Manejo Perioperatorio de los...
40
Manejo Perioperatorio de los Antiplaquetarios José Luis Ferreiro Hospital Universitario de Bellvitge: Área de Enfermedades del Corazón Unidad de Cardiología Intervencionista - Laboratorio de Investigación Cardiovascular Nuevos antiagregantes en SCA. ¿Cómo gestionar el cambio? Madrid, 15 de junio
Transcript of Manejo Perioperatorio de los...

Manejo Perioperatorio de los
Antiplaquetarios
José Luis Ferreiro
Hospital Universitario de Bellvitge: Área de Enfermedades del Corazón
Unidad de Cardiología Intervencionista - Laboratorio de Investigación Cardiovascular
Nuevos antiagregantes en SCA. ¿Cómo gestionar el cambio? Madrid, 15 de junio

CONFLICTOS DE INTERÉS
Honorarios por conferencias: Eli Lilly Co; Daiichi Sankyo, Inc.; AstraZeneca; Grifols
Becas: Sociedad Española de Cardiología

ÍNDICE
Recomendaciones generales
Nuevos agentes
¿Siempre hay que suspender el tto
antiagregante el tiempo recomendado?

RECOMENDACIONES
GENERALES

DURATION OF DAPT IN STENTED PATIENTS
ESC guidelines: ACS: 1 year (irrespective of type of stent)
Stable patient – BMS: 1 month
DES: 6-12 months
ACC/AHA guidelines: ACS: At least 12 months
Non-ACS BMS: 1 month and ideally up to 12 months
Non-ACS DES: at least 12 months (if not high risk of
bleeding)

MAJOR SURGERY AFTER PCI
Incidence of major surgery within 1 year after
stent implantation ≈5%
Savonitto S et al. J Thromb Haemost. 2011;9:2133-42.

INCIDENCE, PREDICTORS, AND OUTCOME OF
THROMBOSIS AFTER DES
Univariate Predictors of Cumulative Stent Thrombosis
0 10 20 30 40
Incidence of Stent Thrombosis
Premature Antiplatelet Therapy Discontinuation
Prior Brachytherapy
Renal Failure
Bifurcation with 2 Stents
Bifurcation Lesion
Unprotected Left Main Artery
Diabetes
Hazard Ratio for ATP Discontinuation = 89
What does premature really mean?
Iakovou I et al. JAMA. 2005;293:2126-30.

ASPIRIN AND CABG
After CABG (48 hours)
Preoperative aspirin (5 days)
Bybee KA et al. Circulation. 2005 Mangano D et al. N Engl J Med. 2002.

PERIOPERATIVE DISCONTINUATION OF
THIENOPYRIDINES AND MACE
Iakovou I et al. JAMA. 2005;293:2126-30.

COMMON SENSE
Knowing the patient needs surgery… No stent: CABG, medical therapy…
If completely necessary: BMS
Once the patient is stented… Elective surgery: Wait until completion of DAPT
Semi-elective / Urgent: Wait as much as possible
Emergent: Surgery
The less common of the senses...

ESC GUIDELINES: RECOMMENDATIONS
Wijns W et al. Eur Heart J. 2010;31:2501-55.

ESC WG THROMBOSIS: RECOMMENDATIONS
Korte W et al. Thromb Haemost. 2011;105:743-9.

IF YOU NEED TO STOP…
Clopidogrel: 5 days
Prasugrel: 7 days
Ticagrelor: 5 days
Bridging therapy with tirofiban Only reports of case series
?

NUEVOS FÁRMACOS
ANTIPLAQUETARIOS

Clopidogrel Prasugrel Ticagrelor Cangrelor Elinogrel
Group Thienopyridine Thienopyridine CPTP ATP analog Quinazolinedione
Administration oral oral oral IV IV and oral
Receptor
blockade irreversible irreversible reversible reversible reversible
Onset of action 2-8 h 30 min-4 h 30 min – 2 h seconds seconds
Offset of action 7-10 days 7-10 days 3-5 days 60-90 minutes 50 min (IV)
12 h (oral)
CYP drug
interactions yes no yes no no
P2Y12 INHIBITORS
Modified from Angiolillo DJ and Ferreiro JL. Rev Esp Cardiol 2010;63:60-76
More potent with less variability

