
Morphological Change on Skull Base by Achondroplasia Yoshitomo Nakai, Hajime Yokota, Kayu Takezawa,...
22
Morphological Change on Skull Base by Achondroplasia Yoshitomo Nakai, Hajime Yokota, Kayu Takezawa, Hisakazu Nakajima, Kitaro Kosaka, Kei Yamada Department of Radilogy, eEdE#: eEdE-13
-
Upload
marcia-griffith -
Category
Documents
-
view
213 -
download
0
Transcript of Morphological Change on Skull Base by Achondroplasia Yoshitomo Nakai, Hajime Yokota, Kayu Takezawa,...
Morphological Change
on Skull Base by
Achondroplasia
Yoshitomo Nakai, Hajime Yokota, Kayu Takezawa, Hisakazu Nakajima, Kitaro Kosaka, Kei Yamada
Department of Radilogy,Kyoto Prefectural University of Medicine
eEdE#: eEdE-134

Background
Achondroplasia(ACH) is a typical disease of dwarfism. FGFR3 gene mutation causes failure of endochondral ossification in ACH. The skull base development is interfered by the mutation, while the cranium is spared because it is composed with membranous ossification. Here, we show the morphologic changes on ACH associated with embryology of the skull.
Findings and procedure details
Anatomy and development of the skull
Terminology is complicated in embryology of the skull. Locations of the skull, type of ossification and mesenchymal origin are included in the terms to explain developmental course of the skull base. Be careful that each term doesn’t match to the other ones.
The first, on locations of the skull, the skull can be divided to the neurocranium and viscerocranium. The former covers and protects the brain and the latter composed the face.
The second, on type of ossification, the most parts of the cranium are made by membranous ossification. On membranous ossification, immature mesenchymal cells evolve into osteoblasts that create bone. On the other hand, the skull base is made by endochondral ossification. On endochondral ossification, immature mesenchymal cells evolve into chondroblasts and then chondrocytes that create cartilage template that turns into bone through the complex steps.
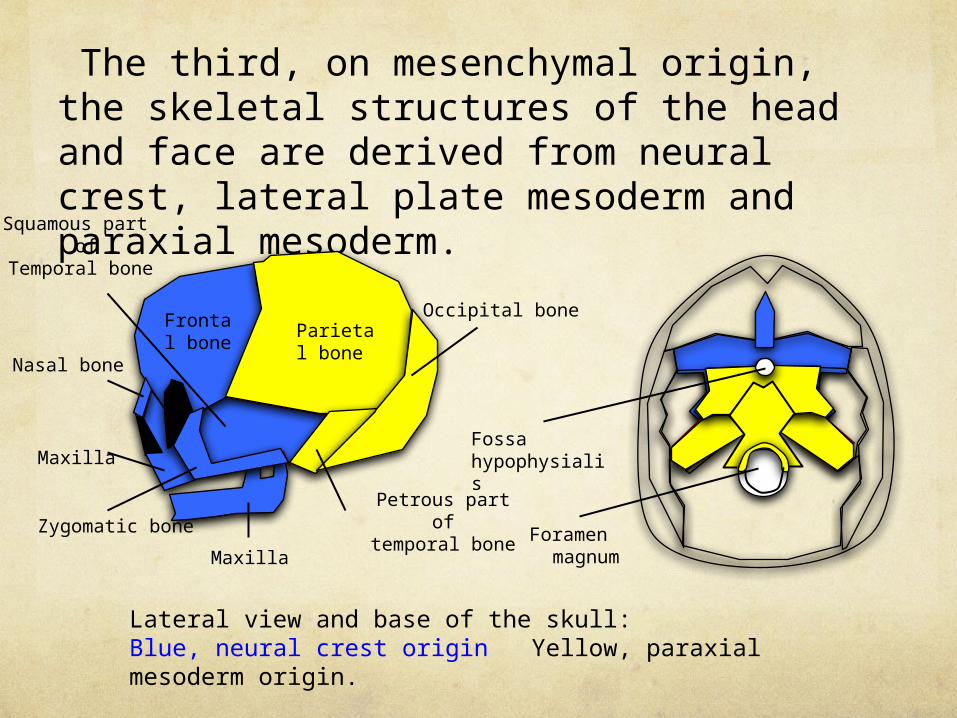
The third, on mesenchymal origin, the skeletal structures of the head and face are derived from neural crest, lateral plate mesoderm and paraxial mesoderm.
