
Aula VIII – Corte · Aula VIII – Corte Prof. Eng. Diogo Pedriali Fevereiro de 2019 Rev. 01

Londrina 2015
PROGRAMA DE PÓS-GRADUAÇÃO STRICTO SENSU DOUTORADO EM ODONTOLOGIA
MARIA BEATRIZ BERGONSE PEREIRA PEDRIALI
ANÁLISE DA ASSOCIAÇÃO DOS POLIMORFISMOS NOS GENES IL1A, IL1B, IL6 E VDR COM A PERIODONTITE CRÔNICA EM IDOSOS COM E SEM OSTEOPOROSE

Londrina 2015
ANÁLISE DA ASSOCIAÇÃO DOS POLIMORFISMOS NOS GENES IL1A, IL1B, IL6 E VDR COM A PERIODONTITE CRÔNICA EM IDOSOS COM E SEM OSTEOPOROSE
Tese apresentada à UNOPAR, como requisito à obtenção do título de Doutora em Odontologia. Orientadora: Profª Drª Regina Célia Poli-Frederico.
MARIA BEATRIZ BERGONSE PEREIRA PEDRIALI
AUTORIZO A REPRODUÇÃO TOTAL OU PARCIAL DESTE TRABALHO, POR QUALQUER MEIO CONVENCIONAL OU ELETRÔNICO, PARA FINS DE ESTUDO E PESQUISA, DESDE QUE CITADA A FONTE.
Dados Internacionais de catalogação-na-publicação Universidade Norte do Paraná
Setor de Tratamento da Informação
Pedriali, Maria Beatriz Bergonse Pereira.
P41a Análise da associação dos polimorfismos nos genes IL1A, IL1B, IL6 e VDR com a periodontite crônica em idosos com e sem
osteorporose. / Maria Beatriz Bergonse Pereira Pedriali. Londrina:
[s.n], 2015 93f.
Tese (Doutorado em Odontologia). Universidade Norte do Paraná.
Orientador: Profª. Drª. Regina Célia Poli-Frederico
1 - Odontologia – tese de doutorado- UNOPAR 2- Osteoporose 3- Idosos 4- Interleucinas 5- Receptor de Vitamina D- I- Poli-
Frederico, Regina Célia; orient. II -Universidade Norte do Paraná.
CDU 616.314-089.27/.28
Londrina, 10 de julho de 2015.
BANCA EXAMINADORA
Profa Dra Orientadora Regina Celia Poli- Frederico
UNOPAR
Profa Dra Componente da Banca
Sandra Kiss Moura UNOPAR
Profa Dra Componente da Banca Jeane Eliete Laguila Visentainer
UEM
Profa Dra Componente da Banca
Sandra Mara Maciel UNOPAR
Profa Dra Componente da Banca
Solange de Paula Ramos UEL
MARIA BEATRIZ BERGONSE PEREIRA PEDRIALI
ANÁLISE DA ASSOCIAÇÃO DOS POLIMORFISMOS NOS GENES IL1A, IL1B, IL6 E VDR COM A PERIODONTITE CRÔNICA EM IDOSOS COM E SEM OSTEOPOROSE
Tese apresentada ao Programa de Pós-Graduação em Odontologia da Universidade Norte do Paraná - UNOPAR, como requisito à obtenção do título de Doutora em Odontologia. Área de Concentração: Dentística Preventiva e Restauradora.

À minha querida família pelo apoio
incondicional em todos os momentos,
principalmente nos de incerteza, sem vocês
nenhuma conquista valeria à pena.
AGRADECIMENTOS
Agradeço primeiramente a Deus por iluminar e guiar meus
caminhos, por me fortalecer e me fornecer a disposição necessária para a realização
deste sonho, pela inspiração de todos os momentos.
À minha amada família, Paulo Marcio, Leonardo e Lucas, pelo
carinho, incentivo, compreensão e encorajamento, durante todo este período.
Aos meus pais, Walter e Leniza, que são e sempre serão o alicerce
da minha educação moral, religiosa e profissional. Obrigada pelos incontáveis
conselhos e pelo constante apoio e incentivo.
À Profa. Dra. Regina Célia Poli-Frederico, muito orgulho tê-la
como minha orientadora, por toda dedicação, ensinamentos, incentivo, amizade e
fundamentalmente por ter acreditado na minha capacidade.
À toda equipe que integrou o projeto EELO (Estudo sobre
Envelhecimento e Longevidade) e aos idosos que participaram da pesquisa.
Ao Prof. Dr. Alcides Gonini Júnior, coordenador do Programa de
Pós-Graduação Stricto Senso em Odontologia, exemplo de liderança e competência.
Manifesto aqui minha gratidão a todos os professores, funcionários e
amigos do Programa de Pós-Graduação em Odontologia, pelo aprendizado ao longo
desses anos que muito contribuíram para minha formação docente.
Agradeço à Universidade Norte do Paraná e ao Programa de
Pós-Graduação Stricto Senso por me acolher como aluna e à Coordenação de
Aperfeiçoamento de Pessoal de Nível Superior (CAPES) pelo suporte financeiro.
Meus sinceros agradecimentos pela contribuição da banca do
exame de qualificação e agradeço a participação dos membros da banca
examinadora da defesa.
E a todos que de alguma forma estão próximos de mim que direta e
indiretamente contribuíram para a realização deste trabalho, meus agradecimentos.
PEDRIALI, Maria Beatriz Bergonse Pereira. Análise da associação dos polimorfismos nos genes IL1A, IL1B, IL6 e VDR com a periodontite crônica em idosos com e sem osteoporose. 85 f. [Tese de Doutorado]. Programa de Pós-Graduação em Odontologia – Universidade Norte do Paraná, Londrina, Londrina, 2015.
RESUMO
Até o momento, vários estudos relatam a associação da doença periodontal com a osteoporose e com polimorfismos genéticos, envolvidos com a densidade óssea mineral, tanto para a doença periodontal quanto para a osteoporose. Porém não existem estudos relacionando os polimorfismos genéticos comuns às duas condições. O objetivo deste estudo foi investigar a associação entre os polimorfismos da IL1A, IL1B, IL6 e VDR e a doença periodontal em idosos com e sem osteoporose. Idosos com 60 anos ou mais de idade, foram examinados clinicamente e a condição periodontal de cada indivíduo foi baseada na quantidade de perda de inserção periodontal (PIP), onde PIP ≤ 3 mm os indivíduos foram considerados saudáveis e PIP ≥ 4 mm foram considerados com periodontite. Todos os indivíduos realizaram o exame de densitometria óssea do fêmur e da coluna lombar (L1-L4) e foram classificados em três grupos: controle, osteopênicos e osteoporóticos. As amostras de DNA foram analisadas para o polimorfismo dos genes: IL1A C-889T, IL1B C+3954T, IL6 G-174C e entre os polimorfismos TaqI, BsmI, ApaI e FokI do gene VDR. Os dados foram analisados utilizando o teste do qui-quadrado, sendo estabelecido um intervalo de confiança de 95% e nível de significância de 5% (p˂0,05). O pacote de programas ARLEQUIN foi usado para calcular as frequências de haplótipos, equilíbrio de Hardy-Weinberg e desequilíbrio de ligação. Para análise de risco de alelos, genótipos e haplótipos o Odds Ratio, com intervalo de confiança de 95%, foi calculado. Houve uma associação significativa entre a frequência genotípica no gene IL1B +3954 em pacientes com osteoporose e com doença periodontal (p=0,02) sendo que 50% dos indivíduos portadores do genótipo CT apresentavam osteoporose e doença periodontal. Para o gene da IL6 -174, foi constatado que indivíduos com osteoporose e portadores do alelo G apresentam maior suscetibilidade à doença periodontal. 84,2% dos indivíduos portadores do genótipo GG apresentavam osteoporose e doença periodontal (p=0,04). O alelo C conferiu 25% de proteção aos indivíduos que abrigam este alelo em comparação aos que possuíam o alelo G. Pode-se verificar que indivíduos portadores do alelo G (genótipos GC e GG) apresentaram maiores níveis plasmáticos da IL-6 em comparação a indivíduos não portadores deste alelo (p=0,04). Os polimorfismos TaqI, BsmI, ApaI e FokI do gene VDR não mostraram diferença estatisticamente significativa entre os grupos controle e periodontite crônica, porém o haplótipo TBAF está associado com a prevalência da periodontite crônica (p=0,04). Podemos concluir, que o genótipo CT do polimorfismo genético da IL1B +3954 e o genótipo GG do polimorfismo genético da IL6 -174 está associado com o aumento da suscetibilidade à periodontite e à osteoporose. E o haplótipo TBAF construído a partir dos polimorfismos TaqI, BsmI, ApaI e FokI do gene VDR está associado com a prevalência da periodontite crônica em idosos Brasileiros.
Palavras-chave: Doença periodontal. Polimorfismo genético. Osteoporose. Idosos. Interleucinas. Receptor de Vitamina D.

PEDRIALI, Maria Beatriz Bergonse Pereira. Analysis of the association of gene polymorphisms in IL1A, IL1B, IL6 and VDR with chronic periodontitis in elderly patients with and without osteoporosis. 85 f. [Tese de Doutorado]. Programa de Pós-Graduação em Odontologia – Universidade Norte do Paraná, Londrina, 2015.
ABSTRACT
Until now, several studies reported an association between periodontal disease and osteoporosis and genetic polymorphisms involved in bone mineral density in both periodontal disease and osteoporosis. But there are no studies linking common genetic polymorphisms for the two conditions. This study investigates the association between IL1A, IL1B, IL6 and VDR polymorphisms and periodontal disease in elderly with or without osteoporosis. Seniors aged 60 and older, were examined clinically and periodontal condition of each individual was based on the amount of periodontal attachment loss, where PIP ≤ 3 mm were considered healthy and individuals with PIP ≥ 4 mm were considered with periodontitis . All subjects performed the examination of bone densitometry of femur and lumbar spine (L1-L4) and were classified into three groups: control, osteopenic and osteoporotic. The DNA samples were analyzed for the polymorphism of the gene: IL1A C-889T, IL1B C + 3954T, IL6 G-174C and TaqI, BsmI, ApaI and FokI VDR polymorphism. Data were analyzed using the chi-square test, and established a 95% confidence interval and a significance level of 5% (p˂0.05). The ARLEQUIN software package was used to calculate the haplotype frequencies, Hardy-Weinberg equilibrium and linkage disequilibrium. For analysis of risk alleles, genotypes and haplotypes the Odds Ratio, with 95% confidence interval, was calculated. There was a significant association between genotype frequency in IL1B +3954 gene in patients with osteoporosis and periodontal disease (p=0,02), and 50% of individuals with the CT genotype had osteoporosis and periodontal disease. For the IL6 -174 gene, it was found that individuals with osteoporosis and G allele carriers show higher susceptibility to periodontal disease. 84.2% of individuals with the GG genotype had osteoporosis and periodontal disease (p=0,04). The C allele conferred 25% protection to individuals carrying this allele compared to those who had the allele G. It can be seen that individuals with the G allele (GC and GG genotypes) had higher plasma levels of IL-6 compared to individuals not carrying this allele (p=0,04). The TaqI, BsmI, ApaI and FokI VDR polymorphisms showed no statistically significant difference between the control group and chronic periodontitis, but TBAF haplotype is associated with the prevalence of chronic periodontitis (p=0,04). We conclude that genotype CT of the IL1B +3954 and genotype GG of the IL6 -174 polymorphism is associated with an increased susceptibility to periodontal disease and osteoporosis. In addition, TBAF haplotype constructed from TaqI, BsmI, ApaI and FokI VDR polymorphisms is associated with the prevalence of chronic periodontitis in Brazilian elderly.
Keywords: Periodontal disease. Genetic polymorphism. Osteoporosis. Elderly. interleukin. Vitamin D receptor.

SUMÁRIO
1 INTRODUÇÃO .................................................................................................... 8
2 REVISÃO DE LITERATURA ............................................................................. 12
2.1 A DOENÇA PERIODONTAL .................................................................................... 12
2.2 DOENÇA PERIODONTAL E A OSTEOPOROSE .......................................................... 14
2.3 DOENÇA PERIODONTAL: POLIMORFISMOS DO GENE RECEPTOR DE VITAMINA D (VDR)
…………………………………………………………………………………..……..15
2.4 DOENÇA PERIODONTAL: POLIMORFISMOS DOS GENES CODIFICADORES DE CITOCINAS
………………………………………………………………………………………….20
3 PROPOSIÇÃO .................................................................................................. 26
3.1 PROPOSIÇÃO GERAL ........................................................................................... 26
3.2 PROPOSIÇÕES ESPECÍFICAS ................................................................................ 26
4 ARTICLE 1 ........................................................................................................ 27
5 ARTICLE 2 ........................................................................................................ 43
6 ARTICLE 3 ........................................................................................................ 58
7 CONCLUSÃO ................................................................................................... 74
REFERÊNCIAS ......................................................................................................... 76
ANEXOS ................................................................................................................... 83
ANEXO A - Parecer do Comitê de Ética em Pesquisa da UNOPAR .................... 84
ANEXO B – Ficha de exame – Condições bucais ................................................. 85

8
1 INTRODUÇÃO
O envelhecimento populacional caracteriza-se pela redução da
participação relativa de criança e jovens, acompanhada do aumento proporcional
dos adultos, particularmente, dos idosos e pode ser considerado um fenômeno
mundial visto o ritmo de crescimento mais elevado do grupo etário acima de 60 anos
quando comparado aos demais grupos, tanto em países desenvolvidos, quanto
naqueles em desenvolvimento.1,2 O crescimento da população idosa deve-se a
vários fatores, dentre eles, a diminuição da taxa de natalidade e fecundidade, o
avanço na ciência com consequente possibilidade de tratamento de doenças, em
particular, doenças infectocontagiosas, além da melhoria nas condições de vida
relacionadas ao saneamento básico e ao acesso aos serviços de saúde.1
Em se tratando da saúde bucal, a realidade atual revela situação
crítica que pode afetar a saúde geral e agravar a qualidade de vida dos idosos.3,4,5
Estudo sobre o impacto das condições bucais na qualidade de vida e no bem-estar
do indivíduo idoso revela que os aspectos funcionais, sociais e psicológicos são
significativamente afetados por uma condição bucal insatisfatória.6 Sendo, portanto,
a proteção e promoção da função mastigatória essencial para manter a qualidade de
vida física e social.7
Resultados dos levantamentos epidemiológicos, de abrangência
nacional, realizados pelo Ministério da Saúde, demonstraram ser grave o quadro
sanitário da saúde bucal em idosos. Os dados obtidos em 2002/2003 demonstraram
que na faixa etária de 65 a 74 anos, a média de dentes atacados pela cárie era de
27,8 dentes; que a percentagem de pessoas com algum problema periodontal, igual
a 92,1%; e que 75% dos idosos não possuíam nenhum dente funcional em pelo
menos uma arcada.8 Resultados preliminares do último levantamento, divulgados
em 2010, apontaram que mais de 3 milhões de idosos necessitam de prótese total
(nas duas arcadas dentárias) e que outros 4 milhões precisam usar prótese parcial
(em uma das arcadas).9
A destruição periodontal é uma experiência frequente entre os
idosos e contribui para a perda de, aproximadamente, um em cada cinco dentes
entre adultos em populações ocidentais.10,11,12,13 É relevante coletar e analisar dados
sobre a progressão da doença periodontal em pessoas idosas, a fim de identificar
aqueles que são propensos a perder os dentes.14

9
A doença periodontal é de etiologia multifatorial relacionada a um
processo inflamatório que leva à destruição dos tecidos de suporte dos dentes.15
Com o acúmulo de biofilme na superfície dental, as células do periodonto entram em
contato com produtos bacterianos e produzem citocinas pró-inflamatórias e outros
mediadores químicos da inflamação que iniciam a resposta inflamatória no interior
dos tecidos periodontais.16
As citocinas, tais como: interleucina-6 (IL-6) e o fator de necrose
tumoral alfa (TNF-α) são proteínas, secretadas por muitos tipos celulares, que agem
como mensageiras, iniciando e mantendo as respostas imunes e inflamatórias,
regulando o crescimento e diferenciação das células.17
Aspectos microbiológicos, imunogenéticos e ambientais estão
ligados ao início e à modulação da doença periodontal. Porém, a resposta aos
agentes etiológicos pode variar entre os indivíduos. Acredita-se que esta resposta
possa ser influenciada pelo perfil genético do indivíduo.18
Atualmente, o enfoque das pesquisas está na influência genética
sobre a doença periodontal crônica, na busca sobre o papel dos genes e na
identificação de polimorfismos genéticos que tenham relação com aspectos
imunológicos do hospedeiro, que poderiam ajudar a elucidar a patogênese e a
progressão da doença.19,20
Doenças com etiopatologia complexa, como a doença periodontal,
são poligênicas, ou seja, vários genes podem contribuir para a progressão e risco do
processo patológico. As variações genéticas poderiam atuar como fatores
modificadores da doença e polimorfismos nesses genes podem proteger o
hospedeiro ou contribuir para o desenvolvimento da doença. No caso da doença
periodontal, o papel dos genes que podem modificar seu curso ainda precisa ser
elucidado.21,22
Desta maneira, o estudo dos polimorfismos genéticos tem o
potencial de identificar as pessoas com maior ou menor predisposição à doença
periodontal, o que possibilitaria um ajuste individualizado da abordagem preventiva e
terapêutica, com resultados clínicos mais positivos e consequente redução da perda
dentária e dos impactos socioeconômicos.
Os polimorfismos genéticos podem ocorrer na região codificadora ou
na região promotora do gene, o que pode ocasionar modificações quantitativas ou
qualitativas da proteína codificada podendo resultar em alterações nas proteínas
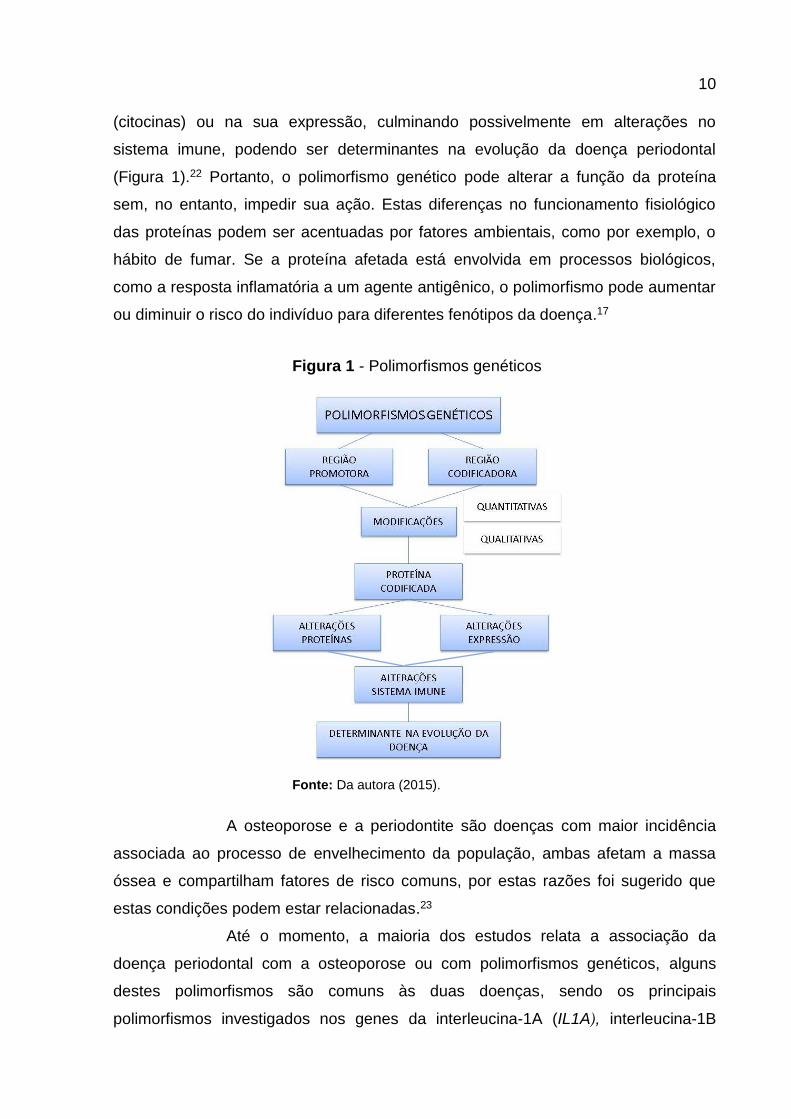
10
(citocinas) ou na sua expressão, culminando possivelmente em alterações no
sistema imune, podendo ser determinantes na evolução da doença periodontal
(Figura 1).22 Portanto, o polimorfismo genético pode alterar a função da proteína
sem, no entanto, impedir sua ação. Estas diferenças no funcionamento fisiológico
das proteínas podem ser acentuadas por fatores ambientais, como por exemplo, o
hábito de fumar. Se a proteína afetada está envolvida em processos biológicos,
como a resposta inflamatória a um agente antigênico, o polimorfismo pode aumentar
ou diminuir o risco do indivíduo para diferentes fenótipos da doença.17
Figura 1 - Polimorfismos genéticos
Fonte: Da autora (2015).
A osteoporose e a periodontite são doenças com maior incidência
associada ao processo de envelhecimento da população, ambas afetam a massa
óssea e compartilham fatores de risco comuns, por estas razões foi sugerido que
estas condições podem estar relacionadas.23
Até o momento, a maioria dos estudos relata a associação da
doença periodontal com a osteoporose ou com polimorfismos genéticos, alguns
destes polimorfismos são comuns às duas doenças, sendo os principais
polimorfismos investigados nos genes da interleucina-1A (IL1A), interleucina-1B

