
Nej Mc 081387
3
correspondence n engl j med 359;12 www.nejm.org september 18, 2008 1291 cultural and social histories. Although it is impos- sible for other countries to copy these histories, Spain and Italy provide important policy lessons on how to reduce inequalities in health: tackling immediate determinants of such inequalities may be an effective way to reduce health inequalities in countries with a reasonable level of welfare pro- vision. Since the publication of our article, we have discovered an error in the mortality data from England, related to an ambiguity in the label of one educational category as used in this data set. The corrected data are available with a revised ver- sion of our article and the full text of this letter at www.nejm.org. These data show that we under- estimated inequalities in mortality in England and Wales, but none of the conclusions of our article are substantially affected. Johan P. Mackenbach, M.D., Ph.D. Irina Stirbu, M.Sc. Anton E. Kunst, Ph.D. Erasmus MC 3000 CA Rotterdam, the Netherlands [email protected] Eikemo TA, Huisman M, Bambra C, Kunst AE. Health in- 1. equalities according to educational level in different welfare re- gimes: a comparison of 23 European countries. Sociol Health Illn 2008;30:565-82. Espelt A, Borrell C, Rodríguez-Sanz M, et al. Inequalities in 2. health by social class dimensions in European countries of dif- ferent political traditions. Int J Epidemiol 2008 March 13 (Epub ahead of print). Dahl E, Fritzell J, Lahelma E, Martikainen P, Kunst A, Mack- 3. enbach J. Welfare state regimes and health inequalities. In: Siegrist J, Marmot M, eds. Social inequalities in health: new evidence and policy implications. Oxford, England: Oxford University Press, 2006:193-222. Kunst AE, Groenhof F, Mackenbach JP, Health EW. Occupa- 4. tional class and cause-specific mortality in middle-aged men in 11 European countries: comparison of population-based studies. BMJ 1998;316:1636-42. Table 1. Patients with Positive Tests for Heparin-Induced Thrombocytopenia.* Country OSCS-Contaminated Heparin Distributed Period before Contamination (November 1, 2006, to February 28, 2007) Period of Contamination (November 1, 2007, to February 28, 2008) Increase in No. of Patients with Positive Tests no. of patients with positive tests/total no. tested % Canada No† 45/373 51/409 13.3 Germany Yes 32/459 64/405 100.0 * Patients were considered to have positive tests for antibodies against heparin-induced thrombocytopenia if both a washed-platelet activation assay and a platelet factor 4–dependent IgG enzyme immunoassay were positive. Patients who underwent repeated tests were counted only once. OSCS denotes oversulfated chondroitin sulfate. † A recall of minimal amounts of OSCS-contaminated products occurred in Canada, without any reports of anaphylac- tic reactions. Contaminated Heparin To the Editor: Kishimoto et al. (June 5 issue) 1 report that contamination of heparin with over- sulfated chondroitin sulfate (OSCS) can induce anaphylactoid reactions through activation of the contact system. OSCS can also induce a clinical syndrome that is indistinguishable from immune heparin-induced thrombocytopenia, 2 since the antigens are not heparin-specific but can be gen- erated by other polysaccharides depending on the chain length and degree of sulfation. 3 Hyper- sulfated polysaccharides behave as “super-hepa- rins” in the induction of immune thrombocyto- penia. 2,3 Heparin-induced thrombocytopenia is relatively common and often consequential. 4 At least 10 to 20% of affected patients die or have permanent sequelae such as stroke or limb amputation; this distinguishes heparin-induced thrombocytopenia from most other adverse drug reactions. 5 From November 1, 2007, to February 28, 2008 (the pe- riod during which anaphylactoid reactions to OSCS-contaminated heparin were observed 1 ), our two laboratories in Canada and Germany con- firmed the diagnosis of heparin-induced throm- bocytopenia in 115 patients. During this period, a substantial increase in laboratory-confirmed heparin-induced thrombocytopenia was observed in Germany, but not in Canada, possibly reflect- The New England Journal of Medicine Downloaded from nejm.org on May 2, 2011. For personal use only. No other uses without permission. Copyright © 2008 Massachusetts Medical Society. All rights reserved.
