Measles
61
1 43 6 DR.SATTI MOHAMMED SALEH MEEQAT HOSPITAL MEDICAL DIRECOR INFECTION CONTROL DIRECTOR CBAHI SIT MEMBER Control of outbreak of Measles in Rehab Center in Medina , June 2015 Effective Infection Control, Teamwork and Preparedness
Transcript of Measles
1436
DR.SATTI MOHAMMED SALEHMEEQAT HOSPITAL MEDICAL DIRECORINFECTION CONTROL DIRECTORCBAHI SIT MEMBER
Control of outbreak of Measles in Rehab Center in Medina, June 2015 Effective Infection Control, Teamwork and Preparedness
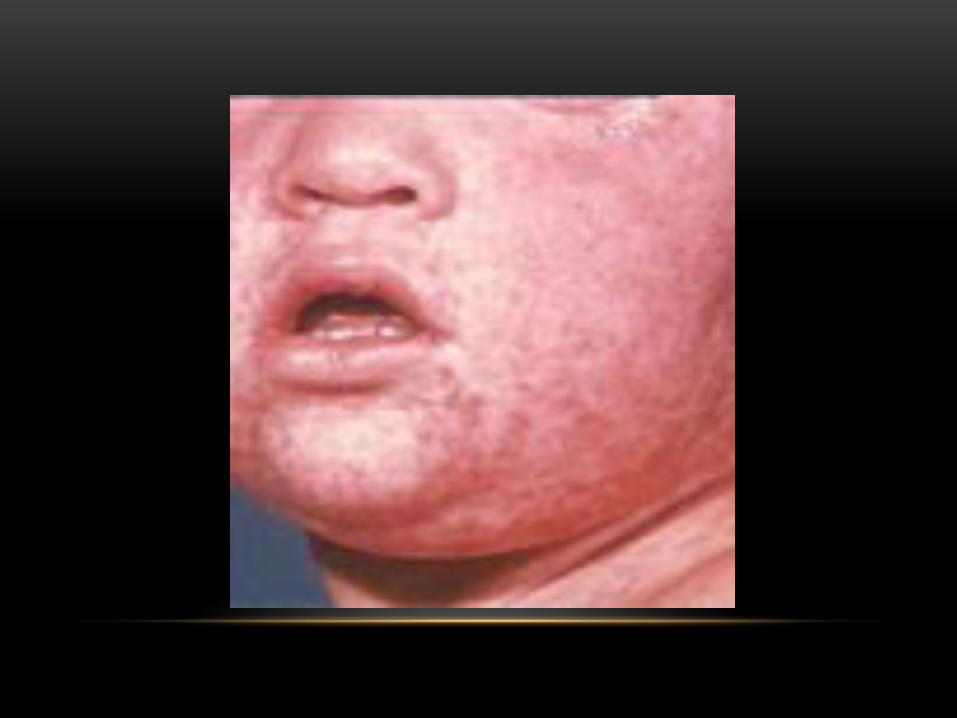
Measles is an acute viral respiratory illness. It is characterized by a prodrome of fever (as high as
105°F) and malaise, cough, coryza, and conjunctivitis -the three “C”s -, a pathognomonic
enanthema (Koplik spots) followed by a maculopapular rash. The rash usually appears
about 14 days after a person is exposed
MEASLES
THE VIRUS
Measles is caused by a single-stranded, enveloped RNA virus with 1 serotype. It is classified as a member of the genus Morbillivirus in the Paramyxoviridae family. Humans are the only natural hosts of measles virus
BackgroundBackgroundBackgroundBackground
In the decade before the live measles vaccine was licensed in 1963, an average of 549,000 measles cases and 495 measles deaths were reported annually in the United States
• Europe, Asia, the Pacific, and Africa. An estimated 20 million people become infected with measles worldwide each year, of whom 146,000 die.
