.2 – 169.0) 78.0 (31.7 – 257.5) 0.884

71
Haptoglobin (ng/mL) 2234.0 (280.0 – 14388) 2164 (279.0 – 29670) 0.5302
Heme (µM) 53.3 (15.8 – 177.0) 50.6 (16.0 – 206.0) 0.5046
Hemopexin (µg/mL) 582.7.1 (76.7 – 1882.0) 677.0 (108.0 – 1937) 0.5046
HbF (%) 6.9 (0.4 – 27.9) 9.4 (0.2 – 35.2) 0.4294
HbS (%) 74.6 (36.4 – 92.1) 69.4 (23.4 – 92.2) 0.174
RBC (million cells/uL)
2.8 (1.0 – 5.6) 2.7 (1.2 – 6.3) 0.8796
Total bilirubin (mg/dL)
1.7 (0.6 – 6.1) 1.3 (0.4 – 6.8) 0.239
Unconj. bilirubin (mg/dL)
1.4 (0.4 – 5.4) 1.0 (0.3 – 6.0) 0.204
Hb (g/dL) 9.4 (4.2 – 15.2) 9.2 (4.8 – 15.2) 0.986
Reticulocyte (×109/L) 252.0 (23.2 – 755) 224.5 (52.0 – 561) 0.7025
LDH (IU) 345.0 (128.0 – 938.0) 325.0 (128.0 – 907.0) 0.5032
Platelet ( X 103/uL) 328.0 (89.0 – 682.0) 338.0 (61.0 – 755) 0.8451
WBC ( X 103/uL) 6.8 (3.2 – 16.4) 7.4 (3.4 – 14.0) 0.6480
NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test, RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-Lactate dehydrogenase.
6.6.3 Leg ulcer
The red blood cell microparticles, heme, LDH, HbS conc, RBC, and Hb conc were
significantly higher in patients who had leg ulcer (p<0.05). No association was
found with the other biologic markers (Table 6).
Table 6: Associations between leg ulcer and biologic markers
Parameters Leg ulcer present (N=17)
No leg ulcer (N=121)
P values
RMP(events/mL) 280,000.0 (40,000.0 -2600000.0)
80,000 (0 – 17840000)
0.0134
Plasma Hb (mg/dL) 81.8 (42.9 – 232.9) 76.8 (28.2– 257.5) 0.3043
Haptoglobin (ng/mL) 2143.0 (279.0 – 7400)
2339 (280.0 – 29670)
0.8202
Heme (µM) 69.2 (33.9 – 206.0) 50.1 (15.8 – 177.0) 0.0079
Hemopexin (µg/mL) 559.3 (108.0 – 978.0)
621.8 (76.0 – 1937) 0.429

72
HbF (%) 12.6 (0.4 – 26.8) 7.5 (0.2 – 35.2) 0.104
HbS (%) 79.4 (46.0 – 96.0) 68.4 (23.4 – 92.2) 0.0041
RBC ( million cells/uL)
2.2 (1.7 – 4.0) 2.9 (1.0 – 6.3) 0.0020
Total bilirubin (mg/dL)
1.5 (0.9 – 5.1) 1.4 (0.4 – 6.8) 0.5605
Unconjugated bilirubin (mg/dL)
1.3 (0.6 – 3.5) 1.1 (0.3 – 6.0) 0.4129
Hb (g/dL) 8.6 (7.0 – 11.3) 9.4 (4.2 – 15.2) 0.0424
Reticulocyte (×109/L) 232.0 (178.0 – 548.0)
231 (23.2 – 755) 0.6812
LDH (IU) 393.5 (210.0 – 711.0)
324.0 (128.0 – 938.0)
0.0129
Platelet ( X 103/uL) 327.5 (99.0 – 592.0)
340.5 (61.0 – 755)
0.6812
WBC ( X 103/uL) 6.0 (3.4 – 10.1) 7.3 (3.2 – 16.4) 0.123 NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test,
RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-
Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-
Lactate dehydrogenase.
6.6.4 Elevated Tricuspid regurgitation velocity (TRV) and risk of pulmonary
hypertension
The red blood cell microparticles, heme, HbF, HbS, and LDH were significantly
higher in patients who had elevated tricuspid regurgitation velocity (TRV) while
their haemoglobin concentration and RBC counts were significantly lower
(p<0.05). No association was found with the other biologic markers (Table 7).
Table 7: Associations between risk for pulmonary hypertension and biologic markers
Parameters Elevated TRV (at risk of pulmonary hypertension) (N=53)
Normal TRV (not at risk of pulmonary hypertension) (N=74)
P values
RMP(events/mL) 200,000.0 (0 -3760000.0)
80,000 (0 – 1800000) 0.0046
Plasma Hb (mg/dL) 79.5 (31.7 – 257.5) 73.1 (28.2– 174.5) 0.5104
Haptoglobin (ng/mL) 2021.0 (279.0 – 11720) 2251 (280.0 – 18180) 0.3196
Heme (µM) 53.4 (16.0 – 206.0) 47.0 (15.8 – 106.0) 0.0375
Hemopexin (µg/mL) 546.8 (76.7 – 1844.0) 668.9 (100.0 – 1937) 0.1620
HbF (%) 12.4 (0.4 – 29.5) 5.5 (0.2 – 35.2) 0.0078
HbS (%) 75.7 (36.4 – 92.0) 62.7 (23.4 – 92.2) 0.0022

73
RBC ( million cells/uL)
2.4 (1.2 – 5.5) 3.2 (1.0 – 6.3) <0.0001
Total bilirubin (mg/dL)
1.5 (0.6 – 6.8) 1.3 (0.4 – 6.0) 0.1404
Unconjugated bilirubin (mg/dL)
1.2 (0.5 – 6.0) 0.9 (0.3 – 5.3) 0.1081
Hb (g/dL) 8.7 (5.1 – 12.8) 9.7 (4.2 – 15.2) 0.0002
Reticulocyte (×109/L) 231.0 (47.2 – 733.0) 213.0 (23.2 – 488.0) 0.370
LDH (IU) 372.0 (128.0 – 668.0) 312.5 (136.0 – 907) 0.0063
Platelet ( X 103/uL) 328.0 (66.0 – 682.0) 344.0 (61.0 – 755) 0.996
WBC ( X 103/uL) 6.6 (3.4 – 16.4) 7.6 (3.3 – 14.7) 0.0747
NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test,
RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-
Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-
Lactate dehydrogenase, TRV-Tricuspid regurgitation velocity, 17 patients with no TRV
records not included.
6.6.5 Stroke
The white blood cell count was associated with the occurrence of stroke among the
patients (Table 8).
Table 8: Associations between stroke and biologic markers
Parameters Stroke present (N=12) No stroke (N=126) P values
RMP(events/mL) 120,000.0 (0 -440000.0) 80,000 (0 – 17840000) 0.7869
Plasma Hb (mg/dL) 87.9 (34.0 – 123.4) 77.8 (28.5– 257.5) 0.3275
Haptoglobin (ng/mL) 2096.0 (1141.0 – 28180) 2176.0(280.0 – 29670) 0.852
Heme (µM) 65.0 (22.9 – 206.0) 58.0 (15.8 – 177.0) 0.7181
Hemopexin (µg/mL) 689.0 (230.0 – 1805.0) 703.0 (76.0 – 1937) 0.838
HbF (%) 14.2 (2.8 – 26.7) 7.5 (0.2 – 35.2) 0.0587
HbS (%) 76.4 (38.2 – 82.0) 69.9 (23.4 – 92.2) 0.559
RBC ( million cells/uL)
2.6 (1.8 – 3.2) 2.9 (1.0 – 6.3) 0.08
Total bilirubin (mg/dL)
1.3 (0.7 – 3.5) 1.5 (0.4 – 6.8) 0.1902
Unconjugated bilirubin (mg/dL)
1.0 (0.5 – 2.9) 1.1 (0.3 – 6.0) 0.323
Hb (g/dL) 8.6 (7.2 – 10.0) 9.4 (4.2 – 15.2) 0.1307
Reticulocyte (×109/L) 210.0 (52.0 – 332.0) 241 (23.2 – 755) 0.1103
LDH (IU) 305.0 (220.0 – 503.0) 339.0 (128.0 – 938.0) 0.803
Platelet ( X 103/uL) 297.5 (174.0 – 755.0) 338.0 (61.0 – 682) 0.7237

74
WBC ( X 103/uL) 5.1 (3.9 – 10.6) 7.3 (3.2 – 16.4) 0.0225
NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test,
RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-
Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-
Lactate dehydrogenase.
6.6.6 Sickle cell disease (SCD) retinopathy
The patients with proliferative SCD retinopathy had significantly lower HbF and higher
RBC counts, and Hb concentration (p<0.05) (Table 9).
Table 9: Associations between proliferative SCD retinopathy and biologic markers
Parameters Retinopathy present (N=33)
No retinopathy (N=105)
P values
RMP(events/mL) 80,000.0 (0 -960000.0) 120,000 (0 – 17840000.0)
0.009
Plasma Hb (mg/dL) 68.1 (31.7 – 232.9) 80. (28.5– 257.5) 0.083
Haptoglobin (ng/mL) 2300.0 (424.0 – 29670) 2140.0(279.0 – 18180) 0.197
Heme (µM) 45.0 (15.8 – 165.0) 53.0 (16.0 – 206.0) 0.026
Hemopexin (µg/mL) 848.0 (114.0 – 1882.0) 540.0 (76.7 – 1937) 0.0084
HbF (%) 1.0 (0.4 – 22.0) 11.2 (0.2 – 35.2) <0.0001
HbS (%) 47.3 (23.4 – 89.5) 74.0 (40.0 – 92.2) <0.0001
RBC (million cells/uL)
3.8 (1.0 – 6.3) 2.6 (1.2 – 6.1) 0.0008
Total bilirubin (mg/dL)
1.2 (0.6 – 3.4) 1.5 (0.4 – 6.8) 0.053
Unconjugated bilirubin (mg/dL)
0.98 (0.4 – 2.9) 1.2 (0.3 – 6.0) 0.05
Hb (g/dL) 10.2 (4.2 – 15.2) 8.8 (4.8 – 13.6) <0.0001
Reticulocyte (×109/L) 245.0 (23.2 – 538.0) 232.5 (47.0 – 755) 0.521
LDH (IU) 294.0 (162.0 – 702.0) 340.0 (128.0 – 938.0) 0.209
Platelet ( X 103/uL) 279.0 (66.0 – 557.0) 346.0 (61.0 – 755) 0.07
WBC ( X 103/uL) 6.8 (3.2 – 14.7) 7.2 (3.4 – 16.4) 0.25
NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test,
RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-
Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-
Lactate dehydrogenase.
6.6.7 Osteonecrosis

75
The RBC counts and hemoglobin concentration of patients who had osteonecrosis were
significantly higher (p=0.0103). No association was found with the other biologic
markers (Table 10).
Table 10: Associations between osteonecrosis and biologic markers
Parameters Osteonecrosis (N=32)
No osteonecrosis (N=106)
P values
RMP(events/mL) 80,000.0 (0 -3760000.0)
120,000 (0 – 17840000)
0.2266
Plasma Hb (mg/dL) 75.7 (31.7 – 257.5) 78.3 (28.5– 239.2) 0.8779
Haptoglobin (ng/mL) 2579.0 (480.0 – 18180)
2020.0(279.0 – 29670)
0.1257
Heme (µM) 49.5 (22.9 – 206.0) 51.0 (15.8 – 177.0) 0.8625
Hemopexin (µg/mL) 683.0 (127.6 – 1930.0)
590.7 (76.7 – 1937) 0.7906
HbF (%) 6.7 (0.4 – 28.0) 9.1 (0.2 – 35.2) 0.4128
HbS (%) 65.3 (38.2 – 92.0) 71.9 (23.4 – 92.2) 0.1986
RBC ( million cells/uL)
3.6 (1.8 – 6.1) 2.6 (1.0 – 6.3) 0.0027
Total bilirubin (mg/dL)
1.3 (0.6 – 6.8) 1.5 (0.4 – 6.1) 0.0911
Unconjugated bilirubin (mg/dL)
1.1 (0.4 – 6.0) 1.2 (0.3 – 5.4) 0.126
Hb (g/dL) 10.2 (7.5 – 15.2) 8.9 (4.2 – 15.2) 0.0041
Reticulocyte (×109/L) 214.0 (52.0 – 561.0) 235.7 (23.2 – 755) 0.4186
LDH (IU) 309.5 (128.0 – 907.0)
339.5 (136.0 – 938.0)
0.139
Platelet ( X 103/uL) 352.0 (61.0 – 557.0) 329.0 (66.0 – 755) 0.992
WBC ( X 103/uL) 5.9 (4.0 – 14.7) 7.2 (3.3 – 16.4) 0.773
NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test,
RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-
Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-
Lactate dehydrogenase.

76
6.6.8 Priapism
None of the measured parameters was associated with the occurrence of priapism among
the patients (Table 10)
Table 11: Associations between priapism and biologic markers
Parameters Priapism (N=5) No priapism (N=46) P values
RMP(events/mL) 200,000 (40,000 -1720000) 120,000 (0 – 17840000) 0.4435
Plasma Hb (mg/dL) 83.6 (51.2 – 169.0) 83.0 (32.2– 232.9) 0.703
Haptoglobin (ng/mL) 2596.0 (1141.0 – 17180) 2339.0(280.0 – 18180) 0.230
Heme (µM) 50.0 (21.8 – 102.0) 51.9 (15.8 – 206.0) 0.646
Hemopexin (µg/mL) 709.0 (100 – 1930.0) 457.0 (116.0 – 1937) 0.1887
HbF (%) 15.7 (6.3 – 17.2) 5.6 (0.4 – 29.5) 0.078
HbS (%) 76.3 (74.3 – 84.1) 70.9 (36.4 – 92.2) 0.387
RBC ( million cells/uL)
2.3 (1.3 – 3.0) 2.7 (1.0 – 6.3) 0.154
Total bilirubin (mg/dL)
1.4 (1.2 – 3.4) 1.7 (0.7 – 5.4) 0.657
Unconjugated bilirubin (mg/dL)
1.2 (0.8 – 2.9) 1.3 (0.5 – 4.3) 0.658
Hb (g/dL) 8.9 (4.9 – 10.0) 9.4 (4.2 – 15.2) 0.366
Reticulocyte (×109/L) 225.9 (195.9 – 331.0) 250.5 (23.2 – 755) 0.7157
LDH (IU) 469.0 (287.0 – 563.0) 369.0 (128.0 – 938.0) 0.4284
Platelet ( X 103/uL) 266.0 (170.0 – 369.0) 300.0 (61.0 – 682) 0.5368
WBC ( X 103/uL) 5.6 (4.4 – 7.8) 5.9 (3.3 – 13.8) 0.5161
NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test,
RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-
Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-
Lactate dehydrogenase.

77
6.6.9 Microalbuminuria
Higher heme level was associated with the occurrence of microalbuminuria among the
patients (Table 12).
Table 12: Associations between microalbuminuria and biologic markers
Parameters Microalbuminuria (N=34)
Microalbuminuria absent (N=101)
P values
RMP(events/mL) 160,000.0 (0 -1960000.0) 80,000 (0 – 17840000) 0.1097
Plasma Hb (mg/dL) 84.0 (28.2 – 232.5) 71.9 (31.7– 257.5) 0.1676
Haptoglobin (ng/mL) 2021.0 (280.0 – 29670) 2377.0(279.0 – 18180) 0.445
Heme (µM) 60.7 (21.9 – 206.0) 48.7 (15.8 – 177.0) 0.0410
Hemopexin (µg/mL) 607.0 (76.7 – 1843.0) 680.0 (100 – 1937) 0.8206
HbF (%) 11.7 (0.4 – 35.2) 8.2 (0.2 – 31.0) 0.387
HbS (%) 75.7 (23.4 – 92.0) 69.0 (38.2 – 92.2) 0.2383
RBC ( million cells/uL)
2.6 (1.2 – 5.0) 2.8 (1.0 – 6.3) 0.3410
Total bilirubin (mg/dL)
1.5 (0.6 – 6.1) 1.4 (0.4 – 6.8) 0.8205
Unconjugated bilirubin (mg/dL)
1.2 (0.4 – 5.4) 1.1 (0.3 – 6.0) 0.8095
Hb (g/dL) 9.1 (5.1 – 13.6) 9.3 (4.2 – 15.2) 0.528
Reticulocyte (×109/L) 225.0 (99.7 – 668.0) 232.0 (23.2 – 755) 0.7479
LDH (IU) 410.0 (180.0 – 702.0) 359 (128.0 – 938.0) 0.1391
Platelet ( X 103/uL) 356.0 (99.0 – 557.0) 330.0 (61.0 – 755) 0.368
WBC ( X 103/uL) 7.1 (3.7 – 14.7) 7.2 (3.2 – 16.4) 0.9153
NB: NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test,
RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-
Hemoglobin concentration, HbS- Hemoglobin S, WBC-White blood cell count, LDH-
Lactate dehydrogenase.

78
7. GENETIC STUDIES AMONG NIGERIAN COHORTS
The Nigerian cohorts consisted of 110 SCD patients made up of 102 SS, and 8 HbSC. In
addition, there were 68 controls in the study and they were made up of 22 AS and 46 AA.
7.1. Clinical events
Sixty two (60.7%) of the SS and five (62.5%) HbSC had bone pain crisis in the preceding
12 months. The longtime complications encountered among the SS cohorts included:
stroke five (4.9%), osteonecrosis five (4.9%), gallstone 6 (5.9%), priapism five (4.9%),
and leg ulcer six (5.9%). Also, one (12.5%) SC patient had stroke.
7.2. Haplotypes (β globin chain)
The βs-haplotypes was successfully determined in 107 patients (101 SS & 6 SC) and 64
controls. Four βs-haplotypes were found. Homozygous Benin haplotype (Benin/Benin)
was predominant and found in 94 (93%) patients and all the 19 (100%) HbAS controls.
The Benin/Cameroun, Benin/Bantu and Benin/Arab haplotypes were found in 4, 2 and 1
patients respectively (Table 13).
7.3. Glucose 6 phosphatase dehydrogenase (G6PD) deficiency
Mutation for G6PD deficiency was successfully determined in 107 patients and 64
controls. The African variant of G6PD deficiency (202G>A), and (A376G) was found in
24(22.4%) patients, 8 (42.1%) HbAS, and 6 (13.3%) HbAA controls. None of the
participants had the (563C>T), (A542T), and (G680T) mutations (Table 13).
Table 13: Distribution of βs-haplotypes and G6PD deficiency among Nigerian cohorts
Parameter
SCA (N=101)
n (%)
SC (N=6) n (%)
SCD (SCA+SC)
N=107 n (%)
AS (N=19) n (%)
AA (N=45) n (%)
βs-haplotypes
Benin/Benin 94 (93) 5 (83.3) 99 (92.5) 19 (100) NA
Benin/Cameroun 4 (4) 0 (0) 4 (3.7) 0 (0) NA
Benin/Bantu 2 (2) 1 (1) 3 (2.8) 0 (0) NA
Benin/Arab 1 (1) 0 (0) 1 (1) 0 (0) NA
G6PD
deficiency
21 (20.7) 3 (50.0) 24 (22.4) 8 (42.1) 6 (13.3)
NB: NA=Not applicable

79
Figure 17: Ethidium bromide-stained 1.5% agarose gel showing restriction analysis with
Nla III of PCR products related to G6PD African mutation (G202A – rs1050828).
Lanes: M: 100 bp Molecular Marker; 1: Not digested PCR (527 bp); 2 and 3: female
heterozygote samples (123, 151, 153 and 376 bp); 4, 5, 7 8 and 9: Hemi or Homozygotes
normal samples (151 and 376 bp); 6 and 10: Hemi or Homozygotes Mutant samples (123,
151 and 253 bp).
7.3.1. Influence of G6PD deficiency on biologic markers of patients
The G6PD deficiency did not significantly influence any marker in the patients
(Table 14).
Table 14 : Associations between G6PD deficiency and biologic markers of Nigerian SS cohorts
Parameters G6PD deficient (N=21)
No G6PD deficiency (N =80)
P value
Total bilirubin (mg/dL) 1.7 (0.5 – 7.7) 2.0 (0.4 – 8.1) 0.10
Unconj. bilirubin (mg/dL)
0.7 (0.1 – 6.3) 1.1 (0.1 – 6.2) 0.315
AST (IU) 41.0 (9.0 – 89.0) 45.0 (7.0 – 89.0) 0.373
LDH (IU) 904.0 (322.0 – 1489.0) 780.0 (197.0 – 1860.0) 0.223
RBC ( million cells/uL) 3.0 (2.2 – 3.9) 2.8 (1.8 – 4.8) 0.06
Hb (g/dL) 7.9 (6.5 – 9.4) 7.5 (6.2 – 11.0) 0.392
MCV (fL) 79.2 (60.0 – 95.0) 82.0 (55.9 – 115.0) 0.066
WBC ( X 103/uL) 12.5 (6.1 – 27.3) 13.2 (6.2 – 29.3) 0.340
Platelet ( X 103/uL) 334.0 (133.0 -601.0) 374.0 (108.0 – 832.0) 0.09
HbF (%) 8.9 (2.3 – 19.1) 9.6 (0.9 – 32.3) 0.376
HbS (%) 81.7 (68.6 – 87.6) 78.1 (44.0 – 92.0) 0.09 NB: Test statistics= Mann-Whitney test, RMP-Red blood cell microparticle, HbF-Fetal
Hemoglobin, RBC-Red blood cell, Hb-Hemoglobin concentration, HbS- Hemoglobin S, WBC-
White blood cell count, LDH-Lactate dehydrogenase

80
7.3.2. Association between G6PD deficiency and clinical events
Presence of G6PD deficiency did not influence the clinical events of patients (Table
15)
Table 15: Co-inheritance of sickle cell anemia with G6PD deficiency and SS clinical events
Clinical events Patients with G6PD
deficiency (N=21)
Patients without G6PD
deficiency (N=80)
P value
Bone pain crisis
(per Year)
Range (0 –6 )
Median 1.5
Range (0 –6 )
Median 1
0.2013†
Blood
Transfusion Per
year
Range (0 – 1)
Median 0
Range (0 – 2)
Median 0
0.299†
Admission Per
year
Range (0 – 6)
Median 2
Range (0 – 8)
Median 1
0.08†
Stroke 2 3 0.60*
Osteonecrosis 0 5 0.324*
Leg ulcer 2 5 0.645*
Gallstone 1 5 1.000*
Priapism n=67 (N=19)
2
(N=48)
2
0.606*
NB- Significant p values are in bold fonts, †= Mann-Whitney Test, *=Fisher`s exact test
7.4. UGT1A1 genotypes (polymorphism)
UGT1A1 genotyping was successfully determined in 107 patients (101-SS &
6HbSC), and 64 controls. Four (TA)n alleles: (TA)5, 6, 7, and 8 were found with gene
frequencies of 0.11, 0.43, 0.41 and 0.05 respectively. The alleles were associated with
10 genotypes:TA5/5, 5/6, 5/7, 5/8, 6/6, 6/7, 6/8, 7/7, 7/8, 8/8. (Figure 18).
The low (TA) 7/7, 7/8, 8/8), intermediate (TA) 6/7, 6/8), and High (TA) 5/5, 5/6, 5/7,
5/8, 6/6,) activity genotypes were found in 38 (22.2%), 63 (38.2%), and 70 (40.9%) of
the participants respectively. Among the SS group, the low activity genotypes were
found in 25 (24.7%) compared to 10 (15.6%) of the controls (P=0.1773). Homozygous
(TA)n TA7/7 was found in 22 (21.7%) of SS compared to 5 (7.8%) controls p=0.018,
(Table16)

81
Table 16: Allele and genotype frequencies of UGT1A1 promoter polymorphism among
participants
Variables SS
N=101
SC
N=6
AS
N=19
AA
N=45
Allelotypes Freq n (%) Freq n (%) Freq n (%) Freq n (%) (TA) 5 18 (11.7) 2 (16.6) 2 (6.7) 10 (12.5) (TA)6 67 (43.5) 3 (25.0) 16 (53.3) 28 (35.0) (TA)7 61 (39.6) 7 (58.4) 10 (33.3) 37 (46.2) (TA)8 8 (5.2) 0 (0) 2 (6.7) 5 (6.3) UGT1A1 Genotypes SS (N=101) SC (N=6) AS (N=19) AA (N=45) Genotypes Freq n (%) Freq n (%) Freq n (%) Freq n (%) TA5/5 0 (0) 0 (0) 0 (0) 1 (2.2) TA5/6 9 (8.9) 1 (16.6) 0 (0) 1 (2.2) TA5/7 6 (6.0) 1 (16.6) 1 (5.2) 8 (17.7) TA5/8 3(2.9) 0 (0) 0 (0) 0 (0) TA6/6 25 (24.7) 1 (16.6) 8 (42.1) 5 (11.1) TA6/7 31 (30.7) 0 (0) 7 (36.8) 21 (46.7) TA6/8 2 (2.0) 0 (0) 1 (5.2) 1 (2.2) TA7/7 22 (21.7) 3 (50.0) 1 (5.2) 4 (8.9) TA7/8 2 (2.0) 0 (0) 1 (5.2) 4 (8.9) TA8/8 1 (1.0) 0 (0) 0 (0) 0 (0) SCA (N=101) SC (N=6) AS (N=19) AA (N=45) UGT1A1 Genotypes
by degree of
Activity
Freq n (%) Freq n (%) Freq n (%) Freq n (%)
Low-Activity genotypes TA (7/7, 7/8, 8/8)
25 (24.7) 3 (50.0) 2 (10.5) 8 (17.8)
Intermediate-Activity genotypes (TA6/7, TA6/8)
33 (32.7) 0 (0) 8 (42.1) 22 (48.9)
High-Activity genotypes TA5/5 , TA5/6, TA5/7, TA5/8, TA 6/6
43 (42.6) 3 (50.0) 9 (47.4) 15 (33.3)

82
Figure 18: UGT1A1 promoter genotypes found among Nigerian groups. A: TA5/TA5; B: TA5/TA6; C: TA5/TA7; D: TA5/TA8; E: TA6/TA6; F: TA6/TA7; G: TA6/TA8; H: TA7/TA7; I: TA7/TA8; J: TA8/TA8.

83
7.4.1. Comparison of serum bilirubin and other laboratory parameters between
patients (SS) and controls
There were significant differences between the patients and controls in all laboratory
parameters p<0.0001 respectively. (Table 17)
Table 17: Comparison of laboratory markers between patients and controls
Parameters SCA (N=101) Median (Range)
Controls (N=64) Median (Range)
Test statistics P value
HbF (%) 8.4 (0.9 – 32.3) 0.9 (0 – 5.8)
p˂0.0001
LDH (IU/L) 771 (197 – 1860)
345(150 – 840) p˂0.0001
Hb Conc (g/dL) 7.4 (6.3 – 11.2) 11.6 (7.8 – 14.8)
p˂0.0001
WBC ( X 103/uL) 12.6 (6.1 – 29.3) 6.6 (4.5 – 14.4)
p˂0.0001
Platelet ( X 103/uL) 343 (118 – 832)
278 (108 – 591)
p˂0.0001
Total Bilirubin (mg/dL)
1.8 (0.42– 8.1)
0.4 (0.1– 2.2)
p˂0.0001
Unconjugated bilirubin (mg/dL)
0.8 (0.1 -6.3) 0.2 (0.03 -0.8) p˂0.0001
AST (IU/L) 42 (17 – 89)
27 (6 – 45) p˂0.0001
ALT (IU/L) 20 (4 – 77)
10 (4 – 51) p˂0.0001
NB:Test statistics =Mann-Whitney , Significant P values are indicated in bold fonts
7.4.2. Effects of UGT1A1 genotype on serum bilirubin and other laboratory
parameters of patients
Both the total bilirubin and unconjugated bilirubin levels showed a trimodal pattern
across the UGT1A1 genotype subgroups with the low affinity genotype group
having the highest levels of serum bilirubin (p<0.0001). The LDH also showed this
trimodal pattern (p=0.0386). However, this was not demonstrated by the other
remaining parameters (Table 18).

84
Table 18: Influence of UGT1A1 genotype on laboratory parameters of SS cohort
Parameter a. Low activity UGT1A1 genotypes
N=25
b. Intermediate activity UGT1A1
genotypes N=33
c. High activity UGT1A1 genotypes
N=43
P1 values
a vs (b+c)
Anova P2 values
(a vs b vs c)
Biochemical and haematologic
Median (Range) Median (Range) Median (Range)
Total Bilirubin (mg/dl)
2.8 (1.2 -8.1) 1.7 (0.8 -4.7) 1.4 (0.4 -3.8) <0.0001* <0.0001**
Unconjugated Bilirubin (mg/dl)
1.8 (0.6 – 6.3) 0.8 (0.1 -3.6) 0.6 (0.1-2.8) <0.0001* <0.0001**
LDH (IU/L) 987(296-1860) 705 (233 -1489) 681 (197-1417) 0.0150* 0.0386**
AST(IU/L) 46 (18 -89) 41 (18 - 89) 37 (17 -89) 0.136* 0.3169**
ALT (IU/L) 25 (4-65) 18 (7- 58) 19 (4 -77) 0.1431* 0.279**
Hb conc (g/dl) 7.3 (6.3 -10) 7.5 (6.3 -11.2) 7.4(6.4 -10) 0.59*65* 0.822**
MCV(fl) 80.6 (66.9 -104.1) 82.3 (60.3 -101.5) 80.9 (55.9 -115) 0.9752* 0.8469**
RBC (x 1012/L) 2.7 (1.9 -4.1) 2.6 (2 -4.7) 2.9 (1.8 -4.8) 0.8427* 0.4438**
WBC (x 109/L) 13 (8.5 -26) 10.5 (6.1 -27) 13.3 (6.4 -29) 0.4814* 0.2997**
Platelet (x 109/L)
367 (118 -771) 342 (167 -593) 358 (118 -832) 0.4717* 0.7494**
HbF (%) 9.7 (1.3 -20.6) 7.3 (1.7 -24.4) 10.4 (0.9 -32) 0.521* 0.7466**
*=Mann-Whitney Test, **=Kruskal-Wallis one way analysis of variance, Significant p
values are indicated in bold fonts.
7.4.3. Effects of UG1TA1 genotype on clinical events
None of the HbSC patients had gallstones. Among the SS group, asymptomatic
gallstones were found in 6 (5.9%) patients. Patients who had gallstones significantly
belonged to the subgroup with low activity genotypes 5 (20%) vs 1(1.3%)
p=0.0024, (Table 19). These were 2 females and 4 males. The two females were
aged 10 and 13 years. The males consisted of a 16-year-old boy with three others
aged 10, 13, and 15 years respectively. Four of them had TA 7/7 genotypes, one
TA 7/8, and TA 6/7 each.

