New sources of big data for precision medicine: are we ready?
67
New sources of big data for precision medicine: are we ready? Melbourne Academic Centre Annual Research Symposium 19-June-2014 Fernando J. Martin-Sanchez Professor and Chair of Health Informatics Melbourne Medical School & Director, Health and Biomedical Informatics Centre (HaBIC)
-
Upload
health-and-biomedical-informatics-centre-the-university-of-melbourne -
Category
Health & Medicine
-
view
869 -
download
1
Transcript of New sources of big data for precision medicine: are we ready?

New sources of big data for precision medicine:
are we ready?
Melbourne Academic Centre Annual Research Symposium
19-June-2014
Fernando J. Martin-Sanchez Professor and Chair of Health Informatics
Melbourne Medical School &
Director, Health and Biomedical Informatics Centre (HaBIC)
2014 FMDHS Research Review

Outline
• New sources of (Big) data • Evolution of the concept -
Precision medicine • Strategic initiatives in UK
and USA • Relevant research • Are we ready? • Conclusions

New sources of (Big) data

Data generation in Biomedicine
• Human Genome – first decoded in
2003 after one decade of work
– nowadays takes one day
• PubMed – 5000 biomedical
research articles are published daily
– Over 22 mill articles
• Global size of “Big Data” in Healthcare stands at roughly 150 Exabytes (1018) in 2011, increasing at a rate between 1.2 and 2.4 Exabytes per year. (SAS)

Genome regulation
Microbiome
Epigenome
Exposome
Inter and intra individual
genetic variation
Phenome levels

Human Genetic Variation – 1000 Genomes project
Nature 491, 56–65 (01 November 2012)

Mapping the Epigenome
New York Times

ENCODE – Encyclopedia of DNA Elements
nature.com/encode

Inter e Intra-tumour heterogeneity


In 2008 the same team described the chemical composition of human cerebrospinal fluid and in 2011 they determined the chemical composition of human blood.
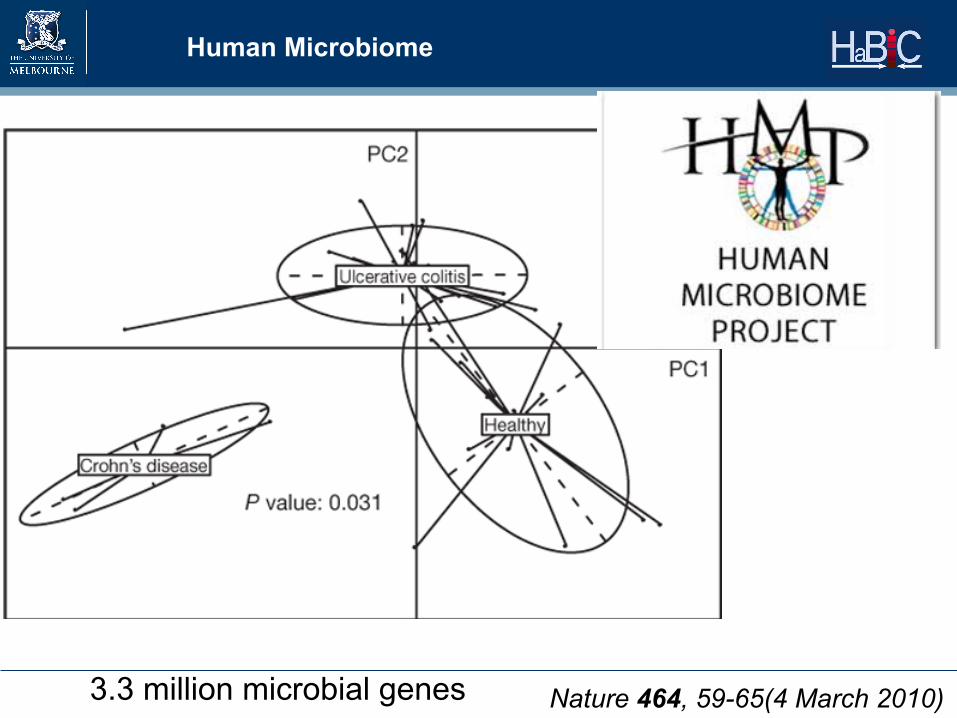
Human Microbiome
Nature 464, 59-65(4 March 2010) 3.3 million microbial genes

Exposome
The exposome has been defined as the life-long exposure to environmental factors of an individual.

