Neonatal Herpes Simplex Infections MAJ Mark Burnett Pediatric ID Fellow MAR 2003.
35
Neonatal Herpes Simplex Infections MAJ Mark Burnett Pediatric ID Fellow MAR 2003
-
Upload
kerry-goodman -
Category
Documents
-
view
224 -
download
0
Transcript of Neonatal Herpes Simplex Infections MAJ Mark Burnett Pediatric ID Fellow MAR 2003.

Neonatal Herpes Simplex Infections
MAJ Mark BurnettPediatric ID Fellow
MAR 2003

Neonatal HerpesBackgroundA Case StudyTypes of InfectionsRisks of InfectionDiagnosticsTreatmentSummary

Herpes Infections“Herpes” – from the Greek “to creep, crawl”“Herpetic eruptions” described as early as 100 AD1960’s – HSV1 and HSV2 differentiated
HHV1 – HSV1HHV2 – HSV2 HHV3 – VZVHHV4 – EBVHHV5 – CMVHHV6 – Causes?HHV7 – HHV8 -

A Case Study – A.B.Term infant born to a 22 y/o GBS+ mother with no Pmhx of HSV-24 doses of IV PCN given PTDROM <18 hours PTD, no maternal feversForceps deliveryAPGARS of 9/9Well until fever to 101.7 at 30 hrs of lifeFever work-up initiated
A.B.WBC 23K (50S 2B 38L)AST 98 ALT 92CSF 48 WBC 2650 RBC Pro 93/Glu 53HSV PCR, Enteroviral PCR, HSV Surface cx – sentExam unremarkableAmp/Gent/Acyclovir initiatedFevers persisted over next 13 hours, again spiking to 101.5AST 147 / ALT 93 two days later

A.B. – additional infoNo history of HSV reported in mother, fatherMother without febrile illnessNiece with a “cold sore” visited prior to delivery, and “held the baby” after he was bornLP repeated two days after initial study with normalization of cell count

A New Development
Questions?What diagnostic tests could we perform, and how reliable are they really?Would it be worthwhile to run tests on mom?Is the niece’s “cold sore” a “red herring” – what are the risks?Bottom line – how worried should we be about HSV, and how would we treat it?

Neonatal HSV 1 in 2,500-5,000 deliveries / 500-1500 per yr.Birth to 7 weeks of lifeHSV2 = 70-75%, HSV1 = 25-30%3 Main Types
Skin, Eye, Mouth (SEM)CNSDisseminated Disease (DISSEM)
At Risk: Premature, ROM >6hr, Fetal scalp monitoringCan be acquired congenitally, during the birth process, and in the post-partum period

Routes of Transmission85% via infected maternal genital tract
Ascending infection?En route
10% postpartum5% (or less) – intrauterine/congenital infection

Congenital HSVRare, most devastatingOnly 50 cases describedSkin vesiclesChorioretinitisMicrocephalyMicro-ophthalmiaIUGR
Archival Photo:HSV “In Utero” Healed by TimeOf Birth – WithMicrocephally

Skin, Eye, Mouth (SEM)Approximately ½ of all HSV infections1st-2nd week presentationLimited to skin, eye, mouth/mucous membranes60-70% of untreated patients progress to CNS/disseminated disease
Groin Vesicles 16 Days of LifeHSV-1, This InfantHad a Cardiac Cath(Groin Line) At 3 Days of Life

SEM (cont)Long term neurologic sequelae seen in 30% of cases – even if treatedOphthalmology involvement

“Presenting Part” (SEM)
HSV 2 Arm Lesions9 Days of LifePresenting Limb in a 34 Week Premature Infant