TRANSMISSION• Measles is one of the most contagious of all
infectious diseases; approximately 9 out of 10 susceptible persons with close contact to a measles patient will develop measles. The virus is transmitted by direct contact with infectious droplets or by airborne spread when an infected person breathes, coughs, or sneezes. Measles virus can remain infectious in the air for up to two hours after an infected person leaves an area
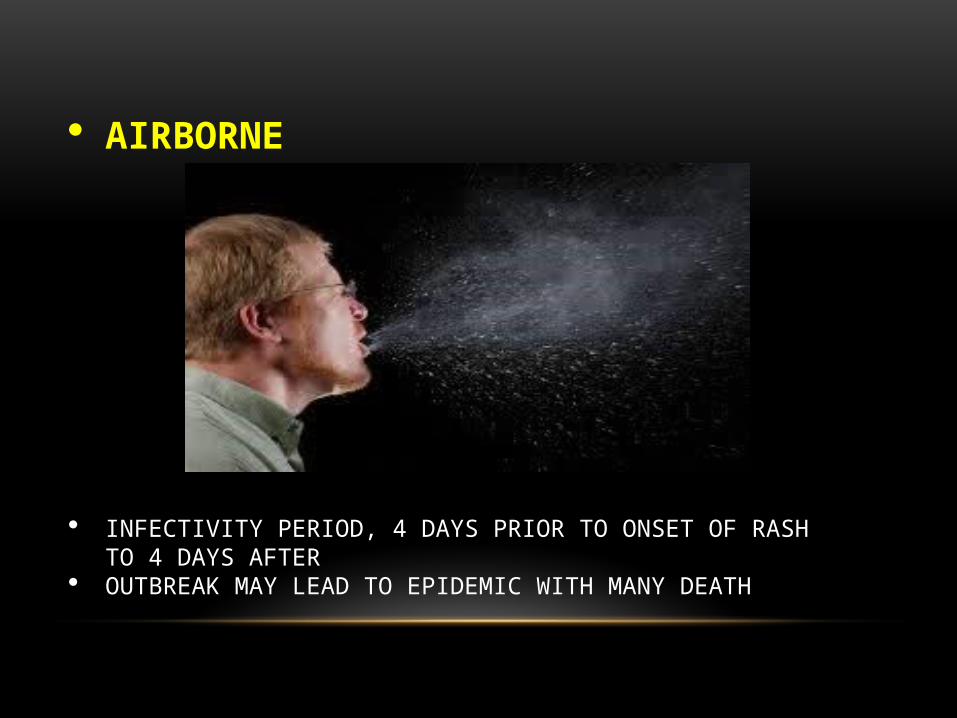
AIRBORNE
INFECTIVITY PERIOD, 4 DAYS PRIOR TO ONSET OF RASH TO 4 DAYS AFTER
OUTBREAK MAY LEAD TO EPIDEMIC WITH MANY DEATH
INCUBATION PERIOD
7 – 14 DAYS
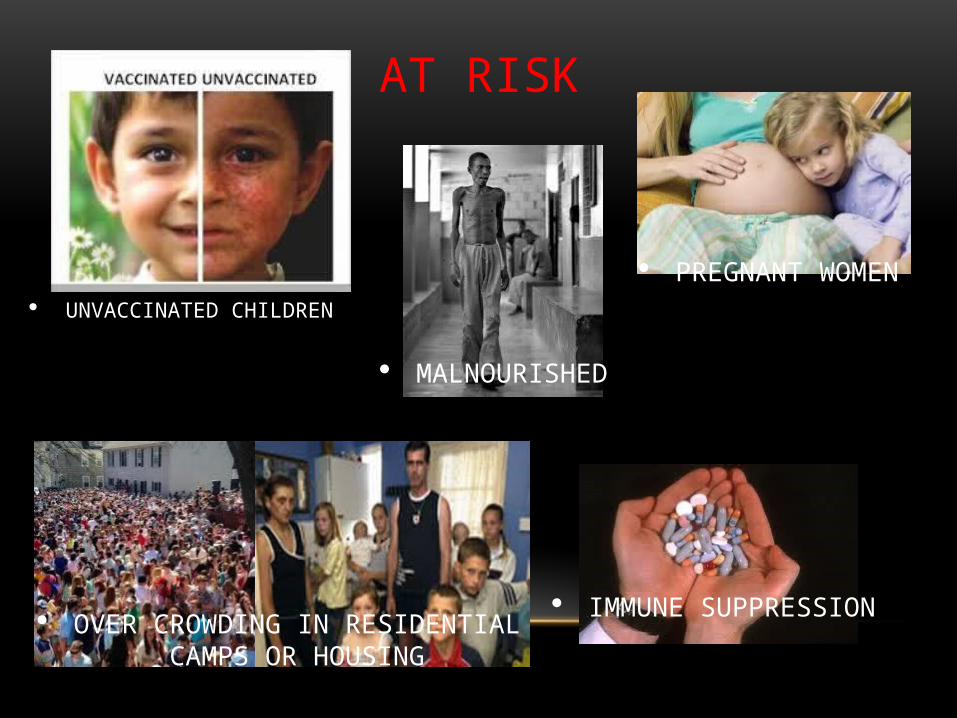
AT RISK
UNVACCINATED CHILDREN
MALNOURISHED
PREGNANT WOMEN
IMMUNE SUPPRESSION OVER CROWDING IN RESIDENTIAL CAMPS OR HOUSING