Genome Exposome
Phenome
Biomarkers (DNA sequence, Epigenetics) Environmental risk factors (pollution, radiation, toxic agents, …)
Anatomy, Physiological, biochemical parameters (cholesterol, temperature, glucose, heart rate…)
Social media / Personal health record / EMRs
Availability of new sensors for data collection

Evolution of the concept Precision Medicine
Origin
• In Ancient Greece, Rufus of Ephesus suggested that drugs have different effects on different people.

Origin
• In 1902, Archibald Garrod suggested individuals were different not only phenotypically, but also at the biochemical level.

Origin
• The term ‘personalised medicine’ was coined in 1999 by Robert Langreth and Michael Waldholz (Wall Street Journal reporters) in an article to describe the development by pharmaceutical companies of:
“a cornucopia of personalized medicines that will produce huge profits into the next
century”.

Evolution
• Clinicians have always practiced personalized medicine, using personal health information to make decisions on diagnosis and treatment.
• When we refer to personal health information we are including genetic, physiological, anatomical, environmental risk factors, socio economic issues, cultural and psychological aspects as well as the familial and individual health history.

Evolution – Genomic Medicine
• However, our ability to collect individual genetic and environmental data has been very limited until recently.
• One major milestone in overcoming those barriers was the Human Genome Project, which together with advances in DNA sequencing technologies, has facilitated a fast and affordable access to personal genetic variation data.
• This marked the beginning of the Genomic Medicine age in the early 2000’s

Evolution – Molecular medicine
• Our increased knowledge about the molecular causes of complex diseases represents another key aspect of the advances that we are witnessing in this field.
• Microarray-based technologies opened the door to the study of functional aspects of DNA and protein expression, which has been referred to as molecular medicine.
Comprehensive molecular portraits of human breast tumours The Cancer Genome Atlas Nature 490, 61–70 (04 October 2012)

Evolution – P3 and P4 Medicine
• The term P4 medicine, coined by Leroy Hood, tries to amalgamate most of these previous objectives, making a greater emphasis on the importance of preventative and participatory medicine.

Evolution P5, P6, …
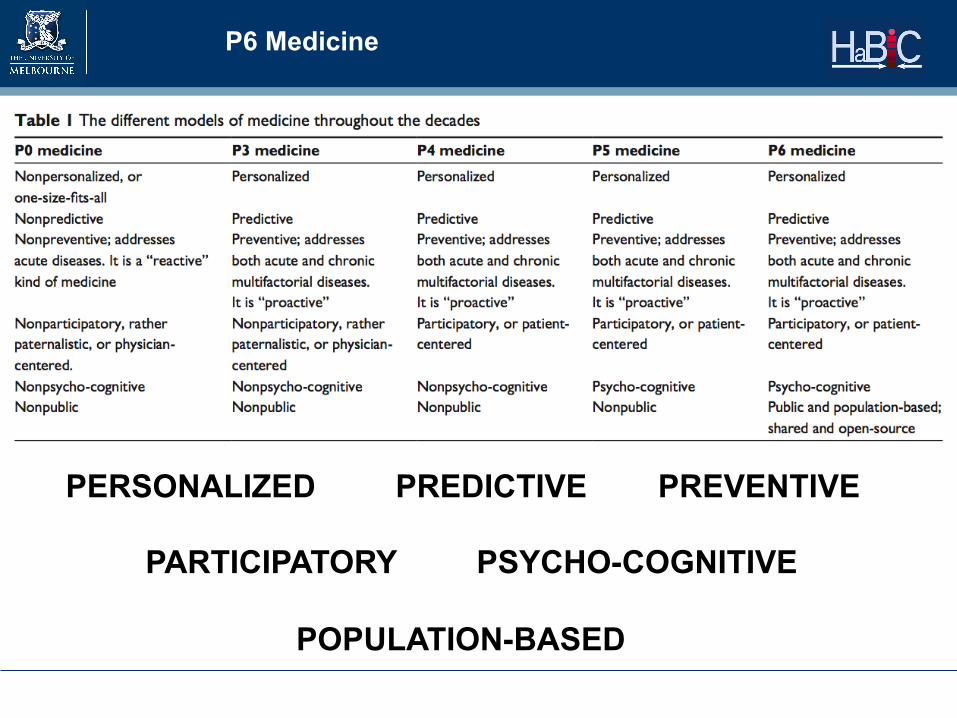
P6 Medicine
PERSONALIZED PREDICTIVE PREVENTIVE PARTICIPATORY PSYCHO-COGNITIVE POPULATION-BASED