85
Table 19: Influence of UGT1A1 genotype on clinical events of SS patients
Clinical events a. Low activity
UGT1A1 genotypes N=25
b. Intermediate activity UGT1A1 genotypes
N=33
c. High activity UGT1A1 genotypes
N=43 P value
VOC per year 2 (0-6) 0 (0-6) 0 (0-6) 0.09*
Overt Stroke 1 2 2 0.9312†
No overt stroke 24 31 41
Osteonecrosis 1 1 3 0.711†
No osteonecrosis
24 32 40
Leg ulcer 0 1 5 0.102†
No Leg ulcer 25 32 38
Gallstones 5 1 0 0.0024†
No Gallstone 20 32 43
Priapism (Male only, N=67)
Priapism 1 2 2 0.927†
No Priapism 16 26 20
*=Mann-Whitney Test, †=Chi-Square Test, Significant p values are indicated in bold
fonts.
7.4.4. Comparison of laboratory parameters between patients with and without
gallstones.
There were significant differences between the serum bilirubin and HbF levels of
patients with gallstones when compared with those without gallstone in general. No
difference was observed in the LDH and age of the two groups. Also, when those with
gallstones were compared with age- and sex-matched peers within the same UGT1A1
genotype subgroup, only serum bilirubin and HbF showed significant differences
between the two groups (Table 20).

86
Table 20: Comparison of parameters in patients with and without gallstones
Parameter Patients with gallstones
(N=6) Median (Range)
Patients without gallstones (N=95) Median (Range)
P value
Total Bilirubin (mg/dl)
6.4 (2.8 -8.1) 1.8 (0.4 -6.7) 0.0001*
Unconjugated Bilirubin (mg/dl)
4.7 (0.9 -6.3) 0.79 (0.1 -5) 0.0007*
LDH (IU/L) 1004 (592 -1860) 794 (197 -1750) 0.1263*
HbF (%) 4.7 (1.3 -6.8) 10.2 (0.9 -32) 0.0107*
Hb (g/dl) 7.1 (6.3 -8.8) 7.5 (6.2 -10) 0.4210*
Age in years 11.5 (8 -16) 9 (2-21) 0.1368*
Sex
Male (n=66) 4 62 1.000†
Female (n=35) 2 33
Parameter Patients with gallstones (N=6)
Median (Range)
Matched peers without gallstones within same
UGT1A1 genotype activity group N=10
Median (Range)
P value
Total Bilirubin (mg/dl)
6.4 (2.8 -8.1) 2.2 (1.9- 3.2) 0.0023*
Unconjugated Bilirubin (mg/dl)
4.7 (0.9 -6.3) 1.2 (1.0 -2.0) 0.0020*
LDH (IU/L) 1004 (592 -1860) 890 (340 -1603) 0.628*
HbF (%) 4.7 (1.3 -6.8) 14.7 (4.2 -17.9) 0.022*
Hb (g/dl) 7.1 (6.3 -8.8) 8.0 (6.5 – 8.9) 0.137* NB Significant P values are indicated in bold fonts, *=Mann-Whitney test, †=Fisher`s
7.4.5. Relationship between serum bilirubin and other parameters of patients
The total serum bilirubin correlated positively with the age of the patients ( r =0.238,
p=0.013), and their LDH levels (r = 0.218, p=0.028). Conversely, it showed a
negative correlation with the HbF levels (r = -0.210, p= 0.035). No significant
correlation was found between the total serum bilirubin and other biomarkers.

87
7.4.5. Relationship between UGT1A1 genotypes and other parameters by
multivariate analysis.
The unconjugated bilirubin was significantly associated with the low activity
UGT1A1 genotypes (Adjusted Odd Ratio (1.08), 95% Confidence interval
(1.034768 – 1.127873), P=0.000). Also, significant association was found with the
total bilirubin when it was used in place of unconjugated bilirubin in the logistic
regression model (Adjusted Odd Ratio (1.05), 95% Confidence interval (1.029172
– 1.089832), P=0.000).
7.5. Alpha Thalassemia trait
Of the 164 samples successfully studied for Alpha thalassemia, Alpha thalassemia
trait was found in 41 SS, one HbSC, and 24 controls. All were due to 3.7 κb α-globin
gene deletion. There was one case of triplication among the SS.
Figure 19: Ethidium bromide-stained 1.2% agarose gel showing α 3.7 deletion by GAP-
PCR.
Lane M: GeneRuler™ 1Kb DNA Ladder; 1: Homozygote sample for 3.7
alpha globin gene deletion (1.9 Kb fragment); 2, 4, 5 and 7: Homozygotes
samples for normal alpha globin gene (2.1 Kb fragment); 3 and 6:
Heterozygotes samples (2.1 Kb and 1.9 Kb fragments)

88
7.5.1. Comparison of biodata and gene frequencies between patients and
controls
The patients consisted of 66 males and 34 females with a median age of 8.5, range
2 – 21 years. The controls were made up of 22 individuals with HbAS and 41 with
HbAA, median age of 8, range 2- 18years. They consisted of 36 males and 27
females. The patients had been on follow up for a median of 4 years, range 1.5 -
14years. There were no differences in the socio-biographic data of patients and
controls (Table 21).
Table 21: Biodata and frequencies of alpha thalassemia alleles
Parameters SCA (SS) N=100 n (%)
AS N=22 n (%)
AA N=41 n (%)
Chi-square, degree of freedom
ᵡ2, df
P value
Age in years Median (Range)
8.5 (2-21) 9 (3 – 17) 8.5 (2 – 18) NA 0.888a
Sex
Male Female
66 (66.0) 34 (34.0)
13 (59.0) 9 (41.0)
23 (56.0) 18 (44.0)
1.350, 2 0.509b
Social Class
Lower Middle Upper
48 (48.0) 44 (44.0) 8 (8.0)
12 (54.5) 8 (36.4) 2 (9.1)
20 (48.8) 18 (43.9) 3 (7.3)
0.4714, 4 0.9762
b
Alpha thalassemia present
41 (41.0) 8 (36.0) 16 (39.0) 0.2866, 2
0.866 b Alpha thalassemia absent
58 (58.0) 13 (62.0) 25 (61.0)
α-globin gene
deletion
SCA (SS) N=100 n (%)
AS N=22 n (%)
AA N=41 n (%)
αα /-α3.7 34 (34.0) 8(36.0) 16 (39.0) 0.327, 2 0.849 b
-α3.7/-α3.7 7 (7.0) 0 (0) 0 (0) NA 0.043*
-α3.7/-α3.7/-α3.7 1 (1.0) 0 (0) 0 (0) NA
Allele frequency Total chromosome
N=200 n(frequency)
Total chromosome
N=44 n(frequency)
Total chromosome
N=82 n(frequency)
Αα 150 (0.75) 36 (0.82) 66 (0.80) 1.590, 2 0.451 b
-α 49 (0.25) 8 (0.18) 16 (0.20) 0.822, 2 0.662 b

89
Ααα 1 (0.005) 0 (0.0) 0 (0.0) NA
NB: a=Kruskal-Wallis test, b= Chi-square test, *=Fisher`s exact test, NA= Not applicable, One
case of Triplicaion not considered as alpha thalassemia, Significant p value is in bold font.
7.5.2. Allele frequency of alpha thalassemia among SS patients and controls
Alpha-thal trait (3.7 κb α-globin gene deletion) was found in 41 (41.0%) patients;
34 with heterozygous deletion (αα/– α3.7), and 7 with homozygous deletion (-α3.7/-
α3.7), while 58 (58.0%) patients had normal genotype (αα/αα). Twenty-four controls
comprising 8 (36.0%) HbAS, and 16 (39.0%) HbAA had α-thal trait and these were
all heterozygous (αα/– α3.7). Also, 38 controls made up of 13 (62.0%) HbAS and 25
(61.0%) HbAA had normal genotype (αα/αα). Of the 200 patients’ chromosomes
analysed, 150 were αα, 49 were –α, and one was ααα, thus giving gene frequencies
of 0.75 (αα), 0.25 (-α), and 0.005 (ααα) respectively. Similarly, the gene frequencies
among the controls were HbAS - 0.82 (αα), 0.18 (-α) and HbAA- 0.80 (αα), 0.20 (-
α) respectively, with no gene triplication (ααα) detected and these were not
significantly different from the frequencies among the patients (Table 21). Taken
together, the prevalence of α-thal was not different across the groups (SCA 42
(42%) vs HbAS 8 (36.0) vs HbAA 16 (39.0), ᵡ2=0.2866, df=2, p=0.866).
7.5.3. Comparison of laboratory parameters between SS patients and controls
There were significant differences between the patients and controls in all
laboratory parameters p<0.05 except mean corpuscular hemoglobin (MCH). (Table
22)
Table 22: Laboratory parameters of patients and controls
Biomarkers HbAA N=41 Median (Range)
HbAS N=22 Median (Range)
HbSS N=100 Median (Range)
P value
Hb (g/dl) 11.5 (7.8 – 13) 11.6 (8 – 14) 7.5 (6.2 – 11.2) ˂0.0001
MCV (fL) 89.4 (66.4 – 102) 79.6 (60.4 – 74.7)
81.1 (60 – 115) 0.0125
RBC(million cells/uL)
4.5 (3.8 – 5.5) 4.6 (2.3 – 6.0) 2.8 (1.8 – 4.8) ˂0.0001
WBC (x 103/uL) 6.3 (4.5 – 14.4) 6.5 (4.5 -12.5) 13.1(6.1 – 29.30) ˂0.0001
Platelet (x 103/uL) 244 (117 – 514) 275 (125 – 578) 361(108 – 832) 0.0004
HbF (%) 0.75 (0 – 2.1) 0.7 (0.2 – 4.7) 9.3 (0.9 – 32.3) ˂0.0001
HbA2 (%) 2.9 (0.8 – 3.6) 3.6 (0.5 – 4.6) 1.5 (0.2 – 4.0) ˂0.0001

90
MCH (pg) 24.4 (17.6 – 27.9)
25.2 ( 18.2 – 29 )
25.3 (16 – 34) 0.260
Total bilirubin (mg/dl)
0.43 (0.1 – 0.45) 0.45 (0.25 – 1) 1.80 (0.5 – 8.1) ˂0.0001
AST (IU/L) 19 (6 – 64) 27 (8 – 75) 43 (12 – 89) ˂0.0001
LDH (IU/L) 360 (150 – 861) 375 (179 – 993) 789.3 (179 – 1860)
˂0.0001
NB- Significant p values are in bold fonts, Test statistics = Kruskal-Wallis ANOVA, Hb-Hemoglobin concentration, RBC-Red blood cells, MCV-Mean corpuscular volume, WBC-White blood cells count, HbF- Fetal hemoglobin, MCH- mean corpuscular hemoglobin, AST-Aspartate transaminase, LDH-Lactate dehydrogenase
7.5.4. Effects of alpha thalassemia on hematological indices and other
laboratory parameters among patients
Co-inheritance of α-thal was significantly associated with higher hemoglobin
concentration (Hb), red blood cell count (RBC) and HbA2 level. On the contrary, it
was associated with lower mean corpuscular volume (MCV) and mean corpuscular
hemoglobin (MCH), while the white blood cell count (WBC) was significantly
lower in patients with homozygous 3.7 κb α-globin gene deletion compared to the
two other groups. No significant differences were observed across α-thal genotypes
in the other laboratory parameters (Table 23).
Table 23: Alpha thalassemia Alleles and laboratory parameters
Biomarkers Alpha thalassemia with Heterozygous deletion N=34 Median (Range)
Alpha thalassemia with Homozygous deletion N=7 Median (Range)
SS with no Alpha Thalassemia Trait N=58 Median (Range)
P Value
Hb (g/dl) 7.6 (6.3-11.2) 8.2 (7.6-10) 7.2 (6.2-11) 0.0199
MCV (fL) 78 (66.9 -94) 74 (60.3 – 101) 84 (56 – 115) 0.0025
RBC (million cells/uL)
2.8 (2.15 -3.9) 3.1 (2.7 – 4.1) 2.7 (1.8 – 4.8) 0.0264
WBC (x 103/uL) 14.7 (6.4 – 26.2) 7.8 (6.1 – 13.2) 13.3 (6.1 – 29.3) 0.0353
Platelet (x 103/uL)
358 (108 -674) 334 (158 -444) 371 (118 -832) 0.2156
HbF (%) 8.8 (0.6 – 28.5) 13.1 (3.7 – 17.5) 10.7 (2.5 – 32.3) 0.1364 HbA2 (%) 1.7 (0.3 – 3.8) 2.8 (1.5 – 4.0) 1.5 (0.2 – 3.1) 0.0002
MCH (pg) 24.5 (18.6 – 30.6)
24.4 (15.7 – 27.1)
26 (15.9 – 34) 0.0021
Total Bilirubin (mg/dl)
2.1 (0.43 – 7.7) 1.8 (1.03 – 8.1) 1.8 (0.8 – 5.2) 0.729
AST (IU/L) 58 (12 – 89) 40 (22 – 89) 43 (7 – 89) 0.3974 LDH (IU/L) 865 (215 –
1860) 771 (705 – 986) 881 (197 – 1681) 0.6469

91
NB- Significant p values are in bold fonts, Test statistics= Kruskal-Wallis ANOVA, Hb-Hemoglobin concentration, RBC-Red blood cells, MCV-Mean corpuscular volume, WBC-White blood cells count, HbF- Fetal hemoglobin, MCH- mean corpuscular hemoglobin, AST-Aspartate transaminase, LDH-Lactate dehydrogenase.
7.5.4. Effects of alpha thalassemia on clinical events among SS patients
Sixty-one (61.0%) patients had bone pain episodes in the preceding one year, And, 6
(6.0%), 5 (5.0%) each had overt stroke and osteonecrosis while 5 (7.5%) males had
priapism as complications of their disease.
The rate of painful crisis was higher in patients with α-thal compared to those without it
(p<0.0001). However, the presence of α-thal protected against leg ulcer as none of the six
patients with leg ulcer had α-thal vs 6 (10.3%), p=0.0384. The leg ulcers were completely
healed in three (50%) patients after a median duration of five months (range 3 – 6
months), and yet to heal in the remaining three patients, two of whom are having
recrudescence of their ulcers. This gives a prevalence of active ulcer as 3%. One of the
two with active ulcers, a 21-year-old also had overt stroke. The ulcers were mostly located
on the ankles in 5 (83.3%) and right big toe in 1 (16.7%). There was a preceding history
of trauma in 4 (66.7%) and this included a case of traditional scarifications for local
therapeutic purposes. No significant association was found in relation to other clinical
events with respect to the presence or absence of α-thal (Table 24).
Table 24: Co-inheritance of sickle cell anemia with Alpha Thalassemia and clinical events
Clinical events Patients with Alpha Thalassemia (N=41)
Patients without Alpha Thalassemia (N=58)
P value
Bone pain crisis per Year
Range (0 –6) Median 3
Range (0 –6) Median 1
˂0.0001†
Stroke 2 3 1.000*
Osteonecrosis 3 2 0.6471*
Leg ulcer 0 6 0.0384 *
Priapism n=66 (Male only)
(N=34) 1
(N=32) 4
0.1974*

92
Gallstone 4 2 0.235* NB- Significant p values are in bold fonts, †= Mann-Whitney Test, *=Fisher`s exact test
7.5.5. Comparison of parameters between patients with and without leg ulcer.
The 6 (6.0%) patients with leg ulcers (both active and healed) were made up of 3 males
and females each: 4.5% vs 8.8%; p=0.393. They were relatively older compared to their
peers: median age, 17.5years (14 – 21) vs 9years (2 – 18), p=0.0002. They were all from
the low socioeconomic class: low class 6 (12.5%) vs others (middle & upper) 0 (0%),
p=0.0103. They also had less bone pain episodes (Table 25).
The LDH, bilirubin, platelet and WBC counts of the patients who had leg ulcer were
relatively higher compared to their peers without leg ulcer, however, these values did not
attain statistical significance (p>0.05). Similarly, although the Hb, RBC, and HbF of the
patients with leg ulcers were lower, these did not attain statistical significance Table 25.
Table 25: Comparison of patients with or without leg ulcer in the absence of Alpha
thalassemia
Parameters Leg ulcer present but absence of α-thalassemia
(N=6) Median (Range)
Absence of both leg ulcer and α-thalassemia
(N=52) Median (Range)
P value
Age in years 17.5 (14 – 21) 9 (2 – 8) 0.0005
Bone pain crisis per year
0.5 (0 – 1) 1 (0 – 6) 0.0301
Total bilirubin (mg/dl)
2.0 (1.0 – 4.1) 1.8 (0.8 – 5.1) 0.75
AST (IU/L) 40 (28 – 56) 38 (7 – 89) 0.89
RBC (million cells/uL)
2.7 ( 2 – 4.1) 2.8 ( 2.1 – 4.8) 0.396
Hb (g/dl) 7.1 ( 6.2 – 8.1) 7.7 (6.3 – 10) 0.214
LDH (IU/L) 972 (681 – 1681) 789 (197 – 1489) 0.130
HbF (%) 8.5 (5.9 – 12.5) 10.3 ( 2.5 – 22) 0.317
Platelet ( X 103/uL) 473 ( 207 – 669) 375 ( 118 – 832) 0.367
WBC ( X 103/uL) 14.5 ( 10 – 21.7 ) 13.5 ( 6 – 27.3) 0.542
NB- Significant p values are in bold fonts, Test statistics = Mann- Whitney Test, Hb-
Hemoglobin concentration, RBC-Red blood cells, MCV-Mean corpuscular volume,
WBC-White blood cells count, HbF- Fetal hemoglobin, MCH- mean corpuscular
hemoglobin, AST-Aspartate transaminase, LDH-Lactate dehydrogenase

93
7.6 Haptoglobin Genotypes
The haptoglobin genotypes determination was successful in 108 patients (SS-101 & SC-
7). The distribution of the haptoglobin genotypes among the patients were as follows: 48
(44.4%) Hp1-1, 41 (38.8%) Hp2-1 and 19 (17.7%) Hp2-2. Five HbSC patients had Hp1-
1 genotype, one Hp2-1, and one Hp2-2. The distribution of the haptoglobin genotypes of
the controls were as follow: 35 (54.6%) Hp1-1, 24 (37.5%) Hp2-1, and 5 (7.9%) Hp2-2.
The frequency of Hp1 alleles and Hp2 alleles were 0.63 an 0.37 in patients and 0.73 and
0.27 in controls respectively and the occurrence of the genotypes were in Hardy Weinberg
equilibrium for both patients ( ᵡ2 =3.36, p=0.186) and controls ( ᵡ2 =0.1, p=0.951).
7.6.1. Influence of haptoglobin genotype on biologic markers of patients
The haptoglobin genotype distribution did not significantly influence the laboratory
parameters of the patients Table 26
Table 26: Associations between Haptoglobin genotypes and biologic markers of Nigerian SS cohorts
Parameters Genotype Hp1-1
N=43
Genotype Hp2-1
N=40
Genotype Hp2-2
N=18
P Value
Total bilirubin (mg/dL)
2.2 (0.9 – 7.7) 1.5 (0.8 – 8.1) 1.7 (0.4 – 5.1) 0.097
Unconj. bilirubin (mg/dL)
1.0 (0.1 -6.2) 0.7 (0.1 – 6.2) 0.8 (0.3 – 3.7) 0.08
AST (IU) 37.0 (12.0 –
89.0)
45.0 (9.0 – 89.0) 37.0 (7.0 – 89.0) 0.066
LDH (IU) 950.0 (197.0 –
1750.0)
726.0 (197.0 –
1860.0)
592.0 (215.0 –
1399.0)
0.056
RBC ( million cells/uL)
2.8 (1.8 – 4.7) 2.8 (1.8 – 4.8) 2.9 (1.9 -3.9) 0.789
Hb (g/dL) 7.5 (6.2 – 11.1) 7.5 (6.3 – 10.1) 7.7 (6.3 – 8.8) 0.988
MCV (fL) 81.0 (60.0 –
115.0)
81.0 (56.0 –
102.0)
80.0 (70.0 –
104.0)
0.8057
WBC ( X 103/uL)
13.0 (6.1 – 26.2) 12.6 (6.1 – 27.3) 13.0 (6.4 – 29.3) 0.533

94
Platelet ( X 103/uL)
328.0 (118.0 –
771.0)
364.0 (108.0 –
832.0)
402.0 (159.0 –
593.0)
0.207
HbF (%) 6.7 (1.7 – 24.4) 10.8 (0.9 – 32.3) 10.2 (3.1 – 21.8) 0.224
HbS (%) 82.0 (44.0 –
91.0)
80.0 (61.0 –
89.0)
80.0 (73.0 –
88.4)
0.319
NB: Test statistics= Kruskal – Wallis Test, RMP-Red blood cell microparticle, HbF-Fetal
Hemoglobin, RBC-Red blood cell, Hb-Hemoglobin concentration, HbS- Hemoglobin S, WBC-
White blood cell count, LDH-Lactate dehydrogenase
7.6.2. Influence of haptoglobin genotype on clinical events
The haptoglobin genotype did not significantly influence the patients` clinical events Table 27
Table 27: Influence of Haptoglobin genotype on clinical events of SS cohorts
Clinical events a. Genotype
Hp1-1
N=43
b. Genotype
Hp2-1
N=40
c. Genotype
Hp2-2
N=18 P value
VOC per year 1 (0-6) 1 (0-6) 2 (0-6) 0.864*
Overt Stroke 2 1 2 0.375†
No overt stroke 41 39 16
Osteonecrosis 0 5 0 0.108†
No osteonecrosis
43 35 18
Leg ulcer 3 3 0 0.498†
No Leg ulcer 40 37 18
Gallstones 3 2 1 0.923†
No Gallstone 40 38 17
Priapism (Male only, N=67)
Priapism 3 2 0 0.632†
No Priapism 32 25 10
*=Mann-Whitney Test, †=Chi-Square Test, Significant p values are indicated in bold
fonts.
7.7 BCL11A and Fetal Haemoglobin

95
The BCL11A polymorphisms was significantly associated with the fetal haemoglobin
levels of the participants. The BC11A polymorphism was successfully studied in 110
patients and 66 controls.
Table28: Table of BCL11A SNPs examined. Code SNP
SNP1 rs4671393
SNP2 rs11886868
SNP3 rs766432
SNP4 rs1427407
SNP8 rs7606173
SNP9 rs6706648
SNP10 rs7557939
SNP11 rs6738440
SNP14 rs6732518
SNP15 rs13019832
All the SNPs were in Hardy – Weinberg equilibrium for both patients and controls:
rs4671393 Controls p value (0.6473436), Patients p value (0.8799153);
rs11886868 Controls p value (0.6473436), Patients p value (0.8799153);
rs766432 Controls p value (0.6473436), Patients p value (0.8799153);
rs7606173 Controls p value (0.9459216), Patients p value
(0.9963276);
rs6706648 Controls p value (0.9003801), Patients p value
(0.9731736);
rs7557939 Controls p value (0.6473436), Patients p value
(0.933441);
rs6738440 Controls p value (0.970751), Patients p value
(0.4929772);
rs6732518 Controls p value (0.3468636), Patients p value
(0.9896354);
rs13019832 Controls p value (0.4873589), Patients p value
(0.6341299);
Comparison of parameters of the BCL11A participants: There is no difference in the distribution of the genotype frequencies of the BCL11A polymorphisms of the patients and controls Table 29

96
Table 29: Descriptive statistics and comparisons SNPs between the patients and controls . Variable Controls Patients Total p-
value
Age (Mean ± SD (N)) 8.5 ± 3.9 (N=66) 9.1 ± 4.6 (N=110) 8.8 ± 4.3 (N=176)
0.4914¹
Age (Median (min-max)) 8.5 (2.0-18.0) 9.0 (2.0-21.0) 9.0 (2.0-21.0)
HbF (Mean ± SD (N)) 0.8 ± 0.6 (N=66) 9.8 ± 6.9 (N=110) 6.4 ± 7.0 (N=176)
<.0001¹
HbF (Median (min-max)) 0.8 (0.0-2.1) 8.4 (0.2-32.3) 3.7 (0.0-32.3)
Gender
FEMALE 27 (40.9%) 38 (34.5%) 65 (36.9%)
0.3971²
MALE 39 (59.1%) 72 (65.5%) 111 (63.1%)
Total 66 110 176
SNP1
AA 1 (1.5%) 8 (7.3%) 9 (5.1%)
0.2067²
AG 22 (33.3%) 39 (35.5%) 61 (34.7%)
GG 43 (65.2%) 63 (57.3%) 106 (60.2%)
Total 66 110 176
SNP2
CC 1 (1.5%) 8 (7.3%) 9 (5.1%)
0.2067²
CT 22 (33.3%) 39 (35.5%) 61 (34.7%)
TT 43 (65.2%) 63 (57.3%) 106 (60.2%)
Total 66 110 176
SNP3
AA 43 (65.2%) 63 (57.3%) 106 (60.2%)
0.2067²
AC 22 (33.3%) 39 (35.5%) 61 (34.7%)
CC 1 (1.5%) 8 (7.3%) 9 (5.1%)
Total 66 110 176
SNP4
GG 43 (65.2%) 65 (59.6%) 108 (61.7%)
0.4275³
GT 22 (33.3%) 38 (34.9%) 60 (34.3%)
TT 1 (1.5%) 6 (5.5%) 7 (4.0%)
Total 66 109 175
SNP8
CC 19 (28.8%) 21 (19.1%) 40 (22.7%)
0.2339²
GC 34 (51.5%) 58 (52.7%) 92 (52.3%)
GG 13 (19.7%) 31 (28.2%) 44 (25.0%)
Total 66 110 176
SNP9
CC 16 (24.2%) 35 (31.8%) 51 (29.0%)
0.2244²
CT 31 (47.0%) 55 (50.0%) 86 (48.9%)
TT 19 (28.8%) 20 (18.2%) 39 (22.2%)
Total 66 110 176
SNP10
AA 43 (65.2%) 62 (56.4%) 105 (59.7%)
0.1906²
AG 22 (33.3%) 40 (36.4%) 62 (35.2%)
GG 1 (1.5%) 8 (7.3%) 9 (5.1%)
Total 66 110 176
SNP11

97
AA 30 (45.5%) 60 (54.5%) 90 (51.1%)
0.3279²
AG 30 (45.5%) 45 (40.9%) 75 (42.6%)
GG 6 (9.1%) 5 (4.5%) 11 (6.3%)
Total 66 110 176
SNP14
CC 2 (3.0%) 12 (10.9%) 14 (8.0%)
0.1724²
CT 30 (45.5%) 47 (42.7%) 77 (43.8%)
TT 34 (51.5%) 51 (46.4%) 85 (48.3%)
Total 66 110 176
SNP15
AA 17 (25.8%) 17 (15.5%) 34 (19.3%)
0.1703²
AG 28 (42.4%) 46 (41.8%) 74 (42.0%)
GG 21 (31.8%) 47 (42.7%) 68 (38.6%)
Total 66 110 176
NB: 1= Mann-Whitney Test, 2= Chi-square Test, 3=Fisher Exact Test
Relationships between the SNPs and HbF levels of the patients: All the SNPs except
one (rs 6732518) were significantly associated with HbF levels (Table 30). Further
analysis for possible alleles combinations associated with higher HbF indicated that
patients with ACCTGCGAG combinations significantly belonged to this group while
patient with GTAGCTAAA combinations tend to have lower HbF (Table 31). A look at
the linkage of the SNPs showed that SNPs rs 4671393, rs11886868, rs766432, rs1427407,
are more related to one another and to rs 7557939 (Figure ANNEX 2).