11
(IL1B), interleucina-6 (IL6) e receptor da vitamina D (VDR), envolvidos com a
densidade óssea mineral, tanto para a doença periodontal quanto para a
osteoporose, no entanto, não existem estudos relacionando as três condições
(doença periodontal, polimorfismos genéticos e a osteoporose).
12
2 REVISÃO DE LITERATURA
2.1 A DOENÇA PERIODONTAL
As doenças periodontais compreendem condições inflamatórias
crônicas e infecciosas provocadas pela interação entre os biofilmes supra e
subgengivais e a resposta inflamatória do hospedeiro. A presença do biofilme, os
próprios micro-organismos que o compõem, e metabólitos bacterianos produzidos
após colonização da área subgengival desencadeia uma resposta inflamatória. A
ativação do sistema imune do hospedeiro, principalmente para fins de proteção,
resulta em destruição dos tecidos, levando a síntese e liberação de citocinas,
mediadores pró-inflamatórios e metaloproteinases da matriz. A progressão e
gravidade da destruição periodontal causada pela periodontite depende do equilíbrio
entre a virulência do biofilme local e a resposta imune do hospedeiro.24
Portanto, a doença periodontal é uma infecção polimicrobiana
multifatorial, sendo considerada a manifestação patológica da resposta do
hospedeiro contra o desafio bacteriano do biofilme na interface dente / gengiva,
caracterizada pela inflamação e destruição dos tecidos de suporte do dente.25
Clinicamente, podem ser formadas bolsas periodontais, ocorrer reabsorção do osso
alveolar e eventual perda do elemento dental.26,27
Embora as bactérias sejam, sem dúvida, a principal causa da lesão
inflamatória inicial, evidências indicam ser mais provável a resposta do hospedeiro
às bactérias que leva às alterações teciduais observadas tanto na gengivite quanto
na periodontite. Assim, parece que é a resposta inflamatória e imune do hospedeiro,
e não uma bactéria específica ou seus fatores de virulência, que determinará o
desenvolvimento e a progressão da periodontite.24,28
As fases do desenvolvimento da doença periodontal são
denominadas de lesão inicial, precoce e estabelecida. Foi observado que a lesão já
estabelecida poderia permanecer inativa e não progredir a menos que algum outro
fator desconhecido interfira na delicada relação micro-organismo-hospedeiro
direcionando para uma maior destruição de tecidos e para o desenvolvimento da
lesão avançada, já demonstrando indícios que a resposta inflamatória e imunológica
descontrolada impulsiona a destruição dos tecidos.27,29

13
A inflamação pode causar destruição do periodonto marginal via dois
mecanismos: pela ação direta dos subprodutos do metabolismo e enzimas
bacterianas; ou estimulando a liberação de mediadores inflamatórios de células do
hospedeiro. Embora a infecção por periodontopatógenos seja essencial para o início
da doença periodontal, sua mera presença na cavidade oral não é suficiente para
explicar diferenças na severidade da doença entre indivíduos.30
O caráter multifatorial da doença periodontal sofre influência de
fatores de risco sistêmicos (diabetes, obesidade, estresse, osteopenia, osteoporose
e consumo inadequado de cálcio e vitamina D), ambientais (tabagismo), bem como
fatores genéticos e comportamentais, tais como a higiene oral. Ressalta-se que a
eliminação ou modificação desses fatores de risco deve fazer parte do tratamento da
doença periodontal. Embora fatores genéticos ou raciais não possam ser alterados,
a identificação de pessoas em risco de resultados adversos por raça ou composição
genética poderia direcionar as intervenções preventivas e terapêuticas.26,31-36
O conceito de fatores de risco e mecanismos envolvidos no início e
progressão da periodontite se desenvolveu drasticamente nas últimas décadas, de
uma visão simplista de micro-organismos diretamente causando os sinais e
sintomas clínicos da periodontite, para a compreensão da importância do sistema
imunológico e da resposta inflamatória do hospedeiro, sendo influenciada por fatores
genéticos e ambientais.24,37
A presença de um fator de risco implica em um aumento direto da
probabilidade de ocorrência de uma doença, e, se um fator de risco está ausente ou
for removido, observa-se uma redução na probabilidade de que a mesma ocorra.38
Há um crescente reconhecimento de que a variabilidade
interindividual da resposta imune se desenvolve como uma consequência de
interações entre o hospedeiro, ambiente e microbiota dando origem a um fenótipo
clínico específico. Sendo assim, este fenômeno representa uma reação biológica
única para cada indivíduo.39 Portanto, cada pessoa tem uma resposta individual ao
desafio bacteriano que determina sua suscetibilidade a doenças, incluindo a
periodontite.40
A inflamação periodontal envolve vários estágios caracterizando a
resposta imune inata. Este processo é controlado por vários genes ou genes
modificadores da doença, que codificam proteínas de natureza diferente (como,
enzimas e citocinas). Devido a variações genéticas (por exemplo, polimorfismos

14
genéticos), a imunidade inata pode ser mais ou menos grave, resultando em perda
óssea imprevisível.39 Atualmente, os pesquisadores têm se concentrado na
identificação de polimorfismos genéticos em vários aspectos da imunidade do
hospedeiro.22
2.2 DOENÇA PERIODONTAL E A OSTEOPOROSE
Estudos têm chamado a atenção para o possível vínculo entre
osteoporose e doença periodontal.41,23 Periodontite e a osteopenia podem ter
agentes etiológicos comuns que podem influenciar diretamente ou modular ambos
os processos de doença.38,42-44 Esta relação surgiu a partir do fato de que ambas as
condições envolvem a perda óssea e podem compartilhar caminhos patológicos
comuns. No entanto, enquanto a osteoporose é uma doença óssea metabólica, a
periodontite é uma doença inflamatória, elas diferem em sua patogênese, mas
compartilham fatores de risco comuns que podem explicar a associação proposta
entre as duas condições.36
A suposição de um risco aumentado de doença periodontal na
presença de osteoporose é baseada na hipótese de que a osteoporose resulta em
perda de densidade mineral óssea em todo o corpo, incluindo a maxila e a
mandíbula. A baixa densidade óssea leva a um aumento da porosidade alveolar, um
padrão trabecular alterado e uma reabsorção óssea alveolar mais rápida após
infecção com patógenos periodontais. Outra explicação é derivada do fato de fatores
sistêmicos que afetam a remodelação óssea podem também modificar a resposta
tecidual local contra uma infecção periodontal, pelo aumento da liberação sistêmica
de citocinas inflamatórias como a IL-1 e IL-6.36
Uma revisão de literatura sobre a relação da osteopenia com a
perda óssea alveolar e a doença periodontal concluiu que a gravidade da osteopenia
está relacionada com a perda da altura da crista óssea alveolar e perda dental em
mulheres na pós-menopausa.45
Um outro estudo investigou se mulheres com osteoporose têm um
aumento da gravidade e extensão da doença periodontal. Trezentas e oitenta
mulheres com idade entre 45-65 anos, com radiografias recentes da coluna vertebral
e do fêmur proximal concordaram em realizar um exame periodontal que incluía
parâmetros de sangramento à sondagem, profundidade de bolsa periodontal,

15
recessão e presença de cálculo. O resultado do estudo concluiu que não houve
associação entre a presença de doença periodontal grave e osteoporose.46
Com objetivo de determinar se a osteoporose alveolar é uma
manifestação local de uma perda óssea sistêmica, com etiologia e fatores de risco
semelhantes, ou um processo independente, dependendo principalmente dos
fatores que causam a periodontite, foi realizada uma revisão sistemática de ensaios
clínicos avaliando a relação entre osteoporose e periodontite.23 A maioria dos
estudos sugeriu uma relação entre a osteoporose e a periodontite, porém a
demonstração dessa relação é complexa, pois são doenças multifatoriais e ambas
compartilham de mecanismos comuns. Assim, existe uma plausibilidade biológica
que sugere que pelo menos parte da destruição periodontal é influenciada pela
perda de massa óssea sistêmica. A maioria dos estudos demonstrou que a
periodontite é um sinal precoce de osteoporose e poderia ser utilizada como uma
ferramenta de rastreamento para identificar indivíduos com alto risco de osteoporose
o que os beneficiaria com medidas preventivas ou terapêuticas. Na prática, este é
um tema controverso, provavelmente devido aos diversos critérios utilizados para
definir a osteoporose e a periodontite na literatura.23 Portanto, os pesquisadores
concluem que existe evidência de uma associação, porém mais estudos controlados
com parâmetros clínicos padronizados de osso a nível sistêmico e doença
periodontal são necessários para melhor elucidar a inter-relação entre a perda óssea
sistêmica e a alveolar, e determinar definitivamente se a osteoporose é um fator de
risco para a doença periodontal e, em caso afirmativo, que medida contribui para o
risco global de doença periodontal.23,35
2.3 DOENÇA PERIODONTAL: POLIMORFISMOS DO GENE RECEPTOR DE VITAMINA D (VDR)
Alguns estudos relataram que a vitamina D possui importante papel
regulatório no metabolismo ósseo,47,48 especialmente na regulação do metabolismo
do cálcio e do fósforo, e ainda no sistema imunológico. A função biológica da
vitamina D está associada com o seu receptor sendo evidente que as variações no
gene receptor da vitamina D (VDR) podem ter profundo efeito sobre o metabolismo
mineral e sobre a densidade mineral óssea (DMO).49,50
Esta vitamina pode ser obtida a partir da ingestão de alguns
alimentos, como peixes e frutos do mar, e suplementos alimentares, porém a síntese
16
cutânea é sua maior fonte, produzida sob estimulação da exposição adequada à
radiação solar ultravioleta B (UVB).51
A vitamina D absorvida no intestino delgado é transportada por
proteínas até o fígado e os rins onde é metabolizada em sua forma ativa, sendo que
somente uma pequena fração é encontrada livre.52 Os níveis plasmáticos de
paratormônio (PTH), cálcio e fósforo, regulam a produção de vitamina D e sua
principal ação é manter os níveis normais de cálcio e fosfato no plasma. Quando
ocorre diminuição desses níveis, o PTH juntamente com a vitamina D ativa,
estimulam a atividade de diferenciação de pré osteoclastos em osteoclastos
maduros, acelerando assim a reabsorção óssea, aumentando os níveis plasmáticos
desses íons. A vitamina D também tem função na mineralização óssea. Quando em
contato com o VDR, promove um feedback negativo, fazendo com que haja menor
liberação de PTH,53,54 como também promove a síntese de RNAm para formação de
proteínas como a osteocalcina que atua na formação óssea pelos osteoblastos.55
O gene VDR está localizado no cromossomo 12, na posição q13.1 e
possui cerca de 100kb e 9 éxons.55 Os polimorfismos do gene VDR e alterações nas
vias sinalizadoras mediadas por VDR podem levar a diferentes efeitos celulares
importantes na ativação de genes, tais como o aumento / diminuição da transcrição,
metabolismo do cálcio, proliferação celular e resposta imunológica.56
Adicionalmente, os polimorfismos neste gene são comumente presentes e foram
associados com a osteoporose.57
Entre os polimorfismos do gene VDR mais estudados, estão os de
nucleotídeos únicos (SNPs): rs1544410I (BsmI), rs7975232 (ApaI), rs731236 (TaqI)
e rs2228570 (FokI).58-60
Polimorfismos são alterações genéticas decorrentes da substituição,
deleção ou inserção de bases nitrogenadas, alterando a sequência de DNA.61
Polimorfismos de um gene ocupando um sítio cromossômico específico (locus) são
chamados alelos. Dois ou mais alelos para um dado locus podem existir na natureza
ao longo da evolução, mas também podem ocorrer a qualquer momento.22 São
herdados pela linhagem germinativa e um polimorfismo genético é caracterizado
pela ocorrência de, pelo menos, dois alelos em um locus, quando o alelo mais raro
ocorre em pelo menos 1% na população.61,62 Estas alterações quando envolvem
somente um nucleotídeo são denominadas de polimorfismo de nucleotídeos únicos
(SNPs) gerando ou não sítios de clivagem para o reconhecimento de enzimas de

17
restrição.61,63 SNPs ocorrem com mais frequência do que qualquer outro tipo de
polimorfismo genético e podem não ter nenhum efeito ou podem promover efeitos
biológicos importantes.22
Os polimorfismos genéticos provavelmente existem em muitos, se
não na maioria dos genes de mediadores inflamatórios e imunes. No entanto, é
provável que: 1) nem todos os polimorfismos conferem suscetibilidade diferencial
aos aspectos destrutivos da doença; 2) certo número de genes serão identificados
como importantes a este respeito; e 3) conhecimento de que estes podem permitir a
determinação do risco individual para muitos indivíduos. A chave será identificar os
polimorfismos que são importantes o suficiente para dar risco significativo de
doença.64
A maioria dos polimorfismos do gene VDR está localizada em
regiões regulatórias, podendo modular a expressão gênica, mas não mudanças
estruturais na sequência de aminoácidos das proteínas codificadas. 65
Há evidências que a deficiência de vitamina D pode colocar
indivíduos em risco, não só para a baixa densidade mineral óssea, mas também em
outras vias metabólicas, tais como aquelas envolvidas na resposta imune, doenças
inflamatórias crônicas e câncer.66 No entanto, não há estudos que demonstrem o
papel que a deficiência de vitamina D pode ter na etiopatogenia da doença
periodontal, como a periodontite. É precisamente por causa de seus efeitos sobre o
metabolismo ósseo, que a vitamina D pode ter um papel fundamental na prática
odontológica.56
O polimorfismo rs1544410 (BsmI) está localizado no intron 8 e
resulta na substituição de adenina por guanina (A/G). Conforme a nomenclatura, é
definido como alelo “B” a presença da base adenina e como alelo “b” a presença da
base guanina. O polimorfismo rs7975232 (ApaI) também está localizado no intron 8
e resulta na substituição de timina por guanina (T/G). A nomenclatura define como
alelo “A” presença da base timina e “a” presença da base guanina. O polimorfismo
rs731236 (TaqI) está localizado no éxon 9 e resulta na substituição de timina por
citosina (C/T), sendo definido como “T” presença da base timina e “t” presença da
base citosina. O polimorfismo rs2228570 (FokI) está localizado na junção do intron 1
com o éxon 2, resultante da substituição de citosina por timina (C/T) e é definido
como “F” quando há presença da base citosina e “f” quando há presença da base
timina.67,68
18
O polimorfismo TaqI gera a troca do códon ATT por ATC, porém não
altera o aminoácido a ser sintetizado, pois ambos os códons sintetizam a isoleucina,
considerado portanto um polimorfismo silencioso.68
Devido ao fato dos polimorfismos BsmI, ApaI e TaqI estarem
localizados próximos a região 3’ não traduzida (3’UTR) surge a hipótese de que a
forma alterada do receptor pode influenciar a estabilidade de transcrição, no entanto
há uma lacuna no conhecimento sobre prováveis efeitos na transcrição do gene ou
na estrutura da proteína.69 Ressalta-se que, o final 3’UTR dos genes é conhecido
por estar envolvido na regulação da expressão gênica, especialmente por meio da
regulação da estabilidade do RNAm. Especula-se que o haplótipo BAt para os
polimorfismos citados acima, apresente um RNAm mais estável e com uma meia-
vida maior. Desta forma, resultaria em aumento no número de VDR presentes em
células-alvo e, assim fornecendo a essas células uma melhor resposta à vitamina D.
70
A presença do alelo f gera uma versão mais longa da proteína com 3
aminoácidos a mais quando comparada com a presença do alelo F. Estudos
demonstram que a proteína mais longa possui menor atividade transcricional quando
comparada à proteína curta, podendo resultar em diminuição da funcionalidade do
VDR, modificando assim o efeito determinado pela vitamina D.67
Alguns estudos se concentram na análise do polimorfismo do gene
VDR Taql, a fim de avaliar a possível associação desse polimorfismo e um aumento
da suscetibilidade individual para o desenvolvimento da periodontite associada com
a perda de osso alveolar. Em particular, o genótipo TT e a presença do alelo T estão
associados com a doença periodontal crônica em pacientes japoneses, chineses e
caucasianos.71,72 Esses dados também estão de acordo com estudo realizado por
Martelli et al.73 que mostrou uma forte correlação entre o genótipo TT de indivíduos
italianos e periodontite crônica, mas também com a doença periodontal agressiva.
Em um estudo transversal, Borges et al.74 examinaram a relação
entre o polimorfismo do VDR TaqI e a microbiota subgengival em adultos brasileiros
com periodontite crônica, mostrando uma associação do genótipo TT com a doença
sem observar qualquer associação entre o genótipo e o componente bacteriano.
Além disso, a deficiência de vitamina D provoca uma diminuição da
densidade mineral óssea a nível esquelético, incluindo a maxila e a mandíbula, com
um aumento da porosidade alveolar e reabsorção mais rápida do osso alveolar,
19
após a invasão de patógenos periodontais. Essas evidências podem explicar a maior
suscetibilidade à periodontite quando os pacientes apresentam genótipo TT,
levantando a hipótese de uma resposta do hospedeiro mais difícil a bactérias
periodontopatogênicas e uma perda óssea acentuada. Em contradição, os estudos
de Hennig et al.75 e Sun et al.57 encontraram uma associação entre o alelo t (alelo
raro) com um risco aumentado de desenvolver a doença periodontal agressiva em
indivíduos Caucasianos e Chineses, respectivamente.
Um estudo mostrou que o suplemento de cálcio e de vitamina D
utilizados para prevenir ou tratar a osteoporose ainda parece ter efeito benéfico
sobre a retenção de dentes.76 Mais recentemente, Miley et al.77 mostraram, em um
estudo randomizado controlado de 5 anos, que indivíduos que tomaram cálcio e
vitamina D perderam menos dentes do que os indivíduos do grupo controle.
Uma vez que a reabsorção de osso alveolar é uma das principais
características da doença periodontal, é possível especular que os mediadores do
metabolismo ósseo como o VDR e seus polimorfismos genéticos desempenham um
papel na determinação da suscetibilidade individual para o desenvolvimento da
periodontite. Por estas razões, o gene VDR pode ser considerado um candidato
interessante para a investigação na prática periodontal, isoladamente ou em
combinação com outros marcadores de inflamação, e a suplementação de vitamina
D pode representar uma forma simples de regular a perda óssea na doença
periodontal.56
A prática odontológica pode ter um papel importante na detecção
precoce da osteoporose. Com o advento de novas técnicas de diagnóstico de
triagem genética, é possível o dentista especialista identificar pacientes com doença
periodontal com a densidade mineral óssea diminuída e, assim, encaminhar o
paciente para uma avaliação da densidade mineral óssea. Pacientes com doença
periodontal também diagnosticados com osteopenia / osteoporose devem ser
tratados clinicamente de forma mais agressiva para eliminar os patógenos
periodontais, devido aos riscos adicionais. Eventualmente, o dentista pode
encaminhar o paciente para um endocrinologista para avaliar abordagens
farmacológicas, como suplementos de vitamina D normais ou drogas mais
específicas, como bisfosfonatos, calcitonina além de modificações no estilo de
vida.56
A conscientização dos cirurgiões-dentistas da forte relação entre a

20
densidade óssea do esqueleto e a saúde periodontal, também permite uma melhor
colaboração dos pacientes na terapia periodontal, percebendo os periodontistas ou a
equipe odontológica como participantes ativos na promoção da saúde geral dos
pacientes.56
2.4 DOENÇA PERIODONTAL: POLIMORFISMOS DOS GENES CODIFICADORES DE CITOCINAS
Tem se observado grande interesse da comunidade científica
internacional sobre o papel que os fatores genéticos podem desempenhar na
doença periodontal e como os resultados seriam aplicados no prognóstico da
doença.34 Uma linha de pesquisa atual tem sido à busca de fatores de risco
genéticos e marcadores, com alta sensibilidade e especificidade que poderia ser
usado para identificar indivíduos com risco à periodontite.36
Os polimorfismos, preferencialmente investigados, são aqueles
presentes em genes que participam da resposta imune do hospedeiro, da
sinalização intracelular ou das vias enzimáticas de degradação tecidual. Nota-se
uma tendência mundial em identificar marcadores genéticos de suscetibilidade não
só à doença periodontal, mas a doenças importantes como câncer, diabetes,
doenças inflamatórias e auto-imunes, como artrite, asma, lúpus eritematoso
sistêmico, entre outras.34
Citocinas são proteínas solúveis de baixo peso molecular que agem
como mensageiras, transmitindo sinais para outras células, e desta forma, atuam
como reguladores positivos e negativos das respostas imunológica e inflamatória e
da resposta de reparo do hospedeiro a lesões.78
A resposta inflamatória local nas periodontopatias é iniciada por
fatores de virulência bacterianos, como os lipopolissacarídeos.79 Estes fatores
estimulam e amplificam a produção de várias citocinas pró-inflamatórias, dentre elas
as interleucinas. Os mediadores inflamatórios possuem primordialmente papel
protetor contra patógenos, mas podem induzir respostas imunes altamente
destrutivas quando há alterações na concentração de citocinas e estimulação de
receptores. A resposta inflamatória aumentada na doença periodontal eleva os
níveis de citocinas, o que pode levar à severa perda de inserção e reabsorção
óssea.80
É aceito que o sistema imune desempenha um papel importante na

21
patogênese da periodontite, pois a maioria dos genes que são considerados
responsáveis pelo desenvolvimento de periodontite estão também relacionados à
resposta imune. Estes incluem os genes que afetam a expressão da IL-1, IL-6, TNF-
, IL-10, E-selectinas, receptor de Fc-gama, CD14, receptores Toll-like e VDR.36
Os primeiros polimorfismos investigados na doença periodontal
foram nos genes que formam o “cluster” ou agrupamento da IL1 (IL1A, IL1B, IL1RN),
além do gene do fator de necrose tumoral-alfa (TNF). Diferenças individuais nos
níveis de interleucina relacionados aos diferentes graus de suscetibilidade à doença
periodontal são atribuídas a polimorfismos nos genes de citocinas.34
A IL-1B pode ter participação na patogênese da periodontite, devido
à suas propriedades pró-inflamatórias e de estimulação à reabsorção óssea (Figura
2). A frequência dos genótipos, incluindo o alelo 2 da IL1B +3953, está
significantemente aumentada em pacientes com periodontite crônica severa
comparado com aqueles com doença em estágios iniciais, sugerindo que o alelo 2
está correlacionado com um aumento na produção da IL-1B, predispondo o
indivíduo a um aumento da gravidade da doença periodontal. Embora este
mecanismo seja incerto, o alelo 2 da IL1B +3953 pode atuar de forma independente
ou interagir epistaticamente com um suposto gene da doença para promover o
desenvolvimento da forma mais grave da periodontite crônica nos casos onde
existem outros fatores de risco para a doença.81
Figura 2 - Propriedades da Interleucina-1
Fonte: Da autora (2015).