Lateral view and base of the skull: Blue, neural crest origin Yellow, paraxial mesoderm origin.
Maxilla
Occipital boneParietal bone
Frontal bone
Squamous part of
Temporal bone
Nasal bone
Maxilla
Zygomatic bonePetrous part
of temporal bone Foramen
magnum
Fossa hypophysialis

Purpose
To understand morphologic change on the skull base by ACH, the second is especially important.Here, we summarize these three classifications.
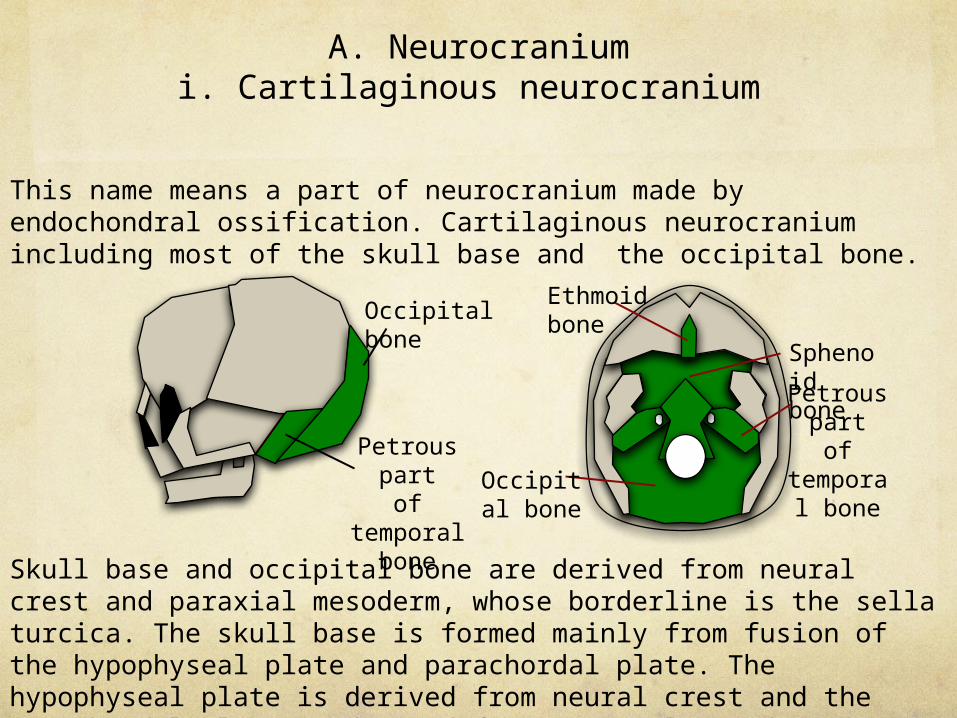
A. Neurocraniumi. Cartilaginous neurocranium
This name means a part of neurocranium made by endochondral ossification. Cartilaginous neurocranium including most of the skull base and the occipital bone.
Skull base and occipital bone are derived from neural crest and paraxial mesoderm, whose borderline is the sella turcica. The skull base is formed mainly from fusion of the hypophyseal plate and parachordal plate. The hypophyseal plate is derived from neural crest and the parachordal plate is derived from paraxial mesoderm. Ossification of the cartilaginous plate proceeds in order of the occipital, sphenoid and ethmoid bones.