98
Table 30: Measures of fetal hemoglobin by allele combination and comparison in Patients group.
SNP1 N Mean SD Minimum Median Maximum p-
value Result
-----------------------------------------------------------------------------
------------------
AA 8 15.88 9.07 3.40 15.80 32.30
0.0022 AA>GG
AG 39 11.47 6.86 0.20 10.70 28.50
GG 63 7.93 5.92 0.40 6.70 21.80
-----------------------------------------------------------------------------
-------------------
SNP2 N Mean SD Minimum Median Maximum p-
value Result ----------------------------------------------------
---------------------------------------
CC 8 15.88 9.07 3.40 15.80 32.30
0.0022 CC>TT
CT 39 11.47 6.86 0.20 10.70 28.50
TT 63 7.93 5.92 0.40 6.70 21.80
-----------------------------------------------------------------------------
-------------------
SNP3 N Mean SD Minimum Median Maximum p-
value Result
-----------------------------------------------------------------------------
------------------
AA 63 7.93 5.92 0.40 6.70 21.80
0.0022 CC>AA
AC 39 11.47 6.86 0.20 10.70 28.50
CC 8 15.88 9.07 3.40 15.80 32.30
-----------------------------------------------------------------------------
--------------------
SNP4 N Mean SD Minimum Median Maximum p-
value Result
-----------------------------------------------------------------------------
------------------
GG 65 7.93 5.87 0.40 6.70 21.8
0.0001 TT>GT,GG
GT 38 11.08 6.91 0.20 9.85 28.5
TT 6 20.30 6.30 14.90 18.75 32.3
-----------------------------------------------------------------------------
-----------------
SNP8 N Mean SD Minimum Median Maximum p-
value Result
-----------------------------------------------------------------------------
-----------------
CC 21 5.59 5.46 0.70 3.70 18.10
<.0001 GG>GC>CC
GC 58 9.31 6.22 0.20 7.90 28.50
GG 31 13.45 7.22 3.40 12.00 32.30
-----------------------------------------------------------------------------
-----------------

99
SNP9 N Mean SD Minimum Median Maximum p-
value Result
-----------------------------------------------------------------------------
-----------------
CC 35 13.09 6.88 3.40 12.00 32.30
0.0002 CC>CT,TT
CT 55 8.78 6.30 0.20 7.30 28.50
TT 20 6.66 6.39 0.70 4.05 20.60
-----------------------------------------------------------------------------
------------------
SNP10 N Mean SD Minimum Median Maximum p-
value Result
-----------------------------------------------------------------------------
-------------------
AA 62 7.79 5.85 0.40 6.70 21.80
0.0011 GG>AA
AG 40 11.61 6.83 0.20 11.20 28.50
GG 8 15.88 9.07 3.40 15.80 32.30
-----------------------------------------------------------------------------
------------------
SNP11 N Mean SD Minimum Median Maximum p-
value Result -----------------------------------------------------
------------------------------------------
AA 60 11.26 6.80 0.20 10.50 32.30
0.0034 AA>GG
AG 45 8.43 6.64 0.40 6.50 28.50
GG 5 3.88 5.01 0.70 1.30 12.60
--------------
SNP14 N Mean SD Minmum Median Maximum p-
value Result
---------------------------------------------------------------------------
---------------------
CC 12 12.23 6.46 0.20 13.85 20.60
0.2293 -
CT 47 10.23 7.69 0.90 7.50 32.30
TT 51 8.76 6.07 0.40 7.40 23.70
---------------------------------------------------------------------------
----------------------
SNP15
Result N Mean SD Minmum Median Maximum p-
valor
---------------------------------------------------------------------------
--------------------
AA 17 5.41 5.04 0.90 4.20 18.10
0.0002 GG>AA
AG 46 8.91 6.78 0.20 7.85 32.30
GG 47 12.18 6.68 2.60 11.60 28.50
---------------------------------------------------------------------------
---------------------
Test statistics: Kruskal Wallis ANOVA, followed by Tukey post hoc test

100
Table 31: Measures of fetal hemoglobin by allele combination and regression analysis. GTAGGCAAG N Mean SD Minimum Median
Maximum p-value¶
----------------------------------------------------------------------------
------------
0 34 8.70 7.88 0.70 4.60 32.30
0.0909
1 75 10.17 6.39 0.20 9.40 28.50
----------------------------------------------------------------------------
-------------
GTAGCTAAA N Mean SD Minimum Median
Maximum p-value ¶
----------------------------------------------------------------------------
-------------
0 55 11.88 7.35 0.70 11.60 32.30
0.0006
1 54 7.49 5.63 0.20 5.55 20.60
----------------------------------------------------------------------------
-------------
GTAGCTAGA N Mean SD Minimum Median
Maximum p-value ¶
----------------------------------------------------------------------------
-------------
0 70 11.22 7.09 0.20 10.25 32.30
0.0007
1 39 6.99 5.63 0.40 4.50 18.30
----------------------------------------------------------------------------
-------------
ACCTGCGAG N Mean SD Minimum Median
Maximum p-value ¶
----------------------------------------------------------------------------
-------------
0 70 7.91 5.92 0.40 6.30 21.80
0.0002
1 39 12.94 7.37 0.20 12.70 32.30
----------------------------------------------------------------------------
-------------
¶ Simple analysis (univariate)
Multiple analysis
GTAGGCAAG 0.3257
GTAGCTAAA 0.1618
GTAGCTAGA 0.2944
ACCTGCGAG 0.0208
Stepwise
ACCTGCGAG 0.0002-High HbF
GTAGCTAAA 0.0277-Low HbF
Patient with higher levels of Hb F presents the sequence ACCTGCGAG, but not
GTAGCTAA.

101
Table 32: Linkage disequilibrium between the SNPs pairs. Pairwise linkage disequilibrium
----------------------------------
SNP2 SNP3 SNP4 SNP8 SNP9 SNP10 SNP11 SNP15
SNP1 D 0.187 0.187 0.163 -0.108 -0.095 0.186 -0.062 -0.059
SNP1 D' 1.000 1.000 0.948 0.946 0.881 1.000 0.999 0.649
SNP1 Corr. 1.000 1.000 0.896 -0.499 -0.444 0.988 -0.333 -0.283
SNP1 X^2 219.836 219.836 175.064 54.702 43.291 214.601 24.389 17.624
SNP1 P-value <2e-16 <2e-16 <2e-16 1.4e-13 4.72e-11 <2e-16 7.87e-07 2.69e-05
SNP1 n 110 110 109 110 110 110 110 110
SNP2 D 0.187 0.163 -0.108 -0.095 0.186 -0.062 -0.059
SNP2 D' 1.000 0.948 0.946 0.881 1.000 0.999 0.649
SNP2 Corr. 1.000 0.896 -0.499 -0.444 0.988 -0.333 -0.283
SNP2 X^2 219.836 175.064 54.702 43.291 214.601 24.389 17.624
SNP2 P-value <2e-16 <2e-16 1.4e-13 4.72e-11 <2e-16 7.87e-07 2.69e-05
SNP2 n 110 109 110 110 110 110 110
SNP3 D 0.163 -0.108 -0.095 0.186 -0.062 -0.059
SNP3 D' 0.948 0.946 0.881 1.000 0.999 0.649
SNP3 Corr. 0.896 -0.499 -0.444 0.988 -0.333 -0.283
SNP3 X^2 175.064 54.702 43.291 214.601 24.389 17.624
SNP3 P-value <2e-16 1.4e-13 4.72e-11 <2e-16 7.87e-07 2.69e-05
SNP3 n 109 110 110 110 110 110
SNP4 D -0.092 -0.086 0.162 -0.057 -0.051
SNP4 D' 0.879 0.867 0.947 0.999 0.616
SNP4 Corr. -0.438 -0.412 0.885 -0.315 -0.254
SNP4 X^2 41.764 37.049 170.561 21.579 14.061
SNP4 P-value 1.03e-10 1.15e-09 <2e-16 3.39e-06 0.000177
SNP4 n 109 109 109 109 109
SNP8 D 0.226 -0.103 0.136 0.168
SNP8 D' 0.960 0.894 0.999 0.845
SNP8 Corr. 0.917 -0.477 0.632 0.700
SNP8 X^2 184.917 50.011 87.910 107.671
SNP8 P-value <2e-16 1.53e-12 <2e-16 <2e-16
SNP8 n 110 110 110 110
SNP9 D -0.091 0.130 0.171
SNP9 D' 0.825 0.919 0.829
SNP9 Corr. -0.420 0.608 0.719
SNP9 X^2 38.827 81.409 113.768
SNP9 P-value 4.63e-10 <2e-16 <2e-16
SNP9 n 110 110 110
SNP10 D -0.064 -0.054
SNP10 D' 0.999 0.587
SNP10 Corr. -0.337 -0.259
SNP10 X^2 24.994 14.767
SNP10 P-value 5.75e-07 0.000122
SNP10 n 110 110
SNP11 D 0.081
SNP11 D' 0.507
SNP11 Corr. 0.387
SNP11 X^2 32.945
SNP11 P-value 9.48e-09
SNP11 n 110

102
8. DISCUSSION
Hemolysis studies
Chronic hemolysis is a fundamental feature of sickle cell disease (SCD). It
contributes not only to its pathophysiology but also, the phenotypic variabilities15,85. In
order, to further strengthen this widely held belief, some hemolytic sub-phenotypes
comprising Leg ulcer, pulmonary hypertension, priapism and stroke have been
described15,85. However, despite these observations, more studies are needed to further
unravel more associates of hemolysis and possibly, elucidate more on the complex
interactions through which hemolysis affects SCD. Due to the impaired feasibility to
measure hemolysis directly in most clinical settings, clinicians use indirect or surrogate
markers to characterize intravascular hemolysis in SCD.15,86
In this study, we were able to establish that the hypothesized markers contribute
to hemolysis in the study cohorts. The relationships between RMP and other surrogate
hemolysis markers studied strongly suggest that RMP may be associated with
intravascular hemolysis in SCD. The correlational studies showed that RMP, plasma
hemoglobin, heme, haptoglobin, and hemopexin are related to one another as well as other
previously established traditional markers of hemolysis like serum bilirubin, LDH and
reticulocyte count15,24,85,86. One very recent study established that the only direct
reflection of the true hemolysis rate in SCA, is the red blood cell survival86. Furthermore,
the authors found that, out of the other traditional surrogate markers of hemolysis being
used, only the reticulocyte count correlated with the red blood cell survival86. Hence, our
observation that the RMP, Plasma hemoglobin, heme, haptoglobin and hemopexin of our
patients correlated with their reticulocyte counts strongly suggests that these parameters
are true markers of hemolysis. Our findings of highest levels of RMP, plasma
hemoglobin, and heme, and lowest levels of haptoglobin and hemopexin in the HbSS
cohorts in comparison to both the HbSC, and the controls is expected and suggest that the
hemolysis intensity in our study participants occured in the order SS>SC>AA. Also, this
study confirms an earlier report that, SCD patients had higher heme and lower
haptoglobin and hemopexin levels compared to healthy controls87. However, unlike in the
study by Muller-Eberhard et al,87 which was limited to only heme, haptoglobin and
hemopexin, in this study, we further extended the scope of their study by examininig the
levels of both the plasma hemoglobin and RMP. Our findings also showed that the levels

103
of these markers were higher in SCD patients compared to the controls and followed the
order SS>SC>AA. This further suggests higher hemolysis rate among the SCD patients.
Although the red blood cell contains abundant antioxidant enzyme systems like super
oxide dismutase, catalase, the peroxiredoxins and a diffusional barrier that limits NO
catabolism,12 during hemolysis, free hemoglobin is released which in turn, inactivates
nitric oxide (NO) in a deoxygenation reaction that also oxidizes the free hemoglobin to
methemoglobin. The methemoglobin so formed is very unstable and readily loses its
heme thus contributing to the various heme-related injuries seen in patients with SCD12.
Furthermore, reactions of NO with oxyhemoglobin have been shown to seriously
scavenge NO and inhibit its signaling34 These interactions lead to the depletion of NO and
subsequently set in motion, injuries to SCD patients in a way similar to damage-
associated molecular pattern molecules (DAMPs). Few examples of DAMPs include:
mitochondrial and cellular DNA, uric acid, adenosine, and other cytoplasmic and nuclear
proteins,12,15 When DAMPs are released outside of the cell, they activate innate immunity
and cause systemic inflammation in the absence of infection12,13,39,41,42. The release of
hemoglobin and its oxidation products from the red blood cells can drive sterile
inflammation via TLR4, causing vascular injuries, and a host of other damages similar to
those caused by DAMPs12,13,39,41,42. As a results of these, the hemoglobin and heme
released during intravascular hemolysis, are now being referred to as, erythrocytic
damage-associated molecular pattern molecules (eDAMPs)12,15. This observation shows
that the quest for markers of hemolysis and their impacts in SCD is ongoing with the
possibilities of more discoveries that could help in better understanding of the disease.
Given that only very few studies have examined the contributions of RMP to
hemolysis88,89, therefore, one important relevance of this study is the finding of the
association of RMP with traditional markers of intravascular hemolysis. Furthermore, no
previous study has jointly examined the relationships between the RMP, plasma
hemoglobin, heme, haptoglobin, and hemopexin together and by extension validate their
joint relationships to other previously established traditional markers of hemolysis as
done in this study. Similar to the findings in this study, Beers et al,88 found that RMP
correlated positively with plasma hemoglobin, and LDH, while Setty and colleagues89
found that RMP positively correlated with reticulocyte count. In addition, Setty et al89
found that RMP of their patients correlated negatively with the HbF of their patients
further confirming that RMP may be associated with hemolysis. Also, similar to our

104
findings, Donadee et al11 found that, RMP positively correlated with both LDH and
plasma hemoglobin in stored blood. They also showed that RMP scavenged NO in their
in-vitro study. The NO scavenging ability of RMP have also been confirmed by both
Camus et al31 and Liu et al.90 These observations highlight the potential roles RMP could
play in the pathophysiology of SCD especially as it relates to hemolysis and NO depletion
with attendant downstream complications. Therefore, our findings on RMP from this
study strongly suggest that RMP should also be considered as a member of the newly
defined eDAMPs family.
That a substantial proportion of the patients in this study were on treatment with
hydroxyurea is not surprising given that, the study participants were adults who could
have been possibly exposed to the SCD and its complications for long time. Hence, the
need for their treatment with hydroxyurea in order to ameliorate their disease
complications.
Hydroxyurea, through its ability to induce the production.of HbF, has emerged to be a
major drug used in managing patients with SCD90,91. The presence of HbF limits the rate
of polymerisation of HbS which is the primary event that leads to the cascades of
pathological and clinical manifestations in SCD48,49,50. To this end, HbF has been found
to be a modifier of anaemia, VOC, and stroke phenotypes in patients with SCD48,49,50
hence its being used regularly to ameliorate these complications.
The observed influences of hydroxurea on the hematologic parameters of the
patients have been described91 Nonetheless, it appears that the influence of hydroxyurea
therapy is more on our SS cohorts compared to their S-Beta counterparts given that more
hematologic indices were affected by the treatment with this drug in the former compared
to the later. Nevertheless, the small number of S-Beta thalassemia patients in this study,
erodes the possibility of any conclusion. Also, it is difficult to draw conclusions on how
hydroxyurea treatment affects some markers of intravacular hemolysis examined in this
study (RMP, plasma haemoglobin, heme, haptoglobin, and hemopexin) because, only few
studies have been conducted on them in-vivo in humans87,92,93,94,95,96,97and, much fewer
commented on their relationships with hydroxyurea treatment94, 96,97.
Although our SS cohorts with hydroxyurea had relatively lowered RMP, plasma
haemoglobin, and heme, however, these did not reach statistical significance.
Nonetheless, significant differences were observed with haptoglobin and hemopexin. The

105
lack of a significant reduction with hydroxyurea treatment vis a vis the other parameters
is not clear to us. However, we suspect that this could be due to the fact that, only a very
small number of patients in this study were not treated with hydroxyurea. Some other
studies have found that hydroxyurea treatment significantly influenced RMP levels of
SCD patients. Nebor et al94 in France, and Piccin et al96 in Italy as well as that by
Gerotziafas et al.97found that hydroxyurea reduces the levels of RMP in SCD patients.
Interestingly, in contrast to these studies,94,96,97 one study by Brunetta et al98 from Brazil,
actually found higher RMP levels in their SCA patients treated with hydroxyurea. They
proposed the possibility of a selection bias as the reason for their findings. They also
argued that SCD patients treated with hydroxyurea often have more severe disease and,
could possibly, suffer more splenic dysfunction and, are therefore, unable to clear RMP
effectively from circulation given that, the spleen is being considered as a clearance site
for RMP98,99,100. Another explanation proposed by them was the risk of direct cytotoxicity
of hydroxyurea leading to megaloblastic red blood cells that could shed more RMP98.
These observations raised the need for more studies to unravel how hydroxyurea
treatment affects RMP, heme, plasma hemoglobin, haptoglobin and hemopexin in SCD
patients.
Two previous studies92,93, demonstrated similar patterns of levels of plasma
hemoglobin across SCD patients` groups as found in this study hinting on the possibility
that in general, the behaviours of the studied hemolysis markers indicated that they concur
with the few available literature. While Adisa et al93 did not include healthy controls in
their study, Brittain et al92 found that, the levels of plasma hemoglobin was lower in
healthy subjects as found in this study.
Regarding the relationships between the studied markers and clinical events, the
observation that patients with osteonecrosis had higher hemoglobin concentration could
be due to the effects of blood rheology in SCD. SCD patients with higher hemoglobin
concentration levels usually have higher blood viscosity attributable to their rheological
effects and this predisposes them to blood viscosity associated phenotypes like
osteonecrosis and VOC101. Also, the finding of lower HbF in the cohorts with SCD
retinopathy might represent another aspect of the numerous ways through which HbF
ameliorate the severity of SCD48.

106
The associations of RMP and heme with leg ulcer in this study is a further confirmation
of their roles as hemolysis markers as previous studies have categorized leg ulcer as
belonging to hemolysis sub-phenotype15,85. In addition, the patients with leg ulcer had
higher LDH and this further confirms the association of LDH with leg ulcer as found in
previous larger studies25,102,103. However, to the best of our knowledge, the association of
both the RMP and heme with leg ulcer in SCD patients, have not been previously reported
thus making this study the first to report such association and therefore unique to it. We
suspect that, the duo perhaps, mediate and promote leg ulceration through the NO
depletion upon their release during intravascular hemolysis. Camus et al31 successively
demonstrated that, upon their release from the red blood cells, RMPs carry with them
trapped hemoglobin and heme. This observation was also confirmed by Liu et al.90 In
addition, Liu et al90 also demonstrated that, the trapped hemoglobin in RMP can be readily
oxidised to heme from their unstable intermediary (methemoglobin). They also
demonstrated that these RMPs are capable of entering significantly, into the free zone of
vasculature next to endothelia cell lining of blood vessels where they mediate NO
depletion thereby causing vascular damages. This is illustrated in Figure 20. Hence, one
could speculate that findings of associations of RMP and heme with the leg ulcer among
the patients is therefore not surprising given that, the SCD leg ulcer phenotype have been
closely linked to vasculopathy in SCD among other mechanisms.102,103.

107
Figure 20
Illustration of regions of modeled Red blood cells and microparticles in the lumen of the blood
vessel, which includes a red blood cell-free zone. NO is produced in the endothelium which is on
the exterior of the blood vessel. The smooth muscle is the outermost layer around the blood vessel.
The rate of NO scavenging depends on the permeability of the cell free zone which in turn, is
influenced by the amount of RMP present within the blood vessel lumen. Liu et al90
Therefore, it is conceivable to postulate that the joint transportation of trapped
plasma hemoglobin and heme by RMP is probably hazardous to SCD patients and may
be a mechanism for vasculopathy-associated phenotypes of SCD. This observations
further comfirm RMP, plasma hemoglobin, and heme as candidate markers of SCD
manifestations. The lower levels of RBC counts and hemoglobin concentration of our
patients with leg ulcer also confirms that leg ulcer is associated with hgher hemolysis and
anemia as previously described85,102,103.
The observed associations between raised TRV and RMP, heme, and worsening
anemia also suggest that TRV is related to hemolysis. Our findings that the TRV of the

108
patients correlated significantly with their RMP, heme, LDH, RBC counts and
hemoglobin concentration further confirm this association. This is in conformity with
previous reports that TRV, is associated with the hemolytic phenotype of SCD104,105. TRV
is a marker of pulmonary vascular disease and possibly, myocardiac stress. Also, elevated
TRVs are consistently associated with hyperhemolysis 15,104,105 . Studies have shown that
SCD patients with raised TRV are at risk of developing pulmonary
hypertension.15,104,105,106 (Illustration in Figure 21).
Given that pulmonary hypertension has been found to be associated with increased
risk of morbidities and deaths among SCD patients,15, 105, 107, 108 patients with SCD can
readily be screened for risk of pulmonary hypertension using TRV. Furthermore,

109
estimation of TRV can be easily done on outpatient basis through the Doppler
echocardiography thus making it useful in estimating pulmonary artery pressure and
predict the risk for pulmonary hypertension as modelled in figure 21 above. Hence, it
represents a simple, none invasive, and outpatients` investigation that can be carried out
to screen SCD patients for the risk of pulmonary hypertension-related problems so that
those patients at risk of complications can be identified for appropriate interventions.
The observation that the RMP, LDH and heme of our study cohorts with elevated TRV
were higher while their RBC count and haemoglobin were lower strongly suggests that
these parameters are associated with elevated TRV and the possible risk for developing
pulmonary hypertension. Although, RMP was not included in the model described by
Gladwin and Sachdev106 for pulmonary hypertension as shown in figure 22, findings from
this study and other emerging evidences are now showing that RMP and heme constitute
important mediators of some SCD complications. Nothing drives home this observation
than the findings in this study that both the RMP and heme were significantly associated
with at least three (leg ulcer, elevated TRV/risk for pulmonary hypertension and,
microalbuminuria/risk for kidney disease), of the hypothesized hemolytic phenotype of
SCD12,15,85, 106.
Given the increased risk of morbidities among SCD patients with elevated TRV and
pulmonary hypertension,15, 105, 107, 108 this study has further exposed the possibility of also
using the RMP and heme as a biomarkers for identifying high risk SCD patients for
further screening /intervention.
Figure 22

110
Mechanisms of hemolytic anemia in reducing NO bioavailability and association with
vasculopathic sub-phenotypes of sickle cell disease
Hemolysis releases cell-free plasma hemoglobin and arginase 1 into plasma, which
catabolize NO and L-arginine. Activation of vascular oxidases, such as xanthine oxidase,
NADPH oxidase and uncoupled eNOS, generate superoxide which scavenges NO.
Hemolytic anemia and reduced NO bioavailability are associated with vasculopathic
clinical complications in SCD patients (Gladwin & Sachdev106).
The proportion of the patients with microalbuminuria in this study confirms
previous observations that glomerulopathy manifesting as albuminuria, is common in
SCD79,109,110. The heme of our study participants with microalbuminuria was significantly
higher than those without. This suggests that the occurrence of microalbuminuria is
probably related to hemolysis intensity of our patients. However, the lack of significant
associations with other markers of hemolysis examined makes this generalization
difficult. Nonetheless, previous studies have established links between albuminuria and
hemolysis in SCD109,110. One study by Eshbach et al111 actually established that free
hemoglobin (a precursor of heme) inhibits albumin uptake by proximal tubule cells111.
This suggests a strong link between some products of hemolysis and renal disease in SCD
as found in this study. One important aspect of our finding is the fact that
microalbuminuria is a sign of early kidney disease and as such, our findings suggest that
SCD patients with high heme levels should be screened for microalbuminuria in order to
allow for early intervention and possible prevention of progression to chronic kidney
disease.

111
DISCUSSION
Genetic studies
Although quite some studies have been carried out in the developed world on the
influence of genetic markers on SCD, there is dearth of information on these from Africa.
The situation is even worse in Nigeria because of inadequate facilities. This is more
worrisome because of the status of Nigeria as the country with the highest number of
patients with SCD in the world3. Given that the effects of some genetic markers could
vary from place to place because of genetic variability and environmental factors in
different populations, it is pertinent that more studies be carried out among cohorts from
different ethnic backgrounds to fully understand the impacts of genetic modifiers on SCD.
The findings in this study are not only diverse but also interesting.
G6PD deficiency
The prevalence of G6PD deficiency among patients in this study (22.4%) is higher than
between 9 and 12% that has been described among children with SCD in Europe58,66 and
USA.66 It is however similar to between 15 and 25% that has been described among other
Africans59,112. The high prevalence of G6PD deficiency in Africa is thought to due to its
protective advantage against malaria57,58. The lack of association betwwen G6PD
deficiency with any laboratory parameters of the patients in this study confirms the lack
of consensus on how this genetic marker modulate SCD. Studies from Saudi Arabia63,
Burkina Faso64, and Senegal112found no effects of G6PD deficiency on the clinical
manifestations and laboratory parameters of SCD patients. The lack of association of
G6PD deficiency with clinical events as found in this study, is in support of some earlier
reports that, G6PD deficiency does not influence SCD significantly.63,64,112. However,
some studies from the USA and France found association of G6PD deficiency with
increased cerebral blood flow velocity, increased rate of acute anaemic events, blood
transfusions, and decreased steady state haemoglobin levels.58,65,66. There is need for more
studies to fully understand how G6PD deficiency influences SCD.
In conclusion, this study shows that G6PD deficiency does not significantly
influence both the clinical events and laboratory parameters of the patients.
UGT1A1 Polymorphism
This study confirms the variability of bilirubin levels based on the activity of the UGT1A1
genotypes as previously reported71,75,113-119. However, we are not aware of any previous

112
study that has described the trimodal pattern of LDH based on UGT1A1 genotypes
activity as found in this study. While the UGT1A1 modulation of serum bilirubin levels
is well understood71,75,113-121 the exact mechanism through which UGT1A1 could be
associated with LDH is not clear. However, it may be possible that there could be a link
through hemolysis because both bilirubin and LDH are derived from RBC and are
markers of hemolysis.122 UGT1A1 plays an important role in haem catabolism upon its
release from RBC and conversion to bilirubin71,75,113,117. Given the association of LDH
with some phenotypes of SCA,24,120 we suggest there is need for future research to unravel
if there is any link between LDH and UGT1A1 activity.
Gilbert syndrome (GS) has been described in individuals with the TA7/7 genotype
and71,75,113-114,119,120 this was more common among our patients 22 (21.7%) vs 5 (7.8%)
controls (p=0.018). This is probably due to the small number of the controls in this study.
Nonetheless, the proportion of patients with TA7/7 in this study is higher than between 6
-11% described among Europeans,123,124 11.7% in Saudi population,120 and between 3-
18% among Brazilians of different descents.76,125,126 Similarly, it is higher than the 6%
found among Kuwait SCA patients,127 and between 5 and 11% described among other
Africans124. However, this is lower than 32% described among the SCA patients in the
USA128. Nonetheless, the TA7/7 genotype prevalence in this study is comparable to the
18.2% and 20.3% earlier described among Nigerians with non SCD-related illnesses129,130
Besides the TA7/7 genotype, other UGT1A1 genotypes found in this study have been
described among other Africans and Nigerians71,124. These observations indicate that the
UGT1A1 genotype is quite variable among Nigerians and confirm the suggestions that
the expression of the UGT1A1 genotype variants is heterogeneous among Africans
compared to the Caucasians71,123,124.
Our finding that the low-activity UGT1A1 genotype was associated with gallstones
confirms previous observations that SCA patients with the low-activity UGT1A1
genotypes especially the TA7/7, are at risk of developing gallstones113,115,116,120. Also,
others,118,119,131 have reported that some other low-activity genotypes like TA7/8 and
TA8/8 predispose SCA patients to gallstones as found in this study.
The proportion of patients with asymptomatic gallstones in this study, 5.9%, is
comparable to between 4 and 6% earlier reported among Nigerian children of similar age
to our cohorts with SCA132-134. This is also similar to the 4% found in Ghana135, a close
neighbour to Nigeria. However, the gallstone prevalence in this study is lower than
between 9 – 58% that have been reported for some African children of similar age group

113
from other countries136-138. Similarly, higher prevalence of 26% and 30% was reported
for children with SCA and of same age range as our study cohorts in Italy139 and the
USA140 respectively. In the same vein, a 45% prevalence was found among a cohort of
Brazilian children with SCD following a median follow up of 7 years141 These
observations highlight the variations in propensity to gallstone development among
children with SCA. Persistent higher serum bilirubin is a risk factor for lithogenesis
among SCA patients 76, 113, 120,127. In addition, diets and environmental factors have also
been implicated138,140. Therefore, the observed similarities between the rates of gallstones
in this study, and, earlier reports from Nigeria132-134, and Ghana135 study, could be
attributed to the fact that, two countries belong to the West Africa region and are probably
exposed to similar diets and environmental factors different from their colleagues in other
distant African parts. Europeans and Americans are exposed to diets different from
African countries. Also, genetic differences among Africans and between Africans and
Europeans and/or Americans could play some roles. The age of onset and the apparent
lack of initial symptoms attributable to gallstones, as found in this study, have been
reported.131,134,138, 140 -142. However, results of follow-up studies have indicated that the
prevalence of gallstones and its complications increase with age of children with
SCA113,127, 131, 138,141 hence, the need to closely follow up these patients.
Despite the observation that the UGT1A1 low -activity genotype is a leading
factor in hyperbilirubinemia and lithogenesis among SCA patients67,113,115,142, none of the
previous studies from Nigeria examined the UGT1A1 of the patients132-134. Hence, to the
best of our knowledge, the contribution of this polymorphism to lithogenesis and
hyperbilirubinemia among Nigerian patients with SCA was not described prior to this
study. This study has shown that SCA children with the low-activity UGT1A1 genotypes
had higher bilirubin levels compared to others. In addition, we found that the low-activity
genotypes were associated with gallstones.
Similarly, although patients with gallstone in this study had higher serum bilirubin
levels and lower HbF levels as previously reported128, following multivariate analysis,
serum bilirubin was the only parameter associated with the UGT1A1 genotype.
Therefore, it thus appears that the pathway to higher serum bilirubin and gallstone
development in our patients is not exclusively driven by hemolysis and the ameliorating
effect of HbF on hemolysis but also by the influence of UGT1A1 genotype activity.
Beyond bilirubin metabolism and gallstone development, it has been suggested
that moderately elevated serum bilirubin can inhibit bacteria and Plasmodium falciparum

114
replication and that perhaps, the heterogeneity of UGT1A1 genotypes among Africans is
a result of genetic evolution to confer selective advantage by protecting from malaria in
a way similar to other genetic traits like G6PD deficiency and/or alpha
thalassemia71,75,124,143. The occurrence of these possibilities could be investigated through
a thorough prospective study.
In conclusion, this study confirms for the first time that UGT1A1 genotypes are
tightly associated with bilirubin levels and development of gallstone among young
Nigerians with SCA. In addition, it also suggests that the pathway to elevated serum
bilirubin and gallstone development among our study cohorts seems not to be exclusively
driven by hemolysis. These observations are in agreement with earlier reports67,128,144, and
highlight the contribution of UGT1A1 polymorphisms, a non-globin genetic factor, to the
clinical manifestations of SCA patients. Children with SCA in developing countries
should be screened for UGT1A1 polymorphisms and gallstones in order to allow for
holistic care.
Alpha thalassemia trait
That none of the participants had alpha thalassemia due to the 4.2kb globin gene
deletion confirms that 3.7kb globin gene deletion is the common form of alpha
thalassemia among Africans as previously described.43
The prevalence of alpha thalassemia among patients in this study (41%) is higher
than between the 13 and 28% described among patients in the Americas145,146,147,148. This
is however lower than the 60% and 77% described among Congolese,149 and Ugandans43
respectively. It is comparable to the 37.3% among Cameroonians, 150 and the 46% among
SCA patients in France151. It is also in agreement with the 40% to 42.5% earlier described
among Nigerians SCA patients152,153. The high prevalence of α-thal in this study, and
others from Africa,43,149,150 may be due to the selective advantage in conferring protection
and survival against malaria154,155,156. The higher prevalence of α-thal in central
Africa,43,149 relative to this study, may derive from its vital impact on survival of SCA
which is more severe in this part of Africa43,149.
The observed hematological profile of patients with α-thal in this study has been
previously described145,146,148,151-154,157. The increased Hb and red blood cell count are
probably due to the decrease in the intracellular concentration of HbS, and number of
dense red blood cells. These, in turn, lead to increased red blood cell deformability and
decreased rates of both HbS-induced RBC polymerization and hemolysis85,158,159.