22
Determinados polimorfismos no “cluster” da IL1 estão relacionados à
doença periodontal em diferentes populações. Alguns alelos desses polimorfismos
mostraram-se raros em algumas populações e prevalentes em outras, ou seja,
apresentaram frequências alélicas diferentes em populações distintas. Portanto,
apesar da importância da IL-1 na resposta imune do indivíduo, deve-se ter cautela
ao utilizar seus polimorfismos como marcadores genéticos da doença periodontal.34
Polimorfismos genéticos na IL1 foram associados com um aumento
nos níveis de mediadores inflamatórios e várias doenças inflamatórias, como a
doença periodontal. Os polimorfismos genéticos da IL1A (-889), IL1A (+4845), e
IL1B (+3954) foram associados com a periodontite crônica em caucasianos. Uma
revisão sistemática e meta-análise foram conduzidas por Karimbux et al.82 na
tentativa de esclarecer se variações genéticas na IL1 estão associadas com
fenótipos clínicos bem definidos de periodontite crônica em pacientes brancos. A
meta-análise encontrou efeitos significativos para duas variações genéticas
individuais, IL1A (odds ratio = 1.48), IL1B (odds ratio = 1.54) e por um genótipo
composto que combina os alelos raros em cada locus (odds ratio = 1.51).
Concluíram que variações genéticas nos genes IL1A e IL1B contribuem
significativamente para a periodontite crônica em caucasianos.
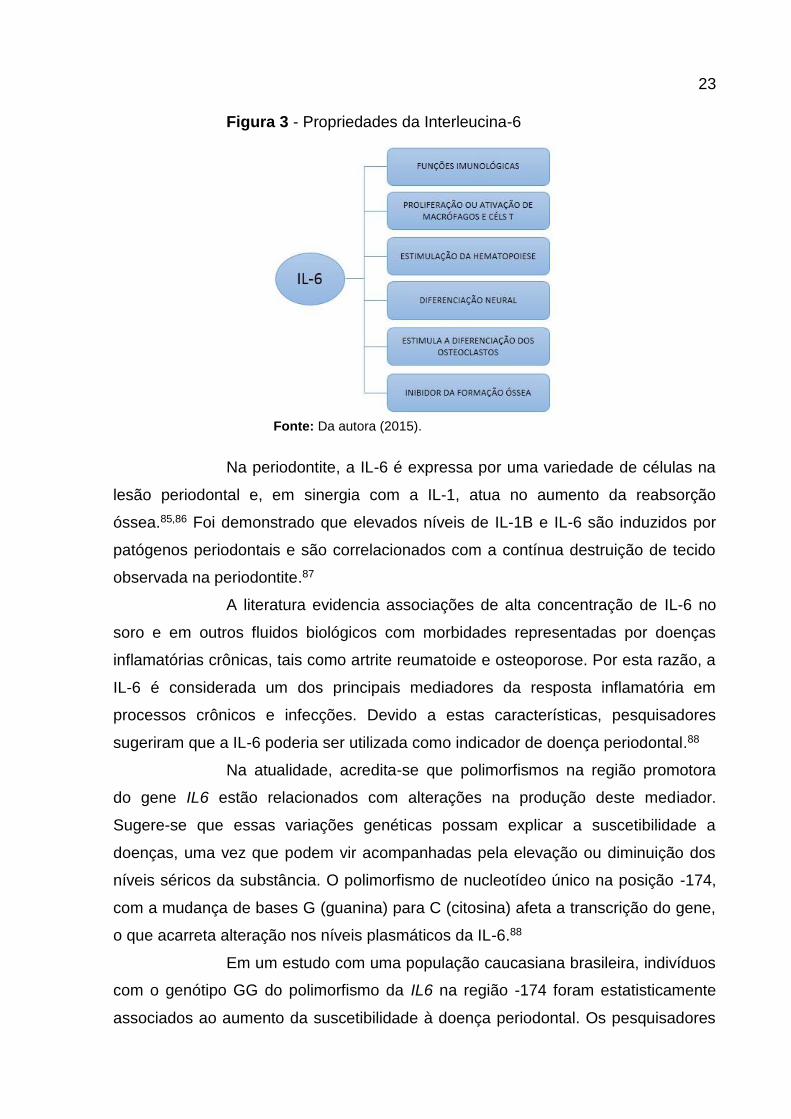
A IL-6 é bastante investigada por apresentar funções imunológicas
importantes, como, estimular a diferenciação ou maturação de células da linhagem B
a secretarem imunoglobulinas. Tem importante papel na proliferação ou ativação de
macrófagos e células T, estimulação da hematopoiese; diferenciação neural,83
estimulador da diferenciação dos osteoclastos e inibidor da formação óssea (Figura
3).78,84
23
Figura 3 - Propriedades da Interleucina-6
Fonte: Da autora (2015).
Na periodontite, a IL-6 é expressa por uma variedade de células na
lesão periodontal e, em sinergia com a IL-1, atua no aumento da reabsorção
óssea.85,86 Foi demonstrado que elevados níveis de IL-1B e IL-6 são induzidos por
patógenos periodontais e são correlacionados com a contínua destruição de tecido
observada na periodontite.87
A literatura evidencia associações de alta concentração de IL-6 no
soro e em outros fluidos biológicos com morbidades representadas por doenças
inflamatórias crônicas, tais como artrite reumatoide e osteoporose. Por esta razão, a
IL-6 é considerada um dos principais mediadores da resposta inflamatória em
processos crônicos e infecções. Devido a estas características, pesquisadores
sugeriram que a IL-6 poderia ser utilizada como indicador de doença periodontal.88
Na atualidade, acredita-se que polimorfismos na região promotora
do gene IL6 estão relacionados com alterações na produção deste mediador.
Sugere-se que essas variações genéticas possam explicar a suscetibilidade a
doenças, uma vez que podem vir acompanhadas pela elevação ou diminuição dos
níveis séricos da substância. O polimorfismo de nucleotídeo único na posição -174,
com a mudança de bases G (guanina) para C (citosina) afeta a transcrição do gene,
o que acarreta alteração nos níveis plasmáticos da IL-6.88
Em um estudo com uma população caucasiana brasileira, indivíduos
com o genótipo GG do polimorfismo da IL6 na região -174 foram estatisticamente
associados ao aumento da suscetibilidade à doença periodontal. Os pesquisadores
24
acreditam que a presença do alelo raro C confere fator de proteção contra a
progressão da doença, já que resulta em menor expressão da IL-6 após estímulo da
resposta inflamatória.88
Resultados similares foram encontrados por Tervonen et al.80, que
evidenciaram uma relação entre sinais clínicos da doença periodontal e a presença
de polimorfismo no gene da IL6 na posição -174, considerando o genótipo
homozigoto GG.
Análogo a outras doenças complexas, foi estimado que para
periodontite, entre 10 e 20 genes modificadores da doença podem estar envolvidos.
No entanto, é importante perceber que o número e o tipo de genes modificadores da
doença para a mesma condição podem não ser iguais para diferentes populações
étnicas e eles também são influenciados por fatores ambientais.22
Uma extensa revisão de polimorfismos genéticos na periodontite
crônica foi realizada por Laine et al.20 que analisaram estudos para os polimorfismos
no cluster da IL1; no cluster do TNF; nos genes IL4 e IL4RA; nos genes IL6 e IL6R;
nos genes IL10; nos genes FcR; nos genes VDR; nos genes de receptores de
reconhecimento de padrões, tais como CD14; e uma série de genes diversos. Muitas
vezes, as associações encontradas são restritas a grupos raciais ou étnicos
específicos. No geral, as evidências apontam para polimorfismos nos genes IL1, IL6,
IL10, VDR e CD14 desempenhando um papel na periodontite crônica, mas a maioria
destas associações é restrita a determinadas populações. Os pesquisadores
concluíram que não existe ainda nenhum polimorfismo genético que foi
definitivamente demonstrado ser um fator de risco para a suscetibilidade à
periodontite crônica em uma população amplamente representativa.
É importante identificar o maior número possível de polimorfismos
genéticos e suas frequências nas populações em todo o mundo para que se possa
atribuir a um determinado polimorfismo, com segurança, uma porcentagem de
suscetibilidade ou severidade à doença. Somente no futuro, e baseado no
conhecimento das frequências dos alelos nas populações, é que um determinado
polimorfismo poderia ser utilizado como marcador genético da doença periodontal.34
Além de conseguir uma melhor compreensão do processo da doença, tais
polimorfismos podem ser usados como marcadores de diagnóstico ou de
prognóstico.89
A correlação destes polimorfismos genéticos com características
25
fenotípicas estáveis de grupos de pacientes com periodontite pode levar à
identificação de biomarcadores moleculares para serem incorporados em perfis de
riscos individuais, além de ajudar a definir as bases para o desenvolvimento de
novas estratégias de tratamento, permitindo aos profissionais personalizar o
tratamento adequadamente.64,90,91
Informações do DNA combinadas com informações clínicas se
tornam uma necessidade para o tratamento periodontal altamente individualizado.
No futuro, pode ser possível usar essas informações para ajustar a resposta do
hospedeiro à infecção microbiana, inibindo ao máximo o micro-organismo e
minimizando os danos inflamatórios.39,92
É importante saber a biologia por trás dos procedimentos, visto que
o papel do cirurgião-dentista já não se limita a ser apenas cuidador, deve-se tentar
compreender as características biológicas de cada paciente que ditam a progressão
da doença para destinar um tratamento de forma eficiente, para que o resultado
clínico possa ser previsto, gerenciando posteriormente melhor os pacientes.39 De
acordo com Kim et al.34, poderia ser confeccionado um “kit”, talvez adaptado para
uma determinada população, para detectar indivíduos com genótipo de alto risco
para a doença, auxiliando desta forma na prevenção da doença periodontal.
Razzouk e Termechi (2013) mencionaram o termo terapia
periodontal individualizada como o próximo conceito de tratamento para um
resultado clínico avançado.39 Até o momento, estudos genéticos de associação de
doenças estimam que haja centenas de genes associados com a periodontite.
Todos esses recursos têm facilitado a compreensão da inflamação na tentativa de
estratificar pacientes de acordo com o risco para uma doença e tornaram-se
necessárias para programar a medicina periodontal individualizada podendo ser
vista como terapia sob medida com base nas interações entre fatores genéticos,
clínicos e ambientais que afetam um indivíduo.91
Portanto, é imperativo que o cirurgião-dentista olhe além da
cavidade oral, para fatores que potencialmente favorecem uma alteração, a fim de
ajudar os pacientes a alcançar o objetivo comum de prevenção ou tratamento da
doença periodontal, e assim, possivelmente, melhorar a saúde de forma geral.35
26
3 PROPOSIÇÃO
3.1 PROPOSIÇÃO GERAL
Investigar a associação entre polimorfismos dos genes IL1A, IL1B,
IL6 e VDR e a doença periodontal, em idosos fisicamente independentes com e sem
osteoporose, cadastrados nas Unidades Básicas de Saúde do município de
Londrina, Pr.
3.2 PROPOSIÇÕES ESPECÍFICAS
- Determinar a prevalência e gravidade da doença periodontal
em idosos com e sem osteoporose fisicamente
independentes;
- Verificar as frequências alélicas e genotípicas de
polimorfismos nos genes IL1A, IL1B, IL6 e VDR na
população de estudo;
- Avaliar a associação entre os polimorfismos desses genes e
a doença periodontal em idosos com e sem osteoporose.

27
4 ARTICLE 1
ANALYSIS OF THE ASSOCIATION BETWEEN POLYMORPHISMS IN THE IL1
GENE, PERIODONTITIS AND OSTEOPOROSIS IN ELDERLY INDIVIDUALS IN
BRAZIL
(Submitted to the “Archives of Oral Biology”)
Running title: Genetic, osteoporosis and periodontitis
M. B. B. P. Pedriali1, S. K. Moura1, S. M. Maciel1, R.C. Poli-Frederico2
1 Department of Restorative Dentistry, Faculty of Dentistry, Norte do Paraná University, Londrina, PR, Brazil 2 MS, PhD, Department of Genetics and Molecular Biology, Faculty of Dentistry, Norte do Paraná University, Londrina, PR, Brazil
CORRESPONDING AUTHOR Regina Célia Poli-Frederico. Universidade Norte do Paraná, Faculdade de Odontologia. Rua Marselha 183, Jardim Piza, Londrina, Pr, Brasil. Cep 86041-120. Phone: +55-43-3371-7820 Fax: +55-43-3371-7741. email: [email protected]

28
Abstract
Objective: Polymorphisms in the IL1 gene have an important role in the pathogenesis of periodontal disease, may cause both quantitative and qualitative changes in the coded protein, and may result in alteration to the proteins or in its expression possibly culminating in alterations to the immune system. This study aimed to investigate the prevalence of the polymorphism in the IL1A -889 and IL1B +3954 genes, as well as their association with periodontal disease, in a sample of Brazilians elderly with and without osteoporosis. Design: A sample of 145 individuals was grouped according to the presence of periodontal disease and the presence of osteopenia or osteoporosis. DNA was extracted from blood, and PCR-RFLP was used to identify the polymorphism: IL1A C-889T (rs1800587) and IL-1B C+3954T (rs1143634). Differences in the genotype/allele frequencies were evaluated using the Chi-squared test (p<0.05). For the risk analysis of the alleles, genotypes and haplotypes, the Odds Ratio (OR) was calculated, with 95% confidence intervals. Results: In the group with periodontal disease, no significant difference was observed in the distribution of the genotypes between patients without osteoporosis and patients with osteopenia and osteoporosis for the IL1A -889 polymorphism. A significant association between the genotypic frequency in the IL1B gene in patients with osteoporosis in the group with periodontal disease where 50% of individuals with the CT genotype had osteoporosis and periodontal disease. Conclusion: Genotype CT of IL1B +3954 polymorphism may be a risk factor for periodontal disease and osteoporosis in a sample of elderly Brazilians.
Keywords: Periodontal disease, genetic polymorphism, osteoporosis, elderly,
interleukin.

29
Introduction
Periodontal disease has a multifactorial etiology related to an inflammatory
process that leads to the destruction of the tooth’s supporting tissue, being regarded
as the pathological manifestation of the host’s response to the bacterial challenge of
the biofilm at the tooth/gum interface (Bodet, Chandad, & Grenier, 2006; Sanz & Van
Winkelhoff, 2011). With the buildup of biofilm on the tooth surface, the cells of the
periodontium come into contact with bacterial products and produce proinflammatory
cytokines, including interleukins and other chemical mediators of inflammation that
initiate inflammatory response inside the periodontal tissue
(Liljenberg, Lindhe, Berglundh, Dahlén, & Jonsson, 1994). Basically, these cytokines
have the role of protecting against pathogens, but they may become highly
destructive when the concentration of these mediators is altered (Tervonen, Raunio,
Knuuttila, & Karttunen, 2007).
Interleukin-1 (IL-1) is an important inflammatory mediator in a variety of
chronic diseases. This cytokine is an activator of the first chemotactic cytokines, as
well as of the expression of adhesion molecules which facilitate the migration of
leukocytes into the tissue (Moreira et al., 2005). It is a protein which appears in two
main forms, alpha (IL-1A) and beta (IL-1B), and is produced by various cell types
such as macrophages, monocytes, polymorphonuclear leukocytes, fibroblasts,
epithelial and endothelial cells and also osteoblasts, in response to bacterial antigens
(Grigoriadou, Koutayas, Madianos, & Strub, 2010; Graves & Cochran, 2003). Studies
have suggested that IL-1 plays a role in the initiation and progression of periodontitis,
relating it to the degradation of the extracellular and bone matrix of the periodontal
tissue. Indeed high levels of IL-1B in the tissue and gingival fluid is associated with
periodontitis (Kinane, Shiba, & Hart, 2005). IL-1 is also known for being a stimulator
of osteoclastic activity in bone resorption (Lang et al., 2000). IL-1, therefore, is a
proinflammatory cytokine that is intimately connected with all inflammatory reactions,
as well as the immune or healing response and any uncontrolled variation in its level
may have far-reaching consequences, not limited to periodontal disease (Kinane,
Shiba, & Hart, 2005). Therefore, polymorphisms in the IL1 gene must have an
important role in the pathogenesis of periodontal disease as these genetic alterations
may cause both, quantitative and qualitative changes in the coded protein and may
result in alteration to the proteins (cytokines) or in its expression, possibly culminating

30
in alterations to the immune system and may be determinants in the evolution of
periodontal disease (Loos, John, & Laine, 2005).
The genetic polymorphism in position -889 of the IL1A gene is related to the
substitution of cytosine with thymine (C/T), and the presence of the allele T is
associated with an almost fourfold increase in the expression of the protein IL-1A
(Shirodaria, Smith, McKay, Kennett, & Hughes, 2000). Moreover, the genetic
polymorphism at position (+3954) of gene IL1B is associated with an increased
production of this cytokine (Moreira et al., 2005). The genotype frequency, including
allele T of IL1B +3954, is significantly higher in patients with severe, chronic
periodontitis when compared to those in the early stages of the disease, suggesting
that the allele T is related to an increase in the production of IL-1B, predisposing the
individual to a greater severity of periodontal disease (Gore, Sandrers, Pandey,
Palesch, & Galbraith, 1998).
It should be pointed out that studies have called attention to the possible link
between osteoporosis and periodontal disease (Martínez-Maestre, González-Cejudo,
Machuca, Torrejón, & Castelo-Branco, 2010). The supposition of increased risk of
periodontal disease in the presence of osteoporosis is based on the assumption that
osteoporosis results in a loss of bone density throughout the whole body, including
the maxilla and mandibular. Low bone density leads to an increase in alveolar
porosity, an altered trabecular pattern and faster alveolar bone resorption after
infection with periodontal pathogens. Another explanation derives from the fact that
systemic factors such as increased release of IL-1 and IL-6 affecting bone
metabolism may also modify the local tissue response to a periodontal infection
(Stabholz, Soskolne, & Shapira, 2010).
Up to now, the majority of studies have related periodontal disease to
osteoporosis or genetic polymorphisms, as well as the association of osteoporosis
and genetic polymorphisms in different populations. Amongst the main
polymorphisms that have been investigated are those of the genes of IL1A and IL1B,
involving bone density, for both periodontal disease and osteoporosis, though there
have been no studies relating the three conditions (periodontal disease, genetic
polymorphisms and osteoporosis). Therefore, the aim of this study is to investigate
the prevalence of the polymorphism in the IL1A -889 and IL1B +3954 genes, as well
as their association with periodontal disease, in a sample of elderly Brazilians with
and without osteoporosis.

31
Materials and methods
Selection of individuals
A sample of individuals aged 60 or above, from both sexes, was selected for
the study based on a cross-sectional study on Aging and Longevity (EELO Project)
conducted at the Norte do Paraná University, Londrina/Paraná, Brazil (approved by
the UNOPAR Research Ethics Committee, PP0070/09). Of the 323 elderly who
comply with the inclusion criteria, 42 were not found, 28 declined, 9 died and 99 were
edentulous. Thus, the present study sample consisted of 145 elderly who agreed to
take the examination of bone densitometry. The patients hail from the southern
region of Brazil and all participants signed the Free and Informed Consent Form.
Eligibility criteria were as follows: aged 60 years and over, of both genders,
who were living independently and classified at level 3 or 4 as proposed by Spirduso
(2005). This classification evaluates the independence level of the elderly, with level
1 indicating a lack of self-mobility and level 5 indicating athletes. Elderly people who
had any illness (other than osteoporosis) or limitation that would prevent the testing,
such as physical or mental disabilities were excluded from the sample.
The diagnosis and classification of periodontal disease were carried out by
way of a physical examination that included an analysis of clinical parameters and
medical and dental histories. The oral cavity was divided into sextants and was
performed the examination of the indexes teeth: 16:17; 11; 26 and 27; 36 and 37; 31;
46 and 47. A sextant was only examined if there were two or more teeth present. In
the absence of indexes teeth, all the remaining teeth that sextant were examined.
The clinical parameters included periodontal probing and the evaluation of clinical
attachment loss (CAL). The CAL were recorded at six points around each tooth.
The periodontal condition of each individual was based on the quantity of
clinical attachment loss. Individuals with CAL ≤ 3 mm were regarded as healthy and
those with a CAL ≥ 4 mm were considered to be suffering from periodontitis.
All the individuals underwent a bone densitometry examination of the femur
and lumbar spine (L1-L4) using a dual-energy densitometer (GE-PRODIGY PRIMO;
X-ray; fan beam). The individuals were sorted into three groups: control (above -1.0
Sd), osteopenic (-1.0 to -2.5 Sd) and osteoporotic (below -2.5 Sd), observing criteria
advocated by the World Health Organization (WHO).

