Malaria
52
In Hajjis &Returned Travelers
Transcript of Malaria

In Hajjis &Returned Travelers

Dr. Satti M. SalehChief of Infectious Diseases Department MGH
Director of IC Unit Meeqat General hospital CBAHI SIT Member
Medical Director Meeqat General Hospital

.


KNOWLEDGE OF THE INFECTING SPECIES
THE LIKELY LOCATION OF INFECTIONGEOGRAPHIC PATTERNS OF DRUG RESISTANCEIF THERE IS ANY DOUBT (TREAT FOR THE WORSE – CASE SCENARIO)CONSIDER ANY FEBRILE ILLNESS FROM MALARIOUS AREA TO BE MEDICAL EMERGENCYCOMPLY WITH TREATMENT GOAL


DEFINITIONmalaria is an acute and chronic disease caused by Protozoa of the genus Plasmodium .

FOUR SPECIES CAUSING HUMAN MALARIA:-
A- Plasmodium Malariae ( Loveran 1881 )B- Plasmodium Vivax ( GRASSI 1981)C- Plasmodium Flaciparum ( Welch 1897)D- Plasmodium Ovale ( Stephens 1922 )
)

300 – 500 million case each year* 3.5 Million death ( Unnecessary

LIFE CYCLE
Life cycle

CLINICAL DIAGNOSIS:- A- HISTORY * TRAVEL TO ENDEMIC AREA WHERE / WHEN* WAS MALARIA DIAGNOSED BEFORE * WHAT MEDICATIONS CHEMO-PROPHYLAXIS* H/O BLOOD TRANSFUSION OR USAGE OF NON-STERILE NEEDLE * ASSOCIATED MEDICAL PROBLEMS

- Cough, fatigue, malaise, shaking chills arthralgia, myalgia.Paroxysms of fever, shaking chills and sweating - no classic paroxysm- maintain a high index of suspension- anorexia, lethargy, nausea, vomiting, diarrhoea, headache.
SYMPTOMS:-

Complications:-A- CEREBRAL MALARIA - coma, altered mental status or multiple seizures with PF in blood- main cause of death in malaria - 15-20 % MortalityB- Seizures C- Renal failure 30% of non-immune adultD- Black water feverHaemolysis, Haemoglobinaemia, Hemoglobinnuria.

E.NON CARDIOGENIC PULMONARY OEDEMA;most common with pregnancy;80% mortalityF. Hypoglycemia Mostly in children and pregnancy- QUININE THERAPY- difficult to diagnose
Lack of adrenergic signs Stupor G. Lactic Acidosis poor prognosis (venous lactate45mg/dl)

H. Anaemia Infected RBCs -haemolysis non-infected RBCs- Dyserythropoeisis- Hypersplenism

LAB. STUDIES
- CBC,electrolytes panel,renal function- Imaging studies- C X-ray- CT

PARASITOLOGICAL TEST:-- thin blood smear- thick blood smear- parasitaemia rate- every 12 hoursOTHERS TEST:- polymerase chain reaction- specific * sensitive- Detect parasitaemia as low as 10 parasites /ml.

-Antigen detection Technique – PFHRP2-fluorescent staining of parasite nuclei- malarial antibody test


stay alert

Criteria for anti malaria treatment policy change ( a change of 1st line treatment) If the total failure proportion > 10 % (12
% in Jazan 2001) Additional factor : the prevalence and
geographical distribution of reported treatment failures (neighboring Yemen)
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 21

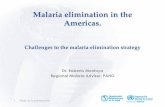
بمنطقة والخبيثة الحميدة المالريا لحاالت بياني تخطيطالمنورة المدينة
من الفترة 1/7/2016وحتى ------ 1/1/2016في ΓέϭϧϣϟΔϧϳΩϣϟΔϘρϧϣΑΔΛϳΑΧϟϭΓΩϳϣΣϟΎϳέϼϣϟΕϻΎΣϟϲϧΎϳΑρϳρΧΗ ϥϣΓέΗϔϟ ϲϓ˺/˺/˻ ˹ ˺ ˿ϰΗΣϭ ------ ˺/̀;/˻ ˹ ˺ ˿
0
2
4
6
8
10
12
έϳΎϧϳ έϳέΑϓ α έΎϣ ϝϳέΑ ϭϳΎϣ ϭϳϧϭϳ
vivax
falciparm
total

2010 20110
20
40
60
80
100
120
140
160
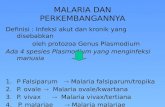
المنورة المدينة منطقة ريا المال حاالتيوليو 2011 ---- 2010 حتى

الميقات بمستشفى المنومة المالريا حاالت يوضح بياني رسمالعام
من الفترة 1/11/1437وحتى------- 1/1/1437في
ϡΎόϟΕΎϘϳϣϟϰϔηΗγϣΑΔϣϭϧϣϟΎϳέϼϣϟΕϻΎΣ ο ϭϳϲϧΎϳΑϡγέ ϥϣΓέΗϔϟ ϲϓ˺/˺/˺ ˽ ˼ ; ˹ϰΗΣϭ -------˺/˺ ˺/˺ ˽ ˼ ;
0
5
10
15
20
25
30
35
falciparm vivax
ΔϠγϠγ˺
Ωϭϣϋ˺
Ωϭϣϋ˻