-
Upload
ickha-wulandary -
Category
Documents
-
view
8 -
download
0
Transcript of Nej Mc 081387

correspondence
n engl j med 359;12 www.nejm.org september 18, 2008 1291
cultural and social histories. Although it is impos-sible for other countries to copy these histories, Spain and Italy provide important policy lessons on how to reduce inequalities in health: tackling immediate determinants of such inequalities may be an effective way to reduce health inequalities in countries with a reasonable level of welfare pro-vision.
Since the publication of our article, we have discovered an error in the mortality data from England, related to an ambiguity in the label of one educational category as used in this data set. The corrected data are available with a revised ver-sion of our article and the full text of this letter at www.nejm.org. These data show that we under-estimated inequalities in mortality in England and Wales, but none of the conclusions of our article are substantially affected.
Johan P. Mackenbach, M.D., Ph.D. Irina Stirbu, M.Sc. Anton E. Kunst, Ph.D.Erasmus MC 3000 CA Rotterdam, the Netherlands [email protected]
Eikemo TA, Huisman M, Bambra C, Kunst AE. Health in-1. equalities according to educational level in different welfare re-gimes: a comparison of 23 European countries. Sociol Health Illn 2008;30:565-82.
Espelt A, Borrell C, Rodríguez-Sanz M, et al. Inequalities in 2. health by social class dimensions in European countries of dif-ferent political traditions. Int J Epidemiol 2008 March 13 (Epub ahead of print).
Dahl E, Fritzell J, Lahelma E, Martikainen P, Kunst A, Mack-3. enbach J. Welfare state regimes and health inequalities. In: Siegrist J, Marmot M, eds. Social inequalities in health: new evidence and policy implications. Oxford, England: Oxford University Press, 2006:193-222.
Kunst AE, Groenhof F, Mackenbach JP, Health EW. Occupa-4. tional class and cause-specific mortality in middle-aged men in 11 European countries: comparison of population-based studies. BMJ 1998;316:1636-42.
Table 1. Patients with Positive Tests for Heparin-Induced Thrombocytopenia.*
CountryOSCS-Contaminated Heparin Distributed
Period before Contamination
(November 1, 2006, to February 28, 2007)
Period of Contamination
(November 1, 2007, to February 28, 2008)
Increase in No. of Patients
with Positive Tests
no. of patients with positive tests/total no. tested %
Canada No† 45/373 51/409 13.3
Germany Yes 32/459 64/405 100.0
* Patients were considered to have positive tests for antibodies against heparin-induced thrombocytopenia if both a washed-platelet activation assay and a platelet factor 4–dependent IgG enzyme immunoassay were positive. Patients who underwent repeated tests were counted only once. OSCS denotes oversulfated chondroitin sulfate.
† A recall of minimal amounts of OSCS-contaminated products occurred in Canada, without any reports of anaphylac-tic reactions.
Contaminated Heparin
To the Editor: Kishimoto et al. (June 5 issue)1 report that contamination of heparin with over-sulfated chondroitin sulfate (OSCS) can induce anaphylactoid reactions through activation of the contact system. OSCS can also induce a clinical syndrome that is indistinguishable from immune heparin-induced thrombocytopenia,2 since the antigens are not heparin-specific but can be gen-erated by other polysaccharides depending on the chain length and degree of sulfation.3 Hyper-sulfated polysaccharides behave as “super-hepa-rins” in the induction of immune thrombo cyto-penia.2,3
Heparin-induced thrombocytopenia is relatively
common and often consequential.4 At least 10 to 20% of affected patients die or have permanent sequelae such as stroke or limb amputation; this distinguishes heparin-induced thrombocytopenia from most other adverse drug reactions.5 From November 1, 2007, to February 28, 2008 (the pe-riod during which anaphylactoid reactions to OSCS-contaminated heparin were observed1), our two laboratories in Canada and Germany con-firmed the diagnosis of heparin-induced throm-bocytopenia in 115 patients. During this period, a substantial increase in laboratory-confirmed heparin-induced thrombocytopenia was observed in Germany, but not in Canada, possibly reflect-
The New England Journal of Medicine Downloaded from nejm.org on May 2, 2011. For personal use only. No other uses without permission.