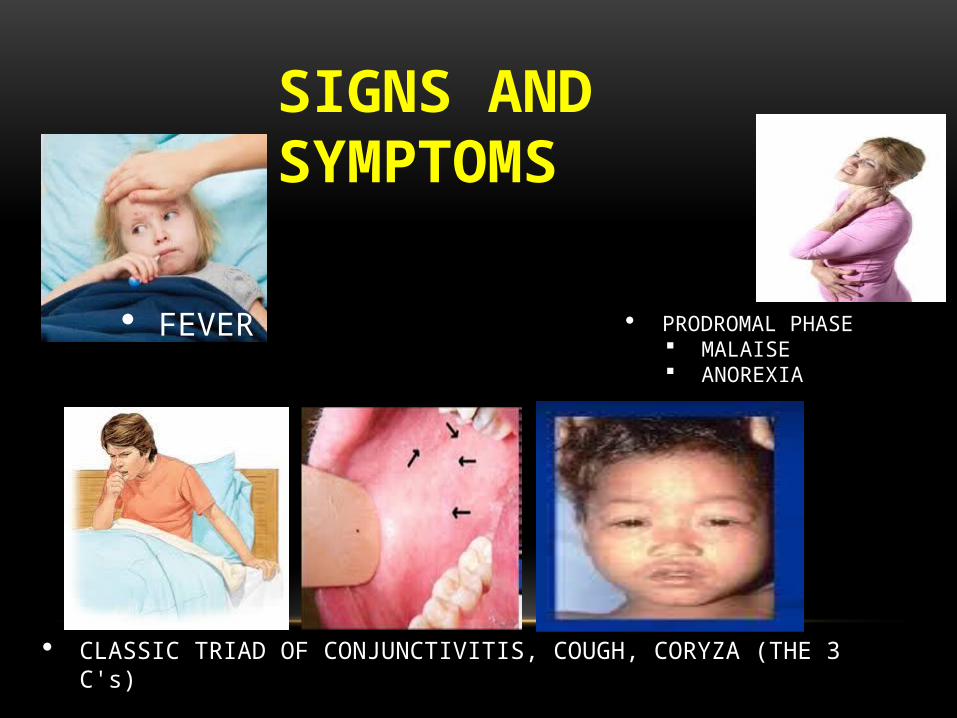
PRODROMAL PHASE MALAISE ANOREXIA
SIGNS AND SYMPTOMS
FEVER
CLASSIC TRIAD OF CONJUNCTIVITIS, COUGH, CORYZA (THE 3 C's)
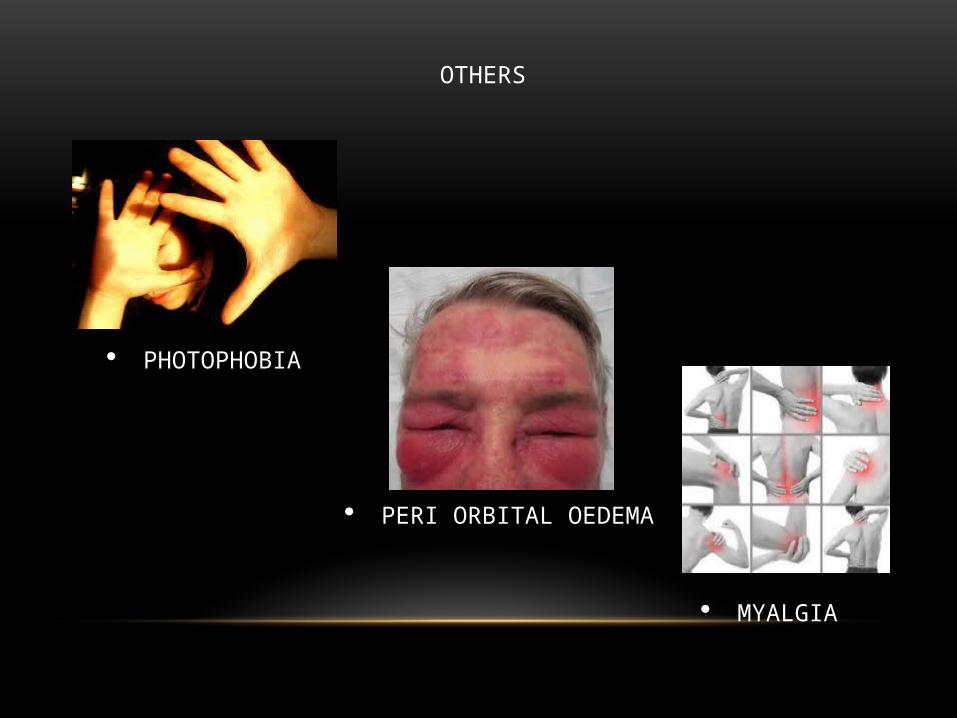
OTHERS
MYALGIA
PHOTOPHOBIA
PERI ORBITAL OEDEMA
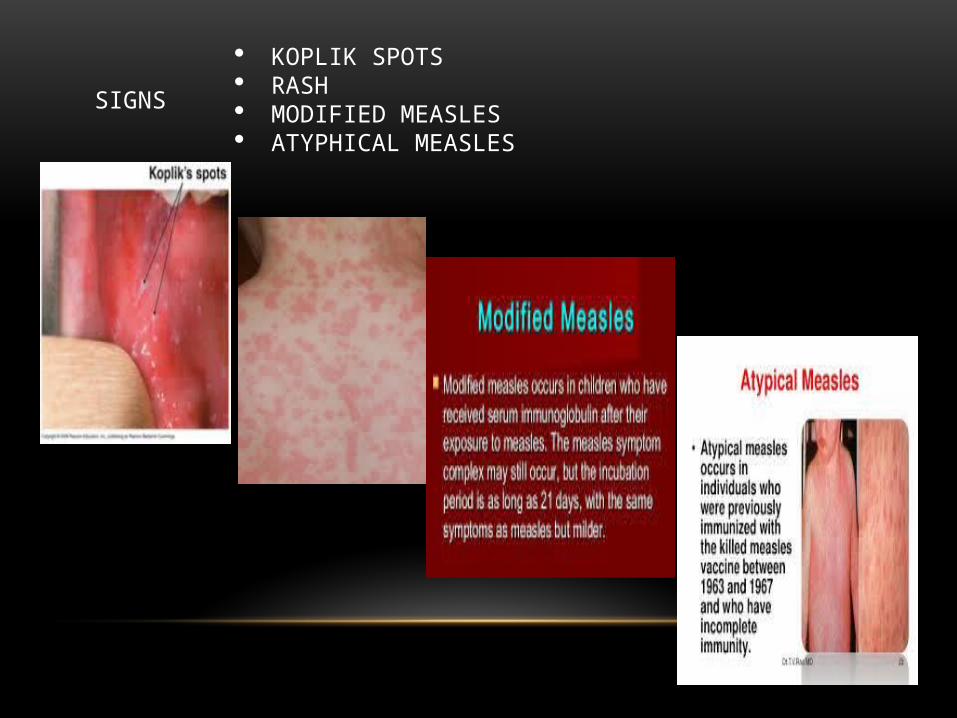
SIGNS
KOPLIK SPOTS RASH MODIFIED MEASLES ATYPHICAL MEASLES

KOPLIK SPOTS
CASE DEFINITION1. SUSPECTED CASE- FEVER WITH RASH2. PROBALBLE CASE
(CLINICAL CASE DEFINITION)NO LAB SUPPORT
3. CONFIRMED CASE- LABORATORY CONFIRMED- EPIDIMIOLOGICALLY LINKED TO
CONFIRMED CASE
PEOPLE AT HIGH RISK FOR COMPLICATIONS
• People at high risk for severe illness and complications from measles include:
• Infants and children aged <5 years• Adults aged >20 years• Pregnant women• People with compromised immune systems
COMPLICATIONS• Common complications from measles include otitis media,• bronchopneumonia,• laryngotracheobronchitis,• and diarrhea.• Even in previously healthy children, measles can cause serious illness
requiring hospitalization.• One out of every 1,000 measles cases will develop acute encephalitis,
which often results in permanent brain damage
DIAGNOSIS AND LABORATORY TESTING• Healthcare providers should consider measles in
patients presenting with febrile rash illness and clinically compatible measles symptoms, especially if the person recently traveled internationally or was exposed to a person with febrile rash illness. Healthcare providers should report suspected measles cases to their local health department within 24 hours
LABORATORY CONFIRMATION• Laboratory confirmation is essential for all sporadic
measles cases and all outbreaks.