Occipital bone
Petrous part of
temporal bone
Sphenoid bonePetrous
part of
temporal bone
Occipital bone
Ethmoid bone
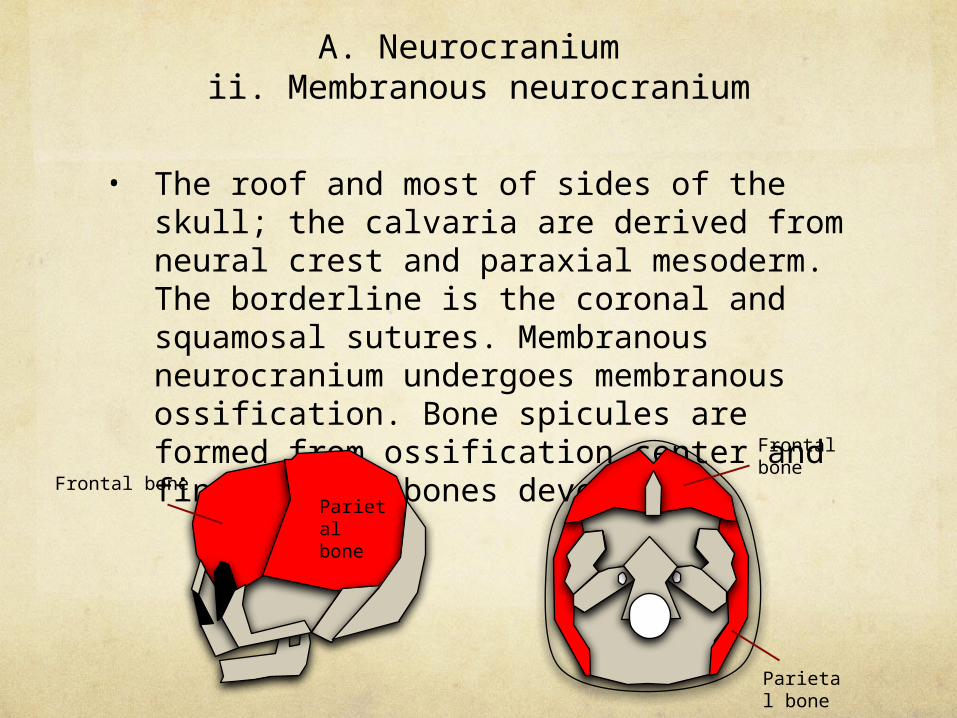
A. Neurocranium ii. Membranous neurocranium
• The roof and most of sides of the skull; the calvaria are derived from neural crest and paraxial mesoderm. The borderline is the coronal and squamosal sutures. Membranous neurocranium undergoes membranous ossification. Bone spicules are formed from ossification center and finally flat bones develop.
Parietal bone
Frontal bone
Frontal bone
Parietal bone

B. Membranous viscerocranium
The squamous temporal bone, maxilla and mandibule undergo membranous ossification. Be careful that the petrous part of the temporal bone and auditory ossicles are composed by endochondral ossification.
Maxilla
Nasal bone
Maxilla
Zygomatic bone
Squamous part of
Temporal bone
Squamous part of
Temporal bone

Why FGFR3 gene mutation causes morphologic
change on the skull base?ACH is due to FGFR3 gene mutation, which effects FGFR3 signalling in chondrocytes. The mutation brings limiting proliferation of chondrocyte and accelerating bone formation. The development of the skull base occurs mainly at the synchondroses, including intersphenoid, sphno-occipital and intraoccipital synchondroses. FGFR3 mutation accelerates ossification of cartilages in these synchondroses and causes early closure. Early closure can be the main reason to hypoplasia of the skull base on ACH.
Speno-occipatal synchondrosis
Anterior-intraoccipital
syncondrosis
Sphenoid bone
Occipital bone
Basioccipital
Exoccipital
Posterior-intraoccipital
syncondrosis
The anatomy of the skull base. There are some synchondroses of the intra- or inter-bones of the skull base.