Copyright © 2008 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 359;12 www.nejm.org september 18, 20081292
ing differences in the distribution of OSCS-con-taminated heparin (Table 1).
OSCS contamination may increase the risk of heparin-induced thrombocytopenia. If so, the re-sulting adverse outcomes associated with heparin-induced thrombocytopenia could well outnumber those attributable to activation of the contact sys-tem. Active surveillance for cases of heparin-induced thrombocytopenia could be a means of monitoring heparin for changes in composition.Andreas Greinacher, M.D.Ernst Moritz Arndt University Greifswald D-17487 Greifswald, Germany
Theodore E. Warkentin, M.D.McMaster University Hamilton, ON L8N 3Z5, Canada [email protected]
Dr. Greinacher reports receiving research support from No-vartis Germany, consulting fees from Organon International (part of Schering-Plough), and lecture fees from Organon Inter-national, Mitsubishi Pharma, and Novartis; and Dr. Warkentin, receiving research support from GlaxoSmithKline, consulting fees from Organon International and Genetics Testing Institute, and lecture fees from GlaxoSmithKline, Organon International, and Sanofi-Aventis. No other potential conflict of interest rele-vant to this letter was reported.
Kishimoto TK, Viswanathan K, Ganguly T, et al. Contami-1. nated heparin associated with adverse clinical events and activa-tion of the contact system. N Engl J Med 2008;358:2457-67.
Greinacher A, Michels I, Schäfer M, Kiefel V, Mueller-Eck-2. hardt C. Heparin-associated thrombocytopenia in a patient treat-ed with polysulphated chondroitin sulphate: evidence for immu-nological crossreactivity between heparin and polysulphated glycosaminoglycan. Br J Haematol 1992;81:252-4.
Greinacher A, Alban S, Dummel V, Franz G, Mueller-Eck-3. hardt C. Characterization of the structural requirements for a carbohydrate based anticoagulant with a reduced risk of induc-ing the immunologic type of heparin-associated thrombocy-topenia. Thromb Haemost 1995;74:886-92.
Warkentin TE. Drug-induced immune-mediated thrombocy-4. topenia — from purpura to thrombosis. N Engl J Med 2007;356: 891-3.
Warkentin TE, Greinacher A, eds. Heparin-induced throm-5. bocytopenia. 4th ed. New York: Informa Healthcare USA, 2007.
To the Editor: On the basis of their in vivo swine model, Kishimoto et al. conclude that ad-verse events linked to contaminated heparin are the result of OSCS-induced activation of the ki-nin–kallikrein system. Given the long-recognized differences in bioavailability between heparin ad-ministered intravenously and heparin administered subcutaneously,1 we used a rat model of OSCS ex-posure to evaluate the effect of the dose and route of administration of heparin on the physiological effects of OSCS.