115
Similarly, the lack of influence of α-thal on the HbF levels of patients in this study, has
been previously reported145,146,148 .
However, contrary to some earlier reports,146,148 the presence of α-thal was associated with
higher rates of bone pain crisis compared to those without α-thal. This finding is in
keeping with that of Renoux et al151 among children with SCA in France and other
previous reports158,159. Vaso-occlusive crisis (VOC) manifesting as bone pain crisis is a
common complication of SCA and, is thought to be associated with increased blood
viscosity151, 158. Studies have demonstrated that SCA patients with α-thal have increased
blood viscosity because of relatively higher levels of Hb and/or hematocrit, among other
mechanisms85,151,158,159. In this study, our SCA patients with α-thal, had higher Hb that
could lead to increased blood viscosity hence, it is conceivable that they could have higher
rates of painful crisis.
Furthermore, as found in this study, authors from different parts of the world have
reported that α-thal protects against leg ulcer in SCA patients149,157,160. However, some
have reported no such association43,150. These observations reflect lack of consensus on
the roles of α-thal in some phenotypes of SCA. Therefore, there’s a need for more studies
from Africa to explain the relationships between α-thal and leg ulcer, and other SCA
phenotypes.
Leg ulcer is a chronic and debilitating complication that is thought to be associated with
very severe phenotype of SCA85,102,103,161,162. Some studies have associated it closely with
some other hemolysis-related phenotypes of SCA such as priapism, stroke and pulmonary
hypertension85,102,161. We could not confirm the diagnosis of pulmonary hypertension
among our patients due to lack of facilities. However, like their leg ulcer counterparts,
most of the few patients with priapism also did not have α-thal, suggesting the possibility
of protection by α-thal against both leg ulcer and priapism.
Furthermore, the bilirubin, LDH, and AST levels of the patients with α-thal were
relatively lower than their counterparts without α-thal and this suggests lower hemolysis
in the former lending credence to the belief that presence of α-thal ameliorates hemolysis
in SCA patients.
When we evaluated the markers of hemolysis of the non-thalassemic cohorts, we
observed that in contrast to the patients with α-thal, the LDH, and bilirubin levels of leg
ulcer patients were relatively higher while their Hb and HbF were lower, compared to
their matched peers. This is further suggestive of increased hemolysis in the leg ulcer
group. However, these differences did not reach statistical significance probably because

116
of our sample size. Other larger studies have reported association of hemolysis markers
with leg ulcer in SCA patients85,102,103. and the presence of α-thal is thought to ameliorate
hemolysis in SCA85,158,159.
The observations that α-thal protect against the occurrence of stroke in children
with SCA163,164 was not sustained in this study. On the contrary, one previous study 153
found that, in combination with BCL11A variants, α-thal was associated with increased
risk for stroke in older SCA patients. The lack of association between α-thal and stroke
in this study, is in keeping with report by Filho et al165. Nonetheless, these findings need
to be interpreted with caution because of differences in age of study cohorts and
possibility of survival bias. In addition, stroke was determined in this study by overt
clinical history and was, in most cases, not confirmed by magnetic resonance imaging or
angiography and this could lead to detection bias and exclusion of cases of silent infarcts
from our analysis. These observations further underscore the need for more studies to
clearly define the prevalence and associations of α-thal with clinical manifestations
among Nigerian SCA patients.
The lack of association between α-thal and osteonecrosis in this study contrasts
with the report by Milner et al166 on children enrolled in the cooperative study of sickle
cell disease in the USA where they found that both α-thal and increasing age were
significantly associated with osteonecrosis. Possible explanations for our findings
included the fact that our study participants were fewer and younger compared to that by
Milner et al.166 The youngest patient in this study was two years old, while theirs` was
five years old. In addition, only five percent of our patients had osteonecrosis compared
to 9.8% in their study.
Osteonecrosis is a disabling and severe complication of SCA associated with
impairments of both functional activities and growth in children. In SCA, it is thought to
be due to bone microcirculation disturbance in the patients and can be observed in
children with SCA as young as five years old with an increasing incidence throughout
childhood and adolescence, peaking in early adulthood167.
Furthermore, this study is important because the modulating effects of alpha
thalassemia on hematologic indices as found, further reinforce the observations by Borges
et al168 that, Alpha thalassemia significantly influences the hematologic parameters
especially the MCV and MCH to the extent that it could easily be misdiagnosed and
confused with iron deficiency anemia. Given the high rates of iron deficiency anemia

117
among children in developing countries like Nigeria169, it is therefore important to
exclude alpha thalassemia in patients suspected to have iron deficiency in the tropics.
In conclusion, this study shows that coexistence of α-thal influences the
hematologic parameters of patients with SCA as previously described145,157,160,168. It also
showed that α-thal was associated with increased rates of bone pain crisis and protects
against the occurrence of leg ulcer.
Haptoglobin Polymorphism: This study confirm that the Hp1 allele and its
associated genotypes (Hp1-1 and Hp2-1) are common among the Nigerian SCD
patients16. This is similar to the pattern observed among SCD cohorts in Northeast
Brazil.18 However, the Hp1-1 genotype was found to be least represented in both
southeast Brazil170 and Kuwait.16 These differences may reflect the genetic backgrounds
of the patients as well as the influence of environmental factors. The similarity between
the haptoglobin genotypes in this study and that from northern Brazil could stem from the
link between SCD in northern Brazil and migration of people from Africa due to the trans-
atlantic slave trade.18 There was lack of any association between the Hp genotypes and
the examined laboratory parameters of the Nigerian cohort. This observation is not
surprising, as a study among a cohort of SCD patients in Brazil170 did not find any
relationship between haptoglobin genotypes and interleukins 6 and 8. Nonetheless, both
the current study and that from Brazil170 did not examine the blood levels of plasma
hemoglobin which has been proven to have links with haptoglobin genotypes.171 The lack
of association between haptoglobin genotypes and clinical events could be due to the fact
that the study cohorts are relatively young and less at risk of some chronic SCD
complications. It also contradicts the speculations that patients or individuals with certain
haptoglobin genotypes (e.g Hp2-2 are more prone to certain health conditions.16-18
BCL11A Polymorphism
While more than 70% of SCD patients worldwide live in Africa, most advances
in the molecular understanding and management of SCD have been based on research
conducted in either the Europe or the USA. It is now incrovertible that fetal hemoglobin
(HbF) has emerged to be an important disease modifying factor in SCD48-55. Previous
analyses of the cooperative studies on sickle cell disease (CSSCD) showed that increased
HbF levels correlate with less severe complications, fewer pain crises172, and improved
survival173. Also, it has been found that common genetic variation at BCL11A associated

118
with HbF levels lies in noncoding sequences associated with an erythroid enhancer
chromatin signature thus suggesting that, the genome wide association-marked BCL11A
enhancer locus may be an attractive target option for therapeutic genome engineering for
the hemoglobinopathies52. However, despite these great potentials of HbF, information
on the influence of genetic influencers of this impotant modifier of SCD severity are
scanty in Africa. This study confirms for the first time that BCL11A polymorphism
modulate HbF levels of the Nigerian SCD cohorts. The observation that nine: (rs
4671393, rs11886868, rs766432, rs1427407, rs 7606173, rs 6706648, rs 7557939, rs
6738440 and rs 13019832) of the ten BCL11A polymorphisms studied were associated
with the HbF levels of the patients further reinforcing the important roles BCL11A
polymorphism play in the regulation of HbF among the Nigerian patients with SCD. This
observation is in agreement with findings from previous studies among Europeans and
Americans50, Tanzania and African British53, African Brazilian and African American174
SCD patients. It also confirms the association of BCL11A polymorphisms with HbF as
found among a cohort of SCA patients in northern Brazil175 and studies from Cameroon 54,55 and Tanzanian53 cohorts both in Africa. In conclusion, this study shows that BCL11A
polymorphism significantly influenced the HbF levels of the Nigerian children with SCD.

119
9. CONCLUSIONS
Hemolysis studies
This study was able to establish that:
a. Serum levels of RMP, heme, and plasma haemoglobin were significantly higher
in SCD patients compared to control while the hemopexin and haptoglobin levels
of SCD patients were significantly lower compared to controls suggesting higher
hemolysis among the SCD cohorts;
b. The intensity of hemolysis appears to be in the following order SS>SC>AA;
c. RMP, plasma hemoglobin, heme, haptoglobin and hemopexin were significantly
associated with traditional markers of hemolysis thus suggesting their roles as
markers of hemolysis;
d. Hydroxyurea therapy did not significantly influence the levels of RMP, heme, and
plasma hemoglobin of the studied HbSS patients;
e. RMP was significantly associated with leg ulcer and elevated TRV among the
patients;
f. Heme was significantly associated with leg ulcer, elevated TRV and the
occurrence of microalbuminuria;
g. Two of the hypothesized hemolytic phenotypes of SCD: leg ulcers and elevated
TRV (risk for pulmonary hypertension) were associated with biological markers
evaluated in this study thus suggesting their importance in the clinical and
pathologic manifestations of SCD;
h. Osteonecrosis was associated with increased levels of hemoglobin concentration;
i. Higher HbF levels were protective against SCD retinopathy;
j. Based on the above observations, it thus appear that there is a catastrophic synergy
between the RMP and heme in the occurrence of adverse clinical events among
the studied patients. Therefore, therapies targeting heme and RMP may be a new
approach to tackling the SCD.

120
Genetic studies
This study was able to establish the following:
a. UGT1A1 genotypes significantly influenced both the serum bilirubin and LDH
levels of the patients;
b. UGT1A1 polymorphism was found to be significantly associated with the
occurrence of gallstone among the Nigerian patients with SCD. This is the first
study to describe the influence of UGT1A1 polymorphism in Nigerian patients
with SCD;
c. Alpha thalassemia significantly influenced the hematologic indices of the
patients;
d. Alpha thalassemia was associated with higher rates of bone pain crisis and could
protect against leg ulcer phenotype.
e. BCL11A polymorphism significantly influenced the HbF of the Nigerian patients
cohort;
f. G6PD deficienccy did not influence both the clinical and laboratory parameters
of the patients;
g. Haptoglobin genotypes did not influence any of the clinical and laboratory
parameters examined among the Nigerian patients.

121
10. REFERENCES
1. Reeds DC, Williams TN, Gladwin MT, Sickle-cell disease. Lancet. 2010;376:2018–31
2. Steinberg MH. Sickle cell anemia, the first molecular disease: overview of molecular
etiology, pathophysiology, and therapeutic approaches. Scientific World Journal.
2008;8:1295-324.
3. Galadanci N, Wudil BJ, Balogun TM, Ogunrinde GO, Akinsulie A , Hasan-Hanga F et
al. Current Sickle cell disease management practices in Nigeria. Int Health
2013;doi:10.1093/inthealth/iht022
4. Piel FB, Patil AP, Nyangiri OA, Mewahyu PWG, Teperely WH et al Global
epidemiology of sickle cell haemoglobin in neonates. Lancet 2013;381:142-51
5. Lervolino LG, Baldin PE, Picado SM, Viel AA, Campos LA. Prevalence of sickle cell
disease in national screening studies. Rev Bras Hematol Hemoter 2011;33(1):49-54
6. Makani J, Ofori-acquah, Nnodu O, Wonkman A, Ohene-frempong K. Sickle cell disease:
New opportunities and challenges in Afirca The Scientiffic World Journal 2013;
doi:10.1155/2013/193252
7. Steinberg MH. Genetic etiologies for phenotypic diversity in sickle cell anemia. The
scientific world journal 2009;9:46-67
8. Milton JN, Rooks H, Draser E, McCabe EL, Baldwin CT et al. Genetic determinants of
hemolysis in sickle cell anemia. Br J Hematol 2013; 161(2):270-78.
9. Nouraie M, Lee JS, Zhang Y, Kanias T, Zhao X et al The relationship between the
severity of hemolysis, clinical manifestations and risk of death in 415 patients with sickle
cell anemia in the US and Europe. Haematologica 2013; 98(3): 464-72
10. Minniti CP, Sable C, Campbell A, Rana S, Ensing C et al. Elevated triscuspid regugitant
jet velocity in children and adolescents with sickle cell disease:association with
hemolysis and haemoglobin oxygen desaturation. Haematologica 2009; 94(3):340-7
11. Donadee C, Raat NJ, Kanias T, Tejero J, Lee JS et al. Nitric oxide scavenging by red
blood cell microparticles and cell free haemoglobin as mechanism for the red cell storage
lesion. Circulation 2011; 124(4):465-76
12. Gladwin MT, Ofori-Acquah SF. Erythroid DAMPs drive inflammation in SCD. Blood
2014;123 (24):3689-90
13. Mendonca R, Silveira AA, Conran N. Red cell DAMPs and inflammation. Inflamm. Res.
2016;65:665-78
14. Gladwin MT, Kanias T, Kim-Shapiro DB. Hemolysis and cell free haemoglobin drive an
intrinsic mechanism for human disease. J Clin Invest. 2012;122(12):1205-8
15. Kato GJ, Steinberg MH, Gladwin MT. Intravascular hemolysis and the pathophysiology
of sickle cell disease. J Clin Invest. 2017;127(3):750-60

122
16. Adekile AD, Haider MZ. Haptoglobin gene polymorphisms in sickle cell disease patients
with different βS-globin gene haplotypes. Med Princ Pract 2010;19:447-50
17. Wobeto VP, Zaccariotto TR, Sonati MF. Polymorphism of human haptoglobin and its
clinical importance. Genetics and Molecular Biol 2008; 31(3):602-20
18. Santos MN, Bezerra MA, Dormigues BL, Zachariotto TR, Oliveira DM. Haptoglobin
genotypes in sickle cell disease. Genetic Test. Mol. Biomarker 2011;15(10):709-13
19. Schaer DJ, Buehler PW, Alayash AI, Belcher JD, Vercellotti GM. Hemolysis and free
haemoglobin revisited: exploring haemoglobin and hemin scavengers as novel class of
therapeutic proteins. Blood 2013;121(8):1276-84
20. Podmore AH. Haptoglobin for the treatment of sickle cell disease. Bioscience Hypothes
2008;1(1):59-63
21. Gosh S, Adisa OA, Chappa P, Tan Fang, Jackson KA, et al. Extracellular hemin crisis
triggers acute chest syndrome in sickle mice. J Clin Invest 2013;123(1):4809-20
22. Vinchi F, Franceschi L, Chigo A, Townes T, Cinimo J et al. Hemopexin theraphy
improves cardiovascular function by preventing heme induced endothelial toxicity in
mouse models of haemolytic diseases. Circulation 2013; 127:1317-29
23. Smith A, Mc Culloh RJ. Hemopexin and haptoglobin: allies against heme toxicity from
haemoglobin not contenders. Front. Physiol 2015;6:187 doi:10.3389/phys.2015.00187
24. Kato GJ, McGowan V, Machado RF, Little JA, Taylor VI J et al. Lactate dehydrogenase
as a biomarker of hemolysis-associated nitric oxide resistance, priapism, leg ulceration,
pulmonary hypertension, and death in patients with sickle cell disease. Blood 2006;
107(6):2279-85.
25. Kato GJ, Nouraie SM, Gladwin MT. Lactate dehydrogenase and hemolysis in sickle cell
disease. Blood 2013; 122(6): 1091-92.
26. Ballas SK. Lactate dehydrogenase and hemolysis in sickle cell disease Blood 2013;
121(1):243-44.
27. Mecabo G, Yamamoto M, Biassi TP, Figueiredo MS. Lactate dehydrogenase isoenzymes
3 and hemolysis in sickle cell anemia a possible correlation. Blood 2015; 125 (24):3821-
22
28. Mikobi TM, Lukusa Tshilobo P, Aloni MN, Mvumbi Lelo G, Akilimali PZ et al.
Correlation between the lactate dehydrogenase levels with laboratory variables in the
clinical severity of sickle cell anemia in Congolese patients. PLoS ONE
2015;10(5):e0123568. Doi:10.1371/journal.pone.0123568.
29. Adegoke SA, Adeodu OO, Adekile AD. Sickle cell disease clinical phenotypes in
children from South-Western Nigeria. Nig J Clin Pract. 2015;18(1):95-101
30. Rubin O, Canellini G, Delobel J, Lion N, Tissot JD. Red blood cell microparticles:
Clinical relevance. Transfus Med Hemother 2012;39:342-47

123
31. Camus SM, De Moraes JA, Bonnin P, Abbyad P, Le Jeune S et al. Circulating cell
membrane microparticles transfer heme to endothelia cells and trigger vaso-occlussions
in sickle cell disease. Blood 2015;125(24):3805-14
32. Van Beers EJ, Schaap MC, Berckmans RJ, Nieuwland R, Sturk A et al. Circulating
erythrocyte derived microparticle are associated with coagulation activation in sickle cell
disease. Haematological 2009;94:1513-19
33. Camus SM, Gausseres B, Bonnin P, Loufrani L, Grimaud L et al. Erythrocyte
microparticles can induce kidney vaso-occlussions in a murine model of sickle cell
disease. Blood 2012;120(25):5050-58
34. Reiter CD, Wang X, Trans-santos JE, Hogg N, Canon RO III et al. Cell free haemoglobin
limits nitric oxide bioavailability in sickle cell disease. Nat Med 2002;8:1383-89
35. Morris CR, Gladwin MT, Kato GJ. Nitric oxide and arginine dysregulation: A novel
pathway to pulmonary hypertension in haemolytic disorders. Curr Mol Med
2008;8(7):620-32
36. Morris CR, Kato GJ, Poljakovic M, Wang X, Blackweider WC et al. Dysregulated
arginine metabolism, hemolysis-associated pulmonary hypertension and mortality in
sickle cell disease. JAMA 2005;294:81-90.
37. Chiabrando D, Mercurio S, Tolosano E. Heme and erythopoesis: more than a structural
role. Hematologica 2014;99(6):973-83.
38. Uzunova VV, Pan W, Galkin O, Vekilov PG. Free heme and the polymerization of sickle
cell haemoglobin. Biophysical Journal 2010;99(6):1976-85.
39. Chen G, Zhang D, Fuchs TA, Mawani D, Wagner DD. Heme induced neutrophil
extracellular traps contribute to the pathogenesis of sickle cell disease. Blood
2014;123(24):3818-27
40. Sakamoto TM, Canalli AA, Traina F, Franco-Penteado C, Gambero S et al. Altered red
cell and platelet adhesion in haemolytic diseases: Hereditory spherocytosis, paroxysmal
nocturnal hemoglobinuria and sickle cell disease. Clinical Biochemistry 2013;46: 1798-
1803
41. Belcher JD, Nat KA, Vercelotti GM. Vasculotoxic and proinflammatory effects of
plasma heme: cell signalling and cytoprotective responses. ISRN Oxidative Medicine
2013;e831596 doi:dx,doi.org/10.1155/2013/831596
42. Guarda CCD, Santiago RP, Fluza LM, Aleluia MM, Ferreira JRD et al. Heme mediated
cell activation: the inflammatory puzzle of sickle cell anemia. Expert Rev Hematol
2017;10(6):533-41
43. Lubega I, Ndugwa CM, Mworozi EA, Tumwine JK. Alpha Thalassemia among sickle
cell anemia patients in Kampala, Uganda. Afri Hlth Sci 2015; 15 (2):682-89

124
44. Omoti CE. Beta thalassaemia traits in Nigerian patients with sickle cell anaemia. Journal
of Biomedical sciences 2005; 4(1):37-43
45. Figueiredo MS. The compound state: Hb S/beta-thalassemia. Rev Bras Hematol Hemoter
2015;37(3):150-152
46. Ataga KI, Cappellini MD, Rachmilewitz EA. Beta-Thalassemia and sickle cell anaemia
as paradigms of hypercoagulability. Br J Haematol 2007; 139:3-13
47. Belisario AR, Sales RR, Viana MB. Very mild forms of Hb S/beta+-thalassemia in
Brazilian children. Rev Bras Hematol Hemoter 2015;37(3): 198-201
48. Akinsheye I, Solovieff N, Ngo D, Malek A, Sebastiani P et al. Fetal haemoglobin in
sickle cell anemia: molecular characterisation of the unusally high fetal haemoglobin
phenotype in African American. Am J Hematology 2012;87(2):217-19
49. Bhagat S, Patra PK, Thakur AS. Association between Xmnl polymorphism and
hemoglobin F level in SCD patients from Chhattisgarh. Int J Biomed Sci. 2012;8(1):36-
9.
50. Wonkam A, Makani J, Ofori-Aquah S, Nnodu OE, Treadwell M et al. Sickle cell disease
and H3Africa: enhancing genomic research on cardivascular diseases in African patients.
Cardiovasc J Afr 2015;26(2): S50-S55
51. Xu J, Peng C, Sakaran VG, et al. Correlation of sickle cell disease in adult mice by
interference with fetal fetal haemoglobin silencing. Science 2011;334(6058):993-6
52. Bauer DE, Kamran SC, Lessard S et al. An erythroid enhancer of BCL11A subject to
genetic variation determines fetal hemoglobin level. Science 2013;342(6155):253-7
53. Makani J, Menzel S, Nkya S et al. Genetics of fetal hemoglobin in Tanzanian andBritish
patients with sickle cell anemia. Blood 2011;117(4):1390-92
54. Wonkam A, Ngo Bitoungui VJ, Vorster AA et al. Association of variants at BCL11A
and HBS1L-MYB with hemoglobin F and hospitalisation rates among sickle cell patients
in Cameroon. PLoS ONE 2014;9(3):e92506
55. Bitoungui VJ, Ngogang J, Wonkman A. Polymorphism at BCL11A compared to HBS1L-
MYB loci explains less of the variance in HBF in patients with sickle cell disease in
cameroon. Blood cells Mol Dis 2014;Nov 25. Pii:S1079-9796(14)00143-0
56. Monteiro WM, Val FF, Siqueira AM, Franca GP, Samparo VS et al. G6PD deficiency in
Latin America: systematic review of prevalence and variants. Mem Inst Oswaldo Cruz
2014;109(5):553-68
57. Orimadegun AE, Sodeinde O, G6PD status and severity of malaria anemia in Nigerian
children. J Infect Dev Ctries 2011;5:792-8
58. Benkerrou M, Alberth C, Couque N, Ba A Missud F et al. Impact of G6PD deficiency
on sickle cell anaemia expression in infancy and early childhood: A prospective study.
Br J Hematol 2013;163(6):646-54

125
59. Williams O, Gbadero D, Edowhorhu G, Brearley A, Slusher et al. G6PD deficiency in
Nigerian children. PLoS ONE 2013;8(9): e68800.doi:10.1371/journal.pone.
60. De-Araujo C, Migot-Nabias F, Guitard J, Pelleau S, Vulliamy T et al. The roles of the
G6PD376G/968C allele in glucose -6-phosphate dehydrogenase deficiency in the seerer
population of Senegal. Hematologica 2006;91:262-63
61. Cappelini MD, Fiorelli G, Glucose 6 phosphate dehydrogenase deficiency. Lancet 2008;
371:64-74
62. Clark TG, Fry AE, Aubums S, Campino S, Diakite M et al. Alleleic heterogeneity of
G6PD deficiency in West Africa and severe malaria susceptibility. Eur J Hum Genet
2009; 17:1080-85
63. Awamy BH. Effect of G6PD deficiency on sickle cell disease in Saudi Arabia. Indian J
Pediatr 1992;59:331-34
64. Simpore J, Ilboudo D, Damintoti D, Sawadogo L, Maria E et al. Glucose 6 phosphate
dehydrogenase deficiency and sickle cell disease in Burkina Faso. Pak J Biol Sci
2007;10(3): 409-14
65. Bernaudin F, Verlhac S, Cheuret S, Torres M, Coic L et al. G6PD deficiency, abscense
of alpha-thalassemia and hemoltic rate at baseline are significant independent risk factors
for abnormally high cerebral velocities In patients with sickle cell anemia. Blood
2008;112:4314-17
66. Nouraie M, Reading NS, Campbell A, Minnitti CP, Rana SR et al. Association of G6PD 202A,376G with lower Hb concentration but not increased hemolysis in patients with sickle
cell anemia. Br J Hematol 2010;150:218-25
67. Milton JN, Sebastiani P, Solovieff N, Hartley SW, Bhatriagar P et al. A genome-wide
association study of total bilirubin and cholelithiasis risk in sickle cell anemia. PLoS ONE
2012; 7(4): e34741.doi:10.1371/journal.pone.
68. Fertrin KY, Costa FF. Genomic polymorphisms in sickle disease: implications for
clinical diversity and treatment. Expert Rev. Hematol 2010;3(4):443-58
69. Sticova E, Jirsa M. New insights in bilirubin metabolism and their clinical implications.
World J Gastroenterol. 2013 Oct 14;19(38):6398-6407.
70. Horsfall LJ, Nazareth I, Pereira SP, et al. Gilbert's syndrome and the risk of death: a
population-based cohort study. J Gastroenterol Hepatol. 2013 Oct;28(10):1643-7. doi:
10.1111/jgh.12279
71. Horsfal LJ, Zeityln D, Tarekegn A, Bekele E, Thomas MG et al. Prevalence of clinically
relevant UGT1A alleles and haplotypes in African populations. Annals of Human
Genetics 2011; 238-248

126
72. Sebastiani P, Solovieff N, Hartley SW,Milton JN, Riva A. Genetic modifiers of the
severity of sickle cell anemia identified through a genomic-wide association study. Am J
Hematol 2010;85:29-35
73. Buch S, Schafmayer C, Volzke H, Seeger M, Miguel JF et al. Loci from a genome-wide
analysis of bilirubin levels are associated with gallstones risk and composition.
Gastroenterology 2010; 139:1942-51
74. Machado RF, Barst RJ, Yovetich NA, Hassel KL, Kato GJ et al. Hospitalisation for pain
inpatient with sickle cell disease with sidenafil for elevated TRV and low exercise
capacity. Blood 2011; 118: 855-64
75. Italia KY, Jijina FF, Jane D, Merchant R, Nadkarni AH et al. The effect of UGT1A
promoter polymorphism on bilrubin response to hydroxyurea in haemogloboinopathies.
Clin Biochem 2010; 43: 1329-32
76. Fertrin KY, Melo MB, Assis AM, Saad ST, Costal FF. UDP-glucuronosyl transgferase1
gene promoter polymorphism is associated with increased serum bilirubin levels and
cholecstectomy in patients with sickle cell anemia. Clini Genet 2003; 64:160-62.
77. Ballas S.K, Lieff S, Benjamin L.J, Dampier C.D, Heeney M.M, Hoppe C, et al.
Definitions of the phenotypic manifestations of sickle cell disease. Am J Hematol
2010;85:6–13.
78. Kato GJ. TRV: A physiological biomarker in sickle cell disease. Pediatr Blood Cancer
2012;58(6):831-2
79. Quin CT, Saraf SL, Gordeuk VR, Fitzhugh CD, Creary SE et al. Losartan for the
nephropathy of sickle cell anemia: A phase-2, multicentre trial. Am J Hematol
2017;92(9):E520-E528. Doi:10.10002/ajh.24810
80. QuantiChromTM Hemoglobin Assay Kit (DIHB-250), BioAssay Systems USA.
Available at www.bioassaysys.com Retrieved 8/9/2017
81. Quantichrom Heme assay kit (DIHM-250) Available at www.bioassaysys.com
Retrieved 8/9/2017
82. ab108859 Hemopexin human ELISA kit Available at www.abcam.com Retrieved
8/9/2017
83. Quantikine Human Haptoglobin (DHAPGO) ELISA kit, R & D Systems USA.
Available at www.RnDSystems.com Retrieved 8/9/2017
84. Wisgrill L, Lamm C, Hartmann J, Preibing F, Dragosits K et al. Cytometry Part A
2016;89A:663-72
85. Kato GJ, Gladwin MT, Steinberg MH. Deconstructing sickle cell disease:reappraisal of
the role of hemolysis in the development of clinical phenotype. Blood Rev.
2007;21(1):37-47

127
86. Quinn CT, Smith EP, Arbabi S, Khera PK, Lindsell CJ et al. Biochemical surrogate
markers of hemolysis do not correlate with directly measured erythrocyte survival in
sickle cell anemia. Am J Hematol 2016;91:1195-201
87. Muller-Eberhard U, Javid J, Liem HH, Hanstein A, Hanna M. Plasma concentration of
hemopexin, haptogloin, and heme in patients with various hemolytic diseases. Blood
1968;35(5):811-5
88. Van Beers EJ, Schaap MC, Berckmans RJ, Nieuland R, Sturk A et al. Circulating
erthrocyte derived microparticles are associated with coagulation activation in sickle cell
disease. Haematological;2009:94:1513-19
89. Setty BN, Kulkarni S, Rao AK, Stuart MJ. Fetal hemoglobin in sickle cell
disease:relationship to erythrocyte phosphatidylserine exposure and coagulation
activation. Blood 2000;96:1119-24
90. Liu C, Zhao W, Christ GJ, Gladwin MT, Kim-Shapiro DB. Nitric oxide scavenging by
red cell microparticles. Free Radic Biol Med 2013;65:1164-73
91. Ware RE. How I use hydroxyurea to treat young patients with SCA. Blood
2010;115(26):5300-11
92. Brittain EL, Janz DR, Austin O, Bastarache JA, Wheeler LA et al. Elevation of plasma
cell free hemoglobin in pulmnary hyperension. CHEST 2014;146(6):1478-85
93. Adisa OA, Hu Y, Ghosh S, Arycee D, Osunkwo I, Ofori-Acquah SF. Association between
plasma free haem and incidence of vaso-occlussive episodes and acute chest syndrome
in children with sickle cell disease. Br J Haematol 2013;162:702-5
94. Nebor D, Romana M, Santiago R, Vachiery N, Picot J et al. Fetal hemoglobin and
hydroxy carbamide modulate both plasma concentration and cellular origin of circulating
microparticles in sickle cell anemia children. Haematological 2013;98(6):862-67
95. Lezcano NE, Odo N, Kutlar A, Brambilla D, Adams RJ. Regular transfusion lowers
plasma free hemoglobin in children with sickle cell disease at risk of stroke.
Stroke.2006;37:1424-26
96. Piccin A, Murphy C, Eakins E, Kunde J, Corvetta D, Di Pierro A et al. Circulating
microparticles , protein C, free protein S, and enndothelial vascular markers in children
with sickle cell anemia. Journal of Extracellular vesicles 2015;4:28414
97. Gerotziafas GT, Van Dreden P, Chaari M, Galea V, Khaterchi A et al. The acceleration
of the propagation phase of thrombin generation in patients with steady state sickle cell
disease is associated with circulating erythrocyte –derived microparticles. Thromb
Haemost 2012;107:1044-52
98. Brunetta DM, De Santis GC, Silva-Pinto AC, Olivera de Olivera LC, Covas DT.
Hydroxyurea increases plasma concentrations of microparticles and reduces coagulation

