NDA 21-576
53
1 Dermatologic and Ophthalmic Drugs Advisory Dermatologic and Ophthalmic Drugs Advisory Committee Committee September 10, 2003 September 10, 2003 NDA 21-576 NDA 21-576 Methyl aminolevulinate Cream (MAL) with Curettage and Photodynamic Therapy (PDT) for Basal Cell Carcinoma (BCC)
description
NDA 21-576. Methyl aminolevulinate Cream (MAL) with Curettage and Photodynamic Therapy (PDT) for Basal Cell Carcinoma (BCC). FDA Clinical and Statistical Reviewers. Brenda Vaughan, M.D., Medical Officer Markham C. Luke, M.D., Ph.D., Dermatology Team Leader - PowerPoint PPT Presentation
Transcript of NDA 21-576

1Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
NDA 21-576NDA 21-576
Methyl aminolevulinate Cream (MAL) with Curettage and
Photodynamic Therapy (PDT) for Basal Cell Carcinoma (BCC)

2Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
FDA Clinical and Statistical FDA Clinical and Statistical ReviewersReviewers
FDA Clinical and Statistical FDA Clinical and Statistical ReviewersReviewers
Brenda Vaughan, M.D., Medical Officer
Markham C. Luke, M.D., Ph.D., Dermatology Team Leader
Shiowjen Lee, Ph.D., Mathematical StatisticianMohamed Alosh, Ph.D., Mathematical Statistics Team
Leader

3Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Treatment of Primary Nodular Treatment of Primary Nodular BCCBCC
Treatment of Primary Nodular Treatment of Primary Nodular BCCBCC
• Curette-MAL-PDT consists of:
– Lesion preparation (Curettage)– Methyl Aminolevulinate (MAL) Cream– Combined with Curelight Lamp (Drug/Device
Combination)
• Curette-MAL-PDT consists of:
– Lesion preparation (Curettage)– Methyl Aminolevulinate (MAL) Cream– Combined with Curelight Lamp (Drug/Device
Combination)

4Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
BackgroundBackgroundBackgroundBackground
• “Provided that efficacy and safety are established for nodular BCC: one independent, multi-center, randomized, active controlled study conducted in patients with primary superficial BCC might be acceptable if supported by strong evidence from a solid database.” Regulatory Guidance Meeting with PhotoCure - March 7, 2000
• “Provided that efficacy and safety are established for nodular BCC: one independent, multi-center, randomized, active controlled study conducted in patients with primary superficial BCC might be acceptable if supported by strong evidence from a solid database.” Regulatory Guidance Meeting with PhotoCure - March 7, 2000

5Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Items for DiscussionItems for DiscussionItems for DiscussionItems for Discussion
•Efficacy– Adequacy of studies for estimating cure rate?
• Early histology and small numbers in pivotal studies• Minimal recurrence data for nodular BCC
– Adequacy of instructions for lesion preparation?• Apparent high VEH-PDT response rate• Center-to-center variability
– Estimate of cure rate for MAL-PDT vs. Surgery?•Safety
– Pain and minimal information regarding anesthesia/pain control
– Contact hypersensitization
•Efficacy– Adequacy of studies for estimating cure rate?
• Early histology and small numbers in pivotal studies• Minimal recurrence data for nodular BCC
– Adequacy of instructions for lesion preparation?• Apparent high VEH-PDT response rate• Center-to-center variability
– Estimate of cure rate for MAL-PDT vs. Surgery?•Safety
– Pain and minimal information regarding anesthesia/pain control
– Contact hypersensitization

6Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Measurements of Efficacy for Treatment of Measurements of Efficacy for Treatment of Basal Cell CarcinomaBasal Cell Carcinoma
Measurements of Efficacy for Treatment of Measurements of Efficacy for Treatment of Basal Cell CarcinomaBasal Cell Carcinoma
• Agency Proposed:– Clinical Observation and Excision Histology– 5 year Recurrence Data (2 year data acceptable
for filing)• What was submitted:
– Excision Histology Alone– Clinical Observation Alone– Recurrence Rates Based on Clinical
Observation
• Agency Proposed:– Clinical Observation and Excision Histology– 5 year Recurrence Data (2 year data acceptable
for filing)• What was submitted:
– Excision Histology Alone– Clinical Observation Alone– Recurrence Rates Based on Clinical
Observation

7Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Clinical StudiesClinical StudiesClinical StudiesClinical Studies
• Studies interpreted for efficacy for nodular BCC– 2 vehicle controlled randomized studies (307 &
308)– 1 open-label randomized MAL-PDT vs.
surgery for recurrence rates (303)– 1 open-label non-randomized MAL-PDT study
for recurrence rates (205) – also had superficial BCC
• Studies interpreted for efficacy for nodular BCC– 2 vehicle controlled randomized studies (307 &
308)– 1 open-label randomized MAL-PDT vs.
surgery for recurrence rates (303)– 1 open-label non-randomized MAL-PDT study
for recurrence rates (205) – also had superficial BCC

8Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Pivotal StudiesPivotal StudiesPivotal StudiesPivotal Studies
• Study 307 - U.S. Study– 33 patients randomized to Curette-MAL-PDT– 32 patients randomized to Curette-VEH-PDT
• Study 308 - Australian Study– 33 patients randomized to Curette-MAL-PDT– 33 patients randomized to Curette-VEH-PDT
• Study 307 - U.S. Study– 33 patients randomized to Curette-MAL-PDT– 32 patients randomized to Curette-VEH-PDT
• Study 308 - Australian Study– 33 patients randomized to Curette-MAL-PDT– 33 patients randomized to Curette-VEH-PDT

9Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Pivotal Studies: Study DesignPivotal Studies: Study DesignPivotal Studies: Study DesignPivotal Studies: Study Design
• First Treatment Cycle - two Curette-(MAL vs. VEH)-PDT treatments 7 days apart followed by clinical assessment at 3 months
• Second Treatment Cycle - if only partial response to First Treatment Cycle - two additional treatments 7 days apart
• First Treatment Cycle - two Curette-(MAL vs. VEH)-PDT treatments 7 days apart followed by clinical assessment at 3 months
• Second Treatment Cycle - if only partial response to First Treatment Cycle - two additional treatments 7 days apart

10Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Pivotal Studies: Study DesignPivotal Studies: Study DesignPivotal Studies: Study DesignPivotal Studies: Study DesignClinical evaluation at 3-months to determine further
management:• Complete response (disappearance of lesions) >>
excision at 6-month for histology.• Partial response (lesion decreased by 50%) >> 2nd
PDT cycle >> excision at 9-month for histology.• No response (lesion decreased by 50%) or
Progression (lesion increased by 20%) >> excision at 3-month.
Complete response is not equal to “cure”.
Clinical evaluation at 3-months to determine further management:
• Complete response (disappearance of lesions) >> excision at 6-month for histology.
• Partial response (lesion decreased by 50%) >> 2nd PDT cycle >> excision at 9-month for histology.
• No response (lesion decreased by 50%) or Progression (lesion increased by 20%) >> excision at 3-month.
Complete response is not equal to “cure”.

11Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
No ClinicalResponse Excise
1st Tx Cycle
3 MONTHS
CompleteClinicalResponse
Excise3 MONTHSLATER
IncompleteClinicalResponse
Excise
7 DAYSAPART
PartialClinicalResponse
2nd Tx Cycle
7 DAYSAPART
3 MONTHS
CompleteClinicalResponse
Excise3 MONTHSLATER
STUDIES307 and 308
RANDOMIZATION
MAL or VEH PDT

12Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Biostatistical Analysis of Pivotal StudiesBiostatistical Analysis of Pivotal Studies

Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Efficacy Evaluation in Pivotal Efficacy Evaluation in Pivotal StudiesStudies
Efficacy Evaluation in Pivotal Efficacy Evaluation in Pivotal StudiesStudies
Primary: Patient complete response rateSecondary: Lesion complete response rate
Criterion for assessing response: a. Clinical and histology - Agency recommendation to PhotoCure on March 7, 2000 b. Histology only – PhotoCure’s protocol (August, 2000)
Complete response is not equal to “cure”.
Primary: Patient complete response rateSecondary: Lesion complete response rate
Criterion for assessing response: a. Clinical and histology - Agency recommendation to PhotoCure on March 7, 2000 b. Histology only – PhotoCure’s protocol (August, 2000)
Complete response is not equal to “cure”.

14Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Overview of Efficacy Findings in Overview of Efficacy Findings in Pivotal Studies Pivotal Studies
Overview of Efficacy Findings in Overview of Efficacy Findings in Pivotal Studies Pivotal Studies
• Curette MAL-PDT is superior to Curette VEH-PDT
• Variability in the success rate estimate for MAL-PDT which might be attributed to:
a) Relatively small studies wide C.I. around these estimates
b) Uncertainty about lesion preparation description
• Curette MAL-PDT is superior to Curette VEH-PDT
• Variability in the success rate estimate for MAL-PDT which might be attributed to:
a) Relatively small studies wide C.I. around these estimates
b) Uncertainty about lesion preparation description

15Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Overview of Efficacy Findings in Overview of Efficacy Findings in Pivotal Studies Pivotal Studies
Overview of Efficacy Findings in Overview of Efficacy Findings in Pivotal Studies Pivotal Studies
Clues:
• High vehicle response rate• Center-to-center variability:
Small studies with few patients per center
Clues:
• High vehicle response rate• Center-to-center variability:
Small studies with few patients per center

16Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Apparent High Vehicle Response Rate Based Apparent High Vehicle Response Rate Based on Histological Evaluationon Histological Evaluation
Apparent High Vehicle Response Rate Based Apparent High Vehicle Response Rate Based on Histological Evaluationon Histological Evaluation
Table 1: Lesions and Patients with Complete Response (Histology– PhotoCure Analysis)Lesion response Patient responseAnalyses
Curette-MAL-PDT
Curette-VEH-PDT
Curette-MAL-PDT
Curette-VEH-PDT
Study 307 ITT, n/N (%) PP, n/N (%)
32/41 (78%)31/39 (79%)
13/39 (33%)13/37 (35%)
25/33 (76%)24/31 (77%)
11/32 (34%)11/32 (34%)
Study 308 ITT, n/N (%) PP, n/N (%)
23/34 (68%)22/30 (73%)
7/36 (19%)7/33 (21%)
22/33 (67%)21/29 (72%)
6/33 (18%)6/32 (19%)

17Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Summary of Response rates along with 95% Summary of Response rates along with 95% Confidence Intervals Confidence Intervals
Summary of Response rates along with 95% Summary of Response rates along with 95% Confidence Intervals Confidence Intervals
Table 2: Patient and Lesion Complete Response Based on Clinical and Histological Evaluations, ITT 1
Patient Response Lesion Response
Study # Curette MAL-PDT Curette VEH-PDT Curette MAL-PDT Curette VEH-PDT
Study 307 n/N ( % ) (95% C.I.)
24/33 (73%) (54%, 87%)
8/32 (25%) (11%, 43%)
28/41 (68%) (52%, 82%)
10/39 (26%) (13%, 42%)
Study 308 n/N ( % ) (95% C.I.)
21/33 (64%)(45%, 80%)
5/33 (15%) (5%, 32%)
22/34 (65%)(46%, 80%)
6/36 (17%)(6%, 33%)
1 Agency Analysis

18Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Estimates of Response for 1Estimates of Response for 1stst Treatment Treatment CycleCycle
Estimates of Response for 1Estimates of Response for 1stst Treatment Treatment CycleCycle
Table 5: PhotoCure and Agency Response Rates for 1 st Treatment Cycle ( Pivotal Studies, ITT )Histological Evaluation Clinical and Histological
EvaluationsStudy/ Analyses
Cur. MAL PDTn/N (%)
Cur. VEH PDTn/N (%)
Cur. MAL PDTn/N (%)
Cur. VEH PDTn/N (%)
Study 307PhotoCure’s Analysis 1
Agency Analysis23/28 (82%)23/41 (56%)
9/30 (30%)9/39 (23%) 19/41 (46%) 7/39 (18%)
Study 308 PhotoCure’s Analysis 1
Agency Analysis18/29 (62%)18/34 (53%)
5/32 (16%)5/36 (14%) 17/34 (50%) 4/36 (11%)
1 Photocure’s Briefing Document for FDA Advisory Committee Meeting, dated 6 August 2003, Table 41, p.94
PhotoCure excluded from the denominator those lesions which had partial response and were treated with a 2nd treatment cycle in post-hoc analysis.
rate is inflated because not all lesions treated with 1st PDT cycle are included in the denominator, as shown in the following table
PhotoCure excluded from the denominator those lesions which had partial response and were treated with a 2nd treatment cycle in post-hoc analysis.
rate is inflated because not all lesions treated with 1st PDT cycle are included in the denominator, as shown in the following table

19Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Treatment Cycle ResponseTreatment Cycle ResponseTreatment Cycle ResponseTreatment Cycle Response
• Study design precludes estimating response rates for only one treatment cycle:– Second treatment cycle is based on
clinical decision regarding first treatment cycle outcome, i.e. “partial response”
– Outcome measure was done at 3 months– No randomization before second cycle
• Study design precludes estimating response rates for only one treatment cycle:– Second treatment cycle is based on
clinical decision regarding first treatment cycle outcome, i.e. “partial response”
– Outcome measure was done at 3 months– No randomization before second cycle

20Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Study 307: Lesion Response Inter-Study 307: Lesion Response Inter-Center VariabilityCenter Variability
Study 307: Lesion Response Inter-Study 307: Lesion Response Inter-Center VariabilityCenter Variability
Table 3: Lesion Response Rate by Center for 1 st treatment cycle and overall , Study 307 1 st PDT Cycle
Clinical & Histological 1 st & 2 nd Cycles
Clinical & Histological 1 st & 2 nd Cycles
HistologicalCenter Cur-MAL-
PDTCur-VEH-PDT
Cur-MAL-PDT
Cur-VEH-PDT
Cur-MAL-PDT
Cur-VEH-PDT
30702 2/7 1/8 4/7 2/8 4/7 2/830703 2/4 0/2 4/4 0/2 4/4 0/230704 0/7 1/7 3/7 1/7 4/7 2/730705 1/2 1/3 2/2 1/3 2/2 2/330706 6/13 4/10 7/13 4/10 10/13 4/1030707 5/5 0/5 5/5 0/5 5/5 0/530709 3/3 0/4 3/3 2/4 3/3 3/4
Total 19/41(46%)
7/39(18%)
28/41(68%)
10/39(26%)
32/41(78%)
13/39(33%)
B-D Test 1 0.025 * 0.134 0.3181 Breslow-Day test for homogeneity of responses across centers as directed sensitivity analysis.* p-value for Zelen’s exact test = 0.072

21Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Study 308: Lesion Response Inter-Study 308: Lesion Response Inter-Center VariabilityCenter Variability
Study 308: Lesion Response Inter-Study 308: Lesion Response Inter-Center VariabilityCenter Variability
Table 4: Lesion Complete Response Rate after the 1st PDT Cycle and Overall by Center, Study 308
1 st PDT CycleClinical & Histological
1 st & 2 nd PDT CyclesClinical & Histological
1 st & 2 nd CyclesHistological
Center Cur-MAL-PDT
Cur-VEH-PDT
Cur-MAL-PDT
Cur-VEH-PDT
Cur-MAL-PDT
Cur-VEH-PDT
30801 1/2 0/3 1 /2 1/3 1/2 1/330802 8/13 3/12 9/13 3/12 9/13 4/12
30803 0/0 0/1 0/0 0/1 0/0 0/130804 2/2 0/3 2/2 0/3 2/2 0/330805 3/4 1/5 3/4 1/5 3 /4 1/530806 3/8 0/7 3/8 0/7 4/8 0/730807 0/5 0/5 3/5 1/5 4/5 1/5
Total 17/34(50%)
4/36(11%)
21/34(62%)
6/36(17%)
23/34(68%)
7/36(19%)
B-D test1 0.56 0.703 0.5681 Breslow-Day (B-D) test for homogeneity of responses across centers.

22Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Pivotal Studies: Pivotal Studies: Summary of Statistical AnalysisSummary of Statistical Analysis
Pivotal Studies: Pivotal Studies: Summary of Statistical AnalysisSummary of Statistical Analysis
• Curette-MAL-PDT is statistically superior to Curette-VEH-PDT for the treatment method used in the protocol of nodular BCC.
• For each pivotal study there is relatively high Curette-VEH-PDT response rate. There is also center-to-center variability in Study 307. This might be attributable to:– Small study size– Lesion preparation for treatment– Accuracy of clinical and histological evaluations
• The center-to-center variability in the efficacy results reduces the reliability in the overall point estimates of Curette-MAL-PDT.
• Curette-MAL-PDT is statistically superior to Curette-VEH-PDT for the treatment method used in the protocol of nodular BCC.
• For each pivotal study there is relatively high Curette-VEH-PDT response rate. There is also center-to-center variability in Study 307. This might be attributable to:– Small study size– Lesion preparation for treatment– Accuracy of clinical and histological evaluations
• The center-to-center variability in the efficacy results reduces the reliability in the overall point estimates of Curette-MAL-PDT.

23Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Efficacy Conclusions from Pivotal StudiesEfficacy Conclusions from Pivotal StudiesEfficacy Conclusions from Pivotal StudiesEfficacy Conclusions from Pivotal Studies
• Curette-MAL-PDT is statistically superior to Curette-VEH-PDT using the protocol guided outcome assessment
• High response rates with Curette-VEH-PDT– Effect of curette– Short follow-up– Low ability to detect residual nodular
BCC by histological methods used
• Curette-MAL-PDT is statistically superior to Curette-VEH-PDT using the protocol guided outcome assessment
• High response rates with Curette-VEH-PDT– Effect of curette– Short follow-up– Low ability to detect residual nodular
BCC by histological methods used

24Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
PhotoCure Video – Lesion Preparation

25Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Effect of CurettageEffect of CurettageEffect of CurettageEffect of Curettage
• Response may depend on extent and depth of curettage– Efficacy shows center dependence– High Curette-VEH-PDT response
• Other factors– Lamp exposure appears to have been
applied in a consistent manner for each pivotal study
• Response may depend on extent and depth of curettage– Efficacy shows center dependence– High Curette-VEH-PDT response
• Other factors– Lamp exposure appears to have been
applied in a consistent manner for each pivotal study

26Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
CurettageCurettageCurettageCurettage
Page 124 of PhotoCure AC Briefing, Figure 20

27Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Recurrence Data: RegulatoryRecurrence Data: RegulatoryRecurrence Data: RegulatoryRecurrence Data: Regulatory• Agency and PhotoCure discussed in the context of
nodular BCC recurrence data, that a minimum of 250 subjects were to be submitted. Pre-NDA meeting minutes with PhotoCure - June 20, 2002
• A two-year follow-up was recommended for NDA submission. Regulatory Guidance Meeting with PhotoCure - March 2000
• It was recommended that patients be followed up to five years post treatment. Regulatory Guidance Meeting with PhotoCure - March 2000
• Agency and PhotoCure discussed in the context of nodular BCC recurrence data, that a minimum of 250 subjects were to be submitted. Pre-NDA meeting minutes with PhotoCure - June 20, 2002
• A two-year follow-up was recommended for NDA submission. Regulatory Guidance Meeting with PhotoCure - March 2000
• It was recommended that patients be followed up to five years post treatment. Regulatory Guidance Meeting with PhotoCure - March 2000

28Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Recurrence Rate DatabaseRecurrence Rate DatabaseRecurrence Rate DatabaseRecurrence Rate Database
• PhotoCure provided 2 year recurrence data for 46 patients (47 lesions) with nodular BCC treated with Curette-MAL-PDT (clinical observation for recurrence): Study 303/99 (Phase 3, randomized open-label).
• Additional data for 30 patients with nodular BCC: Study 205/98 - Phase 2, non-randomized open-label, included both nodular (38 lesions) and superficial (39 lesions) BCC. Focus would be primarily on nodular.
• PhotoCure provided 2 year recurrence data for 46 patients (47 lesions) with nodular BCC treated with Curette-MAL-PDT (clinical observation for recurrence): Study 303/99 (Phase 3, randomized open-label).
• Additional data for 30 patients with nodular BCC: Study 205/98 - Phase 2, non-randomized open-label, included both nodular (38 lesions) and superficial (39 lesions) BCC. Focus would be primarily on nodular.

29Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Assessment of RecurrenceAssessment of RecurrenceAssessment of RecurrenceAssessment of Recurrence
• “Recurrence of lesions is based on clinical assessment (inspection and palpation) confirmed by punch biopsy [when positive clinically].”
• Treated areas that were apparently clinically clear were not biopsied and followed.
• “Recurrence of lesions is based on clinical assessment (inspection and palpation) confirmed by punch biopsy [when positive clinically].”
• Treated areas that were apparently clinically clear were not biopsied and followed.

30Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Study 303Study 303Study 303Study 303
• European randomized, open-label, multicenter study in 101 subjects
• Curette-MAL-PDT (n=52) • Surgical Excision (n=49)• Initial post-treatment assessment at 3
months • Followed by 12 and 24 month clinical
assessments for recurrence
• European randomized, open-label, multicenter study in 101 subjects
• Curette-MAL-PDT (n=52) • Surgical Excision (n=49)• Initial post-treatment assessment at 3
months • Followed by 12 and 24 month clinical
assessments for recurrence

31Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Example of Complete Response?Example of Complete Response?Example of Complete Response?Example of Complete Response?
Page 100 of PhotoCure AC Briefing, Figure 19

32Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Lesion Recurrence Data: Study 303Lesion Recurrence Data: Study 303Lesion Recurrence Data: Study 303Lesion Recurrence Data: Study 303
ARM
Analysis
6 month
12 month
24 month (95% CI)
MAL-PDT
Recurrent Lesions/Lesions with “Complete Response” at 3 or 6 months
1/47 (2%)
3/47 (6%)
4/47 (9%)
(2%, 20%)
to 16/47 (34%)*
(21%, 49%)
Surgery
Recurrent Lesions/Lesions with “Complete Response”
0/51
0/51 to
1/51 (2%)**
1/51 (2%)
(0%, 11%)
to 8/51 (16%)***
(7%, 29%)
* 12 additional lesions missing at 24 months from MAL-PDT arm. ** One lesion missing at 12 months from Surgery arm. *** 7 additional lesions missing at 24 months from Surgery arm

33Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Failure to Cure Analysis: Study 303Failure to Cure Analysis: Study 303Failure to Cure Analysis: Study 303Failure to Cure Analysis: Study 303
ARM
Analysis
6 month
12 month
24 month (95% CI)
MAL-PDT
Failure to Cure*/Total MITT Lesions
9/56 (16%)
12/56 (21%)
25/56 (45%)**
(31%, 59%)
Surgery
Failure to Cure/Total MITT Lesions
0/51
1/51 (2%)
8/51 (16%) (7%, 29%)
* Failure to Cure = Treatment Failures + Recurrences + Missing ** 12 additional lesions missing at 24 months from MAL-PDT arm.

34Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Phase 2 Recurrence StudyPhase 2 Recurrence StudyPhase 2 Recurrence StudyPhase 2 Recurrence Study
• Study 205 – Non-randomized, open-label study with both nodular and superficial BCC
• 57 patients (79 lesions) were evaluated for recurrence at 24 months
• 30 patients with 38 nodular BCC lesions*• 6, 12, and 24 month data available
• * 3 patients with 1 superficial/nodular lesion each were in the study
• Study 205 – Non-randomized, open-label study with both nodular and superficial BCC
• 57 patients (79 lesions) were evaluated for recurrence at 24 months
• 30 patients with 38 nodular BCC lesions*• 6, 12, and 24 month data available
• * 3 patients with 1 superficial/nodular lesion each were in the study

35Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Factors Affecting Applicability of Factors Affecting Applicability of Recurrence Data (Study 205)Recurrence Data (Study 205)
Factors Affecting Applicability of Factors Affecting Applicability of Recurrence Data (Study 205)Recurrence Data (Study 205)
• Different patient population (high risk)• Difference in written instructions for lesion
preparation (curetting below epidermis)• Difference in MAL application border• Different lamps used - Some patients had a
lamp other than that used in the pivotal studies
• Different patient population (high risk)• Difference in written instructions for lesion
preparation (curetting below epidermis)• Difference in MAL application border• Different lamps used - Some patients had a
lamp other than that used in the pivotal studies

36Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Recurrence: Study 205Recurrence: Study 205Recurrence: Study 205Recurrence: Study 205
BCC N*(Lesions) Missing
PhotoCureAnalysis
ofRecurrence
Agency Analysis ofRecurrence
-missing lesions added to numerator(95% CI)
Superficial 39 3 (8%) 8 (21%) 11/39 (28%)(15%, 45%)
Nodular 38 10 (28%) 4 (11%) 14/38 (37%)(22%, 54%)
Superficial &Nodular
3 0 0/2 1/3 (33%)(0%, 91%)
Total 80 13 (16%) 12 (15%) 26/80 (33%)(22%, 43%)
BCC N*(Lesions) Missing
PhotoCureAnalysis
ofRecurrence
Agency Analysis ofRecurrence
-missing lesions added to numerator(95% CI)
Superficial 39 3 (8%) 8 (21%) 11/39 (28%)(15%, 45%)
Nodular 38 10 (28%) 4 (11%) 14/38 (37%)(22%, 54%)
Superficial &Nodular
3 0 0/2 1/3 (33%)(0%, 91%)
Total 80 13 (16%) 12 (15%) 26/80 (33%)(22%, 43%)
Lesion recurrence (at 24 months)
*Early failures are not included

37Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Recurrence: ConclusionsRecurrence: ConclusionsRecurrence: ConclusionsRecurrence: Conclusions
• A database of 46 patients with 2 year recurrence data for primary nodular BCC was submitted by PhotoCure in Study 303.
• The 2 year recurrence rate for MAL-PDT treated patients ranged from 9% to 34% depending on how missing data were accounted for.
• Failure to treat adequately rate was 45% at 2 years.
• A larger database was requested.
• A database of 46 patients with 2 year recurrence data for primary nodular BCC was submitted by PhotoCure in Study 303.
• The 2 year recurrence rate for MAL-PDT treated patients ranged from 9% to 34% depending on how missing data were accounted for.
• Failure to treat adequately rate was 45% at 2 years.
• A larger database was requested.

38Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Cosmetic OutcomeCosmetic OutcomeCosmetic OutcomeCosmetic Outcome• In the pivotal studies, vehicle treated patients had as
good as or better cosmetic outcome than MAL treatment, but poorer response with regard to BCC treatment outcome.
• Cosmetic outcome is considered by Agency to be secondary to non-recurrence of the basal cell carcinoma skin cancer. Recurrence may ultimately result in a worse cosmetic outcome due to need for further treatment.
• The assessment of cosmetic outcomes across treatments were not pre-agreed upon between PhotoCure and FDA.
• In the pivotal studies, vehicle treated patients had as good as or better cosmetic outcome than MAL treatment, but poorer response with regard to BCC treatment outcome.
• Cosmetic outcome is considered by Agency to be secondary to non-recurrence of the basal cell carcinoma skin cancer. Recurrence may ultimately result in a worse cosmetic outcome due to need for further treatment.
• The assessment of cosmetic outcomes across treatments were not pre-agreed upon between PhotoCure and FDA.

39Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Cosmetic OutcomeCosmetic OutcomeCosmetic OutcomeCosmetic Outcome
• Data from the pivotal studies are presented (next slide)
• Limited numbers of patients in each study arm• Photographic basis for assessment was not
provided by PhotoCure to confirm the data• “Cosmetic assessments could be made prior to
surgical excision and supported by blinded independent [review] of photographs.” March, 2000 Regulatory Guidance Meeting Minutes.
• Data from the pivotal studies are presented (next slide)
• Limited numbers of patients in each study arm• Photographic basis for assessment was not
provided by PhotoCure to confirm the data• “Cosmetic assessments could be made prior to
surgical excision and supported by blinded independent [review] of photographs.” March, 2000 Regulatory Guidance Meeting Minutes.

Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Pivotal Studies: Cosmetic Pivotal Studies: Cosmetic OutcomeOutcome
Pivotal Studies: Cosmetic Pivotal Studies: Cosmetic OutcomeOutcome
Cosmetic Outcome for Lesions Having Histological Complete Response -- PhotoCure’s results
Cosmetic Outcome for Lesions Having Histological Complete Response -- PhotoCure’s results
Assessment Excellent Good Fair MissingStudy 307MAL-PDT(N=28)
InvestigatorPatient
17 (61%)18 (64%)
9 (32%)8 (29%)
2 (7%)2 (7%)
44
VEH-PDT(N=10)
InvestigatorPatient
6 (60%)8 (80%)
3 (30%)2 (20%)
1 (10%)0
33
Study 308MAL-PDT(N=22)
InvestigatorPatient
13 (59%)14 (64%)
8 (36%)8 (36%)
1 (5%)0
11
VEH-PDT(N=6)
InvestigatorPatient
2 (33%)5 (83%)
3 (50%)1 (17%)
1 (17%)0
11
Source: PhotoCure’s NDA submission (page 125, Volume 39; page 119, Volume 42).

41Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Safety: Risks IdentifiedSafety: Risks IdentifiedSafety: Risks IdentifiedSafety: Risks Identified
• Local• Pain, Burning & Stinging• Phototoxic Reactions• Contact Sensitization
• Local• Pain, Burning & Stinging• Phototoxic Reactions• Contact Sensitization

42Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Local Adverse Events Local Adverse Events Local Adverse Events Local Adverse Events
Number of Subjects in Pivotal Studies(%)
Curette-MAL-PDT(n=66)
Curette-VEH-PDT(n=65)
Pain skin 12 (18%) 3 (4.5%)
Burning skin 19 (29%) 8 (12%)
Stinging skin 10 (15%) 5 (8%)
Number of Subjects in Pivotal Studies(%)
Curette-MAL-PDT(n=66)
Curette-VEH-PDT(n=65)
Pain skin 12 (18%) 3 (4.5%)
Burning skin 19 (29%) 8 (12%)
Stinging skin 10 (15%) 5 (8%)

43Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Local AEs with MAL-PDTLocal AEs with MAL-PDTLocal AEs with MAL-PDTLocal AEs with MAL-PDTITT Population for Open Label Studies
N=196
Any (% of N)
Mild Moderate Severe
Pain skin 63 (32%) 30 22 11
Burning skin 72 (37%) 22 44 6
Stinging skin 54 (28%) 26 24 4
ITT Population for Open Label Studies N=196
Any (% of N)
Mild Moderate Severe
Pain skin 63 (32%) 30 22 11
Burning skin 72 (37%) 22 44 6
Stinging skin 54 (28%) 26 24 4

44Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Local AE: PhototoxicityLocal AE: PhototoxicityLocal AE: PhototoxicityLocal AE: Phototoxicity
• Patients treated with Curette-MAL-PDT could have skin ulceration, and blisters that last 1 to 2 weeks after treatment and in two cases erythema lasted more than a year.*
• No separate analysis for rates of such occurrence.
*PhotoCure summary of non-U.S. labeling and Summary of Safety
• Patients treated with Curette-MAL-PDT could have skin ulceration, and blisters that last 1 to 2 weeks after treatment and in two cases erythema lasted more than a year.*
• No separate analysis for rates of such occurrence.
*PhotoCure summary of non-U.S. labeling and Summary of Safety

45Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Summary of Local AEs with Summary of Local AEs with MAL-PDTMAL-PDT
Summary of Local AEs with Summary of Local AEs with MAL-PDTMAL-PDT
• Curette-MAL-PDT was associated with higher incidence rates of Pain, Burning, or Stinging than Curette-VEH-PDT.
• The use of local anesthesia with MAL-PDT treatment was not studied in a systematic fashion.
• Minimal instructions for use of anesthesia –“Tumor fragments from most lesions may be removed without damaging normal skin and without use of anaesthetics.”
• Curette-MAL-PDT was associated with higher incidence rates of Pain, Burning, or Stinging than Curette-VEH-PDT.
• The use of local anesthesia with MAL-PDT treatment was not studied in a systematic fashion.
• Minimal instructions for use of anesthesia –“Tumor fragments from most lesions may be removed without damaging normal skin and without use of anaesthetics.”

46Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
SensitizationSensitizationSensitizationSensitization
• Dermal Safety – Sensitization Studies• Subjects during clinical trials
– 2 patients with urticaria/hypersensitivity reaction
• Post-Marketing (Europe) – 2 patients with 1 positive rechallenge
• Dermal Safety – Sensitization Studies• Subjects during clinical trials
– 2 patients with urticaria/hypersensitivity reaction
• Post-Marketing (Europe) – 2 patients with 1 positive rechallenge

47Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Sensitization Study DesignSensitization Study Design Sensitization Study DesignSensitization Study Design
• Induction Phase – MAL and MAL-vehicle applied for 3 weeks
• 2 Week Rest Period• Challenge Phase
– 3 hour MAL/VEH application– 48 hour Aminolevulinate 0.1% in soft
paraffin (ALA) vehicle cross-sensitization challenge
• Induction Phase – MAL and MAL-vehicle applied for 3 weeks
• 2 Week Rest Period• Challenge Phase
– 3 hour MAL/VEH application– 48 hour Aminolevulinate 0.1% in soft
paraffin (ALA) vehicle cross-sensitization challenge

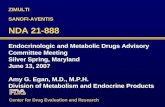
48Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
215 planned
156 Included
58 Drop-outs 98 Continued to Challenge
58 Challenged with MAL
40 Refused MAL
30 Positive
3 Equivocal
25 Negative
Dermal Safety: Sensitization Study
Enrollment stopped due to skin reactions
52% of the 58 Subjects Who Continued and Did
Not Refuse MALWere Sensitized to MAL
Cream

49Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
ALA 48 hour Cross ALA 48 hour Cross Sensitization/Challenge Sensitization/Challenge
Results (N=98)Results (N=98)
ALA 48 hour Cross ALA 48 hour Cross Sensitization/Challenge Sensitization/Challenge
Results (N=98)Results (N=98)
• None judged positive to 0.1% ALA
• 2% (2) were judged equivocal to ALA
• 2% (2) were judged positive to soft yellow paraffin vehicle for ALA
• None judged positive to 0.1% ALA
• 2% (2) were judged equivocal to ALA
• 2% (2) were judged positive to soft yellow paraffin vehicle for ALA

50Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
Safety Conclusions Safety Conclusions Safety Conclusions Safety Conclusions
• MAL has a high sensitization potential (at least 52% sensitization rate in a provocative study)
• Cross sensitization to ALA (an endogenous substance) cannot be ruled out
• Sensitization to MAL of healthcare providers and patients are of concern
• MAL has a high sensitization potential (at least 52% sensitization rate in a provocative study)
• Cross sensitization to ALA (an endogenous substance) cannot be ruled out
• Sensitization to MAL of healthcare providers and patients are of concern

51Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
NDA 21-576: Risk/BenefitNDA 21-576: Risk/BenefitNDA 21-576: Risk/BenefitNDA 21-576: Risk/Benefit•Efficacy
– Curette-MAL-PDT was shown to be statistically superior to Curette-VEH-PDT for the chosen outcome assessment in the pivotal studies.
– Adequacy of studies for estimating treatment effect?• Early histology and small numbers in pivotal studies• Minimal recurrence rate data for nodular BCC
– Adequacy of Instructions for Lesion Preparation?• Apparent high VEH-PDT response rate• Center-to-center variability
– Numerically higher recurrence rate with MAL-PDT vs. Surgery in one small open-label study - exact point estimate is uncertain
•Efficacy– Curette-MAL-PDT was shown to be statistically
superior to Curette-VEH-PDT for the chosen outcome assessment in the pivotal studies.
– Adequacy of studies for estimating treatment effect?• Early histology and small numbers in pivotal studies• Minimal recurrence rate data for nodular BCC
– Adequacy of Instructions for Lesion Preparation?• Apparent high VEH-PDT response rate• Center-to-center variability
– Numerically higher recurrence rate with MAL-PDT vs. Surgery in one small open-label study - exact point estimate is uncertain

52Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
NDA 21-576: Risk/Benefit NDA 21-576: Risk/Benefit (continued)(continued)
NDA 21-576: Risk/Benefit NDA 21-576: Risk/Benefit (continued)(continued)
• Safety– Pain and minimal information regarding
anesthesia/pain control– Contact hypersensitization
• Safety– Pain and minimal information regarding
anesthesia/pain control– Contact hypersensitization

53Dermatologic and Ophthalmic Drugs Advisory Committee Dermatologic and Ophthalmic Drugs Advisory Committee September 10, 2003September 10, 2003
PhotoCure Video