boletin nutricional vol10 CURVAS - Bariatric and Nutritional
description


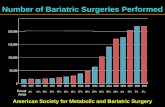
Background

Background

Bariatric surgeryLimitations to medical
treatment
BMI >40, or >35 kg/m2 if co-morbidity
Roux-en-Y gastric bypass, sleeve gastrectomy
BMIClassification
< 18.5Underweight
18.5–24.9normal weight
25.0–29.9 overweight
30.0–34.9class I obesity
35.0–39.9class II obesity
≥ 40.0class III obesity

RCT, N = 60
BMI ~ 45, duration DM ≥ 5 years, HbA1c ~ 8.5 %
Conventional medical therapy or gastric bypass or biliopancreatic diversion
Primary end point: diabetes remission* at 2 years
*FPG <100 mg/dl, HbA1c <6.5% without medication for 1 year
T2DM with severe obesity:
DM REMISSION: Medical therapy < gastric-bypass < biliopancreatic Sx (none) (75%) (95%) HbA1C decrease: 1 % 2 % 3.5 %
BMI and weight loss did NOT predict improvement in hyperglycemia.

Prospective RCT, N = 150 subjects
T2DM with modest obesity BMI 27–42 kg/m2
Primary end point: Resolution of T2DM at 1 year (HbA1c < 6%).

ReT2DM duration 8 yrs, BMI ~36, HbA1C ~9.2%
Medical Rx RYGB Sleeve G
DM resolution 12% 42% 37%
HbA1C decrease: 1.5% 2.8% 2.6%
Weight loss: 5.4 kg 29 kg 25 kg
Insulin resistance (HOMA-IR) improved after Sx.

BackgroundNo data from RCT: long-term
metabolic effects and clinical efficacy outcomes after bariatric surgery in moderately obese subjects with poorly controlled T2DM.

BackgroundThis study is a 2-year extension of a
metabolic substudy of the STAMPEDE trial.
Evaluate the effects of the three treatments on Glucose regulationPancreatic B-cell function (insulin
secretion/sensitivity)Body composition


INCLUSION CRITERIAAge 20 – 60 yrT2DM, HbA1c of ≥7.0% BMI 27 - 43 kg/m2 Candidate for general anesthesia
First consecutive 60 subjects randomized in main trial
~20 randomized to each group
F/U at DM clinic q 3 mo Baseline, at 12 and 24 mo- Metabolic assessment (Mixed-meal tolerance test)- Body composition measurement (DEXA)

Mixed-meal test
Time Plasma glucose
C-peptide
Insulin GLP-1, GIP
Glucagon
Lipids, HbA1c, adipokines, complete metabolic panel
0 min x x x x x x
30 min
60 min x
90 min
120 min x
Diabetes meds stopped 24 h before study, including insulin.NPO overnight 12-14 h.
Liquid mixed meal - commercial product (Boost; 8 ounces, 350
kcal, 55% carbohydrate, 25% protein, 20% fat) Glucose tolerance, insulin sensitivity &
secretion

CalculationsInsulin secretion rate (ISR)
Pancreatic B-cell function: measure by insulin secretion / insulin resistance (disposition) index(Matsuda index)

Statistical analysisNo power calculations for the substudy measures due to
lack of published data regarding specified metabolic outcome measures at the time of trial design (2004–2005), and because of exploratory nature of substudy.
Continuous variables with a normal distribution: means and SDs.
Variables with a non-normal distribution: medians and interquartile ranges.
Categorical variables: frequencies; tested with x2 statistic or Fisher exact test (two-tailed).
One-way ANOVA: continuous laboratory parameters Comparisons between treatment groups: Student t test or
Wilcoxon test. Glucose and insulin measures collected during the mixed
meal tolerance test were plotted graphically.