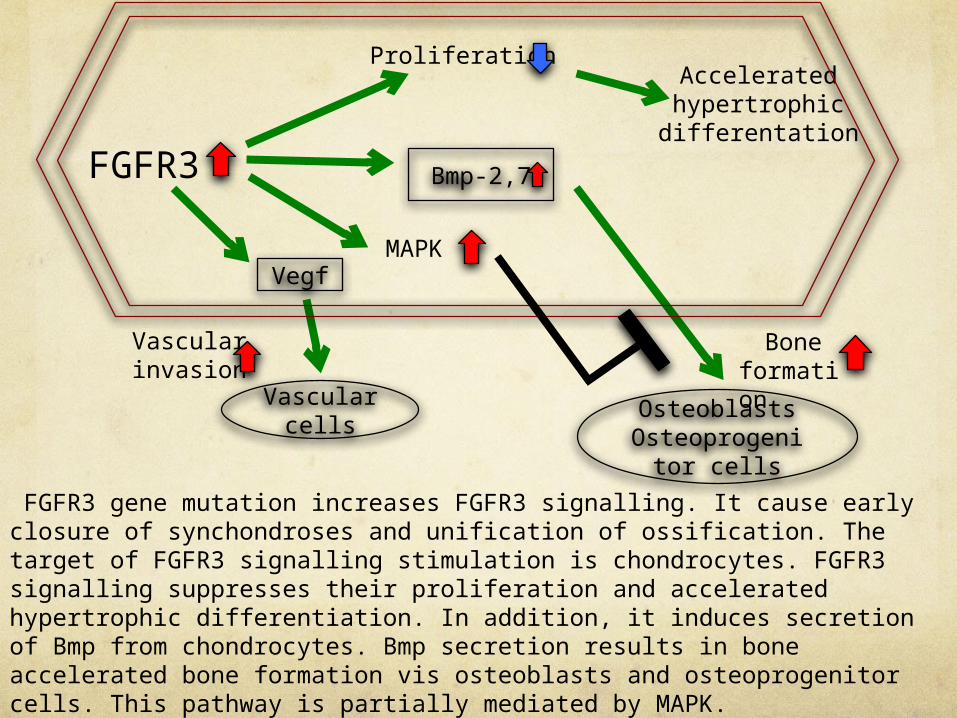
FGFR3 gene mutation increases FGFR3 signalling. It cause early closure of synchondroses and unification of ossification. The target of FGFR3 signalling stimulation is chondrocytes. FGFR3 signalling suppresses their proliferation and accelerated hypertrophic differentiation. In addition, it induces secretion of Bmp from chondrocytes. Bmp secretion results in bone accelerated bone formation vis osteoblasts and osteoprogenitor cells. This pathway is partially mediated by MAPK.Increased Fgfr3 signaling also causes upregulation of Vegf in chondrocytes, promoting vascular invasion. It would accelerate synchondrosis clousere while increased bone formation would accelerate the fusion of ossification centers.
Vascular cells
OsteoblastsOsteoprogenit
or cells
FGFR3
Acceleratedhypertrophicdifferentation
Vegf
Proliferation
Bmp-2,7
MAPK
Vascularinvasion
Boneformation

Summary of imaging findings on ACH
Dysplasia of temporal bone
Stenosis of foramen magnum
Narrowing of the jugular foramen
・ Hydrocephalus ・ Emissary foramina enlargement
Hearing loss
・ Poor development of the mastoid air cells ・ poor eustachian tube function
・ Towering petrous ridges.・ Rotation of the temporal bone structures
otitis media
Sudden death
Early closure of spheno-occipital and occipital bone
synchondroses.
FGFR3 mutations
Distortion of the skull base

I. Early closure of synchondroses
FGFR3 mutation accelerates ossification of the synchondroses.
Left column, case with ACH; right column, normal control of the same age. The spheno-occipital (orange) and intraoccipital synchondroses (blue) are already fused.

II. Small posterior cranial fossa
Small posterior cranial fossa can cause sudden death and hydrocephalus.a. Small foramen magnum having a tail and short clivus
The foramen magnum is small, causing compression to the medullocervical junction(orange). It is related to sudden death. Tail-like notch is often demonstrated at posterior margin (blue). It implies early fusion of intraoccipital synchondroses and influence by membranous ossification of the supraoccipit. Note clivus is very short, while the supraoccipit is not relatively affected, because posterior and lateral margins of the supraoccipit are influenced by membranous ossification. The tail may be formed by imbalance of elongation of the bones.