128
activation and fibrinolysis in patients with sickle cell anemia. Acta Haematol
2015;133:287-94
99. Hebbel RP, Key NS. Microparticles in sickle cell anemia:Promise and pitfalls. Br J
Haematol 2017;174(1):16-29 doi:10.1111/bjh.14112
100. Westerman M, Porter JB. Red blood cell –derived microparticles:An overview.
Blood cells Mol Dis. 2016;59:134-9
101. Steinberg MH. Predicting clinical severity of sickle cell anemia. Br J Haematol.
2005;129:465-81
102. Minniti CP, Taylor JGt, Hildesheim M, O`Neal P, Wilson J et al. Laboratory and
echocardiography markers in sickle cell patients with leg leg ulcers. Am J hematol
2011;86:705-8
103. Minniti CP, Kato GJ. How we treat sickle cell patients with leg ulcers. Am J
Hematol 2016;91(1):22-30
104. Liem RI, Young LT, Thompson AA. Triscupid regurgitant jet velocity is
associated with hemolysis in children and young adults with sickle cell evaluated for
pulmonary hypertension. Haematologica 2007;92(11):1549-52
105. Mehari A, Alam S, Tian X, Cuttical MJ, Barnett CF. Hemodynamic predictors
of mortality in adults with sickle cell disease. Am J Respir Crit Care Med
2013;187(8):840-7
106. Gladwin MT, Sachdev V. Cardiovascular abnormalities in sickle cell disease. J
Am Coll Cardiol 2012;59(3):10.1016/j.jacc.2011.10900
107. Parent F, Bachir D, Inamo J, Lionnel F, Driss F. A hemodynamic study of
pulmonary hypertension in sickle cell disease. N Engl J Med 2011;365;44-53
108. Mehari A, Gladwin MT, Tian X, Machado RF, Kato GJ. Mortality in adults with
sickle cell disease and pulmonary hypertension. JAMA 2012;307(12):1254-56
109. Day TG, Drasar ER, Fulford T, Sharpe CC, Thein SL. Association between
hemolysis and albuminuria in adults with sickle cell anemia. Haematological
2012;97:201-5
110. Ataga KI, Derebail VK, Archer DR. The glomerulopathy of sickle cell disease.
Am J Hematol 2014;89:907-14
111. Eshbach ML, Kaur A, Rbaibi Y, Tejero J, Weisz OA. Hemoglobin inhibits
albumin uptake by proximal tubule cells: implications for sickle cell disease. Am J
Physiol 2017;312:C733-C740
112. Diop S, Sene A, Cisse M, Toure AO, Sow O et al. Prevalence and morbidity of
G6PD deficiency in sickle disease in the homozygote. Dakar Med 2000;50(2):56-60

129
113. Carpenter SL, Lieff S, Howard TA, Eggleston B, Ware RE. UGT1A1 promoter
polymorphisms and the development of hyperbilirubinemia and gallbladder disease in
children with sickle cell anemia. Am J Hematol. 2008;83:800-3
114. Schwertner HA, Vitek L. Gilbert syndrome,UGT1A1*28 allele, and
cardiovascular disease risk: Possible protective effects and therapeutic applications of
bilirubin. Atherosclerosis 2008;198:1-11
115. Ware R, Filston HC, Schultz WH, Kinney TR. Elective cholecystectomy in
young patients with sickle hemoglobinopathies. Ann Surg. 1988;208:17-22
116. Haberkern CM, Neumayr LD, Orringer EP, ett al. Cholecystectomy in sickle cell
anemia patients: Perioperative outcome of 364 cases from the National preoperative
Transfusion Study. Blood 1997;89:1533-42
117. Perera MA, Inocenti F, Ratan MJ. Pharmacology testing for Uridine Diphosphate
Glucuronosyltransferase 1A1 polymorphisms: Are we there yet? Pharmacotherapy.
2008;28(6):755-68
118. Chaouch L, Talbi E, Moumi I, Chaabene AB, Kalai M, Chaouachi D et al. Early
complication in sickle anemia children due to A (TA)n TAA polymorphism at the
promoter of UGT1A1 gene. Disease Markers;35(2):67-72
119. Chaouch L, Miniar K, Chaouchi D, Mallouli F, Hafsia R, Ben Ammar S et al.
Gilbert syndrome acts as a risk factor of developing gallstone among β hemoglobinopathy
Tunisians patients. Le Tunisie Medicale 2015;93(4):237-41
120. Hamad Z, Aljedai A, Halwani R, Alsultan A. UGT1A1promoter polymorphism
associated with serum bilirubin level in Saudi patients with sickle cell disease. Ann. Saudi
Med 2013;33(4):372-76
121. Haverfield EV, McKenzie CA, Forrester et al. UGT1A1 variation and gallstone
formation in sickle cell disease. Blood 2005;105(3):968-72
122. Damanhouri GA, Jarullah J, Marouf S, Hindawi SI, Mushtaq G, Kamal MA.
Clinical biomarkers in sickle cell disease. Saudi J Biological Sciences. 2015;22:24-31
123. Beutler E, Gelbart T, Demina A. Racial variability in the UDP-
glucuronosyltransferase1 (UGT1A1) promoter: a balanced polymorphism for the
regulation of bilirubin metabolism? Proc Natl Acad Sci1998;95:8170-74
124. Premawardhena A, Fisher CA, Liu YT et al. The global distribution of length
polymorphisms of the promoters of the glucuronoslytransferase 1 gene(UGT1A1):
hematologic and evolutionary implications. Blood Cells Mol Dis 2003;31:98-101
125. Fertrin KY, Goncalves MS, Saad STO, Costa FF. Frequencies of UDP-
Glucuronosyltransferase 1 (UGT1A1) gene promoter polymorphisms among distinct
groups from Brazil. Am J Med Genetics. 2002;108:117-19

130
126. Azevedo LA, Santin AP, Wagner SC, Zaleski CF, Bock H, Saiva-Pereira ML et
al. Prevalence of UGT1A1 Gene polymorphism in patients with haemolytic anemia in
Southern Brazil. Genet. Testing and Molecular Biomarkers. 2011;15 (1&2):107-110
127. AlFadhil S, Al-Jafer H, Hadi M, Al-Mutairi M, Nizam R. The effect of UGT1A1
promoter polymorphism in the development of hyperbilrubinemia and cholelithiasis in
hemoglobinopathy patients. PLoS ONE 8(10):e7768.doi:10.1371/journal.pone.0077681
128. Adekile A, Kutlar F, McKie K, Addington A, Elam D, Holley L. et al. The
influence of uridine diphosphate glucuronosyl transferase 1A promoter polymorphisms,
βs-globin gene haplotype and co-inherited α-thalssemia trait and HbF on steady state
serum bilirubin levels in sickle cell anemia. Eur J Haematol 2005;75:150-55
129. Huo D, Kim H, Adebamowo CA, Ogundiran TO, Akang E et al. Genetic
Polymorphisms in uridine diphosphoglucuronosyltransferase 1A1 and cancer risks in
Africans. Breast Cancer Res Treat. 2008;110:367-76
130. Kaplan M, Slusher T, Renbaum P, Essiet DF, Pam S, Levy-Lahad E et al. (TA)n
UDP-Glucuronosyltransferase1a1 Promoter polymorphism in Nigerian neonates. Pediatr
Res 2008;63:109-111
131. Chaar V, Keclard L, Diara JP, Leturdu C, Elion J, Krishnamoorthy R et al.
Association of UGT1A1 polymorphism with prevalence and age of onset of cholelithiasis
in sickle cell anemia. Haematological 2005;90(2):188-93
132. Adekile AD, Makanjuola D, Ultrasonography in children with sickle cell anemia.
Niger J Paediatr 1983;10:35-8
133. Nzeh DA, Adedoyin MA. Sonographic pattern of gallbladder disease in children
with sickle cell anemia. Pediatr Radiol 1989;19(5):290-2
134. Odunvbun ME, Adeyekun AA. Ultrasonic assessment of the prevalence of
gallstones in sickle cell disease children seen at the University of Benin Teaching
Hospital, Benin City, Nigeria. Niger J Paed. 2014;41(4):370-374
135. Darko R, Rodrigues OP, Oliver-Commey JO, Kotei CN. Gallstones in Ghanian
children with sickle cell disease. West Afr J Med 2005;24(4):295-8
136. Longo-Mbenza B, Ngiyulu R, Kizunda P, Kaluila M, Bikangi N. Gallbladder
disease in young Congolese with sickle cell anemia: an ultrasound survey. J Trop Pediatr
2004;5:73-7
137. Attalla BI, Sonographic findings in Sudanese children with sickle cell anemia.
J Diag Med Sonography 2010;26:276-80
138. Attalla BAI, Karrar ZA, Ibnouf G, Mohamed AO, Abdelwahab O, Nasir EM et
al. Outcome of cholelithiasis in Sudanese children with sickle cell anemia after a 13 years
follow up. Afr Hlth Sci 2013;13(1):154-59

131
139. Russo-Mancuso G, Romeo MA, Guardabasso V, Schiliro G. Survey of sickle cell
disease in Italy. Haematologica 1998;83:875-81
140. Passon RG, Howard TA, Zimmerman SA, Schultz WH, Ware RE. Influence of
bilirubin Uridine Diphosphate Glucuronoslytransferase 1A Promoter polymorphisms on
serum bilirubin levels and cholelithiasis in children with sickle cell anemia. J Pediatr
HematolOncol 2001;23:448-51
141. Gumeiro APS, Bellomo-Brandao MA, Costal-Pinto EAL.Gallstones in children
with sickle cell disease followed up at a Brazillian hematology center. Arq Gastroenterol
2008;45(4):313-18
142. Martins R, Morais A, Dias A, Soares I, Rolao C, Ducla-Soares JL et al. Eearly
modification of sickle cell disease clinical course by UDP-glucuronosyltransferase 1A1
gene promoter polymorphism. J Hum Genet 2008;524-28
143. Kumar S, Guha M, Choubey V, Maity P, Srivastava K, Puri S et al. Bilrubin
inhibits Plasmodium falciparum growth through the generation of reactive oxygen
species. Free Radic Biol Med 2008;44:602-13
144. Chaar V, Keclard L, Etienne-Julan M, Diara JP, Elion J, Krishnamoorthy R et al.
UGT1A1 Polymorphism outweighs the modest effect of deletional (-3.7kb) α-
Thalassemia on cholelithogenesis in sickle cell anemia. Am J Hematol 2006;81:377-79.
145. Figueiredo MS, Kerbauy J, Goncalves MS, Arruda VR, Saad STO et al. Effect of
α-thalassemia and β-globin gene cluster haplotypes on the hematological and clinical
features of sickle cell anemia in Brazil. Am J Hematol 1996;53:72-6
146. Adorno EV, Zanette A, Lyra I, Seixas MO, Reis MG et al. Clinical and molecular
characteristics of sickle cell anemia in the northeast of Brazil. Genetics Mol Biol
2008;31(3):621-25
147. Cardoso G, Guerreiro JF. Molecular characterization of sickle cell anemia in the
northern Brazilian state of Para. Am J Hum Biol 2010;22:573-77
148. Camilo-Araujo RF, Amancio OMS, Figueiredo MS, Cabanas-Pedro AC, Braga
JAP. Molecular analysis and associations with clinical and laboratory manifestations in
children with sickle cell anemia. Rev Bras Hematol Hemoter 2014;36(5):334-9
149. Mikobi TM, Lukusa PT, Aloni MN, Lumaka A, Akilimali PZ et al. Association
between sickle cell anemia and alpha thalassemia reveals a high prevalence of the α3.7
triplication in Congolese patients than in worldwide series. J Clin Lab Anal
2017;00:e22186:doi:10.1002/jcla.22186
150. Rumaney MB, Ngo Bitoungui VJ, Vorster AA, Ramesar R, Kengne AP et al. The
co-inheritance of alpha thalassemia and sickle cell anemia is associated with better
hematological indices and lower consultations rate in Cameroonian patients and could

132
improve their survival. PLoS ONE
2014;9(6):e100516.doi:10.1371/journal.pone.0100516
151. Renoux C, Connes P, Nader E, Skinner S, Faes C et al. Apha thalassemia
promotes frequent vaso-occlusive crises in children with sickle cell anemia through
haemorheological changes. Pediatr Blood Cancer
2017;64:e26455.doi:10.1002/pbc.26455
152. Falusi AG, Esan GJF, Ayyub H, Higgs DR. Alpha thalassemia in Nigeria: its
interactions with sickle cell disease. Eur J Haematol. 1987;38:370-75
153. Saraf SL, Akingbola TS, Shah BN, Ezekekwu CA, Sonubi O et al. Associations
of α-thalassemia and BCL11A with stroke in Nigerian, United States, and United
Kingdom sickle cell anemia cohorts. Blood Advances 2017; 1(11):693-8
154. Adekile AD, Liu JC, Sulzer AJ, Huisman THJ. Frequency of the α-thalassemia-
2 gene among Nigerian SS patients and its influence on malaria antibody titers.
Hemoglobin 1993;17(1):73-9
155. Wambua S, Mwacharo J, Uyoga S, Macharia A, Williams TN. Co-inheritance of
α-thalassemia and sickle cell trait results in specific effects on hematological parameters.
Br J Haematol 2006;133(2):206-9
156. Mockenhaupt FP, Ehrhardt S, Gellert S, Otchwemah RN, Dietz E et al. α+-
thalassemia protects African children from severe malaria Blood 2004;104:2003-6
157. Higgs DR, Aldridge BE, Lamb J, Clegg JB, Weatherall DJ et al. The interaction
of alpha thalassemia and homozygous sickle cell disease. N Engl J Med 1982;306:1441-
6
158. Steinberg MH. Predicting clinical severity of sickle cell anemia. Br J Haematol.
2005;129:465-81
159. Steinberg MH, Sebastiani P. Genetic modifiers of sickle cell disease. Am J
Hematol 2012;87(8):795-803
160. Koshy M, Entsuah R, Koranda A, Kraus AP, Johnson R et al. Leg ulcers in
patients with sickle cell disease. Blood 1989;74:1403-8
161. Minniti CP, Eckman J, Sebastiani P, Steinberg MH, Ballas SK. Leg ulcers in
sickle cell disease. Am J Hematol 2010;85:831-3
162. Serjeant GR, Higgs DR, Hambleton IR. Elderly survivors with homozygous
sickle cell disease. N Engl J Med 2007;356(6):642-3
163. Belisaro AR, Rodrigues CV, Martins ML, Silva CM, Viana MB. Coinheritance
of alpha thalassemia decreases the risk of cerebrovascular disease in a cohort of children
with sickle cell anemia. Hemoglobin 2010;34:516-29
164. Flanagan JM, Frohlich TA, Howard WH, Schultz C, Driscoll R et al. Genetic
predictors for stroke in children with sickle cell anemia. Blood 2011;117:6681-84

133
165. Filho IL, Leite AC, Moura PG, Ribeiro GS, Cavalcante FC et al. Genetic
polymorphisms and cerebrovascular disease in children with sickle cell anemia from Rio
de Janeiro, Brazil, Arq. Neuropsiquiatr 2011;69:431-5
166. Milner PF, Kraus AP, Sebes JI, Sleeper LA, Dukes KA et al. Sickle cell disease
as a cause of osteonecrosis of the femoral head. N Engl J Med 1991;325:1476-81
167. Mahadeo KM, Oyeku S, Taragin B, Rajpathak SN, Moody K et al. Increase
prevalence of osteonecrosis of the femoral head in children and adolescent with sickle
cell disease. Am J Hematol 2011;86(9):806-8
168. Borges E, Wening MR, Kimura EM, Gervasio SA, Costa FF, Sonati MF. High
prevalence of alpha thalassemia among individuals with microcytosis and hypochromia
without anemia. Braz J Med Biol Res 2001;34(6):759-62
169. Stevens GA, Finucane MM, De-Regil LM, Paciorek JC, Flaxman SR, Branca F.
Global, regional and national trends in hemoglobin concentration and prevention of total
and severe anemia in children and pregnant and non pregnant women 1999 – 2011. Lancet
Glob Health 2013;e16-e25.
170. Pierrot-Gallo BS, Vicari P, Matsuda SS, Adegoke SA, Mecabo G, Figueiredo
MS. Haptoglobin gene polymorphisms and interleukins 6 and 8 in patients with sickle
cell anaemia. Rev Bras Hematol Hemoter 2015;37(5):329-35
171. Santos MN. Haptoglobin: an emerging candidate for phenotypic modulation of
sickle cell anemia? Rev Bras Hematol Hemoter 2015;37(5)329-35
172. Platt OS, Thorington BD, Brambilla DJ, Milner PF, Rosse WF et al. Pain in sickle
cell disease. Rates and risk factors. N Engl J Med 1991;325:11-16
173. Platt OS, Brambilla DJ, Rosse WF, Milner PF, Castro O et al. Mortality in sickle
cell disease, Life expectancy and risk for early death. N Engl J Med 1994;330:1639-44
174. Lettre G, Sankaran VG, Bezerra MA, Araujo AS, Uda M et al. DNA
polymorphisms at the BCL11A, HBS1L-MYB, and β-globin loci associate with fetal
hemoglobin levels and pain crises in sickle cell disease. Proc. Natl. Acad.Sci. USA
2008;105(33):11869-74
175. Cardoso GL, Diniz IG, Martins da Silva AL, Cunha DA, Da Silva Junior JS et al.
DNA polymorphisms at the BCL11A, HBS1L-MYB, and Xmn1-HBG2 site loci
associate with fetal hemoglobin levels in sickle cell anemia patients from Northern Brazil.
Blood Cells Mol Dis 2014;53:176-9

134
APPENDICES
PULICATIONS IN CONGRESSES
Oladele Simeon Olatunya, Dulcineia Martins de Albuquerque, Daniela Pinheiro
Leonard, Kleber Y. Fertrin, Adekunle Adekile M, Fernando Ferreira Costa. Effects of
UGT1A1 polymorphism, glucose-6-phosphate dehydrogenase deficiency and
deletional (-3.7кb) α-thalassemia among young Nigerians with sickle cell anemia.
Blood 2017;130:2242 (American Society of Hematology 2017)
Oladele Simeon Olatunya, Carolina Lanaro, Ana Leda Longhini, Carla Fernanda Franco
Penteado, Kleber Y. Fertrin, Sara T.O. Saad, Adekunle Adekile, Fernando Ferreira
Costa. Red blood cells microparticles are associated with hemolysis markers and
leg ulceration in patients with sickle cell disease. Blood 2017;130:3510 (American
Society of Hematology 2017)
Oladele Simeon Olatunya, Dulcineia Martins de Albuquerque, Daniela Pinheiro
Leonard, Kleber Y. Fertrin, Adekunle Adekile M, Fernando Ferreira Costa. UGT1A1
promoter polymorphisms and their effects on clinical events and biomarkers of
Nigerian patients with sickle cell disease. FESBE Brasil 2017

135
MANUSCRIPTS SUBMITTED FOR PUBLICATION
MANUSCRIPT 1
Uridine Diphosphate Glucuronosyl Transferase 1A (UGT1A1) Promoter Polymorphism
is associated with hyperbilirubinemia and gallstone among young Nigerians with sickle
cell anaemia.
Authors:
Oladele Simeon Olatunya,a,b, Dulcineia Martins de Albuquerque,a Daniela Pinheiro
Leonard, a Kleber Y. Fertrin, a Adekunle Adekile,c, Fernando Ferreira Costa,a
Affiliations: aHematology and Hemotherapy Center, University of Campinas, São Paulo, Brazil bDepartment of Paediatrics, College of Medicine, Ekiti State University, Ekiti State, Nigeria cDepartment of Pediatrics, Faculty of Medicine, Kuwait University, Kuwait
Corresponding author and address for correspondence:
Oladele Simeon Olatunya Hematology and Hemotherapy Center (Hemocentro),
University of Campinas (UNICAMP),
Rua Carlos Chagas, 480
Barão Geraldo
Campinas 13083-970-SP, Brazil
Tel: +55 19 3521 8382
Email for correspondence: [email protected]

136
ABSTRACT
Background: (TA)n repeat sequence (rs8175347) of UGT1A1 gene promoter
polymorphism is associated with serum bilirubin levels and gallstones among different
sickle cell anaemia (SCA) populations. There are no data on UGT1A1 alleles and their
impact on Nigerian SCA patients.
Objectives: To determine the UGT1A1 genotypes, their association with laboratory
markers and clinical events among young Nigerians with SCA.
Patients and methods: One hundred and one SCA patients were studied and compared
with 64 healthy controls. The influence of UGT1A1 polymorphism on laboratory
parameters and clinical events of the patients was determined.
Results: Four (TA)n alleles:(TA)5, 6, 7, and 8 were found and associated with 10
genotypes:TA5/5, 5/6, 5/7, 5/8, 6/6, 6/7, 6/8, 7/7, 7/8, 8/8. The low- (TA) 7/7, 7/8, 8/8),
intermediate- (TA) 6/7, 6/8), and high-activity (TA) 5/5, 5/6, 5/7, 5/8, 6/5, 6/6,)
genotypes were found in 21.2%, 38.2%, and 40.6% participants respectively. There
were significant differences in serum bilirubin and lactate dehydrogenase (LDH) of the
patients when differentiated by the UGT1A1 genotype activity (p˂0.05). Asymptomatic
gallstones were found in 5.9% of patients and were significantly of low-activity
genotypes sub-group 5 (20%) vs 1(1.3%) p=0.0033. Although, bilirubin and HbF of
patients with gallstones were significantly different from those without gallstone, only
the serum bilirubin was associated with UGT1A1 genotypes on multivariate analysis
(p<0.0001).

137
Conclusion: This study confirms that UGT1A1 genotypes influence bilirubin levels and
development of gallstones among young Nigerians with SCA. Children with SCA
should be screened for UGT1A1 polymorphism and gallstones for holistic care.
Keywords: Sickle cell anaemia, Serum bilirubin, Gallstone, UGT1A1 polymorphism,
Nigeria.
INTRODUCTION
Sickle cell disease (SCD) is a common genetic disorder among Africans. Individuals
with the disease have variable clinical expression but homozygosity for the HbS gene,
also known as sickle cell anaemia (SCA), is the most severe form [1]. Children with
SCA have chronic hemolysis, leading to accumulation of serum bilirubin and
consequent gallstones [2]. Bilirubin is a tetrapyrol that results from the breakdown of
heme in red blood cells. At moderate levels, it is thought to protect against oxidative
stress and inflammatory injuries and some infectious diseases [3-5]. However, excessive
bilirubin levels, as seen in patients with chronic hemolysis, have been linked to
increased incidence of gallstones [1,2,5]. In children with SCA, this risk increases with
advancing age with a cumulative incidence of approximately 50% by adulthood and
some of them may need cholecystectomy [2,6,7].
Uridine diphosphate glucoronosyltransferase 1A isoform 1 (UGT1A1) is a member of
the superfamily of phase II conjugating enzymes that aids the elimination of bilirubin,
drugs and a vast variety of endogenous and exogenous substrates by adding a
glucuronide moiety to the substrates [8,9]. Genetic mutations resulting in absence or
severely reduced UGT1A1 activity leads to Criggler Najjar syndrome, which is

138
characterized by severely elevated serum bilirubin and increased risk of kernicterus
[10]. However, variations in (TA)n tandem repeat sequence within the TATA box
promoter region affect UGT1A1 gene expression and the activity of its (TA)n four
alleles, namely; (TA) 5, 6, 7, and 8 genotypes leading to moderate elevation of serum
bilirubin [9]. There is a negative association between the UGT1A1 and repeat length of
the four alleles attributable to the decreasing promoter activity acting via altered affinity
for the TATA–binding protein [9]. Based on this, the UGT1A1 (TA)n genotypes have
been classified into three sub groups namely; the high-activity genotype subgroup made
up of (TA)5/5, (TA)5/6, (TA)5/7, (TA)5/8, and (TA)6/6; intermediate-activity (TA)6/7,
and (TA)6/8, and low-activity group comprising (TA)7/7, (TA)7/8, (TA)8/8 [9].
Although homozygosity for (TA)7 alleles i.e. (TA)7/7 has been described generally as
Gilbert syndrome genetic hallmark, [2,11], there is an inverse relationship between the
serum bilirubin levels across these subgroups based on the degree of the genotype
activity such that, individuals with low-activity genotypes have elevated levels of serum
bilirubin and are therefore subjected to the modulating effects of higher serum bilirubin
levels including susceptibility to gallstone development [9,11].
Despite the huge burden of SCA in Africa [1], with Nigeria being the country with its
highest burden in the world [12], there is little understanding of the contributions of
genetic modifiers of SCA phenotypes in the country. To the best of our knowledge,
there are no data on the effects of UGT1A1 polymorphisms on the clinical expression of
Nigerian SCA patients. The aim of this study was to determine the UGT1A1 genotypes,
their association with laboratory parameters as well as clinical events in young Nigerian
patients with SCA.
PATIENTS AND METHODS

139
Study participants and settings
The study was conducted on 101 hydroxyurea-naïve children and adolescents with SCA
aged between 2 and 21years (median of 9 years) who are regular attendees at the
paediatric hematology unit of the Ekiti State University Teaching Hospital (EKSUTH),
Ado Ekiti, Ekiti State, in Southwest Nigeria. Sixty four healthy children who
accompanied their siblings to the paediatric haematology clinic or attended the
paediatrics outpatients` well-child clinic of the hospital served as the controls. To
qualify for inclusion, the SCA participants must have been on regular follow up at the
clinic for a minimum of one year prior to recruitment with up-to-date hospital records.
Participants with confirmed or suspected liver or other chronic diseases apart from SCA
were excluded. Also excluded were the few SCA patients on regular blood transfusion
and hydroxyurea therapies.
Ethical considerations
The study was approved by the Ethics and Research Committee of EKSUTH no:
A67/2016/03/003. Written informed consent of parents/caregivers as well as patients’
assents and consents were obtained as applicable after explaining the purpose of the
study to them in clear and plain language.
Data collection
Clinical and laboratory data
A tested chart review form was used to extract relevant information from the hospital
records of participants regarding their steady-state laboratory parameters and clinical
events. Average of at least two steady state results of laboratory parameters performed
between 3 to 6 months intervals by standard techniques were recorded for each

140
participants. The steady state parameters included the complete blood performed by
Sysmex KX21N Hematology analyser (Sysmex Corporation, Kobe, Japan). The serum
lactate dehydrogease (LDH), bilirubin, aspartate transaminase (AST), and alanine
transaminase (ALT) were measured with standard techniques. The quantitative
assessment of HbF, HbA, HbA2, HbS, and HbC was done by high performance liquid
chromatography (HPLC, Bio-Rad Variant D10, USA). Steady state was defined as
being free from any acute event(s) for at least one month and transfusion free for at least
four months [13].
Other information retrieved from patients’ charts included the biodata and details of the
clinical evolution of SCA such as number of bone pain crises requiring admission
and/or administration of opioids within the preceding one year, presence of leg ulcer,
priapism, overt osteonecrosis and/or overt stroke as well as presence of gallstone as
determined by serial abdominal ultrasound scans conducted on the patients as clinically
indicated. Gallstone was diagnosed on the basis of echodense images within the gall
bladder with acoustic shadowing or gravitational changes [14]. In addition, the clinical
records of the patients diagnosed with gallstone by ultrasound were examined for the
presence or absence of symptoms, and or treatment(s) for gallstone complications. The
definitions of clinical events were as previously described [15].
Genetic studies
These were carried out at the Centro de Hematologia e Hemoterapia (Hemocentro),
UNICAMP, Campinas, Sao Paulo State, Brazil. SCA was initially diagnosed by
hemoglobin electrophoresis and high performance liquid chromatography (HPLC) and
was confirmed by DNA studies.