16
Prasugrel Binding to P2Y12

17
Hepatic
metabolism
Clopidogrel
N
S Cl
COOCH3
CYP 3A4(5)
CYP 2C9
CYP 2C19
CYP 2B6
CYP 1A2
CYP 2B6
CYP 2C19
Inactive Metabolites
(85% clopidogrel)
Esterases
CLOPIDOGREL: METABOLISM
Active Metabolite
HOOC
* HS
N
O
Cl
OCH3
CH3
O N
S
O
Cl
O C
2-oxo compound
Hepatic
metabolism

18
N
S
O
C H3 C O
F
O
Prasugrel
Pre-hepatic metabolism Blood and intestine esterases
N
S
O
F
O
HOOC
* HS
N
O
F
2-oxo compound
Active Metabolite
Hepatic metabolism
CYP 3A4(5)
CYP 2C9
CYP 2C19
CYP 2B6
PRASUGREL: METABOLISM

Sugidachi A et al. J Thromb Haemost 2007;5:1545–51.
Concentration (mM)
*
** **
** **
**
** **
0 1 10 100 0
20
40
60
80 P
late
let
ag
gre
gati
on
(%
)
1000
Prasugrel active metabolite Clopidogrel active metabolite
Prasugrel 60 mg Clopidogrel 300 mg
Time from administration (h) 0 6 12 18 24
Pla
sm
ati
c c
on
cen
trati
on
(n
g/m
L)
0.1
1
10
100
1000
ACTIVE METABOLITE
Payne CD et al. J Cardiovasc Pharmacol 2007;50:555-562.
More efficient generation of active metabolite

PRASUGREL:
RAPID ONSET OF ACTION AND GREATER IPA
mean ± SEM
20 μM ADP
Inh
ibit
ion
of
Pla
tele
t A
gg
reg
ati
on
(%
)
0
20
40
60
80
100
Loading dose Maintenance dose
Hours Days
0.25 0.5 1 2 4 6 24 3 4 5 6 7 8 9 0
Clop 300 mg
Clop 75 mg
!
Clop 600 mg
Clop 75 mg
Pras 60 mg
Pras 10 mg
Payne CD et al. J Cardiovasc Pharmacol 2007;50:555-562

PRASUGREL: CABG
Wiviott SD et al. NEJM 2007;357:2001-15.

Smith PK et al. J Am Coll Cardiol. 2012 [Epub ahead of print]
PRASUGREL: CABG
Protection in front of ischemic events???

23
Ticagrelor Binding to P2Y12

TICAGRELOR
Direct acting: Hepatic metabolism not
required for activity
Rapid intestinal absorption
Reversible binding to P2Y12
receptor (different site than ADP): half life ~8 h
Adapted from Husted S et al. Cardiovasc Ther. 2009;27:259-274.
A non-thienopyridine, in the chemical class CPTP (CycloPentylTriazoloPyrimidine)
HO
HN
HO OH
O S
F
F
N
N N
N N
Active metabolite: AR-C124910XX (half-life ~10 hours) accounts
for ~30% to 40% of total activity

Gurbel PA et al. Circulation. 2009;120:2577-85.
TICAGRELOR:
RAPID ONSET / OFFSET & GREATER IPA

0%
20%
40%
60%
80%
100%
1 2 3 4 5 6 7 >8
Ticagrelor Clopidogrel
Major Fatal/Life-Threatening Bleeding by Days from Last Dose of
Treatment to CABG
% P
atie
nts
with
Ble
ed
ing
post-
CA
BG
Days
Bleeding differences favor ticagrelor >5 days post discontinuation
TICAGRELOR: CABG
Held C. J Am Coll Cardiol. 2011;57:672-84.