32
Collection and extraction of DNA
Peripheral blood specimens were collected in 6% Ethylenediaminetetraacetic
acid vacuum tubes. The extraction of the DNA was performed using the PureLink
Genomic DNA Kit (Invitrogen, Foster City, USA), in accordance with the
manufacturer’s instructions. The extracted DNA was stored in a freezer at -80ºC
before polymorphism analyses.
The evaluation of DNA quality and quantity was carried out by analyzing
absorbance in a spectrophotometer (NanoDrop 2000 – Thermo Scientific, USA) at
260 nm and 280 nm. Subsequently the DNA was diluted in Milli-Q® ultrapure water
for a final concentration of 100 ng/µL.
Identification of genetic polymorphisms
PCR-RFLP conditions for the gene IL1A C-889T (rs1800587)
The primers used in the PCR to amplify the samples of genomic DNA were
as follows: 5’-AAGCTTGTTCTACCACCTGAACTAGGC-3’ (forward) and 5’-
TTACATATGAGCCTTCCATG-3’ (reverse) (Nicklin, Weith, & Duff, 1994). The PCR
mixture consisted of a final volume of 50 L containing 75 mM Tris-HCl, 20 mM
(NH4)2SO4, 1.5 mM of MgCl2, 0.2 mM of dNTPs, 20 ρM of each primer, 1 U of Taq
DNA polymerase (Invitrogen) and 2 L of DNA solution. The amplification conditions
consisted of 94ºC for 30s, followed by 45 cycles of 94ºC for 30s, 56ºC for 35s and
72ºC for 30s. After amplification, 10 L of the PCR product were analyzed by
electrophoresis in agarose gel (1%). The gel was then stained using SYBR Safe
(Invitrogen) and the synthesized fragments were viewed under ultraviolet light. The
size of the product amplified by PCR was estimated based on the electrophoretic
migration of the product in relation to the 100 bp DNA Ladder marker (Invitrogen).
For the polymorphism IL1A, 5 U of the Ncol restriction enzyme were used and the
products of digestion obtained were: allele C (83 + 16 bp) and allele T (99 bp). The
product of digestion was viewed via polyacrylamide gel electrophoresis at 10%
stained by silver nitrate.

33
PCR conditions for gene IL1B C+3954T (rs1143634)
The primers used in the PCR to amplify the samples of genomic DNA were
as follows: 5’-CTCAGGTGTCCTCGAAGAAATCAAA-3’ (forward) and 5’-
GCTTTTTTGCTGTGAGTCCCG-3’ (reverse) (Kaarthikeyan et al., 2009). The PCR
mixture consisted of a final volume of 50 L containing 75 mM Tris-HCl, 20 mM
(NH4)2SO4, 5 mM of MgCl2, 0.2 mM of dNTPs, 20 ρM of each primer, 0.4 L of Taq
DNA polymerase (Invitrogen) and 2 L of DNA solution. The amplification conditions
consisted of 94ºC for 30s, followed by 35 cycles of 94ºC for 30s, 55ºC for 35s and
72ºC for 30s. After amplification, 10 L of the PCR product were analyzed by
electrophoresis in agarose gel (2%). The gel was then stained using SYBR Safe
(Invitrogen) and the synthesized fragments were viewed under ultraviolet light. The
size of the product amplified by PCR was estimated based on the electrophoretic
migration of the product in relation to the 100 bp DNA Ladder marker (Invitrogen).
For the polymorphism IL1B, 5 U of the TaqI restriction enzyme were used and the
products of digestion obtained were: allele C (97 + 85 + 12 bp) and allele T (182 + 12
bp). The product of digestion was viewed via polyacrylamide gel electrophoresis at
10% stained by silver nitrate.
Statistical analysis
The differences in the genotypic and allelic frequencies (categorical
variables) were evaluated using the chi-squared test (X2), with Yates correction or
Fisher’s exact test. The differences were deemed to be significant when p <0.05. The
physical proximity of the polymorphisms explains the simultaneous analysis of the
haplotypes. The ARLEQUIN 3.0 (Arlequin, Switzerland) suite of programs was used
to calculate haplotype frequencies, Hardy-Weinberg equilibrium and disequilibrium of
linkage. . The statistical analysis was performed using the application BioStat 2.0 for
Windows (AnalystSoft, Canada), SPSS 10.0 for Windows (SPSS Inc., Chicago, IL),
and the ARLEQUIN 3.0 statistical package (Arlequin, Switzerland).
34
Results
The demographic distribution, genotypic and allelic frequencies of the IL1A
and IL1B genes, periodontal disease and bone mineral density (BMD) of the elderly
individuals are displayed in Table 1.
The mean age of the elderly individuals was 67.95 (± 5.047) years, with a
predominance of ethnic whites (62.1%) and those who have never smoked (58.6%).
A total of 58.6% of the sample were carriers of the CT genotype for the IL1A gene
and 55.2% harbored the CC genotype of the IL1B gene. The majority of the elderly
presented with periodontitis (64.1%) but did not have osteoporosis (56.6%).
The frequency distribution of the genotypes and alleles for the
polymorphisms in the IL1A -889 and IL1B +3954 genes, according to the presence or
absence of periodontal disease in individuals with or without osteoporosis, is
displayed in Table 2.
In the group with periodontal disease, no statistically significant difference
was observed in the distribution of the genotypes between patients without
osteoporosis, patients with osteopenia and patients with osteoporosis for the
polymorphism in the IL1A -889 gene (p=0.22), nor was any statistically significant
association observed between the frequency of alleles for the same polymorphism
(p= 0.39).
There was a significant association between the genotypic frequency in the
IL1B +3954 gene in patients with osteoporosis in the group with periodontal disease
(2= 11.764; p= 0.02). A total of 50% of individuals who were carriers of the CT
genotype presented with osteoporosis and periodontal disease, while 60% of those
elderly individuals harboring the CC genotype were found to be free of osteoporosis.
No significant association was observed, however, between allelic frequency,
periodontal disease and osteoporosis (p= 0.71).
In the group with periodontal disease, there was no significant association in
the haplotype frequency consisting of at least one allele T of the IL1A -889 gene and
an allele T of the IL1B +3954 gene, between patients with periodontal disease and
without OP and those with OPE or OP (p= 0.91).

35
Discussion
Although bacteria are indubitably the prime cause of initial inflammatory
lesion, current evidence suggests that it is the host’s inflammatory and immune
response that will determine the development and progression of periodontitis
(Bartold & Van Dyke, 2013; Page & Kornman, 1997). Therefore, microbiological,
immunogenic and environmental aspects are linked to the onset and modulation of
periodontal disease. The response to the etiological agents may vary between
individuals and it is believed that this response may be influenced by the individual’s
genetic profile (Kinane, Shiba, & Hart, 2005).
Periodontal disease can be associated with many systemic diseases.
Osteoporosis or the reduction in BMD in osteopenia could be a risk factor for alveolar
bone loss resulting in an accelerated progression of bone resorption faced with
infection by oral biofilm and the host’s immune response. Infection by periodontal
pathogenic bacteria leads to the local production of proinflammatory cytokines that
raise the levels of systemic cytokines which aggravate even more the loss of skeletal
bone density (Reddy & Morgan, 2013). These cytokines act like messages
transmitting signals to other cells, acting as positive and negative regulators of the
immune and inflammatory responses and the host’s repair response to lesions
(Oppenheim, Ruscetti, & Faltynek, 1992).
IL-1 is a powerful immune mediator with proinflammatory properties,
stimulating the expression of chemokines and the production of other inflammatory
mediators such as PGE2, contributing to the inflammation, increasing the formation
and activity of the osteoclasts, leading to bone resorption, inducing the expression of
matrix metalloproteinases contributing to a degradation of the conjunctive tissue and
also stimulating the apoptosis of matrix-producing cells limiting repair to the
periodontium (Graves & Cochran, 2003).
Polymorphisms in the IL1 gene were associated with an increase in the
levels of inflammatory mediators in several inflammatory diseases, including
periodontal disease (Karimbux et al., 2012), and may modulate the transcription of
the gene or the production of protein (Loos, John, & Laine, 2005; Pociot, Mølvig,
Wogensen, Worsaae, & Nerup, 1992). The majority of the studies suggest that the
rare allele of a polymorphism in the promoting region results in an increase in gene
expression and, consequently, in high protein levels (Loos, John, & Laine, 2005).

36
In this study, the association was investigated between genetic
polymorphism in IL1A -889 and IL1B +3954, with periodontitis in the elderly, with or
without osteoporosis. Previous studies conducted on the Brazilian population
demonstrated a positive association between the polymorphism in the IL1A -889 and
chronic periodontitis with a high incidence of allele T in the group of individuals with
chronic periodontitis (Moreira, Costa, Gomez, Gollob, & Dutra, 2007). In this study
into individuals with periodontal disease, however, we found no significant difference
in the distribution of genotypes between patients without osteoporosis and patients
with osteopenia and osteoporosis in the polymorphism of the IL1A -889 gene, nor did
we observe a difference in the frequency of the alleles for this polymorphism.
We found a significant association between genotypic frequency in the IL1B
+3954 in patients with osteoporosis and with periodontal disease, where 50% of
individuals carrying the CT genotype presented with osteoporosis and periodontal
disease, corroborating the results of another study with a sample of the Brazilian
population, suggesting that the polymorphism in the IL1B +3954 gene could be a risk
factor for chronic periodontitis (Moreira et al., 2005). In the present study, however, in
individuals with periodontal disease, no difference was observed in haplotype
frequency between patients without osteoporosis and those with osteopenia or
osteoporosis.
A systematic review conducted by Martínez-Maestre, González-Cejudo,
Machuca, Torrejón, & Castelo-Branco (2010) concluded that the majority of studies
suggest a relationship between osteoporosis and periodontitis, however the proof of
this relationship is complex since they are multifactorial diseases and both share
common mechanisms, however there is a biological plausibility that suggests that at
least a part of the periodontal destruction is influenced by the loss of systemic bone
mass and the majority of studies tend to show that periodontitis is an early indicator
of osteoporosis. Therefore, periodontitis could be used as a tracking tool for
identifying individuals with a high risk of developing osteoporosis, which would
benefit them in terms of the preventive or therapeutic measures (Martínez-Maestre,
González-Cejudo, Machuca, Torrejón, & Castelo-Branco, 2010). In contrast, results
of a cross-sectional study established no association between the presence of
serious periodontal disease and osteoporosis (Marjanovic et al., 2013). However, at
the present time, there are no studies that simultaneously relate periodontal disease,
osteoporosis and genetic polymorphism in the IL1, the present study being the first

37
such account thereof.
A number of studies have stated that dentists have a prime role in the early
diagnosis of osteoporosis, through the opportunity to evaluate the patient via dental
x-rays, seeing that it is a routine procedure in clinical practice for the diagnosis and
treatment of dental and periodontal diseases, that are particularly frequent in the
same population affected by osteoporosis, providing clues as to strategies for early
prevention and/or treatment (Guiglia et al., 2013). Therefore, the complete patient
history should include clinical information as well as a medical history and the
environmental factors combined with information on DNA (genomic profile) and
bacterial profile, in order to arrive at a highly personalized periodontal treatment
(Razzouk & Termechi, 2013).
Conclusion
In the present study, we did not observe an association between the
genotype frequency in the IL1B +3954 gene in patients with osteoporosis in the
group with periodontal disease. Thus, genotype CT of IL1B +3954 polymorphism
may be a risk factor for periodontal disease and osteoporosis in a sample of elderly
Brazilians.

38
References Bartold, P. M., & Van Dyke, T. E. (2013). Periodontitis: a host-mediated disruption of
microbial homeostasis. Unlearning learned concepts. Periodontol 2000, 62, 203-217.
Bodet, C., Chandad, F., & Grenier, D. (2006). Porphyromonas gingivalis-induced inflammatory mediator profile in an ex vivo human whole blood model. Clin Exp Immuno,143, 50-57.
Gore, E. A., Sandrers, J. J., Pandey, J. P., Palesch, Y., & Galbraith, G. M. P. (1998). Interleukine-1beta +3953 allele 2: association with disease status in adult periodontitis. J Clin Periodontol, 25, 781-785.
Graves, D. T., & Cochran, D. (2003). The contribution of interleukin-1 and tumor necrosis factor to periodontal tissue destruction. J Periodontol, 74, 391-401.
Grigoriadou, M. E., Koutayas, S-O., Madianos, P. N., & Strub, J-R. (2010). Interleukin-1 as a genetic marker for periodontitis: Review of the literature. Quintessence International, 41, 517-525.
Guiglia, R., Di-Fede, O., Lo-Russo, L., Sprini, D., Rini, G-B., & Campisi, G. (2013). Osteoporosis, jawbones and periodontal disease. Med Oral Patol Oral Cir Bucal, 18, e93–e99.
Kaarthikeyan, G., Jayakumar, N. D., Padmalatha, O., Sheeja, V., Sankari, M., & Anandan, B. (2009). Analysis of the association between interleukin-1beta (+3954) gene polymorphism and chronic periodontitis in a sample of the south Indian population. Indian J Dent Res, 20, 37-40.
Karimbux, N. Y., Saraiya, V., Elangovan, S., Allareddy, V., Kinnunen, T., Kornman, K. S., & Duff, G. W. (2012). Interleukin-1 gene polymorphisms and chronic periodontitis in adult whites: a systematic review and meta-analysis. J Periodontol, 83, 1407-1419.
Kinane, D. F., Shiba, H., & Hart, T. C. (2005). The genetic basis of periodontitis. Periodontol 2000, 39, 91-117.
Lang, N. P., Tonetti, M. S., Suter, J., Sorrell, J., Duff, G. W., & Kornman, K. S. (2000). Effect of interleukin 1 polymorphisms on gengival inflammation assessed by bleeding on probing in a periodontal maintenance population. J Periodontal Res, 35, 102-107.
Liljenberg, B., Lindhe, J., Berglundh, T., Dahlén, G., & Jonsson, R. (1994). Some microbiological, histopathological and immunohistochemical characteristics of progressive periodontal disease. J Clin Periodontol, 21, 720-727.
Loos, B. G., John, R. P., & Laine, M. L. (2005). Identification of genetic risk factors for periodontitis and possible mechanisms of action. J Clin Periodontol, 32,159-179.

39
Marjanovic, E. J., Southern, H. N., Coates, P., Adams, J. E., Walsh, T., Horner, K., & Devlin, H. (2013). Do patients with osteoporosis have an increased prevalence of periodontal disease? A cross-sectional study. Osteoporos Int, 24, 973-979.
Martínez-Maestre, M. Á., González-Cejudo, C., Machuca, G., Torrejón, R., & Castelo-Branco, C. (2010). Periodontitis and osteoporosis: a systematic review. Climacteric, 13, 523-529.
Moreira, P. R., De Sá, A. R., Xavier, G. M., Costa, J. E., Gomez, R. S., Gollob, K. J., & Dutra, W. O. (2005). A functional interleukin-1b gene polymorphism is associated with chronic periodontitis in a sample of Brazilian individuals. J Periodontol Res, 40, 3006-3011.
Moreira, P. R., Costa, J. E., Gomez, R. S., Gollob, K. J., & Dutra, W. O. (2007). The Il1a (-889) gene polymorphism is associated with chronic periodontal disease in a sample of Brazilian individuals. J Periodontal Res, 42, 23-30.
Nicklin, M. J., Weith, A., & Duff, G. W. (1994). A physical map of the region encompassing the human interleukin-1 alpha, interleukin-1 beta, and interleukin-1 receptor antagonist genes. Genomics, 15, 382-384.
Oppenheim, J. J., Ruscetti, F. W., & Faltynek, C. (1992). Citocinas. In: Stites DP, Terr AL, editors. Imunologia básica. Rio de Janeiro: Prentice-Hall.
Page, R. C., & Kornman, K. S. (1997). The pathogenesis of human periodontitis: an introduction. Periodontol 2000, 14, 9-11.
Pociot, F., Mølvig, J., Wogensen, L., Worsaae, H., & Nerup, J. (1992). TaqI polymorphism in the human interleukin-1β (IL-1β) gene correlates with IL-1β secretion in vitro. Eur J Clin Invest, 22, 396-402.
Razzouk, S., & Termechi, O. (2013). Host Genome, Epigenome, and Oral Microbiome Interactions: Toward Personalized Periodontal Therapy. J Periodontol, 84, 266-271.
Reddy, M. S., & Morgan, S. L. (2013). Decreased bone mineral density and periodontal management. Periodontol 2000, 61, 195-218.
Sanz, M., & Van Winkelhoff, A. J. (2011). Periodontal infections: understanding the complexity – Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol, 38, 3-6.
Shirodaria, S., Smith, J., McKay, I. J., Kennett, C. N., & Hughes, F. J. (2000). Polymorphisms in the IL- 1A gene are correlated with levels of interleukin 1 alpha protein in gingival crevicular fluid of teeth with severe periodontal disease. J Dent Res, 79, 1864-1869.
Spirduso, W. W. (2005). Dimensões físicas do envelhecimento. Barueri: Manole.

40
Stabholz, A., Soskolne, W. A., & Shapira, L. (2010). Genetic and environmental risk factors for chronic periodontitis and aggressive periodontitis. Periodontol 2000, 53, 138-153.
Tervonen, T., Raunio, T., Knuuttila, M., & Karttunen, R. (2007). Polymorphisms in the CD14 and IL-6 genes associated with periodontal disease. J Clin Periodontol, 34, 377-383.

41
Table 1 – Demographic distribution, genotypic frequency IL1A and IL1B, periodontal disease and BMD in the elderly (n = 145).
CHARACTERISTICS
n %
Gender Male 65 44.8% Female
80 55.2%
Age Mean (±Sd)
67.95 (± 5.047)
Ethnic group White 90 62.1% Non white
55 37.9%
Smoking habit Never smoked 85 58.6% Ex-smoker 46 31.7% Current smoker
14 9.7%
Genotypic frequency IL1A CC 45 31.0% CT 85 58.6% TT
15 10.3%
Genotypic frequency IL1B CC 80 55.2% CT 40 27.6% TT
25 17.2%
Periodontal disease Healthy 52 35.9% Periodontitis
93 64.1%
BMD Without osteoporosis 82 56.6% With osteopenia 45 31.0% With osteoporosis
18 12.4%

42
Table 2 - Frequency distribution of the genotypes and alleles for polymorphisms in genes IL1A -889 and IL1B +3954, in accordance with the presence or absence of periodontal disease in individuals with or without osteoporosis.
PERIODONTAL
DISEASE
FREQUENCY
WITHOUT
OSTEOPOROSIS n (%)
WITH
OSTEOPENIA n (%)
WITH
OSTEOPOROSIS n (%)
Chi-
squared
VALUE of
P
GENOTYPIC
HEALTHY
IL1A -889 CC 6 (20.7%) 8 (42.1%) 2 (50.0%) 5.134 0.27 CT 20 (69.0%) 8 (42.1%) 1 (25.0%) TT
ALLELIC C T
3 (10.3%)
32 (52.4%) 26 (60.4%)
3 (15.8%)
24 (39.3%) 14 (32.5%)
1 (25.0%)
5 (8.3%) 3 (7.1%)
0.657
0.72
GENOTYPIC IL1B +3954
CC 14 (48.3%) 12 (63.2%) 2 (50.0%) 3.175 0.53 CT 8 (27.6%) 3 (15.8%) 2 (50.0%) TT
ALLELIC C T
7 (24.1%)
32 (49.2%) 22 (62.8%)
4 (21.1%)
27 (41.5%) 11 (31.4%)
0 (0.0%)
6 (9.3%) 2 (5.8%)
1.746
0.41
GENOTYPIC
PERIODONTITIS
IL1A -889 CC 17 (32.1%) 7 (26.9%) 5 (35.7%) 5.660 0.22 CT 33 (62.3%) 14 (53.8%) 9 (64.3%) TT
ALLELIC C T
3 (5.7%)
67 (58.8%) 39 (54.2%)
5 (19.2%)
28 (24.6%) 24 (33.3%)
0 (0.0%)
19 (16.6%) 9 (12.5%)
1.888
0.39
GENOTYPIC IL1B +3954
CC 32 (60.4%) 14 (53.8%) 6 (42.9%) 11.764 0.02 CT 9 (17.0%) 11 (42.3%) 7 (50.0%) TT
ALLELIC C T
12 (22.6%)
73 (55.7%) 33 (60.0%)
1 (3.8%)
39 (29.8%) 13 (23.6%)
1 (7.1%)
19 (14.5%) 9 (16.4%)
0.735
0.71

43
5 ARTICLE 2
ASSOCIATION BETWEEN THE POLYMORPHISM IN THE IL6 GENE,
PERIODONTITIS AND OSTEOPOROSIS IN ELDERLY BRAZILIANS
(Submitted to the “Journal of Periodontal Research”)
M. B. B. P. Pedriali1, S. K. Moura1, S. M. Maciel1, R.C. Poli-Frederico2
1 Department of Restorative Dentistry, Faculty of Dentistry, Norte do Paraná University, Londrina, PR, Brazil 2 MS, PhD, Department of Genetics and Molecular Biology, Faculty of Dentistry, Norte do Paraná University, Londrina, PR, Brazil
Running Title: Genetic, Osteoporosis and Periodontitis
CORRESPONDING AUTHOR Regina Célia Poli-Frederico. Universidade Norte do Paraná, Faculdade de Odontologia. Rua Marselha 183, Jardim Piza, Londrina, Pr, Brasil. Cep 86041-120. Phone: +55-43-3371-7820 Fax: +55-43-3371-7741. email: [email protected]
Keywords: Periodontal disease, genetic polymorphism, osteoporosis,
interleukin-6
44
Abstract
Background: Interleukin-6 (IL6) is considered to be one of the principal inflammatory response mediators in chronic processes and could be used as an indicator of periodontal disease. Osteoporosis and periodontitis are diseases that are frequently part of an individual’s aging process, both of which affect bone mass and share common risk factors. Objective: This study aimed to investigate the prevalence of the IL6 -174 polymorphism, and its association with periodontal disease, in a sample of elderly Brazilians, with and without osteoporosis. Material and Methods: A sample of 191 individuals was grouped according to the presence of periodontal disease and the presence of osteopenia or osteoporosis. DNA was obtained from blood, and PCR-RFLP was used to identify the IL6 -174 polymorphism. The serological quantification of IL-6 was carried out using ELISA kits. Differences in the genotype/allele frequencies were evaluated using the Chi-squared test (p<0.05). To evaluate the differences in genotypic frequencies between the case and control groups, the odds ratio (OR) was calculated, with 95% confidence intervals. Results: Individuals with osteoporosis and carriers of the G allele are more susceptible to periodontal disease. The C allele afforded 25% protection to individuals who harbor this allele compared with those that had the G allele. Individuals who are carriers of the G allele (genotypes GC and GG) had higher IL-6 plasma levels. Conclusion: Genotype GG of the IL6 -174 polymorphism is associated with an increased susceptibility to periodontal disease and osteoporosis, suggesting that the C allele may afford a factor of protection against the development of periodontal disease and osteoporosis.