141
The DNA of each participant extracted from each participant by Qiagen QIAamp DNA
Blood Mini Kit Cat No. 51104 Germany), was used to confirm the diagnosis of SCD by
polymerase chain reaction (PCR).
The rs8175347 identification was performed by Polymerase Chain Reaction (PCR) using
a forward primer 5'- (6-FAM) labelled (*) for detection by fragment analysis in capillary
electrophoresis system. The PCR reaction was prepared in 30 µL volume with 100ng of
genomic DNA; 1X Reaction Buffer (BIOTOOLS B&M Labs, Spain); 2.16mM MgCl2;
1.33 mM of dNTP mix; 133 nM of each primer (Integrated DNA Technologies,
Coralville, Iowa) named UGT1A1_*F: GTCACGTGACACAGTCAAAC and
UGT1A1_R: CAACAGTATCTTCCCAGCATG; and 1 U Taq DNA Polymerase
(BIOTOOLS B&M Labs, Spain). Thermal cycle conditions were as follows: preheating
at 96°C by 2 minutes, followed by 25 cycles of 96°C for 30 seconds, 58°C for 40 seconds,
and 72°C for 40 seconds. An ended step at 72°C for 30 min was performed to promote
adenylation of the PCR products. The PCR product (1 μL) was added to 8.7 μL Hi-Di
Formamide (Applied Biosystems, Carlsbad, CA) and 0.3 μL of a GeneScan™ 500 LIZ™
size standard (Applied Biosystems, Carlsbad, CA) and the fragments ranged from 197 -
203 bp, corresponding to (TA)5 - (TA)8 repeats, respectively, were separated by capillary
electrophoresis on a ABI3500 Genetic Analyzer and analysed by Gene Mapper v 4.1
Software (both Applied Biosystems, Carlsbad, CA).16,17 All DNA studies were carried
out blinded regarding the clinical and laboratory parameters of the participants. The
UGT1A1 genotypes were further classified into three subgroups namely: low,
intermediate and high activity subgroups as previously described [9].
Data Analysis

142
Statistical analysis was performed with the GraphPad Prism Program, version 5 for
Windows (San Diego, California, USA). The normal distribution of the quantitative
variables was verified by the Kolmogorov-Smirnov and Shapiro-Wilk tests. The
frequencies of variables were described and the significance of differences between
groups of patients was assessed using the Kruskal-Wallis analysis of variance
(ANOVA), chi-square, Mann-Whitney or Fisher`s exact tests as appropriate. Odd ratios
were obtained by applying logistic regression to determine the effects of UGT1A1
promoter polymorphism using the UGT1A1 genotype as the independent variable and
other outcomes of interest as the dependent variables. The test for Hardy-Weinberg
equilibrium was performed using the R-Project for statistical computing web tool
available at https://www.R-project.org/. Level of significance was set at P < 0.05 for
all statistical analyses.
RESULTS
The 101 patients with SCA consisted of 66 males and 35 females with median
age of 9, range 2 - 21years. The controls were made up of 19 sickle cell trait (HbAS)
and 45 haemoglobin HbAA, median age of 8 range 2 - 18years (p=0.4260), and 41
males. The SCA patients have been on follow up for a median of 4years, range 1-
14years.
UGT1A1 genotypes
Four (TA)n alleles: (TA)5, 6, 7, and 8 were found with gene frequencies of 0.11, 0.43,
0.41 and 0.05 respectively. The alleles were associated with 10 genotypes:TA5/5, 5/6,
5/7, 5/8, 6/6, 6/7, 6/8, 7/7, 7/8, 8/8 (Figure 1). The low (TA) 7/7, 7/8, 8/8), intermediate
(TA) 6/7, 6/8), and High (TA) 5/5, 5/6, 5/7, 5/8, 6/6,) activity genotypes were found in
35 (21.2%), 63 (38.2%), and 67 (40.6%) of the participants respectively. The low

143
activity genotypes were found in 25 (24.7%) patients and 10 (15.6%) of the controls
(P=0.1773). Homozygous (TA)n TA7/7 was found in 22 (21.7%) patients and 5 (7.8%)
controls p=0.018, (Table1) The observed genotype distributions of the patients and
control group were not significantly different from the values expected under Hardy-
Weinberg equilibrium (ᵡ2=15.10, df= 9, p=0.09), and (ᵡ2=11.86, df= 9, p=0.22),
respectively.
Comparison of serum bilirubin and other laboratory parameters between patients
and controls
There were significant differences between the patients and controls in all laboratory
parameters p<0.0001 respectively. (Table 2)
Effects of UGT1A1 genotype on serum bilirubin and other laboratory parameters
of patients
Both the total bilirubin and unconjugated bilirubin levels showed a trimodal pattern
across the UGT1A1 genotype subgroups with the low affinity genotype group having
the highest levels of serum bilirubin (p<0.0001). The LDH also showed this trimodal
pattern (p=0.0386). However, this was not demonstrated by the other remaining
laboratory parameters (Table 3).
Effects of UG1TA1 genotype on clinical events
Asymptomatic gallstones were found in 6 (5.9%) patients. Patients who had
gallstones significantly belonged to the subgroup with low activity genotypes 5 (20%)
vs 1(1.3%) p=0.0033, (Table 4). These were 2 females and 4 males. The two females
were aged 10 and 13 years. The males consisted of a 16-year-old boy with three others

144
aged 10, 13, and 15 years respectively. Four of the patients with gallstone had TA 7/7
genotypes, one TA 7/8, and TA 6/7 each.
Comparison of laboratory parameters between patients with and without
gallstones.
There were significant differences between the serum bilirubin and HbF levels
of patients with gallstones when compared with those without gallstone in general. No
difference was observed in the LDH and age of the two groups. Furthermore, when
those with gallstones were compared with age- and sex-matched peers within the same
UGT1A1 genotype subgroup, only serum bilirubin and HbF showed significant
differences between the two groups (Table 5).
Relationship between serum bilirubin and other parameters of patients
The total serum bilirubin correlated positively with the age of the patients ( r =0.238,
p=0.013), and their LDH levels (r = 0.218, p=0.028). Conversely, it showed a negative
correlation with the HbF levels (r = -0.210, p= 0.035). No significant correlation was
found between the total serum bilirubin and other biomarkers.
Relationship between UGT1A1 genotypes and other parameters by multivariate
analysis.
The unconjugated bilirubin was significantly associated with the low activity UGT1A1
genotypes (Adjusted Odd Ratio (1.08), 95% Confidence interval (1.034768 –
1.127873), P<0.0001). Also, significant association was found with the total bilirubin
when it was used in place of unconjugated bilirubin in the logistic regression model
(Adjusted Odd Ratio (1.05), 95% Confidence interval (1.029172 – 1.089832),
P<0.0001). No association was found with the other laboratory parameters.

145
DISCUSSION
There are gaps on the knowledge of impacts of genetic modifiers of SCA among
Africans. This is partly due to the lack of data and adequate infrastructure. Given that
genetic influences described among a specific population are not necessarily found in
others, it is pertinent that more studies are carried out among many cohorts to fully
understand the impact of genetic markers on SCA.
This study confirms the variability of bilirubin levels based on the activity of the
UGT1A1 genotypes as previously reported [2,4-5, 8-9,14]. However, we are not aware
of any previous study that has described the trimodal pattern of LDH based on UGT1A1
genotypes activity as found in this study. While the UGT1A1 modulation of serum
bilirubin levels is well understood [2,4,8,9,11,14,18-19], the exact mechanism through
which UGT1A1 could be associated with LDH is not clear. However, it may be possible
that there could be a link through hemolysis because both bilirubin and LDH are
derived from RBC and are markers of hemolysis [20]. UGT1A1 plays an important role
in haem catabolism upon its release from RBC and conversion to bilirubin [2,5,8,9].
Given the association of LDH with some phenotypes of SCA [20,21], we suggest there
is need for future research to unravel if there is any link between LDH and UGT1A1
activity.
Gilbert syndrome(GBS) has been described in individuals with the TA7/7 genotype and
[2,4,5,9,11,14,18], this was more common among our patients 22 (21.7%) vs 5 (7.8%)
controls (p=0.018). This difference could probably be due to the small number of the
controls. Nonetheless, the proportion of patients with TA7/7 genotype, in this study, is
higher than between 6 -11% described among Europeans [22,23], 11.7% in Saudi

146
population [18], and between 3-18% among Brazilians of different descents [24-26].
Similarly, it is higher than the 6% found among Kuwait SCA patients [27], and
between 5 and 11% described among other Africans [11,23]. However, this is lower
than 32% described among the SCA patients in the USA [28]. Nevertheless, the TA7/7
genotype prevalence in this study is comparable to between 18.2% and 20.3% earlier
described among Nigerians with non SCD-related illnesses [29,30]. Besides the TA7/7
genotype, other UGT1A1 genotypes found in this study have been described among
Africans [9,23]. These observations indicate that the UGT1A1 genotype is quite
variable among Nigerians and confirm the suggestions that the expression of the
UGT1A1 genotype variants is heterogeneous among Africans compared to the
Caucasians [9,22,23].
Our finding that the low-activity UGT1A1 genotype was associated with gallstones
confirms previous observations that SCA patients with the low-activity UGT1A1
genotypes especially the TA7/7, are at risk of developing gallstones [2,6,7,11,14,18].
Also, as found in this study, others [11,14,31], have reported that some other low-
activity genotypes like TA7/8 and TA8/8 predispose SCA patients to gallstones.
The proportion of patients with asymptomatic gallstones in this study, (5.9%), is
comparable to between 4-6% earlier reported among Nigerian children of similar age to
our SCA cohorts [32-34], This is also similar to the 4% found in Ghana [35], a close
neighbour to Nigeria. However, the gallstone prevalence in this study is lower than
between 9 – 58% that have been reported for some other African children with SCA of
similar age group [36-38]. Similarly, higher prevalence of between 26% and 30% was
reported for SCA cohorts of same age range as our patients in Italy [39] and the USA
[40] respectively. In the same vein, a higher prevalence of 45% was found among a
cohort of Brazilian children with SCD following a median follow up of 7 years [41].

147
These observations highlight the variations in propensity to gallstone development
among children with SCA from different backgrounds. Persistent higher serum bilirubin
is a risk factor for lithogenesis among SCA patients [2,18,25,27]. Also, diets and
environmental factors have also been implicated in explaining the variations in
propensity for gallstone formation among SCA [38,40]. Hence, the observed similarity
between the rates of gallstones in this study and earlier reports from Nigeria [32-34]
and Ghana [35], could be attributed to the two countries belonging to the West Africa
region and being perhaps, expose to similar diets and environmental factors compared
to their colleagues in other distant African parts, or in Europe, and Americas. In
addition to these earlier mentioned possibilities, genetic variabilities among Africans
and between Africans and Europeans and/or Americans could play some roles. The age
of onset and the apparent lack of initial symptoms attributable to gallstones, as found in
this study, have been reported [31,34,38, 40-42]. However, results of follow-up studies
have indicated that the prevalence of gallstones and its complications increase with age
of children with SCA [2,27,31,38,41] hence, the need to closely follow up these
patients.
Despite the observation that the UGT1A1 low -activity genotype is a leading factor in
hyperbilirubinemia and lithogenesis among SCA patients [2,6,7,42,43], the impact of
UGT1A1 polymorphism on the gallstone phenotype among the Nigerian SCA patients
was unknown prior to this study as none of the previous studies from Nigeria examined
the UGT1A1 of the patients [32-34]. Hence, to the best of our knowledge, the
contribution of this polymorphism to lithogenesis and hyperbilirubinemia among
Nigerian patients with SCA is being described for the first time in this study. This study
has shown that SCA children with the low-activity UGT1A1 genotypes had higher

148
bilirubin levels compared to others. In addition, we found that the low-activity
genotypes were associated with gallstones.
Although patients with gallstone in this study had higher serum bilirubin levels and
lower HbF levels as previously reported [28], following multivariate analysis, serum
bilirubin was the only laboratory parameter associated with the UGT1A1 genotype.
Therefore, it thus appears that the pathway to higher serum bilirubin and probably
gallstone development in our patients is not exclusively driven by hemolysis and the
ameliorating effect of HbF on hemolysis but also, by the influence of UGT1A1
genotype activity.
Beyond bilirubin metabolism and gallstone development, it has been suggested that
moderately elevated serum bilirubin can inhibit bacteria and Plasmodium falciparum
replication. Also it was hypothesised that, perhaps, the heterogeneity of UGT1A1
genotypes among Africans is a result of genetic evolution to confer selective advantage
by protecting from malaria in a way similar to other genetic traits like G6PD deficiency
and/or alpha thalassemia [5,9,23,44], hence, the occurrence of these possibilities could
be investigated through a thorough prospective study.
In conclusion, this study confirms for the first time that UGT1A1 genotypes are tightly
associated with bilirubin levels and development of gallstone among young Nigerians
with SCA. In addition, it also suggests that the pathway to elevated serum bilirubin and
gallstone development among our study cohorts seems not to be exclusively driven by
hemolysis. These observations are in agreement with earlier reports that UGT1A1
polymorphisms influence bilirubin metabolism [11,14,28,43,45], and highlight the
contribution of UGT1A1 polymorphisms, a non-globin genetic factor, to the clinical

149
manifestations of SCA patients. Children with SCA in developing countries should be
screened for UGT1A1 polymorphisms and gallstones in order to allow for holistic care.
FUNDING AND DISCLOSURES
This study was supported by grants No 2014/00984-3 from FAPESP, and grants No
2015/141693-0 from CNPq, Brazil.
The authors declare no conflict of interest with respect to this study. All authors
contributed to critical aspects of the study. OSO, AA, and FFC, conceived the study.
OSO Wrote the paper, participated in data collection, analysis and patients`
management and follow up. DMA & DPL, performed the genetic studies, OAF, & TSK
data collection & analysis. KYF manuscript review. All authors participated in
reviewing the manuscript for important intellectual contents and agreed to the final
version.
ACKNOWLEDGEMENTS
Authors acknowledge with thanks the supports received from participants and their
caregivers/parents during the study.
REFERENCES
[1]. Rees DC, Williams TN, Gladwin MT. Sickle cell disease. Lancet.
2010;376:2018-2031
[2]. Carpenter SL, Lieff S, Howard TA, Eggleston B, Ware RE. UGT1A1
promoter polymorphisms and the development of hyperbilirubinemia and
gallbladder disease in children with sickle cell anemia. Am J Hematol.
2008;83:800-803

150
[3]. Stocker R, Yamamoto Y, McDonagh A, Glazer A. Bilirubin is an
antioxidant of possible physiological importance. Science. 1987;235:1043-1046
[4]. Schwertner HA, Vitek L. Gilbert syndrome,UGT1A1*28 allele, and
cardiovascular disease risk: Possible protective effects and therapeutic
applications of bilirubin. Atherosclerosis 2008;198:1-11
[5]. Italia KY, Jijina FF, Jain D, Merchant R, Nadkarni AH, Mukherjee M, et al.
The effect of UGT1A1 promoter polymorphism on bilirubin response to
hydroxyurea therapy in haemoglobinopathies. Clinical Biochemistry
2010;43:1329-1332
[6]. Ware R, Filston HC, Schultz WH, Kinney TR. Elective cholecystectomy in
young patients with sickle hemoglobinopathies. Ann Surg. 1988;208:17-22
[7]. Haberkern CM, Neumayr LD, Orringer EP, ett al. Cholecystectomy in sickle
cell anemia patients: Perioperative outcome of 364 cases from the National
preoperative Transfusion Study. Blood 1997;89:1533-1542
[8]. Perera MA, Inocenti F, Ratan MJ. Pharmacology testing for Uridine
Diphosphate Glucuronosyltransferase 1A1 polymorphisms: Are we there yet?
Pharmacotherapy. 2008;28(6):755-768
[9]. Horsefall LJ, Zeitlyn D, Tarekegn A, Bekele E, Thomas MG, Bradman N et
al. Prevalence of clinically relevant UGT1A1 Alleles and haplotypes in African
population. Annals of Human Genetics 2011;75:236-246
[10]. Kadakol A, Ghosh SS, Sappal BS et al. Genetic lesions of bilirubin
uridine-diphosphoglucuronate glucuronosyltransferase (UGT1A1) causing
Criggler-Najar and Gilbert Syndromes: correlation of genotype to phenotype.
Hum Mutat 2000;16:297-306

151
[11]. Chaouch L, Talbi E, Moumi I, Chaabene AB, Kalai M, Chaouachi D et al.
Early complication in sickle anemia children due to A (TA)n TAA
polymorphism at the promoter of UGT1A1 gene. Disease Markers;35(2):67-72
[12]. Diakwu-Akinwumi IN, Abubakar SB, Adegoke SA, Adeleke S, Adewoye
O, Adeyemo T. et al Blood Transfusion Services for patients with Sickle Cell
Disease in Nigeria. Int. Health. 2016;8(5):330-335
[13]. Ballas SK. More definitions in sickle cell disease: Steady state v baseline.
Am J Hematol 2011;86:338
[14]. Chaouch L, Miniar K, Chaouchi D, Mallouli F, Hafsia R, Ben Ammar S et
al. Gilbert syndrome acts as a risk factor of developing gallstone among β
hemoglobinopathy Tunisians patients. Le Tunisie Medicale 2015;93(4):237-241
[15]. Ballas SK, Lieff S, Benjamin LJ, Dampier CD, Heeney MM, Hope C.
Definitions of phenotypic manifestations of sicle cell disease. Am J Hematol.
2010;85:6-13
[16]. Abou Tayoun AN, de Abreu FB, Lefferts JA, Tsongalis GJ. A clinical PCR
frangment analysis assay for TA repeat sizing in the UGT1A1 promoter region.
Clinca Chimica Acta 2013;422:1-4
[17]. Gupta N, Benjamin M, Kar A, Munjal SD, Sarangi AN, Dalal A et al.
Identification of promoter and Exonic variations, and functional characterisation
of a splice site mutation in Indian patients with unconjugated hyperbilrubinemia.
PLoS ONE 10 (12): e0145967, doi:10.1371/journal.pone.0145967
[18]. Hamad Z, Aljedai A, Halwani R, Alsultan A. UGT1A1promoter
polymorphism associated with serum bilirubin level in Saudi patients with sickle
cell disease. Ann. Saudi Med 2013;33(4):372-376

152
[19]. Haverfield EV, McKenzie CA, Forrester et al. UGT1A1 variation and
gallstone formation in sickle cell disease. Blood 2005;105(3):968-972
[20]. Damanhouri GA, Jarullah J, Marouf S, Hindawi SI, Mushtaq G, Kamal
MA. Clinical biomarkers in sickle cell disease. Saudi J Biological Sciences.
2015;22:24-31
[21]. Kato GJ, McGowan V, Machado RF, Little JA, Taylor VI J et al. Lactate
dehydrogenase as a biomarker of hemolysis-associated nitric oxide resistance,
priapism, leg ulceration, pulmonary hypertension, and death in patients with
sickle cell disease. Blood 2006; 107(6):2279-2285.
[22]. Beutler E, Gelbart T, Demina A. Racial variability in the UDP-
glucuronosyltransferase1 (UGT1A1) promoter: a balanced polymorphism for the
regulation of bilirubin metabolism? Proc Natl Acad Sci1998;95:8170-8174
[23]. Premawardhena A, Fisher CA, Liu YT et al. The global distribution of
length polymorphisms of the promoters of the glucuronoslytransferase 1
gene(UGT1A1): hematologic and evolutionary implications. Blood Cells Mol
Dis 2003;31:98-101
[24]. Fertrin KY, Goncalves MS, Saad STO, Costa FF. Frequencies of UDP-
Glucuronosyltransferase 1 (UGT1A1) gene promoter polymorphisms among
distinct groups from Brazil. Am J Med Genetics. 2002;108:117-119
[25]. Fertrin KY, Melo MB, Assis AM, Saad STO, Costa FF. UDP-
glucuronosyltransferase 1 gene promoter is associated with increased serum
bilirubin levels and cholecystectomy in patients with sickle cell anemia. Clin
Genet. 2003;64:160-162
[26]. Azevedo LA, Santin AP, Wagner SC, Zaleski CF, Bock H, Saiva-Pereira
ML et al. Prevalence of UGT1A1 Gene polymorphism in patients with

153
haemolytic anemia in Southern Brazil. Genet. Testing and Molecular
Biomarkers. 2011;15 (1&2):107-110
[27]. AlFadhil S, Al-Jafer H, Hadi M, Al-Mutairi M, Nizam R. The effect of
UGT1A1 promoter polymorphism in the development of hyperbilrubinemia and
cholelithiasis in hemoglobinopathy patients. PLoS ONE
8(10):e7768.doi:10.1371/journal.pone.0077681
[28]. Adekile A, Kutlar F, McKie K, Addington A, Elam D, Holley L. et al. The
influence of uridine diphosphate glucuronosyl transferase 1A promoter
polymorphisms, βs-globin gene haplotype and co-inherited α-thalssemia trait and
HbF on steady state serum bilirubin levels in sickle cell anemia. Eur J Haematol
2005;75:150-155
[29]. Huo D, Kim H, Adebamowo CA, Ogundiran TO, Akang E et al. Genetic
Polymorphisms in uridine diphosphoglucuronosyltransferase 1A1 and cancer
risks in Africans. Breast Cancer Res Treat. 2008;110:367-376
[30]. Kaplan M, Slusher T, Renbaum P, Essiet DF, Pam S, Levy-Lahad E et al.
(TA)n UDP-Glucuronosyltransferase1a1 Promoter polymorphism in Nigerian
neonates. Pediatr Res 2008;63:109-111
[31]. Chaar V, Keclard L, Diara JP, Leturdu C, Elion J, Krishnamoorthy R et al.
Association of UGT1A1 polymorphism with prevalence and age of onset of
cholelithiasis in sickle cell anemia. Haematological 2005;90(2):188-193
[32]. Adekile AD, Makanjuola D, Ultrasonography in children with sickle cell
anemia. Niger J Paediatr 1983;10:35-38
[33]. Nzeh DA, Adedoyin MA. Sonographic pattern of gallbladder disease in
children with sickle cell anemia. Pediatr Radiol 1989;19(5):290-292

154
[34]. Odunvbun ME, Adeyekun AA. Ultrasonic assessment of the prevalence of
gallstones in sickle cell disease children seen at the University of Benin
Teaching Hospital, Benin City, Nigeria. Niger J Paed. 2014;41(4):370-374
[35]. Darko R, Rodrigues OP, Oliver-Commey JO, Kotei CN. Gallstones in
Ghanian children with sickle cell disease. West Afr J Med 2005;24(4):295-298
[36]. Longo-Mbenza B, Ngiyulu R, Kizunda P, Kaluila M, Bikangi N.
Gallbladder disease in young Congolese with sickle cell anemia: an ultrasound
survey. J Trop Pediatr 2004;5:73-77
[37]. Attalla BI, Sonographic findings in Sudanese children with sickle cell
anemia. J Diag Med Sonography 2010;26:276-280
[38]. Attalla BAI, Karrar ZA, Ibnouf G, Mohamed AO, Abdelwahab O, Nasir
EM et al. Outcome of cholelithiasis in Sudanese children with sickle cell anemia
after a 13 years follow up. Afr Hlth Sci 2013;13(1):154-159
[39]. Russo-Mancuso G, Romeo MA, Guardabasso V, Schiliro G. Survey of
sickle cell disease in Italy. Haematologica 1998;83:875-881
[40]. Passon RG, Howard TA, Zimmerman SA, Schultz WH, Ware RE.
Influence of bilirubin Uridine Diphosphate Glucuronoslytransferase 1A
Promoter polymorphisms on serum bilirubin levels and cholelithiasis in children
with sickle cell anemia. J Pediatr HematolOncol 2001;23:448-451
[41]. Gumeiro APS, Bellomo-Brandao MA, Costal-Pinto EAL.Gallstones in
children with sickle cell disease followed up at a Brazillian hematology center.
Arq Gastroenterol 2008;45(4):313-318
[42]. Martins R, Morais A, Dias A, Soares I, Rolao C, Ducla-Soares JL et al.
Eearly modification of sickle cell disease clinical course by UDP-

155
glucuronosyltransferase 1A1 gene promoter polymorphism. J Hum Genet
2008;524-528
[43]. Milton JN, Sebastiani P, Solovieff N, Hartley SW, Bhatnagar P, Arking
DE et al. A Genome-wide association study of total bilirubin and cholelithiasis
risk in sickle cell anemia. PLoS ONE 2012; 7(4):e34741.
Doi10.1371/journal.pone.0034741
[44]. Kumar S, Guha M, Choubey V, Maity P, Srivastava K, Puri S et al.
Bilrubin inhibits Plasmodium falciparum growth through the generation of
reactive oxygen species. Free Radic Biol Med 2008;44:602-613
[45]. Chaar V, Keclard L, Etienne-Julan M, Diara JP, Elion J, Krishnamoorthy R
et al. UGT1A1 Polymorphism outweighs the modest effect of deletional (-3.7kb)
α-Thalassemia on cholelithogenesis in sickle cell anemia. Am J Hematol
2006;81:377-379.

156
Figure 1: UGT1A1 promoter genotypes found among participants.
A: TA5/TA5; B: TA5/TA6; C: TA5/TA7; D: TA5/TA8; E: TA6/TA6; F: TA6/TA7; G: TA6/TA8; H: TA7/TA7; I: TA7/TA8; J: TA8/TA8
Table 1: Allele and genotype frequencies of UGT1A1 promoter polymorphism among
participants

157
Variables SCA
N=101
AS
N=19
AA
N=45
Allelotypes Freq n (%) Freq n (%) Freq n (%)
(TA) 5 18 (11.7) 2 (6.7) 10 (12.5)
(TA)6 67 (43.5) 16 (53.3) 28 (35.0)
(TA)7 61 (39.6) 10 (33.3) 37 (46.2)
(TA)8 8 (5.2) 2 (6.7) 5 (6.3)
UGT1A1
Genotypes
SCA (N=101) AS (N=19) AA (N=45)
Genotypes Freq n (%) Freq n (%) Freq n (%)
TA5/5 0 (0) 0 (0) 1 (2.2)
TA5/6 9 (8.9) 0 (0) 1 (2.2)
TA5/7 6 (6.0) 1 (5.2) 8 (17.7)
TA5/8 3(2.9) 0 (0) 0 (0)
TA6/6 25 (24.7) 8 (42.1) 5 (11.1)
TA6/7 31 (30.7) 7 (36.8) 21 (46.7)
TA6/8 2 (2.0) 1 (5.2) 1 (2.2)
TA7/7 22 (21.7) 1 (5.2) 4 (8.9)
TA7/8 2 (2.0) 1 (5.2) 4 (8.9)
TA8/8 1 (1.0) 0 (0) 0 (0)
SCA (N=101) AS (N=19) AA (N=45)
UGT1A1
Genotypes by
degree of Activity
Freq n (%) Freq n (%) Freq n (%)
Low-Activity
genotypes
TA (7/7, 7/8, 8/8)
25 (24.7) 2 (10.5) 8 (17.8)

158
Intermediate-
Activity genotypes
(TA6/7, TA6/8)
33 (32.7) 8 (42.1) 22 (48.9)
High-Activity
genotypes
TA5/5 , TA5/6,
TA5/7, TA5/8, TA
6/6
43 (42.6) 9 (47.4) 15 (33.3)

159
Table 2: Comparison of laboratory markers between patients and controls
Parameters SCA (N=101)
Median (Range)
Controls (N=64)
Median (Range)
Test statistics P value
HbF (%) 8.4 (0.9 – 32.3) 0.9 (0 – 5.8)
p˂0.0001
LDH (IU/L) 771 (197 – 1860)
345(150 – 840) p˂0.0001
Hb Conc (g/dL) 7.4 (6.3 – 11.2) 11.6 (7.8 – 14.8)
p˂0.0001
WBC ( X 103/uL) 12.6 (6.1 – 29.3) 6.6 (4.5 – 14.4)
p˂0.0001
Platelet ( X 103/uL) 343 (118 – 832)
278 (108 – 591)
p˂0.0001
Total Bilirubin
(mg/dL)
1.8 (0.42– 8.1)
0.4 (0.1– 2.2)
p˂0.0001
Unconjugated
bilirubin (mg/dL)
0.8 (0.1 -6.3) 0.2 (0.03 -0.8) p˂0.0001
AST (IU/L) 42 (17 – 89)
27 (6 – 45) p˂0.0001
ALT (IU/L) 20 (4 – 77)
10 (4 – 51) p˂0.0001
NB:Test statistics =Mann-Whitney , Significant P values are indicated in bold fonts

160
Table 3: Influence of UGT1A1 genotype on laboratory parameters
Parameter a. Low activity UGT1A1 genotypes
N=25
b. Intermediate activity UGT1A1 genotypes
N=33
c. High activity UGT1A1 genotypes
N=43
P1 values
a versus (b+c)
Anova
P2
values
(a vs b vs c)
Biochemical and haematologic
Median (Range) Median (Range) Median (Range)
Total Bilirubin (mg/dl)
2.8 (1.2 -8.1) 1.7 (0.8 -4.7) 1.4 (0.4 -3.8) <0.0001* <0.0001**
Unconjugated Bilirubin (mg/dl)
1.8 (0.6 – 6.3) 0.8 (0.1 -3.6) 0.6 (0.1-2.8) <0.0001* <0.0001**
LDH (IU/L) 987(296-1860) 705 (233 -1489) 681 (197-1417) 0.0150* 0.0386**
AST(IU/L) 46 (18 -89) 41 (18 - 89) 37 (17 -89) 0.136* 0.3169**
ALT (IU/L) 25 (4-65) 18 (7- 58) 19 (4 -77) 0.1431* 0.279**
Hb conc (g/dl)
7.3 (6.3 -10) 7.5 (6.3 -11.2) 7.4(6.4 -10) 0.59*65* 0.822**
MCV(fl) 80.6 (66.9 -104.1)
82.3 (60.3 -101.5) 80.9 (55.9 -115) 0.9752* 0.8469**
RBC (x 1012/L)
2.7 (1.9 -4.1) 2.6 (2 -4.7) 2.9 (1.8 -4.8) 0.8427* 0.4438**
WBC (x 109/L)
13 (8.5 -26) 10.5 (6.1 -27) 13.3 (6.4 -29) 0.4814* 0.2997**
Platelet (x 109/L)
367 (118 -771) 342 (167 -593) 358 (118 -832) 0.4717* 0.7494**
HbF (%) 9.7 (1.3 -20.6) 7.3 (1.7 -24.4) 10.4 (0.9 -32) 0.521* 0.7466**
*=Mann-Whitney Test, **=Kruskal-Wallis one way analysis of variance, Significant p values are indicated in bold fonts.

161
Table 4: Influence of UGT1A1 genotype on clinical events of patients
Clinical events
a. Low activity UGT1A1 genotypes
N=25
b. Intermediate activity UGT1A1 genotypes
N=33
c. High activity UGT1A1 genotypes
N=43
P value
VOC per year 2 (0-6) 0 (0-6) 0 (0-6) 0.09*
Overt Stroke 1 1 2 1.000†
No overt stroke
24 32 41
Osteonecrosis 1 1 3 1.000†
No osteonecrosis
24 32 43
Leg ulcer 0 1 5 0.331†
No Leg ulcer 25 32 38
Gallstones 5 1 0 0.0033†
No Gallstone 20 32 43
Priapism (Male only event, N=67)
Priapism 1 2 2 1.000†
No Priapism 16 26 20
*=Mann-Whitney Test, †=Fisher`s exact test, Significant p values are indicated in bold fonts.