Scalp Lesions11 Days of LifeHSV-2, Monitored With Scalp Lead
Scalp Monitors
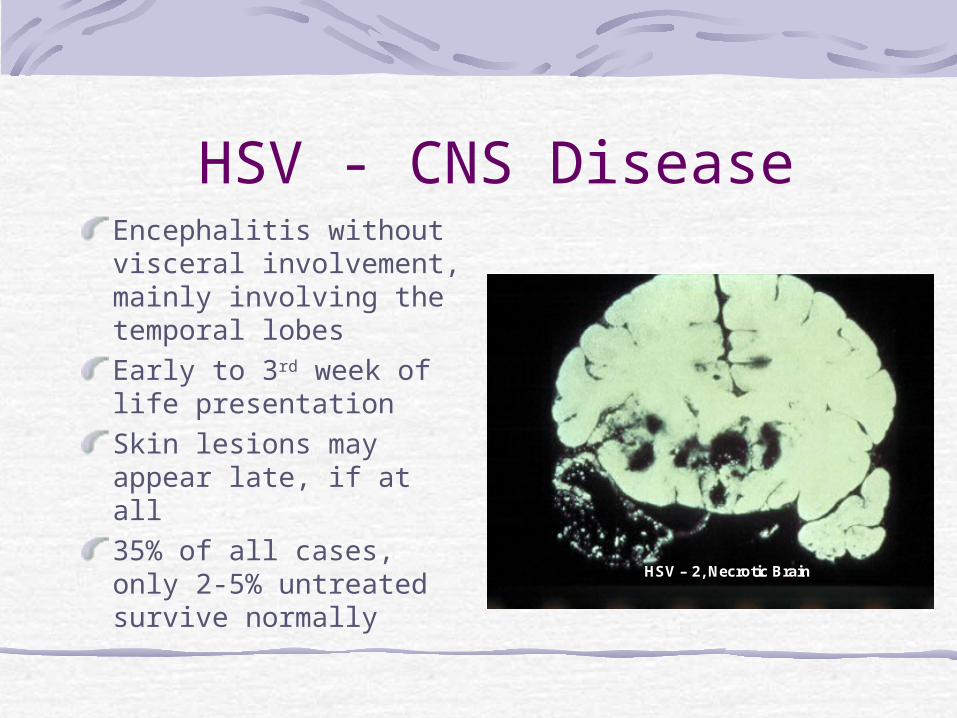
HSV - CNS DiseaseEncephalitis without visceral involvement, mainly involving the temporal lobesEarly to 3rd week of life presentationSkin lesions may appear late, if at all35% of all cases, only 2-5% untreated survive normally
HSV – 2, Necrotic Brain

Radiographic Findings

Disseminated DiseaseApproximately 20% of all infections
HepatitisPneumonitisDIC
Infant may be ill on first day of lifeSkin lesions appear late, or not at all

Signs

Postnatal acquisitionMost commonly HSV1Moms with HSV
MaskBreastfeeding – O.K. if without lesions
The Mohel and the Mezizah

Contacts“Personnel with an active herpetic whitlow should not have direct patient care of neonates”.Family transmission has been described

Morbidity and Mortality
Stretch Break

Take Home MessageInfection is most common when a mother develops a genital infection late in pregnancy ( her primary HSV1 or HSV2 infection) – then delivers before the development of protective maternal antibodies
Herpes Simplex Approximately 5% of the general population has been diagnosed with genital herpes – but approximately 20-30% of women may be infected with HSV-2Viral shedding occurs without identifiable lesions on 1-3% of days

Maternal Testing?Identify discordant couples to avoid transmission in the third trimester
If mom is HSV1/HSV2 negativeIf mom is HSV2 negativeIf mom is HSV2 positive – risk is low for a vaginal delivery?
Is testing after delivery going to be helpful?Will blood tests of the baby be helpful, or just reflect mom’s status?Psychosocial ramifications?

Herpes during PregnancyAs many as 2% of pregnant women are infected with HSV2 during pregnancy25% of women with a history of genital herpes have an outbreak at some time during their pregnancy, 11-14% at time of delivery
36% at delivery for those with first infection!Virus is recovered from 1% of asymptomatic women at delivery

What is the risk?Vaginal delivery when mom has presence of first symptomatic lesions – 50%Vaginal delivery when mom is asymptomatic, but is newly infected – 33%Vaginal delivery when mom has recurrent lesions – 4%Vaginal delivery when mom has a history of herpes lesions in past, none presently – 0.04%

OB Management70’s-80’s – weekly HSV cultures1988 – patient examined at delivery, Cesarean delivery if: (no data)
Identifiable genital lesionsPatient describes prodromal symptoms
Vaginal delivery for those with hx onlyPrimary infection diagnosed - treatEstimated $2-4 million to prevent each case20-30% of infants who are diagnosed with neonatal herpes are delivered by Cesarean delivery

Diagnostics
HSV Cx – positive in 1-2 days (cytopathic effect)DFA – sensitivity/specificity in the 75%-85% range

PCR TestingDetects minute amounts of DNA, RNA
DISSEM – 93%CNS – 76%SEM – 24%
False negative may occur if CSF is obtained “too early”Order through IVF!

Diagnostics (cont)Surface cultures
Mouth (40-50%)Eyes (25%)RectumSkin
CulturesStool UrineCSF >100 WBC/Inc. Pro
Tzanck – neither sensitive nor specific

Treatment - AcyclovirSEM infections
60mg/kg/day divided q8h for 14 daysMay be lengthened to 21 days in the near futureOral Acyclovir needed later in life?
DISSEM and CNS HSV infections60mg/kg/day divided q8h for 21 daysRe-tap if CNS disease exists prior to d/c
Watch for neutropenia – 2x week ANCs

Questions / ControversiesWould maternal “pre-treatment” change the time /clinical presentation of HSV?Should an infant delivered vaginally to a mother with active lesions be treated?Can HSV be resistant to Acyclovir?

Take Home MessagesMost neonates with HSV infection are born to mothers with asymptomatic genital shedding at delivery, with no history of genital herpetic lesionsNo one test is 100% sensitive / specificKeep HSV in mind
How would you manage our case?