Clivus
Tail
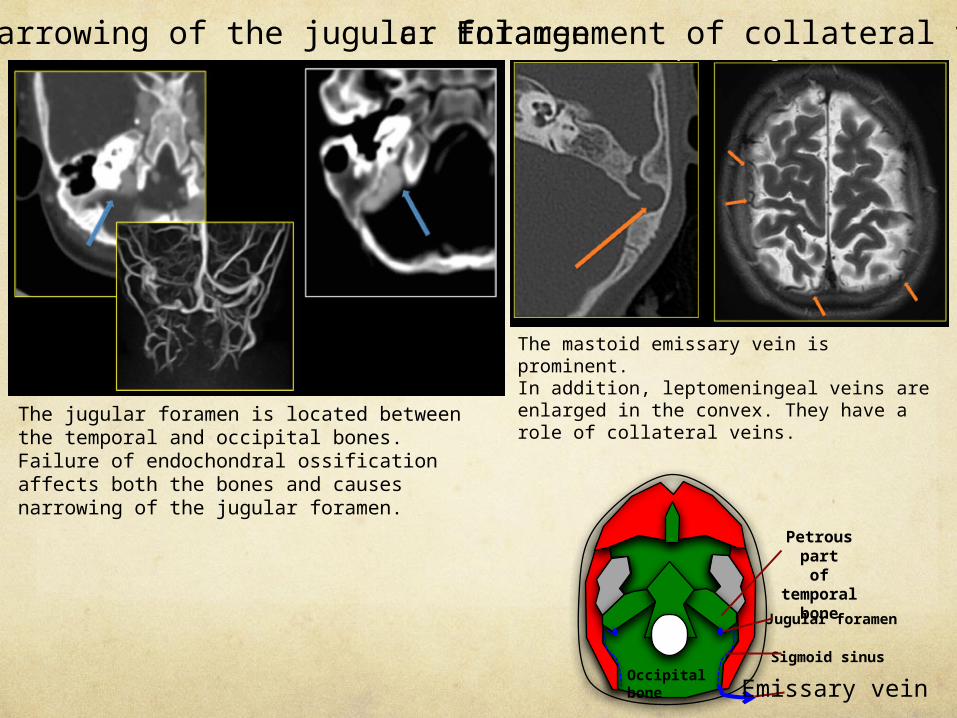
The jugular foramen is located between the temporal and occipital bones. Failure of endochondral ossification affects both the bones and causes narrowing of the jugular foramen.
b. Narrowing of the jugular foramenc. Enlargement of collateral veins
Petrous part of
temporal bone
Occipital bone
Jugular foramen
Sigmoid sinus
Emissary vein
The mastoid emissary vein is prominent.In addition, leptomeningeal veins are enlarged in the convex. They have a role of collateral veins.
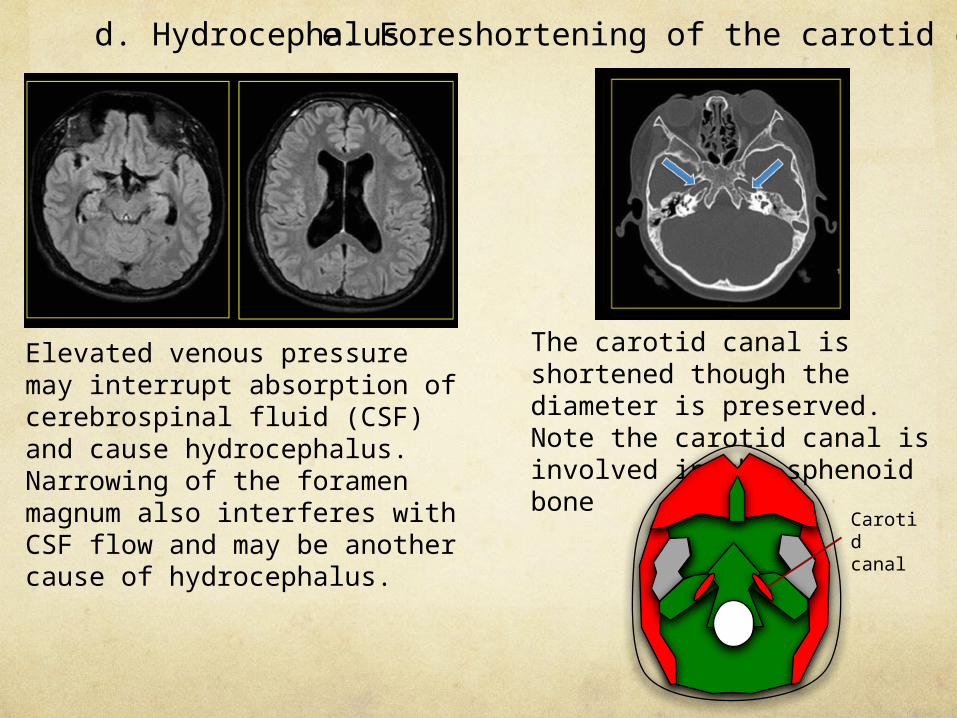
d. Hydrocephalus
Elevated venous pressure may interrupt absorption of cerebrospinal fluid (CSF) and cause hydrocephalus. Narrowing of the foramen magnum also interferes with CSF flow and may be another cause of hydrocephalus.