Evolution – Stratified medicine
• US President’s Council of S&T noted that personalised medicine ‘refers to the tailoring of medical treatment to the individual characteristics of each patient’.
• It does not literally mean the creation of drugs or medical devices that are unique to a patient, but rather the ability to classify individuals into subpopulations that differ in their susceptibility to a particular disease or their response to a specific treatment.
Precision medicine
• Precision Medicine is an approach to discover and develop medicines, vaccines or routes of intervention (behavior, nutrition, etc.) that enable disease prevention and deliver superior therapeutic outcomes for patients, by integrating “Big Data”, clinical, molecular (multi-omics including epigenetics), environmental and behavioral information to understand the biological basis of disease.
• This effort leads to better selection of disease targets and identification of patient populations that demonstrate improved clinical outcomes to novel preventive and therapeutic approaches.
C.M. Christensen et al.. The innovator’s prescription a disruptive solution for health care. McGraw-Hill, 2008

Evolution - Precision medicine
• Work in this area is aimed at redefining disease classification, identifying common underlying causes and representing them into new taxonomies.
Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease (2011)

Academy of Medical Sciences 2013
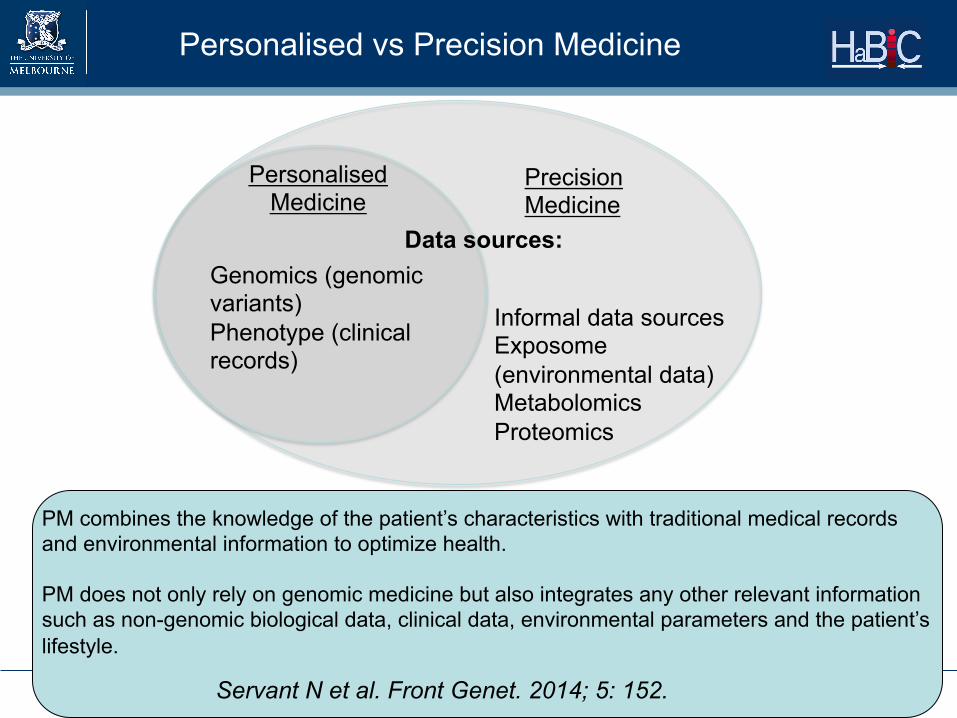
Personalised Medicine
Data sources:
Precision Medicine
Informal data sources Exposome (environmental data) Metabolomics Proteomics
Genomics (genomic variants) Phenotype (clinical records)
Personalised vs Precision Medicine
PM combines the knowledge of the patient’s characteristics with traditional medical records and environmental information to optimize health. PM does not only rely on genomic medicine but also integrates any other relevant information such as non-genomic biological data, clinical data, environmental parameters and the patient’s lifestyle.
Servant N et al. Front Genet. 2014; 5: 152.