Our in vitro data suggest that OSCS induces kallikrein activity in both rat and human plasma
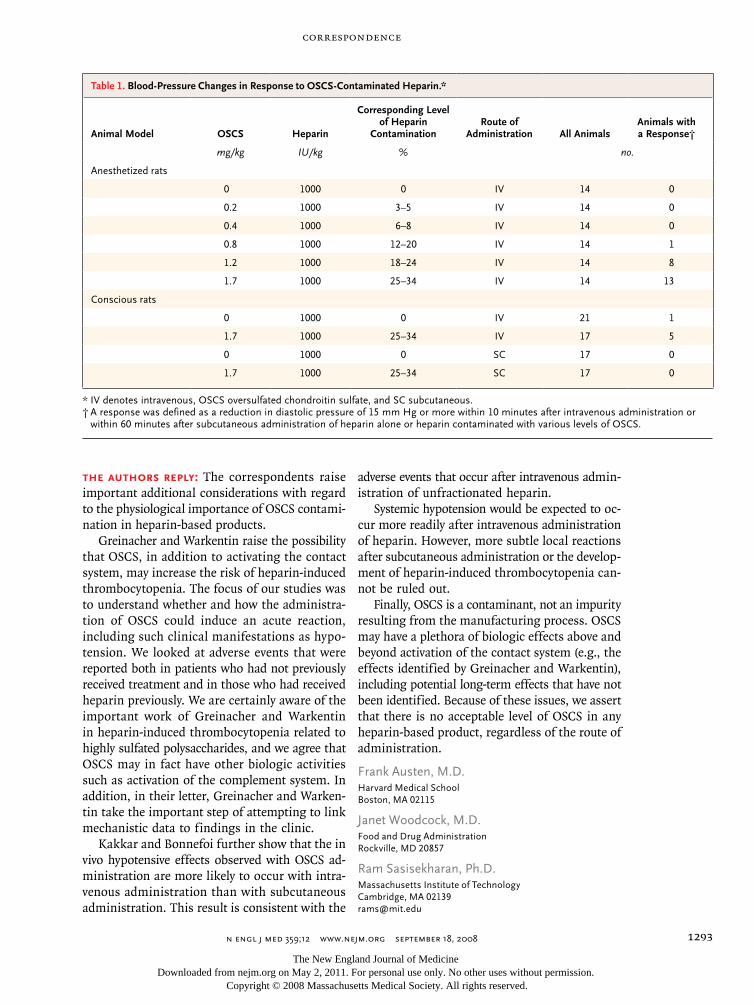
at concentrations of 25 μg per milliliter or more. In anesthetized rats, we observed a 15 mm Hg or greater reduction in diastolic blood pressure with-in 10 minutes after the intravenous administra-tion of synthetic OSCS at a dose of 0.8, 1.2, or 1.7 mg per kilogram of body weight (Table 1). The number of animals that had a response increased in a dose-dependent manner from 1 of 14 animals that received 0.8 mg of OSCS per kilogram (cor-responding to 12 to 20% heparin contamination) to 13 of 14 animals that received 1.7 mg of OSCS per kilogram (corresponding to 25 to 34% hepa-rin contamination).
We also developed a conscious-rat model in order to assess the effect of the route of adminis-tration on the frequency of the hypotensive re-sponse (a reduction in diastolic pressure that was ≥15 mm Hg within 10 minutes after intravenous administration or within 60 minutes after sub-cutaneous administration). Intravenous admin-istration of heparin containing 25 to 34% OSCS induced a hypotensive response in 5 of 17 animals tested (heparin plus OSCS vs. heparin alone, P = 0.07) (Table 1). The mean reduction in diastolic pressure in animals that had a response was 22.8 mm Hg (range, 17 to 28). Significantly more animals had this response after intravenous ad-ministration of heparin containing 25 to 34% OSCS than after subcutaneous administration of the same dose (five animals that received intrave-nous heparin plus OSCS vs. no animals that re-ceived subcutaneous heparin plus OSCS, P = 0.04 by a two-sided Fisher’s exact test) (Table 1).
These data suggest that the adverse events as-sociated with OSCS-contaminated heparin are de-pendent on the dose and route of administration. Further evaluation of the implications of these findings and those of Kishimoto et al. are war-ranted in view of the important role of heparin in the care of many patient populations.