e. Foreshortening of the carotid canals
The carotid canal is shortened though the diameter is preserved. Note the carotid canal is involved in the sphenoid bone
Carotid canal
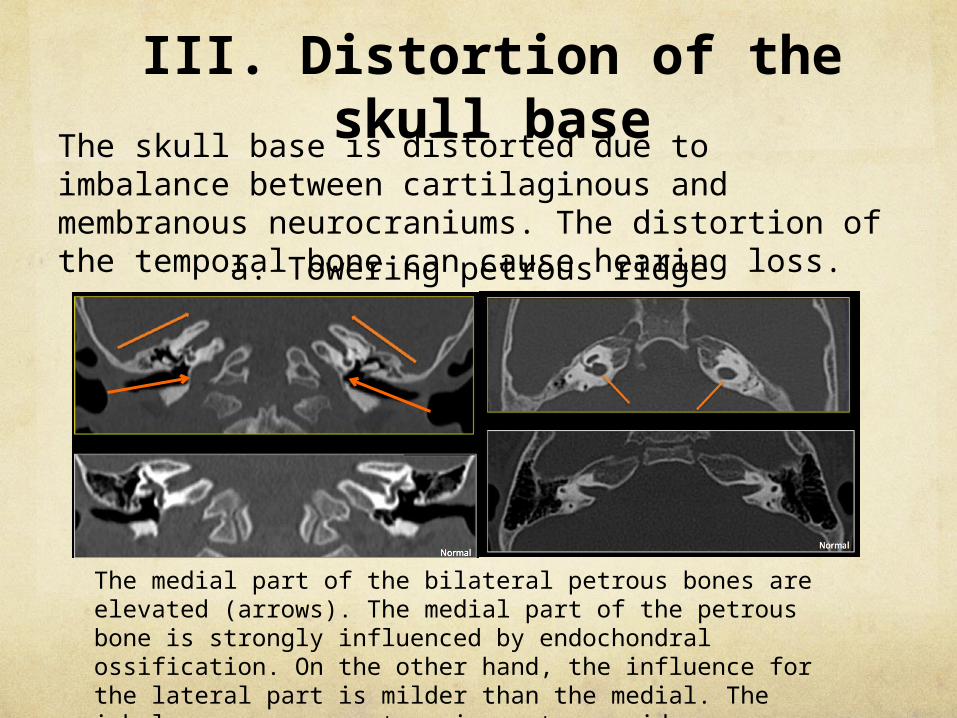
The skull base is distorted due to imbalance between cartilaginous and membranous neurocraniums. The distortion of the temporal bone can cause hearing loss.a. Towering petrous ridge
The medial part of the bilateral petrous bones are elevated (arrows). The medial part of the petrous bone is strongly influenced by endochondral ossification. On the other hand, the influence for the lateral part is milder than the medial. The imbalance can cause towering petrous ridge.