Personalised medicine
• Improving therapy • Looking for the right drug for
the right people
• Companion diagnostics to stratify patients
• Use of genomics data
• Static - “Snapshot”
Precision medicine
• Improving Diagnosis • Looking for the right drug for
the right disease • New taxonomy of disease and
disease reclassification
• New/refined diagnostics methods • Use of molecular (-omics) and
other (i.e. exposome) data sources • Dynamic stratification - Modelling
patient journeys
Personalised vs Precision Medicine

Strategic initiatives in UK and USA
UK NHS
• New CIO – Simon Stevens • Urged the service to become a world leader in
personalised medicine. • National Institute for Health Research
Health Informatics Collaboration (HIC) • Five participating NHS trusts
• This initiative will deliver IT capability to support the sharing and use of NHS data for research.

http://www.mrc.ac.uk/research/initiatives/health-and-biomedical-informatics/

The Lancet Vol 383 March 29, 2014

UK
• The MRC, in partnership with nine other government departments, research councils and charities, have committed over £90m in several initiatives that are aimed at supporting health informatics research, infrastructure and scientists. Their ultimate aim is to build a sustainable capability in health and biomedical informatics in the UK. Ø The Farr Institute of Health Informatics Research £39m was
awarded to four centres based at University College London, and the universities of Manchester, Swansea and Dundee.
Ø UK Health Informatics Research Network (UKHIRN) Ø Strategic Skills Fellowships Ø Medical bioinformatics initiative - £32m - six strategic awards to
combine clinical, health and bioinformatics data Ø Centres for doctoral training - three multi-disciplinary Centres for
Doctoral Training (CDTs), which align with biomedical informatics. Ø ELIXIR partnership (EC infrastructure)

Other UK initiatives
MRC-DH - New £150m initiative in Clinical Research Infrastructure to bring into practice novel technologies to address major scientific challenges relating to the stratification of diseases
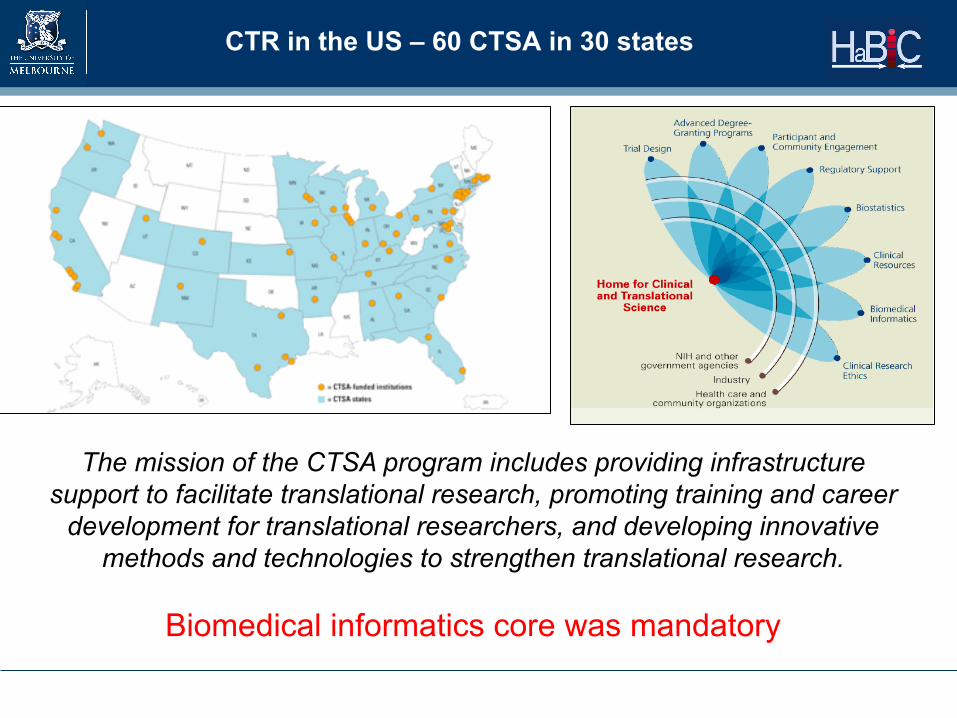
CTR in the US – 60 CTSA in 30 states
The mission of the CTSA program includes providing infrastructure support to facilitate translational research, promoting training and career
development for translational researchers, and developing innovative methods and technologies to strengthen translational research.
Biomedical informatics core was mandatory