45
Introduction
Periodontal disease is a multifactorial, polymicrobial infection and is
considered to be the pathological manifestation of the host’s response to the
bacterial challenge of biofilm at the tooth/gum interface. The periodontitis is
characterized by a chronic inflammation caused by specific bacteria that activate the
host’s immune system in the periodontal tissue, leading to the destruction of the
connective tissue and supporting alveolar bone (1,2). The destruction of the
periodontium is caused by the direct action of bacterial enzymes and the release of
the inflammatory mediators that activate inflammatory cells to degrade extracellular
matriz (3).
Osteoporosis and periodontitis are diseases that are frequently part of an
individual’s aging process. Both affect bone mass and share common risk factors.
For these reasons, it has been suggested that these conditions may be related (4).
Osteoporosis is a common disease amongst the elderly, characterized by
low bone mineral density, deterioration of the bone microarchitecture and greater
susceptibility to non-traumatic fractures (5). It is deemed to be the result of the
interaction of genetic and environmental factors. Certain genes that codify for
cytokines like interleukin 1 (IL1), interleukin 6 (IL6) and tumor necrosis factor alpha
(TNFα), are capable of regulating the bone turnover and remodeling (6).
Polymorphisms in these genes are known to be involved in bone mineral density
(BMD) and the development of osteoporosis (5).
The biological basis for the association of polymorphisms of the genes that
codify for cytokines and periodontal disease is that the presence of certain alleles are
related to an increase in the production of a particular cytokine (7) suggesting that
these genetic variations could explain the susceptibility to diseases, as they could be
accompanied by an increase or decrease in the substance’s serum levels. The
single-nucleotide polymorphism in the promoter region of the IL6 gene at position -
174, with the base change from G (guanine) to C (cytosine) affects the transcription
of the gene, which leads to an alteration in the IL-6 plasma levels, and the presence
of the rare C allele is related to a lower IL-6 expression following the inflammatory
stimulus, reducing susceptibility to periodontal disease (8). For this polymorphism,
the CC genotype is associated with a reduced risk of developing osteoporosis when
compared to the GG genotype in Caucasian subjects (5).
46
Considering a possible role of IL6 polymorphisms in the development of
periodontitis and osteoporosis, the aim of this study is to investigate the prevalence
of the IL6 -174 genetic polymorphism, as well as its association with periodontal
disease, in a sample of elderly Brazilians, with and without osteoporosis.
Materials and methods
Selection of individuals
A sample of 191 individuals aged 60 or above, from both sexes, was
selected for the study based on a cross-sectional study on Aging and Longevity
(EELO Project) conducted at the Norte do Paraná University (approved by the
UNOPAR Research Ethics Committee, record no. PP0070/09). The patients hail from
the southern region of Brazil and all participants signed the Free and Informed
Consent Form.
Eligibility criteria were as follows: aged 60 years and over, of both genders,
who were living independently and classified at level 3 or 4 as proposed by Spirduso
(9). This classification evaluates the independence level of the elderly, with level 1
indicating a lack of self-mobility and level 5 indicating athletes. Elderly people who
had any illness (other than osteoporosis) or limitation that would prevent the testing,
such as physical or mental disabilities were excluded from the sample.
The diagnosis and classification of the periodontal disease were carried out
by way of a physical examination that included an analysis of clinical parameters and
medical and dental histories. The oral cavity was divided into sextants and was
performed the examination of the indexes teeth: 16:17; 11; 26 and 27; 36 and 37; 31;
46 and 47. A sextant was only examined if there were two or more teeth present. In
the absence of indexes teeth, all the remaining teeth that sextant were examined.
The clinical parameters included periodontal probing, presence or absence of
bleeding on probing, presence of dental calculus and the evaluation of clinical
attachment loss (CAL). The CAL were recorded at 6 points around each tooth.
The periodontal condition of each individual was based on the quantity of
clinical attachment loss. Individuals with CAL ≤ 3 mm were regarded as healthy and
those with a CAL ≥ 4 mm were considered to be suffering from periodontitis.
All the individuals underwent a bone densitometry examination of the femur

47
and lumbar spine (L1-L4) using a dual-energy densitometer (GE-PRODIGY PRIMO;
X-ray; fan beam). The groups were defined according to the presence of periodontal
disease and the presence of osteopenia or osteoporosis (Figure 1).
Collection and extraction of DNA
From each patient, 5 mL of blood was collected via venipuncture. The
extraction of the DNA was performed using the PureLink Genomic DNA Kit
(Invitrogen, Foster City, USA), in accordance with the manufacturer’s instructions.
The extracted DNA was stored in a freezer at -80ºC until the polymorphism analyses.
The evaluation of DNA quality and quantity was carried out by analyzing
absorbance in a spectrophotometer (NanoDrop 2000 – Thermo Scientific, USA) at
260 nm and 280 nm. Subsequently, the DNA was diluted in Milli-Q® ultrapure water
for a final concentration of 100 ng/µL.
Identification of genetic polymorphisms
PCR-RFLP conditions for the gene IL6 G-174C (rs1800795)
The primers used in the PCR to amplify the samples of genomic DNA were
as follows: 5’-TTG TCA AGA CAT GCC AAG TGC T-3’ (forward) and 5’-
GCCTCAGAGACATCTCCAGTCC-3’ (reverse) (8). The PCR mixture consisted of a
final volume of 50 L containing 75 mM Tris-HCl, 20 mM (NH4)2SO4, 1.5 mM of
MgCl2, 0.2 mM of dNTPs, 1 pM of each primer, 2.5 U of Taq DNA polymerase
(Invitrogen) and 2 L of DNA solution. The amplification conditions consisted of 95ºC
for 1 minute, followed by 35 cycles of 60ºC for 1 minute and 72ºC for 1 minute. After
amplification, 10 L of the PCR product were analyzed by electrophoresis in agarose
gel (2%). The gel was then stained using SYBR Safe (Invitrogen, Foster City, USA)
and the recently synthesized fragments were viewed under ultraviolet light. The size
of the product amplified by PCR was estimated based on the electrophoretic
migration of the product in relation to the 50 bp DNA Ladder marker (Invitrogen). For
the IL6 polymorphism, 1 U of the NlaIII restriction enzyme was used for every 25 L
of reaction and the products of digestion obtained were: G allele (13+227+59 bp) and
C allele (13+118+109+59 bp). The product of digestion was viewed via

48
polyacrylamide gel electrophoresis at 10% stained by silver nitrate.
Serological quantification of IL-6
The quantification of the cytokines IL-6 was performed in serum samples by
ELISA (Enzyme-Linked Immunosorbent Assay). The whole procedure was performed
according to the manufacturer's instructions and standard operating procedure.
Statistical analysis
The Statistical Package for Social Sciences 20.0 (SPSS, UK) application was
used for the statistical analysis of the data, establishing a confidence interval of 95%
and a level of significance of 5% (p<0.05) for all the tests applied.
For the quantitative variables, the Kolmogorov-Smirnov normality test was
applied and data with normal distribution were displayed using the mean and
standard deviation while data without normal distribution were displayed using the
median and interquartile range.
The Chi-Squared test was used to evaluate a possible association between
the presence of polymorphisms in the IL6 genes with the occurrence of periodontal
disease in elderly subjects with osteoporosis, as well as to check if the genotypic
frequencies were in the Hardy-Weinberg equilibrium. To evaluate the differences in
genotypic frequencies between the case and control groups, the odds ratio (OR) was
estimated with a confidence interval of 95% based on the frequency of the CC
genotype relative to the combined GG+GC genotypes. Kruskall-Wallis test was used
to compare IL-6 serum level according to IL-6 genotype.
Results
A total of 191 elderly individuals took part in this study of which 112 (58.6%)
were women and 79 (41.4%) were men. The majority of patients were aged between
65 and 75 years (57.1%), the mean age 67.84 (SD=5.3), of non-white ethnicity
(60.8%) and those elderly subjects who have never smoked (60.7%). A total of 116
(60.7%) individuals suffered from periodontitis, while 77 (39.3%) were healthy. As far
as the BMD is concerned, 102 (53.4%) did not present with osteoporosis, however

49
63 (33%) and 26 (13.6%) individuals, respectively, had osteopenia and osteoporosis.
The frequency of the G allele in the study sample was 70.9% and the C allele 29.1%,
and 52.4% of the elderly were carriers of the GG genotype (Table 1).
It was found that the frequency of polymorphism genotypes in the IL6 gene is
in agreement with the Hardy-Weinberg equilibrium (p=0.79). The frequency
distribution of the genotypes and the alleles for the polymorphism in the IL6 -174
gene, in individuals with and without periodontal disease, without osteoporosis and
with osteopenia and osteoporosis, are displayed in Table 2. It was found that
individuals with osteoporosis and carriers of the G allele are more susceptible to
periodontal disease (Chi-Squared=10.33; p=0.04, Table 2). 84.2% of individuals who
are carriers of the GG genotype presented with both osteoporosis and periodontal
disease, while 14.5% of the elderly who harbored the CC genotype were found to be
free of osteoporosis. The C allele afforded 25% (OR=0.25; CI 95%: 0.071 - 0.857;
p=0.03) protection to individuals who harbor this allele compared with those that had
the G allele.
It can also be seen that individuals who are carriers of the G allele
(genotypes GC and GG) had higher IL-6 plasma levels (median=69.28 pg/mL;
interquartile range=56.9) compared to individuals who do not carry this allele
(median=42.72 pg/mL; interquartile range=32.3), according to the Kruskall-Wallis test
(p=0.04, figure 2).
Discussion
Cytokines are proteins of low molecular weight involved in the immune and
inflammatory response in which they regulate the amplitude and duration of these
responses. In the progressive form of periodontal disease, high concentration of
these cytokines are secreted culminating in periodontal attachment loss and bone
loss (10). IL-6 is a multifunctional cytokine that is essential for the regulation of
immune response and bone resorption (6). In periodontitis, it is expressed by a
variety of cells and, in common with IL-1, it engages in the increase in bone
resorption activity (11,12). It was demonstrated that high levels of IL-1B and IL-6 are
induced by periodontal pathogens and are related to the continuous destruction of
tissue observed with periodontitis (13).
The single-nucleotide polymorphism with a base change from G to C, at

50
position -174, results in the suppression of the transcription of IL-6 in response to
stimuli, like LPS or IL-1, suggesting it is involved in genetic protection to inflammatory
diseases (14,15). In this study, individuals with the GC genotype of the IL6
polymorphism in the -174 region were statistically associated with the susceptibility to
periodontal disease and osteoporosis. The C allele afforded 25% (OR=0.25; CI 95%:
0.071 - 0.857; p=0.03) protection to individuals harboring this allele in comparison
with those having the G allele.
These results are in agreement with a Brazilian study in which individuals
with the GG genotype were statistically associated with periodontal disease. The
researchers believe that the presence of the rare C allele affords a factor of
protection against the progression of the disease, as it results in lower expression of
IL-6 after stimulation of the inflammatory response (8). Similar results were found by
Tervonen et al. (7), who also found evidence of a relationship between the clinical
signs of periodontal disease and the presence of a polymorphism in the IL6 gene at
position -174, when considering the homozygous GG genotype. These results are
consistent with a meta-analysis which analyzed the relationship between BMD or
osteoporosis and polymorphisms in the promoter region of IL6 -174, providing
additional evidence that the CC genotype may contribute to high BMD, thereby
diminishing the risk of osteoporosis in Caucasians (5). Individuals with CC genotype
have between 3 and 7% higher BMD levels than individuals with GG genotype (16).
These findings are consistent with the understanding of the biological
function of the IL-6, which stimulates the development of osteoclasts, and thus the
process of bone resorption, as well as acting as a mediator of the effects of IL-1, a
powerful stimulator of bone resorption (6,11,12).
In the studied sample, we found a low frequency of the CC genotype in all
groups, related to the similarly low frequency of the C allele (29.1%). This allele
frequency percentage (29.8%) is similar to that found by Trevilatto et al. (8) in a
Caucasian sample of the Brazilian population.
Another important result was the significant correlation between the presence
of the C allele (CC individuals) and the low IL-6 plasma levels, indicating that the
polymorphism reduces gene expression, and the CC genotype is associated with the
low risk of developing osteoporosis when compared to the GG genotype (5).
The study of genetic polymorphisms is interesting from a clinical point of view
since identifying individuals at risk of adverse results on account of race or genetic
51
makeup provides a way to target the interventions (17). In addition to acquiring a
better understanding of the disease process, polymorphisms may be used as
diagnostic or prognostic markers (18). Razzouk and Termechi (19) mentioned
personalized periodontal therapy as the next concept in treatment for an advanced
clinical outcome, i.e. DNA information combined with clinical information is becoming
a necessity for highly personalized periodontal treatment, so that, in the future, it may
be possible to use this information to adapt the host’s response to the microbial
infection, thus minimizing inflammatory damage (19,20).
The results of this study suggest an association between periodontal disease
and osteoporosis and IL6 genetic polymorphism at position -174, corroborating one
of the hypotheses raised by Stabholz et al. (17) that there is an increased risk of
developing periodontal disease with the presence of osteoporosis, deriving from the
fact that systemic factors affecting bone metabolism may also be modifying the local
tissue response to a periodontal infection through an increase in the systemic release
of IL-1 and IL-6, as is the case with genetic polymorphisms.
Given the limitations of this study, we can conclude, based on the distribution
of the genotypes between the groups, that the GG genotype of the IL6 -174 genetic
polymorphism is statistically associated with an increased susceptibility to
periodontitis in patients with osteoporosis, suggesting that the C allele may afford a
factor of protection against the development of periodontal disease and osteoporosis.
52
References
1. Sanz M, Van Winkelhoff AJ, Working Group 1 of Seventh European Workshop on Periodontology. Periodontal infections: understanding the complexity – Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol 2011; 38: 3-6.
2. Kornman KS, Di Giovine FS. Genetic variations in cytokine expression: a risk factor for severity of adult periodontitis. Ann Periodontol 1998; 3: 327-338.
3. Kornman KS, Page R C, Tonetti, M. S. The host response to the microbial challenge in periodontitis: assembling the players. Periodontol 2000 1997; 14: 33-53.
4. Martínez-Maestre MÁ, González-Cejudo C, Machuca G, Torrejón R, Castelo-Branco C.Periodontitis and osteoporosis: a systematic review. Climacteric 2010; 13: 523-529.
5. Ni Y, Li H, Zhang Y, Zhang H, Pan Y, Ma J, et al. Association of IL-6 G-174C polymorphism with bone mineral density. J Bone Miner Metab 2014; 32: 167-173.
6. Ota N, Nakajima T, Nakazawa I, Suzuki T, Hosoi T, Orimo H et al. A nucleotide variant in the promoter region of the interleukin-6 gene associated with decreased bone mineral density. J Hum Genet 2001; 46: 267-272.
7. Tervonen T, Raunio T, Knuuttila M, Karttunen R. Polymorphisms in the CD14 and IL-6 genes associated with periodontal disease. J Clin Periodontol 2007; 34: 377-383.
8. Trevilatto PC, Scarel-Caminaga RM, Brito RB Jr, Souza AP, Line SR.. Polymorphism at position -174 of IL-6 gene is associated with susceptibility to chronic periodontitis in a Caucasian Brazilian population. J Clin Periodontol 2003; 30: 438-442..
9. Spirduso WW. Dimensões físicas do envelhecimento. Barueri: Manole, 2005.
10. Gemmell E, Marshall RI, Seymour GJ. Cytokines and prostaglandins in immune homeostasis and tissue destruction in periodontal disease. Periodontol 2000 1997; 14: 112-143.
11. Hughes FJ, Howells GL. Interleukin-6 inhibits bone formation in vitro. Bone Miner 1993; 21: 21-28.
12. Irwin CR, Myrillas TT. The role of IL-6 in the pathogenesis of periodontal disease. Oral Dis. 1998 Mar;4(1):43-7.
13. Okada H, Murakami S. Cytokine expression in periodontal health and disease. Crit Rev Oral Biol Med 1998; 9: 248-266.
14. Fishman D, Faulds G, Jeferry R, Mohamed-Ali V, Yudkin JS, Humphries S et

53
al. The effect of novel polymorphisms in the interleukin-6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and na association with systemic-onset juvenile chronic arthritis. J Clin Invest 1998; 102: 1369–1376.
15. Shapira L, Wilensky A, Kinane DF. Effect of genetic variability on the inflammatory response to periodontal infection. J Clin Periodontol 2005; 32: 72-86.
16. Garnero P, Borel O, Sornay-Rendu E, Duboeuf F, Jeffery R, Woo P et al.. Association between a functional interleukin-6 gene polymorphism and peak bone mineral density and postmenopausal bone loss in women: the OFELY study. Bone 2002; 31: 43-50.
17. Stabholz A, Soskolne WA, Shapira L. Genetic and environmental risk factors for chronic periodontitis and aggressive periodontitis Periodontol 2000 2010; 53: 138-153.
18. Dentino A, Lee S, Mailhot J, Hefti AF. Principles of periodontology. Periodontol 2000 2013; 61: 16-53.
19. Razzouk S, Termechi O. Host genome, epigenome, and oral microbiome interactions: toward personalized periodontal therapy. J Periodontol 2013; 84: 1266-1271.
20. Frank MO, Mandell GL. Adjuncts to antibacterial therapy. Infect Dis Clin North Am 1995; 9: 769-781.