162
Table 5: Comparison of parameters in patients with and without gallstones
Parameter Patients with gallstones (N=6)
Median (Range)
Patients without gallstones (N=95)
Median (Range)
P value
Total Bilirubin (mg/dl)
6.4 (2.8 -8.1) 1.8 (0.4 -6.7) 0.0001*
Unconjugated Bilirubin (mg/dl)
4.7 (0.9 -6.3) 0.79 (0.1 -5) 0.0007*
LDH (IU/L) 1004 (592 -1860) 794 (197 -1750) 0.1263*
HbF (%) 4.7 (1.3 -6.8) 10.2 (0.9 -32) 0.0107*
Hb (g/dl) 7.1 (6.3 -8.8) 7.5 (6.2 -10) 0.4210*
Age in years 11.5 (8 -16) 9 (2-21) 0.1368*
Sex
Male (n=66) 4 62 1.000†
Female (n=35) 2 33
Parameter Patients with gallstones (N=6)
Median (Range)
Matched peers without gallstones within same UGT1A1 genotype activity group N=10
Median (Range)
P value
Total Bilirubin (mg/dl)
6.4 (2.8 -8.1) 2.2 (1.9- 3.2) 0.0023*
Unconjugated Bilirubin (mg/dl)
4.7 (0.9 -6.3) 1.2 (1.0 -2.0) 0.0020*
LDH (IU/L) 1004 (592 -1860) 890 (340 -1603) 0.628*
HbF (%) 4.7 (1.3 -6.8) 14.7 (4.2 -17.9) 0.022*
Hb (g/dl) 7.1 (6.3 -8.8) 8.0 (6.5 – 8.9) 0.137*

163
NB Significant P values are indicated in bold fonts, *=Mann-Whitney test, †=Fisher`s Exact
MANUSCRIPT 2
Title: Influence of Alpha Thalassemia on Clinical and Laboratory Parameters among
Nigerian Children with Sickle Cell Anemia
Running title: Alpha Thalassemia and Sickle Cell Anemia
Authors:
Oladele Simeon Olatunya,a,b, Dulcineia Martins de Albuquerque,a, Adekunle
Adekile,c, Fernando Ferreira Costa,a
Affiliations: aHematology and Hemotherapy Center, University of Campinas, São Paulo, Brazil bDepartment of Paediatrics, College of Medicine, Ekiti State University, Ekiti State, Nigeria cDepartment of Pediatrics, Faculty of Medicine, Kuwait University, Kuwait
Corresponding author and address for correspondence:
Oladele Simeon Olatunya Hematology and Hemotherapy Center (Hemocentro),
University of Campinas (UNICAMP),
Rua Carlos Chagas, 480
Barão Geraldo
Campinas 13083-970-SP, Brazil
Tel: +55 19 3521 8382
Email for correspondence: [email protected]

164
ABSTRACT
Alpha thalassemia modulates both the clinical and laboratory parameters of sickle cell
anemia (SCA). There is paucity of data on these among Nigerian SCA patients. This
study aimed to determine the prevalence of alpha thalassemia and its association with
laboratory and clinical manifestations among young Nigerians with SCA.
One hundred patients with SCA and 63 healthy controls were studied. Alpha
thalassemia genotyping was done by multiplex gap-PCR. Laboratory parameters,
including complete blood count, hemoglobin quantitation, serum lactate dehydrogenase
(LDH) and bilirubin were determined with standard techniques.
Alpha thalassemia was found in 42 (42.0%) patients compared to 24 (38.1%) controls
(p=0.7433) and all were due to the 3.7 κb α-globin gene deletion. Alpha thalassemia
associated with more frequent bone pain crisis, higher hemoglobin concentration, red
blood cell count and HbA2 level, and lower mean corpuscular volume, mean
corpuscular hemoglobin, and white blood cell count (WBC) in the SCA patients
(p˂0.05). There were 6 (10.3%) patients with leg ulcers, none of whom had alpha
thalassemia, p=0.0384.
This study confirms that coexistence of alpha thalassemia significantly influences both
the clinical and laboratory manifestations of young Nigerians with SCA. The
coexistence of this genetic modifier is associated with increased bone pain crisis and
protects against leg ulcers in SCA patients.
Keywords: Sickle cell anemia, Alpha thalassemia, Laboratory parameters, Clinical
manifestations, Children, Nigeria.

165
INTRODUCTION
Sickle cell anemia (SCA) is very common among Africans [1]. Globally, about 305,800
neonates are born with SCA annually and almost two-thirds of these occur in Africa1and
Nigeria has the highest burden in the world [2]. SCA is characterized by heterogeneous
clinical phenotypes due to the influence of genetic modifiers [3,4].
Alpha thalassemia (α-thal) trait secondary to one (αα/– α3.7) or two (-α3.7/-α3.7) α-gene
deletion has been found to, partly protect patients with SCA from early hyposplenism
[5], gallstones [6], stroke [7], priapism [8], glomerulopathy [9], and leg ulcers [7,10-12].
However, others have reported higher rates of painful crises [13], osteonecrosis [14] and
retinopathy [14] in SCA patients with coexistent α-thal. Although some studies have
described the possible effects of α-thal among patients with SCA in the developed world
[5-7, 9-14], there is paucity of information about the influence of this genetic factor in
African patients with SCA. The few available studies have established that the 3.7 κb α-
globin gene deletion is the common α-thal allele among Africans [15-17], and Nigerians
[18-20]. However, there is lack of consensus on its impacts on the laboratory and
clinical manifestations of patients with SCA [15-20].
Because of genetic variability in different populations, it is pertinent that more studies
are carried out among cohorts from different ethnic backgrounds to fully understand the
impact of genetic modifiers on SCA. The aim of this study was to assess the prevalence
of α-thal trait and its influence on laboratory and clinical events in a group of young
Nigerians with SCA.

166
PATIENTS AND METHODS
The study was conducted on 100 hydroxyurea-naive SCA children and adolescents who
were regular attendees at the pediatric hematology clinic of the Ekiti State University
Teaching Hospital (EKSUTH), Ado Ekiti, Ekiti State, Southwestern Nigeria. Sixty three
healthy children, who accompanied their siblings to or attended the outpatients` well-
child clinic served as controls. To qualify for inclusion, the SCA patients must have
been on regular follow up at the clinic for a minimum of one year prior to recruitment
with up-to-date hospital records. Participants with confirmed or other suspected chronic
diseases apart from SCA, were excluded. Also excluded were the few SCA patients on
regular blood transfusion and hydroxyurea. SCA was initially diagnosed by hemoglobin
electrophoresis and high performance liquid chromatography (HPLC) and was
confirmed by DNA studies.
Ethical considerations
Written informed consent of parents/caregivers as well as patients’ assents and consents
were obtained as applicable. The study was approved by the hospital`s Institutional
Ethics and Research Committee no: A67/2016/03/003.
Data collection
Clinical and laboratory data
A pre-tested chart review form was used to extract relevant information from the
patients’ hospital records regarding their steady-state laboratory parameters and clinical

167
events. An average of, at least, two steady-state results of laboratory parameters
performed between 3 to 6 months intervals were recorded for each participant. The
steady-state parameters included the complete blood count performed by Sysmex
KX21N Haematology analyser (Sysmex Corporation, Kobe, Japan); serum lactate
dehydrogease (LDH), bilirubin, and aspartate transaminase (AST) were measured with
standard techniques. HbF quantitation was done using HPLC (Bio-Rad Variant D10,
USA). Steady state was defined as being free from any acute event(s) for at least one
month and transfusion free for at least four months [21].
Other information retrieved from patients’ charts included their biodata. Data on the
clinical evolution of SCA among the patients were obtained and this included the
number of bone pain crises requiring hospital visit and administration of analgesics
within the preceding one year. In addition, presence or absence of complications of
SCA like leg ulcers, priapism, and overt osteonecrosis or overt stroke were examined.
The definitions of clinical events were as previously described [22].
Genetic studies
These were carried out at the Centro de Hematologia e Hemoterapia (Hemocentro),
UNICAMP, Campinas, Sao Paulo State, Brazil.
DNA extracted from each participant by Qiagen QIAamp DNA (Blood Mini Kit Cat
No. 51104 Germany), was used to confirm the diagnosis of SCA by polymerase chain
reaction (PCR).
Alpha thalassemia determination
Alpha-thalassemia (α3.7Kb deletion) was investigated by GAP-PCR according to Dode
et al [23]. Briefly, the PCR was performed in 25 μL reaction volume containing 100ng

168
of DNA sample; 1X α- Buffer (Tris-HCl 2M (pH 8.6), (NH4)2 SO4 1M, MgCl2 1M,
Na2EDTA 0.2M, BSA and β-mercaptoetanol 14.3M); 1X DMSO; 0.3mM of dNTP
mix; 0.2 µM of each primer (C2: CCATGCTGGCACGTTTCTGA e C10:
GATGCACCCACTGGACTCCT); 1U of GoTaq® Flexi DNA Polymerase (Promega
Corporation, Madison, USA). Thermal cycle conditions were as follows: preheating at
94°C by 5 minutes, followed by 35 cycles of 94°C for 45 seconds, 56°C for 1 minute,
and 72°C for 2 minutes and a final extension at 72°C for 7 minutes was performed.
After electrophoresis in a 1.2% agarose gel a fragment of 2.1Kb could be observed for
normal alleles and 1.9Kb fragment for deleted alleles (-α3.7Kb).
Alpha-thalassemia (α4.2Kb deletion) was investigated by Multiplex-PCR according to
Oron-Karni et al [24]. Briefly, the PCR was performed in 25 μL reaction volume
containing 100ng of DNA sample; 1X α- Buffer (Tris-HCl 2M (pH 8.6),
(NH4)2 SO4 1M, MgCl2 1M, Na2EDTA 0.2M, BSA and β-mercaptoetanol 14.3M); 1X
DMSO; 0.3mM of dNTP mix; 0.4 µM of primer
(P71: TACCCATGTGGTGCCTCCATG e 0.3 µM of each primer P72:
TGTCTGCCACCCTCTTCTGAC and P52: CCTCCATTGTTGGCACATTCC; 1U
of Taq DNA Polymerase (Invitrogen, Carlsbad,CA). Thermal cycle conditions were as
follows: preheating at 94°C by 5 minutes, followed by 35 cycles of 94°C for 45
seconds, 60°C for 1 minute, and 72°C for 2 minutes and a final extension at 72°C for 7
minutes was performed. After electrophoresis in a 1.2% agarose gel a fragment of 1596
bp could be observed for deleted alleles (-α4.2Kb) and 233 bp as an internal control to
verify the quality of DNA sample. All DNA studies were carried out blinded regarding
the clinical and laboratory parameters of the participants.

169
Data Analysis
Statistical analysis was performed with the GraphPad Prism Program, version 5 for
Windows (San Diego, California, USA). The normal distribution of the quantitative
variables was verified by the Kolmogorov-Smirnov and Shapiro-Wilk tests. The
frequencies of variables were described and the significance of differences between
groups of patients was assessed using the Kruskal-Wallis analysis of variance
(ANOVA), chi-square, Mann-Whitney or Fisher`s exact tests as appropriate. Level of
significance was set at P < 0.05
RESULTS
The patients consisted of 66 males and 34 females with a median age of 8.5, range 2 –
21 years. The controls were made up of 22 individuals with HbAS and 41 with HbAA,
median age of 8, range 2- 18years. They consisted of 36 males and 27 females. The
patients had been on follow up for a median of 4 years, range 1.5 -14years. There were
no differences in the socio-biographic data of patients and controls (Table 1).
Allele frequency of alpha thalassemia among patients and controls
None of the participants had the Alpha-thal trait 4.2Kb α-globin gene deletion.
Alpha-thal trait (3.7 κb α-globin gene deletion) was found in 41 (41.0%) patients; 34
with heterozygous deletion (αα/– α3.7), and 7 with homozygous deletion (-α3.7/-α3.7),
while 58 (58.0%) patients had normal genotype (αα/αα). Twenty-four controls
comprising 8 (36.0%) HbAS, and 16 (39.0%) HbAA had α-thal trait and these were all
heterozygous (αα/– α3.7). Also, 38 controls made up of 13 (62.0%) HbAS and 25
(61.0%) HbAA had normal genotype (αα/αα). Of the 200 patients’ chromosomes

170
analysed, 150 were αα, 49 were –α, and one was ααα, thus giving gene frequencies of
0.75 (αα), 0.25 (-α), and 0.005 (ααα) respectively. Similarly, the gene frequencies
among the controls were HbAS - 0.82 (αα), 0.18 (-α) and HbAA- 0.80 (αα), 0.20 (-α)
respectively, with no gene triplication (ααα) detected and these were not significantly
different from the frequencies among the patients (Table 1). Taken together, the
prevalence of α-thal was not different across the groups (SCA 42 (42%) vs HbAS 8
(36.0) vs HbAA 16 (39.0), ᵡ2=0.2866, df=2, p=0.866).
Comparison of laboratory parameters between patients and controls
There were significant differences between the patients and controls in all laboratory
parameters p<0.05 except mean corpuscular hemoglobin (MCH). (Table 2)
Effects of alpha thalassemia on hematological indices and other laboratory
parameters among patients
Co-inheritance of α-thal was significantly associated with higher hemoglobin
concentration (Hb), red blood cell count (RBC) and HbA2 level. On the contrary, it was
associated with lower mean corpuscular volume (MCV) and mean corpuscular
hemoglobin (MCH), while the white blood cell count (WBC) was significantly lower in
patients with homozygous 3.7 kb α-globin gene deletion compared to the two other
groups. No significant differences were observed across α-thal genotypes in the other
laboratory parameters (Table 3).
Effects of alpha thalassemia on clinical events among patients
Sixty-one (61.0%) patients had bone pain episodes, 6 (6.0%), 5 (5.0%) each had overt
stroke and osteonecrosis while 5 (7.5%) males had priapism.

171
The rate of painful crisis was higher in patients with α-thal compared to those without it
(p<0.0001). However, the presence of α-thal protected against leg ulcer as none of the
six patients with leg ulcer had α-thal 0 (0.0%) vs 6 (10.3%), p=0.0384. No significant
association was found in relation to other clinical events with respect to the presence or
absence of α-thal (Table 4).
DISCUSSION
There is scarcity of information on the roles of genetic modifiers on SCA in Africa
despite its huge burden in the continent and this makes comparison of data difficult.
The two α-globin genes are present within a 4-kb duplicated region leading to the
possibility of rearrangements including deletions and triplications with many attendant
downstream consequences [24]. This study confirmed earlier reports that the 3.7 κb α-
globin gene deletion is the common α-thal allele among Africans [15-20] as none of the
participants had the 4.2Kb α-globin gene deletion.
The prevalence of alpha thalassemia among patients in this study (41%) is higher than
between the 13 and 28% described among patients in the Americas [25-28].This is
however lower than the 60% and 77% described among Congolese [17], and Ugandans
[16] respectively. It is comparable to the 37.3% among Cameroonians [15], and the
46% among SCA patients in France [13]. It is also in agreement with the 40% to 42.5%
earlier described among Nigerians SCA patients [19,20]. The high prevalence of α-thal
in this study, and others from Africa [15-17], may be due to the selective advantage in
conferring protection and survival against malaria [18,29,30]. The higher prevalence of
α-thal in central Africa [16,17], relative to this study, may derive from its vital impact
on survival of SCA, which is more severe in this part of Africa [16,17].

172
The observed hematological profile of patients with α-thal in this study has been
previously described [10,13,18-20,25,26,28]. The increased Hb and red blood cell count
are due to the decrease in the intracellular concentration of HbS, and number of dense
red blood cells. These, in turn, lead to increased red blood cell deformability and
decreased rates of both HbS-induced RBC polymerization and hemolysis.3,7,14 Similarly,
the lack of influence of α-thal on the HbF levels of patients in this study, has been
previously reported [25,26,28].
Beyond these, alpha thalassemia hematologic profile also mimicks that of iron
deficiency anemia and individuals with alpha thalassemia may be misdiagnosed for iron
deficiency and mistreated with iron therapy [31]. The contributions of iron deficiency to
the clinical phenotype of SCA is still not fully explored. Nevertheless, some studies
have found that iron deficiency anemia do occur among children with SCA [32,33].The
similarities in the hematological profile of patients with iron deficiency and alpha
thalassemia make it important that alpha thalassemia status of children with SCA are
determined in order to prevent misdiagnosis and mistreatment for iron deficiency. This
is more important for patients in the developing countries given the high prevalence of
both conditions among children in these parts of the world [1,2,34].
Contrary to some earlier reports that alpha thalassemia did not influence the clinical
events in SCA [26,28], the presence of α-thal in this study, was associated with higher
rates of bone pain crisis compared to those without α-thal. This finding is in keeping
with that of Renoux et al [13], among children with SCA in France and other previous
reports [7,14]. Vaso-occlusive crisis (VOC) manifesting as bone pain crisis is a
common complication of SCA and, is thought to be associated with increased blood
viscosity [7,13]. Studies have demonstrated that SCA patients with α-thal have
increased blood viscosity because of relatively higher levels of Hb and/or hematocrit,

173
among other mechanisms [3,7,13,14]. In this study, our SCA patients with α-thal, had
higher Hb that could lead to increased blood viscosity. It is therefore conceivable that,
they could have higher rates of painful crisis.
Furthermore, as found in this study, authors from different parts of the world have
reported that α-thal protects against leg ulcer in SCA patients [10,11,17]. However,
some have reported that, no such association exist [15,16]. These observations reflect
lack of consensus on the roles of α-thal in some phenotypes of SCA. Leg ulcer is a
chronic and debilitating complication that is thought to be associated with very severe
phenotype of SCA [3,12,35-37]. Therefore there’s a need for more studies from Africa
to explain the relationship between α-thal and leg ulcer, and other SCA phenotypes.
The observations that α-thal is associated with lower frequency of stroke in children
with SCA [38,39] was not sustained in this study. On the contrary, one previous study
[20] found that, in combination with BCL11A variants, α-thal was associated with
increased risk for stroke in older SCA patients. The lack of association between α-thal
and stroke in this study, is in keeping with report by Filho et al [40]. Nonetheless, these
findings need to be interpreted with caution because of differences in age of study
cohorts and possibility of survival bias. In addition, stroke was determined in this study
by overt clinical history and was, in most cases, not confirmed by magnetic resonance
imaging or angiography and this could lead to detection bias and exclusion of cases of
silent infarcts from our analysis. These observations further underscore the need for
more studies to clearly define the prevalence and associations of α-thal with clinical
manifestations among Nigerian SCA patients.
The lack of association between α-thal and osteonecrosis in this study contrasts with the
report by Milner et al [41] on children enrolled in the cooperative study of sickle cell

174
disease in the USA where they found that both α-thal and increasing age were
significantly associated with osteonecrosis. Possible explanations for our findings
included the fact that our study participants were fewer and younger compared to that
by Milner et al [41]. The youngest patient in this study was two years old, while theirs`
was five years old. In addition, only five percent of our patients had osteonecrosis
compared to 9.8% in their study.
Osteonecrosis is a disabling and severe complication of SCA associated with
impairments of both functional activities and growth in children. In SCA, it is thought
to be due to bone microcirculation disturbance in the patients and can be observed in
children with SCA as young as five years old with an increasing incidence throughout
childhood and adolescence, peaking in early adulthood [42].
In conclusion, this study shows that coexistence of α-thal influences the hematologic
parameters of Nigerian children with SCA. It also showed that α-thal was associated
with increased rates of bone pain crisis and seems to protect against the occurrence of
leg ulcer.
FUNDING AND DISCLOSURES
This study was supported by grants No 2014/00984-3 from FAPESP, and grants No
2015/141693-0 from CNPq, Brazil.
The authors declare no conflict of interest with respect to this study.
ACKNOWLEDGEMENTS
Authors acknowledge with thanks the supports received from participants and their
caregivers/parents during the study.
REFERENCES

175
[1]. Piel FB, Patil AP, Howes RE et al. Global epidemiology of sickle
hemoglobin in neonates: a contemporary geostatistical model-based map and
population estimates. Lancet 2013; 381:142-51
[2]. Diaku-Akinwumi IN, Abubakar SB, Adegoke SA et al. Blood transfusion
services for patients with sickle cell disease in Nigeria. Int Health
2016;8(5):330-5
[3]. Kato GJ, Gladwin MT, Steinberg MH. Deconstructing sickle cell disease:
Reappraisal of the role of hemolysis in the development of clinical
subphenotypes. Blood Rev.2007;21:37-47
[4]. Goncalves MS. Comment on molecular analysis and association with
clinical and laboratory manifestations in children with sickle cell anemia. Rev
Bras Hematol Hemoter2014;36(5):315-18
[5]. Adekile AD, Tuli M, Haider K et al. Influece of α thalassemia trait on spleen
function in sickle cell anemia patients with high HbF. Am J Hematol 1996;53:1-
5
[6]. MZ Haider, Ashedu S, Aduh P, Adekile AD. Influence of α-thalassemia on
cholelithiasis in SS patients with elevated HbF. Acta Haematol 1998;100:147-50
[7]. Steinberg MH. Predicting clinical severity of sickle cell anemia. Br J
Haematol. 2005;129:465-81
[8]. Ballas SK, Larner J, Smith ED, Surrey S, Schwartz E, Rappaport EF.
Rheology predictors of the severity of the painful crisis. Blood.1988;72:1216-23
[9]. Lamarre Y, Romana M, Lemonne N et al. Alpha thalassemia protects sickle
cell anemia patients from macro-albuminuria through its effects on red blood
cell rheological properties. Clin Hemorheal Micro-circ. 2014;57:63-72

176
[10]. Higgs DR, Aldridge BE, Lamb J et al. The interaction of alpha thalassemia
and homozygous sickle cell disease. N Engl J Med 1982;306:1441-6
[11]. Koshy M, Entsuah R, Koranda A et al. Leg ulcers in patients with sickle
cell disease. Blood 1989;74:1403-8
[12]. Minniti CP, Eckman J, Sebastiani P, Steinberg MH, Ballas SK. Leg ulcers
in sickle cell disease. Am J Hematol 2010;85:831-3
[13]. Renoux C, Connes P, Nader E et al. Alpha thalassemia promotes frequent
vaso-occlusive crises in children with sickle cell anemia through
haemorheological changes. Pediatr Blood Cancer
2017;64:e26455.doi:10.1002/pbc.26455
[14]. Steinberg MH, Sebastiani P. Genetic modifiers of sickle cell disease. Am J
Hematol 2012;87(8):795-803
[15]. Rumaney MB, Ngo Bitoungui VJ, Vorster AA et al. The co-inheritance of
alpha thalassemia and sickle cell anemia is associated with better hematological
indices and lower consultations rate in Cameroonian patients and could improve
their survival. PLoS ONE 2014;9(6):e100516.doi:10.1371/journal.pone.0100516
[16]. Lubega I, Ndugwa CM, Mworozi EA, Tumwine JK. Alpha thalassemia
among sickle cell anemia patients in Kampala, Uganda. Afr Health Sci
2015;15(2):682-89
[17]. Mikobi TM, Lukusa PT, Aloni MN et al. Association between sickle cell
anemia and alpha thalassemia reveals a high prevalence of the α3.7 triplication in
Congolese patients than in worldwide series. J Clin Lab Anal
2017;00:e22186:doi:10.1002/jcla.22186

177
[18]. Adekile AD, Liu JC, Sulzer AJ, Huisman THJ. Frequency of the α-
thalassemia-2 gene among Nigerian SS patients and its influence on malaria
antibody titers. Hemoglobin 1993;17(1):73-9
[19]. Falusi AG, Esan GJF, Ayyub H, Higgs DR. Alpha thalassemia in Nigeria:
its interactions with sickle cell disease. Eur J Haematol. 1987;38:370-75
[20]. Saraf SL, Akingbola TS, Shah BN et al. Associations of α-thalassemia and
BCL11A with stroke in Nigerian, United States, and United Kingdom sickle cell
anemia cohorts. Blood Advances 2017; 1(11):693-8
[21]. Ballas SK. More definitions in sickle cell disease: Steady state v baseline.
Am J Hematol 2011;86:338
[22]. Ballas SK, Lieff S, Benjamin LJ, Dampier CD, Heeney MM, Hope C.
Definitions of phenotypic manifestations of sicle cell disease. Am J Hematol.
2010;85:6-13
[23]. Dode C, Krishnamoorthy R, Lamb J, Rochette J. Rapid analysis of – α3.7
thalassaemia and αααanti3.7 triplication by enzymatic amplification analysis. Br J
Haematol 1993;83:105-111
[24]. Oron-Karni V, Filon D, Oppenheim A, Deborah R. Rapid detection of the
common Mediterranean α-globin deletions/rearrangements using PCR. Am J
Hematol 1998;58:306-310
[25]. Figueiredo MS, Kerbauy J, Goncalves MS et al. Effect of α-thalassemia
and β-globin gene cluster haplotypes on the hematological and clinical features
of sickle cell anemia in Brazil. Am J Hematol 1996;53:72-6
[26]. Adorno EV, Zanette A, Lyra I et al. Clinical and molecular characteristics
of sickle cell anemia in the northeast of Brazil. Genetics Mol Biol
2008;31(3):621-25

178
[27]. Cardoso G, Guerreiro JF. Molecular characterization of sickle cell anemia
in the northern Brazilian state of Para. Am J Hum Biol 2010;22:573-77
[28]. Camilo-Araujo RF, Amancio OMS, Figueiredo MS, Cabanas-Pedro AC,
Braga JAP. Molecular analysis and associations with clinical and laboratory
manifestations in children with sickle cell anemia. Rev Bras Hematol Hemoter
2014;36(5):334-9
[29]. Wambua S, Mwacharo J, Uyoga S, Macharia A, Williams TN. Co-
inheritance of α-thalassemia and sickle cell trait results in specific effects on
hematological parameters. Br J Haematol 2006;133(2):206-9
[30]. Mockenhaupt FP, Ehrhardt S, Gellert S et al. α+-thalassemia protects
African children from severe malaria Blood 2004;104:2003-6
[31]. Borges E, Wenning MR, Kimura EM et al. High prevalence of alpha
thalassemia among individuals with microcytosis and hypochromia without
anemia. Braz J Med Biol Res 2001;34(6):759-62
[32]. Vichinsky E, Kleman K, Embury S, Lubin B. The diagnosis of iron
deficiency anemia in sickle cell disease. Blood 1981;58:963-8
[33]. Akodu SO, Kehinde OA, Diakwu-Akinwumi IN, Njokanma OF. Iron
deficiency anemia among pre-school children with sickle cell anemia: Still a rare
diagnosis? Mediterr J Hematol Infect Dis 2013;5(1):e2013069
doi:10.4084/MJHID.2013.069
[34]. Stevens GA, Finucane MM, De-Regil LM, Paciorek JC, Flaxman SR,
Branca F. Global, regional and national trends in hemoglobin concentration and
prevention of total and severe anemia in children and pregnant and non pregnant
women 1999 – 2011. Lancet Glob Health 2013;e16-e25.

179
[35]. Serjeant GR, Higgs DR, Hambleton IR. Elderly survivors with
homozygous sickle cell disease. N Engl J Med 2007;356(6):642-3
[36]. Minniti CP, Taylor JGt, Hildesheim M et al. Laboratory and
echocardiography markers in sickle cell patients with leg leg ulcers. Am J
hematol2011;86:705-8
[37]. Minniti CP, Kato GJ. How we treat sickle cell patients with leg ulcers. Am
J Hematol 2016;91(1):22-30
[38]. Belisaro AR, Rodrigues CV, Martins ML, Silva CM, Viana MB.
Coinheritance of alpha thalassemia decreases the risk of cerebrovascular disease
in a cohort of children with sickle cell anemia. Hemoglobin 2010;34:516-29
[39]. Flanagan JM, Frohlich TA, Howard WH et al. Genetic predictors for stroke
in children with sickle cell anemia. Blood 2011;117:6681-84
[40]. Filho IL, Leite AC, Moura PG et al. Genetic polymorphisms and
cerebrovascular disease in children with sickle cell anemia from Rio de Janeiro,
Brazil, Arq. Neuropsiquiatr 2011;69:431-5
[41]. Milner PF, Kraus AP, Sebes JI et al. Sickle cell disease as a cause of
osteonecrosis of the femoral head. New Engl J Med 1991;325:1476-81
[42]. Mahadeo KM, Oyeku S, Taragin B et al. Increase prevalence of
osteonecrosis of the femoral head in children and adolescent with sickle cell
disease. Am J Hematol 2011;86(9):806-8

180
Table 1: Biodata and frequencies of alpha thalassemia alleles
Parameters SCA (SS)
N=100
n (%)
AS
N=22
n (%)
AA
N=41
n (%)
Chi-square,
degree of
freedom
ᵡ2, df
P value
Age in years
Median
(Range)
8.5 (2-21) 9 (3 – 17) 8.5 (2 – 18) NA 0.888a
Sex
Male
Female
66 (66.0)
34 (34.0)
13 (59.0)
9 (41.0)
23 (56.0)
18 (44.0)
1.350, 2 0.509b
Social Class
Lower
Middle
Upper
48 (48.0)
44 (44.0)
8 (8.0)
12 (54.5)
8 (36.4)
2 (9.1)
20 (48.8)
18 (43.9)
3 (7.3)
0.4714, 4 0.9762 b
Alpha thalassemia present
41 (41.0) 8 (36.0) 16 (39.0) 0.2866, 2
0.866 b
Alpha thalassemia absent
58 (58.0) 13 (62.0) 25 (61.0)
α-globin
genotype
SCA (SS)
N=100
n (%)
AS
N=22
n (%)
AA
N=41
n (%)
αα/–α
34 (34.0) 8(36.0) 16 (39.0) 0.327, 2 0.849 b
-α/-α
7 (7.0) 0 (0) 0 (0) NA 0.043*
ααα 1 (1.0) 0 (0) 0 (0) NA

181
Allele
frequency
Total
chromosome
N=200
n(frequency)
Total
chromosome
N=44
n(frequency)
Total
chromosome
N=82
n(frequency)
αα 150 (0.75) 36 (0.82) 66 (0.80) 1.590, 2 0.451 b
-α 49 (0.25) 8 (0.18) 16 (0.20) 0.822, 2 0.662 b
ααα 1 (0.005) 0 (0.0) 0 (0.0) NA
NB: a=Kruskal-Wallis test, b= Chi-square test, *=Fisher`s exact test, NA= Not applicable, One
case of Triplicaion not considered as alpha thalassemia, Significant p value is in bold font.