USA Clinical Informatics – Medical subspecialty
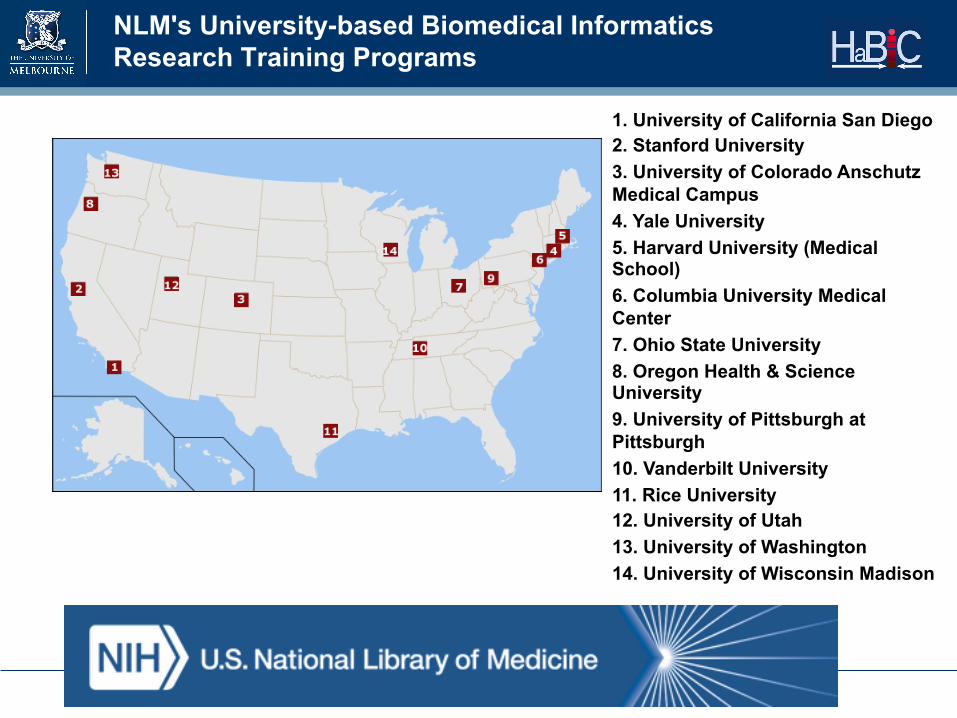
NLM's University-based Biomedical Informatics Research Training Programs
1. University of California San Diego 2. Stanford University 3. University of Colorado Anschutz Medical Campus 4. Yale University 5. Harvard University (Medical School) 6. Columbia University Medical Center 7. Ohio State University 8. Oregon Health & Science University 9. University of Pittsburgh at Pittsburgh 10. Vanderbilt University 11. Rice University 12. University of Utah 13. University of Washington 14. University of Wisconsin Madison

Relevant research

TCGA Genome Pan-Cancer Atlas
• The Cancer Genome Atlas Research Network, John N Weinstein, Eric A Collisson, Gordon B Mills, Kenna R Mills Shaw, Brad A Ozenberger, Kyle Ellrott, Ilya Shmulevich, Chris Sander & Joshua M Stuart Nature Genetics 45, 1113–1120 (2013)
eMERGE
• High-throughput phenomics • Disease specific algorithms scanning across
electronic medical records - generate structured, standardized, anonymized, clinical data sets for research

Exposome related projects around the world
• USA - Funded by the NIEHS – HERCULES. It is a joint centre between Emory University and
Georgia Institute of Technology
• Europe - European Commission funded
– HELIX – Coordinated by the Centre for Research in Environmental Epidemiology (Barcelona, Spain)
– EXPOSOMICS Coordinated by Imperial College of London
– HEALS - Coordinated by the University Pierre and Marie Curie (Paris, France) Health Environment Association based on Large population Surveys
100 Person Wellness Project

Are we ready?

Building blocks
Health Informatics
genomics, genomic epidemiology, bioinformatics and computational biology, molecular biology, biochemistry, stem cells, pharmacology, animal model testing, clinical trials, clinical epidemiology & biostatistics, clinical genetics, biomedical engineering, imaging, health economics, health services research.


Bioinformatics is different from Health informatics
HEALTH & BIOMEDICAL INFORMATICS BIOINFORMATICS & COMPUTATIONAL SYSTEMS BIOLOGY

Health informatics – clinical data
• Data about humans that arises from a growing number of sources and contexts:
– Clinical research – Clinical practice - EHRs – Patient and disease
registries – mHealth apps – Smart devices and
sensors – Environmental data – Social media data
• Distributed (EMR, clinical depts) • Different formats (text, images,
numeric, videos,..) • Same data exists in different
systems • Patient generated data • Data is structured and unstructured • Inconsistent/variable definitions • New data coming out every day • Complexity of data (the human
body) • Changing regulatory requirements • Privacy issues Adapted from Dan LeSueur (Health Catalyst)
Why healthcare data is different…