54
Table 1 - Demographic distribution, allelic and genotypic frequencies for the IL6 gene, periodontal disease and Bone mineral density in the elderly (n= 191).
CHARACTERISTICS
n %
Gender
Male 79 41.4% Female
112 58.6%
Age 60 -64 65 -75 > 75
63 109
19
33.0% 57.1%
9.9%
Ethnic group White 75 39.3% Non white
116 60.8%
Smoking habit Never smoked 116 60.7% Ex-smoker 59 30.9% Current smoker
16 8.4%
Genotype frequency GG 100 52.4% CC 20 10.5% GC
71 37.2%
Allele frequency G 271 70.9% C
111 29.1%
Periodontal Disease Healthy 75 39.3% Periodontitis
116 60.7%
BMD Without osteoporosis 102 53.4% With osteopenia 63 33.0% With osteoporosis
26 13.6%
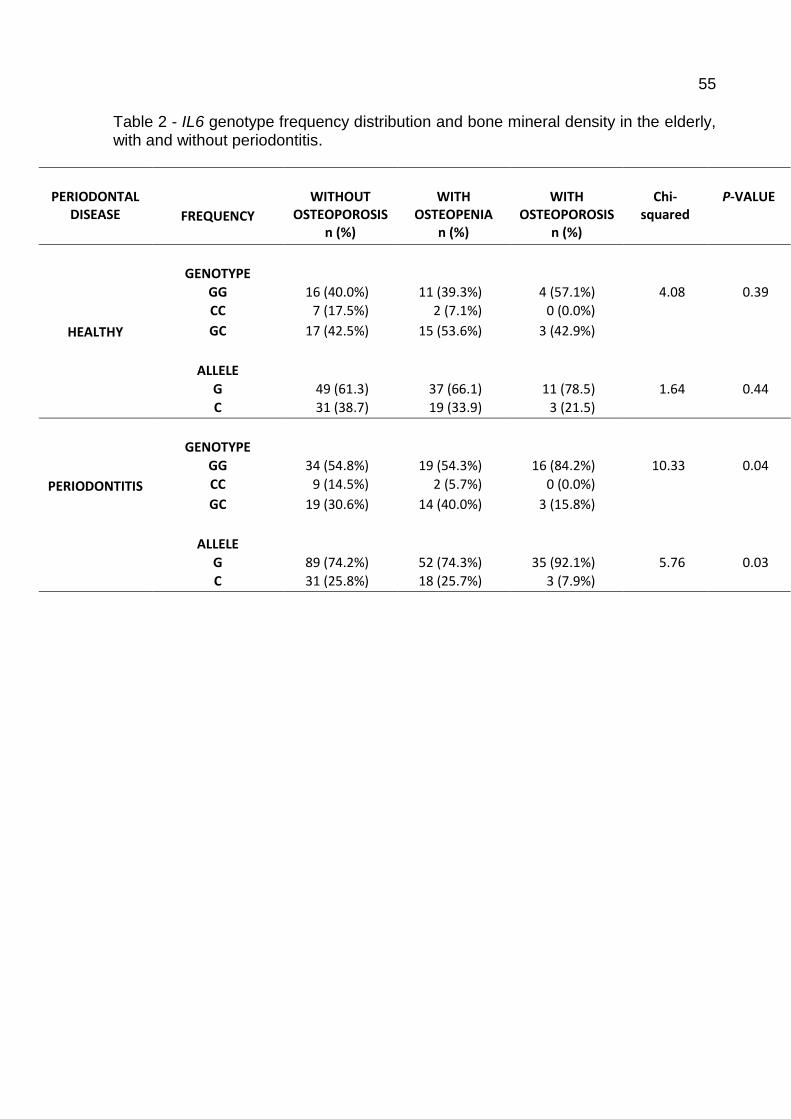
55
Table 2 - IL6 genotype frequency distribution and bone mineral density in the elderly, with and without periodontitis.
PERIODONTAL
DISEASE
FREQUENCY
WITHOUT
OSTEOPOROSIS n (%)
WITH
OSTEOPENIA n (%)
WITH
OSTEOPOROSIS n (%)
Chi-
squared
P-VALUE
HEALTHY
GENOTYPE
GG 16 (40.0%) 11 (39.3%) 4 (57.1%) 4.08 0.39 CC 7 (17.5%) 2 (7.1%) 0 (0.0%) GC 17 (42.5%) 15 (53.6%) 3 (42.9%)
ALLELE
G 49 (61.3) 37 (66.1) 11 (78.5) 1.64 0.44 C 31 (38.7) 19 (33.9) 3 (21.5)
PERIODONTITIS
GENOTYPE
GG 34 (54.8%) 19 (54.3%) 16 (84.2%) 10.33 0.04 CC 9 (14.5%) 2 (5.7%) 0 (0.0%) GC 19 (30.6%) 14 (40.0%) 3 (15.8%)
ALLELE
G 89 (74.2%) 52 (74.3%) 35 (92.1%) 5.76 0.03 C 31 (25.8%) 18 (25.7%) 3 (7.9%)
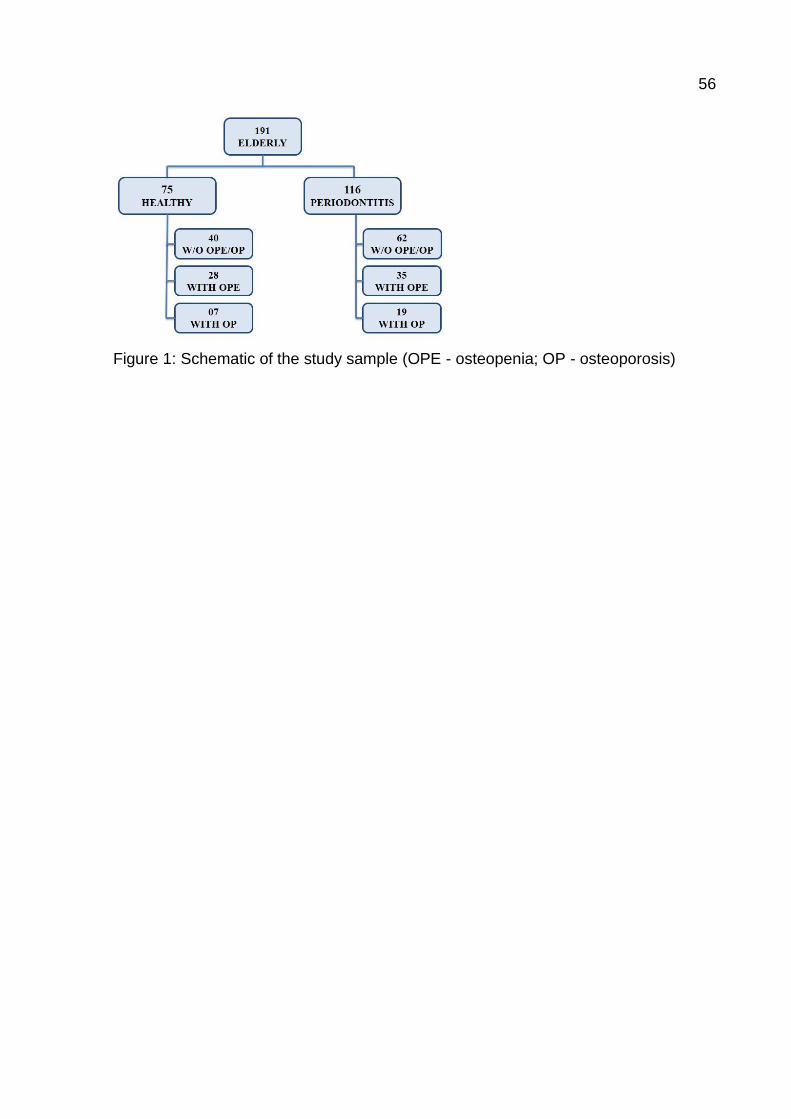
56
Figure 1: Schematic of the study sample (OPE - osteopenia; OP - osteoporosis)

57
Figure 2 - Comparison of serum levels of IL-6 (pg/mL) distribution according to IL-6 gene genotype. * Statistically different from CC genotype, Kruskall-Wallis test.
58
6 ARTICLE 3
ASSOCIATION BETWEEN THE VITAMIN D RECEPTOR GENE (VDR)
HAPLOTYPE AND PERIODONTITIS IN THE ELDERLY IN BRAZIL
(Submitted to the “Journal of Clinical Periodontology”)
M. B. B. P. Pedriali1, E. D. Ruzzon; S. K. Moura1, S. M. Maciel1, R.C. Poli-Frederico2
1 Department of Restorative Dentistry, Faculty of Dentistry, University of North of Parana, Londrina, PR, Brazil 2 MS, PhD, Department of Genetics and Molecular Biology, Faculty of Dentistry, University of North of Parana, Londrina, PR, Brazil
Abstract
Objective: The aim of this study was to investigate the frequency of TaqI, BsmI, ApaI and FokI VDR polymorphism and its haplotypes, and their association with chronic periodontitis, as well as the association of periodontitis and osteoporosis among Brazilian elderly. Material and Methods: Clinical examination including the evaluation of periodontal attachment loss were performed in 125 individuals who were divided into two groups: 93 healthy individuals (control group) and 32 subjects with chronic periodontitis. DNA was extracted from blood, and the VDR TaqI, BsmI, ApaI and FokI polymorphism were genotyped using real-time polymerase chain reaction. Results: The TaqI, BsmI, ApaI and FokI polymorphisms showed no statistically significant difference between the control group and chronic periodontitis group. The haplotype analysis of the combined VDR polymorphism revealed that individuals with 1 or 2 copies of genotype TBAF had a significantly greater chance of developing periodontitis than the others who did not have this genotype (OR = 2.54; CI = 95% 1.11 - 5.85; p = 0.04). No significant difference was found between osteoporosis and the presence of periodontal disease. Conclusion: The TBAF haplotype constructed from the TaqI, BsmI, ApaI and FokI polymorphisms is associated with the prevalence of chronic periodontitis in elderly Brazilians.
CORRESPONDING AUTHOR. Regina Célia Poli-Frederico. Universidade Norte do Paraná, Faculdade de
Odontologia. Rua Marselha 183, Jardim Piza, Londrina, PR, Brasil. CEP 86041-120. Phone: +55-43-3371-7820 Fax: +55-43-3371-7741. Email: [email protected].
59
1. Introduction
Periodontal diseases comprise both inflammatory and infectious conditions
caused by the interaction between biofilm and the inflammatory response of the host.
However inflammatory response to infection in periodontal tissue is influenced both
by environmental and genetic factors (Stabholz et al. 2010) and the evidence points
to individual susceptibility to periodontal disease being partly determined by genetic
predisposition (Mohammad et al. 1994).
One of the fundamental traits of periodontal disease is alveolar bone loss
and several studies have identified genetic polymorphisms that influence
osteoporosis-related bone mineral density and bone loss (Inagaki et al. 2003).
Researchers have suggested an increased risk of developing periodontal disease
when osteoporosis is present, as it results in low bone mineral density (BMD)
throughout the body, including the maxilla and mandibular, leading to an increase in
alveolar porosity, an altered trabecular pattern and faster alveolar bone resorption
following invasion by periodontal pathogens (Amano et al. 2009, Stabholz et al.
2010). Considering that the development of periodontal disease and
osteopenia/osteoporosis presents common pathological mechanisms which involve
the breakdown of bone homeostasis, the hypothesis that these conditions may share
common genetic risk factors is plausible (Henning et al. 1999).
The vitamin D receptor (VDR) regulates vitamin D’s hormonal activity and
plays a fundamental role in bone homeostasis and in the metabolism of calcium as
well as acting on cell proliferation, cell differentiation and even immune-modulating
activity (Henning et al. 1999, Nagpal et al. 2005). VDR gene polymorphisms could
lead to distinct cellular effects on gene activation, such as the increase/decrease in
transcription, the metabolism of calcium, BMD, cell proliferation and immune
response (Martelli, 2014).
The most commonly studied polymorphisms are the single-nucleotides
(SNP): rs1544410I (BsmI), rs7975232 (ApaI), rs731236 (TaqI) and rs2228570 (FokI)
(Horst-Sikorska et al. 2013, Pouresmaeili et al. 2013, Mostowska et al. 2013). In
addition, the polymorphisms in this gene are frequently present in and have been
associated with osteoporosis and periodontal disease (Grant & Ralston 1997, Sun et
al. 2002, Brito Jr et al. 2004, Deng et al. 2011).
The vast majority of studies have focused on analysing the TaqI

60
polymorphism of the VDR gene in order to evaluate the possible association of this
polymorphism and an individual’s increased susceptibility to develop periodontitis
associated with alveolar bone loss. The TT genotype and the presence of the T allele
have been associated with chronic periodontal disease in patients of Japanese,
Chinese and Caucasian origin (Tachi et al. 2001; Nibali et al. 2008). In contrast, a
Brazilian study conducted by Brito Jr et al. (2004), showed that individuals with any
form of the “t” allele, (Tt or tt genotype) are 2.4 times more susceptible to periodontal
disease. Very few studies, however, have looked into the effects of the ApaI, BsmI or
FokI polymorphisms of the VDR gene on periodontal disease (Naito et al. 2007).
Results show that the A allele, for the ApaI polymorphism, and the f allele, for the
FokI polymorphism, may be related to an increased susceptibility to periodontal
disease (Inagaki et al. 2003, Park et al. 2006). Additionally, few studies have
examined the effects of these polymorphisms on periodontitis, although the effects of
VDR gene haplotypes on BMD have been reported on (Jaramillo-Rangel et al. 1999,
Kim et al. 2003, Macdonald et al. 2006).
The objective of this study is to investigate the frequency of the single-
nucleotide polymorphisms (SNP) TaqI, BsmI, ApaI and FokI of the VDR gene and its
haplotypes, and their association with chronic periodontitis, as well as the association
of periodontitis and osteoporosis in a sample of elderly in the Brazilian population.
2. Materials and methods
2.1 Selection of individuals
A sample of 125 individuals aged 60 or above, from both sexes, was
selected based on a cross-sectional study on Aging and Longevity (EELO Project)
conducted at the Norte do Paraná University (approved by the UNOPAR Research
Ethics Committee, record no. PP0070/09). The patients hail from the southern region
of Brazil and all participants signed the Free and Informed Consent Form.
Eligibility criteria were as follows: aged 60 or above, physically independent
and good overall state of health. Elderly individuals who had a systemic disease,
other than osteoporosis, or who suffered from some limitation, such as a physical or
mental disability, were excluded from the sample.
The diagnosis and classification of periodontal disease was carried out by

61
means of a physical examination that included an analysis of clinical parameters and
medical and dental histories. The clinical parameters included periodontal probing,
presence or absence of bleeding on probing, presence of dental calculus and the
evaluation of periodontal attachment loss (PAL). The PAL was checked at 6 points
around each tooth.
The periodontal condition of each individual and the definition of the groups
was based on the quantity of periodontal attachment loss. In the control group,
individuals were considered to be healthy with a PAL ≤ 3 mm (n=93) while the
periodontitis group consisted of individuals with a PAL ≥ 4 mm (n=32).
All individuals underwent a bone densitometry examination of the femur and
lumbar spine (L1-L4) using a dual-energy densitometer (GE-PRODIGY PRIMO; X-
ray; fan beam). The elderly subjects were divided into three groups by a radiologist:
control group (above 1.0 Sd), osteopenic (-1.0 to -2.5 Sd) and osteoporotic (below -
2.5 Sd), in accordance with the criteria advocated by the World Health Organization.
2.2 Collection and extraction of DNA
From each patient, 5 mL of blood was collected via venipuncture. The
extraction of the DNA was performed using the PureLink Genomic DNA Kit
(Invitrogen), in accordance with the manufacturer’s instructions. The extracted DNA
was stored in a freezer at -80ºC awaiting the performance of the polymorphism
analyses.
The evaluation of DNA quality and quantity was carried out by analyzing
absorbance in a spectrophotometer (NanoDrop 2000 - Thermo Scientific) at 260 nm
and 280 nm. Subsequently, the DNA was diluted in Milli-Q® ultrapure water for a final
concentration of 30 ng/µL.
2.3 Genotyping
2.3.1 Real time PCR conditions for the VDR gene
In order to analyse the SNP of the VDR gene, the DNA fragment
amplification technique was performed by means of real-time polymerase chain
reaction (PCR) using the TaqMan® system (Applied Biosystems, Foster City, USA).

62
Four polymorphisms were examined: rs731236 (TaqI - C_2404008_10); rs1544410
(BsmI - C_8716062_10); rs7975232 (ApaI - C_28977635_10) and rs2228570 (FokI -
C_12060045_20 ).
The standardised reaction employed consisted of the following: 20 L of final
volume, comprising 10 L Taqman® Genotyping Master Mix (1x), 0.5 L of probe (1x)
(Applied Biosystems, Foster City, USA), 7.5 L of Milli-Q® ultrapure water and 2 L of
DNA (30 ng/L). The thermal cycler StepOnePlus™ Real-Time PCR System (Applied
Biosystems, Foster City, USA) was used for this activity, using the following cycles:
60ºC for 30 seconds, 95ºC for 10 minutes, 50 cycles at 95ºC for 15 seconds and
60ºC for 90 seconds with a final cycle of 30 seconds at 60ºC. An evaluation of the
results was performed using the software application StepOne Software v2.3.
3. Statistical analysis
The differences in the genotype and allele frequencies (categorical variables)
were evaluated using the chi-squared test (X2), with Yates correction or Fisher’s
exact test. The differences were deemed to be significant when p<0.05. The physical
proximity of the polymorphisms explains the simultaneous analysis of the haplotypes.
The ARLEQUIN 3.0 (Arlequin, Switzerland) suite of programs was used to calculate
haplotype frequencies, Hardy-Weinberg equilibrium and disequilibrium of linkage. For
the risk analysis of the alleles, genotypes and haplotypes, the Odds Ratio (OR) was
calculated, with a confidence interval of 95%. The statistical analysis was performed
using the application BioStat 2.0 for Windows (AnalystSoft, Canada), SPSS 10.0 for
Windows (SPSS Inc., Chicago, IL), and the ARLEQUIN 3.0 statistical package
(Arlequin, Switzerland).
4. Results
Single-nucleotide polymorphism
Table 1 shows the demographic characteristics of the elderly participants,
with or without chronic periodontitis. No statistically significant difference was found
between sex, smoking habits or BMD (bone mineral density: osteopenia and/or
osteoporosis) and the presence of periodontal disease. A significant difference was
found, however, between age and periodontal disease (p < 0.05).

63
Table 2 shows the genotype distribution of each polymorphism of the VDR
gene TaqI, BsmI, ApaI and FokI. For individuals with chronic periodontitis, the most
frequent genotypes of the TaqI, BsmI, ApaI and FokI polymorphisms were Tt
(46.9%), Bb (56.3%), Aa (56.3%) and FF (50%), respectively. The TaqI, BsmI, ApaI
and FokI polymorphisms showed no statistically significant difference between the
control group and chronic periodontitis group. The genotype frequencies were
consistent with the Hardy-Weinberg equilibrium (p > 0.05).
Combined polymorphisms
Fifteen different haplotypes were identified after analysing the combinations
of genotype frequencies of the four VDR gene polymorphisms, the most prevalent in
the sample being TBAF (21.2%), TbAF and Tbaf (12%), tbAf (10%) and TbaF (9.6%)
(Table 3).
The haplotype TBAF (28.1%) was more common amongst individuals with
chronic periodontitis than in those without the disease. Moreover, the haplotype Tbaf
(4.7%) was not as prevalent in individuals with chronic periodontitis when compared
to those without the disease.
The combination of these haplotypes formed 33 genotypes, of which the
highest proportions in the sample were TtBbAaFf (11.2%), TtBbAAFf and TTbbAaFF
(8.8%), TtBbAAFF (7.2%) and TTbbAaFf (6.4%).
There was no statistical difference in the frequency of haplotypes in the
sample, but there was a predominance of the genotype TBAF/tbaf in the control
group (11.8%) and a higher frequency of the genotype TBAF/tbaF in the group of
individuals with chronic periodontitis (15.6%).
As can be observed from Table 4, an association was found between carriers
of combined polymorphisms in the VDR gene and the prevalence of chronic
periodontitis. Hence the data was analysed for those study participants with the most
common haplotypes (TBAF, TbAF, Tbaf, tbaf, tbAf and TbaF). Those elderly
individuals with 1 or 2 copies of genotype TBAF had a significantly greater chance of
developing periodontitis than the others who did not have this genotype (OR = 2.54;
CI = 95% 1.11 - 5.85; p = 0.04). The remaining genotypes (TbAF, Tbaf, tbaf, tbAf and
TbaF) did not exhibit any statistically significant differences between the evaluated
groups.