Patients
N =20 -> 17
N =20 -> 18
N =20 -> 19
10% lost to F/U

Baseline characteristics

Glycemic control
*P for IMT vs. gastric bypass †P for IMT vs. sleeve gastrectomy‡P for gastric bypass vs. sleeve gastrectomy
Gastric bypass: Significantly greater
reduction in FPG, HbA1c

Cardiovascular risk
*P for IMT vs. gastric bypass †P for IMT vs. sleeve gastrectomy‡P for gastric bypass vs. sleeve gastrectomy
Both surgery groups- HDL cholesterol - TG, hsCRP

BW, body composition, adipokines
*P for IMT vs. gastric bypass †P for IMT vs. sleeve gastrectomy‡P for gastric bypass vs. sleeve gastrectomy
Bariatric Sx groups:Greater BW loss after bariatric Sx at 12 months and maintained at 24-mo. Body weight, BMI, and absolute change in total body fat percent at 24 mo.

BW, body composition, adipokines
*P for IMT vs. gastric bypass †P for IMT vs. sleeve gastrectomy‡P for gastric bypass vs. sleeve gastrectomy
Reduction in percent truncal fat was greater in gastric bypass versus sleeve gastrectomy
Leptin levels reduced markedly after surgical weight loss, especially gastric bypass.

Mixed meal tolerance

FPG, 2hPP GB -> Sleeve ->
IMT
Fasting C-peptide (not IMT) 2x PP C-peptide (GB > Sleeve)

Insulin sensitivityMedian values for the insulin sensitivity
(Matsuda index) in noninsulin-using subjects increased at 24 months after gastric bypass by 2.7-fold1.2-fold after sleeve gastrectomyDid not change with IMT
The absolute change in median insulin sensitivity (Matsuda index) at 24 months tended to be higher in gastric bypass compared with sleeve
gastrectomy despite equivalent weight loss.

Pancreatic hormone functionThe absolute change in median values for
pancreatic B-cell function (oral disposition index) at 24 months Markedly greater in gastric bypass than IMT (P
<0.001) but not different between sleeve gastrectomy and
medical therapy
B-cell function from baseline 5.8-fold increase in gastric bypassNegligible increases in sleeve gastrectomy and IMT.

Incretin response
P value 1 for IMT vs. gastric bypass P value 2 IMT vs. sleeve gastrectomy P value 3 Gastric bypass vs. sleeve gastrectomy


DiscussionBariatric surgery provides durable glycemic
control compared with intensive medical therapy at 2 years.
Despite similar weight loss as sleeve gastrectomy,
Gastric bypass uniquely restores pancreatic B-cell function and reduces truncal fat, thus reversing the core defects in diabetes.

Our results extend the findings from our initial 12-month report and
Suggest factors beyond weight loss that are specific to intestinal bypass patients help regulate glucose levels and restore pancreatic B-cell function.

In gastric bypass patients, both insulin sensitivity and secretion components increased but,
Despite comparable weight loss in sleeve gastrectomy, insulin sensitivity was only partially restored and pancreatic B-cell function did not improve.

Both bariatric surgery procedures stimulated incretins with markedly increased postprandial GLP-1 levels as noted in previous observational studies in obese patients with type 2 diabetes.
However, divergence in postprandial GIP levels were noted, with a reduction seen only in gastric bypass that may be related to anatomical exclusion of the duodenum (which produces GIP) or may be reflective of improved GIP action that is noted to be defective in type 2 diabetes.

Marked improvements in insulin sensitivity and glycemic control observed in the gastric bypass group suggest factors specifically linked to the presence of abdominal (truncal) fat.
Ectopic abdominal fat presence has long been recognized to induce insulin resistance, subclinical inflammation, and cardiovascular risk specific to type 2 diabetes.

In the current study, adipogenic inflammation was significantly reduced after both bariatric procedures, especially gastric bypass, mediated by factors such as free fatty acids, leptin, and C-reactive protein, which impair glucose uptake by insulin-dependent tissues (muscle and liver).

LimitationA limitation of this study is the validity of the
incretin hormone responses that were obtained after the assigned interventions.
Concentrations of GLP-1 and GIP were obtained at fasting and at 60 min after meal ingestion, and this likely underestimates the incretin surge that normally occurs rapidly (within 15 min) after meal ingestion.

ApplicationFurther studies are warranted to thoroughly
investigate the long-term effects of bariatric surgery on incretin responses and action to modulate insulin secretion.
More vigorous and behavioral/lifestyle modification strategies as used in the Look AHEAD trial that aggressively target weight loss are clearly needed.
Future randomized control trials are needed to compare such strategies results with bariatric surgery.