III. Distortion of the skull base
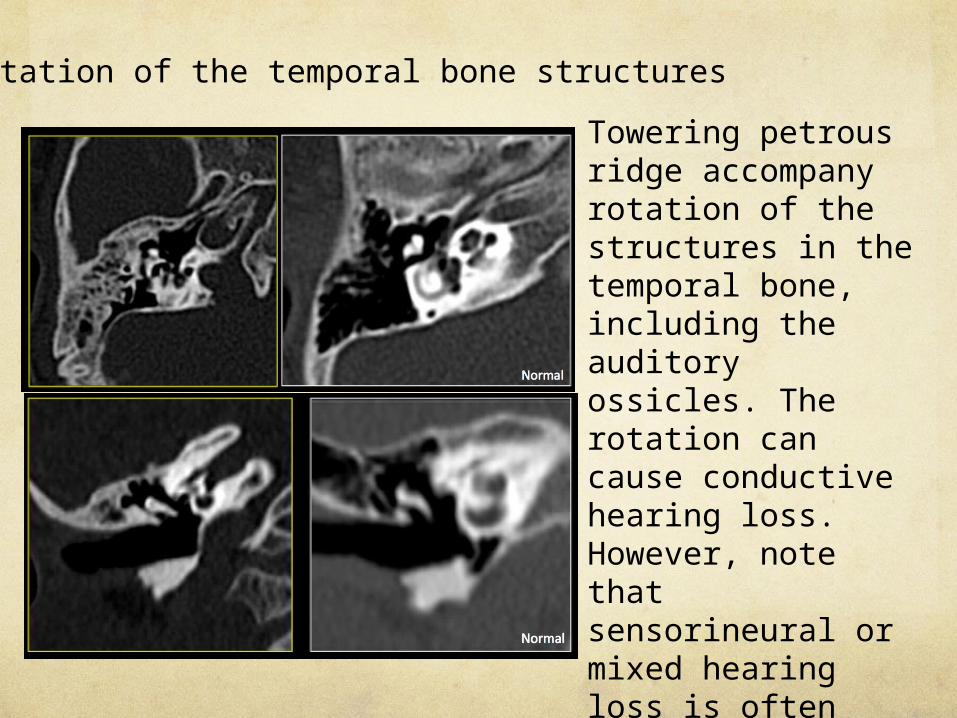
b. Rotation of the temporal bone structures
Towering petrous ridge accompany rotation of the structures in the temporal bone, including the auditory ossicles. The rotation can cause conductive hearing loss. However, note that sensorineural or mixed hearing loss is often observed on ACH. Microscopic inner ear abnormalities may be associated with sensorineural hearing loss.
Petrous part of the temporal
bone
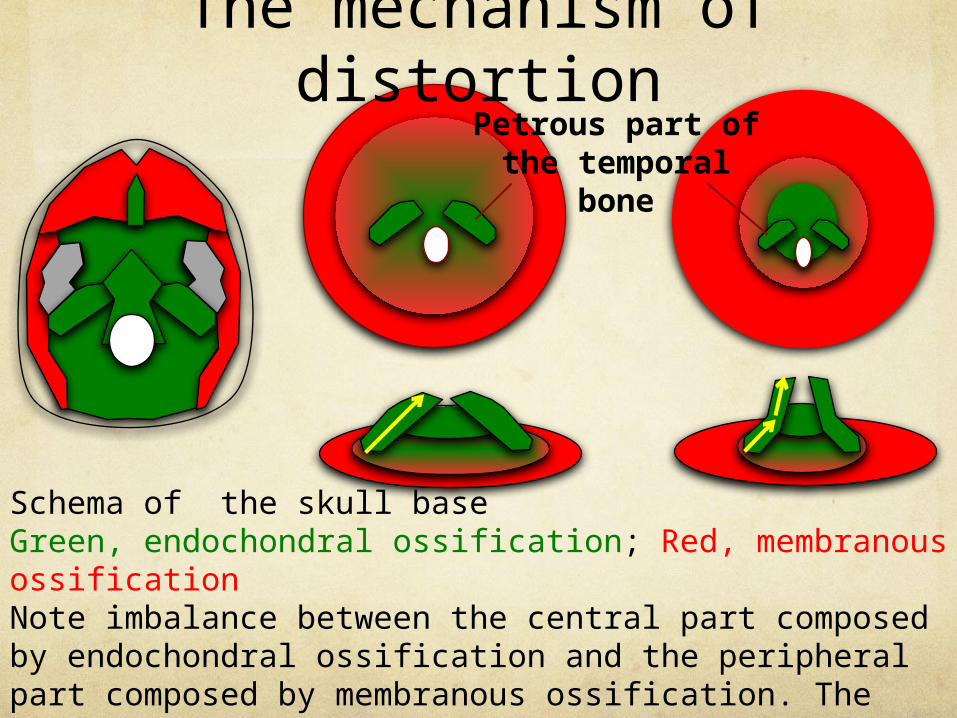
The mechanism of distortion
Schema of the skull baseGreen, endochondral ossification; Red, membranous ossificationNote imbalance between the central part composed by endochondral ossification and the peripheral part composed by membranous ossification. The imbalance causes bending and distortion of the petrous part of the temporal bone.