Health Informatics
Bioinformatics
Proteomics and
Metabolomics Data
Gene expression
Data
Genomic Data
Patient generated
Data
Population Data
Clinical Data
HaBIC @UoM

HaBIC
• The University has recently established a collaborative Health and Biomedical Informatics Centre (HaBIC), with support from the Faculty of Medicine, Dentistry and Health Sciences, the School of Engineering and IBES.
Research
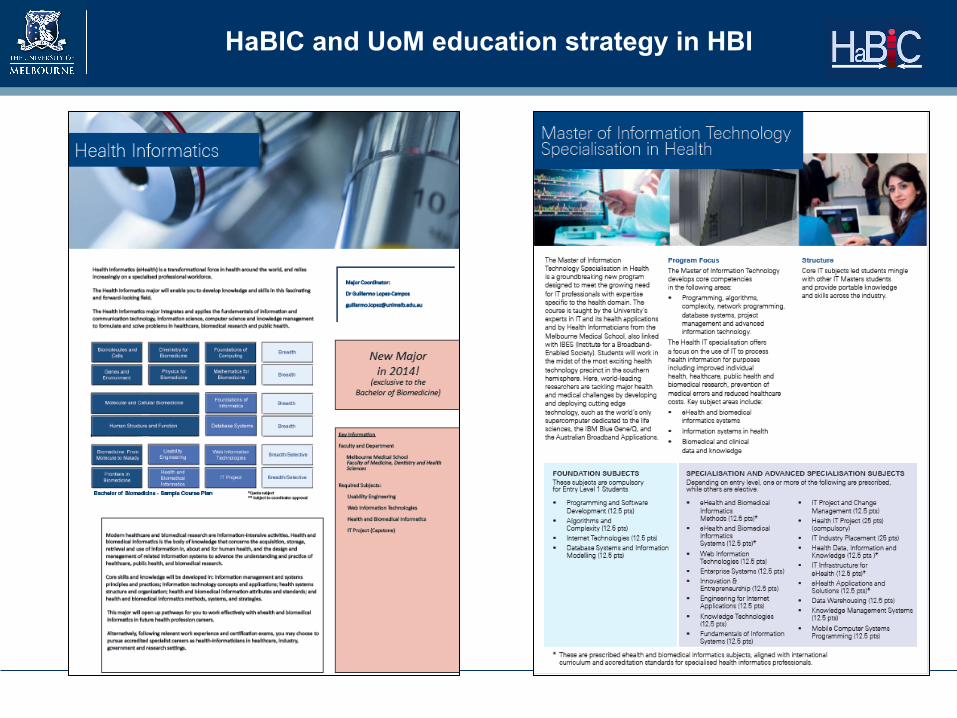
HaBIC and UoM education strategy in HBI


Available platforms
• Infrastructure: – UoM High-end computing. Alliance with ITSr – Research
Cloud, storage facilities, supercomputing – VLSCI
• Platforms for data integration – Biogrid (43 hospitals, clinical data, genomics) – GRHANITE (GPs, labs, rural, )
• Research support tools – REDCap – SAS Visual Analitics – Galaxy - GVL – I2B2

Researcher
Hospital data
GP, labs, pharmacies data
Researcher-entered data

Problems • Lack of understanding
(differences with IT, bioinfo)
• Few training programs • HI is not recognised as an
occupation, Field of Research or Field of Education
• No certification or accreditation
• Research grants are difficult (NHMRC, ARC)
• Electronic medical records
• Sense of failure in Health IT
• Unclear academic home
Solutions?
• This talk, publications, education
• University courses
• Actions through HISA, ACHI
• CHIA program
• Specific Panel and experts appointed as assessors
• Participation in the Ministerial Health Sector IT Advisory Council (DoH Victoria)
• Ascribe to a Department
Current situation of Health Informatics in Australia

Conclusions

Current meaning
• Precision medicine enables a safer, more efficient, preventive and proactive medicine, but needs to tackle the complexity and diversity of personal health information, beyond the genome sequence.
Topol E. Cell 2014


Adapted from: Stead et al. 2011, Acad. Med.

• Both research into and clinical application of stratified medicine, will require comprehensive and robust biomedical and health informatics systems – a key rate-limiting step.
Stratified Medicine: Principles, Promise and Progress UK Academy of Medical Sciences 2013

Biomedical Informatics
Martin-Sanchez F et al. J Am Med Inform Assoc. 2014
Biomedical Informatics

© Copyright The University of Melbourne 2014
Thank you for your attention!