64
5. Discussion
Periodontitis is a chronic disease with a complex, multi-factor
etiopathogenesis in which microbiological factors interact with environmental and
genetic factors to determine the onset and progression of the disease (Nibali et al.
2008).
The concept of risk factors and mechanisms involved in the onset and
progression of periodontitis has developed dramatically in recent decades, from a
simplistic vision of microorganisms directly causing the clinical signs and symptoms
of periodontitis to an understanding of the importance of the host’s immune and
inflammatory response system, influenced by genetic and environmental factors
(Kornman 2008, Page & Kornman 1997).
Periodontal disease results in the destruction of alveolar bone which, if left
untreated, could lead to tooth movement and, potentially, the exfoliation of the teeth,
therefore it is conceivable that the mediators of bone metabolism play a part in the
pathophysiology of periodontitis (Loos et al. 2005).
In this study we investigate the association of the polymorphisms TaqI, BsmI,
ApaI and FokI of the VDR gene and chronic periodontitis in elderly Brazilians. The
TaqI polymorphism of the VDR gene is characterised by a single base transition
(T<C) which leads to an alteration of the codon 352 in exon 9 of the VDR gene,
which creates a TaqI restriction locus (Martelli et al. 2014). The VDR is a nuclear
receptor which binds with the active form of vitamin D and thereby modulates the
expression of the gene by interacting with the promoter region of the target genes
(Nibali et al. 2008). The molecular mechanisms in which bone density is regulated by
the VDR are uncertain, despite the fact that the C allele (t) is related to the increased
transcription activity, to mRNA stability and a high level of serum of 1.25-D3 (Morrison
et al. 1994, Ma et al. 1998). In this study, the polymorphisms TaqI, BsmI, ApaI and
FokI showed no significant statistical difference between the control group and the
group with chronic periodontitis.
The TT genotype and the presence of the T allele of the TaqI polymorphism
were associated with chronic periodontal disease in Japanese, Chinese and
Caucasian patients (Tachi et al. 2001, Nibali et al. 2008). In a cross-sectional study,
Borges et al. (2009) examined the relationship between the TaqI polymorphism of the
65
VDR gene and subgingival microbiota in Brazilian adults with chronic periodontitis,
demonstrating that the Tt genotype was more prevalent in the group of individuals
with periodontitis and no association was observed between genotype and
composition of the subgingival microbiota. When calculating the odds ratio, they
revealed that individuals with the Tt genotype are 4.57 times more susceptible to
periodontal disease. In another Brazilian study conducted by Brito Jr et al. (2004), it
was found that individuals with any form of the t allele, Tt or tt genotype are 2.4 times
more susceptible to periodontal disease.
Previous studies on the BsmI polymorphism conducted on the Brazilian
population (Brito Jr et al. 2004) and the Japanese population (Naito et al. 2007)
found no significant statistical difference in the distribution of the BsmI VDR gene
polymorphism between individuals with and without periodontal disease. Brito Jr et
al. (2004) were the first to analyse the haplotypes formed by the TaqI and BsmI
single-nucleotide polymorphisms of the VDR gene, in which they found that the
patients with the TB haplotype and the TB/tb genotype are more susceptible to
periodontal disease, and are associated with clinical attachment loss in chronic
periodontitis in a sample of the Brazilian population.
Inagaki et al. (2003) demonstrated an association between the ApaI VDR
gene polymorphism and the progression of periodontal disease in adult males,
reporting that the highest rate of alveolar bone loss and clinical attachment occurred
with the AA genotype, when compared with the Aa or aa genotypes. However we
found that the Aa genotype was the most prevalent in elderly subjects with chronic
periodontitis, despite the difference between the genotypes not being statistically
significant.
Park et al. (2006) found an association between the FokI VDR gene
polymorphism and an increased risk of developing generalized aggressive
periodontitis. Similar to our study, Tachi et al. (2003) found no association of the FokI
VDR gene polymorphism, whether genotype or alleles, with chronic periodontitis.
Naito et al. (2007) investigated the relationship between the ApaI, BsmI and
FokI VDR gene polymorphisms and the risk of severe chronic periodontitis amongst
adult Japanese males and they found that homozygous Abf individuals had a
significantly higher prevalence of severe chronic periodontitis than others.
Osteoporosis, or the reduction in BMD with osteopenia, could be a risk factor
for alveolar bone loss, resulting in the accelerated progression of bone resorption

66
faced with infection via oral biofilm and the host’s immune response, and infection
through periodontal pathogenic bacteria leads to the local production of pro-
inflammatory cytokines that raise the levels of systemic cytokines that aggravate
even more the loss of bone mineral density in the skeleton (Reddy & Morgan 2013).
However, the results of a cross-sectional study conducted on women aged between
45 and 65, established no association between the presence of serious periodontal
disease and osteoporosis (Marjanovic et al. 2013). In this study we observed no
statistically significant association between individuals with periodontitis and low
BMD, in both sexes. Some studies have found evidence of an association, although
more controlled studies with standardized clinical parameters regarding systemic
bone loss and periodontal disease are required to clarify the interrelationship
between systemic and alveolar bone loss and to determine if osteoporosis is a risk
factor for periodontal disease and, if it is, what measures contributed to the global
risk of periodontal disease (Martinez-Maestre et al. 2010, Genco & Borgnakke 2013).
The results of this study suggest that the TBAF VDR gene haplotype may be
associated with an increased susceptibility to periodontal disease, however it is still
uncertain if this association is valid amongst individuals under 60 years of age and
for other ethnic groups. Therefore further studies are required to determine if the
combination of VDR gene polymorphisms influences the risk of developing
periodontal disease in diverse situations.
Given the limitations of this study, we may conclude that the TBAF haplotype
constructed from the TaqI, BsmI, ApaI and FokI single-nucleotide polymorphisms of
the VDR gene, is associated with the prevalence of chronic periodontitis in elderly
Brazilians.
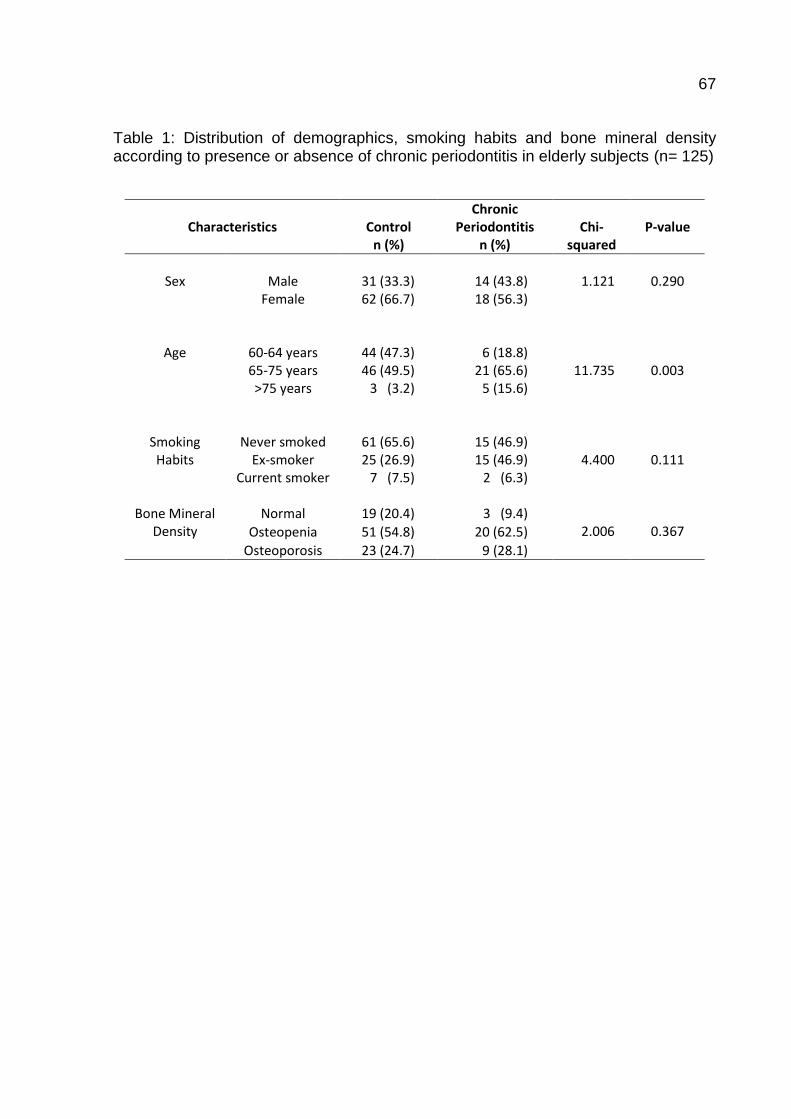
67
Table 1: Distribution of demographics, smoking habits and bone mineral density according to presence or absence of chronic periodontitis in elderly subjects (n= 125)
Characteristics
Control n (%)
Chronic Periodontitis
n (%)
Chi-
squared
P-value
Sex
Male
31 (33.3)
14 (43.8)
1.121
0.290
Female
62 (66.7) 18 (56.3)
Age
60-64 years
44 (47.3)
6 (18.8)
11.735
0.003 65-75 years 46 (49.5) 21 (65.6) >75 years
3 (3.2) 5 (15.6)
Smoking Habits
Never smoked
61 (65.6)
15 (46.9)
4.400
0.111 Ex-smoker 25 (26.9) 15 (46.9) Current smoker 7 (7.5) 2 (6.3)
Bone Mineral
Density
Normal
19 (20.4)
3 (9.4)
2.006
0.367 Osteopenia 51 (54.8) 20 (62.5)
Osteoporosis 23 (24.7) 9 (28.1)

68
Table 2: Distribution of genotype and allele frequency of the TaqI, BsmI, ApaI and FokI VDR gene polymorphisms in healthy individuals and in individuals with chronic periodontitis.
SNP
Genotype
Control
n (%)
Chronic Periodontitis
n (%)
Chi-
squared
P-value
TaqI
TT 33 (35.5) 14 (43.8) 1.859
0.395 Tt 42 (45.2) 15 (46.9)
tt 18 (19.4) 3 (9.4)
T 108 (58.0) 43 (67.2) 1.297
0.254 t 78 (42.0) 21 (32.8)
BsmI
bb
32 (34.4)
13 (40.6)
1.141
0.565 Bb 60 (64.5) 18 (56.3)
BB 1 (1.1) 1 (3.1)
b 124 (66.7) 44 (68.8) 0.023
0.879 B 62 (33.3) 20 (31.2)
ApaI
AA
37 (39.8)
10 (31.3)
0.762
0.683 Aa 45 (48.4) 18 (56.3)
aa 11 (11.8) 4 (12.5)
A 119 (64.0) 38 (59.4) 0.257
0.612 a 67 (36.0) 26 (40.6)
FokI
ff
16 (17.2)
2 (6.3)
2.714
0.257 Ff 41 (44.1) 14 (43.8)
FF 36 (38.7) 16 (50.0)
f 73 (39.2) 18 (28.1) 2.087
0.149 F 113 (60.8) 46 (71.9)

69
Table 3: Frequency of haplotypes and genotypes in the TaqI, BsmI, ApaI and FokI VDR gene polymorphisms.
HAPLOTYPE
CONTROL
n (%)
CHRONIC
PERIODONTITIS
n (%)
GENOTYPE
CONTROL
n (%)
CHRONIC
PERIODONTITIS
n (%)
TbAf 5 (2.7) 1 (1.6) TbAf/tbAf 1 (1.1) 0 (0.0)
tbAf 19 (10.2) 6 (9.4) TBAf/TbAF 1 (1.1) 0 (0.0)
TBAf 7 (3.8) 0 (0.0) Tbaf/Tbaf 1 (1.1) 2 (6.2)
TbAF 22 (11.9) 8 (12.5) TBaf/Tbaf 1 (1.1) 0 (0.0)
Tbaf 22 (11.9) 8 (12.5) TbAf/Tbaf 3 (3.2) 1 (3.1)
TBaf 1 (0.5) 0 (0.0) TbAF/TbAF 1 (1.1) 0 (0.0)
TBAF 35 (18.8) 18 (28.1) TBAF/TbAF 2 (2.2) 1 (3.1)
TbaF 16 (8.6) 8 (12.5) TbaF/TbaF 4 (4.3) 1 (3.1)
tBAf 3 (1.6) 0 (0.0) TbAF/TbaF 7 (7.5) 4 (12.5)
Tbaf 19 (10.2) 3 (4.7) TBAF/TbaF 1 (1.1) 1 (3.1)
tBAF 15 (8.0) 3 (4.7) TBAF/TbAf 1 (1.1) 0 (0.0)
tbAF 13 (7.0) 2 (3.1) Tbaf/Tbaf 5 (5.4) 0 (0.0)
tbaF 8 (4.3) 6 (9.3) TbAF/Tbaf 5 (5.4) 3 (9.4)
tBaf 1 (0.5) 0 (0.0) TBAF/Tbaf 1 (1.1) 0 (0.0)
tBaF 0 (0.0) 1 (1.6) tBAf/tbAf 2 (2.2) 0 (0.0)
tBAf/tbaf 1 (1.1) 0 (0.0)
tBAF/tbAF 6 (6.5) 0 (0.0)
tBAF/tbaF 2 (2.2) 0 (0.0)
tBAF/tbAf 5 (5.4) 2 (6.3)
tBAF/tbaf 2 (2.2) 0 (0.0)
TBAf/tbAf 2 (2.2) 0 (0.0)
TBAf/tbaf 4 (4.3) 0 (0.0)
TBAF/tbAF 7 (7.5) 2 (6.3)
TbAF/tbaF 2 (2.2) 0 (0.0)
TBAF/tbaF 4 (4.3) 4 (15.6)
TbAF/tbAf 2 (2.2) 0 (0.0)
TBAF/tbAf 7 (7.5) 4 (12.5)
TbAF/tbaf 1 (1.1) 0 (0.0)
TBAF/tBaf 1 (1.1) 0 (0.0)
TBAF/tbaf 11 (11.8) 3 (9.4)
TBAF/TBAF 0 (0.0) 2 (3.1)
tBAF/tBaF 0 (0.0) 1 (3.1)
TbaF/tbaF 0 (0.0) 1 (3.1)
Total 186 (100.0) 64 (100.0) Total 93 (100.0) 32 (100.0)

70
Table 4. Association between the combined TaqI, ApaI, BsmI and FokI VDR polymorphism and the risk of chronic periodontitis.
Genotype
CONTROL
CHRONIC PERIODONTITIS
OR
95% CI
P-value
N % N %
TBAF
0 copies 69 74.2 17 53.1
1 or 2 copies 24 25.8 15 46.9 2.54 1.11-5.85 0.04
TbAF
0 copies 72 74.4 24 75.0
1 or 2 copies 21 22.6 8 25.0 1.14 0.45-2.91 0.97
Tbaf
0 copies 76 81.7 26 81.2
1 or 2 copies 17 18.3 6 18.8 1.03 0.37-2.90 0.84
tbaf
0 copies 74 79.6 29 90.6
1 or 2 copies 19 20.4 3 9.4 0.41 0.11-1.46 0.25
tbAf
0 copies 74 79.6 26 81.3
1 or 2 copies 19 20.4 6 18.7 0.90 0.32-2.49 0.96
TbaF
0 copies 89 95.7 31 96.9
1 or 2 copies 4 4.3 1 3.1 0.72 0.08-6.67 0.82

71
Bibliography
Amano, Y., Komiyama, K. & Makishima, M. (2009) Vitamin D and periodontal disease. Journal of Oral Science 51, 11-20.
Borges, M. A. T., Figueiredo, L. C., Brito Jr, R B., Faveri, M. & Feres, M. (2009) Microbiological composition associated with vitamin D receptor gene polymorphism in chronic periodontitis. Brazilian Oral Research 23, 203-208.
Brito Jr, R. B., Scarel-Caminaga, R. M., Trevilatto, P. C., Souza, A. P. & Barros, S. P. (2004) Polymorphisms in the vitamin D receptor gene are associated with periodontal disease. Journal of Periodontology 75, 1090-1095.
Deng, H., Liu, F., Pan, Y., Jin, X., Wang, H. & Cao, J. (2011) BsmI, TaqI, ApaI, and FokI polymorphisms in the vitamin D receptor gene and periodontitis: a meta-analysis of 15 studies including 1338 cases and 1302 controls. Journal of Clinical Periodontology 38, 199-207.
Genco, R. J. & Borgnakke, W. S. (2013) Risk factors for periodontal disease. Periodontology 2000 62, 59-94.
Grant, S. F. A. & Ralston, S. H. (1997) Genes and osteoporosis. Trends Endocrinology & Metabolism 8, 232-236.
Hennig, B. J. Parkhill, J. M., Chapple, I. L., Heasman, P. A. & Taylor, J. J. (1999) Association of a vitamin D receptor gene polymorphism with localized early-onset periodontal diseases. Journal of Periodontology 70, 1032-1038.
Horst-Sikorska, W., Dytfeld, J., Wawrzyniak, A., Marcinkowska, M., Michalak, M., Franek, E., Napiórkowska, L., Drwęska, N. & Słomski, R. (2013) Vitamin D receptor gene polymorphisms, bone mineral density and fractures in postmenopausal women with osteoporosis. Molecular Biology Reports 40, 383-390.
Inagaki, K., Krall, E. A., Fleet, J. C. & Garcia, R. I. (2003) Vitamin D receptor alleles, periodontal disease progression, and tooth loss in the VA dental longitudinal study. Journal of Periodontology 74, 161-167.
Jaramillo-Rangel, G., Cerda-Flores, R. M., Cardenas-Ibarra, L., Tamayo-Orozco, J., Morrison, N. & Barrera-Saldaña, H. A. (1999) Vitamin D receptor polymorphisms and bone mineral density in Mexican women without osteoporosis. Amercian Journal of Human Biology 11, 793-797.
Kim, J. G., Kwon, J. H., Kim, S. H., Choi, Y. M., Moon, S. Y. & Lee, J. Y. (2003) Association between vitamin D receptor gene haplotypes and bone mass in postmenopausal Korean women. American Journal of Obstetrics Gynecology 189, 1234-1240.
Kornman, K. S. (2008) Mapping the pathogenesis of periodontitis: a new look. Journal of Periodontology 79 (Suppl 8), 1560-1568.
72
Loos, B. G., John, R. P. & Laine, M. L. (2005) Identification of genetic risk factors for periodontitis and possible mechanisms of action. Journal of Clinical Periodontology 32 (Suppl. 6) 159-179.
Ma, J., Stampfer, M. J., Gann, P. H., Hough, H. L., Giovannucci, E., Kelsey, K. T., Hennekens, C. H. & Hunter, D. J. (1998) Vitamin D receptor polymorphisms, circulating vit D metabolites, and risk of prostate cancer in United States physicians. Cancer Epidemiology Biomarkers & Prevention 7, 385-390.
Macdonald, H. M., McGuigan, F. E., Stewart, A., Black, A. J., Fraser, W. D., Ralston, S. & Reid, D. M. (2006) Large-scale population-based study shows no evidence of association between common polymorphism of the VDR gene and BMD in British women. Journal of Bone and Mineral Research 21,151-162.
Marjanovic, E. J., Southern, H. N., Coates, P., Adams, J. E., Walsh, T., Horner, K. & Devlin, H. (2013) Do patients with osteoporosis have an increased prevalence of periodontal disease? A cross-sectional study. Osteoporosis International 24, 1973-1979.
Martelli, F. S., Martelli, M., Rosati, C. & Fanti, E. (2014) Vitamin D: relevance in dental practice. Clinical Cases In Mineral And Bone Metabolism 11, 15-19.
Martinez-Maestre, M. A., González-Cejudo, C., Machuca, G., Torrejón, R. & Castelo-Branco, C. (2010) Periodontitis and osteoporosis: a systematic review. Climacteric 13, 523-529.
Mohammad, A. R., Jones, J. D. & Brunsvold, M. A. (1994) Osteoporosis and periodontal disease: a review. Journal of California Dental Association 22, 69-75.
Morrison, N. A., Qi, J. C., Tokita, A., Kelly, P. J., Crofts, L., Nguyen, T. V., Sambrook, P.N. & Eisman, J. A. (1994) Prediction of bone density from vitamin D receptor alleles. Nature 367, 284-287.
Mostowska, A., Lianeri, M., Wudarski, M., Olesińska, M. & Jagodziński, P. P. (2013) Vitamin D receptor gene BsmI, FokI, ApaI and TaqI polymorphisms and the risk of systemic lupus erythematosus. Molecular Biology Reports 40, 803-810.
Nagpal, S., Na, S. & Rathnachalam, R. Noncalcemic actions of vitamin D receptor ligands. Endocrine Society 26, 662-687.
Naito, M., Miyaki, K., Naito, T., Zhang, L., Hoshi, K., Hara, A., Masaki, K., Tohyama, S., Muramatsu, M., Hamajima, N. & Nakayama, T. (2007) Association between vitamin D receptor gene haplotypes and chronic periodontitis among Japanese men. International Journal of Medical Sciences 4, 216-222.
Nibali, L., Parkar, M., D'Aiuto, F., Suvan, J. E., Brett, P. M., Griffiths, G. S., Rosin, M., Schwahn, C. & Tonetti, M. S. (2008) Vitamin D receptor polymorphism (-1056 Taq-I) interacts with smoking for the presence and progression of periodontitis. Journal of Clinical Periodontology 35, 561-567.
Page, R. C. & Kornman, K. S. (1997) The pathogenesis of h uman periodontitis: an introduction. Periodontology 2000 14, 9-11.

73
Park, K. S., Nam, J. H. & Choi, J. (2006) The short vitamin D receptor is associated with increased risk for generalized aggressive periodontitis. Journal of Clinical Periodontology 33, 524-528.
Pouresmaeili, F., Jamshidi, J., Azargashb, E. & Samangouee, S. (2013) Association between vitamin D receptor gene bsml polymorphism and bone mineral density in a population of 146 Iranian women. Cell Journal 15, 75-82.
Reddy, M. S. & Morgan, S. L. (2013) Decreased bone mineral density and periodontal management. Periodontology 2000 61, 195-218.
Stabholz, A., Soskolne, W. A. & Shapira, L. (2010) Genetic and environmental risk factors for chronic periodontitis and aggressive periodontitis. Periodontol 2000 53, 138-153.
Sun, J. L., Meng, H. X., Cao, C. F., Tachi, Y., Shinohara, M., Ueda, M., Imai, H. & Ohura, K. (2002) Relationship between vitamin D receptor gene polymorphism and periodontitis. Journal of Periodontal Research 37, 263–267.
Tachi, Y., Shimpuku, H., Nosaka, Y., Kawamura, T., Shinohara, M., Ueda, M., Imai, H., Ohura, K., Sun, J., Meng, H. & Cao, C. (2001) Association of vitamin D receptor gene polymorphism with periodontal diseases in Japanese and Chinese. Nucleic Acids Research 1, 111-112.
74
7 CONCLUSÃO
Com base na metodologia utilizada e a partir dos resultados obtidos,
pode-se concluir que:
1. Não houve associação significativa entre a doença
periodontal e os pacientes sem osteoporose, com osteopenia
e com osteoporose para o polimorfismo no gene IL1A -889.
2. Houve uma associação significativa entre o polimorfismo no
gene IL1B +3954 e os pacientes com osteoporose e com
doença periodontal, onde 50% dos indivíduos portadores do
genótipo CT apresentavam osteoporose e doença
periodontal, sugerindo que o genótipo CT do polimorfismo da
IL1B +3954 pode ser um fator de risco para à doença
periodontal e à osteoporose em uma amostra de idosos
Brasileiros.
3. Não houve associação significativa na frequência de
haplótipos, consistindo de pelo menos um alelo T do gene
IL1A -889 e um alelo T do gene IL1B +3954, entre os
indivíduos com doença periodontal e sem osteoporose e os
com osteopenia ou osteoporose.
4. Houve associação significativa entre o polimorfismo no gene
da IL6, a osteoporose e a doença periodontal entre os idosos
estudados.
5. Indivíduos com osteoporose e portadores do alelo G do gene
da IL6 apresentam maior suscetibilidade à doença
periodontal.
6. O alelo C do gene da IL6 conferiu 25% de proteção aos
indivíduos que abrigam este alelo em comparação aos que
possuíam o alelo G.
7. Indivíduos portadores do alelo G (genótipos GC e GG) do
gene da IL6 apresentaram maiores níveis plasmáticos da IL-6
em comparação a indivíduos não portadores deste alelo.
75
8. Os polimorfismos de nucleotídeos únicos TaqI, BsmI, ApaI e
FokI do gene VDR não mostraram diferença estatisticamente
significante entre os grupos controle e periodontite crônica.
9. O haplótipo TBAF construído a partir dos polimorfismos TaqI,
BsmI, ApaI e FokI do gene VDR está associado com a
prevalência da periodontite crônica em idosos Brasileiros.
10. Não observamos associação estatisticamente significante
entre periodontite e osteoporose.