Ajay K. Kakkar, M.B., B.S., Ph.D.Barts and the London School of Medicine and Dentistry London EC1 2AT, United Kingdom
Marc Bonnefoi, Ph.D.Sanofi-Aventis Bridgewater, NJ 08807
Dr. Kakkar reports receiving consulting fees, research sup-port, and honoraria from Sanofi-Aventis; and Dr. Bonnefoi, be-ing an employee of Sanofi-Aventis. No other potential conflict of interest relevant to this letter was reported.
Jaques LB. “Low-dose heparin” — significance of subcuta-1. neous injection. Thromb Res 1976;9:205-8.
The New England Journal of Medicine Downloaded from nejm.org on May 2, 2011. For personal use only. No other uses without permission.
Copyright © 2008 Massachusetts Medical Society. All rights reserved.
correspondence
n engl j med 359;12 www.nejm.org september 18, 2008 1293
The authors reply: The correspondents raise important additional considerations with regard to the physiological importance of OSCS contami-nation in heparin-based products.
Greinacher and Warkentin raise the possibility that OSCS, in addition to activating the contact system, may increase the risk of heparin-induced thrombocytopenia. The focus of our studies was to understand whether and how the administra-tion of OSCS could induce an acute reaction, including such clinical manifestations as hypo-tension. We looked at adverse events that were reported both in patients who had not previously received treatment and in those who had received heparin previously. We are certainly aware of the important work of Greinacher and Warkentin in heparin-induced thrombocytopenia related to highly sulfated polysaccharides, and we agree that OSCS may in fact have other biologic activities such as activation of the complement system. In addition, in their letter, Greinacher and Warken-tin take the important step of attempting to link mechanistic data to findings in the clinic.
Kakkar and Bonnefoi further show that the in vivo hypotensive effects observed with OSCS ad-ministration are more likely to occur with intra-venous administration than with subcutaneous administration. This result is consistent with the
adverse events that occur after intravenous admin-istration of unfractionated heparin.
Systemic hypotension would be expected to oc-cur more readily after intravenous administration of heparin. However, more subtle local reactions after subcutaneous administration or the develop-ment of heparin-induced thrombocytopenia can-not be ruled out.
Finally, OSCS is a contaminant, not an impurity resulting from the manufacturing process. OSCS may have a plethora of biologic effects above and beyond activation of the contact system (e.g., the effects identified by Greinacher and Warkentin), including potential long-term effects that have not been identified. Because of these issues, we assert that there is no acceptable level of OSCS in any heparin-based product, regardless of the route of administration.
Frank Austen, M.D.Harvard Medical School Boston, MA 02115
Janet Woodcock, M.D.Food and Drug Administration Rockville, MD 20857
Ram Sasisekharan, Ph.D.Massachusetts Institute of Technology Cambridge, MA 02139 [email protected]
Table 1. Blood-Pressure Changes in Response to OSCS-Contaminated Heparin.*
Animal Model OSCS Heparin
Corresponding Level of Heparin
Contamination Route of
Administration All AnimalsAnimals with a Response†
mg/kg IU/kg % no.
Anesthetized rats
0 1000 0 IV 14 0
0.2 1000 3–5 IV 14 0
0.4 1000 6–8 IV 14 0
0.8 1000 12–20 IV 14 1
1.2 1000 18–24 IV 14 8
1.7 1000 25–34 IV 14 13
Conscious rats
0 1000 0 IV 21 1
1.7 1000 25–34 IV 17 5
0 1000 0 SC 17 0
1.7 1000 25–34 SC 17 0
* IV denotes intravenous, OSCS oversulfated chondroitin sulfate, and SC subcutaneous.† A response was defined as a reduction in diastolic pressure of 15 mm Hg or more within 10 minutes after intravenous administration or
within 60 minutes after subcutaneous administration of heparin alone or heparin contaminated with various levels of OSCS.
The New England Journal of Medicine Downloaded from nejm.org on May 2, 2011. For personal use only. No other uses without permission.
Copyright © 2008 Massachusetts Medical Society. All rights reserved.


