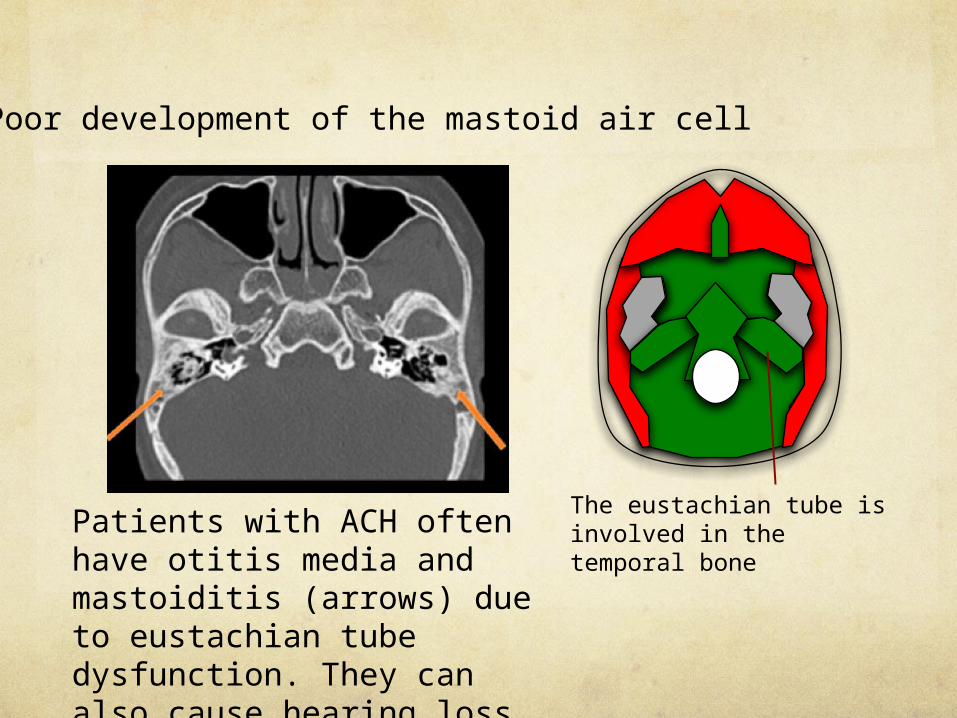
c. Poor development of the mastoid air cell
Patients with ACH often have otitis media and mastoiditis (arrows) due to eustachian tube dysfunction. They can also cause hearing loss.
The eustachian tube is involved in the temporal bone
Conclusion
Understanding vital morphologic changes on the skull base with embryology helps you to know various neurological complications in ACH.

References1. T.W.Sadler,Langmans`s. Medical Embryology(11th) 2009.2. Keith L. Moore,T.V.N.persaud. The Developing Human(8th) 2007.3. Cobb SR, Shohat M, Mehringer CM, et al. CT of the temporal bone in
achondroplasia. AJNR Am J Neuroradiol. 1988:9:1195-9. 4. Hecht JT, Horton WA, Reid CS, et al. Growth of the foramen magnum
in achondroplasia. Am J Med Genet. 1989:32:528-35. 5. Matsushita T, Wilcox WR, Chan YY, et al. FGFR3 promotes
synchondrosis closure and fusion of ossification centers through the MAPK pathway. Hum Mol Genet. 2009:18:227-40.
6. Jung J, Yang C, Lee S, et al. Bilateral ossiculoplasty in 1 case of achondroplasia. Korean J Audiol. 2013:17:142-7.
7. Shohat M, Flaum E, Cobb SR, et al. Hearing loss and temporal bone structure in achondroplasia. Am J Med Genet. 1993:45:548-51.
8. Thangamadhan Bosemani , Gunes Orman , Benedikt Hergan,et al. Achondroplasia in children: correlation of ventriculomegaly, size of foramen magnum and jugular foramina, and emissary vein enlargement . Childs Nerv Syst. 2014.


