182
Table 2: Laboratory parameters of patients and controls
Biomarkers HbAA
N=41
Median
(Range)
HbAS
N=22
Median
(Range)
HbSS
N=100
Median
(Range)
P value
Hb (g/dl) 11.5
(7.8 – 13)
11.6
(8 – 14)
7.5
(6.2 – 11.2)
˂0.0001
MCV (fL) 89.4
(66.4 – 102)
79.6
(60.4 – 74.7)
81.1
(60 – 115)
0.0125
RBC ( million
cells/uL)
4.5
(3.8 – 5.5)
4.6
(2.3 – 6.0)
2.8
(1.8 – 4.8)
˂0.0001
WBC (x
103/uL)
6.3
(4.5 – 14.4)
6.5
(4.5 -12.5)
13.1
(6.1 – 29.30)
˂0.0001
Platelet (x
103/uL)
244
(117 – 514)
275
(125 – 578)
361
(108 – 832)
0.0004
HbF (%) 0.75
(0 – 2.1)
0.7
(0.2 – 4.7)
9.3
(0.9 – 32.3)
˂0.0001
HbA2 (%) 2.9
(0.8 – 3.6)
3.6
(0.5 – 4.6)
1.5
(0.2 – 4.0)
˂0.0001
MCH (pg) 24.4
(17.6 – 27.9)
25.2
( 18.2 – 29 )
25.3
(16 – 34)
0.260
Total
bilirubin
(mg/dl)
0.43
(0.1 – 0.45)
0.45
(0.25 – 1)
1.80
(0.5 – 8.1)
˂0.0001
AST (IU/L) 19
(6 – 64)
27
(8 – 75)
43
(12 – 89)
˂0.0001
LDH (IU/L) 360
(150 – 861)
375
(179 – 993)
789.3
(179 – 1860)
˂0.0001

183
NB- Significant p values are in bold fonts, Test statistics = Kruskal-Wallis ANOVA, Hb-
Hemoglobin concentration, RBC-Red blood cells, MCV-Mean corpuscular volume, WBC-White
blood cells count, HbF- Fetal hemoglobin, MCH- mean corpuscular hemoglobin, AST-Aspartate transaminase, LDH-Lactate dehydrogenase
Table 3: Alpha thalassemia Alleles and laboratory parameters
Biomarkers Alpha
thalassemia
with
Heterozygous
deletion
N=34
Median (Range)
Alpha
thalassemia
with
Homozygous
deletion
N=7
Median (Range)
SS with no
Alpha
Thalassemia
Trait
N=58
Median (Range)
P Value
Hb (g/dl) 7.6 (6.3-11.2) 8.2 (7.6-10) 7.2 (6.2-11) 0.0199
MCV (fL) 78 (66.9 -94) 74 (60.3 – 101) 84 (56 – 115) 0.0025
RBC (million
cells/uL)
2.8 (2.15 -3.9) 3.1 (2.7 – 4.1) 2.7 (1.8 – 4.8) 0.0264
WBC (x 103/uL) 14.7 (6.4 – 26.2) 7.8 (6.1 – 13.2) 13.3 (6.1 – 29.3) 0.0353
Platelet (x
103/uL)
358 (108 -674) 334 (158 -444) 371 (118 -832) 0.2156
HbF (%) 8.8 (0.6 – 28.5) 13.1 (3.7 – 17.5) 10.7 (2.5 – 32.3) 0.1364
HbA2 (%) 1.7 (0.3 – 3.8) 2.8 (1.5 – 4.0) 1.5 (0.2 – 3.1) 0.0002
MCH (pg) 24.5 (18.6 –
30.6)
24.4 (15.7 –
27.1)
26 (15.9 – 34) 0.0021
Total Bilirubin
(mg/dl)
2.1 (0.43 – 7.7) 1.8 (1.03 – 8.1) 1.8 (0.8 – 5.2) 0.729
AST (IU/L) 58 (12 – 89) 40 (22 – 89) 43 (7 – 89) 0.3974
LDH (IU/L) 865 (215 –
1860)
771 (705 – 986) 881 (197 –
1681)
0.6469
NB- Significant p values are in bold fonts, Test statistics= Kruskal-Wallis ANOVA, Hb-
Hemoglobin concentration, RBC-Red blood cells, MCV-Mean corpuscular volume, WBC-White
blood cells count, HbF- Fetal hemoglobin, MCH- mean corpuscular hemoglobin, AST-Aspartate transaminase, LDH-Lactate dehydrogenase

184
Table 4: Co-inheritance of sickle cell anemia with Alpha Thalassemia and clinical events
Clinical events Patients with
Alpha
Thalassemia
(N=41)
Patients without
Alpha
Thalassemia
(N=58)
P value
Bone pain crisis
per Year
Range (0 –6)
Median 3
Range (0 –6)
Median 1
˂0.0001†
Stroke 2 3 1.000*
Osteonecrosis 3 2 0.6471*
Leg ulcer 0 6 0.0384 *
Priapism n=66
(Male only)
(N=34)
1
(N=32)
4
0.1974*
NB- Significant p values are in bold fonts, †= Mann-Whitney Test, *=Fisher`s exact test

185
MANUSCRIPT 3
Evaluation of socio-demographic, clinical and laboratory markers of sickle leg ulcers
among young Nigerians.
Authors:
Oladele Simeon Olatunya,a,b, Dulcineia Martins de Albuquerque,a, Adekunle
Adekile,c, Fernando Ferreira Costa,a
Affiliations: aHematology and Hemotherapy Center, University of Campinas, São Paulo, Brazil bDepartment of Paediatrics, College of Medicine, Ekiti State University, Ekiti State, Nigeria cDepartment of Pediatrics, Faculty of Medicine, Kuwait University, Kuwait
Corresponding author and address for correspondence:
Oladele Simeon Olatunya Hematology and Hemotherapy Center (Hemocentro),
University of Campinas (UNICAMP),
Rua Carlos Chagas, 480
Barão Geraldo
Campinas 13083-970-SP, Brazil
Tel: +55 19 3521 8382
Email for correspondence: [email protected]

186
ABSTRACT
Sickle leg ulcer (SLU) is a chronic and debilitating complication of sickle cell disease
(SCD) associated with huge physical and psychosocial discomfort. The occurrence of
SLU has remained steady despite successful preventive strategies and advances in SCD
care. Although multifactorial factors have been implicated in SLU, these are not fully
understood and data on how these relate to children with SCD are scanty. This study
aimed to evaluate the socio-demographic, clinical and laboratory markers of SLU in a
young SCD cohort.
One hundred and nine young SCD patients had their clinical, socio-demographic, and
laboratory parameters evaluated for SLU and their parameters compared with 67
healthy peers.
There were no differences in the socio-demographic parameters of patients and controls.
However, their laboratory parameters differ significantly (p<0.0001). Six patients with
HbSS genotype had SLU giving a prevalence of 5.9%. There was a preceding history of
trauma in 4 (66.7%) and this included a case of traditional scarifications for local
therapeutic purposes. The ulcers were mostly located on the ankles in 5 (83.3%) and
right big toe in 1 (16.7%). Two of the three males with SLU also had priapism. Patients
with leg ulcer were older, had less frequent bone pain crises, and significantly belonged
to the low socioeconomic class (p<0.05). Although patients with SLU had relatively
higher LDH, platelet count, AST, bilirubin, WBC, and lower Hb concentration and
HbF, these did not attain statistical significance (p>0.05).
This study confirms that SLU is common among HbSS genotype, older children and
those with low socio-economic background. In addition, this study suggests that SLU
could be more related to hemolysis-associated SCD phenotypes thus supporting the

187
previously held hypothesis that SLU is a distinct phenotype that is probably not related
to blood viscosity/rheology complications of SCD.
Keywords: Sickle cell anemia, Children, leg ulcer, Socio-demographic status,
Laboratory parameters, Clinical manifestations, Nigeria.
INTRODUCTION
Sickle cell disease (SCD), is an inherited hemoglobin defect that is very
common among Africans.1 The disease results from the inheritance of an abnormal
hemoglobin known as HbS.1 Patients with SCD present with variable disease severity
but the most severe form is the sickle cell anemia (SCA), which is the homozygous state
for the abnormal HbS.1 Globally, about 305,800 neonates are born with the SCA
annually and almost two-thirds of these occur in Africa2and Nigeria is the country with
the highest burden of SCA in the world.3
The structural abnormality in SCD leads to sickling of the red blood cells at low
oxygen tension. This results in clogging at microvascular level and subsequent vaso-
occlusion, hypoxia and other downstream clinico-pathologic manifestations of the
disease.1 Different aspects of the disease have been described based on these clinico-
pathologic manifestations.1,4
Leg ulcer complicating SCD, otherwise known as sickle leg ulcer (SLU), is a
chronic, and debilitating condition associated with both physical and emotional
disturbances.5,6,7,8 The prevalence of SLU varies among patients with SCD. It is low
before the age of ten years and rare in SCD genotypes other than SCA.6,8 Despite the
fact that SLU was among the complications found in the first documented SCD patient,9

188
advances in understanding its pathophysiology and management have been slow. 6,8
However, it is generally believed that SLU has multifactorial etiology.6,8 Hemolysis
intensity, and deposition of hemolysis products, depletion of nitric oxide and endothelial
function impairments have been implicated in its pathophysiology. 4,5,6,7,8,10 In addition,
SLU is believed to be rare in some parts of the world where prevailing genetic factors
are thought to ameliorate its occureence thus highlighting possible roles for
environmental and geographical factors. 6,8,11 Although, some studies have been
dedicated to the description of SLU,4,5,6,7,8,,10,12 very few studies have solely described
SLU among the young SCD population.4-8,10,12,13
In Nigeria, there is scanty information on SLU among young SCD patients.
Most of the previous studies were conducted among mixed populations of adults and
children.7,13,14 This leaves information on SLU among young SCD patients largely
unknown. This study was carried out on a cohort of young Nigerians with SCD. We
aimed to corroborate or dispute whether SLU is related to some laboratory markers,
hemolysis sub-phenotype and socio-demographic factors. Findings from this study
could help in improving the knowledge on factors influencing the occurrence of SLU
phenotype among young SCD patients.
PATIENTS AND METHODS
This was a cross-sectional study conducted on 109 hydroxyurea-naïve children
and adolescents with SCD in steady state and, who are regular attendees at the pediatric
hematology unit of the Ekiti State University Teaching Hospital (EKSUTH), Ado Ekiti,
Ekiti State, in Southwest Nigeria. Sixty-seven healthy children who accompanied their
siblings to the pediatric hematology clinic or attended the pediatrics outpatients` well
child clinic of the hospital served as the controls. To qualify for inclusion, the SCD
participants must have been on regular follow up at the clinic for a minimum of one

189
year prior to recruitment with up to date hospital records. Participants with confirmed or
suspected to have other chronic diseases apart from SCD were excluded. Also excluded
were the few SCD patients on regular blood transfusion and/or hydroxyurea therapies as
well as those whose caregivers declined to participate. SCD was initially diagnosed by
hemoglobin electrophoresis and high performance liquid chromatography (HPLC) and
was confirmed by DNA studies at the Centro de Hematologia e Hemoterapia
(Hemocentro), University of Campinas (UNICAMP), Brazil.
Ethical considerations
Written informed consents of parents/caregivers were obtained. Also, assents and
consents of patients were obtained as applicable. The study was approved by the
hospital`s Institutional Ethics and Research Committee no: A67/2016/03/003.
Data collection
Clinical, socio-demographic and laboratory data
A tested chart review form was used to extract relevant information from the hospital
records of participants regarding their steady state laboratory parameters and clinical
events. Average of at least two steady state results of laboratory parameters performed
between 3 to 6 months intervals by standard techniques were recorded for each
participant. The laboratory parameters examined for both patients and controls included
the complete blood count performed by Sysmex KX21N Haematology analyser
(Sysmex Corporation, Kobe, Japan). Serum lactate dehydrogease (LDH), bilirubin,
alanine transaminase (AST) and aspartate transaminase (AST) were measured with
standard techniques. The quantitative assessment of HbF, HbA, HbA2, HbS, and HbC
was done by high performance liquid chromatography (HPLC, Bio-Rad Variant D10,

190
USA). Steady state was defined as being free from any acute event(s) for at least one
month and transfusion free for at least three months.1
Details of the clinical events among the patients like: presence of leg ulcer and
its evolution, overt osteonecrosis, overt stroke, priapism, and the number of bone pain
crises requiring admission and/or administration of opioids within the preceding one
year were obtained. The definitions of clinical events were as previously described.15
Other information retrieved from patients’ charts included the biodata and patients were
classified into socioeconomic groups based on the educational level and occupation of
the parents/caregiver.16
Data Analysis
The GraphPad Prism Program, version 5 for Windows (San Diego, California, USA)
was used for the statistical analysis. The normal distribution of the quantitative variables
was verified by the Kolmogorov-Smirnov and Shapiro-Wilk tests. Continuous variables
with non-normal distribution were expressed in median and analyzed by the Mann-
Whitney tests for comparison of two independent groups. Chi-Square test or Fisher`s
Exact Test was used to compare categorical variables as applicable and level of
statistical significance was set at P < 0.05.
RESULTS
The patients were made up of 101 HbSS (SCA) and 8 HbSC. They consisted of
72 males and 37 females with median age of 9, range 2 - 21years. The controls
consisted of 40 males and 27 females and were made up of 22 sickle cell trait (HbAS) &
45 HbAA, with median age of 9, range 2- 18years. The SCD patients have been on

191
follow up for a median of 4 years, range 1.5 -14years. There were no differences in the
socio-biographic data of patients and controls (Table 1).
Comparison laboratory parameters between patients and controls
There were significant differences between the patients and controls in all
laboratory parameters p<0.0001 respectively. (Table 1)
Prevalence and description of leg ulcer among patients
In general, only six (5.5%) patients had SLU (both active and healed) and they
were all HbSS patients (three males and females each) with median age of 17, range 14-
21years, thus representing 5.9% of this group. The leg ulcers were completely healed in
three (50%) after a median duration of five months (range 3 – 6 months), and yet to heal
in the remaining three patients, two of whom are having recrudescence of their ulcers.
One of the two with recrudescence ulcers, a 21-year-old also had overt stroke three
months after her SLU recrudescence and was counselled for hydroxyurea treatment but
never took the drug. Two of the three males with SLU also had priapism. The ulcers
were located on the ankles in 5 (83.3%) and right big toe in 1 (16.7%). There was a
preceding history of trauma in 4 (66.7%) and this included a case of traditional
scarifications for local therapeutic purposes.
Comparison of laboratory parameters between SCA patients with and without leg
ulcer
Although the LDH, bilirubin, AST, platelet and WBC counts of the patients with
SLU were relatively higher compared to their peers without leg ulcer, these values did
not attain statistical significance (p>0.05). Similarly, the lower values of Hb, RBC, and

192
HbF of the patients with SLU compared to their non-SLU HbSS counterparts, did not
attain statistical significance (Table 2).
Associations between leg ulcer phenotype, clinical events and socio-demographic
data of SCA patients
The patients with SLU were relatively older compared to their peers: median
age, 17.5 years (14 – 21) vs 9 years (2 – 18), p=0.0002. They were all from the low
socioeconomic class: low class 6 (12.5%) vs others (middle & upper) 0 (0%), p=0.0097.
They had less bone pain episodes and the males among them were more associated with
priapism (p=0.0132). However, the occurrence of leg ulcer was not differentiated by
the sex of the patients (p>0.05) Table 3.
DISCUSSION
Although improved treatment strategies like vaccinations and prophylaxis
against infections, transfusion services, use of hydroxyurea and other supportive care,
have favourably influenced the prognostic outlook of SCD, SLU still remains a
worrisome complication of the disease.7.8,10
There is scarcity of information on SLU among young African patients with
SCD despite the huge burden of SCD in the continent and this makes comparison of
data difficult. Nonetheless, although fewer than their HbSS counterparts, the
observation that none of the patients with HbSC genotype had SLU confirms the widely
held belief that, SLU is not common among this group of SCD patients.6,8,10,12 Similarly,
the observation that most cases of SLU in this study were preceded by trauma has been
previously reported in both children and adults.8,17,18 and the locations of the ulcers as
found in this study have been previously reported.8,10,17,18

193
However, the observation that SLU occurred as a result of local and unorthodox
therapeutic scarification in a child in this study, may not be unconnected with the strong
belief of Africans in some traditional practices that may be inimical to the health of
children. In some cases, these may be deleterious to the health of the patients18 as found
in this case or constitute some forms of abuse.19 There is therefore the need for more
education of caregivers to desist from such harmful practices.
Similar to previous local17 and international reports 8,10,12 the occurrence of leg
ulcer among our patients is not common within the first decade of life. Also, the 6%
prevalence of leg ulcer in this study is very similar to the 5% among the children in the
USA, 12 between 5.4 and 7.6% described locally by Akinyanju et al17 and Ideawor et al14
respectively in their studies of mixed populations of both children and adults from
Western Nigeria.
However, this is quite higher than 1.3% found among children from Southeast
Nigeria, 13 2.6% among the pediatric cohorts of a mixed study comprising both adults
and children in Brazil,20 It is nonetheless lower than the prevalences of 27% and 22%
by Madu et al7 and Bazuaye et al18 respectively, in their mixed studies of both children
and adults from Eastern and Midwestern Nigeria respectively. Similarly, it is lower
than the 75% described from groups of children and adults in Jamaica.21 These
observations suggest that the occurrence of leg ulcer increases with age and varies from
place to place.8 The studies by both Junior et al20 and Serjeant21 clearly demonstrated
that the prevalence of SLU increases with age. However, the apparently lower
prevalence of SLU among Brazilian children20, could be because of the use of
hydroxyurea by some of the children in the study. Hydroxyurea is known to ameliorate
the severity of SCD and reduce the occurrence of leg ulcer through its induction of HbF

194
and lessening of hemolysis in SCD patients.20 As noted, none of our participants was on
treatment with this drug.
In addition, the findings of association of leg ulcer with low socioeconomic
condition in this study is in tandem with observations by Minniti et al8 and Cumming et
al10 that poor socioeconomic status is a risk factor for leg ulcer among SCA patients.
The lack of sex predilection for leg ulcer in the current study has been reported among
Nigerians14 and patients in other parts of the world.5 However, one Nigerian study,17
found a male preponderance.
There is still a debate about classifying SLU, while some authors thought it is
associated with very severe phenotype of SCD,.4,5,6,20 others have argued that this is
probably not so.7 However, there is a general consensus that, it is closely associated
with hemolysis intensity and some other hemolysis-related phenotypes of SCA such as
priapism, stroke and pulmonary hypertension.4,5,6,20-22 Due to lack of facilities, we could
not confirm the diagnosis of pulmonary hypertension among our patients and only few
patients with overt stroke were diagnosed. There is therefore the possibility of missing
cases of silent infarcts. Nonetheless, most of the few male patients with priapism also
had SLU, suggesting the possibility of higher hemolysis in those affected with both leg
ulcer and priapism.
Furthermore, although not statistically significant, we observed a trend of higher
LDH, AST, and bilirubin among the SLU group while their Hb and HbF were lower,
compared to those without SLU. This is suggestive of possible higher hemolysis in the
leg ulcer group. That these differences did not attain statistical significance might be
due to the sample size of this study given that some larger studies have reported
association of hemolysis markers with leg ulcer in SCA patients.4,6,7,22

195
In this study we found that the SLU patients had less episodes of painful crises (VOC),
which is in keeping with findings by previous authors,7,23 and suggests that the two
complications (SLU and VOC) are distinct phenotypes. This supports the hypothesis
that while VOC is related to blood rheology/viscosity-associated complications, 24,25 the
SLU is linked to hemolysis.4-8,22
This study, being from a single centre, is limited by size. The apparently fewer
complications attributable to SCD phenotypes, could be due to the fact that, the study
participants were children who were relatively young as such yet to develop some of
SCD complications. Despite these limitations, the study was able to show that SLU is
not uncommon among children with SCA. In addition, some socio-demographic and
clinical associates of SLU were found.
In conclusion, this study showed that SLU occurs among young Nigerian SCA
patients with poor socio-economic background and in older children. In addition, this
study suggests that SLU is more related to hemolysis-associated SCD phenotypes thus
supporting the previous hypothesis that SLU is a distinct phenotype that is probably not
related to blood viscosity/rheology complications of SCD. There is need for more
studies on the SLU phenotype among children in order to fully understand how this
phenotype affects children with SCD.
FUNDING AND DISCLOSURES
This study was supported by grants No 2014/00984-3 from FAPESP, and grants No
2015/141693-0 from CNPq, Brazil.
The authors declare no conflict of interest with respect to this study.
ACKNOWLEDGEMENTS

196
Authors acknowledge with thanks the supports received from participants and their
caregivers/parents during the study.
REFERENCES
1. Rees DC, Williams TN, Gladwin MT. Sickle cell disease. Lancet 2010;376:179-
84
2. Piel FB, Patil AP, Howes RE, Nyangiri OA, Gething PW et al. Global
epidemiology of sickle hemoglobin in neonates: a contemporary geostatistical
model-based map and population estimates. Lancet 2013; 381:142-51
3. Diaku-Akinwumi IN, Abubakar SB, Adegoke SA, Adeleke S, Adewoye O et al.
Blood transfusion services for patients with sickle cell disease in Nigeria. Int
Health 2016;8(5):330-5
4. Kato GJ, Gladwin MT, Steinberg MH. Deconstructing sickle cell disease:
Reappraisal of the role of hemolysis in the development of clinical
subphenotypes. Blood Rev.2007;21:37-47
5. Minniti CP, Eckman J, Sebastiani P, Steinberg MH, Ballas SK. Leg ulcers in
sickle cell disease. Am J Hematol 2010;85:831-3
6. Minniti CP, Taylor JGt, Hildesheim M, O`Neal P, Wilson J et al. Laboratory and
echocardiography markers in sickle cell patients with leg leg ulcers. Am J
hematol 2011;86:705-8
7. Madu AJ, Ubesie A, Madu KA, Okwor B, Anigbo C. Evaluation of clinical and
laboratory correlates of sickle leg ulcers. Wound Rep Reg 2013:21:808-12
8. Minniti CP, Kato GJ. How we treat sickle cell patients with leg ulcers. Am J
Hematol 2016;91(1):22-30
9. Herrick J. Peculiar elongated and sickle shaped red blood cell corpuscles in a
case of severe anemia. Arch Intern Med 1910;6:517-21

197
10. Cumming V, King L, Serjeant G, Reid M. Venous incompetence, poverty and
lactate dehydrogenase in Jamaica are important predictors of leg ulceration in
sickle cell anemia. Br J Haematol 2008;142:119-25
11. Adekile AD. Mild –Phenotype of sickle cell disease: molecular basis, clinical
presentation and management recommendations. Current Paediatrics
2005;15:57-61
12. Koshy M, Entsuah R, Koranda A, Kraus AP, Johnson R et al. Leg ulcers in
patients with sickle cell disease. Blood 1989;74:1403-8
13. Chinawa JM, Chukwu BF, Ikefuna AN, Emordi IJ. Musculoskeletal
complications among children with sickle cell anemia admitted in university of
Nigeria teaching hospital (Ituku-Ozalla) Enugu. Ann. Med Health Sci
2013;3:564-7
14. Idaewor PO, Enosolease ME, Momoh MI. Leg ulcer in a population of Nigerian
patients with sickle cell anemia-twenty years experience. JnI Med &Biomedical
Res 2002;110:18-21
15. Ballas SK, Lieff S, Benjamin LJ, Dampier CD, Heeney MM, Hope C.
Definitions of phenotypic manifestations of sicle cell disease. Am J Hematol.
2010;85:6-13
16. Oyedeji GA, Socioeconomic and cultural background of hospitalized children in
Ilesa. Niger J Paediatr 1985;13:111-17
17. Akinyanju O, Akinsete I. Leg ulceration in sickle cell disease in Nigeria. Trop
Geogr Med 1979;31(1):87-91
18. Bazuaye GN, Nwannadi AI, Olayemi EE. Leg ulcers in adult with sickle disease
patients in Benin City Nigeria. Gomal J Med Sci. 2010;8(2):190-4

198
19. Olatunya OS, Isinkaye AO, Oluwadiya KS. Profile of non accidental childhood
injuries at tertiary hospital in South-west Nigeria. J Trop Pediatr 2015;
61(3):174-81
20. Junior EB, Silva DG, Torres L, Okumura JV, Lobo CL, Bonini-Domingos CR.
Severity of Brazilian sickle cell disease patients: Severity scores and feasibility
of the Bayesian network model use. Blood Cells Mol Dis 2015;54:321-7
21. Serjeant GR, Serjeant BE, Mohan JS, Clare A. Leg ulceration in sickle cell
disease; medieval medicine in a modern world. Hematol Oncol Clin North Am
2005;19:943-9ix
22. Kato GJ, McGowan V, Machado RF, Little JA, Taylor VI J, Morris CR et al.
Lactate dehydrogenase as a biomarker of hemolysis-associated nitric oxide
resistance, priapism, leg ulceration, pulmonary hypertension, and death in
patients with sickle cell disease. Blood 2006;107:2279-85
23. Ballas SK. Sickle cell anemia with few painful crises is characterized by
decreased red cell deformability and increased number of dense cells. Am J
Hematol 1991;36:122-30
24. Steinberg MH. Predicting clinical severity of sickle cell anemia. Br J Haematol
2005;129:465-81
25. Renoux C, Connes P, Nader E, Skinner S, Faes C, Petras M et al. Alpha
thalassemia promotes frequent vaso-occlussive crises in children with sickle cell
anemia through haemrheological changes. Pediatr Blood Cancer
2017;64(8):doi:10.1002/pbc.26455

199
Table 1: Bio-demographic and laboratory parameters in patients and control
Parameters SCD Patients
N = 109
Median (Range)
Controls
N = 67
Median (Range)
P value
Age in years 9.0 (2.0 – 21.0) 9.0 (2.0 – 18.0) 0.8786a
Sex Male 72 40 0.4227 b
Female 37 27
Social Class
Upper 10 5 0.7050 c
Middle 49 27
Lower 50 35
Hb (g/dl) 7.5 (6.2 – 11.2) 11.6 (8.0 – 14.2) <0.0001 a
RBC (million cells/uL) 2.8 (1.8 – 4.8) 4.5 (2.5 – 6.5) <0.0001 a
MCV (fL) 80.9 (55.9 – 115.0) 79.0 (60.4 – 102.6) <0.0001 a
HbF (%) 8.4 (0.2 – 28.5) 0.8 (0 – 5.8) <0.0001 a
WBC (x 103/uL) 12.6 (4.1 – 29.3) 6.6 (4.5 – 14.4) <0.0001 a
Platelet (x 103/uL) 343.0 (108.0 – 832.0) 278.0 (117.0 – 591.0) <0.0001 a
LDH (IU/L) 771.4 (166.0 –
1860.0)
360.0 (150.0 – 993.0) <0.0001 a
AST (IU/L) 42.0 (12.0 – 89.0) 20.0 (6.0 – 75.0) <0.0001 a
ALT (IU/L) 20.0 (8.0 – 77.0) 10.0 (4.0 – 45.0) <0.0001 a
Total bilirubin
(mg/dl)
1.8 (0.4 – 8.1) 0.4 (0.1 – 2.2) <0.0001 a
NB: Statistical significant p values are in bold fonts, a=Mann-Whitney Test, b=Fisher`s Exact
Test, c= Chi-Square Test, SCD=Sickle cell disease.

200
Table 2: Laboratory parameters in SCA patients with and without leg ulcer
Parameters SCA wIth leg ulcer
N = 6
SCA wIthout leg
ulcer
N = 95
P value
Hb (g/dl) 7.1 (6.2 – 8.1) 7.5 (6.3 – 10.1) 0.3356 a
RBC (million cells/uL) 2.5 (2.0 – 2.8) 2.8 (1.8 – 4.8) 0.067 a
HbF (%) 7.1 (3.7 – 10.7) 9.4 (0.9 – 28.5) 0.377 a
WBC (x 103/uL) 14.5 (10.0 – 21.3) 13.2 (6.1 – 29.3) 0.4421 a
Platelet (x 103/uL) 473.5 (207.0 – 669.0) 361.0 (108.0 – 832.0) 0.247 a
LDH (IU/L) 972.0 (681.7 –
1682.0)
800.0 (197.0 –
1860.0) 0.095
a
AST (IU/L) 40.0 (35.0 – 56.0) 36.0 (7.0 – 89.0) 0.1541 a
Total bilirubin
(mg/dl)
2.1 (1.3 – 4.1) 1.8 (0.4 – 8.1) 0.570 a
NB: Statistical significant p values are in bold fonts, a=Mann-Whitney Test, SCA=Sickle cell
anemia.

201
Table 3: Associations between leg ulcer phenotype, clinical events and bio-demographics
of SCA patients
Parameters SCA with leg ulcer
N = 6
SCA without leg ulcer
N = 95
P value
Age in years 17.5 (14.0 – 21.0) 9.0 (2.0 – 18.0) 0.0002 a
Sex Male 3 64 0.4016 b
Female 3 31
Social class
Lower 6 42 0.0097 b
Others
(Upper & Middle)
0 53
Bone pain crisis
(VOC)
0.5 (0 -1.0) 2 (0 – 6.0) 0.0382 a
Osteonecrosis 1 4 0.2686 b
Stroke 1 3 0.2203 b
Priapism (Males only
total number = 67)
(N = 3)
2
(N =64)
3
0.0132 b
NB: Statistical significant p values are in bold fonts, a=Mann-Whitney Test, b=Fisher`s Exact
Test, SCA=Sickle cell anemia.

202
ANNEXES
Annex 1
Table : Effects of hydroxyurea treatment on biologic markers of HbS-β thalassemia patients
Parameters HbSS treated with hydroxyurea (N=12)
NO hydroxyurea treatment (N=12)
P values
RMP(events/mL) 60,000.0 (0.0 -440000.0)
60,000 (0 – 280000)
0.8593
Plasma Hb (mg/dL) 62.6 (34.0 – 134.0) 75.6(40.0 – 196) 0.312
Haptoglobin (ng/mL) 2832.0 (480.0 – 11730)
2569.0 (540.0 – 18180)
0.5834
Heme (µM) 48.0 (22.9 – 94.0) 52.3 (23.0 – 119.0) 0.977
Hemopexin (µg/mL) 556.0 (108.0 – 1805.0)
310.0 (127.0 – 1642)
0.6236
HbF (%) 18.9 (0.6 – 35.2) 9.3 (2.0 – 26.2) 0.1487
HbS (%) 67.6 (56.7 – 82.4) 70.8 (46.0 – 89.7) 0.583
RBC ( million cells/uL)
2.8 (2.4 – 4.4) 4.0 (3.2 – 6.1) 0.0009
MCV (fL) 96.7 (79.4 – 118.4) 73.8 (61.8 – 85.9) 0.0002
Total bilirubin (mg/dL)
1.5 (0.6 – 5.1) 1.3 (0.6 – 2.2) 0.418
Unconjugated bilirubin (mg/dL)
1.2 (0.4 – 4.2) 0.9 (0.4 – 1.8) 0.543
Hb (g/dL) 8.7 (6.8 – 11.5) 9.5 (7.2 – 11.0) 0.193
Reticulocyte (×109/L) 232.0(52 – 455) 270.9 (136.0 – 561.0)
0.544
LDH (IU) 276.0 (192.0 – 531.0)
294.0 (128.0 – 496.0)
0.623
Platelet ( X 103/uL) 391.0 (172.0 – 479.0)
332.0 (76.0 – 755.0)
0.298
WBC ( X 103/uL) 5.5 (4.2 – 11.1) 9.2 (4.1 – 16.4) 0.119
NB: Significant p values are in bold fonts, Test statistics= Mann-Whitney test, RMP-Red blood cell microparticle, HbF-Fetal Hemoglobin, RBC-Red blood cell, Hb-Hemoglobin concentration, HbS- Hemoglobin S, MCV- Mean corpuscular volume, WBC-White blood cell count, LDH-Lactate dehydrogenase.

203
Annex 2
Figure annex 02: Linkage disequilibrium map of the SNPs pairs.

204

205
ANEXO:

206

207

208

209