• Detection of measles-specific IgM antibody
• and measles RNA by real-time polymerase chain reaction
• (RT-PCR) are the most common methods for confirming measles infection
HEALTHCARE PERSONNEL
• Healthcare personnel should have documented evidence of immunity against measles, according to the
POST-EXPOSURE PROPHYLAXIS• People exposed to measles who cannot readily
show that they have evidence of immunity against measles should be offered post-exposure prophylaxis (PEP) or be excluded from the setting (school, hospital, childcare). MMR vaccine, if administered within 72 hours of initial measles exposure, or immunoglobulin (IG), if administered within six days of exposure, may provide some protection or modify the clinical course of disease
MMR VACCINE AS POST-EXPOSURE PROPHYLAXIS• If MMR vaccine is not administered within 72 hours of exposure as PEP, MMR
vaccine should still be offered at any interval following exposure to the disease in order to offer protection from future exposures. People who receive MMR vaccine or IG as PEP should be monitored for signs and symptoms consistent with measles for at least one incubation period.
• If many measles cases are occurring among infants younger than 12 months of age, measles vaccination of infants as young as 6 months of age may be used as an outbreak control measure. Note that children vaccinated before their first birthday should be revaccinated when they are 12 through 15 months old and again when they are 4 through 6 years of age.
• Except in healthcare settings, unvaccinated people who receive their first dose of MMR vaccine within 72 hours after exposure may return to childcare, school, or work.
IMMUNOGLOBULIN (IG) AS POST-EXPOSURE PROPHYLAXIS• People who are at risk for severe illness and complications from measles,
such as infants younger than 12 months of age, pregnant women without evidence of measles immunity, and people with severely compromised immune systems, should receive IG. Intramuscular IG (IGIM) should be given to all infants younger than 12 months of age who have been exposed to measles. For infants aged 6 through 11 months, MMR vaccine can be given in place of IG, if administered within 72 hours of exposure. Because pregnant women might be at higher risk for severe measles and complications, intravenous IG (IGIV) should be administered to pregnant women without evidence of measles immunity who have been exposed to measles. People with severely compromised immune systems who are exposed to measles should receive IGIV regardless of immunologic or vaccination status because they might not be protected by MMR vaccine
POST-EXPOSURE PROPHYLAXIS FOR HEALTHCARE PERSONNEL
• If a healthcare provider without evidence of immunity is exposed to measles, MMR vaccine should be given within 72 hours, or IG should be given within 6 days when available. Exclude healthcare personnel without evidence of immunity from duty from day 5 after first exposure to day 21 after last exposure, regardless of post-exposure vaccine
ISOLATION• Infected people should be isolated for four days after they develop a rash.
Healthcare providers should follow respiratory etiquette and airborne precautions in healthcare settings. Regardless of presumptive immunity status, all healthcare staff entering the room should use respiratory protection consistent with airborne infection control precautions (use of an N95 respirator or a respirator with similar effectiveness in preventing airborne transmission). Because of the possibility, albeit low, of MMR vaccine failure in healthcare providers exposed to infected patients, they should all observe airborne precautions in caring for patients with measles. The preferred placement for patients who require airborne precautions is in a single-patient airborne infection isolation room (AIIR).
• People without evidence of immunity who have been exempted from measles vaccination for medical, religious, or other reasons and who do not receive appropriate PEP within the appropriate timeframe should be excluded from affected institutions in the outbreak area until 21 days after the onset of rash in the last case of measles
TREATMENT• There is no specific antiviral therapy for measles. Medical
care is supportive and to help relieve symptoms and address complications such as bacterial infections.