76
REFERÊNCIAS
1. Instituto Brasileiro de Geografia e Estatística. Diretoria de Pesquisa. Coordenação de Trabalho e Rendimento. Pesquisa nacional por amostra de domicílios: síntese de indicadores 2005 [Internet] [acesso em 2015 jun 01]. Rio de Janeiro: IBGE, 2006. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/ trabalhoerendimento/pnad2005/sintesepnad2005.pdf.
2. Camarano AA, Kanso S, Mello JM. Como vive o idoso brasileiro? In. Camarano A A, org. Os novos idosos brasileiros: muito além dos 60? Rio de Janeiro: IPEA; 2004.
3. Pucca Jr. G A. Perfil do edentulismo e do uso de prótese dentária em idosos residentes no município de São Paulo [dissertação]. São Paulo: Universidade Federal de São Paulo/UNIFESP; 1998.
4. Reis SCG, Higino MASP, Melo HMD, Freire MCM. Condição de saúde bucal de idosos institucionalizados em Goiânia-GO, 2003. Rev. Bras. Epidemiol.2005 mar; 8(1): 67-73.
5. Rosa AGF, Fernandez RA, Pinto VG, Ramos LR. Condição de saúde bucal em pessoas de 60 anos ou mais no município de São Paulo (Brasil). Rev. Saúde Pública 1992;26(3): 155-60.
6. Bulgarelli AF, Manço AE. Idosos vivendo na comunidade e a satisfação com a própria saúde bucal. Ci. Saúde Col.2008 jul;3(4):1165-74.
7. Ogawa H, Yoshihara A, Hirotomi T, Ando Y, Miyazaki H. Risk factors for periodontal disease progression among elderly people. J Clin Periodontol. 2002 Jul;29(7):592-7.
8. Ministério da Saúde (BR). Projeto SB Brasil 2003: condição de saúde bucal da população brasileira 2002-2003: resultados principais [Internet] [acesso em 2015 junho 07]. Disponível em:http://www.nescon.medicina. ufmg.br/biblioteca/imagem/1720.pdf.
9. Ministério da Saúde (BR).SB Brasil 2010: Pesquisa Nacional de Saúde Bucal: resultados preliminares. [Internet] 2011. [acesso em 2014 mar 10]. Disponível em: http://dab.saude.gov.br/cnsb/.
10. Slade GD, Spencer AJ. Periodontal attachment loss among adults aged 60 π in South Australia. Community Dent Oral Epidemiol. 1995 Aug;23(4):237-42.
11. Brown LJ, Brunelle JA, Kingman A. Periodontal status in the United States. 1988-91: prevalence, extent, and demographic variation. J Dent Res. 1996 Feb;75 Spec n:672-83.
12. Ainamo J, Sarkki L, Kuhalampi ML, Palolampi L, Piirto O. The frequency of periodontal extractions in Finland. Community Dent Health. 1984 Nov;1(3):165-72.
77
13. Beck JD, Slade GD. Epidemiology of periodontal diseases. Curr Opin Periodontol. 1996;3:3-9.
14. Miyazaki H, Ohtani I, Abe N, Ansai T, Katoh Y, Sakao S et al. Periodontal conditions in older age cohorts aged 65 years and older in Japan, measured by CPITN and loss of attachment. Community Dent Health. 1995 Dec;12(4):216-20.
15. Bodet C, Chandad F, GrenierD. Porphyromonas gingivalis-induced inflammatory mediator profile in an ex vivo human whole blood model. Clin Exp Immuno. 2006 Jan;143(1): 50-7.
16. Liljenberg B, Lindhe J, Berglundh T, Dahlén G, Jonsson R. Some microbiological, histopathological and immunohistochemical characteristics of progressive periodontal disease. J Clin Periodontol. 1994 Nov;21(10):720-7.
17. Lindhe J. Tratado de periodontologia clínica e implantodontia. 3. ed. Rio de Janeiro: Guanabara Koogan; 1999.
18. Kinane DF, Shiba H, Hart TC. The genetic basis of periodontitis. Periodontol 2000. 2005;39:91-117.
19. Brett PM. Functional gene polymorphisms in aggressive and chronic periodontitis. J Dent Res. 2005 Dec;84(12):1149-53.
20. Laine ML, Loos BG, Crielaard, W. Gene polymorphisms in chronic periodontitis. Int J Dent. 2010:1-22.
21. Tabor HK, Risch NJ, Myers RM. Candidate-gene approaches for studying complex genetic traits: practical considerations. Nat Rev Genet. 2002 May;3(5):391-7.
22. Loos BG, ,John RP, Laine ML. Identification of genetic risk factors for periodontitis and possible mechanisms of action. J Clin Periodontol. 2005;32 Suppl 6:159-79.
23. Martínez-Maestre MÁ, González-Cejudo C, Machuca G, Torrejón R, Castelo-Branco C. Periodontitis and osteoporosis: a systematic review. Climacteric. 2010 Dec;13(6):523-9
24. Page RC, Kornman KS. The pathogenesis of human periodontitis: an introduction. Periodontol 2000. 1997 Jun;14:9-11.
25. Sanz M, van Winkelhoff AJ; Working Group 1 of Seventh European Workshop on Periodontology. Periodontal infections: understanding the complexity – Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011 Mar;38 Suppl 11:3-6.
26. Gomez RS, Dutra WO, Moreira PR. Epigenetics and periodontal disease: future perspectives Inflamm Res. 2009 Oct;58(10):625-9.
27. Page RC, Schroeder HE. Pathogenesis of inflammatory periodontal disease.
78
A summary of current work. Lab Invest. 1976 Mar;34(3):235-49.
28. Bartold PM, Van Dyke TE. Periodontitis: a host-mediated disruption of microbial homeostasis. Unlearning learned concepts. Periodontol 2000.2013 Jun; 62(1):203-17
29. Page RC, Offenbacher S, Schroeder HE, Seymour GJ, Kornman KS. Advances in the pathogenesis of periodontitis: summary of developments, clinical implications and future directions Periodontol 2000. 1997 Jun;14:216-48.
30. Kornman KS, Page R C, Tonetti, M. S. The host response to the microbial challenge in periodontitis: assembling the players. Periodontol 2000. 1997 Jun;14:33-53.
31. Johnson GK, Slach NA. Impact of tobacco use on periodontal status. J Dent Educ. 2001 Abr 65(4): 313-21.
32. Mealey BL. Diabetes and periodontal disease: two sides of a coin. Compend Contin Educ Dent. 2000 Nov;21(11):943-6.
33. Shen EC, Gau CH, Hsieh YD, Chang CY, Fu E. Periodontal status in post-menopausal osteoporosis: a preliminary clinical study in Taiwanese women J Chin Med Assoc. 2004 Aug;67(8):389-93.
34. Kim Yj, Viana A C, Scarel-Caminaga R M. Influência de fatores genéticos na etiopatogênese da doença periodontal. Rev. Odontol. UNESP. 2007; 36(2): 175-80.
35. Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000. 2013 Jun;62(1):59-94.
36. Stabholz A, Soskolne WA, Shapira, L. Genetic and environmental risk factors for chronic periodontitis and aggressive periodontitis. Periodontol 2000. 2010 Jun;53:138-53.
37. Kornman KS. Mapping the pathogenesis of periodontitis: a new look. J Periodontol. 2008 Aug;79(8 Suppl):1560-8.
38. Salvi GE, Lawrence HP, Offenbacher S, Beck JD. Influence of risk factors on the pathogenesis of periodontitis. Periodontol 2000. 1997 Jun;14:173-201.
39. Razzouk S, Termechi O. Host Genome, Epigenome, and Oral Microbiome Interactions: Toward Personalized Periodontal Therapy. J Periodontol. 2013 Sep;84(9):1266-71.
40. Diaz PI. Microbial diversity and interactions in subgingival biofilm communities. Front Oral Biol. 2012;15:17-40.
41. Ellis M, Gupta S, Galant S, Hakim S, VandeVen C, Toy C et al. Impaired neutrophil function in patients with AIDS or AIDS-related complex: a comprehensive evaluation. J Infect Dis. 1988 Dec;158(6):1268-76.

79
42. Taguchi A, Tanimoto K, Suei Y, Otani K, Wada T. Oral signs as indicators of possible osteoporosis in elderly women. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995 Nov;80(5):612-6.
43. Cashman, K. D. Diet, nutrition, and bone health. J Nutr. 2007 Nov;137(11 Suppl):2507S-2512S.
44. Genco RJ. Current view of risk factors for periodontal diseases. J Periodontol. 1996 Oct;67(10 Suppl):1041-9.
45. Wactawski-Wende J, Grossi SG, Trevisan M, Genco RJ, Tezal M, Dunford RG. et al. The role of osteopenia in oral bone loss and periodontal disease. J Periodontol. 1996 Oct;67(10 Suppl):1076-84.
46. Marjanovic EJ, Southern HN, Coates P, Adams JE, Walsh T, Horner K et al. Do patients with osteoporosis have an increased prevalence of periodontal disease? A cross-sectional study. Osteoporos Int. 2013 Jul;24(7):1973-9.
47. Baldock PA, Thomas GP, Hodge JM, Baker SU, Dressel U, O'Loughlin PD et al. Vitamin D action and regulation of boné remodeling: supression of osteoclastogenesis by the mature osteoblast. J Bone Miner Res. 2006 Oct;21(10):1618-26.
48. Hussien YM, Shehata A, Karam RA, Alzahrani SS, Magdy H, El-Shafey AM. Polymorphism in vitamin D receptor and osteoprotegerin genes in egyptian rheumatoid arthritis patients with and without osteoporosis. Mol Biol Rep. 2013 May;40(5):3675-80.
49. Lin NU, Malloy PJ, Sakati N, al-Ashwal A, Feldman D. A novel mutation in the deoxyribonucleic acid-binding domain of the vitamin D receptor causes hereditary 1,25-dihydroxyvitamin D-resistant rickets. J Clin Endocrinol Metab. 1996 Jul;81(7):2564-9.
50. Malloy PJ, Eccleshall TR, Gross C, Van Maldergem L, Bouillon R, Feldman D. Hereditary vitamin D resistant rickets caused by a novel mutation in the vitamin D receptor that results in decreased affinity for hormone and cellular hyporesponsiveness. J Clin Invest. 1997 Jan 15;99(2):297-304.
51. Oliveira, N. M. Papel da vitamina D na susceptibilidade para a diabete mellitus tipo 1 [dissertação]. Covilhã: Universidade da Beira Interior; 2010.
52. Barral D, Barros AC, Araújo RPC. Vitamina D: uma abordagem molecular. Pesq. Bras. Odontoped. Clin. Integr. 2007 set/dez; 7(3): 309-15.
53. Holick MF. Resurrection of vitamin D deficiency and rickets. J Clin Invest. 2006 Aug;116(8):2062-72.
54. Holick MF. Vitamin D deficiency. N Engl J Med. 2007 Jul 19;357(3):266-81.
55. Miyamoto K, Kesterson RA, Yamamoto H, Taketani Y, Nishiwaki E, Tatsumi S. et al. Structural organization of the human vitamin D receptor chromosomal gene and its promoter. Mol Endocrinol. 1997 Jul;11(8):1165-79.
80
56. Martelli FS, Martelli M, Rosati C, Fanti E. Vitamin D: relevance in dental practice. Clin Cases Miner Bone Metab. 2014 Jan-Apr; 11(1): 15–19.
57. Sun JL, Meng HX, Cao CF, Tachi Y, Shinohara M, Ueda M et al. Relationship between vitamin D receptor gene polymorphism and periodontitis. J Periodontal Res. 2002 Aug;37(4):263-7.
58. Horst-Sikorska W, Dytfeld J, Wawrzyniak A, Marcinkowska M, Michalak M, Franek E, Napiórkowska L, Drwęska N, Słomski R. Vitamin D receptor gene polymorphisms, boné mineral density and fractures in postmenopausal women with osteoporosis. Mol Biol Rep. 2013 Jan;40(1):383-90.
59. Pouresmaeili F, Jamshidi J, Azargashb E, Samangouee S.. Association between vitamin D receptor gene bsml polymorphism and bone mineral density in a population of 146 iranian women. Cell J. 2013 Spring;15(1):75-82.
60. Mostowska A, Lianeri M, Wudarski M, Olesińska M, Jagodziński PP. Vitamin D receptor gene BsmI, FokI, ApaI and TaqI polymophisms and the risk of systemic lúpus erythematosus. Mol Biol Rep. 2013 Feb;40(2):803-10.
61. Lima RM. Estudo de associação entre polimorfismos no gene receptor de vitamina D e massa livre de gordura em brasileiras pós-menopausadas [dissertação]. Brasília: Universidade Católica de Brasília;2006.
62. Borges-Osório MR, Robinson, WM. Genética humana. 2. ed. Porto Alegre: Artmed; 2001.
63. Schork NJ, Fallin D, Lanchbury JS. Single nucleotide polymorphisms and the future of genetic epidemiology. Clin Genet. 2000 Oct;58(4):250-64.
64. Hart TC, Kornman KS. Genetic factors in the pathogenesis of periodontitis. Periodontol 2000. 1997 Jun;14:202-15.
65. Monticielo OA. Estudo dos polimorfismos BsmI e FokI do receptor da vitamina D e avaliação dos níveis séricos da 25-Hidroxivitamina D em pacientes com lupus eritematoso sistêmico [tese].Porto Alegre: Universidade Federal do Rio Grande do Sul; 2011.
66. Khadilkar VV, Khadilkar AV. Use of vitamin d in various disorders. Indian J Pediatr. 2013 Mar;80(3):215-8.
67. Gross C, Eccleshall TR, Malloy PJ, Villa ML, Marcus R, Feldman D. The presence of a polymorphism at the translation initiation site of the vitamin D receptor gene is associated with low bone mineral density in postmenopausal Mexican American women. J Bone Miner Res 1996; 11:1850-1855.
68. Morrison NA, Qi JC, Tokita A, Kelly PJ, Crofts L, Nguyen TV, Sambrook PN, Eisman JA. Prediction of bone density from vitamin D receptor alleles. Nature. 1994; 367:284 287.
69. Froes NDTC, Pereira ES, Negrelli WF. Osteoporosis risk factors: prevention and detection through clinical and genetic monitoring. Acta Ortop Bras. 2002

81
Jan-Mar; 10(1):52-57.
70. Uitterlinden AG, Fang Y, Van Meurs JB, Pols HA, Van Leeuwen JP. Genetics and biology of vitamin D receptor polymorphisms. Gene. 2004 Sep; 338 (2):143-56.
71. Tachi Y, Shimpuku H, Nosaka Y, Kawamura T, Shinohara M, Ueda M et al. Association of vitamin D receptor gene polymorphism with periodontal diseases in Japanese and Chinese. Nucleic Acids Res Suppl. 2001;(1):111-2.
72. Nibali L, Parkar M, D'Aiuto F, Suvan JE, Brett PM, Griffiths GS, Rosin M et al. Vitamin D receptor polymorphism (-1056 Taq-I) interacts with smoking for the presence and progression of periodontitis. J Clin Periodontol. 2008 Jul;35(7):561-7.
73. Martelli FS, Mengoni A, Martelli M, Rosati C, Fanti E. VDR TaqI polymorphism is associated with chronic periodontitis in Italian population. Arch Oral Biol. 2011 Dec;56(12):1494-8.
74. Borges MAT, Figueiredo LC, Brito Jr RB, Faveri M, Feres M. Microbiological composition associated with vitamin D receptor gene polymorphism in chronic periodontitis. Braz Oral Res. 2009 Apr/June;23(2):203-8.
75. Hennig BJ, Parkhill JM, Chapple IL, Heasman PA, Taylor JJ. Association of a vitamin D receptor gene polymorphism with localized early-onset periodontal diseases J Periodontol. 1999 Sep;70(9):1032-8.
76. Krall, EA, Garcia R I, Dawson-Hughes B. Increased risk of tooth loss is related to bone loss at the whole body, hip, and spine. Calcif Tissue Int. 1996 Dec;59(6):433-7
77. Miley DD, Garcia MN, Hildebolt CF, Shannon WD, Couture RA, Anderson Spearie CL et al. Cross-sectional study of vitamin D and calcium supplementation effects on chronic periodontitis. J Periodontol. 2009 Sep;80(9):1433-9.
78. Oppenheim JJ, Ruscetti FW, Faltynek C. Citocianas. In: Stites DP, Terr AL, editores. Imunologia básica. Rio de Janeiro: Prentice-Hall; 1992.
79. Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent Jr RL. Microbial complexes in subgingival plaque. J Clin Periodontol. 1998 Feb;25(2):134-44.
80. Tervonen T, Raunio T, Knuuttila M, Karttunen R. Polymorphisms in the CD14 and IL-6 genes associated with periodontal disease. J Clin Periodontol. 2007 May;34(5):377-83.
81. Gore EA, Sandrers JJ, Pandey JP, Palesch Y, Galbraith GMP. Interleukine-1beta +3953 allele 2: association with disease status in adult periodontitis. J Clin Periodontol. 1998 Oct; 25(10):781-5.
82. Karimbux NY, Saraiya VM, Elangovan S, Allareddy V, Kinnunen T, Kornman KS et al. Interleukin-1 gene polymorphisms and chronic periodontitis in adult
82
whites: a systematic review and meta-analysis. J Periodontol. 2012 Nov;83(11):1407-19.
83. Klein W, Tromm A, Griga T, Fricke H, Folwaczny C, Hocke M. The polymorphism at position -174 of the IL-6 gene is not associated with inflammatory bowel disease. Eur J Gastroenterol Hepatol. 2001 Jan;13(1): 45-7.
84. Terry CF, Loukaci V, Green FR. Cooperative influence of genetic polymorphisms on interleukin 6 transcriptional regulation. J Biol Chem. 2000 Jun 16;275(24):18138-44.
85. Hughes FJ, Howells G. Interleukin-6 inhibits bone formation in vitro. Bone Miner. 1993 Apr; 21(1):21-28.
86. Irwin C R, Myrillas TT. The role of IL-6 in the pathogenesis of periodontal disease. Oral Dis. 1998 Mar;4(1):43-7.
87. Okada H, Murakami S. Cytokine expression in periodontal health and disease. Crit Rev Oral Biol Med. 1998;9(3):248-66.
88. Trevilatto PC, Scarel-Caminaga RM, Brito Jr RB, Souza AP, Sallum AW, Line SRP. Polymorphism at position -174 of IL-6 gene is associated with susceptibility to chronic periodontitis in a Caucasian Brazilian population. Braz J Oral Sci. 2003 Oct./Dec; 2(7):(5):348-52.
89. Dentino A, Lee S,Mailhot J,Hefti AF. Principles of periodontology. Periodontol 2000. 2013 Feb;61(1):16-53.
90. Grant MM. What do ’omic technologies have to offer periodontal clinical practice in the future? J Periodontal Res. 2012 Feb;47(1):2-14.
91. Chen R, Mias GI, Li-Pook-Than J, Jiang L, Lam HY, Chen R. et al. Personal omics profiling reveals dynamic molecular and medical phenotypes. Cambridge, Cell. 2012 Mar;148(6):1293-1307.
92. Frank MO, Mandell GL. Adjuncts to antibacterial therapy. Infect Dis Clin North Am. 1995 Sep;9(3):769-81.

83
ANEXOS
84
ANEXO A - Parecer do Comitê de Ética em Pesquisa da UNOPAR

85
ANEXO B – Ficha de exame – Condições bucais
INFORMAÇÕES GERAIS NO. IDENTIFICAÇÃO :__________ NOME:_______________________________________ IDADE: SEXO: 1.MASC 2.FEM CÁRIE DENTÁRIA E NECESSIDADE DE TRATAMENTO
COROA RAIZ TRAT. COROA RAIZ TRAT EDENTULISMO USO DE PRÓTESE NECESSIDADE DE PRÓTESE TEMPO DE USO SUP. INF. SUP. INF. SUP: ____________ INF:_____________ CONDIÇÃO PERIODONTAL CPI
17/16 11 26/27 17/16 11 26/27 17/16 11 26/27
47/46 31 36/37 47/46 31 36/37 47/46 31 36/37 17/16 11 26/27 PIP 47/46 31 36/37
18 17 16 15 14 13 12 11 21 22 23 24 25 26 27 28
48 47 46 45 44 43 42 41 31 32 33 34 35 36 37 38
SANGRAMENTO GENGIVAL
CÁLCULO DENTÁRIO
BOLSA
PERIODONTAL
DATA: ___/___/____ EXAMINADOR:____________ ANOTADOR:______________


