Goals Early and correct diagnosis Prompt and effective treatment of all
confirmed and highly suspected cases Prevent the emergence and spread of
resistance to Antimalarial drugs Reduction / interruption of transmission Prevention of relapses in P. vivax and P.
ovale infection
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 25

First – line treatmentArtesunate + Sulfadoxine – Pyrimethamine
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 26

First – line treatment Artesunate + Sulfadoxine – Pyrimetheramine
Currently available as separate scored tablets containing 50 mg of artesunate, and tablets containing 500 mg sulfadoxine + 25 mg pyrimetheramine.
The total recommended dose is 4 mg/kg bw artesunate once a day , and a single administration of sulfadoxine-pyrimthamine (25/1.25 mg base / kg bw) on day -1
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 27

Sulfadoxine- pyrimethamine (500 /25)
Artesunate 50 mg tablets
Age (years) Weight (kg)
Day 1 Day 3 Day 2 Day 1
1/2 1/2 1/2 1/2 Infants 5-10
1 1 1 1 ≤1- <7 > 10-24
2 2 2 2 ≤ 7- 13 >24-50
3 4 4 4 > 13 >50
Reference: guideline for malaria treatment, WHO, 2006
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 28

Management of treatment failure
Early treatment failure (EFT) Late clinical failure (LCF) Late parasitological failure
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 29

Definition of treatment failure
Failure to resolve or recurrence of fever and/or parasitemia within 28 days of the start of treatment
Can be divided to : early and late
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 30

Early treatment failure (EFT) Development of danger signs or severe
malaria on Day 1, Day 2, Day 3, in the presence of parasitemia
Parasitemia on Day 2 higher than Day 0 count irrespective of axillary temperature
Parasitemia on Day 3 with axillary temperature ≥ 37.5˚
Parasitemia on Day 3 ≥ 25 % of count on Day 0
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 31

Late clinical failure (LCF) Development of danger signs or severe
malaria after Day 3 in the presence of parasitemia, without previously meeting any of the criteria of early treatment failure
Presence of parasitemia and axillary temperature ≥ 37.5˚ on any day from Day 4 to Day 28, without previously meeting any of the criteria of Early Treatment Failure
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 32

Late parasitological failure Presence of parasitemia on any day
from Day 7 to Day 28 and axillary temperature < 37.5 ˚ without previously meeting any of the criteria of Early Treatment Failure or Late Clinical Failure
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 33

Second – line treatment
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 34

Artemether – Lumefantrine (Coartem)
Tablets contain 20 mg of artemether and 120 mg of lumefantrine
The total recommended treatment is a six-dose regimen of artemether-lumefantrine twice daily for 3 days
Advantage of the combination: lumefantrine is not available it is recommended for patients > 5 kg
Inform the patient to take it with fat-containing food particularly on the second and third days of treatment ( absorption of lumefantrine is enhanced by co-administration with fat
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 35

Content of Artemether (AM)+Lumefantrine(LM) per dose
Number of tablets per dose (at 0h, 8h, 24h, 36h, 48h, 60h)
Age in years
Weight (kg)
Not recommended < 5
20 mg A + 120 mg L
1 <3 5-14
40 mg A + 240 mg L
2 ≤ 3-8 >14-24
60 mg A + 360 mg L
3 > 8-14 >24-34
80mg A + 480 mg L
4 > 14 >34
DOSAGE
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 36

Management of malaria in pregnancyMalaria in pregnancy is associated with
(abortion, stillbirth, low birth weight, increased anemia, increased risk of severe malaria- in low transmission areas)
1st trimester: Quinine + Clindamycin to be given for 7 days
ACT should be used if it is the only effective treatment available
2nd and 3rd trimesters: ACT
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 37

Treatment of severe and complicated malaria
Severe and complicated malaria is a true emergency associated with severe multi systemic complications, warranting ICU care for close monitoring and subsequent management

Management should include
If severe or complicated malaria is anticipated, empiric treatment should be started without any delay.Parenteral ARTESUNATE is the first drug of choice for the treatment of severe and complicated malaria unless otherwise contraindicated i.e. first trimester of pregnancy. Quinine is the second drug of choice in severe and complicated malaria

Artesunate 2.4 mg/kg i.v. or i.m. given on: admission (time = 0) At 12 hours Then Once daily for 7 days SHIFT TO ORAL route immediately
when the patient’s condition permits
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 40