TICAGRELOR: CABG
Held C. J Am Coll Cardiol. 2011;57:672-84.
Protection in front of ischemic events???

van Giezen JJJ, Humphries RG. Semin Thromb Hemost. 2005;31:195-204.
4Na+
O
HO OH
O P
O P
O P
O–
O O O
O– O–
–O N
N N
NH2
N
ATP
P O
P P
O–
O O O
O– O–
–O
Cl
Cl O
HO OH
O N
N N
HN
N
SMe
S CF3
4Na+
Cangrelor (IV)
CANGRELOR: ATP ANALOG
HO O
OH OH
N
N
N S F
F F
N
HN
S
ATP analog
Direct-acting P2Y12 antagonist
Reversible receptor binding
No hepatic or renal metabolisation: NO interactions
Extremely short half-life: 2-5 minutes
Instant onset of action: steady-state in 30 minutes
Platelet function recovered in 60-90 minutes
Great IPA: >90%

Recovery time
~60 minutes
CANGRELOR: PHARMACODYNAMICS
dose 30ug/kg then 4ug/kg/min
Concentr
ation (
ng/m
L)
% P
late
let A
ctivity
Time (minutes)
Platelet activity
Plasma concentration
infusion bolus
Akers et al. J Clin Pharmacol. 2010;50:27-35

Primary endpoint
Percent of patients with PRU<240 for all on-treatment samples:
30
98,8%
19,0%
0%
20%
40%
60%
80%
100%
Cangrelor Placebo
p<0.0001
OR (95% CI)
353 (45.6-2728)
CANGRELOR: BRIDGE
Angiolillo DJ et al. JAMA 2012;307:265-74.

0
50
100
150
200
250
300
350
400
Baseline Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Last
on-infusion
sample
Pre-CABG
sample
Time Point
n=80 n=70
n=55 n=33 n=7
n=1
n=6
n=85
n=84
n=78
Cangrelor Placebo
Verify
Now
PR
U
N indicates number of patients with valid samples in the intention to treat population; PRU= P2Y12 reaction units; Data expressed as mean±SD
CANGRELOR PRE-CABG
n=76 n=73
n=57 n=34 n=24
n=14 n=86
n=2 n=84
n=75
11,8%
10,4%
0%
5%
10%
15%
Cangrelor Placebo
Excessive CABG-related bleeding
Angiolillo DJ et al. JAMA 2012;307:265-74.
Patients with an ACS or treated with a coronary stent (BMS or DES) on a thienopyridine awaiting CABG.

¿SIEMPRE HAY QUE SUSPENDER
LOS ANTIAGREGANTES EL
TIEMPO RECOMENDADO?

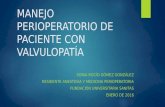
CLOPIDOGREL: OFFSET OF ACTION
Price MJ et al. Am J Cardiol. 2008;102:790-5.

CLOPIDOGREL: TIME TO CABG TARGET-CABG: Primary Endpoint: 24 hr Chest Tube Output
0
500
1000
1500
2000
2500
3000
3500
mL
Clopidogrel naïve (n=86)
On Clopidogrel (n=94)
4 hrs postop 12 hrs postop 24 hrs postop
p = NS p = NS p = NS
Clopidogrel responsiveness (ADP-induced
platelet-fibrin clot strength [MAADP]) was
determined by TEG.
CABG was done within 1 day,
3–5 days, and 5 days in patients with an
MAADP >50 mm, >35–50 mm, and >35 mm,
respectively.
Waiting times to CABG
reduced by ~50% than
recommended in guidelines.
Mahlla E, Gurbel PA et al. Circ Cardiovasc Interv 2012 [in press]

¿¿Sirve la misma talla para
todo el mundo??
Tratamiento
“individualizado”

THERAPEUTIC WINDOW
Inhibition of platelet aggregation
High risk of
ischemic events
High risk of
bleeding events “Sweet spot”
Ischemic risk Bleeding risk Ischemic risk Bleeding risk
Ferreiro JL, Sibbing D & Angiolillo DJl. Thromb Haemost 2010;103:1128-35.
The lower the bleeding risk, the higher the ischemic risk

CONCLUSIONES

CONCLUSIONES Usar el sentido común en pacientes con stent:
Cirugía electiva: Esperar hasta completar DAPT
Semi-electiva / Urgente: Esperar lo que sea posible (individualizar)
Emergente: Cirugía
Considerar mantener DAPT en cirugía de bajo riesgo
Mantener AAS excepto en situaciones de riesgo de sangrado extremedamente alto
Si hay que suspender, como regla general: Clopidogrel: 5 días
Prasugrel: 7 días
Ticagrelor: 5 días
Tests de función plaquetar pueden ayudar a individualizar

GRACIAS POR SU ATENCIÓN