• Severe measles cases among children, such as those who are hospitalized, should be treated with vitamin A. Vitamin A should be administered immediately on diagnosis and repeated the next day. The recommended age-specific daily doses are
• 50,000 IU for infants younger than 6 months of age• 100,000 IU for infants 6–11 months of age• 200,000 IU for children 12 months of age and older

TREATMENT
ANTIBIOTIC FOR SECONDARY INFECTION
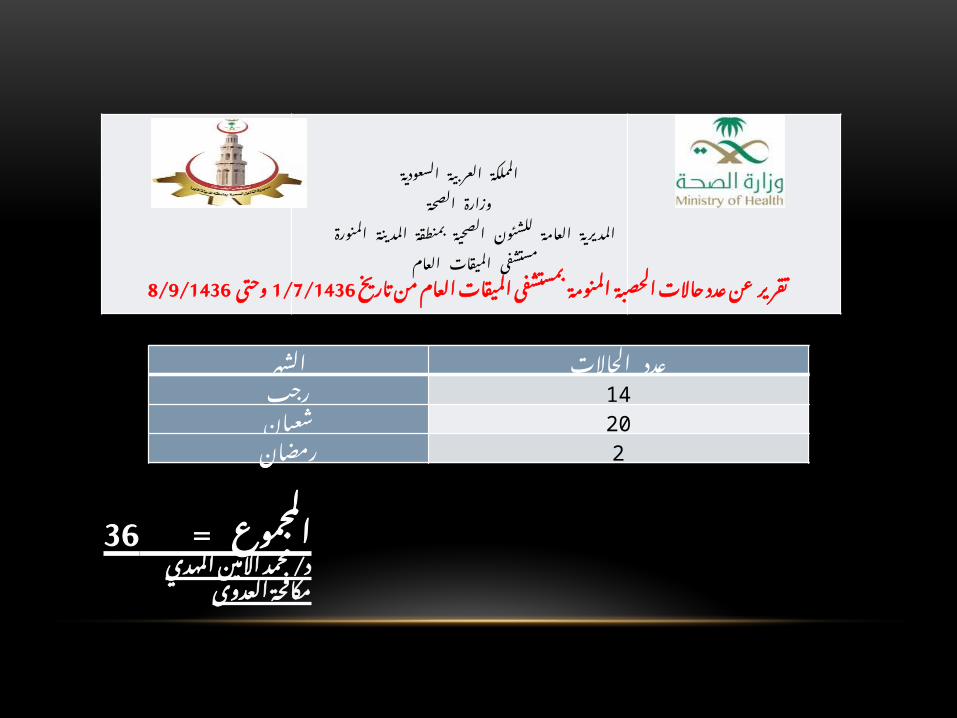
السعودية العربية المملكة
الصحـــة وزارةالمدينة بمنطقة الصحية للشئون العامة المديرية
المنورةالعام الميقات مستشفى
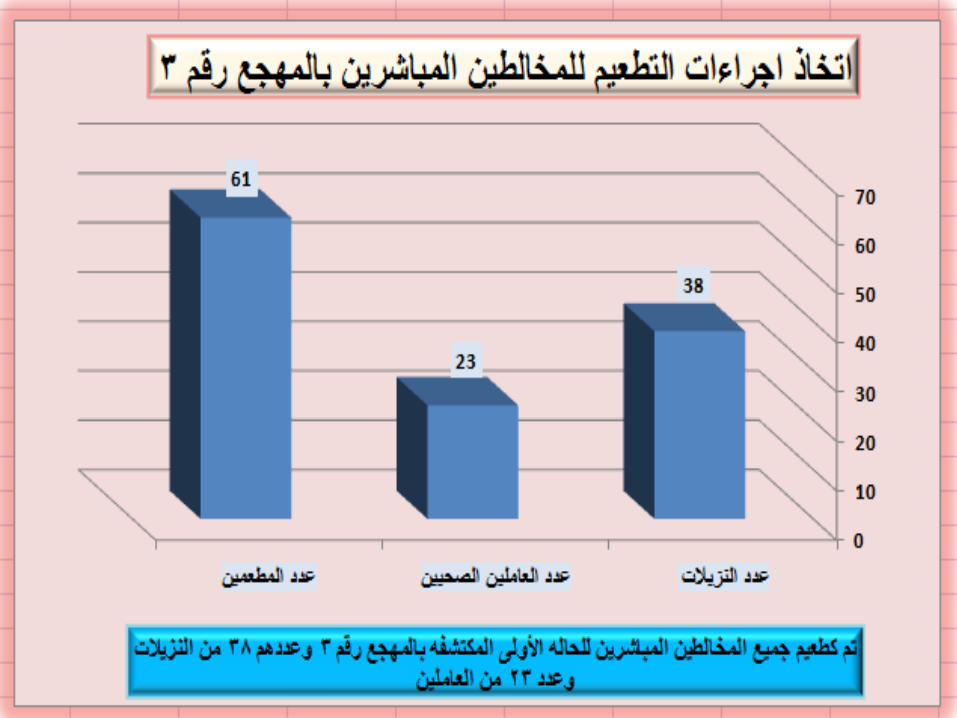
تاريخ من العام الميقات بمستشفى المنومة الحصبة حاالت عدد عن 1/7/1436تقرير8/9/1436وحتى
الشهر الحاالت عددرجب 14
شعبان 20رمضان 2
الشهر الحاالت عددرجب 14
شعبان 20رمضان 2
36المجموع = المهدي/ االمين محمد د
العدوى مكافحة
STEPS FOR OUTBREAK INVESTIGATION
1. VERIFY THE DIAGNOSIS2. CONFIRM THAT OUTBREAK EXIST3. SEARCH FOR ADDITIONAL CASES4. CHARACTERISE CASES BY PERSON, PLACE AND TIME5. (ALINE LISTING AND DRAW EPIDEMIC CURVE)6. FORM ATENTATIVE HYPOTHESIS7. INSTITUTE PRELIMINARY CONTROL MEASURES (HAND
HYGIENE, ISOLATION, ASSISTANCE NEEDED, COHORING, etc.,
8. TEST HYPOTHESIS9. REFINE THE CONTROL MEASURES10. MONITOR AND EVALUATE CONTROL MEASURES


W.H.O. RESPONSE
END OF 2015REDUCE BY 95 %
MEASLES DEATH ACHIEVE MEASLES AND RUBELLA (CR'S)ELIMINATION GOAL
BY END OF 2020 ELIMINATE MEASLES AND RUBELLA IN 5 W.H.O. REGIONS
5 CORE COMPONENTS
1. INCREASE VACCINATION COVERAGE MMR
2. MONITOR DISEASE (SURVEILANCE)3. OUTBREAK PREPAREDNESS4. RAPID RESPONSE AND EFFECTIVE
TREATMENT5. RESEARCH

CONTROL OF COMMUNICABLE DISESES( IMPORTANT MEASURES )1- PATIENTS2- CONTACTS3- ENVIRONMENT.A- MEASURES TOWARDS PATIENTS:-1- EARLY DETECTION2- CONFIRMATION 3- NOTIFICATION ( WRITTEN POLICY ).4- ISOLATION
1- EARLY DETECTION2- INVESTIGATIONS3- VACCINATIONS4- CHEMOPROPHYLAXIS5- OBSERVATION6- TREATMENT7- HEALTH EDUCATION.
B- Measures Towards Contact
PLAN