Quinine Dihydrochloride 20 mg/kg loading dose in 5 % dextrose over 4
hours followed by 10 mg/kg over 4 hours / 8 hours (Max. 1800 mg/day) for 7 days.
The treatment should be SHIFTER TO ORAL quinine (10 mg/kg every 8 h.) as soon as tolerated
A 7 days course of Doxycycline should be given in order to ensure complete cure
Start dose is 200 mg then daily 100 mg for 7 days C.I: pregnants, children < 8 y. age (use
Clindamycin 300 mg 4 times / day for 5 days)
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 41

Management of malaria in lactating women
Special care should be taken when prescribing any antimalarial to a lactating woman (although amount in breast milk are relatively few)
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 42

Management of malaria in infants Malaria is common in infants and under 2 y.
of age in endemic areas with high case-fatality rate
Start Antimalarials immediately in case of suspicion
Accurate diagnosis is important Artemisinin derivatives appear to be safe
and well tolerated
05/01/2023NATIONAL POLICY OF MALARIA CASE
MANAGEMENT IN KSA 43

Choosing a Drug to Prevent Malaria

drug for malaria prophylaxisRecommendations for drugs to prevent malaria differ by country of travel and can be found in the of the Yellow Book. Recommended drugs for each country are listed in alphabetical order and have comparable efficacy in that country.No antimalarial drug is 100% protective and must be combined with the use of personal protective measures, (i.e., insect repellent, long sleeves, long pants, sleeping in a mosquito-free setting or using an insecticide-treated bednet).For all medicines, also consider the possibility of drug-drug interactions with other medicines that the person might be taking as well as other medical contraindications, such as drug allergies.When several different drugs are recommended for an area, the following table might help in the decision process

Atovaquone/Proguanil (Malarone)
Reasons that might make you consider using this drug Reasons that might make you avoid using this drug
Good for last-minute travelers because the drug is started 1-2 days before traveling to an area where malaria transmission occurs
Some people prefer to take a daily medicine
Good choice for shorter trips because you only have to take the medicine for 7 days after traveling rather than 4 weeks
Very well tolerated medicine – side effects uncommon
Pediatric tablets are available and may be more convenient
Cannot be used by women who are pregnant or breastfeeding a child less than 5 kg
Cannot be taken by people with severe renal impairment
Tends to be more expensive than some of the other options (especially for trips of long duration)
Some people (including children) would rather not take a medicine every day

Chloroquine Some people would rather take
medicine weekly Good choice for long trips because
it is taken only weekly Some people are already taking
hydroxychloroquine chronically for rheumatologic conditions. In those instances, they may not have to take an additional medicine
Can be used in all trimesters of pregnancy
Cannot be used in areas with chloroquine or mefloquine resistance
May exacerbate psoriasis Some people would rather not take
a weekly medication For trips of short duration, some
people would rather not take medication for 4 weeks after travel
Not a good choice for last-minute travelers because drug needs to be started 1-2 weeks prior to travel

Mefloquine(Lariam)
Some people would rather take medicine weekly
Good choice for long trips because it is taken only weekly
Can be used during pregnancy
Cannot be used in areas with mefloquine resistance
Cannot be used in patients with certain psychiatric conditions
Cannot be used in patients with a seizure disorder
Not recommended for persons with cardiac conduction abnormalities
Not a good choice for last-minute travelers because drug needs to be started at least 2 weeks prior to travel
Some people would rather not take a weekly medication
For trips of short duration, some people would rather not take medication for 4 weeks after travel

Primaquine It is the most effective medicine for
preventing P. vivax and so it is a good choice for travel to places with > 90% P. vivax
Good choice for shorter trips because you only have to take the medicine for 7 days after traveling rather than 4 weeks
Good for last-minute travelers because the drug is started 1-2 days before traveling to an area where malaria transmission occurs
Some people prefer to take a daily medicine
Cannot be used in patients with glucose-6-phosphatase dehydrogenase (G6PD) deficiency
Cannot be used in patients who have not been tested for G6PD deficiency
There are costs and delays associated with getting a G6PD test done; however, it only has to be done once. Once a normal G6PD level is verified and documented, the test does not have to be repeated the next time primaquine is considered
Cannot be used by pregnant women
Cannot be used by women who are breastfeeding unless the infant has also been tested for G6PD deficiency
Some people (including children) would rather not take a medicine every day
Some people are concerned about the potential of getting an upset stomach from primaquine

Doxycycline
Some people prefer to take a daily medicineGood for last-minute travelers because the drug is started 1-2 days before traveling to an area where malaria transmission occursTends to be the least expensive antimalarialSome people are already taking doxycycline chronically for prevention of acne. In those instances, they do not have to take an additional medicineDoxycycline also can prevent some additional infections
Cannot be used by pregnant women and children <8 years oldSome people would rather not take a medicine every dayFor trips of short duration, some people would rather not take medication for 4 weeks after travelWomen prone to getting vaginal yeast infections when taking antibiotics may prefer taking a different medicinePersons planning on considerable sun exposure may want to avoid the increased risk of sun sensitivitySome people are concerned about the potential of getting an upset stomach from doxycycline


Choosing a Drug to Prevent Malaria