1. TEAM ORGANIZATION2. VISIT THE CRC3. MEETING WITH ADMINISTRATION4. MEETING WITH DOCTORS AND NURSES5. DISCUSS THE SCIENTIFIC FACTS6. DISCUSS THE SERIOUS IMPLICATIONS7. VIEW THE STRUCTURE AND PROCESS
FOLLOWED8. TOUR THROUGH DIFFERENT
DEPARTMENTS WITH OBSERVATIONB, DOCUMENTS REVIEW, INTERVIEW STAFFS.
PLAN AND CONTROL MEASURES
1. MEASURE TOWARDS PATIENTS2. MEASURE TOWARDS CONTACTS3. MEASURE TOWARD ENVIRONMENT
OUT BREAK CONTROL TEAM PLAN1. MEASURES TOWARDS PATIENTS
a. FOR EARLY DIAGNOSIS AND ISOLATIONi. 3 ROOMS WITH HEPA FILTERS FOR SUSPEECTED CASESii. 5 ROOMS WITH HEPA FILTERS FOR PROBALE CASESiii. TRAIN 2 DOCTORS AND NURSING DIRECTOR AND SUPERVISORSiv. TASK FORCE FROM MEEQAT HOSPITAL
A. ICPB. CETD NURSEC. QUALITY NURSED. TRAINERS
2. TEACHING FOR BASIC IC STANDARD3. PROVISION OF SUPPLIES NEEDED4. ANY PATIENT WITH COMPLICATION OR CO MORBID DISEASE TO BE REFERRED TO MEEQAT HOSPITAL5. ISOLATE FOR INFECTIVITY PERIOD6. CONCOMITANT DISINFECTION ANF DISINFECTION AND TERMINAL CLEANING7. VISITORS CONTROL8. CONTROL ALL ACTIVITIES9. 24 HOURS NOTIFIVATION
EVIDENCE OF IMMUNITY• written documentation of adequate vaccination:
• one or more doses of a measles-containing vaccine administered on or after the first birthday for preschool-age children and adults not at high risk
• two doses of measles-containing vaccine for school-age children and adults at high risk, including college students, healthcare personnel, and international travelers
• laboratory evidence of immunity• laboratory confirmation of measles• birth before 1957
FOR CONTACTS:1. EVIDENCE OF IMMUNITY (NONE)2. VACCINATE ALL RESIDENTS WITH MMR3. FOR THOSE WITH COMORBID DISEASE, UNDER
NUTRITION,IMMUNO SUPPRESSION, 2 DOSES, OF MMR (I MONTH APART)

VACCINE RECOMMENDATIONS• Children• CDC recommends routine childhood immunization for MMR vaccine starting with the first
dose at 12 through 15 months of age, and the second dose at 4 through 6 years of age or at least 28 days following the first dose.
• Students at post-high school educational institutions
• Students at post-high school educational institutions without evidence of measles immunity need two doses of MMR vaccine, with the second dose administered no earlier than 28 days after the first dose.
• Adults• People who are born during or after 1957 who do not have evidence of immunity against
measles should get at least one dose of MMR vaccine

SURVEILLANCE
EPIDEMIC CURVE FOLLOW UP DAILY BASIS COLLECT DATA AS NEEDED FOLLOW UP CMPLIANCE WITH IC POLICIES TO CONTINUE SURVEILLANCE FOR 2 WEEKS AFTER THE ONSET OF
RASH IN THE LAST CASE

HEALTHCARE PERSONNEL
• Healthcare personnel should have documented evidence of immunity against measles, according to the
GOALS OF MEASLES OUTBREAK RESPONSE:
• - The primary goal of measles outbreak response was to reduce morbidity and mortality by providing appropriate case management and vaccinating contacts.
SECONDARY GOALS ARE TO :
• - limit the spread of outbreak.• identify high-risk groups/areas for implementing
strategies to improve vaccination • assist in the identification and correction of
weaknesses in immunization and surveillance• raise awareness in the community about the
disease and its prevention
POST-OUTBREAK ACTIVITIES•
• After an outbreak, the Epidemic Response Team must carry out a thorough evaluation of the following:
• cause of the epidemic
• surveillance of measles and detection of the outbreak
• preparedness for the epidemic
• management of the epidemic
• immunization program goals and operations
PREVENTING FUTURE OUTBREAKS:•
• There are 4 main keys in preventing measles outbreak:• Suspecting measles as a possibility and properly
diagnosing patient.• Instituting immediate airborne isolation.• Measles immunization campaigns. • Ensuring easily retrievable measles immunity records for
healthcare workers
IMPRESSION AND RECOMMENDATIONS
• Overcrowded institutions which provide health care to persons with co morbid diseases and decreased immune status should have a policy to combat all vaccine-preventable diseases without waiting for disease to occur to start vaccination
• .
• All healthcare workers should be trained to adhere and implement infection control measures.
•
• Hospital infection control departments should ensure that all healthcare workers are screened and vaccinated against all vaccine-preventable diseases.
• All healthcare workers should have a file with the employee health clinic and infection control unit documenting all their screenings and vaccination as per CBAHI infection control standard e.g. all staff in Al-Meqat General hospital have files documenting their vaccination status and all received MMR during the last outbreak.
• • In the event of an outbreak we should have a way for rapid laboratory
confirmation ( to be discussed with higher authority in MOH ).• • It is recommended to give 2 doses of MMR vaccine, one month interval
for all persons with co morbid or decreased immune status.• • Strengthening the surveillance system at CRC through staff training,
regular active surveillance visits and implementation of HESN program
• Improving overall levels of vaccine coverage in the population.
•
• If an outbreak is anticipated, supplementary immunization activities should be considered.
•
• When an outbreak occurs that has not been predicted, or could not be prevented, the response needs to be rapid, since measles is highly infectious and spreads rapidly
•
• Discussing measles outbreak of CRC in the next meeting of early preparedness for outbreak committee.
•
• Holding health education campaigns to raise public awareness about measles and importance of vaccination
• The establishment of the outbreak Coordination Committee under the chairmanship of HE Assistant General Director of Public Health. The Outbreak Coordinating Committee should ensure that the following actions are carried out:
• Prompt laboratory confirmation of the outbreak,• ensuring adequate clinical management of cases,• intensifying surveillance and notification of suspected cases• investigating a confirmed measles outbreak, • implementing control and preventive measures (including vaccination
activities),• assessing the risk of a large outbreak with high morbidity and
mortality,• ensuring effective community involvement and public awareness.



![[PPT]SURVEILANS DIFTERI - Universitas Dian Nuswantoro ...dinus.ac.id/repository/docs/ajar/SURVEILANS_PD3I.pptx · Web viewEPIDEMIOLOGI CAMPAK disebut measles penyakit yang sangat](https://static.fdocument.pub/doc/165x107/5b0473237f8b9a3c378da3c7/pptsurveilans-difteri-universitas-dian-nuswantoro-dinusacidrepositorydocsajarsurveilanspd3ipptxweb.jpg)